

Abstract
Background:
Community health workers (CHWs) face high levels of stress (both professional and personal) and risk of burnout, highlighting the need for efforts to promote their mental health and well-being. This study seeks to develop a digital stress reduction program for CHWs in rural India.
Methods:
A stepwise design process was employed to adapt and digitize the evidence-based World Health Organization’s Self-Help Plus (SH+) intervention for addressing psychological distress among CHWs in Madhya Pradesh, India. This involved participatory design workshops with CHWs to ensure that the digital stress reduction intervention would be relevant for their needs and the local culture and context. Small groups of CHWs reviewed the adapted program content, allowing the research team to make refinements such as simplifying language, tailoring content to the local setting, and ensuring that program materials are both interesting and relevant. Simultaneously, the research team digitized the content, leveraging a combination of video and graphical content, and uploaded it to the Sangath Learning Management System, a digital platform accessible on a smartphone app.
Results:
In total, 18 CHWs contributed to the adaptation of the SH+ content and digital intervention development. Participants commented on finding some terms difficult to follow and recommended simplifying the language and providing detailed explanations. Participants offered positive feedback on the adapted content, expressing that they found the examples covered in the material both relatable and relevant to their own personal experiences at home and in the workplace. By combining participants’ insights and comments with feedback from content experts, it was possible to finalize a digital Hindi version of the SH+ intervention for CHWs in rural India.
Conclusions:
This study is timely given the continued detrimental impacts of the COVID-19 pandemic, and offers a promising and potentially scalable digital program to alleviate psychological distress among frontline health workers.
Keywords: Community health worker, ASHA, Stress, Burnout, Digital technology, Mental health, Self-help plus
1. Introduction
Community health workers (CHWs) represent the backbone of most health systems, responsible for delivering essential primary care services, particularly in remote and underserved settings in low- and middle-income countries (LMICs) (Vasan et al., 2017; Scott et al., 2018; Tulenko et al., 2013). CHWs are often members of the communities in which they serve (Pallas et al., 2013), whereby they can establish trust and are ideally positioned to deliver a range of services from preventive care and educating community members, to supporting ongoing management of chronic conditions, and acting as the essential connection between community settings and primary healthcare facilities (Black et al., 2017; Lewin et al., 2010; Perry et al., 2014). Despite serving a key role in most health systems, CHWs and other frontline providers take on significant workload and are at high risk of burnout (Dugani et al., 2018; Dubale et al., 2019; Wright et al., 2022).
In the context of India, ASHAs (i.e., Accredited Social Health Activists) represent the health worker cadre closest to the community that takes on an extensive range of programmatic responsibilities. ASHAs are women and community residents, with a minimum of 8 years of formal education, who act as volunteers while receiving incentive-based payments, and typically serve a population of about 1000 (Scott et al., 2019). The ASHA program was launched by the National Rural Health Mission (now National Health Mission), Government of India in 2005, primarily to improve maternal and child health outcomes, and has since broadened its ambit to strengthening the accessibility, availability and acceptability of a broader range of public health services in communities with a focus on enhancing service reach for poor and vulnerable sections (Agarwal et al., 2019; Scott et al., 2019). Over time, the roles and responsibilities of ASHAs have expanded to include conducting health surveys, improving reproductive and child health, and delivering preventive, promotive and curative services related to non-communicable disease programs, promoting vaccination, and supporting institutional births. Since its inception, the ASHA program has been instrumental in improving neonatal, child and maternal mortality, improving vaccination coverage and other key health outcomes across India (Scott et al., 2019). However, like other lower resource contexts, mounting evidence highlights the detrimental impacts of burnout and work-related stress among ASHAs in India, including poor motivation and reduced well-being (Pulagam and Satyanarayana, 2021; Manjunath et al., 2022), serious concerns that have been further exacerbated due to the COVID-19 pandemic (Niyati and Nelson Mandela, 2020; Mishra et al., 2022; Deng and Naslund, 2020). Specifically, recent studies from India have found that upwards of half of frontline health workers, including ASHAs, have experienced high risk of psychological distress during the pandemic, largely driven by longer work hours, emotional exhaustion, detrimental impact on sleep, and fears of contracting the virus (Yella and Dmello 2022; Menon et al., 2022).
ASHAs are particularly susceptible to facing work related stress and being overburdened, which are driven by unequal work distribution (Manjunath et al., 2022; Meena et al., 2020) as well as gender inequities within the health system (Ved et al., 2019). ASHAs experience both workplace and their own personal household stressors, which often makes it difficult for them to meet the multiple demands and expectations placed upon them (Aryal et al., 2019; Deshpande et al., 2019). At the health system level, prior studies have reported that key factors contributing to stress and burnout among ASHAs include low compensation and relying on incentives compared to other salaried health system personnel. Additional factors that contribute to burnout include delays in receiving outcome-based incentive payments, poor institutional support, perception of low incentives as compared to the nature and amount of work, unfulfilled training needs, and a dearth of support and adequate respect from other cadres of health workers (Scott and Shanker, 2010). ASHAs have also highlighted that due to being at the bottom of the health system hierarchy, they feel that they hardly have a ‘voice’ to express their concerns (Mishra, 2014). At the individual level, additional stressors can include patriarchal values embedded within the socio-cultural milieu, familial expectations around gendered role playing of domestic responsibilities, low socioeconomic status and coming from impoverished settings, and limited educational qualification (Ved et al., 2019; Manjunath et al., 2022). Therefore, ASHAs face a two-fold challenge of meeting ever-increasing expectations for addressing health issues of the communities they serve while simultaneously managing stressors experienced in their workplace and personal life.
The efforts needed to address these concerns will require major structural changes at the health system and societal levels. However, there may also be more immediate solutions aimed at promoting the mental health and well-being of frontline CHWs such as ASHAs. There has been a dearth of research addressing stress among CHWs in LMICs such as India (Dugani et al., 2018), while prior studies have predominantly focused on ‘extrinsic’ factors like monetary incentives, improved supervision strategies, flexible tasks, public recognition, and rewards, yet with inadequate consideration of the ‘intrinsic’ factors such as mental health and wellbeing of ASHAs themselves. Finding ways to support ASHAs in managing their stress and burnout could meaningfully support their wellbeing, and may also help them in their work roles and result in benefits for the patients and communities they serve (Willis--Shattuck et al., 2008; Mondal and Murhekar, 2018; Bajpai and Dholakia, 2011; Bhattacharyya et al., 2001; Singh et al., 2015). Therefore, there is a gap in the research on developing and testing an evidence-based, contextually adapted intervention for frontline workers like ASHAs, aimed specifically at strengthening their individual-level management of work-related stress and burnout.
Considering the complex factors contributing to compromised well-being of ASHAs, and drawing from the World Health Organization’s (WHO) five-pillared recommendations of protection of frontline health workers (World Health Organization, 2022), it becomes imperative to devise interventions to support ASHAs and facilitate change towards adopting strategies that can help them cope effectively (Otu et al., 2020; Bo et al., 2021). Recognizing that this would not address broader structural challenges, a brief scalable stress reduction program could offer immediate relief to a frontline workforce experiencing elevated burden and risk of burnout. The WHO has developed a culturally adaptable, low-intensity psychological intervention, called Self-Help Plus (SH+), for stress management (Epping-Jordan et al., 2016). Importantly, this brief intervention is transdiagnostic, and designed with the intention of being easily adaptable to different cultures and contexts while being beneficial and safe for individuals with and without mental disorders (Epping-Jordan et al., 2016). SH+ has demonstrated effectiveness in reducing stress among women in humanitarian settings in Uganda (Tol et al., 2018; Tol et al., 2018). In a cluster-randomized controlled trial (Brown et al., 2018) in 14 villages in Uganda enrolling 694 participants, SH+ contributed to significant reduction in psychological distress compared to enhanced usual care post-intervention (ES = −0.72) and at 3-months follow up (ES = −0.26) (Tol et al., 2020). Furthermore, in a randomized controlled trial conducted across 5 countries in Europe, when compared to treatment as usual, the SH+ intervention demonstrated effectiveness in preventing onset of mental disorders among refugees and asylum seekers post-intervention, though not at 6-months follow up (Purgato et al., 2021). Most recently, the SH+ intervention was found be effective in preventing mental disorders in a randomized controlled trial enrolling 642 Syrian refugees experiencing psychological distress in Turkey (Acarturk et al., 2022). Participants who received the SH+ intervention were significantly less likely to have any mental disorders at 6-month follow up compared to the usual care control group (22% vs. 41%, p < 0.001) (Acarturk et al., 2022).
SH+ has theoretical and conceptual roots grounded in Acceptance and Commitment Therapy (Levin et al., 2015; A-tjak et al., 2015), which can reduce symptoms of depression and anxiety (A-tjak et al., 2015), and combines elements of cognitive behavioral therapy including psycho-education, mindfulness exercises, and promoting psychological flexibility where individuals learn new ways to open up to and cope with difficult thoughts and feelings consistent with their own values, rather than avoiding these thoughts (Hayes et al., 2012). One key feature of SH+ is the broad focus on reducing psychological distress associated with adversity and difficult life experiences (Epping-Jordan et al., 2016), which increases scalability by not requiring use of diagnostic procedures or targeting specific syndromes. Specifically, the SH+ intervention endorses enhancement of psychological elasticity and has the following key components: grounding, unhooking from difficult thoughts and feelings, acting on values, being kind, and making room for difficult emotions. The original SH+ intervention is composed of multimedia and a manual, to be delivered in a group setting consisting of five weekly sessions. Each session focuses on a review of concepts and practice of skills from previous sessions, the introduction of new skills, brief group discussions and self-reflection exercises, and encouragement of daily practice of these key skills (Epping-Jordan et al., 2016). To our knowledge the SH+ intervention has not been previously adapted for use among CHWs in India, yet there is ongoing research using this program for addressing psychological stress among health workers in China (Luo et al., 2022). Furthermore, the simplicity of the program content and emphasis on skill building make this a potentially highly relevant program for empowering ASHAs to better cope with and manage a stressful work environment. Adapting the SH+ intervention to diverse settings also aligns with WHO efforts to develop a range of scalable and effective psychological interventions for release as public goods (Carswell et al., 2018; Harper et al., 2020; Purgato et al., 2019).
In our prior studies, we found that digital interventions are both feasible and acceptable for use with ASHAs in Madhya Pradesh (Muke et al. 2019, 2020), a finding that has similarly been demonstrated in other settings in India (Kapanee et al., 2022), as well as in settings with CHWs outside of India (Rahman et al., 2019). We have found that ASHAs have expressed keen interests in accessing content from mobile devices as it avoids the need to travel long distances and spend time away from their families to attend in-person programs (Muke et al., 2019). Furthermore, we have found in our ongoing work that nearly all ASHAs own cellphones, and over half own smartphones (Naslund et al., 2021), further highlighting the potential for leveraging these widely available devices to offer support and build resilience of this frontline workforce. Importantly, we have also observed high engagement in the use of digital programs accessible from a smartphone app (Muke et al., 2020), emphasizing that it may be an ideal approach for delivering a stress reduction program to this target group of health workers. Use of a mobile app can also avoid drawing attention beyond typical phone use (e. g., easily fits into daily activities), and could minimize concerns or feeling ashamed to seek help by delivering stress reduction content in a non-stigmatizing way (Naslund et al., 2019; Naslund and Deng, 2021). As smartphone ownership continues to increase, health systems in some states, such as Gujarat and Madhya Pradesh, are providing smartphones to frontline health workers including ASHAs to support them in their work (Modi et al., 2019; Saha et al., 2020), further highlighting the potential for a digital self-help intervention to offer widespread scalability. In addition to adapting the SH+ intervention for ASHAs, we also aimed to digitize the content and make it accessible in an individualized self-directed format, as opposed to the group-based format of the prior evaluation studies in Uganda, Turkey and Europe (Tol et al., 2020; Acarturk et al., 2022; Purgato et al., 2021). We intentionally selected the SH+ intervention for adaptation because it consists of many individual activities as well as an illustrated guide that could be adapted in such a way that it could be accessible from a smartphone app in a self-directed format, thereby avoiding the need for travel to a central location, and accommodating the busy schedule of ASHAs.
1.1. Study objectives
This paper describes the approach of adapting and digitizing the language, content and format of the evidence-based Self-Help+ (SH+) intervention for use with CHWs in rural Madhya Pradesh, India. The goal of our adaptation of SH+ was to ensure a culturally and contextually appropriate intervention accessible from a smartphone app for reducing psychological distress, and promoting the mental health and wellbeing of frontline CHWs in rural India. Importantly, we engaged CHWs in adapting and digitizing the evidence-based intervention content for use in India, drawing from the principles of human-centered design whereby the needs of the target user-group are considered central to the design process. Human-centered design can improve user satisfaction and relatability with the intervention, promote ownership of the program content, and enhance effectiveness and opportunities for uptake and sustainability (Wheelock et al., 2020; Triplett et al., 2021). This approach also builds on our prior successful efforts working with and engaging ASHAs in the development of digital training programs (Black et al., 2023). The present study represents the formative phase of the SAMBHAV (Stress Alleviation Methods for community-Based Health ActiVists) project, whose overarching aim is to develop and evaluate the feasibility, acceptability, and preliminary effectiveness of a digital self-directed version of the WHO’s SH+ intervention tailored to the needs, context, and local culture, and to explore the potential for reducing stress and promoting mental wellbeing among ASHAs in rural India.
2. Methods
2.1. Setting
This study was conducted in Sehore district, a rural district in the state of Madhya Pradesh, which is geographically one of the largest states of India with a population over 75 million, of whom nearly 73% reside in rural areas (Suryanarayana et al., 2016; Menon et al., 2008; Kokane et al., 2019; Shidhaye et al., 2017). This state lags behind many other Indian states and ranks among the lowest on the Human Development Index (Suryanarayana et al., 2011). This project expands on our research infrastructure in the region, and involves recruiting CHWs called ASHAs (Accredited Social Health Activists—deployed in India’s National Health Mission), and ASHA Facilitators, who provide monitoring and supervision for ASHAs (Scott et al., 2019). ASHAs were recruited from primary healthcare facilities in Sehore district to contribute to the development and adaptation of the digital SH+ intervention.
2.2. Research design
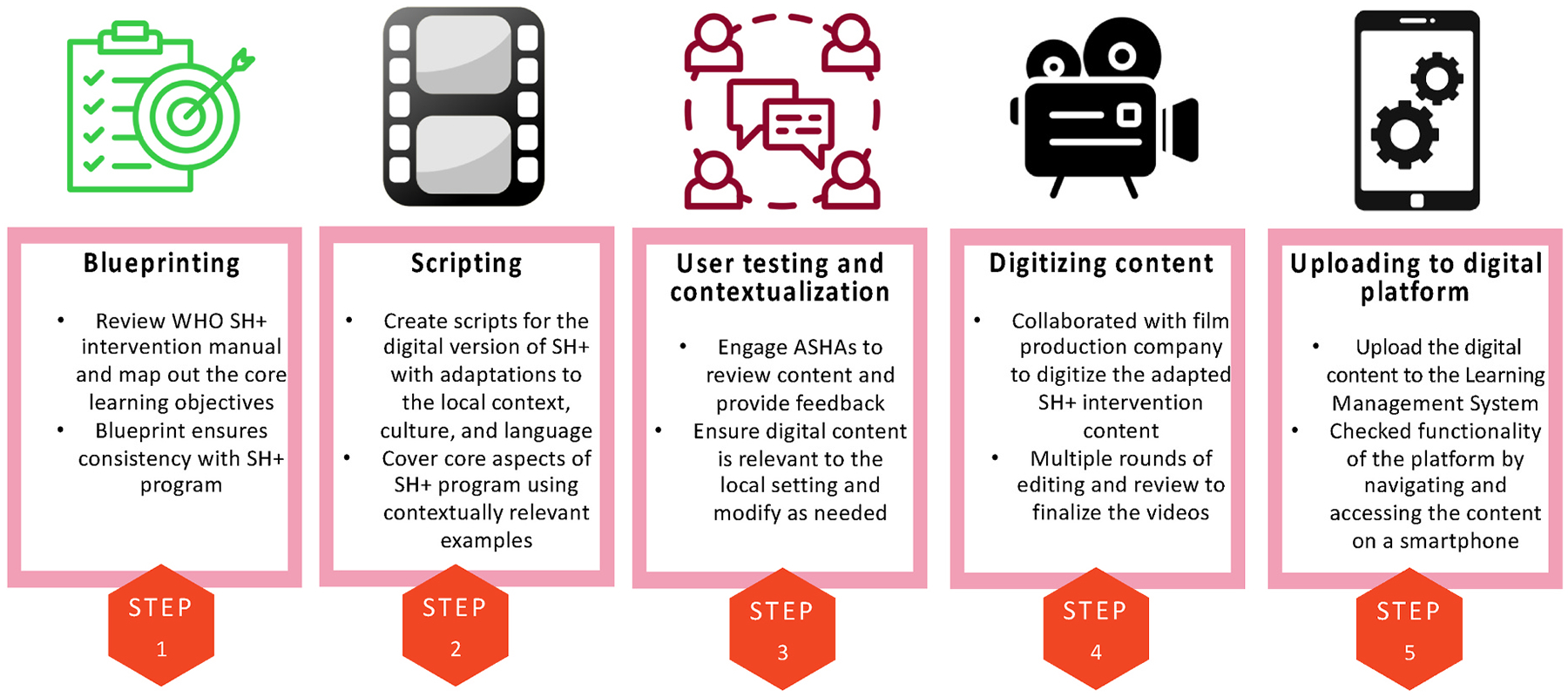
We employed a stepwise design approach to guide the adaptation of the SH+ content and digital intervention development, informed by our prior work in developing interventions for the same target group of ASHAs in rural Madhya Pradesh (Khan et al., 2020) and grounded in principles of human-centered design (Black et al., 2023). Mainly, through engaging the target group of ASHAs throughout the design process to ensure that the adapted content is centered around their needs, which can enhance acceptability, user satisfaction, and improve chances for uptake and adoption (Baker et al., 2020). Additionally, the core content and the concept of the WHO SH+ program was followed throughout the adaptation process (World Health Organization, 2020). The WHO SH+ program covers the self-help stress reduction techniques and teaches the ways to deal with stress through simple exercises and methods. We ensured that the adapted content remained consistent with the original SH+ content by reviewing adapted materials with content experts and ensuring multiple levels of review within our own team. Given our earlier experience of designing and developing digital training interventions, drawing from prior literature in the development of digital interventions (Yardley et al., 2015), we followed a step-wise process to develop the digital self-help stress reduction program for ASHAs (Khan et al., 2020). The steps are illustrated in Fig. 1, and described in the sections that follow.
Fig. 1.
Overview of the stepwise approach to development of the digital program for stress reduction for community health workers in rural India.
Step 1 Development of the digital intervention blueprint
First, we developed a blueprint for the digital stress reduction self-help program (Coderre et al., 2009), which involved carefully reviewing the original WHO SH+ intervention manual and mapping out the core learning objectives (World Health Organization, 2020). In the blueprint for the SH+ program, the different topics from the intervention manual, such as specific techniques and exercises required to deal with the stress and burnout, were organized into six modules, with each module further broken down into short segments covering key lessons. The blueprint serves as a roadmap to guide the development of the digital SH+ course content and acted as the architecture for the overall layout and of the digital self-care intervention. To ensure consistency with the original WHO SH+ intervention manual, the blueprint was created by one member of our research team, and then reviewed by three additional team members to double check that the modules outlined in the blueprint aligned with the original manual. Lastly, the blueprint was reviewed by an external researcher with expertise in the WHO program content. The final blueprint for the adapted version of the digital SH+ intervention is listed in Table 1.
Table 1.
Blueprint for the digital Self-Help+ intervention adapted for ASHAs in rural India.
| Module No. | Module | Learning objectives | Learning outcomes | No of Chapters/Videos per Module (Total videos =) |
|---|---|---|---|---|
| 1 | Grounding |
|
After this module the learner acquires the knowledge:
|
Video-1: Stress, its causes and effects Video-2: What does hooked mean? Video-3: What is Focus, Engage and Pay attention and how does it help? Video-4: Awareness of drinking exercise Video-5: Grounding exercise-1 & 2 (or separate video on exercise-2) |
| 2 | Unhooking |
|
After completing this module, the participant(s) will be:
|
Video-1: Learn unhooking Video-2: Notice and name exercise Video-3: Toolkit to practice grounding and unhooking |
| 3 | Acting On Your Values |
|
After this module the participant(s) will be:
|
Video-1: Values Video-2: Action plan Video-3: Values and action plan exercise |
| 4 | Being Kind |
|
After completing this module, the participant(s) will be able to:
|
Video-1: What is being kind means? Video-2: Unhooking from unkind thoughts exercise |
| 5 | Making Room |
|
After completing this module, the participant(s) will be able to:
|
Video-1: What is making room Video-2: Making room exercise Video-3: Being kind to yourself exercise |
| 6 | Tool Exercises/new exercises with examples |
|
After completing this module, the participant(s) will be able to summarize and practice key concepts and exercises related to:
|
Video-1: Grounding, unhooking Video-2: Acting on your values, being kind Video-3: Making room |
Step 2 Development of SH+ program scripts and content
The development of the self-help content started with the adaptation of the written and graphical content of the WHO SH+ manual (World Health Organization, 2020). We considered our prior formative research activities and focus group discussions with ASHAs to support the development of script ideas that reflect personal stories that are relatable for ASHAs (Muke et al., 2019). The digital content described in the blueprint comprised images, graphics, and short videos illustrating the different skills and techniques covered in the program manual. Development of the video content for the program involved; first, writing scripts in English, following an approach that has previously been applied by our team (Khan et al., 2020). The scripts included original language of the WHO SH+ manual as well as additional supplemental content created to offer illustrative stories, scenarios and real-life examples that align with the local context and closely relate to the experiences encountered by ASHAs, and that could be interactive and engaging for the self-directed delivery format of the adapted digital version of the SH+ program. The scripting for the videos also involved describing use of local settings for filming, and included dialogues, montages and directions for shooting specifications. Two members of our research team (RS and SC) developed the scripts, and the drafts were further discussed within the team to reach consensus before circulating for review from additional research team members (AS, JRH, and JAN) and an external content expert (EK). We made further revisions to finalize the scripts by incorporating the feedback and comments from reviewers.
Since the target population of ASHAs in Madhya Pradesh are Hindi speaking, it was also necessary to translate the scripts. To ensure contextual fit, research team members from the same target setting completed the translation of the scripts, ensuring inclusion of appropriate terms and language reflective of the local culture and language. Other team members fluent in Hindi (RS, SC, and AS) then reviewed the translated scripts to check the alignment with the English content and to ensure simplification or removal of jargon or complex terms, given that many of our target group of health workers have 8th standard education and above, and may have only basic literacy levels. Our final step involved having a clinician with Master’s level training and extensive prior experience working with and training ASHAs in delivery of brief psychological interventions in the target setting in Madhya Pradesh review the Hindi versions of the scripts (AK). We completed a subsequent round of revisions of the Hindi scripts, ensuring that feedback from the multiple rounds of review was fully captured in the final scripts. The process of drafting the English scripts and then translation and finalizing the Hindi scripts was completed over approximately five months.
In parallel to the development of the scripts, our team drafted an adapted version of the WHO SH+ manual (World Health Organization, 2020), following a similar layout and format, but with culturally and contextually relevant images and graphics. Our team worked closely with a graphic designer to create specific images and icons to illustrate the different stress management techniques and strategies described in the SH+ manual. A member of our research team (RS) also carefully reviewed existing training and intervention materials designed for ASHAs and circulated by the Ministry of Health and Family Welfare in India to offer examples of context designed for the target group of health workers i.e., use of relatable and relevant language, scenarios, and examples in the content. Working closely with the graphic designer, our team provided feedback and comments on the different images and to ensure alignment with the original WHO SH+ manual content. After finalizing the images, the content was compiled into a manual format with additional text added (taken from the scripts). The SAMBHAV manual was developed in both English (to allow a version for translation into other languages in India) and Hindi.
Step 3 Content testing and contextualization workshop
This step involved engaging ASHAs to review the content and provide feedback on the cultural acceptance, relevant language modifications, stories and examples covered in the program. We invited 20 ASHAs, employing a convenience sampling approach by drawing from the larger pool of ASHAs enrolled in another ongoing research study (Naslund et al., 2021), to participate in a workshop with the objective to check the language of the content and the appropriateness of the stories included in the scripts, by collecting their perspectives and recommendations for improving the adapted SH+ program content. The participating ASHAs were aged ≥18 years of age, had minimum education level of 8th standard to ensure sufficient literacy level to operate the smartphone and to follow any of the written intervention content, and a willingness to stay in the study area over the duration of the study. Two members of our research team (RS and SC) facilitated the workshop over a 3-day period. On the first day, we tested module-1; followed by module-2 and module-3 in the second day; and module-4 and module-5 were saved for the last day. The ASHAs were informed about the program and invited for the content testing and contextualization workshop after securing necessary government approvals. Of the 20 ASHAs invited to join the design workshops, a total of 18 ASHAs participated, including one ASHA Facilitator. These ASHAs were all women, and ranged in age from 21 to 42 years, had between 8th standard to graduation level of education, and an average of seven years of work experience. Participating ASHAs were also provided with smartphones with the content pre-loaded to the mobile app to minimize potential technical challenges and to ensure access to the content for the purpose of feasibility testing.
The workshops were broken down into two segments. We first introduced the purpose to learn about any difficulties faced by the ASHAs in understanding the language used in the modules and any difficulty in understanding the content, terms, and relating the stories and roleplays to their real-life situations. Printed copies of the materials were given to the ASHAs to read, and they were asked to underline or encircle any sentences or words which they found difficult to understand or to mark any comments related to the stories. In the second session, after ASHAs completed the reading and commenting on the hard copies of the modules, members of our research team sat together with the participating ASHAs in two small groups and discussed the modules with them, and asked them about use of appropriate words, or suggestions for alternative words and sentences that could be used instead of the ones which they found difficult to read and understand. This was followed by a semi-structured focus group discussion to collect insights from this same group of participants from the workshops to inform further modifications and improvements to the content stories and roleplays in the modules. The focus group discussions were facilitated by two members of our team, and guided by targeted questions focused on different aspects of the digital program content, such as: “Are these roleplays and stories relatable to your day-to-day and work-life situations?” or “Are you understanding the content? Could you describe any difficulties you experienced when reading the content?” or “Do you need more explanation or details regarding the content?” and “Any suggestion to use new words for the difficult words?” Two members of our research team documented participants’ feedback and suggestions from the qualitative focus group discussions. Our analysis was guided by the need to inform improvements to the program content; therefore, we employed a rapid thematic analysis approach, consistent with prior studies focused on gathering health worker feedback for informing digital intervention development in low-resource contexts (Tyagi et al., 2023; Kumar et al., 2022), where the two researchers combined their observations, and organized participant feedback according to different aspects of the program that could be improved (i.e., language, stories, difficult wordings, etc.). Next, we convened a discussion with our larger investigative team to review the qualitative insights from participants, to reach consensus on what aspects of the content require improvements, and to plan out next steps for making these modifications accordingly.
Step 4 Digitization of the SH+ content
Our team collaborated with film production teams and actors to digitize the adapted SH+ intervention content. The videos were filmed in several locations, including community health centers, typical locations in villages, and the research office in Bhopal to show the culturally appropriate context in the digital content. The videos consisted of a combination of lectures delivered by a counsellor or fellow CHW, and the use of actors who could emote and deliver the lines, as well as role-play videos, where actors were selected to illustrate mock scenarios involving ASHAs learning and applying the skills and techniques covered in the SH+ intervention during routine everyday scenarios.
We completed the video shooting over 10 days. The research team members (RS and AS) were present during all the days of filming to guide and supervise video production, and to ensure that the filming adhered to the scripts covering the adapted WHO SH+ intervention content. The film production team was selected for this project as they had prior experience working with our team in the digitization of other program content, can ensure the production of high-quality video content, and because the ability for our team to work with them following the video shoot, allowing for multiple rounds of editing required to finalize the videos for uploading to the digital platform. A member of our team was also present throughout the editing process to review each iteration of edits to ensure the correct use of subtitles, icons and images, montages, placement of bullet points and text, sound quality for spoken content and narration, and use of music and other sound effects. Our team simultaneously worked to develop a series of PowerPoint videos consisting of graphics and with voice narration that would be used to supplement the video-based content in the program.
Step 5 Setting up the digital platform
Our team previously developed a Learning Management System (LMS) using the Moodle platform for hosting digital content. While the LMS software is typically designed for delivery of educational content, we opted for this same software for delivery of the SH+ intervention content given that we have previously demonstrated that this platform is both feasible and acceptable for use in the target population of ASHAs for accessing training content focused on depression care (Muke et al. 2019, 2020). Therefore, including targeted self-help content on this platform seemed likely an ideal approach for ensuring familiarity, uptake, and allowing self-directed interaction and use among our target group of ASHAs. Furthermore, given our experience working with this digital platform, uploading the digital content could ensure the timely development of a prototype ready for pilot testing. The structure of the SH+ course was created on the LMS and the various types of content, including videos, PowerPoint videos, graphics, and additional written content, was uploaded. Once the content was uploaded on the LMS, our team checked the functionality and the feasibility of the platform by navigating the platform and accessing the self-help digital content on their smartphones. We also ensured that the content was loaded directly onto smartphones so that it could be accessed in offline functionality to overcome potential technical challenges and to enable access for ASHAs in regions with low bandwidth. Two team members checked the navigation and feasibility, made any final corrections by primarily addressing any technical difficulties or minor changes for clarity in the content. Following this final round of internal revisions, the adapted digital SH+ program, called SAMBHAV (Stress Alleviation Methods for community-Based Health ActiVists), was ready for delivery to ASHAs and pilot testing to assess feasibility, acceptability, and preliminary effectiveness in alleviating stress in this target population of frontline health workers.
2.3. Summarizing adaptations to the SH+ intervention
Our development of the SAMBHAV intervention involved multiple types of adaptations to the SH+ intervention, including adapting the content for use in rural India, tailoring the materials for the needs of ASHAs, and digitizing the content to enable self-directed access from a smartphone app. Therefore, we provide a summary of the different types of adaptations organized according to an existing established model for cultural adaptation of psychological interventions, referred to as the ecological validity model (Bernal et al., 1995). As summarized in Table 2, this model outlines eight important dimensions of interventions, spanning language, persons, metaphors, content, concepts, goals, methods, and context (Bernal et al., 2009), and has been applied widely in the adaptation of brief psychological interventions for diverse settings (Perera et al., 2020; Mabunda et al., 2022). Documenting the different adaptations and modifications to the SH+ program content can enable replication, inform further adaptations by uncovering which dimensions of the program were sufficiently adapted or not, and support subsequent outcome evaluation (Naslund and Spagnolo, 2023).
Table 2.
Summary of adaptations to the SH+ intervention.
| Intervention dimension | Description of adaptation principle | Summary of adaptations to the SH + intervention |
|---|---|---|
| Language | Translation of the program content to the local language; use of culturally appropriate terms |
|
| People | Role of ethnic/racial similarities and differences between persons depicted in the program content and target population |
|
| Metaphors | Use of symbols and concepts that are familiar with the target population |
|
| Content | Alignment between the program content and the cultural knowledge, values, and local practices of the target population |
|
| Concepts | Ensuring the program content aligns with concepts of stress that are familiar to the target population |
|
| Goals | Program goals align with social and cultural values of the target population |
|
| Methods | Program delivery in a format that is acceptable to the target population |
|
| Context | Consideration of barriers to accessing and benefitting from the program content for the target population |
|
2.4. Ethics
Ethics approval for this study was obtained from the Institutional Review Boards at Sangath, India (Number: AB_2021_73) and Harvard Medical School, USA (Number: IRB22–0974). All the study participants provided written informed consent to be included in the study. To ensure participants’ confidentiality, raw data were deidentified and maintained in password-protected computers.
3. Result
3.1. Key recommendations for informing digital intervention development
During the intervention development process, the 18 ASHAs joined the design workshop and focus group discussions at our site office in Sehore district. Importantly, they offered feedback and recommendations pertaining to the content at the early stages of the digitizing process. In general, the ASHAs liked the content, and they perceived it to be new to them initially, especially considering some of the concepts and words that were introduced pertaining to identifying and managing stressors. Then, after having a chance to read through the content and examples in greater details, as well as review stories and images in the scripts, it was observed that the ASHAs found the content to be understandable and easy to follow. They only provided feedback regarding some of the technical words that were used, such as “hooking”, “grounding”, or “bridge” in the context of stress reduction. Most of the participating ASHAs highlighted these terms as being difficult to understand and suggested using simpler words and offering additional details and explanation of technical words. Regarding the roleplays and stories created for the training content, the ASHAs reported that they liked the explanation of content throughout the roleplays and stories, and they expressed being able to relate to these to their own real-life situations as well as their experiences of workplace stress. Table 2 provides a summary of the specific adaptations to the SH+ intervention content according to the eight dimensions of the ecological validity model proposed by Bernal et al. (1995).
3.2. Digital SH+ program called SAMBHAV
After integration of the feedback and recommendations of the participating ASHAs, the result of this project was the development of SAMBHAV, a fully digital SH + intervention package accessible from the Sangath LMS on a smartphone app. The adaptation and development of the digital SH + intervention was completed over 12 months from August 2021 to September 2022. The final digital program consisted of 6 modules, as summarized in Table 3. These modules contained a total of 20 short videos with 3 video lectures, 8 role-play videos, 6 PowerPoint lectures with voiceover, and 3 summary videos providing a recap of the content displayed in a given module. The videos ranged in duration from about 1 min to 13 min, with the average duration being approximately 6 min. We specifically kept the videos in short segments based on user feedback because this made it easier to stay engaged with shorter videos when accessing the content from a smartphone app (while also making it easier to load the digital content when considering challenges with low-bandwidth). In addition to the video content, we included a total of 27 engagement quizzes and 30 knowledge assessment questions embedded throughout the modules. The total duration of the digital SH+ intervention was about 4–5 h of delf-directed content.
Table 3.
Summary of digital SH+ intervention content in final adapted program.
| Module | Type of Video | Duration of Video (In Minutes) |
|---|---|---|
| Module-1 | ||
| Video 1. Stress, its causes and effects | Lecture | 8.51 |
| Video 2. What does Hooked mean? | Lecture | 10.21 |
| Video 3. What is Focus, Engage and Pay attention and how does it help? | Lecture | 2.11 |
| Video 4. Awareness of drinking exercise | Role play 1 | 7.00 |
| Video 5. Grounding exercise 1 | Role play 2 | 10.12 |
| Video 6. Grounding exercise 2 | Role play 3 | 2.53 |
| Module-2 | ||
| Video 1. Learn Unhooking | Role play 4 | 3.00 |
| Video 2. Notice and Name Exercise | Role play 5 | 6.10 |
| Video 3. Toolkit to practice Grounding and Unhooking | PPT-video | 3.00 |
| Module-3 | ||
| Video 1. Values | PPT-video | 4.00 |
| Video 2. Action Plan | PPT-video | 5.15 |
| Video 3. Values and action Plan Exercise | Role play 6 | 5.52 |
| Module-4 | ||
| Video 1. What is being kind means? | PPT-video | 10.11 |
| Video 2. Unhooking from unkind thoughts Exercise | Role play 7 | 6.15 |
| Module-5 | ||
| Video 1. What is Making Room | PPT-video | 4.20 |
| Video 2. Making Room Exercise | Role play 8 | 11 |
| Video 3. Being Kind to Yourself Exercise | Role play 9 | 8.04 |
| Module -6 | ||
| Video 1. Summary of Module 1 | PPT-video | 9.00 |
| Video 2. Summary of Module 2 & 3 | PPT-video | 6.00 |
| Video 3. Summary of Module 4 & 5 | PPT-video | 5.35 |
As illustrated in Fig. 2, the central components of SAMBHAV, i.e., the adapted digital SH+ intervention, were the instructional videos. These short videos consisted of lectures covering the core content of SH+, as well as role play videos demonstrating the application of the various skills and techniques for managing stress in everyday scenarios tailored to what ASHAs may typically encounter. The lectures included a variety of digital elements to support learning, such as visual graphics, text in bullet points, figures, tables, narration, footage from local community settings and health facilities, and example interactions between patients and health care providers in the community or at the clinic. Role-play videos were used to demonstrate the use of specific self-help techniques, and interaction between ASHAs and counsellors during learning sessions. The lecture and role-play videos were supplemented with PowerPoint lectures with voiceover, and with use of graphics and images tailored to the local context (see sample graphics in Fig. 3). We also used a variety of engagement and assessment activities, such as multiple-choice questions, drag and drop response options, and true/false questions covering the content to accompany the instructional videos and to support participant engagement in the program. The final digital content was uploaded to the Sangath LMS and is accessible from a smartphone app.
Fig. 2.

Sample video content from the digital SH+ intervention adapted for ASHAs in rural India.
Fig. 3.
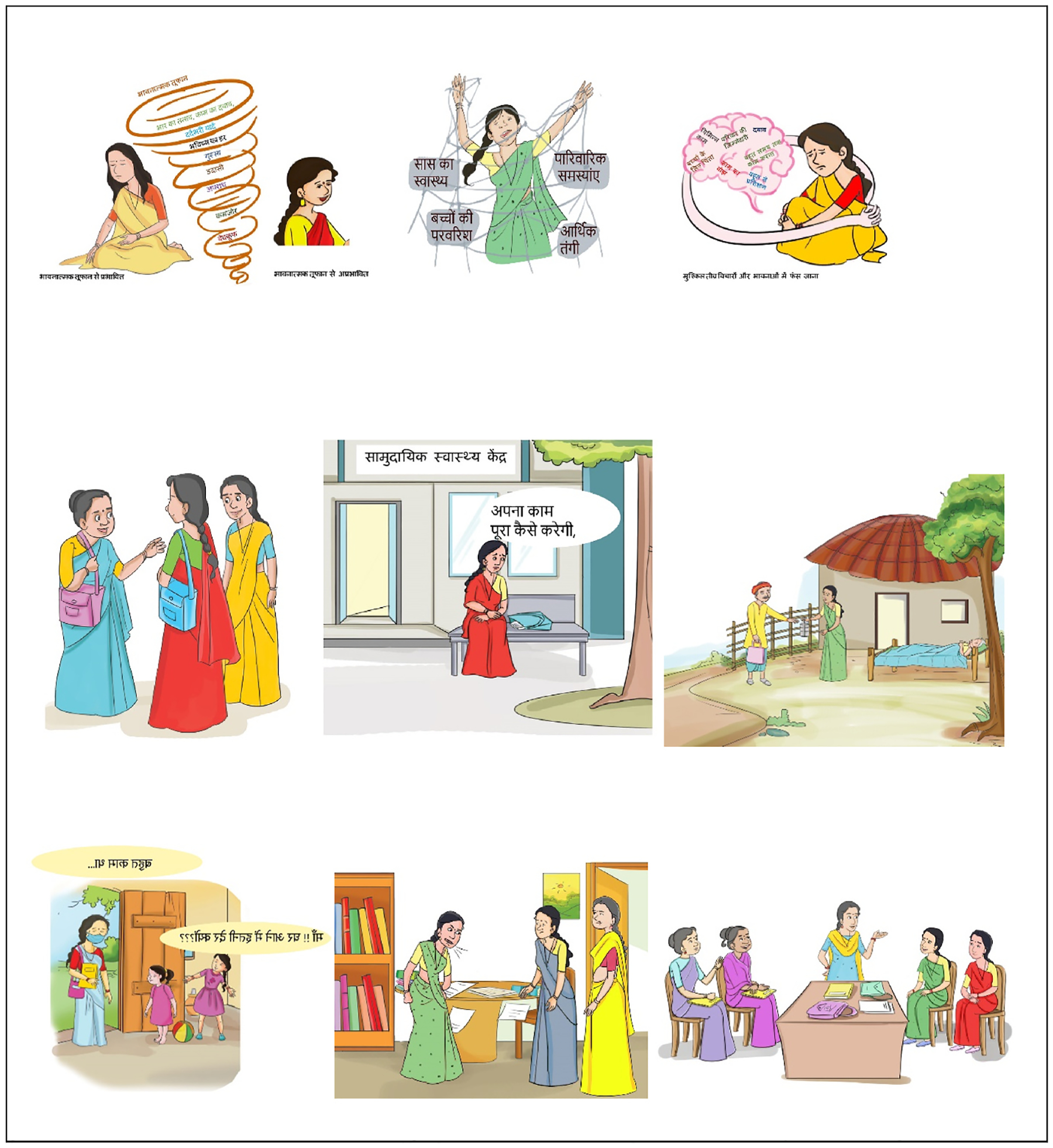
Sample graphics from the digital SH+ intervention adapted for ASHAs in rural India.
3.3. Illustrated SAMBHAV manual
The SAMBHAV manual was designed to specifically include storytelling and relatable examples for ASHAs, and is closely aligned with the original WHO SH+ manual content and layout. The manual follows the same six modules in the digital intervention, offering a supplement that participants can use to reinforce the concepts and revisit the different stress management techniques and strategies if the digital platform is not available or to allow flexibility for accessing a different format (for instance in areas with low-bandwidth). In each module there are different characters, such as ASHAs and a counsellor, who are narrating their own stories of experiencing low mood and burnout and the solutions that they employed to overcome these challenges as outlined in the SH+ intervention. The characters and the stories were inspired from the real-life incidents and the problems that ASHAs face in their daily working life and in maintaining work life balance. Sample content from the illustrated manual is presented in Fig. 4.
Fig. 4.
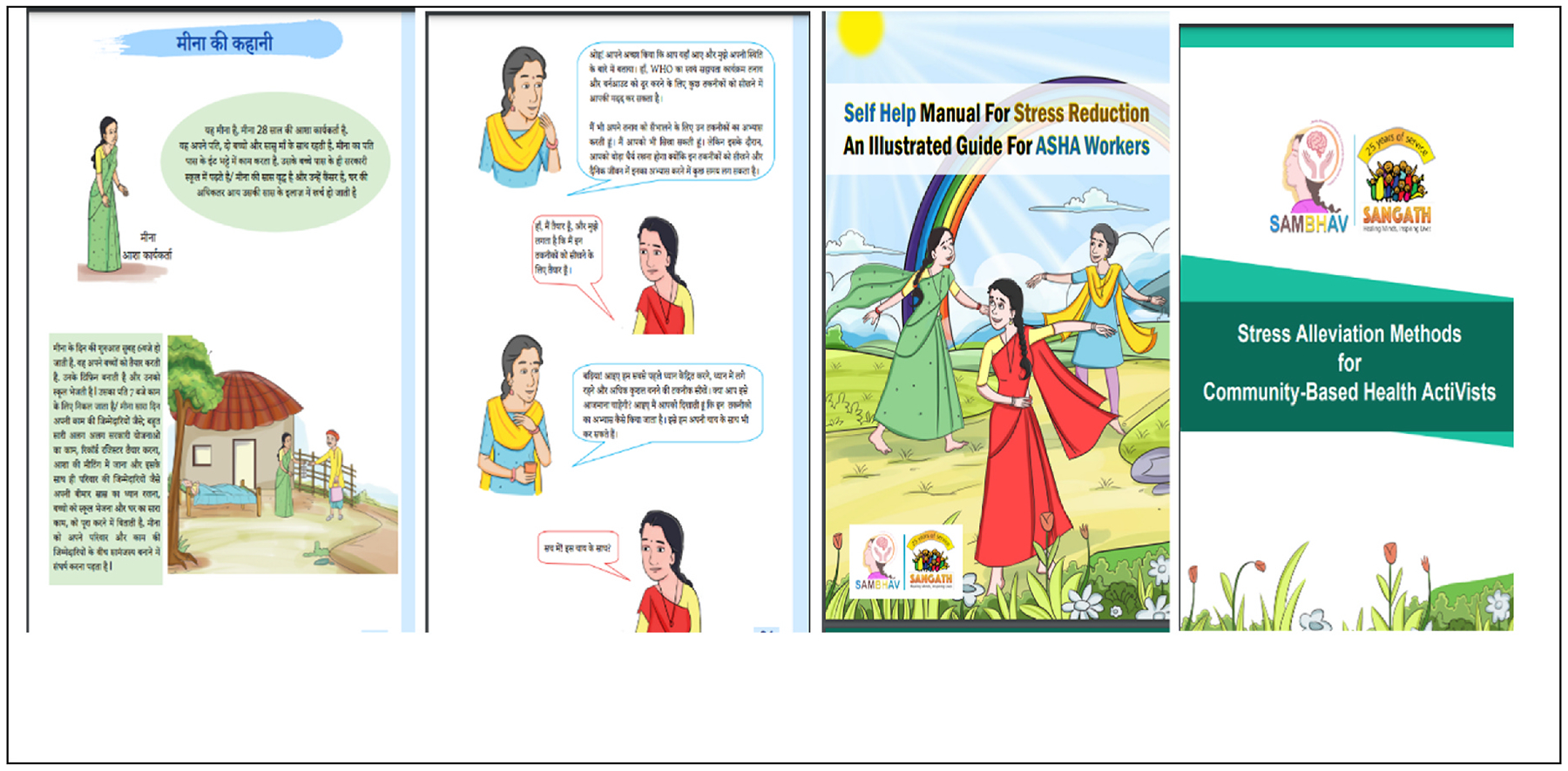
Sample content from the SAMBHAV program manual adapted from the WHO SH+ manual for use with ASHAs in rural India.
4. Discussion
This preliminary study involved the development and adaptation of a digital version of the WHO SH+ intervention consisting of multiple rounds of review within our research team, and integrating feedback from ASHAs to ensure that the content was systematically adapted to the local language and culture, while remaining consistent with the evidence-based SH+ program materials (Epping-Jordan et al., 2016). Importantly, this study builds on our team’s track record developing digital programs for training and supporting ASHAs in rural India (Muke et al. 2019, 2020; Joshi et al., 2022; Khan et al. 2020, 2023; Tyagi et al., 2023), as well as our established research infrastructure in the region (Shidhaye et al., 2019), and longstanding collaboration with the Ministry of Health and Family Welfare, Government of Madhya Pradesh. The digital adapted SH+ intervention for ASHAs developed in this study, called SAMBHAV, holds promise for offering a scalable self-directed approach for reducing stress to support frontline community health workers in primary care settings in India.
This study adds to mounting recognition of the need for novel approaches to address the elevated burnout and distress impacting front-line health workers in LMICs (Wright et al., 2022). CHWs in LMICs are at an increased risk of burnout and distress and many of these frontline health workers live in the same impoverished communities as the patients they serve, travel long distances to rural and underserved areas, and receive low compensation for demanding and emotionally exhausting work (Li et al., 2014; Haq et al., 2008; Selamu et al. 2017, 2019; Dugani et al., 2018; Saprii et al., 2015). Though multiple research studies in LMICs have acknowledged that higher levels of distress and risk of burnout among frontline providers are a result of heavy workload, lack of perceived support, gender inequality, health system power hierarchy, interpersonal conflict, younger age, fewer years in practice, and lower work satisfaction (Ge et al., 2011; Malakouti et al., 2011), there remains a scarcity of research studies focusing on implementing support programs for the well-being of these frontline health workers. Studies have also found that CHWs report being more likely to quit their job when facing these higher levels of burnout (Kim et al., 2018; Mbanga et al., 2018). Despite recent global health system strengthening initiatives focused on enhancing performance of CHWs to improve patient outcomes, increase access to care, and adhere to treatment protocols (Ballard and Paul, 2017; Vasan et al., 2017; Agarwal et al., 2019), there has been virtually no consideration of the mental health needs of this workforce (Naimoli et al., 2014; Scott et al., 2018; Heller et al., 2019). Therefore, addressing psychological distress among CHWs, such as through mindfulness-based skills training (Jacobs et al., 2017) or using evidence-based self-help stress management techniques (Epping-Jordan et al., 2016), could strengthen workforce capacity and overcome challenges to sustained delivery of quality care (Dugani et al., 2018).
Due to the impacts of the COVID-19 pandemic the current study is timely as there have been a multitude of reports documenting the significant increase in workload and resulting risk of burnout among CHWs like ASHAs (Deng and Naslund, 2020). Among ASHAs, recent studies during the pandemic have documented that there has been an ‘intensification’ in their daily responsibilities and tasks, as reflected by an increase in as many as 2–3 additional work hours per day given the added demands for responding to the pandemic containment and vaccination efforts (Niyati and Nelson Mandela, 2020; Upadhyaya, 2022). Additionally, ASHAs have reported receiving reduced or irregular pay given that many incentive-based activities were suspended, or delayed payments, while simultaneously being required to work in unsafe conditions without adequate protective equipment (Niyati and Nelson Mandela, 2020; Nanda et al., 2020; Upadhyaya, 2022). In the most serious instances, ASHAs experienced elevated mental distress as they were the target of discrimination and violence in several communities given their role in containing the pandemic and facilitating case finding activities, further fueled by fears of contracting the virus as well as fears among villagers that they could spread the virus (Konduru et al., 2022; Upadhyaya, 2022). With recent research and reports shedding light on the many challenges that ASHAs have been facing in their day-to-day work over the course of the COVID-19 pandemic, there have been calls to improve the working conditions and ensuring dedicated efforts to both empower and address the psychosocial and material needs of this essential workforce (Nanda et al., 2020). Specifically, the scalable digital stress reduction program developed in this study could complement additional efforts aimed at providing intrinsic support to ASHAs, and potentially mitigating some of the lasting consequences of the pandemic.
Our study also expands on new efforts seeking to leverage widely available digital technologies for supporting frontline health workers in diverse settings across India. While many of these prior studies, including work by our team, have primarily focused on training and supervision for ASHAs (Saha et al., 2020; Singh et al., 2021; Gopalakrishnan et al., 2020; Muke et al., 2020; Kaphle et al., 2016), few programs have considered whether digital technology could enable delivery of brief self-help interventions aimed at empowering ASHAs in responding to work-related stressors. Our study advances these efforts by considering the potential to leverage these same digital platforms used for training to offer stress reduction content aimed at preventing burnout and promoting the wellbeing of the workforce. This also is complementary to recent developments in India, where the disruption to routine care services caused by the COVID-19 pandemic has resulted in accelerated adoption and use of digital technology throughout the health system (Narayanan, 2021). This has also sparked the Government’s launch of the National Digital Health Mission as part of the Ayushman Bharat initiative in 2021, with the aim to develop the backbone necessary for supporting an integrated digital health infrastructure across the country (National Health Authority, 2022). As a result, there has been renewed interest in the use of digital technologies for supporting non-communicable disease care (Gudi et al., 2021), and specifically for training and supporting frontline health workers (Gautam et al., 2021). Therefore, there is immediate potential and opportunity for digital technology to achieve wide reach for supporting this essential workforce (Ved et al., 2019).
4.1. Limitations
It is important to consider some of the limitations with this initial formative study. While we describe the process for adapting the WHO SH+ intervention content and then developing the digital intervention tailored to the context for ASHAs in rural India, we have not yet assessed whether the digital SH+ intervention is effective and can achieve its desired goal of reducing psychological distress and burnout, and promoting mental health and well-being of the target group of ASHAs. Furthermore, continued efforts will be needed to determine whether such a scalable digital intervention, when made available across the broader workforce of ASHAs, can contribute to improvements in their job satisfaction, work performance, and ultimately, improving patient care while preventing health worker burnout and attrition. It seems intuitive that mentally healthy and motivated ASHAs will be better positioned to deliver high quality care to their patients; however, implementation research is necessary to consider this potential relationship, particularly in lower resource settings like India. As our team systematically adapted the evidence-based WHO SH+ intervention content for use with ASHAs in rural India, and further digitized the content for self-directed delivery on a smartphone application, it is possible that additional perspectives related to the feasibility and acceptability of the intervention content were not sufficiently captured given the small sample size. Furthermore, there was limited involvement of ASHA Facilitators in this study, which could partly be because the ASHA Facilitators were too busy as they typically assume a greater workload relative to ASHAs. This highlights the need to reach this group as they could stand to benefit from access to the digital stress reduction intervention. We also recognize that the ASHAs who enrolled in this study came from one rural district in a large state in Central India, and that they were previously engaged in other research and training activities being conducted by our team. It is likely that they were already highly interested in the focus of the current study and had prior exposure to digital intervention content, and therefore may not be representative of ASHAs in other settings across India. We worked to overcome this concern by tailoring the content to the everyday experiences of ASHAs, while simultaneously maintaining consistency with the original content of the SH+ intervention manual to ensure widespread applicability. Nonetheless, further region-specific modifications may be necessary to accommodate diverse languages, cultures, and contexts. Additionally, we focused specifically on reaching ASHAs with the adapted SH+ intervention because ASHAs represent the largest single workforce of CHWs on the globe, numbering over 1 million (Ved et al., 2019); however, ASHAs are all women, meaning that our findings likely do not generalize to male frontline health workers, highlighting another important focus area for future efforts. While use of digital interventions hold potential for achieving greater scalability, the reliance on smartphone devices with adequate connectivity may create barriers for reaching ASHAs working in the most impoverished settings where there is limited bandwidth, while also limiting the use of such interventions for CHWs who do not have access to digital devices or who may not have the necessary digital literacy skills for navigating the program content. In India, there has been increasing adoption of digital technology among frontline health workers in recent years (Bashingwa et al., 2021), yet ongoing attention will be necessary to overcome digital barriers to achieving scale up of such programs. For example, one approach could involve use of the written content for the program augmented with brief SMS text messaging support from a health coach to avoid the need for more costly smartphones and reliable online connectivity. Lastly, the current study and intervention development process was voluntary, meaning that the ASHAs who chose to contribute to our work may have already been experiencing distress, and therefore, may have been especially interested in learning more about stress management techniques. This may limit the generalizability of our program, highlighting the need for real world testing where the program can be made more widely available and allow tracking of levels of engagement and adoption among the target population of ASHAs.
5. Conclusion and next steps
The COVID-19 pandemic has put additional stress and risk of burnout on healthcare providers in resource constrained settings, and especially among frontline CHWs such as AHSAs in rural India. The need of the hour is to care for the carers and provide psychosocial support promoting the mental health and well-being is one of the key recommendations offered by the WHO for ensuring an efficient and responsive healthcare system (World Health Organization, 2022). There has been limited consideration within most health systems globally on the mental health and psychosocial needs of CHWs (Wright et al., 2022); therefore, the SAMBHAV program adapted from the WHO’s SH+ intervention holds promise. Our immediate next step is to pilot test the final digital intervention developed in the current formative research study with a larger cohort of ASHAs, where we will have the opportunity to collect measures of preliminary effectiveness in reducing psychological distress, while also capturing additional insights related to feasibility and acceptability of the program that could inform further modifications to facilitate implementation and scale up. If found to be effective, we are confident that the SAMBHAV digital stress reduction program would help to address an immense unmet need by empowering frontline community health workers to recognize work-related stressors and equip them with skills for managing these challenges and negotiating other concerns in their daily work and life.
This formative study is the first of its kind in India, and offers an initial step towards promoting the mental health and well-being of the world’s largest cohort of CHWs, the ASHAs numbering over 1 million, using a scalable digital version of the evidence-based WHO SH+ intervention (Tol et al., 2020; Epping-Jordan et al., 2016). Our preliminary efforts also set the groundwork to be considered by the state and central health systems policymakers to adapt and adopt this simple digital intervention for improving the well-being of their critically important work cadre. These efforts can also extend beyond the study sites in India for supporting CHWs in other low-resource settings, especially in the context of strengthening health systems due to the impacts of the COVID-19 pandemic. By recognizing the mental health and well-being needs of CHWs such as ASHAs, our exploratory study addresses a major gap in the global health literature, where there is urgent need to address the elevated stress and risk of burnout experienced by these frontline health workers (Wright et al., 2022).
Acknowledgements
We are thankful to Harvard Global Health Institute for funding the project. We are grateful to our collaborators, the Chief Medical and Health Officer office, Sehore and Dr Sharad Tiwari and Dr Shailesh Sakalle from the National Health Mission, Madhya Pradesh for their guidance and support for this project. Most importantly, we wish to thank the ASHAs who participated in this study and who volunteered their time to support the adaptation and development of SAMBHAV, a digital version of the WHO’s SH+ intervention.
Funding
This study was supported by grant funding from the Harvard Global Health Institute Burke Fellowship. Additional support came from a grant awarded from the National Institute of Mental Health (U19MH113211-01).
Footnotes
CRediT authorship contribution statement
Ritu Shrivastava: Conceptualization, Methodology, intervention development, Writing – original draft, All authors have read and agreed to the published version of the manuscript. Abhishek Singh: Conceptualization, Methodology, intervention development, Writing – original draft, Writing – review & editing, All authors have read and agreed to the published version of the manuscript. Azaz Khan: Conceptualization, Methodology, content review, All authors have read and agreed to the published version of the manuscript. Shivangi Choubey: intervention development, All authors have read and agreed to the published version of the manuscript. Juliana Restivo Haney: content review, Writing – review & editing, All authors have read and agreed to the published version of the manuscript. Eirini Karyotaki: content review, All authors have read and agreed to the published version of the manuscript. Deepak Tugnawat: Conceptualization, Methodology, Supervision, Project administration, All authors have read and agreed to the published version of the manuscript. Anant Bhan: Conceptualization, Methodology, Supervision, Writing – review & editing, All authors have read and agreed to the published version of the manuscript. John A. Naslund: Conceptualization, Methodology, content review, Writing – original draft, Writing – review & editing, Funding acquisition, All authors have read and agreed to the published version of the manuscript.
Declaration of competing interest
The authors declare no competing interests.
References
- A-tjak, Jacqueline GL, Davis Michelle L., Morina Nexhmedin, Powers Mark B., Smits Jasper AJ., Emmelkamp Paul MG., 2015. ‘A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems’. Psychother. Psychosom 84, 30–36. [DOI] [PubMed] [Google Scholar]
- Acarturk Ceren, Uygun Ersin, Ilkkursun Zeynep, Carswell Kenneth, Tedeschi Federico, Batu Mine, Eskici Sevde, Kurt Gulsah, Anttila Minna, Au Teresa, 2022. ‘Effectiveness of a WHO self-help psychological intervention for preventing mental disorders among Syrian refugees in Turkey: a randomized controlled trial’. World Psychiatr. 21, 88–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agarwal Smisha, Curtis Sian L., Angeles Gustavo, Speizer Ilene S., Singh Kavita, Thomas James C., 2019a. The impact of India’s accredited social health activist (ASHA) program on the utilization of maternity services: a nationally representative longitudinal modelling study. Hum. Resour. Health 17, 1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agarwal Smisha, Sripad Pooja, Johnson Caroline, Kirk Karen, Bellows Ben, Joseph Ana, Blaser Vince, Kumar Meghan Bruce, Buchholz Kathleen, Casseus Alain, 2019b. A conceptual framework for measuring community health workforce performance within primary health care systems. Hum. Resour. Health 17, 86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aryal Santosh, Shastry CS, Chand Sharad, Bhandari Ramesh, Bahadur Rawal Kala, Voora Lavanya, 2019. The linkage between occupation and stress among community health workers: an indo-global perspective. Biomed 39, 388–393. [Google Scholar]
- Bajpai Nirupam, Dholakia Ravindra H., 2011. ‘Improving the Performance of Accredited Social Health Activists in India. Columbia Global Centres South Asia, Mumbai. [Google Scholar]
- Baker III, Fredrick W, Moukhliss Sarah, 2020. ‘Concretising design thinking: a content analysis of systematic and extended literature reviews on design thinking and human-centred design’. Rev. Educ 8, 305–333. [Google Scholar]
- Ballard Madeleine, Paul Montgomery, 2017. ‘Systematic review of interventions for improving the performance of community health workers in low-income and middle-income countries’. BMJ Open 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bashingwa Harrisson, Juste Jean, Shah Neha, Mohan Diwakar, Scott Kerry, Chamberlain Sara, Mulder Nicola, Rahul Sai, Arora Salil, Chakraborty Arpita, Ummer Osama, 2021. Examining the reach and exposure of a mobile phone-based training programme for frontline health workers (ASHAs) in 13 states across India. BMJ Glob. Health 6, e005299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernal Guillermo, Bonilla Janet, Bellido Carmen, 1995. ‘Ecological validity and cultural sensitivity for outcome research: issues for the cultural adaptation and development of psychosocial treatments with Hispanics’. J. Abnorm. Child Psychol 23, 67–82. [DOI] [PubMed] [Google Scholar]
- Bernal Guillermo, Jiménez-Chafey María I., Rodríguez Melanie M Domenech, 2009. ‘Cultural adaptation of treatments: a resource for considering culture in evidence-based practice’. Prof. Psychol. Res. Pract 40, 361. [Google Scholar]
- Bhattacharyya Karabi, Peter Winch, LeBan K, Tien M, 2001. Community Health Worker Incentives and Disincentives. USAID-BASICS II, Virginia. [Google Scholar]
- Black Candace J., Jenna M Berent, Joshi Udita, Khan Azaz, Chamlagai Lila, Shrivastava Ritu, Gautam Bhuwan, Negeye Abdikadir, Nor Iftin, Abdi Ali, Halimo, 2023. Applying human-centered design in global mental health to improve reach among underserved populations in the United States and India. Glob. Health Sci. Pract 11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Black Robert E., Taylor Carl E., Arole Shobha, Bang Abhay, Bhutta Zulfiqar A., Mushtaque A, Chowdhury R, Kirkwood Betty R., Kureshy Nazo, Lanata Claudio F., Phillips James F., 2017. ‘Comprehensive review of the evidence regarding the effectiveness of community–based primary health care in improving maternal, neonatal and child health: 8. summary and recommendations of the Expert Panel’. J. Global Health 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bo Hai-Xin, Wen Li, Yuan Yang, Wang Yu, Zhang Qinge, Cheung Teris, Wu Xinjuan, Xiang Yu-Tao, 2021. ‘Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China’. Psychol. Med 51, 1052–1053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown FL, Carswell Kenneth, Augustinavicius Jura, Adaku Alex, Leku MR, White RG, Ventevogel Peter, Kogan CS, García-Moreno C, Bryant RA, 2018. ‘Self Help Plus: study protocol for a cluster-randomised controlled trial of guided self-help with South Sudanese refugee women in Uganda’. Global Mental Health 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carswell Kenneth, Harper-Shehadeh Melissa, Watts Sarah, van’t Hof Edith, Abi Ramia Jinane, Heim Eva, Wenger Andreas, van Ommeren Mark, 2018. ‘Step-by-Step: a new WHO digital mental health intervention for depression’. mHealth 4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coderre Sylvain, Woloschuk Wayne, Mclaughlin Kevin, 2009. ‘Twelve tips for blueprinting’. Med. Teach 31, 322–324. [DOI] [PubMed] [Google Scholar]
- Deng Davy, Naslund John A., 2020. ‘Psychological Impact of COVID-19 Pandemic on Frontline Health Workers in Low-And Middle-Income Countries. Harvard public health review, Cambridge, Mass, p. 28. [PMC free article] [PubMed] [Google Scholar]
- Deshpande Swati, Barsha Gadapani P, Manapurath Rukman M., 2019. ‘Analyzing the challenges and demotivating factors faced by accredited social health activist workers in tribal India in implementing their roles’. Int. J. Med. Sci. Publ. Health 9, 1. [Google Scholar]
- Dubale Benyam W., Friedman Lauren E., Chemali Zeina, Denninger John W., Mehta Darshan H., Alem Atalay, Fricchione Gregory L., Dossett Michelle L., Gelaye Bizu, 2019. ‘Systematic review of burnout among healthcare providers in sub-Saharan Africa’. BMC Publ. Health 19, 1247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dugani Sagar, Afari Henrietta, Hirschhorn Lisa R., Ratcliffe Hannah, Veillard Jeremy, Martin Gayle, Lagomarsino Gina, Basu Lopa, Bitton Asaf, 2018. ‘Prevalence and Factors Associated with Burnout Among Frontline Primary Health Care Providers in Low-And Middle-Income Countries: a Systematic Review, vol. 2. Gates open research. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Epping-Jordan JoAnne, E., Harris Russ, Brown Felicity L., Carswell Kenneth, Foley Claudette, García-Moreno Claudia, Kogan Cary, van Ommeren Mark, 2016. ‘Self-Help Plus (SH+): a new WHO stress management package’. World Psychiatr. 15, 295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gautam Shefali, Shukla Aparna, Mishra Neelkamal, Kohli Monika, Singh Gyan P., 2021. ‘Effectiveness of virtual training for medical officers and community health officers in the critical care management of COVID-19 patients in the intensive care unit’. Indian J. Anaesth 65, S168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ge Cuixia, Fu Jialiang, Chang Ying, Wang Lie, 2011. ‘Factors associated with job satisfaction among Chinese community health workers: a cross-sectional study’. BMC Publ. Health 11, 1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gopalakrishnan Lakshmi, Buback Laura, Fernald Lia, Walker Dilys, Smith Diamond, Nadia, in addition to The CAS Evaluation Consortium, 2020. ‘Using mHealth to improve health care delivery in India: a qualitative examination of the perspectives of community health workers and beneficiaries’. PLoS One 15, e0227451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gudi Nachiket, Yadav Uday N., John Oommen, Webster Ruth, 2021. ‘Challenges and opportunities in employing digital health to address self-management needs of people with NCDs in India’. BMJ Innovat.: bmjinnov 2020, 000620. [Google Scholar]
- Haq Zaeem, Iqbal Zafar, Rahman Atif, 2008. Job stress among community health workers: a multi-method study from Pakistan. Int. J. Ment. Health Syst 2, 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harper Shehadeh, Joanne Melissa, Ramia Abi, Jinane Cuijpers, Pim El Chammay, Rabih Heim, Eva Kheir, Wissam Saeed, Khalid, van Ommeren Mark, van’t Hof Edith, Watts Sarah, 2020. ‘Step-by-Step, an e-mental health intervention for depression: a mixed methods pilot study from Lebanon’. Front. Psychiatr 10, 986. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes Steven C., Pistorello Jacqueline, Levin Michael E., 2012. ‘Acceptance and commitment therapy as a unified model of behavior change’. Counsel. Psychol 40, 976–1002. [Google Scholar]
- Heller David J., Kumar Anirudh, Kishore Sandeep P., Horowitz Carol R., Joshi Rohina, Vedanthan Rajesh, 2019. ‘Assessment of barriers and facilitators to the delivery of Care for Noncommunicable Diseases by nonphysician health Workers in low-and Middle-Income Countries: a systematic review and qualitative analysis’. JAMA Netw. Open 2, e1916545–e45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacobs Rachel H., Guo Sisi, Kaundinya Prabha, Lakind Davielle, Klein Jesse, Rusch Dana, Walden Angela, Mehta Tara, Atkins Marc, 2017. ‘A pilot study of mindfulness skills to reduce stress among a diverse paraprofessional workforce’. J. Child Fam. Stud 26, 2579–2588. [Google Scholar]
- Joshi Udita, Naslund John A., Anand Aditya, Tugnawat Deepak, Ram Vishwakarma, Bhan Anant, Patel Vikram, Lu Chunling, 2022. Assessing costs of developing a digital program for training community health workers to deliver treatment for depression: a case study in rural India. Psychiatr. Res 307, 114299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kapanee Mary, Rose Aruna, Meena Kolar S., Nattala Prasanthi, Narayana Manjunatha, Sudhir Paulomi M., 2022. Design and development of a training video for Accredited Social Health Activists (ASHAs) on brief psychological intervention for depression. J. Fam. Med. Prim. Care 11, 3862–3867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaphle Sangya, Matheke-Fischer Michael, Neal Lesh, 2016. Effect of performance feedback on community health workers’ motivation and performance in Madhya Pradesh, India: a randomized controlled trial. JMIR Public Health Surveill. 2, e3381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khan Azaz, Sharma Lochan, Agrawal Surbhi, Nayak Sneha Rani, Shrivastava Ritu, Ahuja Romi, Pandit Payal, Singh Abhishek, Singh Spriha, Naslund John A., 2023. ‘Development of a character-strengths based coaching program for rural community health workers to address their work stress in Madhya Pradesh, India’. Curr. Psychol 1–20. [Google Scholar]
- Khan Azaz, Shrivastava Ritu, Tugnawat Deepak, Singh Abhishek, Dimidjian Sona, Patel Vikram, Bhan Anant, Naslund John A., 2020. ‘Design and development of a digital program for training non-specialist health workers to deliver an evidence-based psychological treatment for depression in primary care in India’. J. Technol. Behav. Sci 5, 402–415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim Maria H., Mazenga Alick C., Simon Katie, Yu Xiaoying, Ahmed Saeed, Nyasulu Phoebe, Kazembe Peter N., Stanley Ngoma, Abrams Elaine J., 2018. ‘Burnout and self-reported suboptimal patient care amongst health care workers providing HIV care in Malawi’. PLoS One 13, e0192983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kokane Arun, Pakhare Abhijit, Gururaj Gopalkrishna, Varghese Mathew, Benegal Vivek, Rao Girish N., Arvind Banavaram, Shukla Mukesh, Mitra Arun, Yadav Kriti, 2019. Mental health issues in Madhya Pradesh: insights from national mental health survey of India 2016. Health Care 53 (Multidisciplinary Digital Publishing Institute; ). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Konduru Laalithya, Das Nishant, Kothari-Speakman Gargi, Behura Ajit Kumar, 2022.’Experiencing the COVID-19 pandemic as a healthcare provider in rural Dhanbad, India: an interpretative phenomenological analysis’. PLoS One 17, e0273573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kumar Manasi, Paul Macharia, Vincent Nyongesa, Joseph Kathono, Yator Obadia, Mwaniga Shillah, McKay Mary, Huang Keng Yen, Shidhaye Rahul, Simon Njuguna, 2022. ‘Human-centered design exploration with Kenyan health workers on proposed digital mental health screening and intervention training development: thematic analysis of user preferences and needs’. Digit. Health 8, 20552076221090035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levin Michael E., Pistorello Jacqueline, Hayes Steven C., Seeley John R., Levin Crissa, 2015. ‘Feasibility of an acceptance and commitment therapy adjunctive web-based program for counseling centers’. J. Counsel. Psychol 62, 529. [DOI] [PubMed] [Google Scholar]
- Lewin Simon, Munabi-Babigumira Susan, Glenton Claire, Daniels Karen, Bosch-Capblanch Xavier, Brian Van Wyk E, Odgaard-Jensen Jan, Johansen Marit, Aja Godwin N., Zwarenstein Merrick, 2010. Lay health workers in primary and community health care for maternal and child health and the management of infectious diseases. Cochrane Database Syst. Rev 3. CD004015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li Li, Hu Hongyan, Zhou Hao, He Changzhi, Fan Lihua, Liu Xinyan, Zhang Zhong, Li Heng, Sun Tao, 2014. ‘Work stress, work motivation and their effects on job satisfaction in community health workers: a cross-sectional survey in China’. BMJ Open 4, e004897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo Rui, Guo Pengyue, Shang Menglin, Cai Yuqi, Huang Jinying, He Yiling, Mo Phoenix KH., Wu Anise MS., Xu Roman Dong, Li Jinghua, 2022. Psychological stress self-help interventions for healthcare workers in the context of COVID-19 in China: a randomized controlled trial protocol. Internet Intervent. 28, 100541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mabunda Dirceu, Oliveira Déborah, Sidat Mohsin, Cavalcanti Tavares, Maria Cumbe, Vasco Mandlate, Flávio Wainberg, Milton Cournos, Francine, de Jesus Mari Jair, 2022. ‘Cultural adaptation of psychological interventions for people with mental disorders delivered by lay health workers in Africa: scoping review and expert consultation’. Int. J. Ment. Health Syst 16, 14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malakouti Seyed Kazem, Nojomi Marzieh, Salehi Maryam, Bijari Bita, 2011. Job stress and burnout syndrome in a sample of rural health workers, behvarzes, in Tehran, Iran. Iran. J. Psychiatry 6, 70. [PMC free article] [PubMed] [Google Scholar]
- Manjunath Usha, Sarala R, Rajendra D, Deepashree MR, Chokshi Maulik, Mokashi Tushar, 2022. ‘Assessment of workload of ASHAs: a multi-stakeholder perspective study for task-sharing and task-shifting’. J. Health Manag 24, 62–73. [Google Scholar]
- Mbanga Clarence, Makebe Haman, Tim Divine, Fonkou Steve, Toukam Louise, Njim Tsi, 2018. ‘Determinants of burnout syndrome among nurses in Cameroon’. BMC Res. Notes 11, 1–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meena Sadhana, Rathore Monika, Kumawat Pragya, Singh Arpit, 2020. Challenges faced by ASHAs during their field works: a cross sectional observational study in rural area of Jaipur, Rajasthan. Int. J. Med. Publ. Health 10. [Google Scholar]
- Menon Geetha R., Yadav Jeetendra, Aggarwal Sumit, Singh Ravinder, Kaur Simran, Chakma Tapas, Periyasamy Murugesan, Venkateswaran Chitra, Singh Prashant Kumar, Balachandar Rakesh, 2022. ‘Psychological distress and burnout among healthcare worker during COVID-19 pandemic in India—a cross-sectional study’. PLoS One 17, e0264956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Menon Purnima, Deolalikar Anil, Bhaskar Anjor, 2008. The India State Hunger Index: Comparisons of Hunger across States.
- Mishra Arima, 2014. ‘‘Trust and teamwork matter’: community health workers’ experiences in integrated service delivery in India’. Global Publ. Health 9, 960–974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mishra Bijaya Kumar, Kanungo Srikanta, Patel Kripalini, Swain Swagatika, Dwivedy Subhralaxmi, Panda Subhashree, Karna Sonam, Bhuyan Dinesh, Som Meena, Merta Raj, Brajesh, 2022. Resolution of resilience: empirical findings on the challenges faced and the mitigation strategies adopted by community health workers (CHWs) to provide maternal and child health (MCH) services during the COVID-19 pandemic in the context of odisha, India. In: Healthcare. MDPI, p. 88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Modi Dhiren, Dholakia Nishith, Gopalan Ravi, Venkatraman Sethuraman, Dave Kapilkumar, Shah Shobha, Desai Gayatri, Qazi Shamim A., Sinha Anju, Pandey Ravindra Mohan, 2019. ‘mHealth intervention “ImTeCHO” to improve delivery of maternal, neonatal, and child care services—a cluster-randomized trial in tribal areas of Gujarat, India’. PLoS Med. 16, e1002939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mondal Nilanjan, Murhekar Manoj V., 2018. ‘Factors associated with low performance of accredited social health activist (ASHA) regarding maternal care in Howrah district, West Bengal, 2015–’16: an unmatched case control study’. Clin. Epidemiol. Global Health 6, 21–28. [Google Scholar]
- Muke S, Shrivastava R, Mitchell L, Khan A, Murhar V, Tugnawat D, Shidhaye R, Patel V, Naslund JA, 2019. Acceptability and feasibility of digital technology for training community health workers to deliver brief psychological treatment for depression in rural India. Asian J. Psychiatr 45, 99–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muke S, Tugnawat D, Joshi U, Anand A, Khan A, Shrivastava R, Singh A, Restivo JL, Bhan A, Patel V, Naslund JA, 2020. ‘Digital training for non-specialist health workers to deliver a brief psychological treatment for depression in primary care in India: findings from a randomized pilot study’. Int. J. Environ. Res. Publ. Health 17, 6368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Naimoli Joseph F., Frymus Diana E., Wuliji Tana, Franco Lynne M., Newsome Martha H., 2014. ‘A community health worker “logic model”: towards a theory of enhanced performance in low-and middle-income countries’. Hum. Resour. Health 12, 56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nanda Priya, Lewis Tom Newton, Das Priya, Krishnan Suneeta, 2020. From the frontlines to centre stage: resilience of frontline health workers in the context of COVID-19. Sexual Reprod. Health Matters 28, 1837413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Narayanan Krishnan, 2021. Digital Health in India’, Itihaasa Research and Digital. Accessed June 20. https://itihaasa.com/public/pdf/Digital_Health_in_India.pdf.
- Naslund John A., Deng Davy, 2021. ‘Addressing mental health stigma in low-income and middle-income countries: a new frontier for digital mental health’. Ethics Med. Public Health 19, 100719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Naslund John A., Gonsalves Pattie P., Gruebner Oliver, Pendse Sachin R., Smith Stephanie L., Sharma Amit, Raviola Giuseppe, 2019. Digital innovations for global mental health: opportunities for data science, task sharing, and early intervention. Curr. Treatment Options Psychiatr 6, 337–351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Naslund John A., Spagnolo Jessica, 2023. Cultural adaptations of digital therapeutics. In: Digital Therapeutics for Mental Health and Addiction. Elsevier. [Google Scholar]
- Naslund John A., Tugnawat Deepak, Anand Aditya, Cooper Zafra, Dimidjian Sona, Fairburn Christopher G., Hollon Steven D., Joshi Udita, Khan Azaz, Lu Chunling, 2021. ‘Digital training for non-specialist health workers to deliver a brief psychological treatment for depression in India: protocol for a three-arm randomized controlled trial’. Contemp. Clin. Trials 102, 106267. [DOI] [PubMed] [Google Scholar]
- National Health Authority, 2022. Ayushman Bharat Digital Mission. Government of India. Accessed June 20. https://ndhm.gov.in/. [Google Scholar]
- Niyati S, Nelson Mandela S, 2020. ‘Impact of the pandemic on accredited social health activists (ASHA) in India’. Rev. Agrarian Stud 10. [Google Scholar]
- Otu Akaninyene, Charles Carlo Handy, Yaya Sanni, 2020. ‘Mental health and psychosocial well-being during the COVID-19 pandemic: the invisible elephant in the room’. Int. J. Ment. Health Syst 14, 1–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pallas Sarah Wood, Minhas Dilpreet, Pérez-Escamilla Rafael, Taylor Lauren, Curry Leslie, Bradley Elizabeth H., 2013. Community health workers in low-and middle-income countries: what do we know about scaling up and sustainability? Am. J. Publ. Health 103, e74–e82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perera Camila, Salamanca-Sanabria Alicia, Caballero-Bernal Joyce, Feldman Lya, Hansen Maj, Bird Martha, Hansen Pernille, Dinesen Cecilie, Wiedemann Nana, Vallìeres Frédérique, 2020. ‘No implementation without cultural adaptation: a process for culturally adapting low-intensity psychological interventions in humanitarian settings’. Conflict Health 14, 1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perry Henry B., Zulliger Rose, Rogers Michael M., 2014. ‘Community health workers in low-, middle-, and high-income countries: an overview of their history, recent evolution, and current effectiveness’. Annu. Rev. Publ. Health 35, 399–421. [DOI] [PubMed] [Google Scholar]
- Pulagam Praveenya, Satyanarayana Pradeep Tarikere, 2021. Stress, anxiety, work-related burnout among primary health care worker: a community based cross sectional study in Kolar. J. Fam. Med. Prim. Care 10, 1845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Purgato Marianna, Carswell Kenneth, Acarturk Ceren, Au Teresa, Akbai Sena, Anttila Minna, Baumgartner Josef, Bailey Della, Biondi Massimo, Bird Martha, 2019. ‘Effectiveness and cost-effectiveness of Self-Help Plus (SH+) for preventing mental disorders in refugees and asylum seekers in Europe and Turkey: study protocols for two randomised controlled trials’. BMJ Open 9, e030259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Purgato Marianna, Carswell Kenneth, Tedeschi Federico, Acarturk Ceren, Anttila Minna, Au Teresa, Bajbouj Malek, Baumgartner Josef, Biondi Massimo, Churchill Rachel, 2021. ‘Effectiveness of self-help plus in preventing mental disorders in refugees and asylum seekers in Western Europe: a multinational randomized controlled trial’. Psychother. Psychosom 90, 403–414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rahman Atif, Akhtar Parveen, Hamdani Syed Usman, Atif Najia, Nazir Huma, Uddin Iftikhar, Nisar Anum, Huma Zille, Maselko Joanna, Sikander Siham, 2019. ‘Using technology to scale-up training and supervision of community health workers in the psychosocial management of perinatal depression: a non-inferiority, randomized controlled trial’. Global Mental Health 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saha Somen, Priya Kotwani, Pandya Apurvakumar, Patel Chintan, Shah Komal, Saxena Deepak, Puwar Tapasvi, Desai Shrey, Patel Dashrath M., Sethuraman AV, 2020. ‘Addressing comprehensive primary healthcare in Gujarat through mHealth intervention: early implementation experience with TeCHO+ programme’. J. Fam. Med. Prim. Care 9, 340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saprii Lipekho, Richards Esther, Kokho Puni, Theobald Sally, 2015. ‘Community health workers in rural India: analysing the opportunities and challenges Accredited Social Health Activists (ASHAs) face in realising their multiple roles’. Hum. Resour. Health 13, 1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scott Kerry, Beckham SW, Gross Margaret, George Pariyo, Krishna D Rao, Cometto Giorgio, Perry Henry B., 2018. ‘What do we know about community-based health worker programs? A systematic review of existing reviews on community health workers’. Hum. Resour. Health 16, 39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scott Kerry, George Asha S., Rajani R Ved, 2019. Taking stock of 10 years of published research on the ASHA programme: examining India’s national community health worker programme from a health systems perspective. Health Res. Pol. Syst 17, 1–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scott Kerry, Shanker Shobhit, 2010. ‘Tying their hands? Institutional obstacles to the success of the ASHA community health worker programme in rural north India’. AIDS Care 22, 1606–1612. [DOI] [PubMed] [Google Scholar]
- Selamu Medhin, Hanlon Charlotte, Medhin Girmay, Graham Thornicroft, Fekadu Abebaw, 2019. ‘Burnout among primary healthcare workers during implementation of integrated mental healthcare in rural Ethiopia: a cohort study’. Hum. Resour. Health 17, 58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Selamu Medhin, Graham Thornicroft, Fekadu Abebaw, Hanlon Charlotte, 2017. ‘Conceptualisation of job-related wellbeing, stress and burnout among healthcare workers in rural Ethiopia: a qualitative study’. BMC Health Serv. Res 17, 412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shidhaye R, Lyngdoh T, Murhar V, Samudre S, Krafft T, 2017. ‘Predictors, help-seeking behaviour and treatment coverage for depression in adults in Sehore district, India’. BJPsych Open 3, 212–222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shidhaye Rahul, Baron Emily, Murhar Vaibhav, Rathod Sujit, Khan Azaz, Singh Abhishek, Shrivastava Sanjay, Muke Shital, Shrivastava Ritu, Lund Crick, 2019. Community, facility and individual level impact of integrating mental health screening and treatment into the primary healthcare system in Sehore district, Madhya Pradesh, India. BMJ Glob. Health 4, e001344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singh Debra, Negin Joel, Otim Michael, Orach Garimoi, Christopher Cumming, Robert, 2015. The effect of payment and incentives on motivation and focus of community health workers: five case studies from low-and middle-income countries. Hum. Resour. Health 13, 1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singh Neha S., Scott Kerry, George Asha, Amnesty Elizabeth LeFevre, Ved Rajani, 2021. ‘A tale of ‘politics and stars aligning’: analysing the sustainability of scaled up digital tools for front-line health workers in India’. BMJ Glob. Health 6, e005041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suryanarayana MH, Agrawal Ankush, Seeta Prabhu K, 2016. ‘Inequality-adjusted human development Index: states in India’. Indian J. Hum. Dev 10, 157–175. [Google Scholar]
- Suryanarayana MH, Agrawal A, Seeta Prabhu K, 2011. Inequality-adjusted Human Development Index for India’s States 2011. http://www.undp.org/content/dam/india/docs/inequality_adjusted_human_development_index_for_indias_state1.pdf.
- Tol WA, Augustinavicius J, Carswell K, Brown Fl, Adaku A, Leku MR, Garcia-Moreno C, Ventevogel P, White RG, Van Ommeren M, 2018. ‘Translation, adaptation, and pilot of a guided self-help intervention to reduce psychological distress in South Sudanese refugees in Uganda’. Global Mental Health 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tol Wietse A., Augustinavicius Jura, Carswell Kenneth, Leku Marx R., Adaku Alex, Brown Felicity L., García-Moreno Claudia, Ventevogel Peter, White Ross G., Kogan Cary S., 2018. Feasibility of a guided self-help intervention to reduce psychological distress in South Sudanese refugee women in Uganda. World Psychiatr. 17, 234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tol Wietse A., Leku Marx R., Lakin Daniel P., Carswell Kenneth, Augustinavicius Jura, Adaku Alex, Teresa M Au, Brown Felicity L., s Richard A., Garcia-Moreno Claudia, 2020. ‘Guided self-help to reduce psychological distress in South Sudanese female refugees in Uganda: a cluster randomised trial’. Lancet Global Health 8, e254–e263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Triplett Noah S., Munson Sean, Mbwayo Anne, Mutavi Teresia, Weiner Bryan J., Collins Pamela, Amanya Cyrilla, Shannon Dorsey, 2021. ‘Applying human-centered design to maximize acceptability, feasibility, and usability of mobile technology supervision in Kenya: a mixed methods pilot study protocol’. Implement. Sci. Commun 2, 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tulenko Kate, Mgedal Sigrun, Afzal Mahmood, Muhammad Frymus, Diana Oshin, Adetokunbo Pate, Muhammad Quain, Estelle Pinel, Arletty Wynd, Shona Zodpey, Sanjay, 2013. Community health workers for universal health-care coverage: from fragmentation to synergy. Bull. World Health Organ 91, 847–852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tyagi Vidhi, Khan Azaz, Siddiqui Saher, Abhilashi Kakra, Minal Dhurve, Pooja Tugnawat, Deepak Bhan, Anant Naslund, John A, 2023. ‘Development of a digital program for training community health workers in the detection and referral of schizophrenia in rural India’. Psychiatr. Q 1–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Upadhyaya Manorama, 2022. Invisible frontline warriors of COVID-19: an intersectional feminist study of ASHA workers in India. In: Systemic Inequality, Sustainability and COVID-19. Emerald Publishing Limited. [Google Scholar]
- Vasan Ashwin, Mabey David C., Chaudhri Simran, Helen-Ann Brown Epstein, Lawn Stephen D., 2017. ‘Support and performance improvement for primary health care workers in low-and middle-income countries: a scoping review of intervention design and methods’. Health Pol. Plann 32, 437–452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ved Rajani, Scott Kerry, Gupta Garima, Ummer Osama, Singh Swaran, Srivastava Anuj, George Asha S., 2019. ‘How are gender inequalities facing India’s one million ASHAs being addressed? Policy origins and adaptations for the world’s largest all-female community health worker programme’. Hum. Resour. Health 17, 1–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wheelock Alyse, Bechtel Christine, Bruce Leff, 2020. ‘Human-centered design and trust in medicine’. JAMA 324, 2369–2370. [DOI] [PubMed] [Google Scholar]
- Willis-Shattuck Mischa, Bidwell Posy, Thomas Steve, Wyness Laura, Blaauw Duane, Ditlopo Prudence, 2008. ‘Motivation and retention of health workers in developing countries: a systematic review’. BMC Health Serv. Res 8, 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization, 2020. Doing what Matters in Times of Stress: an Illustrated Guide.
- World Health Organization, 2022. ‘Caring for those who care: guide for the development and implementation of occupational health and safety programmes for health workers.’. In: Caring for Those Who Care: Guide for the Development and Implementation of Occupational Health and Safety Programmes for Health Workers. [Google Scholar]
- Wright Tanya, Mughal Faraz, Babatunde Opeyemi O., Dikomitis Lisa, Mallen Christian D., Helliwell Toby, 2022. ‘Burnout among primary health-care professionals in low-and middle-income countries: systematic review and meta-analysis’. Bull. World Health Organ 100, 385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yardley Lucy, Morrison Leanne, Bradbury Katherine, Muller Ingrid, 2015. ‘The person-based approach to intervention development: application to digital health-related behavior change interventions’. J. Med. Internet Res 17, e4055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yella Tanuja, Dmello Mackwin K., 2022. ‘Burnout and sleep quality among community health workers during the pandemic in selected city of Andhra Pradesh’. Clin. Epidemiol. Global Health 16, 101109. [DOI] [PMC free article] [PubMed] [Google Scholar]