

Abstract
OBJECTIVE:
To evaluate the efficacy of electroacupuncture (EA) intervention on myocardial protection and postoperative rehabilitation in patients undergoing cardiac surgery with cardiopulmonary bypass (CPB).
METHODS:
Eight databases, including PubMed, Embase, the Cochrane Library, Web of Science, Chinese BioMedical Literature Database, China National Knowledge Infrastructure Database, Wanfang Data, China Science and Technology Journal Database, and two clinical trial registries, were searched. All randomized controlled trials (RCTs) related to EA intervention in cardiac surgery with CPB were collected. Based on the inclusion and exclusion criteria, two researchers independently screened articles and extracted data. After the quality evaluation, RevMan 5.3 software was used for analysis.
RESULTS:
Fourteen RCTs involving 836 patients were included. Compared with the control treatment, EA significantly increased the incidence of cardiac automatic rebeat after aortic unclamping [relative risk (RR) = 1.15, 95% confidence interval (CI) (1.01, 1.31), P < 0.05; moderate]. Twenty-four hours after aortic unclamping, EA significantly increased the superoxide dismutase [standardized mean difference (SMD) = 0.96, 95% CI(0.32, 1.61), P < 0.05; low], and interleukin (IL)-2 [SMD = 1.33, 95% CI(0.19, 2.47), P < 0.05; very low] expression levels and decreased the malondialdehyde [SMD =-1.62, 95% CI(-2.15, -1.09), P < 0.05; moderate], tumour necrosis factor-α [SMD = -1.28, 95% CI(-2.37, -0.19), P < 0.05; moderate], and cardiac troponin I [SMD = -1.09, 95% CI(-1.85, -0.32), P < 0.05; low] expression levels as well as the inotrope scores [SMD = -0.77, 95% CI(-1.22, -0.31), P < 0.05; high]. There was no difference in IL-6 and IL-10 expression levels. The amount of intraoperative sedative [SMD = -0.31, 95% CI(-0.54, -0.09), P < 0.05; moderate] and opioid analgesic [SMD = -0.96, 95% CI(-1.53, -0.38), P < 0.05; low] medication was significantly lower in the EA group than in the control group. Moreover, the postoperative tracheal intubation time [SMD = -0.92, 95% CI(-1.40, -0.45), P < 0.05; low] and intensive care unit stay [SMD = -1.71, 95% CI(-3.06, -0.36), P < 0.05; low] were significantly shorter in the EA group than in the control group. There were no differences in the time to get out of bed for the first time, total days of antibiotic use after surgery, or postoperative hospital stay. No adverse reactions related to EA were reported in any of the included studies.
CONCLUSIONS:
In cardiac surgery with CPB, EA may be a safe and effective strategy to reduce myocardial ischaemia-reperfusion injury and speed up the recovery of patients after surgery. These findings must be interpreted with caution, as most of the evidence was of low or moderate quality. More RCTs with larger sample sizes and higher quality are needed to provide more convincing evidence.
Keywords: electroacupuncture, cardiopulmonary bypass, thoracic surgery, myocardial ischaemia-reperfusion injury, myocardial protection, postoperative rehabilitation, Meta-analysis, randomized controlled trial
1. INTRODUCTION
In 1953, Gibbon completed the world’s first open-heart surgery with a vertical screen oxygenator and a roller pump.1 Since then, open-heart surgery has become an important way to treat heart disease because of its intuitive operation experience. Cardiopulmonary bypass (CPB) is an important method of open-heart surgery.2 However, according to statistics, the mortality or the rate of heart failure caused by myocardial ischaemia-reperfusion injury (MIRI) is 10% and 25%,3 which is the most important cause of heart failure and myocardial injury.4 MIRI after CPB has brought serious harm to patients, as it increases the morbidity and mortality of patients after open-heart surgery.5
Although the safety of CPB has been improved with the use of MIRI prevention and treatment drugs and the improvement of CPB equipment,6,7 it still cannot meet the actual clinical needs. The latest guidelines for CPB in adult cardiac surgery combined with the results of a Meta-analysis indicate that comparing crystalloid with blood cardioplegia, there was no difference between the groups regarding the rates of perioperative myocardial infarction and death. It is recommended to adopt a patient-centred myocardial protection strategy based on the patient's condition and the complexity of the operation.8 Therefore, new cardiac protection strategies are urgently needed to reduce the risk of MIRI.
In contrast with traditional acupuncture, electro-acupuncture (EA) involves the insertion of needles into acupoints and the introduction of an electrical current through that needle, thus combining electricity and the needle to enhance the stimulation by and effects of acupuncture.9 Acupuncture stimulates energy pathways through specific acupoints to rebalance "Qi" within body and organ systems, to regulate blood circulation and to affect physiological system function.10,11 Biological mechanisms such as central sensitization,12 neurotransmitters,13 immune regulation,14 oxidative stress,15 and inflammatory action16 may be involved. It has been proven to have certain effects in many aspects, such as postoperative or poststroke cognitive impairment,17,18 angina pectoris,19 emesis,20 etc. In addition, acupuncture had a lower incidence of adverse effects than other treatments or drugs. A systematic review related to EA intervention in cardiac surgery published in the Journal of Intensive Care Medicine in 2017,21 Meta-analysed the preliminary efficacy of EA in cardiac surgery. Evidence is limited, however, by the small number of included studies, additional types of heart surgery, and the lack of specificity. The current systematic review and Meta-analysis therefore aimed to evaluate the efficacy of EA for myocardial protection and postoperative rehabilitation in patients after MIRI.
2. METHODS
2.1. Research registration
We registered our agreement with INPLASY PROTOCOL (202140045), an international forwards-looking systematic review registration (www.inplasy.com). According to the Cochrane manual for systematic reviews22 and based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), full-text reports were examined (supplementary Table 1).23
2.2. Search strategy
The two authors (QIN Xiaoyu and ZHANG Jie) searched the PubMed, Embase, Cochrane Library, Web of Science, Chinese Biomedical Literature Database (CBM), China National Knowledge Infrastructure Database (CNKI), Wanfang Database, and China Science and Technology Journal Database (VIP), as well as the Chinese Clinical Trial Registry (www.chictr.org.cn) and the North American Clinical Trial Registry (www.clinicaltrials.gov). All randomized controlled trials (RCTs) related to EA intervention in cardiac surgery with CPB were collected. The time limit was from the establishment of the database to February 7, 2021. The last search was conducted on May 24, 2022. The keywords in the retrieval strategy were electro-acupuncture, acupuncture, acupuncture therapy, cardiac surgical procedures, coronary artery bypass, cardiopulmonary bypass, and RCTs. The detailed search strategy for each database is given in supplementary Table 2.
2.3. Eligibility criteria
When the study met the following inclusion criteria, it was used for further analysis: (a) study design: RCTs; (b) participants: patients undergoing cardiac surgery with CPB; (c) intervention: patients receiving only EA therapy before or during surgery; (d) control: patients receiving sham EA or no intervention; (e) outcomes: the primary outcome measures were the indicators related to myocardial damage. These included the incidence of cardiac automatic rebeat after aorta unclamping; oxidative stress indicators: superoxide dismutase (SOD), malondialdehyde (MDA); inflammatory factor indicators: interleukin (IL)-2, IL-6, IL-10, tumour necrosis factor (TNF)-α; myocardial injury markers: cardiac troponin I (cTnI); and inotrope scores. We extracted the data of each index 24 h after aorta unclamping. The secondary outcome indicators were intraoperative anaesthetic drug usage and postoperative general conditions. These included sedatives: propofol, midazolam, etomidate; opioid analgesics: fentanyl, sufentanil, remifentanil; postoperative tracheal intubation time; the time to get out of bed for the first time; the total days of antibiotic use after surgery; intensive care unit (ICU) stay; postoperative hospital stay.
The following types of studies were excluded: (a) studies that included some patients who underwent cardiac surgery without CPB or for whom there was insufficient information to determine whether a procedure was performed with CPB; (b) studies of patients with severe systemic diseases; (c) studies not published in English or Chinese.
For the same research results that could be searched in both dissertations and journals, we choose to include the journal papers. If the journal paper had insufficient information on the outcome indicators we were interested in, we used the dissertation as a supplement. Some outcome indicators in the previous registration scheme had no summary analysis conducted because none of the eligible studies reported on it or only one study reported on it. These indicators included the free radical nitric oxide (NO), IL-8, lactate dehydrogenase (LDH), creatine kinase-MB (CK-MB), arrhythmia score, and EA-related adverse reactions. Nevertheless, intraoperative anaesthetic drug usage and postoperative rehabilitation-related indicators were newly added to better evaluate the overall benefits of EA for patients during the entire perioperative period.
2.4. Screening and data extraction
We used EndNote X9 software (Thomson Corp, Stanford, CT, USA) to manage the retrieved records. Two reviewers independently screened the title and abstract of each record based on the qualification criteria and reviewed the full text of potentially related studies. Disagreements were resolved through discussion or consultation with a third reviewer. Microsoft Excel (Microsoft Corp, Redmond, WA, USA) was used to collect the following information: research characteristics (first author, year of publication, and research source), population characteristics (age, sample size, American Society of Anaesthesiologists classification, cardiac function classification, type of operation), bypass conditions (CPB time, aortic clamping time), intervention details (frequency and intensity of EA, selection of acupuncture points) and results of interest. Two reviewers (QIN Xiaoyu and LU Xiaoting) independently extracted the data and discussed them with another author (WANG Chunai) to resolve any differences.
2.5. Risk of bias assessment
The risk of bias for the included RCTs was assessed independently by two researchers (QIN Xiaoyu and DING Shengshuang) based on Cochrane risk-of-bias criteria,24 and each quality item was graded as low risk, high risk, or unclear risk. The seven items used to evaluate bias in each trial included randomization sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases (baseline imbalances, conflicts of interest, etc.). The risk of bias for each item was assessed based on the following criteria:24 (a) If the methodology of the relevant items reported in the research was correct or the risk of bias did not affect the research results, it was judged as "low risk". The reliability of the findings would not be affected. (b) If there was a methodological error in the content of the relevant items reported in the study, this would lead to a greater risk of bias, which was judged as "high risk". The credibility of the findings would be severely weakened. (c) If the relevant item content information reported in the research was incomplete, it was judged as "unclear risk". The findings may be suspect due to potential bias. The conflict was resolved through discussion with another author (GE Long).
2.6. Certainty of the evidence
We used the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) method to rate the quality of the evidence, which divided the evidence into high, medium, low, and very low levels.25 The starting point of randomized controlled trials is very high, but due to serious research limitations, inconsistencies, imprecision, indirectness, and publication bias, it may be reduced.
2.7. Data synthesis and analysis
All data were Meta-analysed under the random-effects model. Relative risk (RR) and standardized mean difference (SMD) were calculated for binary data and continuous data. The 95% confidence interval (95% CI) was also provided. Statistical heterogeneity between summary data was evaluated using the I 2 statistic. Sensitivity analysis to find sources of heterogeneity and evaluate the robustness of findings was conducted. To evaluate the effect of EA on the use of each anaesthetic drug, we specified subgroups based on the different drugs. Statistical analysis was performed using Review Manager (RevMan) version 5.3 (The Nordic Cochrane Centre, Rigshospitalet, Copenhagen, Denmark). All comparisons were 2-tailed using a threshold P ≤ 0.05.
We tried to convert and unify the data units extracted from the same indicator before merging. For some documents that provided data in chart format, we contacted the corresponding author, and in cases of failure, Engauge Digitizer version 9.8 software (Markmitch, Torrance, CA, USA) was used to extract the data. For some data provided in the median or mean ± standard error format, we converted it into the mean ± standard deviation before entering.26,27 To determine whether the current sample was sufficient in our Meta-analysis, PASS version 15 software (NCSS, LLC, Kaysville, UT, USA) was used to estimate the optimal information size (OIS) based on the given data.28
3. RESULTS
3.1. Identification of relevant studies
The systematic search identified 3843 documents, of which 2333 were from the Chinese database, 1503 were from the English database, and 7 were from the website of the Chinese Clinical Trial Registry (ChiCTR; www.chictr.org.cn) and ClinicalTrials.gov, as well as references and related systematic reviews of qualified documents. A total of 836 patients in 17 articles29,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓-45 (14 RCTs) proved to be eligible (Figure 1). Among these publications, 13 articles29,31,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓-40,42,44 were published in Chinese (including 2 dissertations31,33), and 4 articles30,41,43,45 were published in English.
Figure 1. Flow diagram of the study selection.
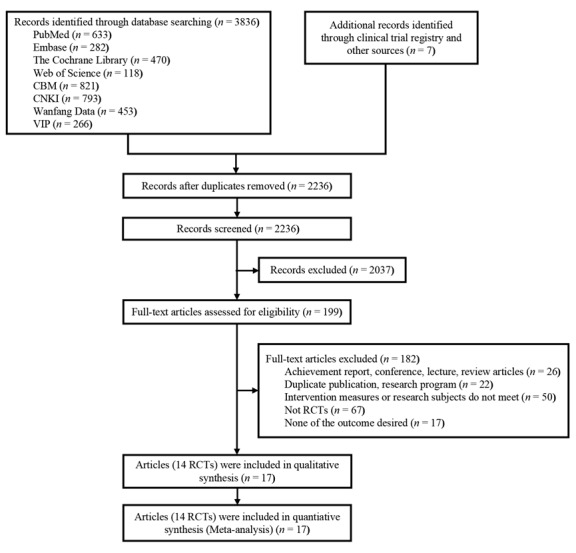
CBM: Chinese biomedical literature database; CNKI: China national knowledge infrastructure database; VIP: China science and technology journal database; RCTs: randomized controlled trials.
3.2. Characteristics of the included studies
Fourteen studies29,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓-45 were published between 1999 and 2020, all of which came from China. The sample size involved in the study ranged from 20 to 200. Two subjects30,42 included in the study were paediatric patients, and the subjects of the remaining studies29,31,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓-41,43,⇓-45 were adults, with a mean age between 3.45 and 53.8 years old. The intervention measures included in the study were all EA interventions. Four studies30,36,42,⇓-44 in the control group used sham EA, and the remaining studies29,31,⇓,⇓,⇓-35,37,⇓,⇓,⇓-41,45 were blank controls with conventional general anaesthesia. Four studies30,36,41,43,44 reported that EA treatment was carried out by experienced acupuncturists or trained anaesthesiologists. The time of EA treatment reported in 2 studies40,41 was once a day for five consecutive days before surgery, and the patients in the remaining studies29,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓-39,42-45 were treated after entering the operating room. The frequencies of EA were mostly 3-4 Hz and 2/100 Hz. The Neiguan (PC6) point was the most selected acupuncture point, which was selected in 11 studies.29,⇓,⇓,⇓,⇓,⇓-35,39,⇓,⇓,⇓,⇓ - 44 Ten studies30,⇓-32,34,⇓,⇓,⇓,⇓,⇓,⇓-41,45 were funded by government departments, and 4 studies29,33,42,⇓-44 did not report any funding information. Five studies30,36,40,41,43,44 registered their research protocols. Table 1 summarizes the detailed characteristics of the included studies.
Table 1.
Characteristics of the included trials
| Study | Number of patients | Age (years) | Heart function degree | Operation type | EA parameter | Acupoint | Outcome | ||
|---|---|---|---|---|---|---|---|---|---|
| EA | Control | ||||||||
| Ma FG et al 201529 | 50 | 45±16 | 46±15 | Ⅱ-Ⅲ | Valve replacement | Sparse-dense wave at a frequency of 2/100 Hz. The intensity is 2.34-6.24 mA, adjusted according to the patient's tolerance. | PC6 | Incidence of cardiac automatic rebeat, SOD, MDA, cTnI | |
| Ni XL et al 201230 | 70 | 3.95 | 3.45 | Unreported | Repair of congenital heart disease | Sparse-dense wave at a frequency of 2/100 Hz. The intensity is 14±3 mA. | PC6 | IL-6, IL-10, TNF-α, cTnI, Sedative drug usage, analgesic usage, tracheal intubation time, length of ICU stay, length of hospital stay | |
| Shan JG 2009;31 Shan JG et al 201032 | 30 | 31.1±15.7 | 32.5±13.6 | Unreported | Valve replacement, septal defect repair, incision of pulmonary stenosis | Sparse-dense wave at a frequency of 2/100 Hz. The intensity is adjusted according to the patient's tolerance. | PC6, LU7, LU2 | Incidence of cardiac automatic rebeat, IL-2, IL-10, TNF-α, total days of antibiotic use, Length of ICU stay, length of hospital stay | |
| Tao YY 200933 | 23 | 31.8±13.6 | 35.9±8.5 | Ⅱ-Ⅲ | Valve replacement, septal defect repair, septal defect repair and valvuloplasty | Sparse-dense wave at a frequency of 2/100 Hz. The intensity is 1-3 mA. | PC6, LU7, LU2 | Incidence of cardiac automatic rebeat, cTnI, sedative drug usage, analgesic usage, Tracheal intubation time, length of ICU stay | |
| Wang XR et al 199934 | 28 | 27.4±8.9 | 28.9±10.1 | Ⅰ-Ⅱ | Septal defect repair | The frequency is 3-4 Hz and the intensity is 0.5-1 mA. | PC6, LU7, LU2 | Incidence of cardiac automatic rebeat | |
| Wang YQ et al 201235 | 40 | 42.5 ± 6.5 | 43.3±6.8 | Ⅱ-Ⅲ | Valve replacement | The frequency is 3-4 Hz and the intensity is adjusted according to the patient's tolerance. | PC6, LU7, LU2 | SOD, MDA | |
| Wang Y et al 201936 | 60 | 44±4 | 45±5 | Ⅱ-Ⅲ | Valve replacement | Sparse-dense wave at a frequency of 2/15 Hz. the intensity is 1 mA. | GV20, EX-HN3, GV26 | IL-6, IL-10, TNF-α, length of ICU stay, length of hospital stay | |
| Wu DQ et al 2018;37 Wu DQ et al 201938 | 40 | 48±10.4 | 47.4±10.4 | Unreported | Valve replacement | Sparse-dense wave at a frequency of 2/100 Hz. The intensity is 1-24 mA, adjusted according to the patient's tolerance. | LI4, LI11, ST36, SP9 | Sedative drug usage, analgesic usage, tracheal intubation time, length of ICU stay | |
| Yang QG et al 200639 | 20 | 31.3±7.6 | 31.8±11.5 | Unreported | Septal defect repair | The frequency is 3-4 Hz and the intensity is adjusted according to the patient's tolerance. | PC6, LU7, LU2 | IL-2, IL-6, IL-10 | |
| Yang LF et al 200940 | 75 | 50±4 | 51±6 | Ⅱ-Ⅲ | Valve replacement, coronary artery bypass grafting | Sparse-dense wave at a frequency of 5-6/25-30 Hz. The intensity is 2.34-6.24 mA, adjusted according to the patient's tolerance. | PC6, LU7, LU2 | Incidence of cardiac automatic rebeat, Sedative drug usage, analgesic usage, length of hospital stay | |
| Yang YL et al 202042 | 100 | 6.9±2.4 | 7.3±2.2 | Unreported | Repair of tetralogy of fallot | Sparse-dense wave at a frequency of 2/100 Hz. The intensity is 6 mA, | GV20, PC6, LI4, PC4 | IL-6, TNF-α, analgesic usage, tracheal intubation time, length of ICU stay, hospital stay | |
| Zhang FX et al 2017;43 Xiao H et al 201844 | 40 | 44±6 | 47±5 | Ⅱ-Ⅲ | Valve replacement | Sparse-dense wave at a frequency of 2/100 Hz. The intensity is 0.5-1.2 mA, adjusted according to the patient's tolerance. | PC6, PC4, GV24, GV20 | Incidence of cardiac automatic rebeat, MDA, cTnI, inotrope scores, sedative drug usage, analgesic usage, tracheal intubation time, time to get out of bed for the first time, length of ICU stay, length of hospital stay | |
| Zhou J et al 201145 | 200 | 51.3 | 53.8 | Ⅰ-Ⅲ | Repair of congenital heart disease, valve replacement, valvuloplasty | The frequency is 3-4 Hz and the intensity is adjusted according to the patient's tolerance. | LU1, LU7, PC4 | Time to get out of bed for the first time, total days of antibiotic use, length of ICU stay, length of hospital stay | |
Notes: EA: electroacupuncture; SOD: superoxide dismutase; MDA: malondialdehyde; TNF: tumour necrosis factor; cTnI: cardiac troponin I; IL: interleukin; ICU: intensive care unit; LU1: Zhongfu; PC4: Ximen; PC6: Neiguan; LU7: Lieque; LU2: Yunmen; GV20: Baihui; EX-HN3: Yintang; GV24: Shenting; GV26: Renzhong; LI4: Hegu; LI11: Quchi; ST36: Zusanli; SP9: Yinlingquan.
3.3. Risk of bias and quality of evidence
Among the 14 included studies, 6 studies29,⇓,⇓-32,36,42,⇓-44 (43%) adopted the correct random sequence generation method, and 3 studies30,41,43,44 (21%) carried out adequate allocation concealment. Since the outcomes we included were all objective indicators, according to the principles of the Cochrane Manual,15 14 studies29,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓-45 (100%) were rated as low risk in both the blinding of participants and the blinding of outcome assessment; 13 studies29,⇓,⇓,⇓-33,35,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓-45 (93%) had complete outcome data. None of the 14 studies29,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓,⇓-45 (100%) found selective reporting bias. Four studies30,36,42,⇓-44 (29%) declared no conflicts of interest, and no other biases were found (Figure 2, supplementary Table 3). The certainty of evidence evaluated by GRADE is shown in Table 2. The certainty of the evidence was mostly rated as moderate or low for all the outcomes. The most common reason was the risk of bias due to an inadequately generated randomization sequence and concealment, blinding or selective reporting of outcomes.
Figure 2. Risk of bias graph.
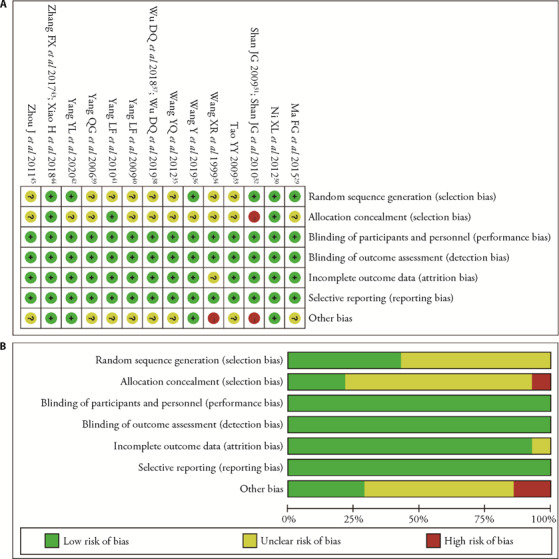
A: risk of bias in all included studies; B: risk of bias summary.
Table 2.
GRADE evidence profile of EA vs control cardiac surgery with cardiopulmonary bypass
| Outcome | No. of studies | No. of patients | Quality assessment | Relative effect (95% CI) | Quality | ||||
|---|---|---|---|---|---|---|---|---|---|
| Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | |||||
| Incidence of cardiac automatic rebeat | 7 | 306 | Seriousa | None | None | None | None | RR 1.15 (1.01, 1.31) | Moderate |
| Oxidative stress indicators (SOD) | 2 | 90 | Seriousa | Seriousb | None | None | None | SMD 0.96 (0.32, 1.61) | Low |
| Oxidative stress indicators (MDA) | 3 | 130 | Seriousa | None | None | None | None | SMD -1.62 (-2.15, -1.09) | Moderate |
| Inflammatory factor indicators (IL-2) | 2 | 50 | Seriousa | Seriousb | None | Seriousc | None | SMD 1.33 (0.19, 2.47) | Very low |
| Inflammatory factor indicators (IL-6) | 4 | 250 | None | Seriousb | None | None | None | SMD -0.69 (-1.43, 0.05) | Moderate |
| Inflammatory factor indicators (IL-10) | 4 | 180 | Seriousa | Seriousb | None | Seriousc | None | SMD 0.65 (-0.01, 1.32) | Very low |
| Inflammatory factor indicators (TNF-α) | 4 | 260 | None | Seriousb | None | None | None | SMD -1.28 (-2.37, -0.19) | Moderate |
| Myocardial injury markers (cTnI) | 5 | 243 | Seriousa | Seriousb | None | None | None | SMD -1.09 (-1.85, -0.32) | Low |
| Inotrope scores | 2 | 100 | None | None | None | None | None | SMD -0.77 (-1.22, -0.31) | High |
| Sedative drug usage | 12 | 586 | Seriousa | None | None | None | None | SMD -0.31 (-0.54, -0.09) | Moderate |
| Sedative drug usage (propofol) | 5 | 238 | Seriousa | Seriousb | None | None | None | SMD -0.28 (-0.78, 0.23) | Low |
| Sedative drug usage (midazolam) | 6 | 308 | Seriousa | None | None | None | None | SMD -0.33 (-0.57, -0.09) | Moderate |
| Sedative drug usage (etomidate) | 1 | 40 | Seriousa | None | None | Seriousc | None | SMD -0.36 (-0.99, 0.27) | Low |
| Analgesic usage | 8 | 448 | Seriousa | Seriousb | None | None | None | SMD -0.96 (-1.53, -0.38) | Low |
| Analgesic usage (fentanyl) | 4 | 228 | Seriousa | Seriousb | None | None | None | SMD -0.78 (-1.72, 0.15) | Low |
| Analgesic usage (sufentanil) | 3 | 180 | Seriousa | None | None | None | None | SMD -0.98 (-1.29, -0.67) | Moderate |
| Analgesic usage (remifentanil) | 1 | 40 | Seriousa | None | None | Seriousc | None | SMD -1.91 (-2.67, -1.15) | Low |
| Tracheal intubation time | 6 | 333 | Seriousa | Seriousb | None | None | None | SMD -0.92 (-1.40, -0.45) | Low |
| Time to get out of bed for the first time | 2 | 240 | Seriousa | Seriousb | None | Seriousc | None | SMD -6.58 (-18.70, 5.53) | Very low |
| Total days of antibiotic use | 2 | 230 | Seriousa | Seriousb | None | Seriousc | None | SMD -3.13 (-6.89, 0.63) | Very low |
| Length of ICU stay | 9 | 623 | Seriousa | Seriousb | None | None | None | SMD -1.71 (-3.06, -0.36) | Low |
| Length of hospital stay | 8 | 635 | Seriousa | Seriousb | None | Seriousc | None | SMD -0.71 (-1.56, 0.14) | Very low |
Notes: EA: electroacupuncture; GRADE: Grades of Recommendation, Assessment, Development, and Evaluation; SMD: standardized mean difference; RR: relative risk; CI: confidence interval. GRADE Working Group grades of evidence: high quality: we are very confident that the true effect lies close to that of the estimate of the effect; moderate quality: we are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of effect. aQuality was rated down for risk of bias due to inadequately generated randomization sequence, inadequate concealment and blinding, or selectively report of outcomes; bModerate or severe heterogeneity (> 50% heterogeneity); cThe total sample size is insufficient or the outcome is not robust.
3.4. Meta-analysis
Related indicators of myocardial injury: (a) Incidence of cardiac automatic rebeat: After aorta unclamping, compared with the control group, EA significantly increased the incidence of cardiac automatic rebeat29,31,⇓,⇓-34,40,41,43,44 [RR = 1.15, 95% CI (1.01, 1.31), P < 0.05; moderate] (Figure 3A); (b) Oxidative stress indicators: 24 h after aorta unclamping, the SOD expression level29,35 [SMD = 0.96, 95% CI (0.32, 1.61), P < 0.05; low] was higher in the EA group than in the control group (Figure 3B), and the MDA expression level29,35,43,44 in the EA group [SMD = -1.62, 95% CI (-2.15, -1.09), P < 0.05; moderate] was lower than that in the control group (Figure 3C). (c) Inflammatory factor indicators: Twenty-four hours after aortic unclamping, compared with the control treatment, EA significantly increased the IL-2 expression level31,32,39 [SMD = 1.33, 95% CI (0.19, 2.47), P < 0.05; moderate] (Figure 3D) and reduced the TNF-α expression level30,⇓-32,36,42 [SMD = -1.28, 95% CI (-2.37, -0.19), P < 0.05; moderate] (Figure 3E). There was no significant difference in IL-630,36,39,42 [SMD = -0.69, 95% CI (-1.43, 0.05), P > 0.05; moderate] (Figure 3F) or IL-1030,⇓-32,36,39 [SMD = 0.65, 95% CI (-0.01, 1.32), P > 0.05; very low] expression levels between the EA and control groups (Figure 3G). (d) Myocardial injury markers: Twenty-four h after aortic unclamping, the cTnI expression level29,30,33,41,43,44 [SMD = -1.09, 95% CI (-1.85, -0.32), P < 0.05; low] was lower in the EA group than in the control group (Figure 3H). (e) Inotrope scores: Twenty-four hours after aortic unclamping, compared with the control treatment, EA significantly reduced the inotrope scores41,43,44 [SMD = -0.77, 95% CI (-1.22, -0.31), P < 0.05; high] (Figure 3I). (Postoperative myocardial contractility score:41,43,44 μg·kg-1·min-1 as the unit, calculation formula: dopamine × 1 + dobutamine × 1 + amrinone × 1 + milrinone × 15 + epinephrine × 100 + norepinephrine × 100 + isoproterenol × 100.)
Figure 3. Comparison of related indicators of myocardial injury between the EA and control groups.
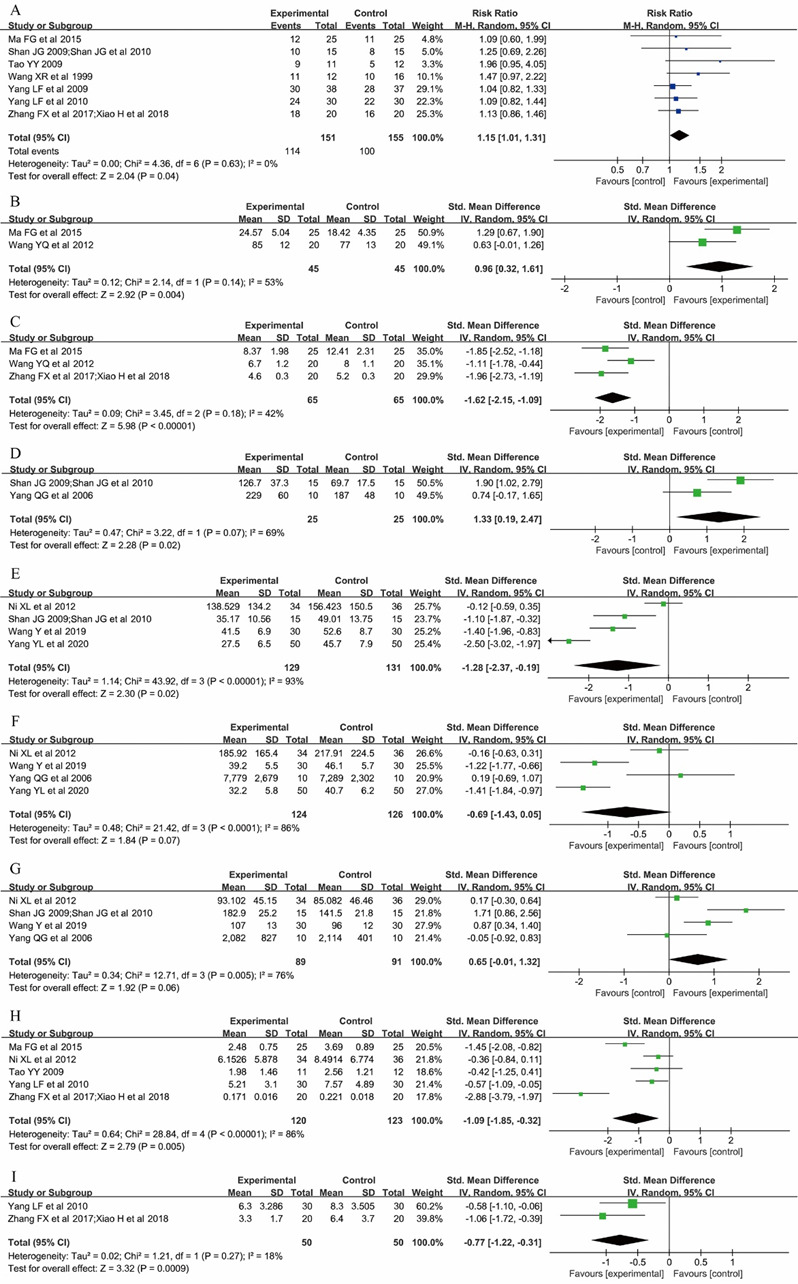
A: the incidence of cardiac automatic rebeat; B: the SOD expression level 24 h after aorta unclamping; C: the MDA expression level 24 h after aorta unclamping; D: IL-2 expression level 24 h after aortic unclamping; E: TNF-α expression level 24 h after aortic unclamping. F: IL-6 expression level 24 h after aortic unclamping; G: IL-10 expression level 24 h after aortic unclamping; H: cTnI expression level 24 h after aortic unclamping; I: inotrope scores 24 h after aortic unclamping. EA: electroacupuncture; SOD: superoxide dismutase; MDA: malondialdehyde; IL: interleukin; TNF: tumour necrosis factor; cTnI: cardiac troponin I.
Intraoperative anaesthetic drug usage: In the EA group, the dosages of the intraoperative sedative30,33,37,38,40,41,43,44 [SMD = -0.31, 95% CI (-0.54, -0.09), P < 0.05; moderate] (Figure 4A) and opioid analgesics30,33,37,38,40,⇓,⇓,⇓-44 [SMD = -0.96, 95% CI (-1.53, -0.38), P < 0.05; low] were less than those in the control group (Figure 4B).
Figure 4. Comparison of the intraoperative anaesthetic drug usage between the EA and control groups.
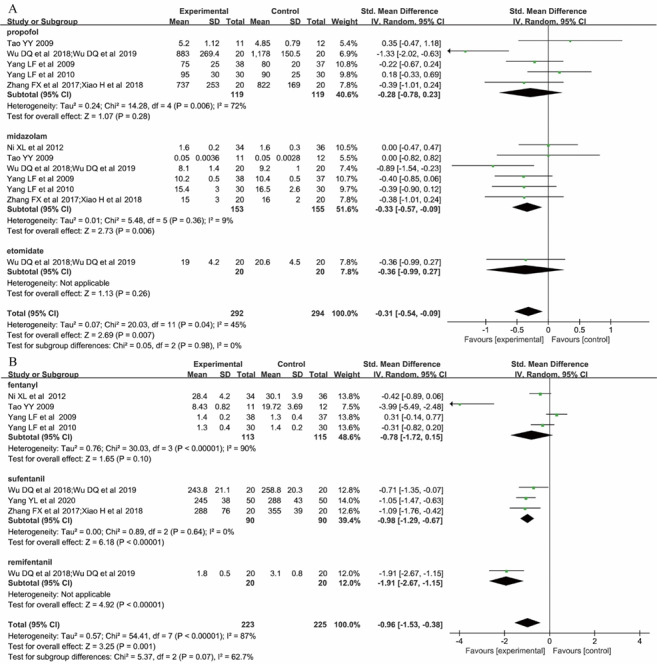
A: intraoperative sedative usage; B: intraoperative opioid analgesic usage. EA: electroacupuncture.
Outcome of postoperative rehabilitation: Compared with the control group, EA significantly reduced the postoperative tracheal intubation time30,33,37,38,41,⇓,⇓-44 [SMD = -0.92, 95% CI (-1.40, -0.45), P < 0.05; low] (supplementary Figure 1A) and ICU stay30-33,36,⇓-38,41,⇓,⇓-44 [SMD = -1.71, 95% CI (-3.06, -0.36), P < 0.05; low] (supplementary Figure 1B). There were no significant differences between EA and the control group in the time to get out of bed for the first time43,⇓-45 [SMD = -6.58, 95% CI (-18.70, 5.53), P > 0.05; very low] (supplementary Figure 1C), the total days of antibiotic use after surgery31,32,45 [SMD = -3.13, 95% CI (-6.89, 0.63), P > 0.05; very low] (supplementary Figure 1D) and the postoperative hospital stay30,⇓-32,36,40,⇓,⇓,⇓,⇓-45 [SMD = -0.71, 95% CI (-1.56, 0.14), P > 0.05; very low] (supplementary Figure 1E).
3.5. OIS calculation
The OIS was calculated to explore whether the cumulative data of each result were adequate. For the outcome, if the sample size was insufficient, its level would be lowered by one level in the GRADE evidence quality rating due to its serious imprecision.
3.6. Subgroup analysis
Subgroup analyses were conducted for intraoperative anaesthetic usage according to the different drugs. The pooled results indicated that EA significantly reduced midazolam30,33,37,38,40,41,43,44 [SMD = -0.33, 95% CI (-0.57, -0.09), P < 0.05; moderate] and sufentanil37,38,42,⇓-44 [SMD = -0.98, 95% CI (-1.29, -0.67), P < 0.05; moderate] usage. There were no significant differences between EA and the control group in terms of propofol33,37,38,40,41,43,44 [SMD = -0.28, 95% CI (-0.78, 0.23), P > 0.05; low] and fentanyl30,33,40,41 [SMD = -0.78, 95% CI (-1.72, 0.15), P > 0.05; low] usage.
3.7. Sensitivity analysis
Sensitivity analysis demonstrated the robustness of the results of the incidence of cardiac automatic rebeat, oxidative stress indicators, inflammatory factor indicators (IL-2, TNF-α), myocardial injury markers, inotrope scores, intraoperative anaesthetic drug usage, and the outcome of postoperative rehabilitation (postoperative tracheal intubation time, ICU stay time) using RE vs FE (supplementary Figures 2-12).
4. DISCUSSION
Our Meta-analysis revealed that the effectiveness of EA was better than that of the control treatment in reducing MIRI during CPB. This may be related to the ability of EA to reduce oxidative stress and inflammation after reperfusion. In addition, the dosages of anaesthetics, postoperative intubation time and ICU stay of patients were also reduced. Although EA has shown certain advantages, the results of some indicators were not stable due to the few studies included. These indicators included the expression levels of IL-2 and IL-10 24 h after aorta unclamping, as well as the time to get out of bed for the first time and total days of antibiotic use after surgery. In addition, there was a high degree of heterogeneity in the results of some Meta-analyses. Although the method of elimination one by one was used to find the source of heterogeneity, a significant decrease in heterogeneity was not found after a single study was excluded (I 2 ≤ 50%). The reason may be related to the differences in the frequency and stimulation intensity of EA in different studies.46,47
Two previous Meta-analyses analyzed the influence of EA on myocardial protection.21,48 The results of a basic research Meta-analysis showed that EA treatment reduced the myocardial infarct size and the expression of cTnI and CK-MB in rats with MIRI, proving the myocardial protective effect of EA in this disease model.48 However its clinical applicability is limited since clinical studies were not included. Another Meta-analysis showed that EA reduced the expression of cTnI and TNF-α after cardiac surgery, reduced the dose of intraoperative sedative drugs and postoperative vasoactive drugs, and shortened the postoperative tracheal intubation and ICU hospitalization time.21 This finding is basically consistent with the results of our study. However, the study showed that EA can increase the expression of the anti-inflammatory factor IL-10 without reducing the use of intraoperative opioid analgesics, which is contrary to our findings in this review. Only seven articles were included in the study, and the authors' inclusion criteria were all cardiac procedures, including those performed without cardiopulmonary bypass.
In this umbrella evaluation, we analysed 16 evaluation indicators. The effects of EA on the use of intraoperative anaesthetics, postoperative myocardial injury and rapid recovery in cardiac surgery with cardiopulmonary bypass were discussed. There was one outcome supported by high evidence, five outcomes supported by moderate evidence, five outcomes supported by low evidence, and five associations supported by very low evidence. In light of the existing evidence, EA provides effective adjunctive analgesia. It could reduce the use of intraoperative anaesthetics, and the evidence was low to moderate. The clinical practice guidelines formulated by our team in the early stage recommend that EA can also be used as a method for postoperative multimodal analgesia to better improve pain.49 In addition to mechanical damage during surgery, CPB was the main cause of myocardial injury.50 The myocardial protective effect of EA is of great significance for CPB surgery. EA significantly reduced postoperative oxidative stress, inflammatory cytokines and cTnI expression and increased the incidence of cardiac automatic rebeat after aortic unclamping, but the quality of the evidence ranged from very low to moderate. Nonetheless, this does not mean the conclusion is wrong. At present, the biological mechanism of acupuncture's protective effect on MIRI has been proposed by numerous studies.51,⇓-53 A more important finding in our study was that EA treatment accelerated postoperative recovery, especially in terms of reduced postoperative tracheal intubation and shorter ICU hospitalization, and the quality of evidence was rated as low. This further reduced the incidence of complications for patients in the ICU. By providing evidence-based information for the application of acupoint stimulation in fast-recovery surgery, our results may give cardiac surgery patients and health care workers new insights into clinical practice.
Although the EA treatment protocols used in different studies vary widely, the included randomized controlled trials show that the Neiguan (PC6), Lieque (LU7), and Yunmen (LU2) points were the most commonly used acupoints for cardiac surgery under cardiopulmonary bypass. According to the meridian system of acupuncture based on TCM, the Neiguan (PC6) acupoint can regulate functions, activate blood and dredge collaterals and is a special acupoint for the treatment of heart disease. Acupuncture at the Neiguan (PC6) acupoint could regulate the excitability of the central nervous system, regulate the production and release of biologically active substances, and change the response mode of cardiomyocytes. It can improve acute myocardial ischaemia, myocardial ischaemia-reperfusion injury and chronic myocardial ischaemia.54 In addition, basic research has also shown that EA at Neiguan (PC6) or Lieque (LU7) can affect the expression of protein kinase in myocardial cells in rats with myocardial ischaemia and play a role in protecting the myocardium, but the efficacy of acupuncture at Lieque (LU7) is inferior to that of acupuncture at Neiguan (PC6).55 The effects of EA also depend on current parameters (frequency, intensity, and duration of pulses).56 In the included studies in our Meta-analysis, most of the EA parameters used low-frequency stimulation or a combination of high- and low-frequency sparse and dense waveforms. Basic research has shown that the high frequency group (100 Hz) is more able to reduce myocardial reperfusion injury than the low frequency group (2 Hz).57 However, this is contrary to the findings of Shi et al.58 Although EA has brought benefits to surgical patients, there is no international unified standard for the selection criteria of acupoint compatibility, parameter selection and treatment time. These problems have limited the application and popularization of Traditional Chinese Medicine (TCM) acupoint stimulation technology in the perioperative period to a certain extent, and they are also challenges faced by clinicians. More research is needed to provide an accurate and objective basis for the perioperative application of EA.
The mechanism of EA preconditioning on myocardial protection is not fully understood, but optimistic research results are being confirmed by some limited studies. Animal experiments showed that compared with the control treatment, EA reduced the levels of myocardial injury markers, myocardial cell apoptosis, oxidative stress, and inflammation. The protective effect of EA on myocardial injury after CPB may be achieved by restoring the apelin/APJ signalling pathway.59 Another study found that acupuncture preconditioning had a certain protective effect on MIRI. The mechanism may be related to upregulating the expression of the Nrf 2-ARE pathway, activating the endogenous antioxidant pathway, improving the scavenging ability of oxygen free radicals, and reducing lipid peroxidation damage.60 During myocardial ischaemia, the generation of free radicals increases, and the activity of antioxidant enzymes decreases.61 The production of oxygen free radicals is an important cause of MIRI, which can cause severe damage to myocardial cells and even apoptosis.62 The decrease in superoxide dismutase (SOD) activity in myocardial cells in the ischaemic area means that the body's ability to scavenge oxygen free radicals has decreased.63 At the same time, the content of malondialdehyde (MDA) in the myocardial cells of the ischaemic area increases, and the degree of lipid peroxidation in the cells also increases.64 Antioxidant interventions, such as scavenging reactive oxygen free radicals, can help reduce tissue ischaemia‒reperfusion injury.65 EA can affect the reactive oxygen species (ROS) content, SOD activity, and MDA content through the p38 MAPK signalling pathway to reduce MIRI.66 cTnI is a specific molecular marker of cardiomyocytes and an important regulatory protein involved in cardiomyocyte contraction. Its specificity and sensitivity are better than those of serum enzymatic indicators, and it can be used to detect the degree of cardiomyocyte damage.67 An increase in cTnI levels after surgery indicates myocardial injury and a poor prognosis.68 Studies have found that the content of cTnI decreases after EA intervention, and the myocardial damage caused by MIRI is reduced.69,⇓-71 Inflammation plays an important role in the process of myocardial ischaemia and reperfusion. During the period of ischaemia-reperfusion, leucocytes (mainly neutrophils) increase significantly, and the more infiltration there is, the more serious the damage to myocardial tissue. Activated neutrophils can release a large number of inflammatory substances, causing damage to themselves and vascular endothelial cells.72 In a mouse lung ischaemia-reperfusion model, the ERK1/2 pathway has been shown to trigger Egr-1 expression and subsequent inflammatory damage.73 Studies have shown that EA stimulation of the Neiguan (PC6) point can significantly reduce the upregulation of Egr-1 and ERK1/2 induced by myocardial ischaemia/reperfusion.74 Research by Li et al 75 demonstrated that EA preconditioning can significantly improve the cardiac function of rats after myocardial ischaemia-reperfusion, reduce the infarct size, and reduce inflammatory factors. Through the comparison of gene expression quantitative detection methods, it was found that this protective effect may be produced by regulating the FXR/SHP apoptosis signalling pathway. EA preconditioning can also enhance the electrical activity of the vagus nerve while inhibiting the discharge of sympathetic nerves, thereby exerting a synergistic regulatory effect to improve acute myocardial ischaemia.76
As early as 1980, the World Health Organization recommended acupuncture as an analgesic-based treatment for neuromusculoskel et al diseases in the World Health Acupuncture Special.77 EA may block pain by activating a variety of bioactive chemicals through peripheral, spinal, and supraspinal mechanisms. These include opioids, which desensitize peripheral nociceptors and reduce proinflammatory cytokines peripherally and in the spinal cord, and serotonin and norepinephrine, which decrease spinal N-methyl-d-aspartate receptor subunit GluN1 phosphorylation. Additional studies suggest that EA, when combined with low dosages of conventional analgesics, provides effective pain management that can forestall the side effects of often debilitating pharmaceuticals.78 Although the mechanism of acupuncture analgesia is not fully understood, it has produced many beneficial effects during clinical application. In our study, it was found that when it is associated with general anaesthesia, it significantly reduces the dosage of intraoperative anaesthetics. The analgesic and sedative effects of EA have also been verified in other clinical studies.79,80
In the postoperative period, the tracheal intubation duration and ICU stay of patients in the EA group were significantly shortened, which may have reduced patient medical expenses and improved patient satisfaction with their medical treatment. In addition, the rapid recovery of cardiac surgery patients during the perioperative period was strengthened. It was difficult to draw a clear conclusion that EA was more effective than other therapies. EA has been widely used in China, and it relieves pain safely and effectively for many patients.81 Its mechanism and effects are worthy of further study.
In this comprehensive study, we screened a large amount of literature and evaluated multiple clinical results. Additionally, the OIS of each study was calculated, and the GRADE approach was used to evaluate the quality of the evidence. However, our study also has some limitations. First, our review included fewer documents, even though we searched eight databases and two clinical registries. The reference lists of related studies were manually searched to include all qualified randomized controlled trials. Second, the sample size of all studies was relatively small, which may lead to the summary still being inadequate. Third, since the results we are concerned about are all objective indicators, the blinding method of the result evaluator has almost no influence on the judgement of the result. Therefore, we did not consider the blinding method of outcome evaluation when we used the Cochrane risk bias tool to assess the risk of bias of a single study and the GRADE to assess the quality of the outcome evidence. Fourth, although we conducted a sensitivity analysis to find the source of heterogeneity, some factors were not evaluated due to limited data. Fifth, none of the studies reported any adverse reactions related to EA, and we have insufficient evidence on the safety of EA. Therefore, the current investigation results should be interpreted with caution.
In conclusion, this Meta-analysis showed that EA intervention can reduce MIRI after cardiac surgery with CPB and the dosage of intraoperative anaesthetics and accelerate the postoperative recovery of patients. In the future, more high-quality and large-sample RCTs are still needed to prove that EA can reduce MIRI.
5. SUPPORTING INFORMATION
Supporting data to this article can be found online at http://www.journaltcm.com.
REFERENCES
- 1. Cardoso TAAM, Kunst G, Neto CN, et al. Effect of sevoflurane on the inflammatory response during cardiopulmonary bypass in cardiac surgery: the study protocol for a randomized controlled trial. Trials 2021; 22: 25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Yan N, Yang W, Dong X, et al. Promotion of anoxia-reoxygenation-induced inflammation and permeability enhancement by nicotinamide phosphoribosyltransferase-activated MAPK signaling in human umbilical vein endothelial cells. Exp Ther Med 2017; 14: 4595-601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Zhao YL, Ao HS. Research progress of myocardial ischemia reperfusion injury. Zhong Guo Xun Huan Za Zhi 2011; 26: 396-8. [Google Scholar]
- 4. Snijder PM, de Boer RA, Bos EM, et al. Gaseous hydrogen sulfide protects against myocardial ischemia-reperfusion injury in mice partially independent from hypometabolism. PLoS One 2013; 8: e63291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Li KP, Zhang HY, Xu XD, Ming Y, Li TJ, Song ST. Recombinant human brain natriuretic peptide attenuates myocardial ischemia-reperfusion injury by inhibiting CD4+ T cell proliferation via PI3K/AKT/mTOR pathway activation. Cardiovasc Ther 2020; 1389312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Tang Y, Zhou G, Yao L, et al. Protective effect of Ginkgo biloba leaves extract, EGb761, on myocardium injury in ischemia reperfusion rats via regulation of TLR-4/NF-κB signaling pathway. Oncotarget 2017; 8: 86671-80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Zhou J, Zhou N, Wu XN, et al. Role of the Toll-like receptor 3 signaling pathway in the neuroprotective effect of sevoflurane preconditioning during cardiopulmonary bypass in rats. Mol Med Rep 2015; 12: 7859-68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Wahba A, Milojevic M, Boer C, et al. 2019 EACTS/EACTA/EBCP guidelines on cardiopulmonary bypass in adult cardiac surgery. Eur J Cardiothorac Surg 2020; 57: 210-51. [DOI] [PubMed] [Google Scholar]
- 9. Wu JL, Yu ZS, Wei QS, Li HL, Xing GY, Sun ZR. Influence of ‘combining medicine and engineering’ on reform of acupuncture and moxibustion’s needles. Zhong Hua Zhong Yi Yao Za Zhi 2018; 33: 5409-11. [Google Scholar]
- 10. Longhurst JC. Defining meridians: a modern basis of understanding. J Acupunct Meridian Stud 2010; 3: 67-74. [DOI] [PubMed] [Google Scholar]
- 11. Yang ES, Li PW, Nilius B, Li G. Ancient Chinese medicine and mechanistic evidence of acupuncture physiology. Pflugers Arch 2011; 462: 645-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Lyu Z, Guo Y, Gong Y, et al. The role of neuroglial crosstalk and synaptic plasticity-mediated central sensitization in acupuncture analgesia. Neural Plast 2021; 8881557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Li Y, Yang M, Wu F, et al. Mechanism of electroacupuncture on inflammatory pain: neural-immune-endocrine interactions. J Tradit Chin Med 2019; 39: 740-9. [PubMed] [Google Scholar]
- 14. Yu SG, Jing XH, Tang Y, et al. Acupuncture and moxibustion and immunity: the actuality and future. Zhen Ci Yan Jiu 2018; 43: 747-53. [DOI] [PubMed] [Google Scholar]
- 15. Zeng XH, Li QQ, Xu Q, Li F, Liu CZ. Acupuncture mechanism and redox equilibrium. Evid Based Complement Alternat Med 2014; 2014: 483294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Li N, Guo Y, Gong Y, et al. The anti-inflammatory actions and mechanisms of acupuncture from acupoint to target organs via neuro-immune regulation. J Inflamm Res 2021; 14: 7191-224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Qin XY, Zhang J, Ding SS, et al. Effects of electroacupuncture combined with general anesthesia on postoperative neurocognitive dysfunction and inflammatory factors in elderly patients: a Meta-analysis. World J Integr Tradit West Med 2022; 8: 19-28. [Google Scholar]
- 18. Zhan J, Wang XW, Cheng NF, Tan F. Electroacupuncture for post-stroke cognitive impairment: a systematic review and Meta-analyses. Zhong Guo Zhen Jiu 2017; 37: 1119-25. [DOI] [PubMed] [Google Scholar]
- 19. Liu Y, Liu P, Hou L, et al. Analysis of the effects of electroacupuncture at the pericardium 6 acupoint on heart function in patients with angina using equilibrium radionuclide angiocardiography quantity analysis technique. J Altern Complement Med 2014; 20: 466-71. [DOI] [PubMed] [Google Scholar]
- 20. Shen J, Wenger N, Glaspy J, et al. Electroacupuncture for control of myeloablative chemotherapy-induced emesis: a randomized controlled trial. JAMA 2000; 284: 2755-61. [DOI] [PubMed] [Google Scholar]
- 21. Asmussen S, Przkora R, Maybauer DM, et al. Meta-analysis of electroacupuncture in cardiac anesthesia and intensive care. J Intensive Care Med 2019; 34: 652-61. [DOI] [PubMed] [Google Scholar]
- 22. Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021). Cochrane, 2021. Available from www.training.cochrane.org/handbook.www.training.cochrane.org/handbook [Google Scholar]
- 23. Shamseer L, Moher D, Clarke M, et al. Preferred reporting items for systematic review and Meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ 2015; 350: g7647. [DOI] [PubMed] [Google Scholar]
- 24. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 2011; 343: d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol 2011; 64: 383-94. [DOI] [PubMed] [Google Scholar]
- 26. McGrath S, Zhao X, Steele R, Thombs BD, Benedetti A. DEPRESsion Screening Data (DEPRESSD) Collaboration. Estimating the sample mean and standard deviation from commonly reported quantiles in Meta-analysis. Stat Methods Med Res 2020: 962280219889080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Hu ZD. Standard deviation and standard error: two concepts that often confuse people. Lin Chuang Yu Bing Li Za Zhi 2015; 35: 2063-5. [Google Scholar]
- 28. Guyatt GH, Oxman AD, Kunz R, et al. GRADE guidelines 6. Rating the quality of evidence--imprecision. J Clin Epidemiol 2011; 64: 1283-93. [DOI] [PubMed] [Google Scholar]
- 29. Ma FG, Zhang YP, Chen HL, Sun LX, Wang MS. Impacts on oxidative stress in the patients with cardiac value replacement treated with electroacupuncture at Neiguan (PC6). Zhong Guo Zhen Jiu 2015; 35: 707-10. [PubMed] [Google Scholar]
- 30. Ni XL, Xie YN, Wang Q, et al. Cardioprotective effect of transcutaneous electric acupoint stimulation in the pediatric cardiac patients: a randomized controlled clinical trial. Paediatr Anaesth 2012; 22: 805-11. [DOI] [PubMed] [Google Scholar]
- 31. Shan JG. Clinic study of acupuncture-drug compound anesthesia on the regulation of immune function in patients undergoing open-heart surgery. Shanghai: Shanghai Jiao Tong University 2009: 1-48. [Google Scholar]
- 32. Shan JG, Xue S, Xu GX, et al. Effects of acupuncture-drug compound anesthesia on perioperative inflammatory factors in patients undergoing cardiac surgery. Zhong Guo Zhen Jiu 2010; 30: 585-8. [PubMed] [Google Scholar]
- 33. Tao YY. Effect of combined acupuncture and medical anesthesia on perioperative cardiovascular system in patients undergoing cardiac surgery under cardiopulmonary bypass. Shanghai: Shanghai Jiao Tong University, 2009: 1-54. [Google Scholar]
- 34. Wang XR, Hang YN, Sun DJ, Zhang MZ, Xu CR. Clinical observation on the adjustment of body’s functions by acupuncture in patients undergoing cardiac surgery. Shanghai Zhen Jiu Za Zhi 1999; 18: 6-7. [Google Scholar]
- 35. Wang YQ, Wang LK, Wu Z, Li YH. Effect of acupuncture-drug compound anesthesia on erythrocyte immunity in patients undergoing open-heart surgery under cardiopulmonary bypass. Anhui Yi Ke Da Xue Xue Bao 2012; 47: 876-8. [Google Scholar]
- 36. Wang Y, Li J, Han MM, Kang F, Feng F, Wang HT. Effect of electroacupuncture preconditioning on postoperative delirium and early outcomes in patients undergoing cardiac valve replacement with cardiopulmonary bypass. Zhong Hua Ma Zui Xue Za Zhi 2019; 39: 660-4. [Google Scholar]
- 37. Wu DQ, Zou XH, Zhang FX, et al. Effect of electroacupuncture stimulation on dosage of propofol and midazolam in cardiac valve replacement. Guizhou Yi Ke Da Xue Xue Bao 2018; 43: 1060-4. [Google Scholar]
- 38. Wu DQ, Zou XH, Zhang FX, et al. Effect of electroacupuncture stimulation on the dosage of analgesic drugs in heart valve replacement. Guizhou Yi Yao 2019; 43: 54-6. [Google Scholar]
- 39. Yang QG, Hang YN, Sun DJ, et al. Changes of IFN-γ, IL-2, IL-6, and IL-10 in the patient with cardiac surgery under combined acupuncture anesthesia. Zhong Guo Zhen Jiu, 2006; 503-6. [PubMed] [Google Scholar]
- 40. Yang LF, Xiong LZ, Lu ZH, et al. Influence of electroacupuncture preconditioning on early cognitive disturbance in patients undergoing cardiac surgery. Xin Zang Za Zhi 2009; 21: 712-5. [Google Scholar]
- 41. Yang LF, Yang J, Wang Q, et al. Cardioprotective effects of electroacupuncture pretreatment on patients undergoing heart valve replacement surgery: a randomized controlled trial. Ann Thorac Surg 2010; 89: 781-6. [DOI] [PubMed] [Google Scholar]
- 42. Yang YL, Zhu GS, Rong XF, Qiu L. Improvement in outcomes by acupuncture-drug balanced anesthesia following radical correction of tetralogy of Fallot under cardiopulmonary bypass in pediatric patients. Zhong Hua Ma Zui Xue Za Zhi 2020; 40: 462-5. [Google Scholar]
- 43. Zhang FX, Yu XD, Xiao H. Cardioprotection of electroacupuncture for enhanced recovery after surgery on patients undergoing heart valve replacement with cardiopulmonary bypass: a randomized control clinical trial. Evid Based Complement Alternat Med 2017; 6243630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Xiao H, Wu DQ, Zhang FX, Chen BN, Zhang JC, Luo YP. Cardioprotection of electroacupuncture in patients undergoing heart surgery with cardiopulmonary bypass. Zhong Hua Ma Zui Xue Za Zhi 2018; 38: 146-9. [Google Scholar]
- 45. Zhou J, Chi H, Cheng TO, et al. Acupuncture anesthesia for open-heart surgery in contemporary China. Int J Cardiol 2011; 150: 12-6. [DOI] [PubMed] [Google Scholar]
- 46. Han JS. Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies. Trends Neurosci 2003; 26: 17-22. [DOI] [PubMed] [Google Scholar]
- 47. Zhou F, Guo J, Cheng J, Wu G, Xia Y. Electroacupuncture increased cerebral blood flow and reduced ischemic brain injury: dependence on stimulation intensity and frequency. J Appl Physiol (1985) 2011; 111: 1877-87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Yang HS, Wu S, Zheng QY, et al. Meta-analysis on the protective effect of electroacupuncture at “Neiguan” (PC6) in rats with reperfusion injury-induced myocardial ischemia. World J Acupunct Moxibustion 2015; 25: 43-53. [Google Scholar]
- 49. Chinese Society of Integrative Anesthesiology, Gansu Provincial Society of Integrative Anesthesiology . Clinical practice guidelines for acupoint stimulation as an adjuvant treatment of postoperative pain (2021). Zhong Hua Ma Zui Xue Za Zhi 2021; 41: 1159-65. [Google Scholar]
- 50. De Hert S, Moerman A. Myocardial injury and protection related to cardiopulmonary bypass. Best Pract Res Clin Anaesthesiol 2015; 29: 137-49. [DOI] [PubMed] [Google Scholar]
- 51. Li YC, Zhang WL, Chi YL. Research progress of acupuncture in prevention and treatment of perioperative myocardial ischemia-reperfusion injury. Liaoning Zhong Yi Yao Da Xue Xue Bao 2022; 24: 163-7. [Google Scholar]
- 52. Han YL, Chen S, Peng X. Electroacupuncture Pretreatment at Neiguan (PC6) attenuates autophagy in rats with myocardial ischemia reperfusion through the phosphatidylinositol 3-kinase-Akt-mammalian target of rapamycin pathway. J Tradit Chin Med 2021; 41: 455-62. [DOI] [PubMed] [Google Scholar]
- 53. Tian Y, Gao H, Wang J, Zhai C, Li L. Effect of electroacupuncture at Ximen (PC 4) and Hegu (LI 4) on expression of Akt in rats with myocardial ischemia-reperfusion injury. J Tradit Chin Med 2017; 37: 835-840. [PubMed] [Google Scholar]
- 54. Liu HJ, Wang J, Ouyang LZ, Hu SN, Chang XY. Application of acupuncture in anesthesia and perioperative period. Liaoning Zhong Yi Za Zhi 2021; 48: 156-8. [Google Scholar]
- 55. Wang Y, Li D, Dai JY, et al. Effect of electro-acupuncture at Neiguan (PC6) and Lieque (LU7) on the expression of protein kinases in cardiomyocytes of myocardial ischemia rats. Zhong Guo Zhong Xi Yi Jie He Za Zhi 2015; 35: 338-42. [PubMed] [Google Scholar]
- 56. Yu Z, Luo L, Li Y, et al. Different manual manipulations and electrical parameters exert different therapeutic effects of acupuncture. J Tradit Chin Med 2014; 34: 754-8. [DOI] [PubMed] [Google Scholar]
- 57. Lin YP, Wang XS, Yi SX, Zhou GX. Influence on content of IMA and CGRP in blood of the MI and reperfusion injured rats after different frequency of electro-acupuncture at Neiguan. Zhong Hua Zhong Yi Yao Za Zhi 2012; 27: 2152-4. [Google Scholar]
- 58. Shi L, Zhou ZK, Miao RH, Jiang M. Effect of electro-needling PC6 on M2AChR and α7nAChR of myocardiac tissue in miri rats. Zhen Jiu Lin Chuang Za Zhi 2020; 36: 65-70. [Google Scholar]
- 59. Wang K, Ju Z, Chen C, et al. Cardioprotective effect of electroacupuncture in cardiopulmonary bypass through apelin/APJ signaling. Life Sci 2020; 242: 117208. [DOI] [PubMed] [Google Scholar]
- 60. Shao ML, Li Y, Cui HF, Jiang M, Tan QW. Protective effect of acupuncture preconditioning on oxidative stress injury induced by myocardial ischemia-reperfusion injury in rats. Zhong Guo Zhen Jiu 2017; 37: 285-90. [DOI] [PubMed] [Google Scholar]
- 61. Zhao DJ, Yang J, Yang LF. Insights for oxidative stress and mTOR signaling in myocardial ischemia/reperfusion injury under diabetes. Oxid Med Cell Longev 2017; 6437467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Bolli R. Oxygen-derived free radicals and myocardial reperfusion injury: an overview. Cardiovasc Drugs Ther 1991; 5 Suppl 2: 249-68. [DOI] [PubMed] [Google Scholar]
- 63. Chi LG, Tamura Y, Hoff PT, et al. Effect of superoxide dismutase on myocardial infarct size in the canine heart after 6 h of regional ischemia and reperfusion: a demonstration of myocardial salvage. Circ Res 1989; 64: 665-75. [DOI] [PubMed] [Google Scholar]
- 64. Corcoran TB, Engel A, Sakamoto H, O'Shea A, O'Callaghan-Enright S, Shorten GD. The effects of propofol on neutrophil function, lipid peroxidation and inflammatory response during elective coronary artery bypass grafting in patients with impaired ventricular function. Br J Anaesth 2006; 97: 825-31. [DOI] [PubMed] [Google Scholar]
- 65. Zhang Y, Li L, Xiang C, Ma Z, Ma T, Zhu S. Protective effect of melatonin against Adriamycin-induced cardiotoxicity. Exp Ther Med 2013; 5: 1496-500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Chen S, Han YL, Wu S, et al. Electroacupuncture preconditioning at "Neiguan" prevents myocardial ischemia-reperfusion injury in rats by activating p38-MAPK pathway. Hua Zhong Ke Ji Da Xue Xue Bao (Yi Xue Ban) 2017; 46: 526-30. [Google Scholar]
- 67. Zhang YM, Shi GG, Zheng JH, et al. The protective effects of N-n-butyl haloperidol iodide on myocardial ischemia-reperfusion injury in rats by inhibiting Egr-1 overexpression. Cell Physiol Biochem 2007; 20: 639-48. [DOI] [PubMed] [Google Scholar]
- 68. Modi P, Imura H, Angelini GD, et al. Pathology-related troponin I release and clinical outcome after pediatric open-heart surgery. J Card Surg 2003; 18: 295-300. [DOI] [PubMed] [Google Scholar]
- 69. Lin YP, Yan J, Wang C, Tian YF, Yi SX, Chang XR. Effect of electroacupuncturing Neiguan on cardiac troponin T and genes expression of bax in myocardial ischemia and reperfusion lesion. Hunan Zhong Yi Yao Da Xue Xue Bao 2006; 26: 40-2. [Google Scholar]
- 70. Wei XT, Li LY, Zhang YT, et al. Electroacupuncture preconditioning alleviates myocardial ischemia-reperfusion injury through the hypothalamic paraventricular nucleus-interposed nucleus nerve pathway. J Tradit Chin Med 2022; 42: 379-88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Lu SF, Huang Y, Wang N, et al. Cardioprotective Effect of electroacupuncture pretreatment on myocardial ischemia/reperfusion injury via antiapoptotic signaling. Evid Based Complement Alternat Med 2016; 4609784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Mu XY, Song YH, Zhang D, Sun JL, Tan QW. Preconditioning of needling PC6 improving miri: a study of research progress. Zhen Jiu Lin Chuang Za Zhi 2018; 34: 75-9. [Google Scholar]
- 73. Fujita T, Asai T, Andrassy M, et al. PKCbeta regulates ischemia/reperfusion injury in the lung. J Clin Invest 2004; 113: 1615-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Zhang J, Song J, Xu J, et al. ERK1/2-Egr-1 signaling pathway-mediated protective effects of electroacupuncture in a mouse model of myocardial ischemia-reperfusion. Evid Based Complement Alternat Med 2014; 2014: 253075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Li C, Zhang XL, Xue YX, et al. Protective effect and regulating effect on FXR/SHP gene of electroacupuncture preconditioning on myocardial ischemia-reperfusion injury in rats. Zhong Guo Zhen Jiu 2019; 39: 861-6. [DOI] [PubMed] [Google Scholar]
- 76. Cui S, Xu J, Wang J, Wu SB, Zhou YP, Zhou MQ. Effect of electroacupuncture stimulation of heart meridian on autonomic nervous activities in acute myocardial ischemia rats. Zhen Ci Yan Jiu 2016; 41: 515-20. [PubMed] [Google Scholar]
- 77. Hu JS. What are the 43 types of diseases that the WHO (World Health Organization) publishes and promotes acupuncture and moxibustion treatment? Zhong Yi Za Zhi 1989; 34: 57. [Google Scholar]
- 78. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology 2014; 120: 482-503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Teoh AYB, Chong CCN, Leung WW, et al. Electroacupuncture-reduced sedative and analgesic requirements for diagnostic EUS: a prospective, randomized, double-blinded, sham-controlled study. Gastrointest Endosc 2018; 87: 476-85. [DOI] [PubMed] [Google Scholar]
- 80. Hu XH, Xie YN, Lu ZH, Wang Q. Application of transcutaneous electrical acupoint stimulation for analgesia in patients with breast cancer radical mastectomy. Zhong Guo Xian Dai Yi Yao Za Zhi 2014; 16: 13-6. [Google Scholar]
- 81. Xu B. Basic principles of the scientific basis of combination of acupuncture and medicines. Shi Jie Zhong Yi Yao 2020; 15: 3179-83, 87. [Google Scholar]