

Abstract
Introduction
Cystectomy is the last treatment option for Hunner‐type interstitial cystitis. However, consensus regarding optimal patient selection or treatment approaches is lacking.
Case presentation
A 27‐year‐old woman presented to a regional hospital with bladder pain and frequent urination. Antimicrobial therapy was administered; however, her symptoms persisted and she was finally diagnosed with HIC. Multiple endoscopic fulgurations of Hunner's lesions with bladder hydrodistension or intravesical therapy were performed; however, the symptoms persisted. A urethral catheter was inserted 1 month before she visited our clinic because of a severely contracted bladder. We performed female pelvic organ‐preserving robot‐assisted simple cystectomy and intracorporeal ileal neobladder reconstruction. The patient's postoperative course was uneventful and her symptoms resolved.
Conclusion
This is the first report of pelvic organ‐preserving robot‐assisted simple cystectomy and intracorporeal ileal neobladder reconstruction in a young woman with HIC.
Keywords: Hunner‐type interstitial cystitis, intracorporeal neobladder, robot‐assisted cystectomy
Abbreviations & Acronyms
- HIC
Hunner‐type interstitial cystitis
- IC/BPS
Interstitial cystitis/bladder pain syndrome
Keynote message.
Reconstructive surgery is considered for patients with refractory HIC. However, there is a lack of consensus regarding the optimal patient selection or treatment approaches. To the best of our knowledge, this is the first reported case of HIC that was treated with robot‐assisted cystectomy. In young women with refractory HIC, pelvic organ‐preserved robot‐assisted cystectomy and an intracorporeal neobladder may be the optimal treatment option.
Introduction
IC/BPS is a chronic disease characterized by suprapubic pain and lower urinary tract symptoms, in the absence of infection or other identifiable causes. IC/BPS is divided into HIC and BPS. HIC shows characteristic cystoscopic findings of severe inflammatory changes and histopathological epithelial denudation, whereas BPS lacks these characteristics. 1 , 2
If Hunner‐type lesions are detected by cystoscopy, submucosal injections of corticosteroids and/or fulguration can be performed. Oral cyclosporine A and/or other multimodal therapies may be offered to patients with HIC who are unresponsive to corticosteroid injections and fulguration. 2 , 3 However, intractable bladder pain and associated lower urinary tract symptoms may persist even after repeated fulguration sessions. Major surgeries such as substitution cystoplasty or urinary diversion with or without cystectomy are the last treatment options for intractable and/or severely contracted bladders. 2 Approximately 10% of patients with IC/BPS have irreversible end‐stage disease that requires surgical therapy. 4 However, to date, optimal patient selection and standardized surgical procedures have not been established. 5 Here we describe the first case of a young woman with HIC who underwent pelvic organ‐preserving robot‐assisted simple cystectomy and intracorporeal ileal neobladder reconstruction.
Case report
A 27‐year‐old woman presented to a regional hospital with a 2‐year history of bladder pain and frequent urination. She was diagnosed with acute cystitis for which antibiotics were administered; however, her symptoms persisted without valid HIC treatment. The patient was diagnosed as having HIC at another hospital. Multiple endoscopic fulgurations of Hunner's lesions with bladder hydrodistension and intravesical therapy with corticosteroids were performed; however, the symptoms persisted. She was admitted to the hospital with acute pyelonephritis and postrenal dysfunction due to a severely contracted bladder, 1 month before visiting our clinic. A urethral catheter was inserted and the patient was referred to our hospital.
With hospital ethics committee approval, due to recurrent pyelonephritis caused by obstruction of the urethral catheter and high intraluminal bladder pressure (Fig. 1), we performed a female pelvic organ‐preserving robot‐assisted simple cystectomy and intracorporeal ileal neobladder reconstruction, according to a previous report. 6 As for a cystectomy briefly, the anterior vaginal wall was dissected off the posterior wall of the bladder toward the pelvic floor by putting a sponge in the vagina to ensure the line, and the bladder pedicles were isolated and divided near the bladder at the nearest line as possible. The bladder–urethral junction was easily identified and the urethra was dissected at the nearest line of the bladder neck.
Fig. 1.
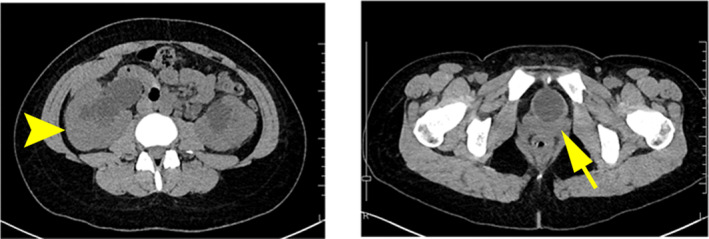
Computed tomography images show bilateral hydronephrosis (arrowhead) and contracted bladder (arrow).
The operation time was 12 h and 30 min, and the blood loss was 1213 mL (including urine).
The bladder contracted severely and the retroperitoneal space around the bladder, together with the bilateral ureters, showed inflammatory changes. During cystectomy, as much of the peritoneum as possible is preserved to cover the neobladder for retroperitoneal application. Histological examination revealed severe urothelial denudation and lymphocyte infiltration in the submucosal layer of the bladder (Fig. 2a), along with bladder wall fibrosis (Fig. 2b,c).
Fig. 2.
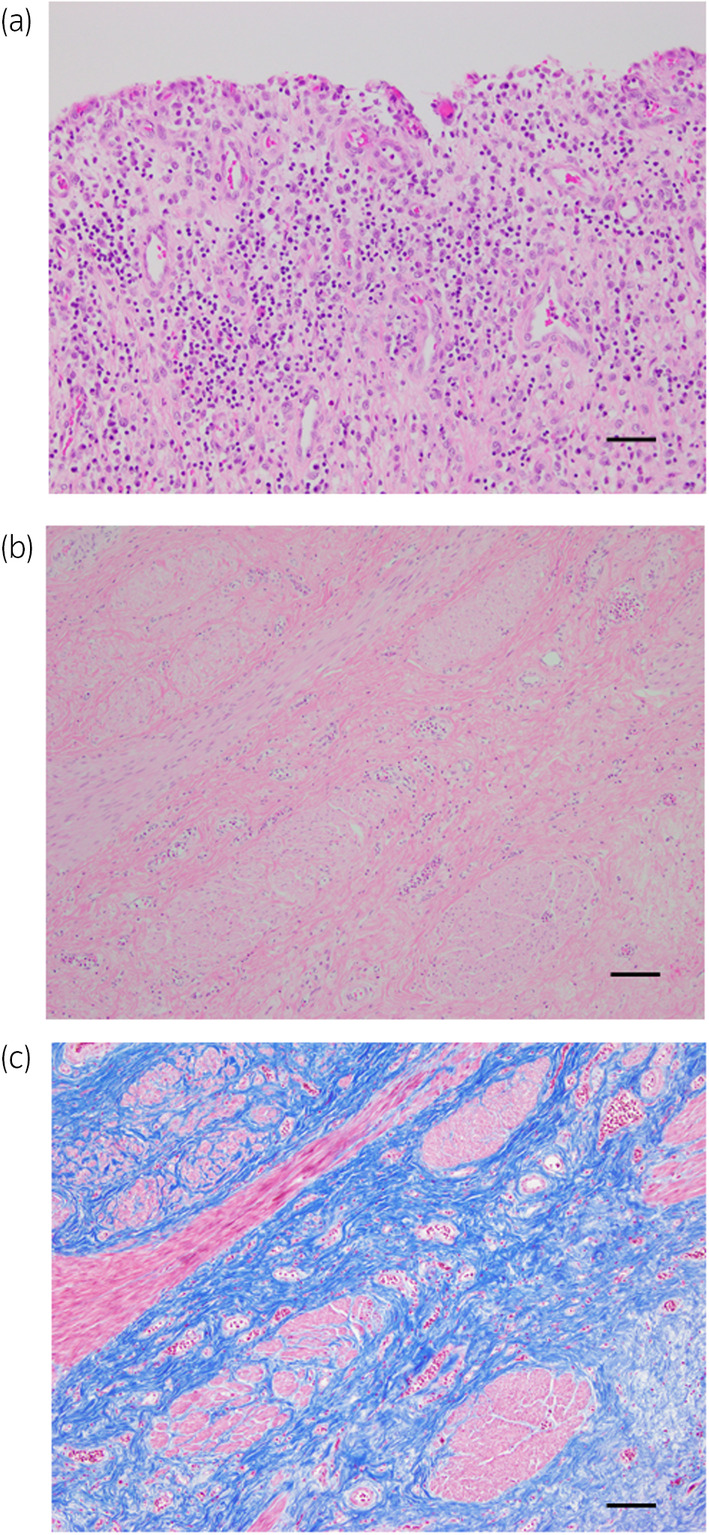
Histological examination revealed severe urothelial denudation and lymphocyte infiltration into the submucosal layer of the bladder (a: hematoxylin and eosin staining) with bladder wall fibrosis (b: hematoxylin and eosin staining; c: Masson's trichrome staining). Scale bar: 50 μm.
The patient's postoperative course was uneventful; hydronephrosis and bladder pain disappeared, her menstrual cycle returned to normal, and she resumed social activities. She achieved complete urinary continence but required clean intermittent catheterization.
Discussion
The prevalence of HIC is higher in middle‐aged and older adults and lower in those in their 20s. 7 Approximately 10% of patients with IC/BPS are estimated to have severe disease requiring reconstructive surgery. 4
Our case of HIC in a woman in her 20s who underwent cystectomy was extremely rare. We discuss the following three points:
First, why did her HIC become more severe?
Endoscopic bladder fulguration of Hunner's lesions and hydrodistension are valid treatments for HIC. However, intractable bladder pain and lower urinary tract symptoms persisted after several treatment sessions. She had undergone multiple endoscopic bladder fulgurations and a hydrodistention procedure before visiting our clinic. Despite some controversy, this may result in bladder wall fibrosis and reduced bladder capacity. 8 , 9 The cystectomy specimen demonstrated severe inflammation with lymphoplasmatic infiltration, which may also induce bladder wall fibrosis. 9 Retrospectively, we should carefully determine the area for fulguration of Hunner's lesions before hydrodistension using a narrow‐band imaging system to minimize the fulguration area to reduce bladder wall fibrosis. 10 Furthermore, she was treated with antibacterial agents for several months for bacterial cystitis and did not receive valid HIC treatments such as bladder submucosal injections of corticosteroid and/or fulguration. The delay in initial treatment may have worsened the disease.
Second, was total cystectomy the best treatment option in this case?
The role of definitive surgical management in treating patients with HIC remains unknown, and it is generally reserved for patients who are refractory to all other conservative treatments and suffer from severely contracted bladders. 4 Supratrigonal cystectomy and augmentation cystoplasty are reportedly less invasive than cystectomy, which is associated with a high satisfaction rate and few complications with long‐term follow‐up. 1 , 11 However, a nonnegligible number of cases recur shortly after surgery and require cystectomy. 11 , 12 Because her bladder pain had resolved for a short period after fulguration of Hunner's lesions, we were convinced that Hunner's ulcers had caused bladder pain. Additionally, although the bladder pain mostly resolved after bladder catheterization, indicating no or less trigonalgia, she experienced pyelonephritis twice with bilateral hydronephrosis within a few months after catheter replacement without definitive proof of trigonal involvement. Cystectomy was selected due to the patient's strong desire for early symptom relief.
Third, was the ileal neobladder the optimal selection for urinary diversion?
An assessment of the outcomes of cystectomy and cystourethrectomy in patients with intractable IC/BPS revealed no difference, and urethrectomy was not routinely required. 13 With regard to her young age and sexual activity, we ultimately considered an orthotopic ileal neobladder for her urinary diversion with thorough discussion, although the benefits related to robot‐assisted intracorporeal urinary reconstruction have not yet been proven. 14 In a study evaluating postoperative urinary continence in 20 sexually active women who underwent female pelvic organ‐preserving robot‐assisted radical cystectomy and neobladder reconstruction at a single institution, 14 (70%) patients achieved daytime continence and 16 (80%) achieved nighttime continence, with majority resuming sexual activity after surgery. 6 Accordingly, we followed the procedure and preserved the female internal genitalia. However, when considering future pregnancies, despite retroperitonealization of the neobladder, experience after the construction of a continent urinary reservoir is limited. 15 We should carefully follow this patient to monitor for metabolic and nutritional complications such as hyperchloremic metabolic acidosis, osteoporosis, and vitamin B12 deficiency, as well as for future pregnancies. 16 , 17
Conclusion
This is the first case of pelvic organ‐preserving robot‐assisted simple cystectomy and intracorporeal ileal neobladder reconstruction in a young woman with HIC.
Author contributions
Hiroyuki Oue: Writing – original draft. Takahiro Inoue: Supervision; writing – original draft; writing – review and editing. Tomohiro Ueda: Writing – review and editing. Katsunori Uchida: Writing – review and editing. Kouhei Nishikawa: Writing – review and editing. Satoru Masui: Writing – review and editing. Manabu Kato: Writing – review and editing. Takeshi Sasaki: Writing – review and editing. Shinichiro Higashi: Writing – review and editing. Shiori Miyachi: Writing – review and editing.
Conflict of interest
The authors declare no conflict of interest.
Approval of the research protocol by an Institutional Reviewer Board
Not applicable.
Informed consent
Consent to participate in publication was acquired from the patient.
Registry and the Registration No. of the study/trial
Not applicable.
Acknowledgments
We acknowledge the clinical staff of the Department of Nephron‐Urologic Surgery.
References
- 1. Ueda T, Hanno PM, Saito R, Meijlink JM, Yoshimura N. Current understanding and future perspectives of interstitial cystitis/bladder pain syndrome. Int. Neurourol. J. 2021; 25: 99–110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Homma Y, Akiyama Y, Tomoe H et al. Clinical guidelines for interstitial cystitis/bladder pain syndrome. Int. J. Urol. 2020; 27: 578–589. [DOI] [PubMed] [Google Scholar]
- 3. Clemens JQ, Erickson DR, Varela NP, Lai HH. Diagnosis and treatment of interstitial cystitis/bladder pain syndrome. J. Urol. 2022; 208: 34–42. [DOI] [PubMed] [Google Scholar]
- 4. Osman NI, Bratt DG, Downey AP, Esperto F, Inman RD, Chapple CR. A systematic review of surgical interventions for the treatment of bladder pain syndrome/interstitial cystitis. Eur. Urol. Focus 2021; 7: 877–885. [DOI] [PubMed] [Google Scholar]
- 5. Akiyama Y, Niimi A, Igawa Y et al. Cystectomy for patients with Hunner‐type interstitial cystitis at a tertiary referral center in Japan. LUTS 2022; 14: 102–108. [DOI] [PubMed] [Google Scholar]
- 6. Lavallée E, Dovey Z, Pathak P et al. Functional and oncological outcomes of female pelvic organ‐preserving robot‐assisted radical cystectomy. Eur. Urol. Open Sci. 2022; 36: 34–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Doiron RC, Tolls V, Irvine‐Bird K, Kelly KL, Nickel JC. Clinical phenotyping does not differentiate Hunner lesion subtype of interstitial cystitis/bladder pain syndrome: a relook at the role of cystoscopy. J. Urol. 2016; 196: 1136–1140. [DOI] [PubMed] [Google Scholar]
- 8. Furuta A, Suzuki Y, Igarashi T, Kimura T, Egawa S, Yoshimura N. Reduction of bladder capacity under anesthesia following multiple recurrences and repeated surgeries of Hunner lesions in patients with interstitial cystitis. Int. Neurourol. J. 2022; 26: 45–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Akiyama Y, Zaitsu M, Watanabe D et al. Relationship between the frequency of electrocautery of Hunner lesions and changes in bladder capacity in patients with Hunner type interstitial cystitis. Sci. Rep. 2021; 11: 105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Ueda T, Nakagawa M, Okamura M, Tanoue H, Yoshida H, Yoshimura N. New cystoscopic diagnosis for interstitial cystitis/painful bladder syndrome using narrow‐band imaging system. Int. J. Urol. 2008; 15: 1039–1043. [DOI] [PubMed] [Google Scholar]
- 11. Queissert F, Bruecher B, van Ophoven A, Schrader AJ. Supratrigonal cystectomy and augmentation cystoplasty with ileum or ileocecum in the treatment of ulcerative interstitial cystitis/bladder pain syndrome: a 14‐year follow‐up. Int. Urogynecol. J. 2022; 33: 1267–1272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Nielsen KK, Kromann‐Andersen B, Steven K, Hald T. Failure of combined supratrigonal cystectomy and Mainz ileocecocystoplasty in intractable interstitial cystitis: is histology and mast cell count a reliable predictor for the outcome of surgery? J. Urol. 1990; 144: 255–258. [DOI] [PubMed] [Google Scholar]
- 13. Yang TX, Luo DY, Li H, Wang KJ, Shen H. Is urethrectomy necessary during cystectomy in patients with interstitial cystitis or bladder pain syndrome? Urology 2016; 97: 73–79. [DOI] [PubMed] [Google Scholar]
- 14. Catto JWF, Khetrapal P, Ricciardi F et al. Effect of robot‐assisted radical cystectomy with intracorporeal urinary diversion vs open radical cystectomy on 90‐day morbidity and mortality among patients with bladder cancer: a randomized clinical trial. JAMA 2022; 327: 2092–2103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Kołodziej A, Krajewski W, Tupikowski K et al. Pregnancy and delivery in a patient with a Studer orthotopic ileal neobladder. Cent. Eur. J. Urol. 2016; 69: 431–433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Roth JD, Koch MO. Metabolic and nutritional consequences of urinary diversion using intestinal segments to reconstruct the urinary tract. Urol. Clin. North Am. 2018; 45: 19–24. [DOI] [PubMed] [Google Scholar]
- 17. Steiner MS, Morton RA. Nutritional and gastrointestinal complications of the use of bowel segments in the lower urinary tract. Urol. Clin. North Am. 1991; 18: 743–754. [PubMed] [Google Scholar]