

Abstract
Background
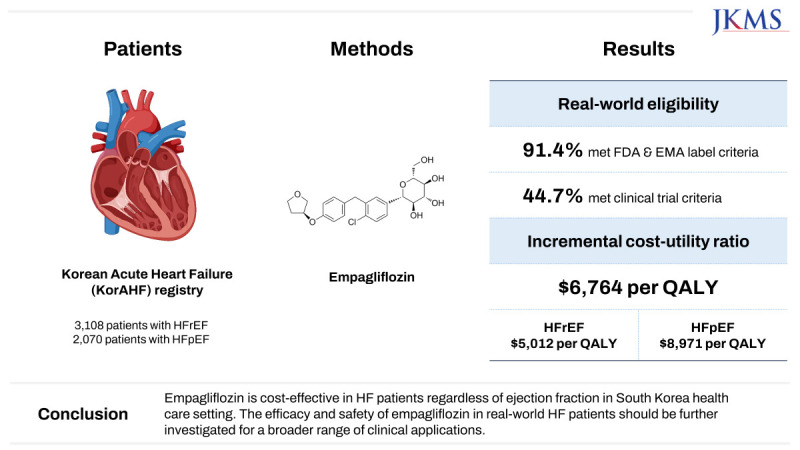
The US Food and Drug Administration (FDA) and European Medicines Agency (EMA) approved empagliflozin for reducing cardiovascular mortality and heart failure (HF) hospitalization in patients with both HF with reduced ejection fraction (HFrEF) and HF with preserved ejection fraction (HFpEF). However, limited data are available on the generalizability of empagliflozin to clinical practice. Therefore, we evaluated real-world eligibility and potential cost-effectiveness based on a nationwide prospective HF registry.
Methods
A total of 3,108 HFrEF and 2,070 HFpEF patients from the Korean Acute Heart Failure (KorAHF) registry were analyzed. Eligibility was estimated by inclusion and exclusion criteria of EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Reduced Ejection Fraction (EMPEROR-Reduced) and EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Preserved Ejection Fraction (EMPEROR-Preserved) trials and by FDA & EMA label criteria. The cost-utility analysis was done using a Markov model to project the lifetime medical cost and quality-adjusted life year (QALY).
Results
Among the KorAHF patients, 91.4% met FDA & EMA label criteria, while 44.7% met the clinical trial criteria. The incremental cost-effectiveness ratio of empagliflozin was calculated at US$6,764 per QALY in the overall population, which is far below a threshold of US$18,182 per QALY. The cost-effectiveness benefit was more evident in patients with HFrEF (US$5,012 per QALY) than HFpEF (US$8,971 per QALY).
Conclusion
There is a large discrepancy in real-world eligibility for empagliflozin between FDA & EMA labels and clinical trial criteria. Empagliflozin is cost-effective in HF patients regardless of ejection fraction in South Korea health care setting. The efficacy and safety of empagliflozin in real-world HF patients should be further investigated for a broader range of clinical applications.
Trial Registration
ClinicalTrials.gov Identifier: NCT01389843
Keywords: SGLT2 Inhibitors, Empagliflozin, Heart Failure, Drug Therapy, Cost-Effectiveness Analysis
Graphical Abstract
INTRODUCTION
The sodium-glucose co-transporter 2 (SGLT2) inhibitors have provided notable benefits to patients with heart failure (HF) with reduced ejection fraction (HFrEF).1 Currently, both empagliflozin and dapagliflozin are recommended for patients with HFrEF.2,3,4 Until recently no therapy has been definitively shown to improve outcomes in patients with HF with preserved ejection fraction (HFpEF), despite its substantial morbidity, mortality, and socioeconomic impact.2,3,5
The EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Preserved Ejection Fraction (EMPEROR-Preserved) trial first showed that empagliflozin reduced the combined endpoint of hospitalization for HF and cardiovascular (CV) death in patients with HFpEF regardless of diabetes,6 while dapagliflozin also showed clinical benefits in HFpEF patients in the recent DELIVER trial.7 Empagliflozin has been approved by the US Food and Drug Administration (FDA) and European Medicines Agency (EMA) for HF, irrespective of left ventricular ejection fraction (LVEF).8,9 Nevertheless, the proportion of real-world HF patients may be eligible for empagliflozin is yet to be ascertained, especially for a large-scale prospective cohort.
Criteria of the EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Reduced Ejection Fraction (EMPEROR-Reduced) and EMPEROR-Preserved trials were specific in inclusion enrollment with various detailed exclusion standards.6,10 It is well known that the characteristics of patients enrolled in randomized clinical trials show a discrepancy with those of real-world patients.11,12 Furthermore, from a socioeconomic perspective, applying empagliflozin to real-world HF patients should consider the balance between the clinical benefit and the cost related to the drug.
Early initiation of guideline-directed medical therapy (GDMT) and management of side effects and tolerability, especially during the transition period, has been emphasized recently.2,3 Initiation of GDMT in recovered stabilized patients with acute HF hospitalization, who are ready to discharge, represents an important avenue to improve the implementation of therapies that can greatly alter the clinical course. Therefore, we evaluated the candidacy for initiation of empagliflozin at discharge based on the EMPEROR-Reduced and EMPEROR-Preserved trials and FDA & EMA label criteria. We also analyzed the potential cost-effectiveness of empagliflozin in both HFrEF and HFpEF patients by using the Korean Acute Heart Failure (KorAHF) registry.
METHODS
Data collection and study population
The patient information was from the KorAHF registry. The registry is an observational, nationwide, multicenter, prospective cohort study. Between March 2011 and March 2014, 5,625 patients hospitalized in 10 tertiary university hospitals were included in the registry. The results and design of the study were published previously (ClinicalTrial.gov, NCT01389843).13 The in-hospital mortality was determined by the independent event committee.
Study variables and definitions
Patients discharged and recovered from an acute HF event were eligible for the study. When patients met the EMPEROR-Reduced and EMPEROR-Preserved trial’s inclusion and exclusion criteria, they were analyzed as candidates for empagliflozin. The eligibility was also estimated by FDA & EMA label criteria. The label-based indication of empagliflozin is shown in Supplementary Table 1. Current HF guidelines classified HFpEF as having an LVEF threshold of ≥ 50% and those with LVEF between 41% and 49% as in terms of HF with mildly reduced ejection fraction.2,3 However, for the study, HFrEF was defined as LVEF ≤ 40% and HFpEF as LVEF > 40%, according to EMPEROR-Reduced and EMPEROR-Preserved trial. LVEF measurements were by visual estimation, the biplane Simpson technique, or M-mode. Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.14
Statistical analysis
Categorical data were summarized as frequencies and proportions and compared using the χ2 test (or Fisher’s exact test for counts < 5 with a 2 × 2 table). For the expression of continuous variables, mean ± standard deviation was used. The t-test and analysis of variance were used for comparison. A P value < 0.05 on both sides was considered statistically significant. Statistical analyses were done using IBM SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, NY, USA).
Cost-utility analysis
Using the Markov model, the lifetime cost and effectiveness were estimated for each 10,000-hypothetical cohort with empagliflozin add-on therapy and standard of care (SoC). The cohort comprises the HFrEF and HFpEF patients with New York Heart Association (NYHA) classification II–IV. The characteristics of the population, including medication administration within the model, are regarded as equivalent to the study populations of the EMPEROR-Reduced and EMPEROR-Preserved trials. The health status was defined as alive, hospitalization, alive with adverse events (AEs), and death. The schematic representation of the Markov model is shown in Supplementary Fig. 1. The cohorts monthly transited the health status depending on the transition probability. In this model, the mortality was separated into CV mortality and non-CV mortality. The age-specific non-CV mortality was adopted from the life tables of Korean population statistics. The transition probability of CV death and hospitalization was computed using the EMPEROR-Reduced and EMPEROR-Preserved results. For example, a monthly transition probability of 0.89% was calculated by using the formula: Probability = 1 − Exp(−Rate × Time) = 1 − Exp[−0.107 × (1 ÷ 12)], when the hospitalization rate is reported as 10.7 events per 100 patient-year in HFrEF group with empagliflozin. The input parameters applied in the Markov model are listed in Supplementary Table 2.
From a healthcare system perspective, the costs of medication, dispensing, outpatient visits, monitoring, and AE-related expenses were included in the analysis. Here, the empagliflozin costs US$0.6 (660 won, considering that US$1 is 1,100 Korean won) per tablet in Korea. Costs of dispensing, outpatients visit, and monitoring were calculated using the micro-costing method by referring to the items of the previous Korean economic evaluation. For hospitalization costs, US$3,717.5 and US$3,348.8, the median hospitalization costs of patients included in the KorAHF registry, were applied in HFrEF and HFpEF, respectively. The AE-related costs and costs for administration were extracted from the open data Health Insurance Review and Assessment Service provided. Terminal care cost was the cost of hospitalization, which occurred in-hospital mortality in KorAHF registry patients.
In this cost-utility study, long-term cost and quality-adjusted life year (QALY) were predicted using Microsoft Excel 2019 (Microsoft Corp., Redmond, Washington, USA). The utility value was obtained from the Korean population survey. Based on the estimated cost and QALYs, the incremental cost-effectiveness ratio (ICER) was determined. ICER is the ratio of incremental cost and QALYs of empagliflozin relative to SoC. The willingness-to-pay (WTP) threshold of US$18,182 (KRW 20 million) per QALY was determined based on previous literature from cost-effective analyses conducted in South Korea.15,16 When the ICER of the intervention fell below the threshold, the intervention’s cost-effectiveness was validated. One-way deterministic sensitivity analyses were performed to ensure the robustness of the results by varying the values and assumptions about time horizon, discount rate, utilities, transition probabilities, and medical costs.
Ethics statement
The study protocol was approved by the ethics committee at each participating tertiary university hospital in Korea (Institutional Review Board [IRB] of Seoul National University Bundang Hospital, IRB No. B1104 125 014; IRB of Seoul National University Hospital, IRB No. 1102-072-352; IRB of Yonsei University Severance Hospital, IRB No. 4-2011-0075; IRB of Kyungpook National University Hospital, IRB No. 2011-04-016; IRB of Asan Medical Center, IRB No. 2011-0204; IRB of Seoul St Mary’s Hospital, IRB No. KC110IMI0172; IRB of Chonnam National University Hospital, IRB No. CHUN-2011-061; IRB of Chungbuk National University Hospital, IRB No. 201103-008; IRB of Samsung Medical Center, IRB No. 2013-040017; IRB of Wonju Severance Christian Hospital, IRB No. CR311003). Informed consent was submitted by all subjects when they were enrolled. If patients were unable to provide consent due to disease severity or other reasons, informed consent was obtained from relatives or a legal guardian.
RESULTS
Baseline clinical characteristics
The KorAHF registry enrolled 5,625 patients. Supplementary Fig. 2 shows the patient disposition. From 5,625 registered patients, 211 patients with unavailable LVEF measurements and 236 patients with in-hospital mortality were excluded. Table 1 shows the baseline characteristics of the 3,108 HFrEF and 2,070 HFpEF patients in the registry compared with EMPEROR-Reduced and EMPEROR-Preserved trials. Patients in the registry had more frequent NYHA class III and IV symptoms, a relatively lower body mass index and comorbidities of hypertension (HTN) and diabetes mellitus (DM), lower incidence of implantable cardioverter-defibrillator insertion, and lower systolic blood pressure (SBP), higher heart rate and N-terminal pro-B type natriuretic peptide (NT-proBNP) levels compared to both clinical trials. The mean value of the eGFR was higher, and the percentage of patients with eGFR values lower than 60 mL/min/1.73 m2 was lower in KorAHF patients.
Table 1. Baseline characteristics in KorAHF registry, EMPEROR-Reduced and EMPEROR-Preserved trial patients.
| Variables | KorAHF-HFrEF (n = 3,108) | EMPEROR-Reduceda (n = 3,730) | KorAHF-HFpEF (n = 2,070) | EMPEROR-Preserved (n = 5,988) | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age, yr | 66.1 ± 14.8 | 66.5 ± 11.2 | 71.6 ± 13.3 | 72.0 ± 9.0 | |
| Women, % | 39.4 | 24.4 | 58.1 | 45.0 | |
| Asian race, % | 100.0 | 18.1 | 100.0 | 14.0 | |
| Body mass index, kg/m2 | 23.2 ± 3.8 | 27.8 ± 5.3 | 23.7 ± 4.0 | 30.0 ± 6.0 | |
| Co-morbidities, %b | |||||
| Hypertension | 58.6 | 72.3 | 67.3 | 90.0 | |
| Diabetes mellitus | 41.6 | 49.8 | 35.6 | 49.0 | |
| Chronic kidney disease | 25.8 | - | 23.0 | 50.0 | |
| Coronary artery disease | 37.8 | - | 32.2 | 35.0 | |
| Atrial fibrillation/flutter | 39.2 | 37.8 | 53.7 | 52.0 | |
| COPD | 10.6 | - | 11.8 | 13.0 | |
| Malignancy | 8.6 | - | 7.3 | 10.0 | |
| ICD | 3.5 | 31.8 | 2.0 | 4.0 | |
| NYHA functional class, % | |||||
| I | 0 | 0 | 0 | 0 | |
| II | 13.8 | 75.0 | 17.8 | 82.0 | |
| III | 37.5 | 24.4 | 37.2 | 18.0 | |
| IV | 48.6 | 0.6 | 45.0 | 0.3 | |
| Left ventricular ejection fraction, % | 27.1 ± 7.7 | 27.2 ± 6.1 | 54.0 ± 8.9 | 54.0 ± 9.0 | |
| Heart rate, bpm | 77.7 ± 14.0 | 71.5 ± 11.8 | 75.5 ± 14.2 | 70.0 ± 12.0 | |
| Systolic blood pressure, mmHg | 112.8 ± 16.9 | 121.4 ± 15.4 | 118.0 ± 18.1 | 132.0 ± 16.0 | |
| Diastolic blood pressure, mmHg | 67.1 ± 11.3 | - | 67.1 ± 11.8 | 76.0 ± 11.0 | |
| NT-proBNP, pg/mL | 3,866 (1,670–9,136) | 1,926 (1,153–3,525) | 2,412 (1,073–5,495) | 974 (499–1,730) | |
| Estimated glomerular filtration rate | |||||
| Mean value, mL/min/1.73 m2 | 70.2 ± 29.7 | 62.2 ± 21.5 | 69.2 ± 28.6 | 60.6 ± 19.8 | |
| Value of < 60 mL/min/1.73 m2, % | 35.4 | 48.6 | 35.6 | 49.9 | |
| Hemoglobin, g/dL | 12.4 ± 2.2 | - | 11.7 ± 2.0 | 13.0 ± 2.0 | |
| Hemoglobin A1c, % | 6.8 ± 1.4 | - | 6.6 ± 1.3 | 7.3 ± 1.5 | |
Continuous data presented as mean ± standard deviation or median (interquartile range), as appropriate. Categorical data presented as proportions. Vital signs and laboratory parameters were from at discharge (only hemoglobin A1c were collected at admission).
COPD = chronic obstructive pulmonary disease, EMPEROR-Preserved = EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Preserved Ejection Fraction, EMPEROR-Reduced = EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Reduced Ejection Fraction, HFpEF = heart failure with preserved ejection fraction, HFrEF = heart failure with reduced ejection fraction, ICD = implantable cardioverter–defibrillator, KorAHF = Korean Acute Heart Failure, NT-proBNP = N-terminal pro-B type natriuretic peptide, NYHA = New York Heart Association.
aDemographics and clinical characteristics of EMEPEROR-Reduced were based on the placebo group.
bIncludes in-hospital diagnoses.
Fig. 1 shows the background medical therapies in the clinical trials and KorAHF registry. Compared with the EMPEROR-Reduced trial, the use of angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs), beta-blockers (β-blockers), and mineralocorticoid receptor antagonists (MRAs) was lower in KorAHF HFrEF patients. The KorAHF HFpEF patients had a lower prescription of ACEIs or ARBs and β-blockers than the EMPEROR-Preserved trial cohort.
Fig. 1. Comparison of background medical therapies. Background medical therapies were compared between EMPEROR-Reduced, EMPEROR-Preserved trial, and KorAHF registry.

ACEI = angiotensin-converting enzyme inhibitor, ARB = angiotensin receptor blocker, β-blocker = beta-blocker, EMPEROR-Preserved = EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Preserved Ejection Fraction, EMPEROR-Reduced = EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Reduced Ejection Fraction, HFpEF = heart failure with preserved ejection fraction, HFrEF = heart failure with reduced ejection fraction, KorAHF = Korean Acute Heart Failure, MRA = mineralocorticoid receptor antagonist.
Eligibility for the criteria of EMPEROR-Reduced and EMPEROR-Preserved trial
Fig. 2 shows the eligibility for the empagliflozin based on the inclusion and exclusion criteria of EMPEROR-Reduced and EMPEROR-Preserved trials. Among the 3,108 HFrEF and 2,070 HFpEF patients, 85.8% and 70.2% met the inclusion criteria (i.e., age ≥ 18 years, NYHA class II–IV, and elevated NT-proBNP at discharge), respectively. After combining the inclusion and main exclusion criteria, the cumulative eligibility of empagliflozin was 46.5% in HFrEF and 41.9% in HFpEF patients. In total, 44.7% of the patients in the registry were candidates for empagliflozin treatment. When patients were divided into a subpopulation of DM or without DM, eligibility for empagliflozin was 45.6% in DM and 44.1% in non-DM patients, as shown in Supplementary Fig. 3.
Fig. 2. Flow chart of empagliflozin eligibility selection. Empagliflozin eligibility were selected based on the inclusion & exclusion criteria of EMPEROR-Reduced and EMPEROR-Preserved trial in HFrEF and HFpEF patients in KorAHF registry.

A-Fib = atrial fibrillation, A-Flutter = atrial flutter, eGFR = estimated glomerular filtration rate, EMPEROR-Preserved = EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Preserved Ejection Fraction, EMPEROR-Reduced = EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Reduced Ejection Fraction, HFpEF = heart failure with preserved ejection fraction, HFrEF = heart failure with reduced ejection fraction, KorAHF = Korean Acute Heart Failure, NT-proBNP = N-terminal pro-B type natriuretic peptide, NYHA = New York Heart Association.
Table 2 shows the prevalence of the patient population satisfying each inclusion and exclusion criteria of the clinical trial. The main reason for not meeting the exclusion criteria was the SBP criteria. Overall, 18.7% of patients with HFrEF and 11.1% with HFpEF had SBP > 180 mmHg or < 100 mmHg. Other reasons were acute (< 4 weeks) myocardial infarction and impaired renal function (eGFR < 20 mL/min/1.73 m2 or requiring dialysis).
Table 2. Prevalence of excluded patients from the inclusion & exclusion criteria of EMPEROR-Reduced and EMPEROR-Preserved trial.
| EMPEROR-Reduced & EMPEROR-Preserved criteria | Prevalence | |||
|---|---|---|---|---|
| KorAHF-HFrEF (n = 3,108) | KorAHF-HFpEF (n = 2,070) | KorAHF-Total (n = 5,178) | ||
| No. of patients who unsatisfied the inclusion criteria | ||||
| Age < 18 yr | 0 (0) | 0 (0) | 0 (0) | |
| NYHA class I | 0 (0) | 0 (0) | 0 (0) | |
| Unelevated NT-proBNPa | 440 (14.2) | 616 (29.8) | 1,056 (20.4) | |
| No. of patients who satisfied the exclusion criteria | ||||
| Systolic blood pressure ≥ 180 mmHg or < 100 mmHg | 582 (18.7) | 230 (11.1) | 812 (15.7) | |
| Systolic blood pressure < 100 mmHg | 580 (18.7) | 227 (11.0) | 807 (15.6) | |
| eGFR < 20 mL/min/1.73 m2 or requiring dialysis | 273 (8.8) | 172 (8.4) | 446 (8.6) | |
| Cardiomyopathy (infiltrative, accumulation, reversible cause) | 170 (5.5) | 83 (4.0) | 253 (4.9) | |
| History of acute (< 4 wk) myocardial infarction | 345 (11.1) | 218 (10.5) | 563 (10.9) | |
| A-Fib/A-Flutter with a resting heart rate of > 110 bpm | 26 (0.8) | 25 (1.2) | 51 (1.0) | |
| Active or suspected malignancy | 267 (8.6) | 152 (7.3) | 419 (8.1) | |
| Hemoglobin of < 9 g/dL | 110 (3.5) | 120 (5.8) | 230 (4.4) | |
Values are presented as number (%).
A-Fib = atrial fibrillation, A-Flutter = atrial flutter, eGFR = estimated glomerular filtration rate, EMPEROR-Preserved = EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Preserved Ejection Fraction, EMPEROR-Reduced = EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Reduced Ejection Fraction, HFpEF = heart failure with preserved ejection fraction, HFrEF = heart failure with reduced ejection fraction, KorAHF = Korean Acute Heart Failure, LVEF = left ventricular ejection fraction, NT-proBNP = N-terminal prohormone B-type natriuretic peptide, NYHA = New York Heart Association.
a40% < LVEF: NT-proBNP ≤ 300 pg/mL in patients without atrial fibrillation and ≤ 900 pg/mL in patients with atrial fibrillation. 40% ≥ LVEF: NT-proBNP < 600 pg/mL in patients without atrial fibrillation and < 1,200 pg/mL in patients with atrial fibrillation.
Since low SBP was the main clinical barrier to eligibility, further analysis was performed to compare patients with SBP lower and higher than 100 mmHg. Supplementary Table 3 compares the clinical characteristics of the two groups. Patients with low SBP showed younger age and LVEF and higher heart rate and eGFR than those in the high SBP group. The prevalence of HTN, DM, CKD, coronary artery disease, and frequency of eGFR < 60 mL/min/1.73 m2 was higher in the high SBP group. Supplementary Fig. 4 compares the prescription rates of ACEIs or ARBs, β-blockers, and MRA at discharge between the two groups. In the low SBP group, the use of β-blockers was lower, and MRA was higher, even within the HFrEF and HFpEF patients. The use of ACEIs or ARBs was similar in all patients with HFrEF. However, in HFpEF patients, the use of ACEIs and ARBs was lower in the low SBP group.
Comparison of empagliflozin eligibility for FDA & EMA label criteria
Empagliflozin is approved for adults with HF by FDA and symptomatic adults with chronic HF by EMA. Both do not recommend empagliflozin for patients with eGFR < 20 mL/min/1.73 m2 and are contraindicated when requiring dialysis.8,9 Since the patients in the KorAHF registry were symptomatic patients, NYHA class II–IV, the calculation of empagliflozin eligibility was the same between FDA and EMA.
Applying to the registry, as shown in Supplementary Fig. 5, 91.4% of patients were eligible by FDA and EMA label criteria. When divided into HFrEF and HFpEF, the eligibility was 91.2% and 91.6%. The FDA and EMA label-based empagliflozin-eligible patients include more HFpEF patients than clinical trial-based patients. Supplementary Table 4 shows a clinical characteristics comparison between FDA and EMA label-based and clinical trial-based empagliflozin eligible patients. The label-based patients were young, had less HTN, DM, and CKD, the level of NT-proBNP were low, and eGFR was higher when compared to clinical trial-based patients.
Cost-effectiveness of empagliflozin in the KorAHF registry
A cost-utility analysis was performed based on the Markov model. Based on the results of the analysis, the assessment of the cost-effectiveness of empagliflozin is shown in Table 3. In the HFrEF population, the empagliflozin and SoC groups gained total QALYs of 6.18 and 5.98, respectively. Total costs per patient throughout the lifetime were estimated to be US$20,041 for the empagliflozin group and US$19,082 for the SoC group. As a result, the ICER of empagliflozin compared to SoC was US$5,012 in the HFrEF group. The total QALY gains for the empagliflozin and SoC groups were 8.28 and 8.03 in the HFpEF population, respectively. The estimated lifetime expenses per patient for the empagliflozin group and the SoC group were US$20,118 and US$17,850, and the ICER of empagliflozin compared to SoC was consequently US$8,971 in the HFpEF group. The ICER of the overall population was estimated using the weighted average of QALYs and the costs of the HFrEF and HFpEF population. The weight was based on the proportion empagliflozin-eligible patients of HFrEF (n = 1,445) and HFpEF (n = 868) in the KorAHF registry. The ICER of empagliflozin was estimated at US$6,764 per QALY in the overall population. Consequently, empagliflozin is a highly cost-effective option within a WTP threshold of US$18,182 per QALY. This finding was robust according to one-way sensitivity analyses, shown in Fig. 3.
Table 3. Results of the cost-utility analysis for empagliflozin add-on therapy compared to standard of care.
| Variables | QALYs | Incremental QALYs | Costsa | Incremental costs | ICER | |
|---|---|---|---|---|---|---|
| HFrEF | ||||||
| Empagliflozin | 6.18 | 0.19 | 20,041 | 959 | 5,012 | |
| Standard of care | 5.98 | 19,082 | ||||
| HFpEF | ||||||
| Empagliflozin | 8.28 | 0.25 | 20,118 | 2,268 | 8,971 | |
| Standard of care | 8.03 | 17,850 | ||||
| Overall populationb | ||||||
| Empagliflozin | 6.97 | 0.21 | 20,070 | 1,450 | 6,764 | |
| Standard of care | 6.75 | 18,618 | ||||
HFpEF = heart failure with preserved ejection fraction, HFrEF = heart failure with reduced ejection fraction, ICER = incremental cost-effectiveness ratio, QALY = quality-adjusted life year.
aIn US dollars (exchange rate: 1 USD = 1,100 KRW).
bWeighted average based on the proportion of HFrEF (n = 1,445) and HFpEF (n = 868) in the Korean Acute Heart Failure (KorAHF) registry.
Fig. 3. Tornado diagram for one-way sensitivity analysis. The variables are listed in order of influence on economic evaluation. The value of each variable was changed from the base case and shown as the maximum and minimum incremental cost-effectiveness ratio, which are indicated as bars.

QALY = quality-adjusted life year.
DISCUSSION
Among real-world patients in the KorAHF registry, 44.7% of the patients were eligible for empagliflozin at discharge, according to the inclusion and exclusion criteria for the EMPEROR-Reduced and EMPEROR-Preserved trials. HFrEF patients had higher eligibility for empagliflozin compared to HFpEF patients. The main exclusion factor for ineligible empagliflozin use was low SBP (< 100 mmHg), which was more frequent in patients with HFrEF. Other major factors leading to exclusion include a history of acute myocardial infarction and impaired renal function. The empagliflozin-eligible patients meeting FDA & EMA label criteria were 91.4%.
When using empagliflozin, the estimated ICER was US$6,764 per QALY in the total population and is a cost-effective option within a threshold of US$18,182 per QALY. Additionally, the lower the cost per hospitalization, the smaller the cost-saving effect. However, empagliflozin-eligible patients in HFpEF had a higher ICER than HFrEF patients. The ICER represents the increased cost per hospitalization event. When the ICER is less than the WTP, the new intervention can be more cost-effective than the comparator. However, the ICER threshold may vary across different nations, even in countries that implement health technology assessment. Therefore, these results should be extrapolated with caution.
Guideline-recommended HF treatment based on renin-angiotensin system inhibitors, β-blockers, and MRAs has remained relatively constant over many years until the addition of sacubitril/valsartan, an angiotensin receptor-neprilysin inhibitor (ARNI), as recommended in the current guidelines.2,3,4 Here, SGLT2 inhibitors were included in front-line therapy with notable results in clinical trials.2,3,17 The EMPA-REG OUTCOME trial first showed that the SGLT2 inhibitor had a significantly lower rate of death from CV causes with empagliflozin than with placebo among patients with type 2 DM (hazard ratio [HR], 0.62; 95% confidence interval [CI], 0.49–0.77).18 Furthermore, the EMPEROR-Reduced and EMPEROR-Preserved trial found that empagliflozin was associated with a lower risk than placebo of a composite outcome of CV death or hospitalization for HF in patients with both HFrEF (HR, 0.75; 95% CI, 0.65–0.86) and HFpEF (HR, 0.79; 95% CI, 0.69–0.90), with or without type 2 DM.6,10
However, due to the constraints of patient enrollment criteria in randomized clinical trials, it is difficult to apply emerging therapies with limited evidence in everyday practice. Especially in HF, which is known to have frequent comorbidities and other factors that might influence outcomes, many patients are excluded due to the stringent enrollment criteria used in clinical trials. Based on the PARADIGM-HF trial, less than 25% of patients had eligibility for sacubitril/valsartan when strictly following the criteria.19,20 In SGLT2 inhibitors, the eligibility of empagliflozin or dapagliflozin in HFrEF patients of other registries was below 50% based on the EMPA-REG OUTCOME and DAPA-HF trial criteria.21,22
In our study, among patients with HF, the main factor for empagliflozin non-eligibility was low SBP. It has been reported that HTN is one of the main risk factors for HF.23,24 However, once patients develop HF, lower SBP is associated with an advanced disease state, which leads to higher CV morbidity and mortality.25 Although empagliflozin showed clinical benefits for both HFrEF and HFpEF patients, there is a risk of hypotension in patients with a low baseline SBP due to the antihypertensive effect of SGLT2 inhibitors.26
When comparing the cost-effectiveness analysis results with previous studies, empagliflozin was cost-effective in the HFrEF group, as the results of the current study.27,28,29 However, in a study using a database of patients in Thailand, empagliflozin was found to be cost-effective in patients with HFrEF but not in those with.30 Compared with the current study, which analyzed that empagliflozin would be cost-effective in HFpEF, this discrepancy might be induced by the difference in medical costs between the two countries. In Thailand, the price of empagliflozin is higher than that of empagliflozin in Korea (US$110.35 vs. US$54.79 for three months). Conversely, the cost of hospitalization is higher in Korea (about US$3,500) than in Thailand (US$1,696). Therefore, it can be interpreted that in Thailand, the effect of reducing hospitalization costs caused by empagliflozin use is lower than in Korea.
Here, we found that the clinical characterization of patients in the real-world HF population differs from the clinical trials. We also compared the current HF medication use between patients in real-world and clinical trials, subclassified by HFrEF and HFpEF. Although GDMT for HFrEF is associated with reduced mortality, actual patients are less likely to use evidence-based medications than patients in clinical trials. These findings are in line with previous reports derived from other registries.31,32 In a situation where GDMT remains low, applying empagliflozin and other SGLT2 inhibitors immediately in everyday clinical practice will be difficult. In particular, it is unclear whether up-titration of the currently recommended therapy to the target dose is better than using SGLT2 inhibitors as a replacement rather than an add-on. In HFpEF, many established treatments were found to be ineffective, and the pathophysiology of HFpEF differs from that of HFrEF.33 Since empagliflozin first demonstrated its effectiveness in HFpEF patients and the proper use of SGLT2 inhibitors has yet to be established, the demand for a new clinical guideline for the treatment of HFpEF is gaining more interest.
The indication of FDA and EMA approval or empagliflozin covers more patients than EMPEROR-Reduced and EMPEROR-Preserved trials, resulting in 91.4% of total patients in the KorAHF registry. Here, there is a large gap between the eligibility based on the clinical trial criteria and the label, raising the possibility that patients without meticulous validation of eligibility criteria could be treated with empagliflozin. After the publication of the RALES trial, the inappropriate use of spironolactone resulted in more hospitalizations and deaths due to side effects such as hyperkalemia.34 Hence, it is necessary to confirm their efficacy in patients with old age, low blood pressure, cancer, or advanced CKD.
The strict inclusion and exclusion criteria in clinical trials may result in lower patient eligibility. However, in clinical practice, patients with HF who have low SBP or high stage CKD appear to tolerate empagliflozin administration well. Recently, studies based on the EMPEROR-Reduced trials showed that empagliflozin was safe and effective, regardless of SBP and severity of kidney impairment at baseline.35,36 Likewise, studies like post-hoc analysis or retrospective cohort will be required to determine whether empagliflozin and other SGLT2 inhibitors show clinical benefits to patients outside of the current clinical trial’s criteria.
Our study has some limitations. First, the patients enrolled in the KorAHF registry were not chronic HF outpatients but hospitalized patients recruited only from tertiary hospital centers. In this respect, a direct comparison of clinical characteristics or background medication with EMPEROR-Reduced or EMPEROR-Preserved trials might not be ideally matched. Furthermore, the higher-risk patients would be observed in the analytic population compared to the general chronic HF outpatient population, making a comparison with EMPEROR-Reduced or EMPEROR-Preserved trials difficult. However, the patient characteristic data for the empagliflozin eligibility analysis were collected when patients were discharged for outpatient care, having recovered from the acute stage. Furthermore, the current HF guidelines emphasize initiating and optimizing GDMT during the transitional period before discharge. Given this context, assessing the eligibility for empagliflozin in patients discharged from hospitalization using KorAHF registry can hold clinical significance. Second, we only analyzed the main criteria from the trials. Other exclusion criteria (e.g., liver disease, known allergy or hypersensitivity to SGLT2 inhibitors, and history of ketoacidosis) were unavailable in the registry. Eligibility of empagliflozin could be lower when all minor criteria were applied. However, their small population is unlikely to affect the results. Third, since the disease status of HF patients may change throughout the aging process, the eligibility for empagliflozin can be affected. Fourth, the ARNI was not approved by the Korea Food and Drug Administration during the registry enrollment. Thus, the eligibility of empagliflozin in patients treated with ARNI is unknown. However, the utilization of ARNI in the EMPEROR-Reduced trial was 18.3%, and that of ARNI in the EMPEROR-Preserved trial was only 2%. Given these proportions, the influence of ARNI on the comparison between KorAHF and the clinical trials is likely to be minimal. Fifth, the limited availability of certain values might have impacted the result. In the Markov model, the incidence of treatment effects was based on the clinical trial. There is an increased uncertainty due to extrapolation when the observation period goes beyond the follow-up period of the clinical trial. Also, the source of the hospitalization cost was from tertiary hospitals, and there is a possibility that the actual cost could be lower. In addition, when considering mortality reduction, the kidney-protective effect of empagliflozin, and recovery of productivity loss costs due to morbidity and mortality, the expected cost reduction when using empagliflozin will be increased. With regard to clinical aspects, cost-effectiveness may be affected by diabetes and symptom severity. However, the additional sensitivity analyses were unavailable.
In summary, 44.7% in a nationwide prospective HF registry met the clinical trial criteria, and 91.4% met FDA and EMA label criteria for empagliflozin treatment. When using empagliflozin for eligible patients, the estimated ICER was US$6,764 per QALY and was a cost-effective option within a threshold of US$18,182 per QALY in South Korea health care setting. The potential cost-effectiveness benefit was more evident in HFrEF than in HFpEF. Since there is a large discrepancy between eligible patients based on the clinical trials and FDA and EMA approval, elucidating the effectiveness of SGLT2 inhibitors in patients not included in the clinical trial criteria will be crucial. In addition, updating treatment guidelines for HF, especially in HFpEF where there is now evidence of substantial clinical benefit from clinical trials with both empagliflozin and dapagliflozin, could help contribute to better patient care.
ACKNOWLEDGMENTS
The authors express sincere gratitude to all Korean Acute Heart Failure (KorAHF) investigators, research coordinators and the participants who enabled this study.
Footnotes
Funding: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Ministry of Science and ICT (NRF-2021R1F1A1063430), by the Catholic Medical Center Research Foundation (2023), the Research Fund of Seoul St. Mary’s Hospital, Catholic University of Korea (2022), the Catholic University of Korea Research Fund (2020), and by the Research of Korea Centers for Disease Control and Prevention (2010-E63003-00, 2011-E63002-00, 2012-E63005-00, 2013-E6300300, 2014-E63003-01, 2015-E63003-02, 2016-ER6303-00, and 2017-ER6303-01). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure: The authors have no potential conflicts of interest to disclose.
Data Availability Statement: The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
- Conceptualization: Kim ES, Park SK, Youn JC.
- Data curation: Youn JC, Lee HS, Lee HY, Cho HJ, Choi JO, Jeon ES, Lee SE, Kim MS, Kim JJ, Hwang KK, Cho MC, Chae SC, Kang SM, Park JJ, Choi DJ, Yoo BS, Cho JY, Kim KH, Oh BH, Baek SH.
- Formal analysis: Kim ES, Park SK.
- Supervision: Youn JC.
- Writing - original draft: Kim ES, Park SK.
- Writing - review & editing: Kim ES, Park SK, Youn JC, Greenberg B.
SUPPLEMENTARY MATERIALS
Prescribing information of empagliflozin for heart failure patients in FDA and EMA
Input parameters applied in the cost-utility analysis of empagliflozin
Clinical characteristics of patients in Korean Acute Heart Failure registry, stratified by systolic blood pressure
Clinical characteristics of empagliflozin eligible patients according to FDA & EMA label, EMPEROR-Reduced, and EMPEROR-Preserved trial criteria
Schematic representation of the Markov model. HF patients can stay alive, hospitalized, alive with adverse events, or dead in the model. The health status was monthly transited depending on the transition probability.
Flow chart of the study population.
Compared eligibility of empagliflozin between diabetic and non-diabetic patients in KorAHF registry.
Comparison of prescription rate of ACEI or ARB, β-blocker, and MRA. Prescription rate of ACEI or ARB, β-blocker, and MRA between were compared according to SBP level in KorAHF registry.
Comparison of empagliflozin eligibility between the clinical trial and FDA & EMA label. (A) Frequency of empagliflozin eligible patients in KorAHF registry. Proportion of HFrEF and HFpEF patients in empagliflozin eligible patients based on (B) FDA & EMA label and (C) clinical trial criteria.
References
- 1.Kim ES, Youn JC, Baek SH. Update on the pharmacotherapy of heart failure with reduced ejection fraction. Cardiovasc Prev Pharmacother. 2020;2(4):113–133. [Google Scholar]
- 2.McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. Corrigendum to: 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2021;42(48):4901. doi: 10.1093/eurheartj/ehab670. [DOI] [PubMed] [Google Scholar]
- 3.Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 2022;145(18):e895–1032. doi: 10.1161/CIR.0000000000001063. [DOI] [PubMed] [Google Scholar]
- 4.Hyun J, Cho JY, Youn JC, Kim D, Cho DH, Park SM, et al. Korean Society of Heart Failure guidelines for the management of heart failure: advanced and acute heart failure. Korean Circ J. 2023;53(7):452–471. doi: 10.4070/kcj.2023.0115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Youn JC, Han S, Ryu KH. Temporal trends of hospitalized patients with heart failure in Korea. Korean Circ J. 2017;47(1):16–24. doi: 10.4070/kcj.2016.0429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Anker SD, Butler J, Filippatos G, Ferreira JP, Bocchi E, Böhm M, et al. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med. 2021;385(16):1451–1461. doi: 10.1056/NEJMoa2107038. [DOI] [PubMed] [Google Scholar]
- 7.Solomon SD, McMurray JJ, Claggett B, de Boer RA, DeMets D, Hernandez AF, et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N Engl J Med. 2022;387(12):1089–1098. doi: 10.1056/NEJMoa2206286. [DOI] [PubMed] [Google Scholar]
- 8.US Food and Drug Administration. FDA approves treatment for wider range of patients with heart failure. [Updated 2022]. [Accessed August 15, 2022]. https://www.fda.gov/news-events/press-announcements/fda-approves-treatment-wider-range-patients-heart-failure .
- 9.European Commission. Union Register of medicinal products for human use. [Updated 2022]. [Accessed 15 August, 2022]. https://ec.europa.eu/health/documents/community-register/html/h930.htm .
- 10.Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, Carson P, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383(15):1413–1424. doi: 10.1056/NEJMoa2022190. [DOI] [PubMed] [Google Scholar]
- 11.Masoudi FA, Havranek EP, Wolfe P, Gross CP, Rathore SS, Steiner JF, et al. Most hospitalized older persons do not meet the enrollment criteria for clinical trials in heart failure. Am Heart J. 2003;146(2):250–257. doi: 10.1016/S0002-8703(03)00189-3. [DOI] [PubMed] [Google Scholar]
- 12.Kim JJ, Youn JC. Eligibility and usage of sacubitril/valsartan in Korea. Int J Heart Fail. 2019;1(1):69–71. doi: 10.36628/ijhf.2019.0008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lee SE, Cho HJ, Lee HY, Yang HM, Choi JO, Jeon ES, et al. A multicentre cohort study of acute heart failure syndromes in Korea: rationale, design, and interim observations of the Korean Acute Heart Failure (KorAHF) registry. Eur J Heart Fail. 2014;16(6):700–708. doi: 10.1002/ejhf.91. [DOI] [PubMed] [Google Scholar]
- 14.Inker LA, Eneanya ND, Coresh J, Tighiouart H, Wang D, Sang Y, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. N Engl J Med. 2021;385(19):1737–1749. doi: 10.1056/NEJMoa2102953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Song HJ, Lee EK. Evaluation of willingness to pay per quality-adjusted life year for a cure: a contingent valuation method using a scenario-based survey. Medicine (Baltimore) 2018;97(38):e12453. doi: 10.1097/MD.0000000000012453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ahn J, Kim Y, Shin S, Park SY, Song HJ, Park J, et al. Research on Methodologies for Evidence-Based Healthcare Decision-Making Processes in Korea. Seoul, Korea: National Evidence-based Healthcare Collaborating Agency (NECA); 2010. [Google Scholar]
- 17.Seferovic PM, Polovina M, Milinkovic I, Anker S, Rosano G, Coats A. Expect the unexpected in the medical treatment of heart failure with reduced ejection fraction: between scientific evidence and clinical wisdom. Int J Heart Fail. 2021;3(4):205–218. doi: 10.36628/ijhf.2021.0013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–2128. doi: 10.1056/NEJMoa1504720. [DOI] [PubMed] [Google Scholar]
- 19.Oh J, Lee CJ, Park JJ, Lee SE, Kim MS, Cho HJ, et al. Real-world eligibility for sacubitril/valsartan in heart failure with reduced ejection fraction patients in Korea: data from the Korean Acute Heart Failure (KorAHF) registry. Int J Heart Fail. 2019;1(1):57–68. doi: 10.36628/ijhf.2019.0007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Norberg H, Bergdahl E, Lindmark K. Eligibility of sacubitril-valsartan in a real-world heart failure population: a community-based single-centre study. ESC Heart Fail. 2018;5(2):337–343. doi: 10.1002/ehf2.12251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Maltês S, Cunha GJ, Rocha BM, Presume J, Guerreiro R, Henriques C, et al. Dapagliflozin in a real-world chronic heart failure population: how many are actually eligible? Cardiology. 2021;146(2):201–206. doi: 10.1159/000512432. [DOI] [PubMed] [Google Scholar]
- 22.Arnold SV, Inzucchi SE, Tang F, McGuire DK, Mehta SN, Maddox TM, et al. Real-world use and modeled impact of glucose-lowering therapies evaluated in recent cardiovascular outcomes trials: an NCDR® Research to Practice project. Eur J Prev Cardiol. 2017;24(15):1637–1645. doi: 10.1177/2047487317729252. [DOI] [PubMed] [Google Scholar]
- 23.Levy D, Larson MG, Vasan RS, Kannel WB, Ho KK. The progression from hypertension to congestive heart failure. JAMA. 1996;275(20):1557–1562. [PubMed] [Google Scholar]
- 24.Staessen JA, Wang JG, Thijs L. Cardiovascular protection and blood pressure reduction: a meta-analysis. Lancet. 2001;358(9290):1305–1315. doi: 10.1016/S0140-6736(01)06411-X. [DOI] [PubMed] [Google Scholar]
- 25.Lee TT, Chen J, Cohen DJ, Tsao L. The association between blood pressure and mortality in patients with heart failure. Am Heart J. 2006;151(1):76–83. doi: 10.1016/j.ahj.2005.03.009. [DOI] [PubMed] [Google Scholar]
- 26.Kario K, Ferdinand KC, Vongpatanasin W. Are SGLT2 inhibitors new hypertension drugs? Circulation. 2021;143(18):1750–1753. doi: 10.1161/CIRCULATIONAHA.121.053709. [DOI] [PubMed] [Google Scholar]
- 27.Liao CT, Yang CT, Kuo FH, Lee MC, Chang WT, Tang HJ, et al. Cost-effectiveness evaluation of add-on empagliflozin in patients with heart failure and a reduced ejection fraction from the healthcare system’s perspective in the Asia-Pacific region. Front Cardiovasc Med. 2021;8:750381. doi: 10.3389/fcvm.2021.750381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Jiang Y, Zheng R, Sang H. Cost-effectiveness of adding SGLT2 inhibitors to standard treatment for heart failure with reduced ejection fraction patients in China. Front Pharmacol. 2021;12:733681. doi: 10.3389/fphar.2021.733681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Lin X, Lin M, Liu M, Huang W, Nie X, Chen Z, et al. Cost-effectiveness of empagliflozin as a treatment for heart failure with reduced ejection fraction: an analysis from the Chinese healthcare perspective. J Thorac Dis. 2022;14(5):1588–1597. doi: 10.21037/jtd-22-463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Krittayaphong R, Permsuwan U. Cost-utility analysis of combination empagliflozin and standard treatment versus standard treatment alone in Thai heart failure patients with reduced or preserved ejection fraction. Am J Cardiovasc Drugs. 2022;22(5):577–590. doi: 10.1007/s40256-022-00542-9. [DOI] [PubMed] [Google Scholar]
- 31.Teng TK, Tromp J, Tay WT, Anand I, Ouwerkerk W, Chopra V, et al. Prescribing patterns of evidence-based heart failure pharmacotherapy and outcomes in the ASIAN-HF registry: a cohort study. Lancet Glob Health. 2018;6(9):e1008–18. doi: 10.1016/S2214-109X(18)30306-1. [DOI] [PubMed] [Google Scholar]
- 32.Greene SJ, Butler J, Albert NM, DeVore AD, Sharma PP, Duffy CI, et al. Medical therapy for heart failure with reduced ejection fraction: the CHAMP-HF registry. J Am Coll Cardiol. 2018;72(4):351–366. doi: 10.1016/j.jacc.2018.04.070. [DOI] [PubMed] [Google Scholar]
- 33.Youn JC, Ahn Y, Jung HO. Pathophysiology of heart failure with preserved ejection fraction. Heart Fail Clin. 2021;17(3):327–335. doi: 10.1016/j.hfc.2021.02.001. [DOI] [PubMed] [Google Scholar]
- 34.Juurlink DN, Mamdani MM, Lee DS, Kopp A, Austin PC, Laupacis A, et al. Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study. N Engl J Med. 2004;351(6):543–551. doi: 10.1056/NEJMoa040135. [DOI] [PubMed] [Google Scholar]
- 35.Böhm M, Anker SD, Butler J, Filippatos G, Ferreira JP, Pocock SJ, et al. Empagliflozin improves cardiovascular and renal outcomes in heart failure irrespective of systolic blood pressure. J Am Coll Cardiol. 2021;78(13):1337–1348. doi: 10.1016/j.jacc.2021.07.049. [DOI] [PubMed] [Google Scholar]
- 36.Zannad F, Ferreira JP, Pocock SJ, Zeller C, Anker SD, Butler J, et al. Cardiac and kidney benefits of empagliflozin in heart failure across the spectrum of kidney function: insights from EMPEROR-Reduced. Circulation. 2021;143(4):310–321. doi: 10.1161/CIRCULATIONAHA.120.051685. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Prescribing information of empagliflozin for heart failure patients in FDA and EMA
Input parameters applied in the cost-utility analysis of empagliflozin
Clinical characteristics of patients in Korean Acute Heart Failure registry, stratified by systolic blood pressure
Clinical characteristics of empagliflozin eligible patients according to FDA & EMA label, EMPEROR-Reduced, and EMPEROR-Preserved trial criteria
Schematic representation of the Markov model. HF patients can stay alive, hospitalized, alive with adverse events, or dead in the model. The health status was monthly transited depending on the transition probability.
Flow chart of the study population.
Compared eligibility of empagliflozin between diabetic and non-diabetic patients in KorAHF registry.
Comparison of prescription rate of ACEI or ARB, β-blocker, and MRA. Prescription rate of ACEI or ARB, β-blocker, and MRA between were compared according to SBP level in KorAHF registry.
Comparison of empagliflozin eligibility between the clinical trial and FDA & EMA label. (A) Frequency of empagliflozin eligible patients in KorAHF registry. Proportion of HFrEF and HFpEF patients in empagliflozin eligible patients based on (B) FDA & EMA label and (C) clinical trial criteria.