

Abstract
It is estimated 1.5 billion of the global population suffer from chronic pain with prevalence increasing with demographics including age. It is suggested long-term exposure to chronic could cause further health challenges reducing people’s quality of life. Therefore, it is imperative to use effective treatment options. We explored the current pharmaceutical treatments available for chronic pain management to better understand drug efficacy and pain reduction. A systematic methodology was developed and published in PROSPERO (CRD42021235384). Keywords of opioids, acute pain, pain management, chronic pain, opiods, NSAIDs, and analgesics were used across PubMed, Science direct, ProQuest, Web of science, Ovid Psych INFO, PROSPERO, EBSCOhost, MEDLINE, ClinicalTrials.gov and EMBASE. All randomised controlled clinical trials (RCTs), epidemiology and mixed-methods studies published in English between the 1st of January 1990 and 30th of April 2022 were included. A total of 119 studies were included. The data was synthesised using a tri-partied statistical methodology of a meta-analysis (24), pairwise meta-analysis (24) and network meta-analysis (34). Mean, median, standard deviation and confidence intervals for various pain assessments were used as the main outcomes for pre-treatment pain scores at baseline, post-treatment pain scores and pain score changes of each group. Our meta-analysis revealed the significant reduction in chronic pain scores of patients taking NSAID versus non-steroidal opioid drugs was comparative to patients given placebo under a random effects model. Pooled evidence also indicated significant drug efficiency with Botulinum Toxin Type-A (BTX-A) and Ketamine. Chronic pain is a public health problem that requires far more effective pharmaceutical interventions with minimal better side-effect profiles which will aid to develop better clinical guidelines. The importance of understanding ubiquity of pain by clinicians, policy makers, researchers and academic scholars is vital to prevent social determinant which aggravates issue.
Subject terms: Neuropathic pain, Drug development
Introduction
Chronic non-cancer pain conditions are prevalent, highly debilitating and have high cost implications to health and social care. These conditions affect patients, their families and society at large, impacting 20% of the global population1. The prevalence of pain conditions among females of all ages appears to be increasing2. Complexities around diagnosis and treatment of chronic pain conditions have meant that there is a paucity of standardised clinical guidelines that could potentially improve the clinical practice landscape, globally.
Convalescent periods for many chronically ill patients can be protracted and daunting. This may be especially true where pain medication has been used in the long term3. Long-term exposures to chronic pain coincide with mental health and wellbeing, exacerbating patient-reported outcomes such as sleep disturbances, depression, dependence and morbidities such as myalgia and fatigue4. Better understanding of long-term implications requires consideration of “life-course approaches” and at present, this could evolve further within pain medicine epidemiology5.
Increases in chronic pain conditions contributes to higher healthcare costs towards clinical management of patients and also reduced levels of productivity for employers6. This may be partly due to increases in opioid use within this population of patients, often reducing their capacity to conduct normal working hours. Current clinical guidelines recommend non-invasive pain management options as a first-line treatment among non-cancer patients in particular, although overdose, dependency and mortality due to opioid use has consistently increased over time7,8. It was reported that global opioid use has doubled between 2001 and 2003 to 2011 and 2013 to 7.35 billion daily doses per year9,10.
It is particularly important to develop evidence-based guidelines specific to each condition, with flexible pain medication use as a single regimen or a combination of treatments that could improve the overall quality of life of these patients11,12. The premise to increase the strength and frequency of pain medications is in general based on disease burden i.e., progression of symptoms and patients reported symptoms4.
We have designed the POP project as the initial step to conduct exploratory work on pharmaceutical management of chronic pain. With the rising need for comparative effectiveness research, increasingly more systematic reviews focus on evaluating the relative efficacy and acceptability of drugs and therapeutic interventions3,13. However, some of the interventions for long-term conditions are not available for clinical practice and there are several options with varying efficacy even within a specific class of interventions14.
Methods
We developed a wide systematic methodology and published this as a protocol with multiple research questions in the first instance in PROSPERO (CRD42021235384). Data from studies meeting the inclusion criteria were extracted and Pairwise Meta-Analysis with random and fixed effects models was carried out. Pooled mean difference (MD) together with 95% confidence intervals (CIs) are reported overall and for sub-groups. By combining the direct and indirect comparisons between different interventions, Network Meta-Analysis was conducted to explore the relative treatment effects among all the drugs included in our analysis.
Aims
The aims of the study was to explore the prevalence of treatments of effects in chronic pain based on pharmaceutical treatments.
Search strategy
The search strategy used key words of chronic pain, opioids, acute pain, pain management, opiods, NSAIDs, analgesics across multiple databases (PubMed, Science direct, ProQuest, Web of science, Ovid Psych INFO, PROSPERO, EBSCOhost, MEDLINE, ClinicalTrials.gov and EMBASE).
Eligibility criteria
All randomised controlled clinical trials (RCTs), epidemiology and mixed-methods studies reporting the use of pain medication for non-cancer chronic pain conditions published in English between the 1st January 1990 and 30st April 2022 were included. Opinions, commentaries and editorials were excluded (Fig. 1).
Figure 1.

PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only15.
Data extraction
Participants included in the study populations had chronic non-cancer pain conditions. All studies reporting drug efficacy were extracted by way of the interventions, measures of tool and numeric results. An extraction template specific to the objectives of the study was developed. Sub-studies were extracted from the same clinical trials with different duration periods.
Data was extracted by two investigators and any disputes for eligibility was discussed and agreed with the Chief Investigator of the study. All studies included within the analyses were independently reviewed.
Outcome measures
Outcomes were reported as mean, median, standard deviation and confidence intervals. Mean and Standard deviation (SD) were extracted as the main outcomes including pre-treatment pain scores at baseline, post-treatment pain scores and pain score changes of each group.
Multiple pain assessments for confirming a clinical diagnosis, severity and progression of chronic pain were identified. These include VAS (visual analogue scale, 0–10 or 0–100), NRS (11-point numeric rating scale, 0–10), BPI (Brief Pain Inventory interference scale, 0–10), MPQS (McGill Pain Questionnaire-Short Form (Sensory and Affective subscales, VAS intensity measure, 0–10), VRS (verbal rating scale, 0–10), NIH-CPSI (National Institutes of Health Chronic Prostatitis Symptom Index, pain scores, 0–21), PI (pain intensity on a 20-point scale, 0–20).
As most widely used tools for assessing pain such as VAS, NRS, VRS, use a 11-point numeric rating scale from 0 to 10, the following standardisation formula was used to unify all pain scores into the same scale:
As all outcomes of interest were continuous, the calculation based on pain scores was performed by using mean differences (MD) with a 95% confidence interval (CI) to report the effects between the group comparisons.
Exposures
The exposures of interest were selected based on the key features of pharmacological management used to treat non-cancer chronic pain, including and not limited to a pain condition being the primary or the secondary condition. Neurological and psychological symptoms leading up to the use of pharmaceutical use within the included population were also considered.
Statistical analysis plan
A meta-analysis, pairwise meta-analysis (PMA) and Network meta-analysis (NMA) were used to compare all treatments used in managing non-cancer chronic pain. The fundamental difference between them is that PMA produced only one estimate of pooling effects from the selected pair of interventions, while the NMA produced multiple comparative estimates of pooling effects by connecting all alternative interventions16.
We incorporated direct and indirect treatment comparisons within the NMA providing greater statistical precision compared to a PMA. Rankings of a set of drugs or combined interventions for assessing chronic pain with respect to their efficacy was calculated based on the network models. Homogeneity and Consistency were tested to see if the assumptions in NMA were violated. The overall pharmaceutical efficacy of extracted studies was produced by pooling all treatment effects. PMA was also used on studies with the same drug as the treatment group to see the specific drug efficacy.
and p-value were commonly used to detect statistical heterogeneity. A value of larger than 50% with a much smaller p-value indicates strong heterogeneity. Correspondingly, less than 50% with a large p-value indicates fairly weak heterogeneity17. A random effects model was chosen when there was high heterogeneity, whereas a fixed effects model was used if weak or no heterogeneity was detected18. Due to the presence of high heterogeneity, subgroup analyses were carried out to identify the sources. To assess the robustness of the pooled results within the PMA, a sensitivity analysis was completed. Publication bias was evaluated with funnel plots and Egger tests. The statistical analyses were produced by R and packages were used to provide outputs in compliance with best practice and reporting guidelines19.
Results
Of the 119 systematically included studies (Table 1) with 17,708 participants, 24 studies were used in the meta-analysis and 34 within the NMA to build a connected network.
Table 1.
Characteristics of the studies included in systematic review.
| Study ID | Authors | Publication year | Study type | Pain type | Intervention | Sample size | Mean age | Country | Included for MA | Included for NMA |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Weizman et al. | 2018 | P–C, RCT | Chronic-pain | THC | 17 | 33.3 | Israel | No | No |
| 2 | Krebs et al. | 2018 | RCT | Back, Arthritis, Chronic-pain | Opioid | 240 | 56.8 | USA | No | No |
| 3 | AbdelHafeez et al. | 2019 | Double-blind, P–C, RCT | Chronic-pain | Gabapentin | 60 | 32.7 | UK | Yes | Yes |
| 4 | Bushey et al. | 2021 | RCT | Chronic-pain | Opioid | 241 | 37 | USA | No | No |
| 5 | Bruehl et al. | 2021 | Double-blind, P–C, RCT, Crossover | Low-back, Chronic-pain | Morphine + Naloxone | 191 | 36.5 | USA | No | No |
| 6 | Worley et al. | 2015 | RCT | Chronic-pain | Buprenorphine/Naloxone | 149 | USA | No | No | |
| 7 | Dindo et al. | 2018 | Single-blinded, RCT | Postsurgical, Chronic-pain | ACT | 76 | 62.2 | USA | No | No |
| 8 | Hruschak et al. | 2019 | Single-blinded, RCT | Chronic-pain | IPGT | 30 | 53.9 | USA | No | No |
| 9 | Azevedo et al. | 2013 | Chronic-pain | Opioid | 2213 | 45 | Portugal | No | No | |
| 10 | Gudin et al. | 2020 | Open-label, P–C, Uncontrolled | Low-back, Noncancer, Chronic-pain | NKTR-181 | 402 | 52 | USA | No | No |
| 11 | Stahl et al. | 2019 | RCT | Low-back, Chronic-pain | Venlafaxine | 209 | 69.6 | USA | No | No |
| 12 | Schliessbach et al. | 2018 | Double-blind, P–C, RCT | Low-back, Chronic-pain | Imipramine | 50 | 54.4 | Switzerland | No | No |
| 13 | Mohamed et al. | 2016 | Double-blind, RCT | PostsurgicalNeuropathic, Cancer, Chronic-pain | Morphine | 90 | 50.43 | Egypt | No | No |
| 14 | Schliessbach et al. | 2018 | P–C, RCT | Low-back, Chronic-pain | Oxycodone + Imipramine + Clobazam | 98 | 55 | Switzerland | No | Yes |
| 15 | Hermans et al. | Double-blind, P–C, RCT, Crossover | Arthritis, Chronic-pain | Naloxone | 31 | 39.8 | Belgium | No | No | |
| 16 | Todorov et al. | 2005 | Chronic-pain | Gabapentin + Tiagabine | 91 | 42 | USA | No | Yes | |
| 17 | Sadatsune et al. | Double-blind, P–C, RCT | Chronic-pain | Gabapentin | 40 | 51.5 | Brazil | No | No | |
| 18 | Edwards et al. | 2016 | RCT | Back, Chronic-pain | Opioid | 31 | 49 | USA | No | No |
| 19 | Katz et al. | 2011 | Double-blind, P–C, RCT | Low-back, Chronic-pain | Naproxen + Tanezumab | 129 | 52.1 | USA | No | No |
| 20 | Hayek et al. | 2021 | Double-blind, RCT, Crossover | Chronic-pain | Opioid + Bupivacaine | 16 | 63.1 | USA | No | No |
| 21 | Schliessbach et al. | 2017 | Double-blind, P–C, Crossover | Back, Chronic-pain | Clobazam | 49 | 54.3 | Switzerland | No | Yes |
| 22 | Bruehl et al. | 2004 | Double-blind, P–C, RCT, Crossover | Low-back, Noncancer, Chronic-pain | Opioid | 28 | 37.3 | USA | No | No |
| 23 | Kim et al. | 2018 | Double-blind, RCT | Postsurgical, Chronic-pain | Nefopam | 58 | 40 | South korea | No | No |
| 24 | Eisenach et al. | 2010 | Double-blind, P–C, RCT, Crossover | Chronic-pain | Ketorolac | 15 | 44 | No | No | |
| 25 | Rauck et al. | 2014 | Single-blinded, RCT, Crossover | Chronic-pain | Adenosine/Clonidine | 22 | 44 | USA | No | No |
| 26 | Buchheit et al. | 2019 | Double-blind, P–C, RCT | Postsurgical, Chronic-pain | Valproate | 128 | 57 | USA | No | No |
| 27 | Papadokostakis et al. | 2005 | Back, Chronic-pain | Calcitonin | 110 | 65 | Greece | No | No | |
| 28 | Gould et al. | 2020 | Double-blind, 4-arm, RCT | Back, Chronic-pain | Desipramine | 141 | 51.5 | USA | No | Yes |
| 29 | Schnitzer et al. | 2016 | Double-blind, P–C, RCT | Back, Chronic-pain | D-cycloserine | 41 | 53.2 | USA | No | No |
| 30 | Nenke et al. | 2015 | Double-blind, P–C, RCT, Crossover | Low-back, Noncancer, Chronic-pain | Hydrocortisone | 26 | 71 | Australia | Yes | Yes |
| 31 | Sopata et al. | 2015 | Double-blind, P–C, RCT | Chronic-pain | Opioid | 100 | 62.1 | Poland | No | No |
| 32 | Kendall et al. | Double-blind, P–C, RCT | Postsurgical, Chronic-pain | Lidocaine | 148 | 48 | usa | No | No | |
| 33 | Hongo et al. | 2015 | RCT | Back, Chronic-pain | Risedronate + Elcatonin | 45 | 70.9 | Japan | No | No |
| 34 | Amr and Yousef | 2010 | Double-blind, RCT | Postsurgical, Chronic-pain | Venlafaxine + Gabapentin | 150 | 45 | Egypt | No | No |
| 35 | Pedersen et al. | 2014 | Double-blind, RCT | Chronic-pain | Codeine + Paracetamol | 58 | 49 | Norway | No | No |
| 36 | Choi et al. | 2016 | Double-blind, RCT | Postsurgical, Chronic-pain | Lidocaine | 90 | 34 | Korea | No | No |
| 37 | Bruehl et al. | 2014 | P–C, RCT | Back, Chronic-pain | Morphine + Naloxone | 50 | 36.9 | USA | Yes | Yes |
| 38 | Chrubasik et al. | 2010 | Double-blind, P–C, RCT | Chronic-pain | Capsicum | 130 | 48.9 | Germany | No | No |
| 39 | Schliessbach et al. | 2017 | Double-blind, P–C, RCT, Crossover | Back, Chronic-pain | Oxycodone | 50 | 55 | Switzerland | No | Yes |
| 40 | Bruehl and Chung | 2006 | Double-blind, P–C, RCT, Crossover | Low-back, Chronic-pain | Naloxone | 119 | 35.1 | USA | No | No |
| 41 | Bruehl et al. | 2013 | Double-blind, P–C, RCT, Crossover | Low-back, Chronic-pain | Naloxone + Morphine | 76 | 37.9 | USA | No | No |
| 42 | Burns et al. | 2017 | Double-blind, P–C, RCT | Low-back, Chronic-pain | Naloxone + Morphine | 89 | 36.9 | USA | No | No |
| 43 | Eker et al. | 2016 | Double-blind, RCT | Knee, Arthritis, Chronic-pain | Lidocaine | 52 | 65.15 | Turkey | Yes | Yes |
| 44 | Kim et al. | 2015 | Double-blind, RCT | Cancer, Chronic-pain | Opioid | 49 | 62 | Korea | No | No |
| 45 | Kimos et al. | 2007 | Double-blind, P–C, RCT | Chronic-pain | Gabapentin | 50 | 33.58 | Canada | Yes | Yes |
| 46 | Narang et al. | 2008 | Double-blind, P–C, RCT, Crossover | Chronic-pain | Opioid | 30 | 43.5 | USA | No | No |
| 47 | Peyton et al. | 2017 | P–C, RCT | Postsurgical, Chronic-pain | Ketamine | 80 | 55.3 | Australia | No | No |
| 48 | Katz et al. | 2005 | P–C, RCT, Crossover | Low-back, Chronic-pain | Bupropion | 60 | 49.8 | Yes | Yes | |
| 49 | Hashmi et al. | 2012 | Double-blind, P–C, RCT | Back, Chronic-pain | Lidocaine | 30 | 51.36 | USA | No | No |
| 50 | Shimoyama et al. | 2014 | Double-blind, P–C, RCT, Crossover | Cancer, Chronic-pain | Fentanyl | 51 | 59.1 | Japan | No | No |
| 51 | Wreje and Brorsson | 1995 | RCT | Chronic-pain | Sterile water | 117 | > = 25 | Sweden | No | No |
| 52 | Han et al. | 2016 | Double-blind, P–C, RCT | Neuropathic, Chronic-pain | BTX-A | 40 | 53.1 | korea | Yes | Yes |
| 53 | Rauck et al. | 2014 | Double-blind, P–C, RCT | Chronic-pain | Hydrocodone | 510 | 50.4 | USA | No | No |
| 54 | Kim et al. | 2010 | Double-blind, P–C, RCT | Postsurgical, Chronic-pain | Pregabalin | 94 | 39 | Korea | No | No |
| 55 | Lee et al. | 2019 | RCT | Chronic-pain | BTX-A | 60 | 50.9 | Korea | No | No |
| 56 | Rashiq et al. | 2003 | Double-blind, P–C, RCT, Crossover | Low-back, Chronic-pain | Fentanyl | 28 | 54 | Yes | Yes | |
| 57 | Kang et al. | 2020 | Double-blind, P–C, RCT | Postsurgical, Chronic-pain | Ketamine | 168 | 50.8 | korea | No | No |
| 58 | Lipton et al. | 2021 | P–C, RCT | Chronic-pain | Erenumab | 955 | 41.1 | Canada-13* | No | No |
| 59 | Williamson et al. | 2014 | P–C, RCT | Low-back, Knee, Arthritis, Chronic-pain | Duloxetine | 780 | 63.2 | Canada | No | No |
| 60 | Guo et al. | 2020 | RCT | Low-back, Chronic-pain | Celecoxib Eperisone | 150 | 36 | China | No | No |
| 61 | Damjanov et al. | 2018 | Double-blind, P–C, RCT | Chronic-pain | ACS | 32 | 59 | No | No | |
| 62 | Abd-Elshafy et al. | 2019 | Double-blind, RCT | Postsurgical, Chronic-pain | Bupivacaine | 60 | 35 | Egypt | No | Yes |
| 63 | Levesque et al. | 2021 | Double-blind, RCT | Chronic-pain | BTX + Ropivacaïne | 80 | 53.1 | No | No | |
| 64 | Maher et al. | 2018 | P–C, RCT | Chronic-pain | Ketamine | 79 | 50.32 | USA | No | No |
| 65 | Barry et al. | 2019 | RCT | Back, Chronic-pain | Methadone | 40 | 37.7 | USA | No | No |
| 66 | Shokeir and Mousa | 2015 | Double-blind, P–C, RCT | Chronic-pain | Bupivacaine | 60 | 32.8 | Egypt | Yes | Yes |
| 67 | Scudds et al. | 1995 | Double-blind, P–C, RCT | Chronic-pain | Lidocaine | 61 | 46.1 | Canada | No | No |
| 68 | Gimbel et al. | 2016 | Double-blind, P–C, RCT | Low-back, Chronic-pain | Buccal buprenorphine | 510 | 52.8 | USA | No | No |
| 69 | Matsuoka et al. | 2019 | P–C, RCT | Neuropathic, Cancer, Chronic-pain | Duloxetine | 70 | 64.7 | Japan | No | No |
| 70 | Yurekli et al. | 2008 | Double-blind, P–C, RCT | Chronic-pain | Sodium valproate | 70 | 40 | Turkey | Yes | Yes |
| 71 | Maarrawi et al. | 2018 | Double-blind, P–C, RCT | Chronic-pain | Amitriptyline | 112 | 43.54 | Lebanon | Yes | Yes |
| 72 | Li et al. | 2018 | Double-blind, RCT | Postsurgical, Chronic-pain | Ropivacaine + Dexamethasone | 52 | 62 | China | No | No |
| 73 | Almog et al. | 2020 | Double-blind, 3-arm, RCT, Crossover | Chronic-pain | THC | 27 | 48.3 | Israel | No | No |
| 74 | Wylde et al. | 2015 | Double-blind, RCT | Postsurgical, Knee, Chronic-pain | Bupivacaine | 273 | 66 | UK | No | No |
| 75 | Matsukawa et al. | 2020 | RCT | Chronic-pain | Cernitin + Tadalafil | 100 | 65.9 | Japan | No | No |
| 76 | Haddad et al. | 2018 | Double-blind, P–C, RCT, Crossover | Chronic-pain | Apomorphine | 35 | 56.2 | Israel | No | No |
| 77 | de Vries et al. | 2016 | Double-blind, P–C, RCT | Postsurgical, Chronic-pain | THC | 65 | 52.2 | Netherlands | Yes | Yes |
| 78 | Urquhart et al. | 2018 | Double-blind, RCT | Low-back, Chronic-pain | Amitriptyline | 146 | 53.5 | Australia | No | Yes |
| 79 | Lichtman et al. | 2018 | Double-blind, P–C, RCT | Cancer, Chronic-pain | Nabiximols | 397 | 59.2 | Belgium-12* | No | No |
| 80 | Schiphorst et al. | 2014 | Trible-Blind, P–C, RCT | Low-back, Chronic-pain | Acetaminophen/Tramadol | 50 | 42 | Netherlands | No | No |
| 81 | Cardenas et al. | 2002 | RCT | Chronic-pain | Amitriptyline | 84 | 41 | USA | Yes | Yes |
| 82 | Arnold et al. | 2012 | Double-blind, P–C, RCT | Chronic-pain | Milnacipran | 1025 | 49.1 | USA | No | No |
| 83 | Wasan et al. | 2005 | Double-blind, P–C, RCT, Crossover | Low-back, Chronic-pain | Morphine | 20 | 44.2 | USA | No | No |
| 84 | Baron et al. | 2014 | Double-blind, RCT | Neuropathic, Low-back, Chronic-pain | Tapentadol/Pregabalin | 445 | 56.3 | Germany | No | No |
| 85 | Portenoy et al. | 2007 | Double-blind, P–C, RCT | Low-back, Chronic-pain | Fentanyl | 77 | 48.9 | USA | No | No |
| 86 | Likar et al. | 1997 | Double-blind, RCT, Crossover | Arthritis, Chronic-pain | Morphine | 21 | 68 | Austria | No | No |
| 87 | Schwartzman et al. | 2009 | Double-blind, P–C, RCT | Chronic-pain | Ketamine | 20 | 38 | USA | Yes | Yes |
| 88 | Chu et al. | 2012 | Double-blind, P–C, RCT | Back, Chronic-pain | Morphine | 139 | 44 | USA | Yes | Yes |
| 89 | Sandrini et al. | 2011 | Double-blind, P–C, RCT | Chronic-pain | BoNTA | 56 | 48.5 | USA | No | No |
| 90 | Mahowald et al. | 2009 | Single-blinded, P–C, RCT | Arthritis, Chronic-pain | BoNTA | 40 | > = 48 | USA | Yes | Yes |
| 91 | Loftus et al. | 2010 | Double-blind, P–C, RCT | Back, Chronic-pain | Ketamine | 102 | 51.7 | Lebanon /USA | Yes | Yes |
| 92 | Lehmann et al. | 1997 | P–C, RCT | Postsurgical, Chronic-pain | Fentanyl | 29 | 44.15 | USA | No | No |
| 93 | Kahlenberg et al. | 2017 | P–C, RCT | Chronic-pain | Celecoxib | 98 | 34.2 | USA | Yes | Yes |
| 94 | Silberstein et al. | 2009 | Double-blind, P–C, RCT | Chronic-pain | Topiramate | 306 | 38.2 | USA | No | No |
| 95 | Burgher et al. | 2011 | Double-blind, RCT | Low-back, Chronic-pain | Lidocaine | 26 | 44.1 | USA | No | No |
| 96 | McCleane | 1999 | Double-blind, P–C, RCT, Crossover | Neuropathic, Chronic-pain | Phenytoin | 20 | 40 | Ireland | Yes | Yes |
| 97 | Naliboff et al. | 2011 | 2-arm, RCT | Chronic-pain | Opioid | 135 | 52.7 | USA | No | No |
| 98 | Booth et al. | 2017 | P–C, RCT | Postsurgical, Chronic-pain | Morphine | 74 | 28 | USA | No | Yes |
| 99 | Lee et al. | 2006 | Single-blinded, RCT | Chronic-pain | Rowatinex/Ibuprofen | 50 | 44.2 | Korea | No | No |
| 100 | Levendoglu et al. | 2004 | Double-blind, P–C, RCT, Crossover | Neuropathic, Chronic-pain | Gabapentin | 20 | 35.9 | Turkey | Yes | Yes |
| 101 | Yousef and Alzeftawy | 2018 | Double-blind, RCT | Chronic-pain | Opioid | 100 | 53.44 | Egypt | No | Yes |
| 102 | Yelland et al. | 2009 | Double-blind, P–C, RCT, Crossover | Neuropathic, Chronic-pain | Gabapentin | 73 | 57.8 | Australia | No | No |
| 103 | Yucel et al. | 2004 | Double-blind, P–C, RCT | Neuropathic, Chronic-pain | Venlafaxine | 55 | 48.94 | Turkey | No | No |
| 104 | Hudson et al. | 2021 | Double-blind, P–C, RCT | Knee, Arthritis, Chronic-pain | Nortriptyline | 205 | 64.4 | New Zealand | Yes | Yes |
| 105 | Rauck et al. | 2006 | Double-blind, P–C, RCT | Chronic-pain | Ziconotide | 220 | 52.5 | USA | No | No |
| 106 | Sandner-Kiesling et al. | 2010 | Double-blind | Noncancer, Chronic-pain | Naloxone + Oxycodone | 379 | 56.2 | Austria/Germany | No | No |
| 107 | Wang et al. | 2017 | RCT | Chronic-pain | Diosmin | 300 | 41 | China | No | Yes |
| 108 | Hawley et al. | 2020 | Double-blind, P–C, RCT, Crossover | Cancer, Chronic-pain | Lidocaine | 25 | 53.76 | Canada | No | No |
| 109 | Mathieson et al. | 2017 | Double-blind, P–C, RCT | Chronic-pain | Pregabalin | 209 | 66 | Australia | No | No |
| 110 | Wetzel et al. | 2015 | Double-blind, P–C, RCT, Crossover | Low-back, Noncancer, Chronic-pain | Nonopioid analgesic drugs | 36 | 55 | Austria | No | No |
| 111 | Khan et al. | 2019 | P–C, RCT | PostsurgicalNeuropathic, Cancer, Chronic-pain | Lidocaine + Pregabalin | 100 | 55.2 | Canada | No | No |
| 112 | Clarke et al. | 112 | Double-blind, RCT | Postsurgical, Chronic-pain | Gabapentin | 126 | 58.9 | Canada | Yes | Yes |
| 113 | Ma et al. | 113 | Double-blind, P–C, RCT | Chronic-pain | Oxycodone | 116 | 58.2 | China | Yes | Yes |
| 114 | J. H. Lee and C. S. Lee | 114 | Double-blind, P–C, RCT | Low-back, Chronic-pain | TA-ER | 245 | 59.9 | Korea | No | No |
| 115 | Imamura et al. | 2016 | Trible-Blind, RCT | Low-back, Chronic-pain | Lidocaine | 378 | 48.26 | Brazil | No | No |
| 116 | Baron et al. | 2015 | RCT | Neuropathic, Low-back, Chronic-pain | Tapentadol | 258 | 58.1 | Germany | No | No |
| 117 | Kim et al. | 2017 | Double-blind, RCT | Postsurgical, Cancer, Chronic-pain | Lidocaine + Magnesium | 126 | 48.7 | Korea | Yes | Yes |
| 118 | Iwamura et al. | 2015 | RCT | Chronic-pain | Eviprostat | 100 | 50.1 | Japan | No | No |
| 119 | Zhang et al. | 2021 | Double-blind, P–C, RCT | Chronic-pain | Ningmitai | 120 | 33.7 | China | No | No |
Canada-13*: “Canada-13” was used as the group of 13 countries: “Canada, Austria, Belgium, Czech Republic, Finland, Germany, Poland, Slovakia, Sweden, the United Kingdom, Turkey, the Netherlands and USA”.
Belgium-12*: “Belgium-12” was used as the group of 12 countries: “Belgium, Bulgaria, Czechia, Germany, Hungary, Latvia, Lithuania, Poland, Puerto Rico, Romania, United Kingdom, United States”.
Opioids (Table 2) were tested in 32 (26.89%) studies with 5518 (31.16%) participants, where Morphine, Oxycodone and Fentanyl were common. Lidocaine, Naloxone and Gabapentin were the most frequently tested non-opioid drugs for chronic pain. The most common pain among chronic pain patients were lower back pain, which was explored in 26 (21.85%) studies with a pooled sample of 4626 (26.12%) while 13 studies reported chronic back pain among 1068 (6.03%) participants. The following pain types are post-surgical pain and neuropathic pain with 19 (15.97%) and 10 (8.4%) studies involved to test the efficiency of NSAID drugs on patients.
Table 2.
Summary of drug and pain types included in systematic review.
| Classes | Drug types | Studies (number, %) | Participants (number, %) |
|---|---|---|---|
| Opioids 32 (26.89%) | Oxycodone | 4 (3.36%) | 643 (3.63%) |
| Fentanyl | 4 (3.36%) | 185 (1.04%) | |
| Methadone | 1 (0.84%) | 40 (0.23%) | |
| Morphine | 9 (7.56%) | 750 (4.24%) | |
| Buprenorphine | 2 (1.68%) | 659 (3.72%) | |
| Codeine | 1 (0.84%) | 58 (0.33%) | |
| Other Opioids | 11 (9.24%) | 3183 (17.97%) | |
| Nonopioids | Naloxone | 8 (6.72%) | 1084 (6.12%) |
| Gabapentin | 8 (6.72%) | 610 (3.44%) | |
| Lidocaine | 10 (8.4%) | 1036 (5.85%) | |
| Ketamine | 5 (4.2%) | 449 (2.54%) | |
| Amitriptyline | 3 (2.52%) | 342 (1.93%) | |
| Bupivacaine | 4 (3.36%) | 409 (2.31%) |
Meta-analysis of mean difference of pain scores were applied to 24 studies with a sample of 2546 participants, producing a pooled mean difference (MD) of – 0.89 (95% CI [− 1·31, − 0·47]). There was a significant difference between chronic pain scores of patients taking NSAIDs compared to a placebo. Averagely, 0.89 point (0–10 scale) of pain reduction was observed based on the random effects model. A significant statistical drug efficiency was observed with BTX-A and Ketamine. A negative pooled mean difference was determined between BTX-A and Ketamine versus a placebo with a pain reduction of 0.98–1.26 based on a − 10 scale, respectively. Similar statistical results were not observed with other drugs in comparison to a placebo.
Within the common comparator as a “placebo”, the connected network included 34 studies, 52 pairwise comparisons, 32 interventions and 29 study designs. Gabapentin had a significant mean difference equalling to – 1.49 (95% CI [− 2⋅76, − 0⋅23], p-value < 0.05). Most interventions had a negative mean difference compared to a placebo, but a 95% CI covering 0 indicated insignificant effects for reducing pain. The results within the network were more conservative with the combination of direct and indirect evidence indicating most pharmaceutical interventions selected might have benefited from the “placebo effect”.
Pairwise meta-analysis (PMA)
The PMA included 24 studies with pairwise comparisons between drugs and a placebo. The experimental and control group comprised of "Amitriptyline", "BTX-A”, “Gabapentin", "Ketamine", "Lidocaine", "Morphine", "Naloxone" and a placebo, respectively. A single study reported "Fentanyl", "Ningmitai", "THC", and "Oxycodone".
PMA for baseline pain score
The PMA was used to test baseline pain score differences between the experimental and control group in 18 studies which comprised of a total sample of 1691 participants. The experimental and control groups comprised of 837 and 854 participants, respectively, with a pooled mean difference (MD) of – 0.02 (95% CI [− 0.13, 0.08]). The 95% CI was 0 and therefore, no statistically significant difference between baseline pain scores of two groups (Fig. 2). A weak statistical heterogeneity of 15% of (p = 0.26) was determined. This combined with the statistical insignificance indicates the randomisation of was completed accurately and that it is scientifically justifiable to use the post-treatment pain scores directly as the outcomes to evaluate treatment effects.
Figure 2.

Forest plot for the baseline pain scores of experimental group and control group across 18 studies.
PMA for drug efficacy between NSAID compared to a placebo
This PMA included 24 studies (Fig. 3) with 2418 participants, with a MD of − 0.89 (95% CI [− 1.31, − 0.47]). The experimental and control group comprised of 1219 and 1199, respectively. A significant statistical heterogeneity of 92% of (p-value < 0.01) was identified. Mean difference (MD) was calculated to assess if there is statistically significant difference of post-treatment pain scores between experimental group and control group. The 95% CI was less than 0 which indicated a significant treatment effect with a reduction in pain by 0.89-point (0–10 scale) compared to those who were given a placebo.
Figure 3.

Forest plot for the pain scores of experimental group and control group across 24 studies testing all NSAID drugs (including some unnamed Opioids drugs).
Meta-analyses
A statistically low heterogeneity of 0% of (p-value > 0.5) was identified among studies with BTX-A, Ketamine and Naloxone (Fig. 4b,d). BTX-A (Fig. 4b) and Ketamine (Fig. 4d) indicated statistically significant drug efficacy of – 1.07 [−1.51, − 0.64] and − 1.26 [− 1.85, − 0.68], respectively. The treatment efficiency compared to the placebo had a 1 point pain reduction within a 0–10 evaluation scale. Ketamine demonstrated optimal efficacy with a 1·26 point pain reduction on average.
Figure 4.

(a) Forest plot for drug efficiency of Amitriptyline. (b) Forest plot for drug efficiency of BTX-A. (c) Forest plot for drug efficiency of Gabapentin. (d) Forest plot for drug efficiency of Ketamine. (e) Forest plot for drug efficiency of Lidocaine. (f) Forest plot for drug efficiency of Morphine. (g) Forest plot for drug efficiency of Naloxone.
The PMA for BTX-A (Fig. 4b) and Naloxone (Fig. 4g) showed a low heterogeneity as the data was pooled from a single study.
Studies on Amitriptyline, Gabapentin, Lidocaine and Morphine had a high heterogeneity and a statistically insignificant drug efficacy (Fig. 4a,c,e,f). The mean difference of 95% CI was 0 indicating an insignificant treatment difference between the drugs and placebo based on the random effects model.
Opioids drugs
A meta-analysis was conducted with 4 studies (Fig. 5). A pooled MD of – 0.65 and a 95% CI [− 1.67, 0.37] was determined indicating an insignificant treatment effect of opioids drugs compared to a placebo. A statistically significant heterogeneity of 92% of (p-value < 0·01) was identified.
Figure 5.

Forest plot for drug efficiency of Opioids drugs*.
Network meta-analysis (NMA)
A NMA (Fig. 6) was completed for 34 studies. The nodes correspond to each intervention included within the network where the interventions with direct comparisons are linked with a line. The thickness of lines corresponds to the number of trials evaluating the comparison. A connected network was built based on the placebo which was mostly Tolterodine based on the original studies. The evaluations between interventions were supported by direct comparison and indirect comparison.
Figure 6.

Network plot where Placebo was the reference group with 34 studies and 32 interventions.
In the network with the placebo as the reference group, Gabapentin (Fig. 7) comprised of a MD equaling to – 1.49 (95% CI [− 2.76, − 0.23], p-value < 0.05) indicating a significant effect on reducing chronic pain and direct comparisons were made using 4 studies (Fig. 8a). The pooled MD of Botulinum and Ketamine were −1.06 and – 1.24, respectively. These were similar to the results in the PWA, but their 95% CI was 0 therefore showed insignificant effect on pain reduction compared to a placebo. Most combined interventions had a negative MD compared to a placebo with a 95% CI of 0 indicated statistically insignificant results for reducing pain.
Figure 7.

Forest plot for intervention efficiency compared to Placebo in NMA.
Figure 8.

Forest plot for intervention efficiency compared to Placebo in NMA with detailed direct and indirect comparisons.
Imipramine, Diosimin, Desipramine, Clobazam, Piroxicam and Tiagabine had not been directly compared to a placebo based on the identified data therefore the comparative treatment effected between them and a placebo was not possible to complete.
Subgroup analysis
A subgroup analyses was conducted for 24 studies within the meta-analysis to explore the sources of heterogeneity and unbiased estimation based on age, pain type, period and geographical location (Fig. 9). The sub-group analysis for pain type, time period and geographical location can be found in the Supplementary file whilst average age is shown below.
Figure 9.

Forest plot for the mean difference of pain scores between experimental group and control group across different mean age of participants.
Subgroup analysis for pain core difference based on different age groups
It showed that the heterogeneity among studies with participants who were older than 50 years old had changed with decreased I2 (I2 = 48% for “51–60”, I2 = 68% for “61–71”). A common effects model was chosen for subgroup “51–60”, which produced a higher estimation of pain reduction with a mean difference of – 1.46 (95% CI [− 1.74, − 1.18]). Based on the high heterogeneity (I2 > 50%), random effects models were built for other subgroups. The group with participants younger than 40 years older obtained a significant drug efficiency (MD − 1·05, 95% CI [− 1.85, − 0.24]). The pooled drug effects (Fig. 9) in the 41–50 and 61–71 years of age groups were much lower than the overall treatment effect of NSAID drugs identified in the PMA. The 95% CI of 0 indicated statistically ineffective compared to the placebo. The random effects models showed the decrease of heterogeneity indicating that age may be a source of heterogeneity.
Sensitivity analysis
The sensitivity analysis was conducted (Fig. 10) for the PMA where some studies influenced the pooled results compared to the overall estimation (− 0.89). To test this theory, study number 71 and 100 were omitted and the pooled results were much lower, − 0.82 and – 0.79, respectively. Studies with Amitriptyline and Gabapentin produced unstable treatment results, and the absence of these showed an overestimation (study 81, 45) or underestimates (study 71, 100). Collectively, the high heterogeneity (I2 = 92% p-value < 0.01) was stable and a robust treatment effect with negative mean differences and a significant 95% CI remained. Therefore, the pooled treatment effects identified was credible.
Figure 10.

Forest plot for sensitivity analysis with studies in MA.
Publication bias
The funnel plots (Fig. 11) within the PMA indicated symmetry. Although several studies were not within the remit of the funnel, the Egger’s test showed a p value (0.22) larger than 0.05 which indicated the lack of small-study effects (Table 3).
Figure 11.
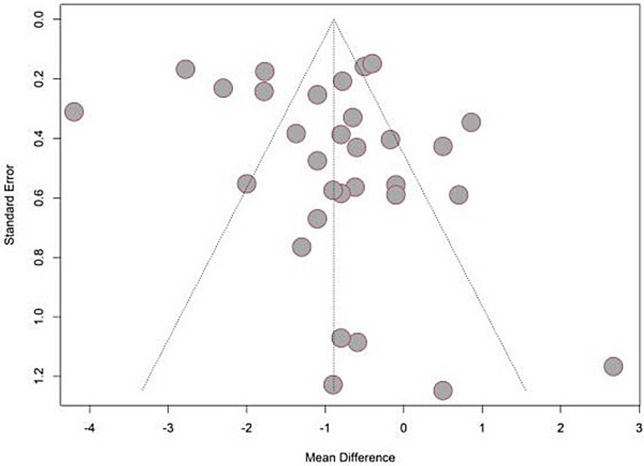
Funnel plot for studies used in PMA.
Table 3.
Egger test results for studies used in PMA.
| Test result | t = 1.24, df = 29, p-value = 0.2247 | |||
|---|---|---|---|---|
| Sample estimates | Bias | SE.bias | Intercept | SE.intercept |
| 1.49 | 1.2 | − 1.593 | 0.3737 | |
Discussion
We identified opioids and non-opioids were the two primary classes of pharmacological interventions in chronic pain management. Opioids are widely used in the management of cancer pain and non-cancer associated pain20,21. The long-term use of opioids in the management of chronic non-malignant pain has come under scrutiny more recently and is now recommended only if benefits of initiating treatment would significantly outweigh the potential risks, and possibly as an adjunct to the primary intervention22,23. Our study has shown that judicious use of non-opioid medications along with other treatment modalities could provide better outcomes in managing chronic pain thereby removing long-term side-effects observed during opioid therapy. With cancer patients increasingly being cured or achieving long term remission, prolonged use of opioids could result in aberrant behaviour and dependence. Awareness of an opioid crisis globally has prompted clinicians to exercise caution in their prescription habits, but the WHO supports the use of opioids including Fentanyl and Methadone as an essential class of medication for the management of cancer pain24,25.
The meta-analysis of baseline pain scores lacked statistical significance between experimental and control groups. The significant reduction in chronic pain scores of patients taking NSAID versus non-steroidal opioid drugs compared to patients given placebo under a random effects model. The presence of a significant drug efficiency with BTX-A and Ketamine is interesting although the pooled results of other drugs and interventions had statistically insignificant results with a 95% CI of 0. The pooled evidence indicated Ketamine showed the highest pain reduction (1.26) followed by BTX-A (0.98). Studies testing on other drugs including Amitriptyline, Gabapentin, Morphine and Lidocaine had a high heterogeneity and insignificant drug efficiency. Overall, evidence from the PMA showed a strong efficacy within the NSAIDs group with managing pain which were remarkably narrowed when exclusive trials with low risk of bias were included26–28.
In this study, a pairwise meta-analysis and NMA consolidating the evidence of 46 studies was carried out, with the former comparing several different opioids. Morphine has traditionally been used for the management of moderate to severe chronic pain29. Despite morphine being a potent analgesic [MD 0.01 (95% CI [− 1.18, 1.21], newer opioids are now being employed owing to their superior safety profile. Oxycodone and Fentanyl appear to be popular due to better availability and vast clinical experience including the well accepted effectiveness demonstrated, as per patient and clinically reported outcomes. Our results are aligned to these trends where the effectiveness is shown to include a MD 1.77 (95% CI [− 2.11, − 1.43]) for Oxycodone and a MD of − 0.90 (95% CI [− 2.03, 0.23])] for Fentanyl (32). However, untoward gastrointestinal effects (constipation, nausea, and vomiting) still remain a major concern with opioid use and are often responsible for discontinuation of treatment30,31. Recent evidence favours the use of a combination of oxycodone and naloxone in patients with chronic pain (after ensuring that there is no cause for porto-systemic anastomosis), to offer an improved bowel function without any effective change in analgesia32. The concerns of developing tolerance, opioid-induced hyperalgesia, aberrant behaviour and dependence with opioids is a pragmatic reason to develop effective alternative treatment modalities especially for vulnerable individuals. In pairwise comparison, we observed Ketamine to be superior to other pharmacological interventions with a mean difference MD − 1.26 (95% CI [− 1.85, − 0.68]).
There are several guidelines recommending the use of Pregabalin, Gabapentin, Duloxetine, and Amitriptyline as first line drugs in the management of neuropathic pain33–35. However, the use of gabapentinoids is being challenged as it lacks favourable robust evidence for efficacy against pain syndromes other than fibromyalgia, post herpetic neuralgia and diabetic neuropathy, and many clinicians have also highlighted the potential for misuse and developing dependence36–38. The use of BTX-A, Ketamine, Ningmitai and THC for the management of various chronic pain conditions is popular and well established39–43 and our study shows the effective use of these as analgesics when compared to placebo. There is evidence to support the efficacy of BTX-A for the management of neuropathic pain although the sample sizes used in the studies were small and therefore the real-world applicability remains limited29. BTX-A is also used in management of myofascial pains44,45 although further evidence on the efficacy and tolerability within all populations, especially those with existing co-morbidities needs to be evaluated. Ketamine was found to be beneficial in managing some neuropathic pains46 and as an infusion the rates of serious adverse effects were found to be similar to placebo47,48. Further studies are required to gather evidence to better understand its psychedelic effects and its role in the management of PTSD, anxiety and depression. A renewed use of magnesium in managing chronic pain has been demonstrated in some literature49. Our results indicate similar evidence in the use of magnesium, but will require further research to determine the efficacy, safety and effectiveness in managing short, medium and long-term pain.
The NMA provided more reliable results with direct and indirect comparisons between different drugs under different study designs. However, only a small number of multi-arm trials were eligible and the distribution of trials studying different drugs was uneven. It resulted in the lack of direct evidence of certain drugs and their relative efficacy in the network was unstable due to excessive reliance on indirect comparisons. Therefore, well designed and robust clinical trials should be conducted to verify the efficacy of pharmaceutical interventions used in chronic pain management.
Conclusion
To the best of our knowledge, this is the first pairwise MA and NMA reporting the synthesis of the prevalence of the efficacy of pharmacological treatments used in the management of chronic pain with a large sample size of 17,708 participants. Management of long-term chronic pain needs to be prioritised for several reasons including humanitarian, the strain on the healthcare systems and the impact on the economy due to loss of productivity. The use of pharmaceutical agents in the long-term management of chronic pain has been debated for several decades, yet there has not been a consensus on this matter. This study supports the importance of generating better evidence by way of robust clinical trials, the need for drafting clinical guidelines that is pragmatic, practical as well as clinically significant and the use of better data-connectivity methods to improve clinical practice in the real-world.
Supplementary Information
Acknowledgements
Dr Anish Thillainathan involved in formatting process.
Appendix
See Table 4.
Table 4.
Interventions used in studies.
| Study number | Author | Intervention abbreviation | Intervention details |
|---|---|---|---|
| 1 | Weizman et al. | THC | Cannabis |
| 2 | Krebs et al. | Opioid | Opioid and nonopioid medication therapy |
| 3 | AbdelHafeez et al. | Gabapentin | Gabapentin 2700 mg daily |
| 4 | Bushey et al. | Opioid | Analgesic |
| 5 | Bruehl et al. | Morphine + Naloxone | Morphine and Naloxone |
| 6 | Worley et al. | Buprenorphine/Naloxone | Buprenorphine/naloxone |
| 7 | Dindo et al. | ACT | Acceptance and Commitment Therapy |
| 8 | Hruschak et al. | IPGT | Psychoeducation, motivational interviewing, cognitive Behavioral therapy, mindfulness, and peer suppor |
| 9 | Azevedo et al. | Opioid | Opioid |
| 10 | Gudin et al. | NKTR-181 | NKTR-181 administered at doses of 100–600 mg twice daily |
| 11 | Stahl et al. | Venlafaxine | Lower-dose venlafaxine (≤ 150 mg/day) |
| 12 | Schliessbach et al. | Imipramine | Imipramine 75 |
| 13 | Mohamed et al. | Morphine | Topical morphine (in 1 of 3 doses: 5, 10, or 15 mg) |
| 14 | Schliessbach et al. | Oxycodone + Imipramine + Clobazam | Oxycodone 15 mg, imipramine 75 mg, clobazam 20 mg |
| 15 | Hermans et al. | Naloxone | 0 mg morphine or 0.2 mg/mL Naloxone) and placebo (2 mL Aqua) group |
| 16 | Todorov et al. | Gabapentin + Tiagabine | Gabapentin and Tiagabine |
| 17 | Sadatsune et al. | Gabapentin | Gabapentin Group received 600 mg of gabapentin preoperatively, one hour prior to surgery, and Control Group received placebo |
| 18 | Edwards et al. | Opioid | Oral opioid therapy |
| 19 | Katz et al. | Naproxen + Tanezumab | Intravenous tanezumab 200 μg/kg plus oral placebo (n = 88), intravenous placebo plus oral naproxen 500 mg twice a day (n = 88), or intravenous placebo plus oral placebo (n = 41) |
| 20 | Hayek et al. | Opioid + Bupivacaine | opioid with bupivacaine |
| 21 | Schliessbach et al. | Clobazam | Received a single oral dose of clobazam 20 mg or active placebo tolterodine 1 mg |
| 22 | Bruehl et al. | Opioid | Opioid |
| 23 | Kim et al. | Nefopam | Infused with the same volume of saline or nefopam (0.2 mg/kg bolus, 120 μg/kg/h continuous infusion) during surgery |
| 24 | Eisenach et al. | Ketorolac | Drug administration |
| 25 | Rauck et al. | Adenosine/Clonidine | Intrathecal clonidine, 100 μg, or adenosine, 2 mg |
| 26 | Buchheit et al. | Valproate | Oral valproic acid |
| 27 | Papadokostakis et al. | Calcitonin | 200 IU intranasal salmon calcitonin and 1000 mg of oral calcium daily |
| 28 | Gould et al. | Desipramine | Desipramine titrated to reach a serum concentration level of 15 to 65 ng/mL; |
| 29 | Schnitzer et al. | D-cycloserine | d-Cycloserine |
| 30 | Nenke et al. | Hydrocortisone | 10 mg/m2/day of oral hydrocortisone in three divided doses o |
| 31 | Sopata et al. | Opioid | opioids |
| 32 | Kendall et al. | Lidocaine | 1.5 mg/kg bolus of intravenous lidocaine followed by a 2 mg/kg/h infusion |
| 33 | Hongo et al. | Risedronate + Elcatonin | risedronate plus elcatonin |
| 34 | Amr and Yousef | Venlafaxine + Gabapentin | Venlafaxine 37.5 mg/day, gabapentin 300 mg/day |
| 35 | Pedersen et al. | Codeine + Paracetamol | 30 mg codeine and 400 or 500 mg of paracetamol |
| 36 | Choi et al. | Lidocaine | The patients received 2 mg/kg of lidocaine followed by continuous infusions of 3 mg/kg/h of lidocaine |
| 37 | Bruehl et al. | Morphine + Naloxone | Naloxone (8 mg), morphine (0.08 mg/kg) |
| 38 | Chrubasik et al. | Capsicum | Cream containing capsaicin 0.05% |
| 39 | Schliessbach et al. | Oxycodone | Oxycodone 15 mg |
| 40 | Bruehl and Chung | Naloxone | 8 mg dose of naloxone |
| 41 | Bruehl et al. | Naloxone + Morphine | Naloxone, morphine |
| 42 | Burns et al. | Naloxone + Morphine | Naloxone and morphine |
| 43 | Eker et al. | Lidocaine | Group I (n = 26) received 7 mL 0.5% lidocaine |
| 44 | Kim et al. | Opioid | Opioid therapy |
| 45 | Kimos et al. | Gabapentin | Gabapentin |
| 46 | Narang et al. | Opioid | Opioids |
| 47 | Peyton et al. | Ketamine | Ketamine |
| 48 | Katz et al. | Bupropion | Bupropion |
| 49 | Hashmi et al. | Lidocaine | Lidocaine |
| 50 | Shimoyama et al. | Fentanyl | Fentanyl |
| 51 | Wreje and Brorsson | Sterile water | Sterile water |
| 52 | Han et al. | BTX-A | Botulinum toxin type A |
| 53 | Rauck et al. | Hydrocodone | Hydrocodone 20–100 mg every 12 h) |
| 54 | Kim et al. | Pregabalin | pregabalin |
| 55 | Lee et al. | BTX-A | Botulinum Toxin Injection |
| 56 | Rashiq et al. | Fentanyl | Opioid |
| 57 | Kang et al. | Ketamine | 0.12 mg/kg/h of ketamine |
| 58 | Lipton et al. | Erenumab | Erenumab 70 and 140 mg |
| 59 | Williamson et al. | Duloxetine | Duloxetine |
| 60 | Guo et al. | Celecoxib Eperisone | Celecoxib Eperisone |
| 61 | Damjanov et al. | ACS | Autologous conditioned serum (ACS; marketed as Orthokine®) |
| 62 | Abd-Elshafy et al. | Bupivacaine |
Drug: Dexmedetomidine isobaric bupivacaine 0.5% (0.3 ml/kg) and dexmedetomidine (1 mcg/kg) Drug: Bupivacaine isobaric bupivacaine 0.5% (0.3 ml/kg) |
| 63 | Levesque et al. | BTX + Ropivacaïne |
Drug: botulinum toxin A + ropivacaïne Drug: Ropivacaïne |
| 64 | Maher et al. | Ketamine | Ketamine |
| 65 | Barry et al. | Methadone | Methadone |
| 66 | Shokeir and Mousa | Bupivacaine | Bupivacaine |
| 67 | Scudds et al. | Lidocaine | Lidocaine |
| 68 | Gimbel et al. | Buccal buprenorphine | Buccal buprenorphine |
| 69 | Matsuoka et al. | Duloxetine | Duloxetine 20 mg |
| 70 | Yurekli et al. | Sodium valproate | Sodium valproate |
| 71 | Maarrawi et al. | Amitriptyline | Amitriptyline |
| 72 | Li et al. | Ropivacaine + Dexamethasone | Single 20-ml injection of 0.50% ropivacaine plus 10 mg dexamethasone |
| 73 | Almog et al. | THC | THC: 0.5 mg, 1 mg |
| 74 | Wylde et al. | Bupivacaine | Anaesthetic with 3 mL of 0.5% plain bupivacaine |
| 75 | Matsukawa et al. | Cernitin + Tadalafil | Tadalafil |
| 76 | Haddad et al. | Apomorphine | Apomorphine |
| 77 | de Vries et al. | THC | Tetrahydrocannabinol |
| 78 | Urquhart et al. | Amitriptyline | Amitriptyline; 25 mg per day |
| 79 | Lichtman et al. | Nabiximols | Nabiximols |
| 80 | Schiphorst et al. | Acetaminophen/Tramadol | Acetaminophen/tramadol 325 mg/37.5 mg |
| 81 | Cardenas et al. | Amitriptyline | Amitriptyline |
| 82 | Arnold et al. | Milnacipran | Chronic pain |
| 83 | Wasan et al. | Morphine | Morphine |
| 84 | Baron et al. | Tapentadol/Pregabalin | Tapentadol PR 300 mg/day + pregabalin |
| 85 | Portenoy et al. | Fentanyl | Fentanyl |
| 86 | Likar et al. | Morphine | Morphine hydrochloride |
| 87 | Schwartzman et al. | Ketamine | Ketamine |
| 88 | Chu et al. | Morphine | Morphine |
| 89 | Sandrini et al. | BoNTA | Onabotulinum toxin A |
| 90 | Mahowald et al. | BoNTA | Botulinum Toxin Type A |
| 91 | Loftus et al. | Ketamine | Ketamine infusions |
| 92 | Lehmann et al. | Fentanyl | Transdermal fentanyl |
| 93 | Kahlenberg et al. | Celecoxib | Celecoxib |
| 94 | Silberstein et al. | Topiramate | Topiramate |
| 95 | Burgher et al. | Lidocaine | Lidocaine and either clonidine (200 or 400mcg) or triamcinolone |
| 96 | McCleane | Phenytoin | Phenytoin (Parke Davis) |
| 97 | Naliboff et al. | Opioid | Opioids |
| 98 | Booth et al. | Morphine | 300 mcg spinal morphine and 1 g acetaminophen |
| 99 | Lee et al. | Rowatinex/Ibuprofen | Rowatinex 200 mg/ibuprofen 600 mg |
| 100 | Levendoglu et al. | Gabapentin | Gabapentin |
| 101 | Yousef and Alzeftawy | Opioid | Oral perixicam |
| 102 | Yelland et al. | Gabapentin | Gabapentin |
| 103 | Yucel et al. | Venlafaxine | Venlafaxine |
| 104 | Hudson et al. | Nortriptyline | Nortriptyline |
| 105 | Rauck et al. | Ziconotide | Ziconotide |
| 106 | Sandner-Kiesling et al. | Naloxone + Oxycodone | Oxycodone PR/naloxone PR |
| 107 | Wang et al. | Diosmin | Diosmin |
| 108 | Hawley et al. | Lidocaine | Lidocaine |
| 109 | Mathieson et al. | Pregabalin | Pregabalin at a dose of 150 mg |
| 110 | Wetzel et al. | Nonopioid analgesic drugs | Oral nonopioid analgesic drug |
| 111 | Khan et al. | Lidocaine + Pregabalin | Pregabalin |
| 112 | Clarke et al. | Gabapentin | Gabapentin |
| 113 | Ma et al. | Oxycodone | Oxycodone |
| 114 | J. H. Lee and C. S. Lee | TA-ER | Tramadol hydrochloride 75-mg/acetaminophen 650-mg |
| 115 | Imamura et al. | Lidocaine | Paraspinous lidocaine injection |
| 116 | Baron et al. | Tapentadol | Tapentadol |
| 117 | Kim et al. | Lidocaine + Magnesium | Lidocaine (L), magnesium (M |
| 118 | Iwamura et al. | Eviprostat | Eviprostat |
| 119 | Zhang et al. | Ningmitai | Ningmitai Capsule |
Author contributions
A.S. and G.D. developed the study protocol and embedded this within the POP project. G.D. and J.Q.S. designed and completed the study analysis. The data extraction was completed by H.C. and C.D. All authors critically appraised and commented on previous versions of the manuscript. All authors read and approved the final manuscript. All authors consented to publish this manuscript.
Funding
University College London Hospitals NHS Foundation Trust.
Data availability
The authors will consider sharing the dataset gathered upon receipt of reasonable requests.
Code availability
The authors will consider sharing the novel code created upon receipt of reasonable requests.
Competing interests
AS has received funding from Medtronic and Nevro Corp USA. PP has received research grants from Novo Nordisk, Queen Mary University of London, John Wiley & Sons, Otsuka, outside the submitted work. AB has received speaker fees and has been an advisory board member from Pfizer, Vectura-Fertin and Reckitt. All other authors report no conflict of interest. The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health and Social Care or the Academic institutions.
Footnotes
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
These authors contributed equally: Ash Shetty, Gayathri Delanerolle, Heitor Cavalini and Chunli Deng.
Supplementary Information
The online version contains supplementary material available at 10.1038/s41598-023-49761-3.
References
- 1.Dahlhamer J, Lucas J, Zelaya C, et al. Prevalence of chronic pain and high-impact chronic pain among adults: United States, 2016. MMWR Morb. Mortal. Wkly. Rep. 2018;67:1001–1006. doi: 10.15585/mmwr.mm6736a2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zimmer Z, Fraser K, Grol-Prokopczyk H, Zajacova A. A global study of pain prevalence across 52 countries: examining the role of country-level contextual factors: Examining the role of country-level contextual factors. Pain. 2022;163:1740–1750. doi: 10.1097/j.pain.0000000000002557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brown CA, Lilford RJ. The stepped wedge trial design: A systematic review. BMC Med. Res. Methodol. 2006;6:54. doi: 10.1186/1471-2288-6-54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Turk DC, Monarch ES. Biopsychosocial Perspective on Chronic Pain. Psychological Approaches to Pain Management: A Practitioner’s Handbook. 2. Guilford; 2002. [Google Scholar]
- 5.Li T, Puhan MA, Vedula SS, et al. Network meta-analysis-highly attractive but more methodological research is needed. BMC Med. 2011;9:79. doi: 10.1186/1741-7015-9-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Caldwell D, Ades A, Higgins J. Simultaneous comparison of multiple treatments: Combining direct and indirect evidence. BMJ. 2005;331:897–900. doi: 10.1136/bmj.331.7521.897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Opioid Overdose. Who.int. www.who.int/news-room/fact-sheets/detail/opioid-overdose.
- 8.Opioid Opioid overdose crisis: Time for a radical rethink. Lancet Public Health. 2022;7:e195. doi: 10.1016/S2468-2667(22)00043-3. [DOI] [PubMed] [Google Scholar]
- 9.Berterame S, Erthal J, Thomas J, et al. Use of and barriers to access to opioid analgesics: A worldwide, regional, and national study. Lancet. 2016;387(10028):1644–1656. doi: 10.1016/S0140-6736(16)00161-6. [DOI] [PubMed] [Google Scholar]
- 10.Jansen JP, Fleurence R, Devine B, et al. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: Report of the ISPOR task force on indirect treatment comparisons good research practices: Part 1. Value Health. 2011;14(4):417–428. doi: 10.1016/j.jval.2011.04.002. [DOI] [PubMed] [Google Scholar]
- 11.Efthimiou O, Debray TP, van Valkenhoef G, et al. GetReal in network meta-analysis: A review of the methodology. Res. Synth. Methods. 2016;7(3):236–263. doi: 10.1002/jrsm.1195. [DOI] [PubMed] [Google Scholar]
- 12.Dallenbach KM. Pain: History and present status. Am. J. Psychol. 1939;52:331. [Google Scholar]
- 13.Levene JL, Weinstein EJ, Cohen MS, et al. Local anesthetics and regional anesthesia versus conventional analgesia for preventing persistent postoperative pain in adults and children: A Cochrane systematic review and meta-analysis update. J. Clin. Anesth. 2019;55:116–127. doi: 10.1016/j.jclinane.2018.12.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Campbell, J. (1996, November 11). Presidential Address. Speech given at the American Pain Society, Washington, DC.
- 15.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. (National Academies Press, 2011). [PubMed]
- 17.Pain Management Best Practices Inter-Agency Task Force Report: Updates, Gaps, Inconsistencies, and Recommendations. (U. S. Department of Health and Human Services, 2019). https://www.hhs.gov/ash/advisory-committees/pain/reports/index.html.
- 18.Borenstein M, Hedges LV, Higgins JP, Rothstein HR. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods. 2010;1:97–111. doi: 10.1002/jrsm.12. [DOI] [PubMed] [Google Scholar]
- 19.Rothstein HR, Sutton AJ, Borenstein M. Publication Bias in Meta Analysis: Prevention, Assessment and Adjustments. Wiley; 2005. [Google Scholar]
- 20.Busse JW, Wang L, Kamaleldin M, et al. Opioids for chronic noncancer pain: A systematic review and meta-analysis: A systematic review and meta-analysis. JAMA. 2018;320:2448–2460. doi: 10.1001/jama.2018.18472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain: United States, 2022. MMWR Recomm. Rep. 2022;71:1–95. doi: 10.15585/mmwr.rr7103a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Boudreau D, Von Korff M, Rutter CM, et al. Trends in long-term opioid therapy for chronic non-cancer pain. Pharmacoepidemiol. Drug Saf. 2009;18:1166–1175. doi: 10.1002/pds.1833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Noori A, Sadeghirad B, Wang L, et al. Comparative benefits and harms of individual opioids for chronic non-cancer pain: A systematic review and network meta-analysis of randomised trials. Br. J. Anaesth. 2022;129:394–406. doi: 10.1016/j.bja.2022.05.031. [DOI] [PubMed] [Google Scholar]
- 24.World Health Organization Model List of Essential Medicines: 22nd List, 2021. (WHO/MHP/HPS/EML/2021.02). (World Health Organization, 2021).
- 25.World Health Organization . Cancer Pain Relief, Second Edition, With a Guide to Opioid Availability. World Health Organization; 1996. [Google Scholar]
- 26.Trelle S, Reichenbach S, Wandel S, et al. Cardiovascular safety of non-steroidal anti-inflammatory drugs: Network meta-analysis. BMJ. 2011;342:c7086. doi: 10.1136/bmj.c7086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Da Costa BR, Pereira TV, Saadat P, et al. Effectiveness and safety of non-steroidal anti-inflammatory drugs and opioid treatment for knee and hip osteoarthritis: Network meta-analysis. BMJ. 2021;375:n2321. doi: 10.1136/bmj.n2321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Enthoven WTM, Roelofs PDDM, Deyo RA, van Tulder MW, Koes BW. Non-steroidal anti-inflammatory drugs for chronic low back pain. Cochrane Database Syst. Rev. 2016;2:012087. doi: 10.1002/14651858.CD012087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hary V, Schitter S, Martinez V. Efficacy and safety of botulinum A toxin for the treatment of chronic peripheral neuropathic pain: A systematic review of randomized controlled trials and meta-analysis. Eur. J. Pain. 2022;26:980–990. doi: 10.1002/ejp.1941. [DOI] [PubMed] [Google Scholar]
- 30.Meng Z, Yu J, Acuff M, et al. Tolerability of opioid analgesia for chronic pain: A network meta-analysis. Sci. Rep. 2017;7:1995. doi: 10.1038/s41598-017-02209-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Caraceni A, Hanks G, Kaasa S, et al. Use of opioid analgesics in the treatment of cancer pain: Evidence-based recommendations from the EAPC. Lancet Oncol. 2012;13:e58–68. doi: 10.1016/S1470-2045(12)70040-2. [DOI] [PubMed] [Google Scholar]
- 32.Huang L, Zhou J-G, Zhang Y, et al. Opioid-induced constipation relief from fixed-ratio combination prolonged-release oxycodone/naloxone compared with oxycodone and morphine for chronic nonmalignant pain: A systematic review and meta-analysis of randomized controlled trials. J. Pain Symp. Manage. 2017;54:737–748.e3. doi: 10.1016/j.jpainsymman.2017.07.025. [DOI] [PubMed] [Google Scholar]
- 33.Alberti FF, Becker MW, Blatt CR, Ziegelmann PK, da Silva Dal Pizzol T, Pilger D. Comparative efficacy of amitriptyline, duloxetine and pregabalin for treating fibromyalgia in adults: An overview with network meta-analysis. Clin. Rheumatol. 2022;41:18965–18978. doi: 10.1007/s10067-022-06129-8. [DOI] [PubMed] [Google Scholar]
- 34.Urquhart DM, Wluka AE, van Tulder M, et al. Efficacy of low-dose amitriptyline for chronic low back pain: A randomized clinical trial: A randomized clinical trial. JAMA Intern. Med. 2018;178:1474–1481. doi: 10.1001/jamainternmed.2018.4222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Sankar V, Oommen AE, Thomas A, Nair JV, James JS. Efficacy, safety and cost effectiveness of amitriptyline and pregabalin in patients with diabetic peripheral neuropathy. Indian J. Pharm. Sci. 2017 [Google Scholar]
- 36.Wiffen PJ, Derry S, Bell RF, et al. Gabapentin for chronic neuropathic pain in adults. Cochrane Database Syst. Rev. 2017;6:007938. doi: 10.1002/14651858.CD007938.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Shanthanna H, Gilron I, Rajarathinam M, et al. Benefits and safety of gabapentinoids in chronic low back pain: A systematic review and meta-analysis of randomized controlled trials. PLoS Med. 2017;14:e1002369. doi: 10.1371/journal.pmed.1002369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Evoy KE, Morrison MD, Saklad SR. Abuse and misuse of pregabalin and gabapentin. Drugs. 2017;77:403–426. doi: 10.1007/s40265-017-0700-x. [DOI] [PubMed] [Google Scholar]
- 39.Jin C, Chen Z, Zhang J. Meta-analysis of the efficacy of Ningmitai capsule on the treatment of chronic prostatitis in China. Medicine. 2018;97:e11840. doi: 10.1097/MD.0000000000011840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Whiting PF, Wolff RF, Deshpande S, et al. Cannabinoids for medical use: A systematic review and meta-analysis: A systematic review and meta-analysis. JAMA. 2015;313:2456–2473. doi: 10.1001/jama.2015.6358. [DOI] [PubMed] [Google Scholar]
- 41.Wei J, Zhu X, Yang G, et al. The efficacy and safety of botulinum toxin type A in treatment of trigeminal neuralgia and peripheral neuropathic pain: A meta-analysis of randomized controlled trials. Brain Behav. 2019;9:e01409. doi: 10.1002/brb3.1409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Zhang K, Liu Y, Yang W, et al. Efficacy and safety of Ningmitai capsule in patients with chronic prostatitis/chronic pelvic pain syndrome: A multicenter, randomized, double-blind, placebo-controlled trial. Urology. 2021;153:264–269. doi: 10.1016/j.urology.2021.01.018. [DOI] [PubMed] [Google Scholar]
- 43.Jing Z, Liying G, Zhenqing W, et al. Efficacy and safety of Ningmitai capsules in patients with chronic epididymitis: A prospective, parallel randomized controlled clinical trial. Evid Based Complement. Altern. Med. 2021;2021:9752592. doi: 10.1155/2021/9752592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Khalifeh M, Mehta K, Varguise N, Suarez-Durall P, Enciso R. Botulinum toxin type A for the treatment of head and neck chronic myofascial pain syndrome. J. Am. Dent. Assoc. 2016;147:959–973.e1. doi: 10.1016/j.adaj.2016.08.022. [DOI] [PubMed] [Google Scholar]
- 45.Meister MR, Brubaker A, Sutcliffe S, Lowder JL. Effectiveness of botulinum toxin for treatment of symptomatic pelvic floor myofascial pain in women: A systematic review and meta-analysis: A systematic review and meta-analysis. Female Pelvic. Med. Reconstr. Surg. 2021;27:e152–e160. doi: 10.1097/SPV.0000000000000870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Guimarães Pereira JE, Ferreira Gomes Pereira L, Mercante Linhares R, et al. Efficacy and safety of ketamine in the treatment of neuropathic pain: A systematic review and meta-analysis of randomized controlled trials. J. Pain Res. 2022;15:1011–1037. doi: 10.2147/JPR.S358070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Cohen SP, Bhatia A, Buvanendran A, et al. Consensus guidelines on the use of intravenous ketamine infusions for chronic pain from the American society of regional anesthesia and pain medicine, the American academy of pain medicine, and the American society of anesthesiologists. Reg. Anesth. Pain Med. 2018;1:47–50. doi: 10.1097/AAP.0000000000000808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Orhurhu V, Orhurhu MS, Bhatia A, Cohen SP. Ketamine infusions for chronic pain: A systematic review and meta-analysis of randomized controlled trials. Anesth. Analg. 2019;129:241–254. doi: 10.1213/ANE.0000000000004185. [DOI] [PubMed] [Google Scholar]
- 49.Park R, Ho AM-H, Pickering G, Arendt-Nielsen L, Mohiuddin M, Gilron I. Efficacy and safety of magnesium for the management of chronic pain in adults: A systematic review. Anesth. Analg. 2020;131:764. doi: 10.1213/ANE.0000000000004673. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The authors will consider sharing the dataset gathered upon receipt of reasonable requests.
The authors will consider sharing the novel code created upon receipt of reasonable requests.