

Abstract
Background
Chronic inflammatory disorders in peritoneal dialysis (PD) contribute to the adverse clinical outcome. Systemic immune inflammation index (SII) is the novel and convenient measurement that is positively associated with various diseases. However, scarce is known regarding the association between SII with all-cause mortality among PD patients.
Methods
In this multi-center retrospective cohort study, 1,677 incident patients with PD were enrolled. Eligible patients were stratified into groups based on SII level: tertile 1(< 456.76), tertile 2(456.76 to 819.03), and tertile 3(> 819.03). The primary endpoint was the all-cause mortality. Both Cox regression analysis and competing risk models were used to examine the association between SII and all-cause mortality. Subgroup analysis was performed to assess the influence of the SII tertiles on all-cause mortality in different subgroups.
Results
During the follow-up period of 30.5 ± 20.0 months, 26.0% (437/1,677) patients died, of whom the SII tertile 3 group accounted for 39.1% (171/437) of the deaths. Patients in the SII tertile 3 group had a higher all-cause mortality rate than patients in the SII tertile 1 and 2 groups (log-rank = 13.037, P < 0.001). The SII tertile 3 group was significantly associated with 80% greater risk (95% confidence interval:1.13 to 2.85; P = 0.013) compared with the SII tertile 1 group in multivariable Cox regression analysis. The competing risk model also indicated that the relationship between SII tertiles and all-cause mortality remains (subdistribution hazard ratio: 1.86; 95% confidence interval: 1.15 to 2.02, P = 0.011). Furthermore, the relationship between the log-transformed SII and all-cause mortality in patients with PD was nearly linear (P = 0.124).
Conclusion
A close relationship was observed between the SII and all-cause mortality in patients undergoing PD, suggesting that more attention should be paid to the SII, which is a convenient and effective measurement in clinical practice.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12882-023-03451-4.
Keywords: Systemic immune inflammation index, Inflammation, All-cause mortality, Prognosis, Peritoneal dialysis
Introduction
Currently, peritoneal dialysis (PD) accounts for approximately 11% of all dialysis patients worldwide [1]. The risk of mortality has increased in patients undergoing PD due to increasing risk for infections, malnutrition and cardiovascular diseases (CVD), which are to blame for approximately 40%–60% of all-cause mortality in the PD population [2]. Some traditional CVD risk factors [3] including smoking, physical activity, hypertension, diabetes, and hyperlipidemia, may contribute to poor survival outcomes among PD patients [4]. Other studies have shown that inflammatory status [5, 6], malnutrition [6–9], electrolyte disturbance [10–12], metabolic disorder [13–15], lower plant-based protein intake [16], alkaline phosphatases [17], and older age [18] were risk factors for all-cause mortality in patients undergoing PD. These factors above, particularly inflammation, are well-known nontraditional CVD risk factors [3] and may further increase the risk of death in such populations [19].
The pathogenic process of inflammation is typically complicated and multifactorial, involving both dialysis-related and dialysis-unrelated factors, which may lead to malnutrition, an adverse cardiovascular prognosis, and mortality in patients undergoing PD [20]. Certain inflammatory markers, such as C-reactive protein (CRP), neutrophil-to-lymphocyte ratio (NLR), and monocyte-to-lymphocyte ratio (MLR), which represent the systemic inflammatory response, are independent predictors of mortality in patients with PD [5, 18, 21]. Recently, a novel inflammatory marker, the systemic immune inflammation index (SII), which is inexpensive and easily accessible, has been a “hot issue”, and associated with cognitive decline [22], cerebrovascular diseases [23], atrial fibrillation [24], and poor prognosis of cancer [25]. Additionally, in the general population [23] of cardiovascular [26] or cerebrovascular disease patients [27], the correlation between SII and adverse overall survival has been found. A large, prospective, population-based study recently reported that compared with the lowest quantile of SII, the highest quantile of SII was associated with an approximate 24.6% greater risk of all-cause mortality. Thus, it may be as a useful marker of all-cause mortality in general population [23]. Moreover, there is a nearly linear relationship between log-transformed SII and all-cause mortality in patients with acute ischemic stroke [27], but a non-linear relationship between the log-transformed SII and all-cause death in patients with CVD [26, 28].
The SII may be better than other inflammation markers (such as CRP, NLR, and MLR) in clinical practice. First, as a new inflammatory biomarker, the SII can provide a more balanced and comprehensive assessment of immune and inflammatory responses [29]. As the SII level increases, inflammatory activity in various diseases may increase, leading to poor clinical outcomes [30]. Second, based on the counts of three types of circulating immune cells—neutrophils, platelets, and lymphocytes—the SII value reflects the inflammatory state and can present a better predictive value than the NLR and MLR [22, 31]. Third, compared with other inflammatory indicators such as CRP and interleukin-6 (IL-6), the SII can be easily obtained, routinely collected, and tested in hospitalized patients; thus, it might be useful in predicting poor prognosis.
Nevertheless, to the best of our knowledge, the association between the SII and all-cause mortality in patients undergoing PD has been elucidated only by a few papers. Therefore, we conducted this multi-center retrospective cohort study to test the hypothesis that the inflammatory status defined by the SII is associated with all-cause mortality in patients undergoing PD, ultimately laying the theoretical basis for its potential clinical assessment value.
Material and methods
Study population
A multi-center retrospective cohort study was conducted with 2,469 incident patients with PD between January 1, 2010, and December 31, 2018, who underwent PD treatment for at least 3 months at PD centers of six tertiary hospitals in China. Distributed in several provinces such as Guangdong, Shanghai, and Henan, each hospital has a specialized data registrar, follow-up management system, and electronic medical record system, and has over 400 patient undergoing PD. The main exclusion criteria were as follows: 1) patients with follow-up time less than 3 months (n = 81); 2) patients younger than 18 years or older than 80 years (n = 70); and 3) patients with a history of hematological diseases (n = 6), or rheumatic diseases (n = 25), with medication of corticosteroids (n = 40) or immunosuppressive agents (n = 11), as they could affect the lymphocyte and platelet counts. Patients without SII values were also excluded (n = 559). Finally, 1,677 patients were included in the study and followed up until the end of the study, or December 31, 2019. The flowchart is shown in Fig. 1. This study was approved by the investigational review board of Jiangmen Central Hospital (approval number 2022101) and was conducted in accordance with the Declaration of Helsinki in 2022. Written informed consent was not required because this retrospective study collected pre-existing hospital data.
Fig. 1.

Flow chart of this study
Data collection
All baseline data were collected 3 months after the initiation of PD therapy. Baseline demographic data included age; sex; current smoking and drinking habits; the presence of diabetes, hypertension, stroke, and cardiovascular diseases; and medication use, which was recorded based on the prescriptions. Clinical and biochemical data included blood pressure, white blood cells, hemoglobin, platelets, neutrophils, lymphocytes, serum creatinine, urea nitrogen, serum albumin, alkaline phosphatase, total cholesterol, triglycerides, sensitivity C-reactive protein (s-CRP), liver function, magnesium, calcium, phosphorus, and intact parathyroid hormone (iPTH). The SII was calculated as platelet count × neutrophil count/lymphocyte count. The baseline residual renal function was assessed using the Chronic Kidney Disease Epidemiology Collaboration creatinine equation. Total Kt/V was calculated using PD Adequest Software 2.0 (Baxter Healthcare Corp., Deerfield, Illinois, USA).
Follow-up and study endpoint
The primary endpoint was the all-cause mortality rate. All patients were followed up until death, cessation of PD (switching to hemodialysis or renal transplantation), loss of follow-up, or the end of follow-up on December 31, 2019.
Statistical analysis
The eligible patients were divided into three groups based on the tertile values of the SII. The lowest (Tertile 1), middle (Tertile 2), and highest (Tertile 3) SII tertile had an SII value of < 456.76, 456.76 to 819.03, and > 819.03, respectively. Continuous variables with a normal distribution were expressed as mean ± standard deviation, and those with a skewed distribution were described as median (25%–75% interquartile range [IQR]). Categorical data are expressed as frequencies or percentages (%). The SII was converted into logSII by the log transformation because of the non-normal distribution. Differences among the three groups were assessed using a one-way analysis of variance, the Kruskal–Wallis test, or χ2 test, as appropriate. Cumulative survival curves were generated using the Kaplan–Meier method and compared using the log-rank test. Cumulative incident curves were evaluated using the Fine and Gray method. The associations between the SII tertiles and all-cause mortality were evaluated using the Cox proportional hazards and subdistribution hazards models for competing risk analysis. To account for the non-linear correlation between the SII and all-cause mortality in patients with PD, we also employed a restricted cubic spline regression model to evaluate non-linearity.
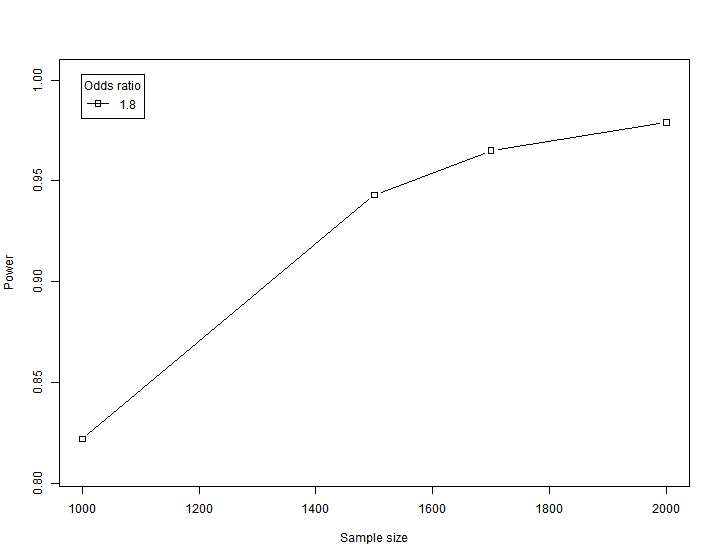
We apply the method of “Computer Simulation Statistical Efficiency” to evaluate the sample size, which was performed using Empower(R) (www.empowerstats.com, X&Ysolutions, Inc., Boston, MA) [32]. The parameter settings are well documented according to the result of our study. The figure below shows the degree of research reliability corresponding to different sample size and odd ratio. The horizontal axis represents the sample size, the vertical axis represents the degree of reliability of the study. It can be seen that when the odd ratio value is 1.8 and the sample size is 1700, the test efficiency is over 0.95, which is already very reliable. Therefore, it can be considered that the sample size used in our article is appropriate.
Subgroup analyses
To evaluate subgroup modification effects on the relationship between SII stratification and all-cause mortality, we conducted subgroup analyses of the association between SII stratification and all-cause mortality stratified by male and female, less than 65 years and older than or equal to 65 years, with or without diabetes, with or without hypertension, and those with or without a history of pre-existing CVD. The interaction between the SII tertiles and subgroups on all-cause mortality was examined using a formal interaction test.
SPSS statistical software version 22 (IBM Corp., Armonk, NY, USA) and R package 3.6.0 (https://www.r-project.org/) were used for the statistical analyses. Statistical significance was set at P < 0.05.
Results
A total of 1,677 incident patients with PD were recruited and divided into three groups based on the tertiles of baseline SII value: the tertiles 1 (SII value < 456.79, n = 559), 2 (456.79 ≤ SII value ≤ 819.03, n = 559), and three groups (SII value > 819.03, n = 559). Among 1,677 patients, the mean age of the study population was 50.5 ± 14.0 years, 44.3% were female, and the percentages of hypertension, diabetes, and CVD history were 77.6%, 22.5%, and 23.4%, respectively. The mean follow-up period was 30.5 ± 20.0 months. At the end of this study, 26.01% (437/1,677) of patients had died, of whom the tertile 3 group accounted for 39.1% (171/437) of the deaths; 18.90% (317/1,677) of patients had undergone kidney transplantation and were transferred to hemodialysis; 3.64% (61/1,677) had been lost to follow-up; and the remaining 51.40% (862/1,677) of patients were still being followed up at these PD centers. Among the 437 deaths, 196 (44.8%) were attributed to cardiovascular mortality, 49 (11.2%) to cerebrovascular disease, 56 (12.8%) to infectious diseases, 9 (2.0%) to gastrointestinal bleeding, 11 (2.5%) to malignancy, 63 (14.4%) to other causes, and 53 (12.1%) to unknown causes.
Comparisons of clinical parameters between groups
The baseline demographics and clinical and laboratory characteristics of the total study population after stratification by tertiles of SII values are summarized in Table 1. Patients in groups with a higher baseline SII level (tertile 3) compared with the reference group (tertile 1) tended to be male, older, and had higher levels of white blood cells, hemoglobin, platelets, neutrophils, monocytes, total cholesterol, triglycerides, calcium, and serum sCRP, but lower levels of lymphocytes, serum albumin, and iPTH (all P < 0.05). They also had a higher percentage of diabetes mellitus, angiotensin receptor blockers, statins, and aspirin use (all P < 0.05; Table 1).
Table 1.
Baseline characteristics of individuals stratified by tertiles of SII
| Variables | Total (n = 1677) |
Tertiles 1 (n = 559) |
Tertiles 2 (n = 559) |
Tertiles 3 (n = 559) |
p value |
|---|---|---|---|---|---|
| Sex, female(%) | 743 (44.3) | 276 (49.5) | 237 (42.3) | 230 (41.1) | 0.010 |
| Age(years) | 50.5 ± 14.0 | 49.3 ± 14.4 | 50.3 ± 13.6 | 52.0 ± 14.0 | 0.005 |
| Diabetes, n(%) | 377 (22.5) | 101 (18.1) | 129 (23.1) | 147 (26.3) | 0.004 |
| Hypertension, n(%) | 1299 (77.6) | 427 (76.7) | 425 (76.2) | 447 (80) | 0.254 |
| Stroke, n(%) | 80 ( 9.4) | 24 (10.2) | 30 (10.4) | 26 (7.9) | 0.499 |
| CVD, n(%) | 199 (23.4) | 52 (21.7) | 59 (21) | 88 (26.6) | 0.203 |
| Systolic pressure(mmhg) | 144.0 ± 24.1 | 142.0 ± 22.5 | 145.3 ± 24.5 | 144.7 ± 25.2 | 0.081 |
| Diastolic pressure(mmhg) | 85.4 ± 15.1 | 85.5 ± 15.1 | 86.1 ± 14.6 | 84.6 ± 15.7 | 0.341 |
| Medication | |||||
| CCB, n (%) | 1221 (78.2) | 395 (76.4) | 410 (77.1) | 416 (81.2) | 0.124 |
| ACEI, n (%) | 81 (5.7) | 28 (5.9) | 21 (4.4) | 32 (6.8) | 0.265 |
| ARB, n (%) | 564 (38.2) | 172 (35.4) | 183 (36.6) | 209 (42.7) | 0.043 |
| Statin, n (%) | 219 (14.9) | 53 (10.9) | 76 (15.4) | 90 (18.5) | 0.004 |
| Aspirin, n (%) | 174 (12.0) | 37 (7.7) | 55 (11.3) | 82 (17) | < 0.001 |
| Laboratory variables | |||||
| White blood cell(10^9/L) | 6.5 ± 2.3 | 5.1 ± 1.5 | 6.3 ± 1.7 | 8.1 ± 2.6 | < 0.001 |
| Platelet(10^9/L) | 194.3 ± 80.5 | 142.8 ± 57.4 | 192.7 ± 59.7 | 247.3 ± 84.5 | < 0.001 |
| Hemoglobin(g/L) | 89.4 ± 22.1 | 86.2 ± 22.5 | 90.2 ± 22.6 | 91.8 ± 20.8 | < 0.001 |
| Neutrophils(10^9/L) | 4.5 ± 2.1 | 3.1 ± 1.0 | 4.3 ± 1.3 | 6.1 ± 2.3 | < 0.001 |
| Monocyte(10^9/L) | 0.4 ± 0.2 | 0.4 ± 0.2 | 0.4 ± 0.2 | 0.5 ± 0.2 | < 0.001 |
| Lymphocyte(10^9/L) | 1.3 ± 0.5 | 1.4 ± 0.6 | 1.3 ± 0.5 | 1.1 ± 0.4 | < 0.001 |
| Serum creatinine(umol/L) | 788.4 ± 318.2 | 801.2 ± 323.8 | 797.6 ± 318.1 | 766.5 ± 312.0 | 0.133 |
| Urea nitrogen(mmol/L) | 22.4 ± 14.9 | 23.0 ± 9.6 | 22.1 ± 9.2 | 22.1 ± 22.2 | 0.526 |
| Albumin(g/L) | 36.0 ± 5.7 | 36.2 ± 5.5 | 36.3 ± 5.5 | 35.4 ± 6.1 | 0.016 |
| Alkaline phosphatase(U/L) | 84.6 ± 61.7 | 84.3 ± 73.3 | 82.3 ± 55.1 | 87.4 ± 55.0 | 0.374 |
| Aspartate aminotransferase(U/L) | 21.6 ± 15.1 | 22.1 ± 14.9 | 21.1 ± 16.4 | 21.7 ± 14.0 | 0.489 |
| Alanine aminotransferase(U/L) | 18.9 ± 24.5 | 20.3 ± 31.1 | 18.9 ± 23.7 | 17.5 ± 16.3 | 0.162 |
| Total bilirubin(umol/L) | 4.9 ± 3.1 | 5.0 ± 3.5 | 4.7 ± 2.6 | 5.0 ± 3.0 | 0.214 |
| Cholesterol(mmol/L) | 4.5 ± 1.3 | 4.3 ± 1.2 | 4.6 ± 1.4 | 4.7 ± 1.3 | < 0.001 |
| Triglyceride(mmol/L) | 1.6 ± 1.2 | 1.4 ± 0.9 | 1.7 ± 1.6 | 1.6 ± 1.0 | < 0.001 |
| High density lipoprotein(mmol/L) | 1.2 ± 0.4 | 1.2 ± 0.4 | 1.2 ± 0.4 | 1.2 ± 0.4 | 0.900 |
| Low density lipoprotein(mmol/L) | 2.8 ± 6.5 | 2.6 ± 1.0 | 3.1 ± 1.1 | 2.8 ± 1.0 | 0.380 |
| iPTH(pg/ml) | 198.0 (96.6, 351.4) | 214.2 (114.3, 361.3) | 199.4 (97.7, 352.5) | 179.8 (68.1, 338.0) | 0.017 |
| Calcium(mmol/L) | 2.1 ± 0.3 | 2.0 ± 0.3 | 2.1 ± 0.3 | 2.1 ± 0.3 | < 0.001 |
| Phosphorus(mmol/L) | 1.8 ± 2.8 | 1.8 ± 0.5 | 2.0 ± 4.7 | 1.7 ± 0.6 | 0.364 |
| Magnesium(mmol/L) | 0.9 ± 0.4 | 0.9 ± 0.4 | 0.9 ± 0.3 | 0.9 ± 0.5 | 0.369 |
| sCRP(mg/l) | 3.2 (1.3, 8.5) | 2.7 (1.2, 5.8) | 3.0 (1.2, 6.5) | 4.2 (1.6, 12.0) | < 0.001 |
| Total Kt/V | 2.3 ± 1.2 | 2.3 ± 1.0 | 2.4 ± 1.7 | 2.3 ± 0.9 | 0.420 |
| RRF(mL/min/1.73m2) | 4.1 ± 3.6 | 3.9 ± 3.2 | 4.2 ± 3.5 | 4.1 ± 3.9 | 0.416 |
| SII (10^9/L) | 611.1 (393.0, 963.0) | 316.8 (240.3, 392.4) | 610.9 (525.8, 710.4) | 1214.0 (963.0, 1696.0) | < 0.001 |
Abbreviations: CVD cardiovascular diseases, CCB calcium channel blocker, ACEI angiotensin-converting enzyme inhibitor, ARB angiotensin receptor blocker, iPTH intact parathyroid hormone, sCRP sensitive C-reactive protein, Total Kt/V K, dialyzer clearance of urea; t dialysis time; V volume of distribution of urea, RRF renal residual function, SII systemic immune inflammation index
Associations between SII and all-cause mortality
To confirm the association of the SII with all-cause mortality in the population, Cox regression analyses and a competitive risk model were utilized. Kaplan–Meier curves showed significant differences in all-cause mortality between the SII tertiles. Individuals in the SII tertile 3 group had a significantly higher death rate (SII tertile 3 group vs. SII tertile 2 group vs. SII tertile 1 group; 39.1% vs. 33.1% vs. 27.6%, respectively; P < 0.001, log-rank test; Fig. 2). In univariable Cox regression analyses, we found that compared with the lowest SII tertile group, the highest SII tertile group was associated with an approximate 54% greater risk of all-cause mortality (HR: 1.54, 95% CI: 1.21 to 1.95, P < 0.001). After a full adjustment for covariates, the association between SII tertiles and all-cause mortality in patients with PD remains (HR: 1.80, 95% CI: 1.13 to 2.85, P = 0.013). (Table 2).
Fig. 2.

Kaplan–Meier curves for all-cause mortality stratified by SII
Table 2.
The associations of SII stratification with all-cause mortality in PD patients
| Variables | Model 1(unadjusted) | Model 2(full adjusted) | ||
|---|---|---|---|---|
| HR or SHR(95%CI) | p value | HR or SHR(95%CI) | p value | |
| All-cause mortality(Cox regression analysis) | ||||
| Tertles 1 of SII | Reference | Reference | ||
| Tertles 2 of SII | 1.16 (0.90, 1.48) | 0.248 | 1.35 (0.82, 2.25) | 0.241 |
| Tertles 3 of SII | 1.54 (1.21, 1.95) | < 0.001 | 1.80 (1.13, 2.85) | 0.013 |
| All-cause mortality(set switching to hemodialysis and kidney transplants as competitive risk) | ||||
| Tertles 1 of SII | Reference | Reference | ||
| Tertles 2 of SII | 1.16(0.90, 1.49) | 0.242 | 1.48(0.88, 2.46) | 0.136 |
| Tertles 3 of SII | 1.58(1.20, 1.94) | < 0.001 | 1.86(1.15, 2.02) | 0.011 |
Model 1: unadjusted
Model 2: adjusted for age, sex, diabetes mellitus, hypertension, strokes, pre-existing cardiovascular disease, drug medication, total Kt/V, RRF, hemoglobin, urea nitrogen, Serum creatinine, albumin, cholesterol, triglyceride, High density lipoprotein, Low density lipoprotein, alkaline phosphatase, magnesium, calcium, phosphorus, iPTH, aspartate aminotransferase, alanine aminotransferase, total bilirubin
Abbreviations: SII systemic inflammatory index, Total Kt/V K, dialyzer clearance of urea; t dialysis time; V volume of distribution of urea, RRF renal residual function, iPTH intact parathyroid hormone, HR hazard ratio, SHR Subdistribution Hazard Ratio, CI confidence interval
In the Fine and Gray competing risk models, a higher SII was associated with a higher risk of all-cause mortality (gray value = 14.104, P < 0.001) (Fig. 3). After full adjustment, compared with the lowest SII tertile group, the highest SII tertile group was associated with an approximate 86% increased risk of all-cause mortality (SHR: 1.86, 95% CI: 1.15 to 2.02, P = 0.011). (Table 2).
Fig. 3.

Cumulative incidence curves for all-cause mortality stratified by SII
Moreover, we used the cox regression model to analyze the relationship between CRP and mortality. The result showed that CRP > 3 mg /L was also correlated with mortality. However, when we adjusted for covariates, we found that CRP > 3 mg /L had nonsignificant effect on mortality, possibly due to the influence of CRP on mortality being influenced by other factors such as complications and nutritional status (Supplementary Table 1).
In addition, the restricted cubic splines showed that the risk of all-cause mortality increased gradually when log-transformed SII was > 2.78, while the risk of all-cause mortality remained unchanged when log-transformed SII was ≤ 2.78. The association between the log-transformed SII and all-cause mortality was nearly linear (P = 0.124, Fig. 4).
Fig. 4.

HR and 95% CI for the risk of all-cause mortality in PD patients along with the changes of logSII from the restricted cubic spline model
Relationship between SII stratification and all-cause mortality in different subgroups
We investigated the association between SII tertiles and all-cause mortality in different subgroups, including male or female, less than 65 years and older than or equal to 65 years, with or without diabetes, with or without hypertension, and those with or without a history of pre-existing CVD. In the subgroup analysis, the results indicated that compared to the SII tertile 1 group, the SII tertile 3 group was associated with a 1.06 times greater risk of all-cause mortality for less than 65-year-old patients, 93% for those with hypertension, 4.62 times for those with diabetes, and 1.54 times for those without a history of pre-existing CVD (all P < 0.05, Table 3). However, these trends were not observed among patients aged 65 years or older, without hypertension, without diabetes, or with a history of pre-existing CVD. Moreover, no interaction was observed between sex, age, diabetes mellitus, hypertension, pre-existing CVD, or all-cause mortality.
Table 3.
Subgroup analysis for the association of SII stratification and all-cause mortality in PD patients
| Variables | Tertiles 1 | Tertiles 2 | Tertiles 3 | P for interaction | ||
|---|---|---|---|---|---|---|
| HR(95%CI) | p value | HR(95%CI) | p value | |||
| Age | 0.891 | |||||
| < 65 years | 1.00 | 1.49 (0.79 ~ 2.82) | 0.216 | 2.09 (1.16 ~ 3.76) | 0.014 | |
| ≥ 65 years | 1.00 | 1.07 (0.25 ~ 4.55) | 0.929 | 0.92 (0.26 ~ 3.28) | 0.894 | |
| Gender | 0.310 | |||||
| Male | 1.00 | 0.84 (0.32 ~ 2.21) | 0.723 | 1.49 (0.63 ~ 3.5) | 0.362 | |
| Female | 1.00 | 1.7 (0.86 ~ 3.37) | 0.129 | 1.88 (1 ~ 3.53) | 0.052 | |
| Hypertension | 0.756 | |||||
| No | 1.00 | 0.82 (0.44 ~ 1.51) | 0.524 | 1.7 (0.97 ~ 2.99) | 0.065 | |
| Yes | 1.00 | 1.67 (0.96 ~ 2.91) | 0.071 | 1.93 (1.16 ~ 3.22) | 0.011 | |
| Diabetes | 0.925 | |||||
| No | 1.00 | 1.15 (0.63 ~ 2.07) | 0.652 | 1.48 (0.85 ~ 2.59) | 0.169 | |
| Yes | 1.00 | 1.14 (0.3 ~ 4.29) | 0.846 | 5.62 (1.2 ~ 26.43) | 0.029 | |
| Pre-existing cardiovascular disease | 0.251 | |||||
| No | 1.00 | 1.53 (0.79 ~ 2.94) | 0.207 | 2.54 (1.35 ~ 4.8) | 0.004 | |
| Yes | 1.00 | 1.95 (0.66 ~ 5.75) | 0.226 | 2.9 (0.88 ~ 9.56) | 0.079 | |
Abbreviations: SII systemic inflammatory index, Total Kt/V K, dialyzer clearance of urea; t dialysis time, V volume of distribution of urea, RRF renal residual function, iPTH intact parathyroid hormone, HR hazard ratio, CI confidence interval; adjusted for age, sex, diabetes mellitus, hypertension, strokes, pre-existing cardiovascular disease, drug medication, total Kt/V RRF, hemoglobin, urea nitrogen, Serum creatinine, albumin, cholesterol, triglyceride, High density lipoprotein, Low density lipoprotein, alkaline phosphatase, magnesium, calcium, phosphorus, iPTH aspartate aminotransferase, alanine aminotransferase, total bilirubin
Discussion
It is estimated that over 272,000 patients receive PD as a treatment for end-stage renal disease globally [1], and the number is increasing, with a considerable risk of adverse clinical prognosis. This study demonstrated that during the follow-up period of 30.5 ± 20.0 months, 437 (26.01%) patients died, which was consistent with other previous studies [33, 34], indicating that patients undergoing PD suffered an undesirable survival outcome. Thus, exploring the prognostic factors for survival in PD populations is crucial.
Calculated as (platelet count × neutrophil count/lymphocyte count), the SII is based on peripheral blood parameters that reflect the balance between inflammation and immunity [35, 36]. Growing evidence has been observed that the SII, as a novel inflammatory indicator, is correlated with a variety of adverse clinical outcomes [22–25, 31]. Notably, only a few studies focusing on the general population or patients with vascular disease have found that SII is independently correlated with all-cause mortality [23, 26–28]. Consistent with previous studies, our study showed an association between SII and all-cause mortality in patients undergoing PD and found that a higher SII corresponded to an increased risk of death in the PD population. Patients in the highest SII tertile had a significantly higher mortality rate, accounting for 39.1%. Compared with the lowest SII tertile group, the highest SII tertile group was associated with an approximately 80% greater risk of all-cause mortality, suggesting that the SII may act as a potential predictor of all-cause mortality in patients undergoing PD. Currently, this is a study applied by competitive risk model to focus on patients with PD to evaluate the value of SII in predicting all-cause mortality. Unlike other studies, our study applied competitive risk models and RCS curves to further demonstrate the relationship between SII and all-cause mortality in patients undergoing peritoneal dialysis. Althougt there exist several related studies, our manuscript is novel to a certain extent.
However, the underlying mechanisms by which the SII affects survival in these populations remain unknown and may be complicated. There are several possible explanations for these findings. One of the possible mechanisms may be the manifestation of systemic inflammation, whose prevalence ranges between 12 and 65% in PD populations [37], and which is a well-known risk factor for PD related mortality and plays an important role in poor prognosis [38]. SII is positively correlated with inflammatory indicators, including sCRP, NLR, and MLR, which have been regarded as prognostic biomarkers of poor survival in patients with PD [5, 6, 18–21]. Our study also found that patients in the groups with a higher baseline SII tended to have higher levels of serum CRP, which is a marker of inflammation and is significantly associated with a negative prognosis. Compared with composite indicators, such as NLR and MLR, a comprehensive indicator of neutrophils, platelets, and lymphocytes may be more stable, thereby increasing the application value of predicting the prognosis of patients with PD. A higher SII may represent a higher number of neutrophils and platelets, which stimulate the release of inflammatory mediators [39]. During inflammation, various pro-inflammatory cytokines and growth factors are released to stimulate the proliferation of macrophages, subsequently leading to the deterioration of body function [34]. Moreover, the higher the SII, the more severe the imbalance between inflammation and immunity and the more serious the inflammatory response [23].
Another potential mechanism might be the risk of malnutrition underlying the SII. Our study found that patients in groups with a higher baseline SII tended to have lower levels of serum albumin, which is a parameter representing nutritional status, indicating that SII may be related to nutritional status to a certain extent. Inflammation and malnutrition interact with and promote each other in dialysis patients [40], leading to poor overall survival.
In the subgroup analysis of patients over 65 years of age, the results showed no significance. We speculate that patients over 65 years of age are more susceptible to the majority of comorbidities and that the cause of death may not be exclusively inflammatory. Furthermore, our study indicated that, compared to the SII tertile 1 group, the SII tertile 3 group was associated with a 4.62 times greater risk of all-cause mortality in those with diabetes. Other study reported a relationship between SII and diabetes [41]. The inflammatory response is considered a potential mechanism involved in glucometabolic processes [41]. However, the underlying mechanism remains unclear.
The SII may be a prognostic marker of survival due to the following potential reasons. First, compared to neutrophil, platelet, or lymphocyte counts alone, the SII is relatively more stable and less likely to be changed by different pathological circumstances. Second, the SII integrates inflammatory response and immune regulation. Finally, the SII is a low-cost, easily obtainable and practical parameter; thus, it might be useful in predicting mortality risk among patients with PD.
It is noteworthy that several limitations of current research also exist. First, the present study is a retrospective study, thus, bias was inevitable. Second, we only collected baseline value of SII. Dynamically monitoring how SII changes is of highly necessity and worthy of further research. Third, we did not measure the markers of oxidative stress or inflammation, such as superoxide dismutase, malonaldehyde, IL-6, or tumor necrosis factor α, at baseline, which may also related with adverse prognosis in patients undergoing PD. Finally, due to the limitations of retrospective research, we did not collect sufficient clinical data on comorbidities scores. Also, we did not collect the characteristics of different dialysis centers.
Conclusions
In summary, this study showed that systemic inflammation, defined by the SII, an inexpensive and easily accessible marker, may be a predictive factor for all-cause mortality in patients with PD. Improving the inflammatory status in patients with PD may provide clinical benefits for the long-term survival of the population; however, the mechanisms underlying SII are intricate and require further exploration.
Supplementary Information
Additional file 1: Supplementary Table 1.
{kind=link}
Additional file 2: Supplementary Figure 1. Sample size statistical efficiency. The figure shows the degree of research reliability corresponding to different sample size and odd ratio. The horizontal axis represents the sample size, the vertical axis represents the degree of reliability of the study. It can be seen that when the odd ratio value is 1.8 and the sample size is 1700, the test efficiency is over 0.95, which is already very reliable.
Acknowledgements
We are indebted to all nephrologists and nurses in the six centers for their excellent management of peritoneal dialysis patients. We also thank the staffs involved in the retrospective multi-centers cohort study.
Authors’ contributions
Ruiying Tang involved in the conception, study design, and writing of the paper; Jiexin Chen involved in acquisition of data and analysis and interpretation; Qian Zhou took part in analysis and interpretation of the data; Jihong Deng, Xiaojiang Zhan, Xiaoyang Wang, Yueqiang Wen, Ning Su, Xiaoran Feng involved in acquisition of data and data verification; Qingdong Xu took part in revising or critically reviewing the article, gave final approval of the version to be published, and have agreed on the journal to which the article has been submitted. All authors reviewed the manuscript.
Funding
This work was supported by Science and Technology Research Project of Jiangmen City, China (No. 2021YL01083).
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
This study was approved by the investigational review board of Jiangmen Central Hospital (approval number 2022101) and was carried out in accordance with the Declaration of Helsinki in 2022. As it was a retrospective study, the Human Ethics Committee of Jiangmen Central Hospital waived the need for informed consent in the study. All clinical data analyzed were obtained from pre-existing datasets at the hospital.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Li PK, Chow KM, Van de Luijtgaarden MW, Johnson DW, Jager KJ, Mehrotra R, et al. Changes in the worldwide epidemiology of peritoneal dialysis. Nat Rev Nephrol. 2017;13(2):90–103. doi: 10.1038/nrneph.2016.181. [DOI] [PubMed] [Google Scholar]
- 2.Tonelli M, Karumanchi SA, Thadhani R. Epidemiology and mechanisms of uremia-related cardiovascular disease. Circulation. 2016;133(5):518–536. doi: 10.1161/CIRCULATIONAHA.115.018713. [DOI] [PubMed] [Google Scholar]
- 3.Fassett RG, Driver R, Healy H, Coombes JS. Cardiovascular disease in peritoneal dialysis patients. Panminerva Med. 2009;51(3):151–161. [PubMed] [Google Scholar]
- 4.Wanner C, Amann K, Shoji T. The heart and vascular system in dialysis. Lancet. 2016;388(10041):276–284. doi: 10.1016/S0140-6736(16)30508-6. [DOI] [PubMed] [Google Scholar]
- 5.Li M, Feng S, Zhan X, Peng F, Feng X, Zhou Q, et al. Neutrophil to high-density lipoprotein ratio associates with higher all-cause mortality and new onset cardiovascular events in peritoneal dialysis patients. Int Urol Nephrol. 2022;54(10):2745–2754. doi: 10.1007/s11255-022-03202-8. [DOI] [PubMed] [Google Scholar]
- 6.Liu S, Qiu P, Luo L, Jiang L, Chen Y, Yan C, et al. Serum C-reactive protein to albumin ratio and mortality associated with peritoneal dialysis. Ren Fail. 2020;42(1):600–606. doi: 10.1080/0886022X.2020.1783680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lai KJ, Hsieh YP, Chiu PF, Lin PR. Association of albumin and globulin with mortality risk in incident peritoneal dialysis patients. Nutrients. 2022;14(14):2850. doi: 10.3390/nu14142850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ye M, Li J, Liu Y, He W, Lin H, Fan R, et al. Serum Prealbumin and echocardiography parameters predict mortality in peritoneal dialysis patients. Kidney Blood Press Res. 2020;45(5):671–685. doi: 10.1159/000507331. [DOI] [PubMed] [Google Scholar]
- 9.Kim C, Kim JK, Lee HS, Kim SG, Song YR. Longitudinal changes in body composition are associated with all-cause mortality in patients on peritoneal dialysis. Clin Nutr. 2021;40(1):120–126. doi: 10.1016/j.clnu.2020.04.034. [DOI] [PubMed] [Google Scholar]
- 10.Zhou L, Wang X, Zhan X, Feng X, Wang N, Peng F, et al. Serum Chloride and Mortality in patients on continuous ambulatory peritoneal dialysis: a multi-center retrospective study. EClinicalMedicine. 2021;41:101133. doi: 10.1016/j.eclinm.2021.101133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ravel VA, Streja E, Mehrotra R, Sim JJ, Harley K, Ayus JC, et al. Serum sodium and mortality in a national peritoneal dialysis cohort. Nephrol Dial Transplant. 2017;32(7):1224–1233. doi: 10.1093/ndt/gfw254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zhang F, Wu X, Wen Y, Zhan X, Peng FF, Wang X, et al. Hypomagnesemia is a risk factor for cardiovascular disease- and noncardiovascular disease-related mortality in peritoneal dialysis patients. Blood Purif. 2022;51(1):23–30. doi: 10.1159/000514148. [DOI] [PubMed] [Google Scholar]
- 13.Shi Y, Cai J, Shi C, Liu C, Li Z. Incidence and mortality of new-onset glucose disorders in peritoneal dialysis patients in China: a meta-analysis. BMC Nephrol. 2020;21(1):152. doi: 10.1186/s12882-020-01820-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zeng C, Yan C, Guo S, Zhu H, Chen Y, Zhan X. High-density lipoprotein cholesterol to apolipoprotein A1 ratio and all-cause mortality among incident peritoneal dialysis patients. Nutr Metab Cardiovasc Dis. 2021;31(12):3457–3463. doi: 10.1016/j.numecd.2021.09.008. [DOI] [PubMed] [Google Scholar]
- 15.Kang T, Hu Y, Huang X, Amoah AN, Lyu Q. Serum uric acid level and all-cause and cardiovascular mortality in peritoneal dialysis patients: a systematic review and dose-response meta-analysis of cohort studies. PLoS One. 2022;17(2):e0264340. doi: 10.1371/journal.pone.0264340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Liu X, Hu Z, Xu X, Li Z, Chen Y, Dong J. The associations of plant-based protein intake with all-cause and cardiovascular mortality in patients on peritoneal dialysis. Nutr Metab Cardiovasc Dis. 2020;30(6):967–976. doi: 10.1016/j.numecd.2020.03.003. [DOI] [PubMed] [Google Scholar]
- 17.Liu X, Guo Q, Feng X, Wang J, Wu J, Mao H, et al. Alkaline phosphatase and mortality in patients on peritoneal dialysis. Clin J Am Soc Nephrol. 2014;9(4):771–778. doi: 10.2215/CJN.08280813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zhang J, Lu X, Li H, Wang S. Risk factors for mortality in patients undergoing peritoneal dialysis: a systematic review and meta-analysis. Ren Fail. 2021;43(1):743–753. doi: 10.1080/0886022X.2021.1918558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Li PK, Ng JK, McIntyre CW. Inflammation and Peritoneal Dialysis. Semin Nephrol. 2017;37(1):54–65. doi: 10.1016/j.semnephrol.2016.10.007. [DOI] [PubMed] [Google Scholar]
- 20.Wang AY. Consequences of chronic inflammation in peritoneal dialysis. Semin Nephrol. 2011;31(2):159–171. doi: 10.1016/j.semnephrol.2011.01.005. [DOI] [PubMed] [Google Scholar]
- 21.Wen Y, Zhan X, Wang N, Peng F, Feng X, Wu X. Monocyte/Lymphocyte ratio and cardiovascular disease mortality in peritoneal dialysis patients. Mediators Inflamm. 2020;2020:9852507. doi: 10.1155/2020/9852507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lu W, Zhang K, Chang X, Yu X, Bian J. The association between systemic immune-inflammation index and postoperative cognitive decline in elderly patients. Clin Interv Aging. 2022;17:699–705. doi: 10.2147/CIA.S357319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Jin Z, Wu Q, Chen S, Gao J, Li X, Zhang X, et al. The Associations of two novel inflammation indexes, SII and SIRI with the risks for cardiovascular diseases and all-cause mortality: a ten-year follow-up study in 85,154 individuals. J Inflamm Res. 2021;14:131–140. doi: 10.2147/JIR.S283835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lin KB, Fan FH, Cai MQ, Yu Y, Fu CL, Ding LY, et al. Systemic immune inflammation index and system inflammation response index are potential biomarkers of atrial fibrillation among the patients presenting with ischemic stroke. Eur J Med Res. 2022;27(1):106. doi: 10.1186/s40001-022-00733-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Xie QK, Chen P, Hu WM, Sun P, He WZ, Jiang C, et al. The systemic immune-inflammation index is an independent predictor of survival for metastatic colorectal cancer and its association with the lymphocytic response to the tumor. J Transl Med. 2018;16(1):273. doi: 10.1186/s12967-018-1638-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.He L, Xie X, Xue J, Xie H, Zhang Y. Association of the systemic immune-inflammation index with all-cause mortality in patients with arteriosclerotic cardiovascular disease. Front Cardiovasc Med. 2022;9:952953. doi: 10.3389/fcvm.2022.952953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wu S, Shi X, Zhou Q, Duan X, Zhang X, Guo H. The association between systemic immune-inflammation index and all-cause mortality in acute ischemic stroke patients: analysis from the MIMIC-IV database. Emerg Med Int. 2022;2022:4156489. doi: 10.1155/2022/4156489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Xiao S, Wang Z, Zuo R, Zhou Y, Yang Y, Chen T, et al. Association of systemic immune inflammation index with all-cause, cardiovascular disease, and cancer-related mortality in patients with cardiovascular disease: a cross-sectional study. J Inflamm Res. 2023;16:941–961. doi: 10.2147/JIR.S402227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Fest J, Ruiter R, Ikram MA, Voortman T, van Eijck CHJ, Stricker BH. Reference values for white blood-cell-based inflammatory markers in the Rotterdam study: a population-based prospective cohort study. Sci Rep. 2018;8(1):10566. doi: 10.1038/s41598-018-28646-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Huang J, Zhang Q, Wang R, Ji H, Chen Y, Quan X, et al. Systemic immune-inflammatory index predicts clinical outcomes for elderly patients with acute myocardial infarction receiving percutaneous coronary intervention. Med Sci Monit. 2019;25:9690–9701. doi: 10.12659/MSM.919802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Fu H, Zheng J, Cai J, Zeng K, Yao J, Chen L, et al. Systemic Immune-Inflammation Index (SII) is useful to predict survival outcomes in patients after liver transplantation for hepatocellular carcinoma within Hangzhou criteria. Cell Physiol Biochem. 2018;47(1):293–301. doi: 10.1159/000489807. [DOI] [PubMed] [Google Scholar]
- 32.Zuo PY, Chen XL, Liu YW, et al. Non-HDL-cholesterol to HDL-cholesterol ratio as an independent risk factor for the development of chronic kidney disease. Nutr Metab Cardiovasc Dis. 2015;25:582–597. doi: 10.1016/j.numecd.2015.03.003. [DOI] [PubMed] [Google Scholar]
- 33.Yang TL, Lin YC, Lin YC, Huang CY, Chen HH, Wu MS. Total bilirubin in prognosis for mortality in end-stage renal disease patients on peritoneal dialysis therapy. J Am Heart Assoc. 2017;6(12):e007507. doi: 10.1161/JAHA.117.007507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Liu S, Yang M, Zhao Q, Zhang L, Chen Q, Wang Y. Platelet-to-lymphocyte ratio is associated with the mortality in peritoneal dialysis patients. Iran J Kidney Dis. 2021;15(3):206–212. [PubMed] [Google Scholar]
- 35.Ding P, Yang P, Sun C, Tian Y, Guo H, Liu Y, et al. Predictive effect of systemic immune-inflammation index combined with prognostic nutrition index score on efficacy and prognosis of Neoadjuvant intraperitoneal and systemic paclitaxel combined with Apatinib conversion therapy in gastric cancer patients with positive peritoneal lavage cytology: a prospective study. Front Oncol. 2021;11:791912. doi: 10.3389/fonc.2021.791912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ding P, Guo H, Sun C, Yang P, Kim NH, Tian Y, et al. Combined systemic immune-inflammatory index (SII) and prognostic nutritional index (PNI) predicts chemotherapy response and prognosis in locally advanced gastric cancer patients receiving neoadjuvant chemotherapy with PD-1 antibody sintilimab and XELOX: a prospective study. BMC Gastroenterol. 2022;22(1):121. doi: 10.1186/s12876-022-02199-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Cho Y, Hawley CM, Johnson DW. Clinical causes of inflammation in peritoneal dialysis patients. Int J Nephrol. 2014;2014:909373. doi: 10.1155/2014/909373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Cobo G, Lindholm B, Stenvinkel P. Chronic inflammation in end-stage renal disease and dialysis. Nephrol Dial Transplant. 2018;33(suppl_3):iii35–iii40. doi: 10.1093/ndt/gfy175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Xie R, Liu X, Wu H, Liu M, Zhang Y. Associations between systemic immune-inflammation index and abdominal aortic calcification: results of a nationwide survey. Nutr Metab Cardiovasc Dis. 2023;3:1437. doi: 10.1016/j.numecd.2023.04.015. [DOI] [PubMed] [Google Scholar]
- 40.Stenvinkel P, Heimburger O, Paultre F, Diczfalusy U, Wang T, Berglund L, et al. Strong association between malnutrition, inflammation, and atherosclerosis in chronic renal failure. Kidney Int. 1999;55(5):1899–1911. doi: 10.1046/j.1523-1755.1999.00422.x. [DOI] [PubMed] [Google Scholar]
- 41.Chen G, Tan C, Liu X, Wang X, Tan Q, Chen Y. Associations between systemic immune-inflammation index and diabetes mellitus secondary to pancreatic ductal adenocarcinoma. J Clin Med. 2023;12(3):756. doi: 10.3390/jcm12030756. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Supplementary Table 1.
Additional file 2: Supplementary Figure 1. Sample size statistical efficiency. The figure shows the degree of research reliability corresponding to different sample size and odd ratio. The horizontal axis represents the sample size, the vertical axis represents the degree of reliability of the study. It can be seen that when the odd ratio value is 1.8 and the sample size is 1700, the test efficiency is over 0.95, which is already very reliable.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.