

Abstract
Background:
It is unclear how older adults with chronic conditions, who have greater risk of alcohol-related adverse outcomes, used alcohol throughout the COVID-19 pandemic. We assess changes in hazardous drinking prevalence May 2020-December 2021 and factors associated with hazardous drinking.
Methods:
Data are from structured phone interviews of older adults (age 60+) with chronic conditions (e.g. hypertension, diabetes, pulmonary disease, heart disease) in a Chicago-based longitudinal cohort (Chicago COVID-19 Comorbidities survey, Waves 3–7, n=247). We tested differences in the prevalence of hazardous drinking (defined as AUDIT-C score of 3+ for women and 4+ for men) across waves for the full sample, by demographic group (sex, race and ethnicity), and by chronic condition burden (<3 conditions, 3+ conditions). Generalized estimating equations investigated associations of hazardous drinking with sociodemographic and pandemic coping-related factors (stress, loneliness, outside contacts, depression, anxiety).
Results:
Participants were 66.8% female; 27.9% non-Hispanic Black, 14.2% Hispanic, 4.9% other race. Hazardous drinking was reported by 44.9% of participants in May 2020, but declined to 23.1% by July-August 2020 and continued to slowly decline to 19.4% by September-December 2021. Differences from May 2020 were significant at the 0.05 level. Subgroups followed similar trajectories. Hazardous drinking prevalence was initially higher but declined more among men than women, consistently higher among non-Hispanic White respondents than among Hispanic and non-Hispanic Black respondents, and declined more rapidly among adults with 3+ chronic conditions. In adjusted models, race and ethnicity were associated with lower prevalence of hazardous drinking (non-Hispanic Black: adjusted prevalence ratio (aPR) =0.50, 95% confidence interval (CI) = 0.33, 0.74; other race: aPR=0.26, 95% CI=0.09, 0.81, compared with non-Hispanic White). No coping-related factors were significantly associated with hazardous drinking.
Conclusion:
Among a cohort of older adults with chronic conditions, almost half engaged in hazardous drinking in early summer of the COVID-19 pandemic. While prevalence fell, these rates reinforce the need for alcohol screening and intervention in clinical settings among this population.
Keywords: hazardous drinking, chronic conditions, COVID-19
Introduction
Since its appearance in the United States in early 2020, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease 2019 (COVID-19) have wrought waves of morbidity and mortality as well as fear, anxiety, social isolation, economic hardship, and other significant disruptions to daily life. It is likely that these circumstances and the resultant psychological distress, coupled with decreased access to substance use treatment services,1,2 led to increased alcohol use among U.S. adults. It is well-recognized that coping with negative feelings can motivate drinking.3–5 Indeed, studies of the early months of the COVID-19 pandemic identified increases in the average number of drinking days among U.S. adults, albeit with considerable heterogeneity across groups.6–8
It remains unclear, however, how older adults in the U.S. have used alcohol throughout the pandemic. Older adults experienced significant psychological stressors throughout this time given their higher risk of severe illness;9 they were more likely to perceive the disease as a major threat to health,10 to have lost partners and peers,11 and to have engaged in social distancing than younger adults.12–14 While work suggests that older adults have been more resilient in terms of mental health than their younger counterparts,15,16 older adults have still experienced declines in mental health from pre-pandemic levels and approximately one in five older adults have reported experiencing feelings of loneliness as a result of the pandemic.17,18 Yet, evidence on alcohol use by U.S. older adults during the pandemic is limited, particularly in terms of longer-term effects. Most of the few studies assessing changes in drinking habits focused on the earliest months in the pandemic (i.e. spring and early summer of 2020).6,19 Studies considering the relationships between psychological distress and changes in alcohol use have also yielded inconsistent results.19–21
Alcohol use can be particularly detrimental to the health of older adults, especially those with chronic conditions. The body’s ability to metabolize alcohol slows with age22 and alcohol use places older adults at greater risk for falls, injuries, and adverse interactions with medications.22 Alcohol can also contribute to many of the chronic conditions prevalent among this age group (e.g. hypertension, diabetes, cancer, dementia).23–26 As such, it is critical that we better understand how older adults have consumed alcohol throughout the pandemic and any predictors of hazardous drinking (drinking in a way that puts one at risk of physical or psychological harm27) amongst this population.
In this analysis, we assess rates of hazardous drinking among older adults with chronic conditions who participated in the Chicago COVID-19 Comorbidities (C3) survey, a longitudinal cohort, from May 2020 through December 2021 as well as differences by sex, by race and ethnicity, and by burden of chronic conditions. We also investigate the association of various sociodemographic factors and factors related to coping with the COVID-19 pandemic (e.g. stress, loneliness, outside contacts, depression, and anxiety) with hazardous drinking. We hypothesize that high levels of such factors will be associated with hazardous drinking, as suggested by pre-pandemic work linking bereavement, loss of work, boredom, and loneliness with higher alcohol use among older adults.22,28,29
Methods
Data
The data for this study came from the Chicago COVID-19 Comorbidities (C3) survey, an ongoing longitudinal telephone-based survey of Chicago-based adults with at least one chronic condition (e.g. heart disease, pulmonary disease, diabetes, hypertension). The objective of the survey is to assess COVID-19 knowledge, attitudes, and behaviors among a cohort of adults who would be at higher risk for severe illness.30 Participants for the survey were recruited from four other federally funded research projects that themselves recruited from five academic medical centers and two federally qualified health centers in greater Chicago. These studies varied in their eligibility criteria but generally recruited middle-aged and older, primarily English-speaking adults with chronic conditions. All studies excluded individuals who had severe and uncorrectable cognitive, visual, or hearing impairments that would compromise their ability to fully participate.
To be eligible for the C3 survey, individuals had to have at least one chronic condition, have participated in their parent study since 2018 (to ensure the most accurate data), and have given consent to be contacted for future research. These individuals were contacted by phone by trained interviewers and invited to participate in the C3 survey. After obtaining verbal consent, interviewers administered the survey and recorded responses in REDCap software. The initial survey took approximately ten minutes to complete, and respondents were provided a $10 gift certificate in compensation. After the initial survey, additional consent procedures took place at Waves 2 and 5 to include the additional waves of data collection. The study was approved by the Northwestern University Institutional Review Board. Additional details on the C3 survey and the parent projects can be found in the supplementary materials and in previous publications.30–35
The first wave of the survey took place March 13–20, 2020. Of 2,010 eligible individuals, 733 were contacted and 630 completed the survey (85.9% cooperation rate) and were eligible to participate in subsequent waves. This study is limited to respondents aged 60 and older at the time of the interview (n=436). This study uses data from Waves 3 through 7, which took place in May 2020, July-August 2020, November 2020-March 2021, April-July 2021, and September-December 2021, respectively. For reference, the Illinois stay-at-home order expired June 5, 2020, between Waves 3 and 4. Data from Waves 1 and 2 were not used because information on alcohol use was not collected until Wave 3.
The Wave 3 survey was undertaken by 395 respondents aged 60 and older, of which 351 had complete data on relevant variables (88.9%). To assess changes in drinking across waves, the sample was restricted to respondents who subsequently completed surveys in each of Waves 4 through 7 (n=247, 70.4%). Attrition at each wave and sociodemographic characteristics of those who were and were not lost to follow up are presented in the supplementary materials (Supplementary Tables S2 and S3).
Measures
Outcome
Hazardous drinking was assessed and defined using the Alcohol Use Disorders Identification Test Consumption (AUDIT-C) questions, a validated three-item instrument used to screen for hazardous alcohol use and alcohol use disorder.36–38 This instrument is a shorter version of the ten-item AUDIT, which includes questions about typical alcohol consumption as well as drinking behaviors (e.g. drinking first thing in the morning) and alcohol-related consequences (e.g. injuries from drinking).27 The AUDIT-C is comprised of only the questions related to alcohol consumption, but performs similarly to the ten-item AUDIT.36,39
In each of the survey waves under study, participants were asked the instrument’s three questions about their current alcohol use: “how often do you have a drink containing alcohol?”, “how many standard drinks containing alcohol do you have on a typical day?”, and “how often do you have six or more drinks on one occasion?”. Answers were scored (see Supplementary Table S4) and women with scores of three or higher and men with scores of four or higher were considered to engage in hazardous drinking.39
Correlates of hazardous drinking
Sociodemographic factors
Multiple sociodemographic factors were assessed as possible correlates of hazardous drinking. These factors included sex, with categories of male or female, and age, measured categorically as 60–69 years old and 70 years old or above. Race and ethnicity were measured using a variable with mutually exclusive categories for non-Hispanic Black, non-Hispanic White, Hispanic of any race, and other race or ethnicity. Highest level of education was collected as high school or less, some college, and college or higher. Employment status was assessed using an indicator variable denoting whether a participant was currently working for pay or not, and another indicator was used to denote whether the participant was living under the poverty level, as indicated by the 2020 federal poverty guidelines.40 The number of household members was measured with a discrete variable and marital status was assessed using an indicator variable for currently married versus not married. Finally, chronic disease burden was measured using an indicator variable for having three or more chronic conditions compared to fewer than three conditions. Employment status was time varying (assessed during each wave); baseline measurements were used for all other factors (obtained from the most recent parent study interview).
COVID-19 coping-related factors
We also considered several factors related to how respondents were responding to and coping with the COVID-19 pandemic. These factors, all time-varying and assessed at each survey wave, included stress, loneliness, having outside contacts, depression, and anxiety. For stress and loneliness, participants were asked, over the past week, how often they felt “nervous or ‘stressed’ because of the coronavirus” and how often they felt “alone or lonely because of the coronavirus,” with possible responses of “never,” “some of the time,” “most of the time,” or “all of the time.” Responses were dichotomized to capture whether participants reported having these feelings never or some of the time versus most or all of the time. To assess outside contacts, participants were asked if there were “any other people outside those in [their] household that [they were] seeing regularly or having close contact with,” and having such contacts was operationalized with an indicator variable. Both depression and anxiety were assessed using the validated Patient-Reported Outcomes Measurement Information System four-item short-form questionnaires.41 The raw scores were transformed into T-scores with a mean of 50 and a standard deviation of ten. These scores are normed against the general U.S. population and higher scores indicate more symptoms.
Statistical analysis
We first calculated descriptive statistics for the sample at Wave 3 (means and standard deviations or frequencies and percentages). We then examined the prevalence of hazardous drinking in each survey wave and tested for significant differences between prevalence at Wave 3 and prevalence in each subsequent wave (Waves 4, 5, 6, and 7) using McNemar’s tests. Separate tests were conducted for each of the subsequent waves, comparing prevalence in that wave alone to prevalence at Wave 3, to ensure that any changes that occurred during particular periods could be observed. These tests were conducted for the full sample and then stratified by sex (male and female), by race and ethnicity (non-Hispanic Black, Hispanic, and non-Hispanic White only due to limited representation of other race and ethnicities), and by chronic condition burden (three or more conditions versus fewer than three conditions).
Finally, we investigated the associations of each of the sociodemographic and COVID-19 coping-related factors with hazardous drinking in this population. We estimated modified Poisson models42 using generalized estimating equations. We included each of the observations available per respondent (Waves 3, 4, 5, 6, and 7) and specified an exchangeable covariance structure to account for within-person correlation. Model 1 included the sociodemographic factors, Model 2 included the coping-related factors, and Model 3 included both sets of factors. All models also adjusted for survey wave to account for unobserved time-related confounders and for parent study to account for any study-specific similarities among respondents. Estimates were considered statistically significant at the 0.05 level. All analyses were conducted in Stata version 17.0.
Results
Approximately two thirds of the C3 respondents were women (66.8%) and one third were men (33.2%). The mean age was 69 years (standard deviation = 5.9). Almost half of the respondents were non-Hispanic White (53.0%), around a quarter were non-Hispanic Black (27.9%), 14.2% were Hispanic, and only 4.9% were of other races or ethnicities. Just over half of respondents (51.4%) had three or more chronic conditions. These and other sociodemographic characteristics are presented in Table 1.
Table 1.
C3 respondent characteristics at survey wave 3, May 2020 (n=247)
| Mean ± SD or n (%) | |
|---|---|
|
| |
| Sex | |
| Male | 82 (33.2) |
| Female | 165 (66.8) |
| Race and ethnicity | |
| Non-Hispanic Black | 69 (27.9) |
| Hispanic | 35 (14.2) |
| Non-Hispanic White | 131 (53.0) |
| Other | 12 (4.9) |
| Age (category) | |
| 60–69 years old | 140 (56.7) |
| 70+ years old | 107 (43.3) |
| Age (mean) | 69 ± 5.9 |
| Educational attainment | |
| High school degree of less | 52 (21.1) |
| Some college | 59 (23.9) |
| College degree or higher | 136 (55.1) |
| Currently working for pay | |
| Yes | 46 (18.6) |
| No | 201 (81.4) |
| Living below poverty level | |
| Yes | 50 (20.2) |
| No | 197 (79.8) |
| Marital status | |
| Married | 101 (40.9) |
| Not married | 146 (59.1) |
| Number of household members | 0.9 ± 1.0 |
| Number of chronic conditions | |
| <3 conditions | 120 (48.6) |
| 3+ conditions | 127 (51.4) |
| Stressed due to COVID-19 | |
| Never or some of the time | 206 (83.4) |
| Most or all of the time | 41 (16.6) |
| Lonely due to COVID-19 | |
| Never or some of the time | 214 (86.6) |
| Most or all of the time | 33 (13.4) |
| Sees other people regularly | |
| Yes | 81 (32.8) |
| No | 166 (67.2) |
| PROMIS Anxiety t-score | 49.9 ± 8.2 |
| PROMIS Depression t-score | 51.7 ± 8.6 |
At the Wave 3 survey (May 2020), only 16.6% of respondents reported feeling stressed most or all of the time because of COVID-19. Only 13.4% reported feeling lonely most or all of the time, despite the fact that the majority of respondents (67.2%) did not regularly see people outside of their households (see Table 1).
Almost half of respondents (44.9%) engaged in hazardous drinking at Wave 3 (May 2020). This rate declined substantially by Wave 4 (July-August 2020) to 23.1% and then declined only minimally thereafter: prevalence of hazardous drinking was 21.1% at Wave 5 (Nov. 2020-Mar. 2021), 19.8% at Wave 6 (April-July 2021), and 19.4% at Wave 7 (Sep.-Dec. 2021). All prevalences at later waves were significantly different at the 0.05 level from the prevalence at Wave 3 in McNemar’s tests. Similar trajectories were observed across subgroups. The prevalence of hazardous drinking was considerably higher among men than among women in Wave 3 (56.1% compared to 39.4%). However, prevalence declined more substantially among men throughout the waves, resulting in lower prevalence among men as compared with women by Wave 7 (14.6% compared to 21.8%). Across all survey waves, non-Hispanic White respondents had the highest prevalence of hazardous drinking, followed by Hispanic respondents and non-Hispanic Black respondents. The trajectory for Hispanic respondents deviated from trajectories observed for other respondents, as they experienced a slight uptick in prevalence at Wave 7. Prevalence of hazardous drinking was relatively similar across chronic condition burden at Wave 3, but it declined more among those with three or more conditions than those with fewer than three conditions in the subsequent waves. These results are presented in Figure 1 and Table 2.
Figure 1.
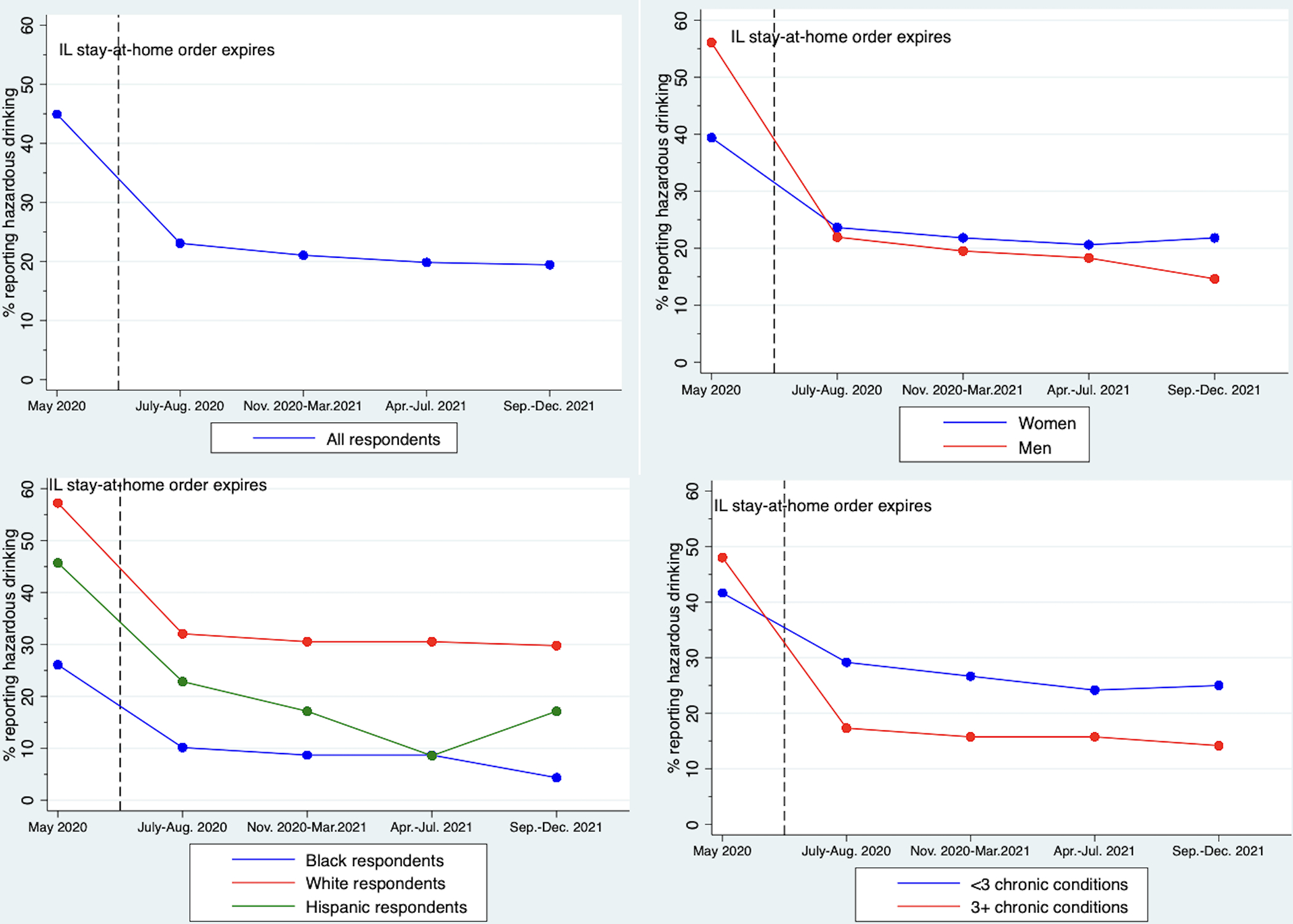
Prevalence of hazardous drinking across survey waves for full sample and by sex, race and ethnicity, and chronic condition burden
Table 2.
Prevalence of hazardous drinking among C3 participants by survey wave
| Wave 3 May 2020 | Wave 4 July-Aug. 2020 | Wave 5 Nov. 2020 - Mar. 2021 | Wave 6 April - July 2021 | Wave 7 Sep.-Dec. 2021 | |
|---|---|---|---|---|---|
|
| |||||
| % | % p-value | % p-value | % p-value | % p-value | |
|
| |||||
| Full cohort (n=247) | 44.9 | 23.1 <0.001 |
21.1 <0.001 |
19.8 <0.001 |
19.4 <0.001 |
| By sex | |||||
| Women (n=165) | 39.4 | 23.6 <0.001 |
21.8 <0.001 |
20.6 <0.001 |
21.8 <0.001 |
| Men (n=82) | 56.1 | 22.0 <0.001 |
19.5 <0.001 |
18.3 <0.001 |
14.6 <0.001 |
| By race and ethnicity | |||||
| Non-Hispanic Black respondents (n=69) | 26.1 | 10.1 0.008 |
8.7 0.005 |
8.7 0.001 |
4.4 0.001 |
| Hispanic respondents (n=35) | 45.7 | 22.9 0.021 |
17.1 0.004 |
8.6 <0.001 |
17.1 0.008 |
| Non-Hispanic White respondents (n=131) | 57.3 | 32.1 <0.001 |
30.5 <0.001 |
30.5 <0.001 |
29.8 <0.001 |
| By chronic condition burden | |||||
| <3 conditions (n=120) | 41.7 | 29.2 0.002 |
26.7 <0.001 |
24.2 <0.001 |
25.0 <0.001 |
| 3+ conditions (n=127) | 48.0 | 17.3 <0.001 |
15.8 <0.001 |
15.8 <0.001 |
14.2 <0.001 |
Note. Tables displays prevalence (%) of hazardous drinking and p-values associated with McNemar’s chi-squared statistics comparing prevalence at specified wave to prevalence at Wave 3.
In the population-averaged model adjusting for both sociodemographic and COVID-19 coping-related factors (Model 3), only race was significantly associated with hazardous drinking (see Table 3). Non-Hispanic Black respondents and respondents of other race or ethnicity had lower prevalence of hazardous drinking as compared with non-Hispanic White respondents (adjusted prevalence ratio (aPR) =0.50, 95% confidence interval (CI) = 0.33, 0.74; aPR=0.26, 95% CI=0.09, 0.81, respectively). None of the other sociodemographic or coping-related factors were significantly associated with hazardous drinking.
Table 3.
Associations of sociodemographic and COVID-19 related factors with hazardous drinking among C3 respondents, May 2020-December 2021 (n=1,235)
| Model 1 Adjusted prevalence ratio (95% CI) | Model 2 Adjusted prevalence ratio (95% CI) | Model 3 Adjusted prevalence ratio (95% CI) | |
|---|---|---|---|
|
| |||
| Sociodemographic factors | |||
| Sex | |||
| Male | Ref. | Ref. | |
| Female | 0.96 (0.71, 1.30) |
0.89 (0.66, 1.21) |
|
| Race and ethnicity | |||
| Non-Hispanic White | Ref. | Ref. | |
| Non-Hispanic Black |
0.47
***
(0.31, 0.70) |
0.50
***
(0.33, 0.74) |
|
| Hispanic | 0.84 (0.53, 1.33) |
0.83 (0.53, 1.31) |
|
| Other |
0.25
*
(0.07, 0.83) |
0.26
*
(0.09, 0.81) |
|
| Age | |||
| 60–69 years old | Ref. | Ref. | |
| 70+ years old | 0.92 (0.69, 1.21) |
0.91 (0.69, 1.21) |
|
| Educational attainment | |||
| High school degree of less | Ref. | Ref. | |
| Some college |
1.74
*
(1.05, 2.90) |
1.60~ (0.97, 2.64) |
|
| College degree or higher | 1.60~ (0.97, 2.63) |
1.49 (0.92, 2.41) |
|
| Currently working for pay | |||
| No | Ref. | Ref. | |
| Yes | 1.13 (0.90, 1.41) |
1.14 (0.91, 1.44) |
|
| Living below poverty level | |||
| No | Ref. | Ref. | |
| Yes | 0.80 (0.52, 1.22) |
0.84 (0.56, 1.27) |
|
| Marital status | |||
| Not married | Ref. | Ref. | |
| Married | 1.21 (0.90, 1.63) |
1.21 (0.90, 1.64) |
|
| Number of household members | 0.89 (0.74, 1.06) |
0.90 (0.76, 1.06) |
|
| Number of chronic conditions | |||
| <3 conditions | Ref. | Ref. | |
| 3+ conditions | 1.01 (0.73, 1.40) |
1.02 (0.74, 1.40) |
|
| COVID-19-related factors | |||
| Stressed due to COVID-19 | |||
| Never or some of the time | Ref. | Ref. | |
| Most or all of the time | 0.98 (0.78, 1.23) |
1.00 (0.79, 1.28) |
|
| Lonely due to COVID-19 | |||
| Never or some of the time | Ref. | Ref. | |
| Most or all of the time | 1.17 (0.90, 1.53) |
1.21 (0.92, 1.58) |
|
| Sees other people regularly | |||
| No | Ref. | Ref. | |
| Yes | 0.89 (0.76, 1.05) |
0.90 (0.77, 1.06) |
|
| PROMIS Anxiety t-score | 1.00 (0.99, 1.02) |
1.00 (0.99, 1.02) |
|
| PROMIS Depression t-score | 1.00 (0.99, 1.02) |
1.01 (0.99, 1.02) |
|
Note. Estimates are from modified Poisson regression (i.e. with robust standard errors) using generalized estimating equations with exchangeable covariance structure. Models include 1,235 observations from 247 respondents. Models also control for survey wave and parent study. 95% CI = 95% confidence interval. Ref. = reference category. Boldface indicates statistical significance at 0.05 level
(p<0.001,
p<0.01,
p<0.05,
p<0.10)
Discussion
Among older adults in a Chicago-based cohort, nearly half engaged in hazardous drinking in the early summer months of the COVID-19 pandemic. This rate declined considerably by mid- to late summer 2020 and throughout the following years, but, even at its lowest prevalence, over 19% of the population reported drinking in ways considered hazardous. Race was associated with hazardous drinking but stress, loneliness, outside contacts, depression, and anxiety resulting from the pandemic were not associated with hazardous drinking.
The finding that such a large percentage of respondents engaged in hazardous drinking is alarming, but not entirely surprising. Alcohol use, both moderate and hazardous, is not uncommon among older adults: according to the National Survey on Drug Use and Health, in 2019, almost 44% of adults age 65 or older reported using alcohol in the past month and over 10% engaged in binge drinking.43 Rates appear to have been similar in 2020, although they cannot be directly compared due to changes in survey methodology.44 It should be noted that the AUDIT-C can yield highly variable rates of hazardous drinking when used in different populations of older adults.45–48 For instance, in a study of residents of a large planned retirement community in Florida, approximately 15% engaged in hazardous drinking according to the cut-offs used in this study,45 but in a study of community dwelling adults ages 55–70 in New Zealand, 57% of men and 44% of women engaged in hazardous drinking.46 Thus, while high, the rates observed in this study are plausible.
The decrease in prevalence observed between May and July-August 2020 is substantial and corresponds with the expiration of the stay-at-home order in Illinois, suggesting that the locked-down early months of the pandemic did have a substantial impact on the drinking of older adults with chronic conditions. To our knowledge, no other studies have assessed hazardous drinking as determined by the AUDIT-C among older adults in the U.S. during the COVID-19 pandemic, making comparisons to the other COVID-19 literature challenging. However, one study of adults of all ages in Arkansas conducted May-June 2020 found that 35% engaged in hazardous drinking as determined by the AUDIT-C.49 Another using a national convenience sample from April-September 2020 found that the number engaging in hazardous drinking increased from 21% to 41% for those under stay-at-home orders but did not increase for those who were not.50 Such findings support the numbers observed in this study.
The results regarding race and hazardous drinking correspond with what is known from previous research about alcohol use across minoritized populations. National surveys suggest that rates of binge drinking and alcohol consumption in general are lower among non-Hispanic Black adults than among non-Hispanic White adults in the U.S,51–53 despite the fact that Black Americans face greater social and economic hardships linked with distress and alcohol use.54,55 One theory posited to explain this trend is that resources that may protect against heavy drinking, such as religiosity, “drier” drinking norms and social networks, and family social support, are more prevalent in Black communities than in White communities.56 Previous research has found that Black men and women were more likely than White men and women to be lifetime abstainers throughout early adulthood and middle age57 and that, among past-year monthly drinkers aged 55 and older, Black respondents were more likely to cease drinking than White respondents.58 Protective resources may have been influenced by the pandemic. The findings regarding respondents of other race and ethnicities are difficult to contextualize within the literature given the diversity inherent in this categorization, and the results should be interpreted with caution given the small number of respondents in this category (n=12).
The findings that none of the COVID-19 coping-related factors were associated with hazardous drinking are contrary to our hypotheses, which were based on pre-pandemic findings about psychological and situational predictors of alcohol use amongst older adults.22,28,29 Drinking to cope with negative emotions is common motivation for alcohol use among all ages,3,59 and previous work has identified associations of bereavement, involuntary retirement, daily boredom, and loneliness with greater alcohol use among older adults.22,28,29 However, in aggregate, the evidence on such predictors is mixed,22 and other works on their relationships with alcohol use among older adults during the pandemic have yielded conflicting results. One study using a national sample of adults over age 55 found increases in drinking were related to pandemic-induced depression, anxiety, and lonliness,19 yet another using the Medicare Current Beneficiary Survey found changes in alcohol use was not linked to depression or anxiety about COVID-19.21 While our findings relate to engagement in hazardous drinking rather than changes in drinking over time, they are more consistent with those of the latter study. As such, they provide additional support to other findings about the resiliency of this population during the pandemic.15,16 The models we estimated did control for survey wave, so it is also possible that the COVID-19-related factors under study are not associated with hazardous drinking independent of the impact of the initial lock-down period.
While we do find that rates of hazardous drinking declined following May 2020, approximately one in five respondents engaged in hazardous drinking throughout the remaining study period. As noted, such drinking can be detrimental to the health of older adults with chronic conditions. In addition to increasing risks of injuries and adverse reactions to medications, hazardous drinking can contribute to chronic conditions (e.g. alcohol use has a dose response relationship with blood pressure25,60) and can also complicate the management of these conditions (e.g. hinders medication and diet adherence, symptom monitoring61–63). Evidence suggests that, among individuals who have hypertension and diabetes, having alcohol use disorder is associated with greater odds of adverse condition-related events (e.g. cerebrovascular events, renal failure, myocardial infarction)64,65 as well as higher costs and greater service utilization.66 As such, the results of this study speak to the importance of having robust processes for screening, brief intervention, and referral to treatment for older adults, particularly those with chronic conditions, in primary and specialty care. Rates of screening and brief intervention are currently quite low67 and are below rates of receipt by younger adults.68,69 Given the hazardous drinking observed in this analysis, it is critical that we develop care pathways and processes that may improve the delivery of these services and care coordination for individuals who need further treatment.
This study is the first to assess longer-term hazardous drinking among U.S. older adults with chronic conditions during the COVID-19 pandemic. However, it is subject to several important limitations. First, the data are self-reported, and respondents may not have felt comfortable truthfully reporting alcohol use. However, if so, the rates of hazardous drinking that we observed would be underestimates. Second, the AUDIT-C was not administered in survey Waves 1 and 2 nor in the parent studies from which respondents were recruited. As such, we are not able to observe drinking patterns in the pandemic’s earliest days or changes in habits from prior to the pandemic. Third, given the sample was limited to older adults with chronic conditions residing in Chicago, the results are not generalizable to a larger or more diverse population.
Conclusion
In this study, we find that, among older adults with chronic conditions in a Chicago-based cohort, almost half engaged in hazardous drinking in the early summer of May 2020, during the state’s COVID-19 stay-at-home order. The rate of hazardous drinking declined substantially by the end of the summer and remained lower throughout the subsequent years, but still 19% of these respondents continued to engage in hazardous drinking. The considerable rates of hazardous drinking seen in both the peak and troughs of the pandemic in this population, which is at higher risk of alcohol-related adverse outcomes due to older age and chronic condition burden, speaks to the need for better identification and treatment of hazardous drinking in health care settings, regularly and in exceptional circumstances.
Supplementary Material
Key points:
44.9% of older adults with chronic conditions reported hazardous drinking in May 2020.
Prevalence declined by late summer to 23.1%, remaining similar through Dec. 2021.
Why does this matter?
Given higher risk of alcohol-related adverse outcomes, screening and brief intervention for hazardous drinking is warranted.
Acknowledgements:
Conflicts of interest:
MSW reports grants from the NIH during the conduct of the study; grants from Merck, the Gordon and Betty Moore Foundation, the NIH, and Eli Lilly outside the submitted work; and personal fees from Sanofi, Pfizer, and Luto outside the submitted work. MRC reports grants from the NIH during the conduct of the study and personal fees from the Centers for Disease Control and Prevention for contract work outside the submitted work. RML reports grants from the NIH (NIA, NINDS) and awards from the Health Assessment Lab. AZP was supported by a NIH T32 training grant from NHLBI. MB has no conflicts.
Sponsors’ role:
The sponsors had no role in the design, methods, subject recruitment, data collections, analysis, and preparation of this paper.
Disclosures:
This work was supported by the following grants from the National Institutes of Health: R01AG030611, R01AG046352, R01DK110172, R01NR015444, and T32HL069771. It has not been submitted to or presented at meetings nor published as a preprint.
Footnotes
Supplementary materials: Additional data descriptions
References
- 1.Attonito J, Villalba K, Fontal S. Priorities for Alcohol Use Disorder Treatment and Prevention During COVID-19’s Second Wave. Am J Public Health. 2021;111(3):359–362. doi: 10.2105/AJPH.2020.306070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mellis AM, Potenza MN, Hulsey JN. COVID-19-related treatment service disruptions among people with single- and polysubstance use concerns. Journal of Substance Abuse Treatment. 2021;121:108180. doi: 10.1016/j.jsat.2020.108180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sher KJ, Grekin ER, Williams NA. The Development of Alcohol Use Disorders. Annu Rev Clin Psychol. 2005;1(1):493–523. doi: 10.1146/annurev.clinpsy.1.102803.144107 [DOI] [PubMed] [Google Scholar]
- 4.Cooper ML, Kuntsche E, Levitt A, Barber LL, Wolf S. Motivational Models of Substance Use. Vol 1. (Sher KJ, ed.). Oxford University Press; 2015. doi: 10.1093/oxfordhb/9780199381678.013.017 [DOI] [Google Scholar]
- 5.Mezquita L, Ibáñez MI, Moya J, Villa H, Ortet G. A Longitudinal Examination of Different Etiological Pathways to Alcohol Use and Misuse. Alcohol Clin Exp Res. 2014;38(6):1770–1779. doi: 10.1111/acer.12419 [DOI] [PubMed] [Google Scholar]
- 6.Nordeck CD, Riehm KE, Smail EJ, et al. Changes in drinking days among United States adults during the COVID-19 pandemic. Addiction. Published online July 12, 2021:add.15622. doi: 10.1111/add.15622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Pollard MS, Tucker JS, Green HD. Changes in Adult Alcohol Use and Consequences During the COVID-19 Pandemic in the US. JAMA Netw Open. 2020;3(9):e2022942. doi: 10.1001/jamanetworkopen.2020.22942 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sohi I, Chrystoja BR, Rehm J, et al. Changes in alcohol use during the COVID-19 pandemic and previous pandemics: A systematic review. Alcohol Clin & Exp Res. 2022;46(4):498–513. doi: 10.1111/acer.14792 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.National Center for Chronic Disease Prevention and Health Promotion. COVID-19 Risks and Vaccine Information for Older Adults. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; https://www.cdc.gov/aging/covid19/covid19-older-adults.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fneed-extra-precautions%2Folder-adults.html [Google Scholar]
- 10.Schaeffer K, Rainie L. Experiences with the COVID-19 Outbreak Can Vary for Americans of Different Ages. Pew Research Center; 2020. https://www.pewresearch.org/fact-tank/2020/06/16/experiences-with-the-covid-19-outbreak-can-vary-for-americans-of-different-ages/ [Google Scholar]
- 11.Centers for Disease Control and Prevention. COVID Data Tracker. Published online May 3, 2022. Accessed May 4, 2022. https://covid.cdc.gov/covid-data-tracker/#demographics
- 12.Hutchins HJ, Wolff B, Leeb R, et al. COVID-19 Mitigation Behaviors by Age Group — United States, April–June 2020. MMWR Morb Mortal Wkly Rep. 2020;69(43):1584–1590. doi: 10.15585/mmwr.mm6943e4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kim JK, Crimmins EM. How does age affect personal and social reactions to COVID-19: Results from the national Understanding America Study. Sykes BL, ed. PLoS ONE. 2020;15(11):e0241950. doi: 10.1371/journal.pone.0241950 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Moore RC, Lee AY, Hancock JT, Halley MC, Linos E. Age-Related Differences in Experiences With Social Distancing at the Onset of the COVID-19 Pandemic: A Computational and Content Analytic Investigation of Natural Language From a Social Media Survey. JMIR Hum Factors. 2021;8(2):e26043. doi: 10.2196/26043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cray HV, Vahia IV. Two Years of COVID-19: Understanding Impact and Implications for the Mental Health of Older Adults. The American Journal of Geriatric Psychiatry. 2022;30(4):444–447. doi: 10.1016/j.jagp.2022.02.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Riehm KE, Brenneke SG, Adams LB, et al. Association between psychological resilience and changes in mental distress during the COVID-19 pandemic. Journal of Affective Disorders. 2021;282:381–385. doi: 10.1016/j.jad.2020.12.071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Holaday LW, Oladele CR, Miller SM, Dueñas MI, Roy B, Ross JS. Loneliness, sadness, and feelings of social disconnection in older adults during the COVID -19 pandemic. J American Geriatrics Society. 2022;70(2):329–340. doi: 10.1111/jgs.17599 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Choi NG, Hammaker S, DiNitto DM, Marti CN. COVID-19 and Loneliness among Older Adults: Associations with Mode of Family/Friend Contacts and Social Participation. Clinical Gerontologist. 2022;45(2):390–402. doi: 10.1080/07317115.2021.2013383 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Eastman MR, Finlay JM, Kobayashi LC. Alcohol Use and Mental Health among Older American Adults during the Early Months of the COVID-19 Pandemic. IJERPH. 2021;18(8):4222. doi: 10.3390/ijerph18084222 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Finlay JM, Kler JS, O’Shea BQ, Eastman MR, Vinson YR, Kobayashi LC. Coping During the COVID-19 Pandemic: A Qualitative Study of Older Adults Across the United States. Front Public Health. 2021;9:643807. doi: 10.3389/fpubh.2021.643807 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Robbins R, Weaver MD, Czeisler MÉ, Barger LK, Quan SF, Czeisler CA. Associations Between Changes in Daily Behaviors and Self-Reported Feelings of Depression and Anxiety About the COVID-19 Pandemic Among Older Adults. Kelley J, ed. The Journals of Gerontology: Series B. Published online June 22, 2021:gbab110. doi: 10.1093/geronb/gbab110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kuerbis A, Moore AA, Sacco P, Zanjani F. Alcohol and Aging. Springer; 2016. [Google Scholar]
- 23.Rehm J, Roerecke M. Cardiovascular effects of alcohol consumption. Trends in Cardiovascular Medicine. 2017;27(8):534–538. doi: 10.1016/j.tcm.2017.06.002 [DOI] [PubMed] [Google Scholar]
- 24.Rehm J, Gmel G, Sempos CT, Trevisan M. Alcohol-related morbidity and mortality. Alcohol Res Health. 2003;27(1):39–51. [PMC free article] [PubMed] [Google Scholar]
- 25.Roerecke M, Kaczorowski J, Tobe SW, Gmel G, Hasan OSM, Rehm J. The effect of a reduction in alcohol consumption on blood pressure: a systematic review and meta-analysis. The Lancet Public Health. 2017;2(2):e108–e120. doi: 10.1016/S2468-2667(17)30003-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rehm J, Hasan OSM, Black SE, Shield KD, Schwarzinger M. Alcohol use and dementia: a systematic scoping review. Alz Res Therapy. 2019;11(1):1. doi: 10.1186/s13195-018-0453-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption--II. Addiction. 1993;88(6):791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x [DOI] [PubMed] [Google Scholar]
- 28.Kuerbis A, Sacco P. The impact of retirement on the drinking patterns of older adults: A review. Addictive Behaviors. 2012;37(5):587–595. doi: 10.1016/j.addbeh.2012.01.022 [DOI] [PubMed] [Google Scholar]
- 29.Kuerbis A, Treloar Padovano H, Shao S, Houser J, Muench FJ, Morgenstern J. Comparing daily drivers of problem drinking among older and younger adults: An electronic daily diary study using smartphones. Drug and Alcohol Dependence. 2018;183:240–246. doi: 10.1016/j.drugalcdep.2017.11.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wolf MS, Serper M, Opsasnick L, et al. Awareness, Attitudes, and Actions Related to COVID-19 Among Adults With Chronic Conditions at the Onset of the U.S. Outbreak: A Cross-sectional Survey. Ann Intern Med. 2020;173(2):100–109. doi: 10.7326/M20-1239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lovett RM, Opsasnick L, Russell A, et al. Prevalence of anxiety and depressive symptoms and impact on self-management among adults with chronic conditions in Chicago, Illinois, USA, during the COVID-19 pandemic: a cross-sectional survey. BMJ Open. 2022;12(1):e052495. doi: 10.1136/bmjopen-2021-052495 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.O’Conor R, Arvanitis M, Wismer G, et al. Rationale and design of the regimen education and messaging in diabetes (REMinD) trial. Contemp Clin Trials. 2019;83:46–52. doi: 10.1016/j.cct.2019.06.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bailey SC, Wismer GA, Parker RM, et al. Development and rationale for a multifactorial, randomized controlled trial to test strategies to promote adherence to complex drug regimens among older adults. Contemp Clin Trials. 2017;62:21–26. doi: 10.1016/j.cct.2017.08.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Wolf MS, Curtis LM, Wilson EAH, et al. Literacy, cognitive function, and health: results of the LitCog study. J Gen Intern Med. 2012;27(10):1300–1307. doi: 10.1007/s11606-012-2079-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Serper M, Ladner DP, Curtis LM, et al. Transplant regimen adherence for kidney recipients by engaging information technologies (TAKE IT): Rationale and methods for a randomized controlled trial of a strategy to promote medication adherence among transplant recipients. Contemporary Clinical Trials. 2021;103:106294. doi: 10.1016/j.cct.2021.106294 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Bradley KA, DeBenedetti AF, Volk RJ, Williams EC, Frank D, Kivlahan DR. AUDIT-C as a brief screen for alcohol misuse in primary care. Alcohol Clin Exp Res. 2007;31(7):1208–1217. doi: 10.1111/j.1530-0277.2007.00403.x [DOI] [PubMed] [Google Scholar]
- 37.Bradley KA, Bush KR, Epler AJ, et al. Two brief alcohol-screening tests From the Alcohol Use Disorders Identification Test (AUDIT): validation in a female Veterans Affairs patient population. Arch Intern Med. 2003;163(7):821–829. doi: 10.1001/archinte.163.7.821 [DOI] [PubMed] [Google Scholar]
- 38.Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch Intern Med. 1998;158(16):1789–1795. doi: 10.1001/archinte.158.16.1789 [DOI] [PubMed] [Google Scholar]
- 39.Reinert DF, Allen JP. The alcohol use disorders identification test: an update of research findings. Alcohol Clin Exp Res. 2007;31(2):185–199. doi: 10.1111/j.1530-0277.2006.00295.x [DOI] [PubMed] [Google Scholar]
- 40.Assistant Secretary for Planning and Evaluation. 2020 Poverty Guidelines. U.S. Department of Health and Human Services; https://aspe.hhs.gov/topics/poverty-economic-mobility/poverty-guidelines/prior-hhs-poverty-guidelines-federal-register-references/2020-poverty-guidelines [Google Scholar]
- 41.Cella D, Riley W, Stone A, et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. Journal of Clinical Epidemiology. 2010;63(11):1179–1194. doi: 10.1016/j.jclinepi.2010.04.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Zou G. A Modified Poisson Regression Approach to Prospective Studies with Binary Data. American Journal of Epidemiology. 2004;159(7):702–706. doi: 10.1093/aje/kwh090 [DOI] [PubMed] [Google Scholar]
- 43.Center for Behavioral Health Statistics and Quality. 2019 National Survey on Drug Use and Health: Detailed Tables. Substance Abuse and Mental Health Services Administration; 2020. https://www.samhsa.gov/data/report/2019-nsduh-detailed-tables [Google Scholar]
- 44.Center for Behavioral Health Statistics and Quality. 2020 National Survey on Drug Use and Health: Detailed Tables. Substance Abuse and Mental Health Services Administration; 2021. [Google Scholar]
- 45.Fishleder S, Schonfeld L, Corvin J, Tyler S, VandeWeerd C. Drinking behavior among older adults in a planned retirement community: results from The Villages survey: Depression and alcohol use in a retirement community. Int J Geriatr Psychiatry. 2016;31(5):536–543. doi: 10.1002/gps.4359 [DOI] [PubMed] [Google Scholar]
- 46.Towers A, Stephens C, Dulin P, Kostick M, Noone J, Alpass F. Estimating older hazardous and binge drinking prevalence using AUDIT-C and AUDIT-3 thresholds specific to older adults. Drug and Alcohol Dependence. 2011;117(2–3):211–218. doi: 10.1016/j.drugalcdep.2011.02.008 [DOI] [PubMed] [Google Scholar]
- 47.Chavez LJ, Liu CF, Tefft N, et al. Unhealthy alcohol use in older adults: Association with readmissions and emergency department use in the 30 days after hospital discharge. Drug and Alcohol Dependence. 2016;158:94–101. doi: 10.1016/j.drugalcdep.2015.11.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Gilson KM, Bryant C, Judd F. Exploring Risky Drinking and Knowledge of Safe Drinking Guidelines in Older Adults. Substance Use & Misuse. 2014;49(11):1473–1479. doi: 10.3109/10826084.2014.912233 [DOI] [PubMed] [Google Scholar]
- 49.Sherman AC, Williams ML, Amick BC, Hudson TJ, Messias EL. Mental health outcomes associated with the COVID-19 pandemic: Prevalence and risk factors in a southern US state. Psychiatry Research. 2020;293:113476. doi: 10.1016/j.psychres.2020.113476 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Killgore WDS, Cloonan SA, Taylor EC, Lucas DA, Dailey NS. Alcohol dependence during COVID-19 lockdowns. Psychiatry Research. 2021;296:113676. doi: 10.1016/j.psychres.2020.113676 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Delker E, Brown Q, Hasin DS. Alcohol consumption in demographic subpopulations: an epidemiologic overview. Alcohol research: current reviews. 2016;38(1):7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Grucza RA, Sher KJ, Kerr WC, et al. Trends in Adult Alcohol Use and Binge Drinking in the Early 21st-Century United States: A Meta-Analysis of 6 National Survey Series. Alcoholism: Clinical and Experimental Research. 2018;42(10):1939–1950. doi: 10.1111/acer.13859 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Centers for Disease Control and Prevention. CDC Health Disparities and Inequalities Report - United States, 2011.; 2011.
- 54.Jones-Webb R, Karriker-Jaffe KJ, Zemore SE, Mulia N. Effects of Economic Disruptions on Alcohol Use and Problems: Why Do African Americans Fare Worse? J Stud Alcohol Drugs. 2016;77(2):261–271. doi: 10.15288/jsad.2016.77.261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Mulia N, Schmidt L, Bond J, Jacobs L, Korcha R. Stress, social support and problem drinking among women in poverty. Addiction. 2008;103(8):1283–1293. doi: 10.1111/j.1360-0443.2008.02234.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Mulia N, Ye Y, Karriker-Jaffe KJ, Zemore SE, Jones-Webb R. Protective Factors as an Explanation for the “Paradox” of Black–White Differences in Heavy Drinking. Substance Use & Misuse. 2018;53(12):2003–2016. doi: 10.1080/10826084.2018.1451892 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Lui CK, Kerr WC, Li L, et al. Lifecourse Drinking Patterns, Hypertension, and Heart Problems Among U.S. Adults. American Journal of Preventive Medicine. 2020;58(3):386–395. doi: 10.1016/j.amepre.2019.10.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Dawson DA, Goldstein RB, Grant BF. Prospective correlates of drinking cessation: variation across the life-course: Prospective correlates of drinking cessation. Addiction. 2013;108(4):712–722. doi: 10.1111/add.12079 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Cooper ML, Kuntsche E, Levitt A, Barber LL, Wolf S. Motivational models of substance use: A review of theory and research on motives for using alcohol, marijuana, and tobacco. Published online 2016.
- 60.Puddey IB, Mori TA, Barden AE, Beilin LJ. Alcohol and Hypertension—New Insights and Lingering Controversies. Current Hypertension Reports. 2019;21(10). doi: 10.1007/s11906-019-0984-1 [DOI] [PubMed] [Google Scholar]
- 61.Rittmueller SE, Frey MS, Williams EC, Sun H, Bryson CL, Bradley KA. Association Between Alcohol Use and Cardiovascular Self-Care Behaviors Among Male Hypertensive Veterans Affairs Outpatients: A Cross-Sectional Study. Substance Abuse. 2015;36(1):6–12. doi: 10.1080/08897077.2014.932318 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Thomas RM, Francis Gerstel PA, Williams EC, et al. Association between alcohol screening scores and diabetic self-care behaviors. Fam Med. 2012;44(8):555–563. [PubMed] [Google Scholar]
- 63.Chew LD, Nelson KM, Young BA, Bradley KA. Association between alcohol consumption and diabetes preventive practices. Fam Med. 2005;37(8):589–594. [PubMed] [Google Scholar]
- 64.Winhusen T, Theobald J, Kaelber DC, Lewis D. Increased Morbidity and Mortality in Hypertensive Patients With Substance Use Disorders: Electronic Health Record Findings. Journal of Studies on Alcohol and Drugs. 2020;81(4):471–478. doi: 10.15288/jsad.2020.81.471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Winhusen T, Theobald J, Kaelber DC, Lewis D. Medical complications associated with substance use disorders in patients with type 2 diabetes and hypertension: electronic health record findings. Addiction. 2019;114(8):1462–1470. doi: 10.1111/add.14607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Sporinova B, Manns B, Tonelli M, et al. Association of Mental Health Disorders With Health Care Utilization and Costs Among Adults With Chronic Disease. JAMA Network Open. 2019;2(8):e199910. doi: 10.1001/jamanetworkopen.2019.9910 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Mauro PM, Askari MS, Han BH. Gender differences in any alcohol screening and discussions with providers among older adults in the United States, 2015 to 2019. Alcohol Clin Exp Res. 2021;45(9):1812–1820. doi: 10.1111/acer.14668 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Sorocco KH, Ferrell SW. Alcohol Use Among Older Adults. The Journal of General Psychology. 2006;133(4):453–467. doi: 10.3200/GENP.133.4.453-467 [DOI] [PubMed] [Google Scholar]
- 69.DiBartolo MC, Jarosinski JM. Alcohol Use Disorder in Older Adults: Challenges in Assessment and Treatment. Issues in Mental Health Nursing. 2017;38(1):25–32. doi: 10.1080/01612840.2016.1257076 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.