

Abstract
Background:
Sub-optimal response in schizophrenia is frequent, warranting augmentation strategies over treatment-as-usual (TAU).
Methods:
We assessed nutraceuticals/phytoceutical augmentation strategies via network meta-analysis. Randomized controlled trials in schizophrenia/schizoaffective disorder were identified via the following databases: PubMed, MEDLINE, EMBASE, Scopus, PsycINFO, CENTRAL, and ClinicalTrials.gov. Change (Standardized Mean Difference=SMD) in total symptomatology and acceptability (Risk Ratio=RR) were co-primary outcomes. Secondary outcomes were positive, negative, cognitive, and depressive symptom changes, general psychopathology, tolerability, and response rates. We conducted subset analyses by disease phase and sensitivity analyses by risk of bias and assessed global/local inconsistency, publication bias, risk of bias, and confidence in the evidence.
Results:
The systematic review included 49 records documenting 50 studies (n=2,384) documenting 22 interventions. Citicoline (SMD=−1.05,95%CI=−1.85; −.24), L-lysine (SMD=−1.04,95%CI=−1.84;−.25), N-acetylcysteine (SMD=−.87,95%CI=−1.27;−.47) and sarcosine (SMD=−.5,95%CI=−.87−.13) outperformed placebo for total symptomatology. High heterogeneity (tau2=.10, I2=55.9%) and global inconsistency (Q=40.79, df=18, p=.002) emerged without publication bias (Egger’s test, p=.42). Sarcosine improved negative symptoms (SMD=−.65, 95%CI=−1.10; −.19). N-acetylcysteine improved negative symptoms (SMD=−.90, 95%CI=−1.42; −.39)/general psychopathology (SMD=−.76, 95%CI=−1.39; −.13). No compound improved total symptomatology within acute phase studies (k=7, n=422). Sarcosine (SMD=−1.26,95%CI=−1.91; −.60), citicoline (SMD=−1.05,95%CI=−1.65;−.44), and N-acetylcysteine (SMD=−.55,95%CI=−.92,−.19) outperformed placebo augmentation in clinically stable participants. Sensitivity analyses removing high-risk-of-bias studies confirmed overall findings in all phases and clinically stable samples. In contrast, the acute phase analysis restricted to low risk-of-bias studies showed a superior effect vs. placebo for N-acetylcysteine (SMD=−1.10,95%CI=−1.75,−.45), L-lysine (SMD=−1.05,95%CI=−1.55,−.19), omega-3 fatty acids (SMD=−.83,95%CI=−1.31,−.34) and withania somnifera (SMD=−.71,95%CI=−1.21,−.22). Citicoline (SMD=−1.05,95%CI=−1.86,−.23), L-lysine (SMD=−1.04,95%CI=−1.84,−.24), N-acetylcysteine (SMD=−.89,95%CI=−1.35,−.43) and sarcosine (SMD=−.61,95%CI=−1.02,−.21) outperformed placebo augmentation of TAU (“any phase”). Drop-out due to any cause or adverse events did not differ between nutraceutical/phytoceutical vs. placebo+TAU.
Conclusions:
Sarcosine, citicoline, and N-acetylcysteine are promising augmentation interventions in stable patients with schizophrenia, yet the quality of evidence is low to very low. Further high-quality trials in acute phases/specific outcomes/difficult-to-treat schizophrenia are warranted.
Keywords: Nutraceuticals, phytoceuticals, schizophrenia, treatment-resistance, systematic review, nutritional psychiatry, network meta-analysis, psychiatry, psychosis
Introduction
Schizophrenia and related disorders affect 23,6 million people worldwide, accounting for a significant burden 1, 2. People with schizophrenia often require long-term treatment with complex pharmacotherapy 3, especially in treatment-resistant cases 4. Nevertheless, up to 40% of patients fail to respond to standard antipsychotic treatment 5. While significant research is ongoing, currently, no novel mechanism-of-action medications for schizophrenia have been approved besides postsynaptic dopamine receptor antagonism 6. Hence, even small additional benefits from safe augmentation strategies are of potential value 7. Although 42 different pharmacologic augmentation strategies of antipsychotic agents were assessed in a previous umbrella review, the results were inconclusive due to the limited quality of the meta-analyzed studies and significantly greater effect sizes in lower-quality studies 8.
Nutraceuticals and phytoceuticals are increasingly used among non-pharmacological treatments due to their favorable safety and tolerability 9, 10. Yet, conclusive results are needed to establish their potential role in treating schizophrenia 11. Historically, the term nutraceutical has had various definitions 12, 13. Per previous umbrella reviews in this field, we refer to any nutrient-based intervention, such as vitamins, minerals, amino acids, and fatty acids 14. We also define phytoceuticals as any intervention that uses plant-based compounds such as herbal formulations 15.
Existing meta-analytic evidence 14, 15 and the most current World Federation of Societies of Biological Psychiatry (WFSBP) and Canadian Network for Mood and Anxiety Treatments (CANMAT) clinical guidelines 11 inform about the efficacy, safety, and tolerability of different nutraceuticals and phytoceuticals in the treatment of schizophrenia. However, no network meta-analysis (NMA) has been conducted to assess these compounds’ efficacy, acceptability, and tolerability in schizophrenia directly, except for a recent Bayesian NMA appraising selected compounds 16.
Therefore, the present NMA aimed to appraise the efficacy, acceptability, and tolerability of multiple nutraceuticals and phytoceuticals, either as mono- or augmentation therapy, in treating schizophrenia.
Methods
The present systematic review (SR) and NMA evaluated nutraceutical and phytoceutical interventions in schizophrenia using randomized controlled trials (RCTs). The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension statement for network meta-analysis (PRISMA-NMA) 17. The protocol was registered via PROSPERO (CRD42022375946).
Search strategy and selection criteria
We systematically searched PubMed/MEDLINE, EMBASE, Scopus, PsycINFO, Cochrane CENTRAL, and ClinicalTrials.gov from journal inception to October 17th, 2023. No language restriction was applied. The following search terms were adopted and augmented across different databases: psychosis, schizo*, nutraceuticals, phytoceuticals, and randomized controlled trials. The appendix (S1) details the search strategy. The electronic search was supplemented by a manual search of the reference list of all retrieved trials and relevant SRs and meta-analyses to identify additional relevant RCTs. Two authors (MB and MF) independently screened the papers and extracted data. Any disagreement was resolved by consensus with a third author (CC).
Inclusion criteria were: i) RCT; ii) inclusion of any nutraceutical/phytoceutical treatment, either as monotherapy or augmentation of treatment as usual (TAU), compared to either another nutraceutical/phytoceutical compound, placebo, TAU, or placebo + TAU; iii) involving adult (age ≥ 18 years) in- or outpatients with a primary diagnosis of schizophrenia or schizoaffective disorder, according to the Diagnostic and Statistical Manual of Mental Disorders (DSM), any edition/text revision, or International Classification of Disease (ICD), any edition; iv) providing quantitative data about the change in disease-specific symptomatology, measured through adequate rating scales, treatment response, all-cause drop-outs (acceptability) and, intolerability-related drop-outs (tolerability).
Excluded were studies with i) observational or non-randomized design; ii) without a suitable control group (e.g., studies comparing two different doses of the same nutraceutical/phytoceutical molecule); iii) involving < 10 patients per arm, consistent with most WFSBP/CANMAT guidelines 11; iv) crossover design not providing pre-cross-over data (otherwise included in the SR portion only); v) special populations, like first-episode psychosis (since a definitive diagnosis of schizophrenia is unclear), high-/ultra-high risk populations, pediatric populations (age < 18 years); vi) unstratified results for different diagnostic populations (e.g., schizophrenia and bipolar disorder merged altogether).
Study selection, extraction, and outcomes
The following data were extracted: author(s), year, nutraceutical/phytoceutical and control interventions, mean dose of the active intervention, study design (parallel-group or crossover), trial duration, sample size (total, cases, controls), mean age and % of females in each arm, diagnostic criteria and (semi)structured interview, acceptability, tolerability, efficacy measures as reported in RCTs for the primary outcome (mean difference in scoring at endpoint from baseline, response rate). We also recorded whether the outcomes were reported per intention-to-treat (ITT) (i.e., last observation carried forward [LOCF]) or per-protocol (i.e., completers). All outcomes were measured at the study endpoint. For crossover RCTs, only the pre-cross-over effect was considered. The following were deemed co-primary outcomes: i) efficacy, as the mean change in the total score of schizophrenia-specific rating scales, and ii) acceptability. Secondary outcomes were: i) mean change in positive, negative, cognitive, and depressive symptoms and general psychopathology, ii) intolerability-related drop-out, and iii) treatment response. Contact with study authors was attempted when data were unavailable.
Risk of bias, confidence in the evidence, and quality appraisal
The risk of bias was assessed using the Cochrane Risk of Bias tool, second edition (RoB2) 18. Confidence in the evidence for the primary outcomes was evaluated within the Confidence In Network Meta-Analysis (CINeMA) framework 19. Finally, an adapted version of the AMSTAR plus content total score 8 was employed to rate the quality of the included RCTs, weighted for the number of comparisons (score range = 0–7, owing to the following adapted items: 1) Blindness yes/no (score range 0–1); 2) sample size (n < 20 score = 0, n = 20–100 score 1, n > 100 score = 2); 3) findings replicated in at least one comparison (1 point) and n > 20 in at least one study arm (1 point); 4) ITT (no = 0, yes = 1); 5) High (score = 0) or low risk (score = 1) of bias at the Rob2 regressed against the primary efficacy outcome effect size (change in total PANSS score: SMD, 95%CI).
Data analysis
We performed a random-effect NMA within the frequentist framework using the netmeta package v.2.1–0, RStudio version 4.2.1. We computed standardized mean difference (SMD) for continuous outcomes and risk ratio (RR) for binary ones. For studies failing to report the mean changes but only baseline and endpoint data, the SMD and standard deviation (SD) were estimated for each study arm using the methods outlined in the Cochrane Handbook 20.
The homogeneity of direct evidence (within each pairwise comparison) was assessed using tau2. Global inconsistency was evaluated by considering a full-design-by-treatment model. Local inconsistency was measured with a node-splitting approach to assess the agreement between direct and indirect estimates for each outcome. The study node was the nutraceutical/phytoceutical molecule. Publication bias was measured for each outcome by visually examining the funnel plot and Egger’s test for studies with ≥ 10 participants 21.
The relative ranking of different nutraceutical/phytoceutical interventions was estimated using the surface under the cumulative ranking curves (SUCRA). The higher the SUCRA value, the better the rank of the intervention within the accounted series of interventions.
The following subgroup analyses were planned for efficacy outcomes: acute vs. maintenance phase schizophrenia and clozapine vs. non-clozapine antipsychotics. The following sensitivity analyses were planned for the co-primary outcomes: i) excluding studies with a high risk of bias and ii) focusing on schizophrenia studies only.
Results
The systematic search yielded 12,744 results, reduced to 11,754 after 990 duplicates were automatically detected and removed. Title and abstract screening led to 135 records eligible for the full-text screening. After the full-text assessment, 50 records were included in the SR 22–70. One record provided two independent studies 34. An exhaustive list of excluded studies with reasons is reported in the appendix, S8. The PRISMA flow diagram is summarized in Fig. 1. All included studies compared nutraceutical/phytoceutical compounds + TAU to placebo + TAU. Three studies did not enter the NMA synthesis: two37, 39 due to the lack of TAU and one22 due to unreliable TAU (Table 1).
Figure 1.
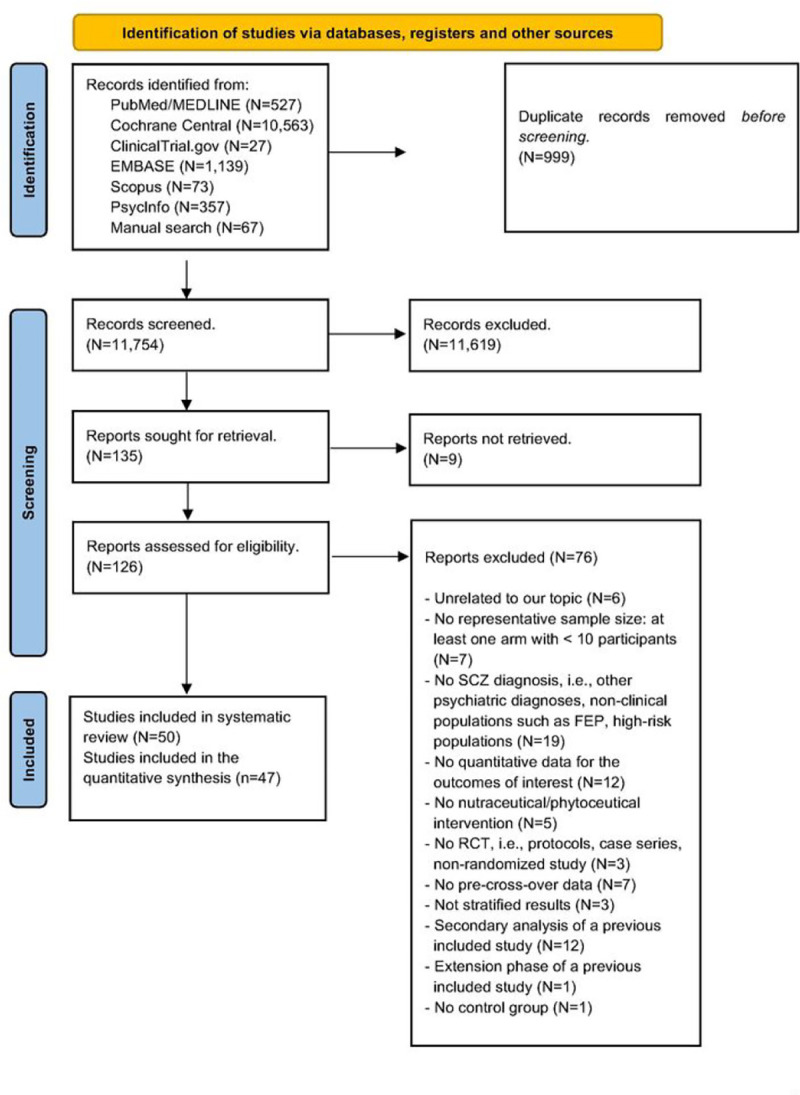
PRISMA 2020 flow diagram.
Table n.1:
Characteristics of included studies assessing nutraceuticals and phytoceuticals in treating schizophrenia.
| Author(s), Year | Population, N=sample size, PANSS baseline, if provided | Mean age in years. Female % | Diagnosis DSM/ICD and type of interview | Duration and design; ITT/PP analysis | Sponsor | Nutraceutical/phytoceutical intervention |
|---|---|---|---|---|---|---|
| Atmaca M et al., 2005 | Not better-specified phase of illness SCZ outpatients N=29 |
Age: 27.9 F: 78.9% |
DSM IV semi-structured interview (unspecified) | Eight weeks, parallel. Intent-to-treat analysis |
Not reported | Ginkgo biloba (300mg/day) +olanzapine (5 20mg/day; mean dose at week 8: 14.7mg/day) |
| Berk M. et al., 2008 | Clinically stable SCZ outpatients N=140 45% on clozapine, 20% on olanzapine Mean PANSS baseline 64 and 64.4 for groups I and II, respectively |
Age: 36.6 F: 30% |
DSM IV-TR, MINI | 24 weeks, parallel; Intent-to-treat analysis | A grant from the Stanley Medical Research Institute | N-acetylcysteine(2g/day) + antipsychotic treatment (mean CPZ-equivalent 716.4 mg/day) |
| Breier A. et al., 2018 | Clinically stable SCZ Spectrum outpatients (SCZ, schizophreniform, schizoaffective, NOS) N=60 The mean PANSS baseline was 56.6 and 56.4 for groups I and II, respectively. |
Age: 23.6 F: 21.66% |
DSM IV-TR, SCID | 52 weeks, parallel; intent-to-treat analysis | Funded by the Stanley Medical Research Institute (10T-002) | N-acetylcysteine (3.6g/day) +antipsychotics (mean CPZ-equivalent 130.9mg/day) |
| Chen EYH et al., 2011 | Clinically stable SCZ outpatients N=64 |
Age: 43.41 F: 20.3% |
DSM IV | 4. weeks, parallel; intent-to-treat analysis | Supported by a research grant from Afexa Life Sciences | Ginseng(200mg/day) +antipsychotics (mean CPZ-equivalent 964.54 mg/day) |
| Hosseininasab Met al., 2021 | Clinically stable SCZ outpatients with predominantly negative symptoms N=58 Mean baseline PANSS 66.8 and 70.6 for groups I and II, respectively |
Age: 48.55 F: not reported |
DSM-5, clinical interview based on DSM-5 | 16 weeks, parallel; per-protocol analysis | Grant number 83 from the Mazandaran University of Medical Sciences research council to N.H. | Nanocurcumin(160mg/day) +risperidone, perphenazine, or clozapine (mean CPZ-equivalent 950mg/day) |
| Miodownik C et al., 2019 | Clinically stable SCZ outpatients with persistent negative symptoms (SANS>30) N=38 Mean baseline PANSS 99.8 and 91.5 for groups I and II, respectively |
Age: 53.76 F: 34.2% |
DSM-IV | 24 weeks, parallel; intent-to-treat analysis | Not reported | Curcumin (3000mg/day) +antipsychotics (mean CPZ-equivalent 1009.1 mg/day) |
| Roffman JL et al., 2017 | Not better-specified phase of illness SCZ outpatients N=55 Baseline PANSS 74.5 and 79.7 for groups I and II, respectively |
Age: 45.54 F: 21.8% |
DSM-IV-TR, SCID | 12 weeks, parallel; intent-to-treat analysis | Funded by Pamlab and NIMH (R01MH101425, S10RR023043, S10RR023401, K24MH094614) | L-methyl-folate(15mg/day) +antipsychotics, antidepressants, or anticonvulsants |
| Roffman JL et al., 2013 | Clinically stable SCZ outpatients with persistent symptoms N=140 PANSS > 60 |
Age: 45.5 F: 28.6% |
DSM-IV-TR, SCID | 16 weeks, parallel; intent-to-treat analysis | NIMH grant R01MH070831 and the Howard Hughes Medical Institute Early Career Physician-Scientist Award. | Folate (2mg/day) and vitamin B12 (400mcg/day) +antipsychotics, antidepressants, or anticonvulsants |
| * Levine et al., 2006 | Clinically stable SCZ outpatients N=42 Mean baseline PANSS 94.4 and 93 in groups I and II, respectively |
Age: 40 F: not reported |
DSM-IV | 12 weeks, crossover; per-protocol analysis | Stanley Medical Research Institute grant (to RHB, JL) | Folate (2mg/day), pyridoxine (25mg/day), and vitamin B12 f400mcg/day) + antipsychotics, lithium, anticonvulsants (mean CPZ-equivalent 900mg/day) |
| Hill M et al., 2011 | Clinically stable SCZ outpatients with residual negative symptoms N=32 Mean baseline PANSS 69.6 and 75.3 for groups I and II, respectively |
Age: 45.9 F: 18.7% |
DSM-IV, clinical interview | 12 weeks, parallel; per-protocol analysis | Funded by the NARSAD 2003 Investigator Award | Folate (2mg/day) +antipsychotics |
| Krivoy A et al., 2017 | Acute SCZ outpatients treated with clozapine. N=47 Baseline PANSS >60 |
Age: 40.9 F: 31.9% |
DSM-IV-TR | Eight weeks, parallel; intent-to-treat analysis | grant from Stanley Medical Research Institute (grant 08–13T) | Vitamin D (14000IU/week) +clozapine (414.6mg/day |
| Sheikmoonesi F et al., 2016 | Not better-specified phase of illness SCZ outpatients with residual symptoms N=80 |
Age: 47.2 F: 0% |
DSM-IV-TR | 16 weeks, open, parallel; per-protocol analysis | supported by Mazandaran University of Medical Sciences (grant number: 15629) | Vitamin D3 (600000IU/month) +antipsychotics (mean CPZ-equivalent 350mg/day) |
| Farokhnia M et al., 2013 | Acute SCZ outpatients N=42 PANSS baseline > 60 (mean PANSS baseline 113.42 and 114.61 for groups I and II, respectively) |
Age: 32.7 F: 52.5% |
DSM-IV-TR, SCID | Eight weeks, parallel; intent-to-treat analysis | S.A. has received a grant from Tehran University of Medical Sciences | N-acetylcysteine(2g/day) +risperidone (up to 6mg/day; mean dose 4.2mg/day) |
| Sepehrmanesh Z et al.,2017 | Not better-specified phase of illness SCZ outpatients N=84 baseline PANSS >55 (mean baseline PANSS 104 and 87.7 in groups I and II, respectively) |
Age: 39 F: 51.8% |
DSM-IV-TR, SCID | 12 weeks, parallel; per-protocol analysis | funding from the research and technical council of Kashan University of Medical Sciences | N-acetylcysteine(1200mg/day) +antipsychotics |
| Qiao X et al., 2020 | Acute hospitalized aggressive inpatients with SCZ N=67 |
Age: 34.05 F: 47.7% |
ICD-10 | Eight weeks, parallel; intent-to-treat analysis | grants from The Three-Year Action Plan for The Construction of Public Health System in Shanghai, the National Natural Science Foundation of China, and Quantitative evaluation strategic research of interventions on relapse of schizophrenia | Omega-3 (EPA540mg/day, DFIA360mg/day) + |
| Fenton WS et al., 2001 | The not better-specified phase of illness SCZ outpatients or schizoaffective disorder and residual symptoms N=87 Mean baseline PANSS 74 and 76 for groups I and II, respectively |
Age: 40 F: 39% |
DSM-IV | 16 weeks, parallel; intent-to-treat analysis | grant from the Stanley Foundation/National Alliance for the Mentally III Research Institute | ethyl EPA(3g/day) +antipsychotics |
| Pawelczyk T et al., 2016 | Acute SCZ Outpatients with the first episode N=71 Mean baseline PANSS 98 |
Age: 23.2 F: 40.8% |
ICD-10, MINI | 26 weeks, parallel; intent-to-treat analysis | grant no. N N402 243435 obtained from the Polish Science National Center | Omega-3 (EPA 1.32g/day, DHA 0.88g/day)+antipsychotics (mean CPZ-equivalent 263.16mg/day) |
| Emsley R et al., 2002 | Not better-specified phase of illness SCZ outpatients and persistent symptoms despite six months of antipsychotic treatment N=40 Baseline PANSS >50 |
Age: 44.9 F: not reported |
DSM-IV | 12 weeks, parallel; intent-to-treat analysis | grant from the Medical Research Council of South Africa | ethyl EPA(3g/day) +antipsychotics (mean CPZ-equivalent lOllmg/day) |
| * Emsley R et al., 2014 | Clinically stable SCZ outpatients who discontinued antipsychotics after 2–3 years of treatment N=33 |
Age: 29.7 F: 27.3% |
DSM-IV, SCID | Two years, parallel; intent-to-treat analysis | Stanley Medical Research Institute (Grant #09T-1281) | Omega3 (EPA 2g/day, DFIA I g/day) and alpha-lipoic acid (300mg/day). Note: once randomized, the patient discontinued the antipsychotic treatment. |
| Jamilian H et al., 2014 | Not better-specified phase of illness SCZ outpatients N=60 Baseline PANSS >60 (mean baseline PANSS 96.13 and 98.26 in groups I and II, respectively) |
Age: 31.5 F: 48.35% |
DSM-IV-TR, clinical interview | Eight weeks, parallel; intent-to-treat analysis | Deputy of Research of Arak University of Medical Sciences | Omega3 (1 g/day) +antipsychotics |
| Peet M et al., 2001 (1) | Not better-specified phase of illness SCZ outpatients N=45 Baseline PANSS>40 |
Age: 43.3 F: 33.3% |
DSM-IV | 12 weeks, parallel; intent-to-treat analysis | Laxdale Limited | EPA(2g/day) +antipsychotics |
| DFIA(2g/day) +antipsychotics | ||||||
| Peet M et al., 2001 (2) | Not better-specified phase of illness SCZ outpatients N=26 | Age: 35.5 F: 40% |
DSM-IV | 12 weeks, parallel; per-protocol analysis | Funded by Laxdale Limited | EPA(2g/day)+antipsychotics (if necessary) |
| Peet M et al., 2002 | Not better-specified phase of illness SCZ outpatients on persistent ongoing symptoms N=115 PANSS>50 |
Age: 37 F: 33.91% |
DSM-IV | 12 weeks, parallel; intent-to-treat analysis | funded by Laxdale Ltd. | ethyl EPA (1–4g/day)+antipsychotics |
| Tang W et al., 2020 | Clinically stable SCZ outpatients N=80 PANSS baseline <60 |
Age: 28.4 F: 37.5% |
DSM-IV, SCID | 12 weeks, parallel; per-protocol analysis | supported by the National Key Research and Development Program of China, the National Natural Science Foundation of China, the Shanghai Science and Technology Commission Foundation | Omega3 (EPA720mg/day, DFIA 480mg/day)+olanzapine (mean dose 17.81mg/day) |
| Ritener MS et al., 2010 | Clinically stable SCZ outpatients or schizoaffective disorder N=40 |
Age: 33.3 F: 22.5% |
DSM-IV | Eight weeks, parallel; per-protocol analysis | Clinical Trials Grant (#06TGF-911) from the Stanley Medical Research Institute, Bethesda | L-theanine (400mg/day)+antipsychotics (mean CPZ-equivalent 520mg/day) |
| * Jamilian H et al., 2021 | Not better-specified phase of illness SCZ outpatients N=51 Mean baseline PANSS 81.1 and 80.6 in groups I and II, respectively |
Age: 45.1 F: not reported |
DSM-IV-TR, semi-structured interview not specified | 12 weeks, parallel; per-protocol analysis | Arak University of Medical Sciences (AUMS) funds this study | Selenium (200mcg/day) and probiotic (L.acidophilus, B.lactis, B.bifidum, and B.longum, each 2×10^9/day |
| Ghaderi A et al., 2019 | The not better-specified phase of illness SCZ outpatients N=60 Mean baseline PANSS 85.4 and 87.5 in groups I and II, respectively |
Age: 44 F: 6.7% |
DSM-IV-TR, semi-structured interview not specified | 12 weeks, parallel; intent-to-treat analysis | The research grant provided by the Research Deputy of Kashan University of Medical Sciences (KAUMS) | VitaminD3 (50000IU/2 weeks) and probiotics (L.acidophilus, B.lactis, B.bifidum, and B.longum, each 2x10^9/day)+chlorpromazine (300– 1000mg/day) |
| Dakhale GN et al., 2005 | Acute SCZ outpatients N=40 |
Age: 38.5 F: not reported |
DSM-IV | Eight weeks, parallel; intent-to-treat | Not reported | Vitamin C (500mg/day) +olanzapine (10mg/day) or quetiapine (200mg/day) or ziprasidone(40mg/day) |
| Zhang XY et al., 2000 | Not better-specified phase of illness SCZ outpatients N=82 |
Age: 44.4 F: 42.7% |
ICD-10 | 12 weeks, parallel; intent-to-treat analysis | Not reported | Ginkgo biloba (360mg/day)+haloperidol (12–24 mg/day; mean dose 16.6mg/day) |
| Doruk A et al., 2008 | Not better-specified phase of illness TRS SCZ outpatients N=42 |
Age: 30.85 F: 33.3% |
DSM-IV-TR, SCID | 12 weeks, parallel; per-protocol analysis | Not reported | Ginkgo biloba(120mg/day)+clozapine(415mg/day |
| Chengappa KNR et al., 2018 | Acute SCZ outpatients or schizoaffective disorder and psychotic symptoms exacerbation N=68 |
Age: 46.3 F:48.5% |
DSM-IV-TR, MINI | 12 weeks, parallel; intent-to-treat analysis | funded by the Stanley Medical Research Institute, Maryland, under grant award 12T-001 | Whitania somnífera (1000mg/day) SE+antipsychotics, antidepressants, mood stabilizers, anxiolytics, hypnotics/sedatives (OLA-equivalents 16.39 mg/day for subjects taking atypical antipsychotics) |
| Miyaoka T et al., 2014 | Clinically stable SCZ outpatients with treatment-resistant N=117 |
Age: 46.5 F: 37.6% |
DSM-IV-TR, SCID | Four weeks, parallel; intent-to-treat analysis | supported by Grants in Aid for the Ministry of Health, Labor, and Welfare of Japan | Yokukansan (7.5g/day)+ antipsychotics (mean CPZ-equivalent 2037.2mg/day) |
| Dickerson F et al., 2021 | Not better specified phase of illness SCZ outpatients or schizoaffective disorder with stable symptoms (residual psychotic symptoms or at least moderate severity) N=64 Baseline PANSS>60 |
Age: 44.25 F: 23.5% |
DSM-5, SCID | 16 weeks, parallel; intent-to-treat analysis | supported by the Stanley Medical Research Institute (15T-001 to FD) | Glucoraphanin 16 mg Tablets (6 Tablets/day) +antipsychotics. 6 Tablets/day yields about 100 μmol of sulforaphane. |
| Xiao S-F et al., 2011 | Not better-specified phase of illness SCZ outpatients and dominant negative symptoms N=80 Mean baseline PANSS 63.9 and 72.1 in groups I and II, respectively |
Age: 50.5 F: 51.2% |
DSM-IV | Eight weeks, parallel; per-protocol analysis | supported by the grant of Stanley Medical Research Institute (No. 021–005), USA | Sarsasapogenin(200mg/day)+ risperidone (range 2–4mg/day; mean dose 3.33mg/day |
| Lane K-Y et al., 2006 | Not better-specified phase of illness TRS SCZ outpatients N=20 Mean baseline PANSS 78.2 and 77.7 for groups I and II, respectively |
Age: 36.1 F: 30% |
DSM-IV, SCID | Six weeks, parallel; intent-to-treat analysis | supported by the National Science Council, the National Health Research Institutes, the Development Center for Biotechnology, the National Research Program for Genomic Medicine, the Committee on Chinese Medicine and Pharmacy at the Department of Health, and the China Medical University (Taiwan) | Sarcosine(2g/day)+clozapine (mean dose 306mg/day) |
| Lane K-Y et al., 2005 | Acute SCZ outpatients N=65 The mean baseline PANSS was 86.5 for the sarcosine group, 82.2 for the D-serine group, and 80.7 for the placebo group. |
Age: 34 F: 44.4% |
DSM-IV, SCID | Six weeks, parallel; per-protocol analysis | supported by grants from the National Science Council (Taipei), the National Health Research Institutes (Taipei), the China Medical University (Taiwan) | Sarcosine (2g/day) +risperidone (mean dose 3.9mg/day) |
| D-serine(2g/day) +risperidone(mean dose 4.1mg/day) | ||||||
| Lane H-Y et al., 2010 | Not better-specified phase of illness SCZ outpatients N=60 The mean baseline PANSS was 85.3 for the sarcosine group, 88.4 for the D-serine group, and 88.7 for the placebo group |
Age: 30.5 F: 40% |
DSM-IV, SCID | Six weeks, parallel; per-protocol analysis | funded by the National Science Council (Taiwan), the National Health Research Institutes (Taiwan) and China Medical University (Taiwan) | Sarcosine (2g/day) +risperidone (4.1 mg/day), or quetiapine (400– 600mg/day) |
| D-serine(2g/day)+risperidone(4.2mg/day) or olanzapine (20mg/day) or quetiapine (400mg/day) | ||||||
| Tsai GE et al., 2004 | Not better-specified phase of illness SCZ outpatients N=38 Mean baseline PANSS 82.6 and 85.2 in groups I and II, respectively |
Age: 31.8 F: 39.6% |
DSM-IV, SCID | Six weeks, parallel; per-protocol analysis | supported by funding from the National Science Council (Taiwanl, and the National HeaIth Research Institutes (Taiwan) | Sarcosine (2g/day)+antipsychotics (mean CPZ-equivalents 409mg/day) |
| Stizelecki D et al., 2018 | Clinically stable SCZ outpatients with predominantly negative symptoms N=59 Mean baseline PANSS 69.3 and 72.4 for groups I and II, respectively |
Age: 38.7 F: 42.4% |
DSM-IV-TR and ICD-10, MINI | 24 weeks, parallel; intent-to-treat analysis | Polish Ministry of Science and Higher Education (grant N402 268836). | Sarcosine(2g/day)+antipsychotics except for clozapine (defined daily dose 1.94), antidepressants (prescribed daily dose 0.58) |
| Lin C-Y et al., 2015 | Clinically stable SCZ outpatients N=63 Mean baseline PANSS was 87.1 for the sarcosine group, 84.9 for the sarcosine+benzoate group, 86.1 for the placebo group |
Age: 38.4 F: 38% |
DSM-IV | 12 weeks, parallel; per-protocol analysis | Hospital Administration Commission, Ministry of Health and Welfare, Taiwan; the Ministry of Science and Technology; Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence; China Medical University Hospital, Taiwan; Chang-Flua Hospital Program Grant 102–8 | Sarcosine(2g/day)+antipsychotics (OLA-equivalents 14.5mg/day) |
| Sarcosine(2g/day) and sodium benzoate (1 g/day)+antipsychotics(OLA-equivalents 13.5mg/day) | ||||||
| Tsai GE et al., 2005 | Not better-specified phase of illness SCZ outpatients N=32 Mean baseline PANSS 80.8 and 82.4 for groups I and II, respectively |
Age: 31.4 F: 53.1% |
DSM-IV, SCID | Six weeks, parallel; intent-to-treat analysis | Not reported | D-alanine(100mg/kg/day)+antipsychotics (mean CPZ-equivalents 468 mg/day) |
| Xiao S-H et al., 2012 | Not better-specified phase of illness SCZ outpatients with predominant negative symptoms N=101 The mean baseline PANSS was 90.56 and 89.39 in groups I and II, respectively |
Age: 48 F:25.7% |
DSM-IV | Four weeks, parallel; per-protocol analysis | supported by the Stanley Medical Research Institute (grant no. 021– 005). | Cerebrolysin (30ml i.v/day Monday to Friday)+risperidone (2–4mg/day; mean dos 3.56mg/day) |
| Ghajar A et al., 2018 | Clinically stable SCZ outpatients N=66 The mean baseline PANSS was 47.76 and 48.67 in groups I and II, respectively. |
Age: 47.1 F: 10.5% |
DSM-5 | Eight weeks, parallel; per-protocol analysis | Grant 27749 from Tehran University of Medical Sciences | Citicoline (2500mg/day)+risperidone(mean dose 4.45mg/day) |
| Turner A et al., 2021 | Not better-specified phase of illness SCZ outpatients or schizoaffective disorder N=148 Mean baseline PANSS 73.4 and 70.2 in groups I and II, respectively |
Age: 38.8 F: 50% |
DSM-5 | 24 weeks, parallel; intent-to-treat analysis | Stanley Medical Research Institute MD, USA | Mangosteen(1000mg/day)+antipsychotics antidepressants, mood stabilizers, benzodiazepines |
| Zeinoddini A et al., 2014 | Acute SCZ outpatients N=72 Baseline PANSS 105 for both groups |
Age: 33.2 F: 68% |
DSM-IV-TR, SCID | Eight weeks, parallel; per-protocol analysis | grant 16005 from the Tehran University of Medical Sciences | L-lysine(6g/day) +risperidone (2–6mg/day; mean dose 4.6mg/day) |
| Tsai GE et al., 1999 | Not better-specified phase of illness TRS SCZ outpatients N=20 |
Age F: 45% |
DSM-IV, SCID | Six weeks, parallel; intent-to-treat analysis | Supported by a Young Investigator Award from the National Alliance for Research on Schizophrenia and Depression and a Stanley Foundation Research Award | D-serine+clozapine (mean dose 363mg/day) |
| D’Souza DC et al., 2013 | Clinically stable SCZ outpatients N=104 Mean baseline PANSS 58.14 |
Age: 37.2 F: 25% |
DSM-IV | 12 weeks, parallel; intent-to-treat analysis | funding from the Stanley Medical Research Institute, the Donaghue Foundation, a VA Career Award, the VA Schizophrenia Center, and the VA Cooperative Studies Program | D-serine (30mg/kg/day)+CRT+antipsychotics D-serine (30mg/kg/day)+controlCRT+antipsychotici |
| Heresco-Levy U et al., 2005 | Clinically stable TRS SCZ outpatients N=39 Mean baseline PANSS 100.7 and 103.7 in groups I and II, respectively |
Age: 44.8 F: 35.9% |
DSM-IV, semi-structured psychiatric interview | Six weeks, crossover; intent-to-treat analysis | supported by a research award from the Stanley Medical and Research Institute, Bethesda | D-serine (30mg/kg/day)+olanzapine or risperidone |
| Evins AE et al., 2000 | Clinically stable SCZ outpatients N=27 Mean baseline PANSS 70 and 75 in groups I and II, respectively |
Age: 39 F: 22.2% |
DSM-IV | Eight weeks, parallel; intent-to-treat analysis | Supported by a National Alliance for Research on Schizophrenia and Depression Young Investigator Award | Glycine (60g/day)+clozapine |
| Serrita J et al., 2019 | Clinically stable SCZ outpatients or schizoaffective disorder and AUD N=20 Mean baseline PANSS 65.4 and 57.3 for groups I and II, respectively |
Age: 48.8 F: 0% |
DSM-IV, SCID | 12 weeks, parallel; intent-to-treat analysis | Stanley Foundation (grant # 02T-241) and Veterans Affairs VISN I Mental Illness Research Education and Clinical Center (MIRECC) | Glycine (0.8/kg/day)+antipsychotics excep for clozapine |
| Buchanan RW et al., 2007 | Clinically stable SCZ outpatients or schizoaffective disorder with persistent negative symptoms N=157 |
Age: 43.4 F: not reported |
DSM-IV, SCID | 16 weeks, parallel; intent-to-treat analysis | Supported by the Treatment of Negative Symptoms and Cognitive Impairments grants; Advanced Center for Intervention and Services Research grant; and VA Capitol Network MIRECC | Glycine (60g/day)+ antipsychotics, mood stabilizers, antidepressants, anxiolytics, anticholinergic drugs D-cycloserine (50mg/day)+antipsychotics, mood stabilizers, antidepressants, anxiolytics, anticholinergic drugs |
Abbreviations: AIMS=Abnormal Involuntary Movements Scale; BARS=Barnes Akathisia Rating Scale; BDNF=Brain Derived Neurotrophic Factor; BPRS=Brief Psychiatric Rating Scale; CANTAB=Cambridge Automated Neuropsychological Test Battery; CDSS=Calgary Depression Scale for Schizophrenia; CGI=Cllnlcal Global Impression; DHA=docosahexaenoic acid; EPA=eicosatetraenoic acid; ESRS=Extrapyramidal Symptoms Rating Scale; GAF=Global Assessment of Functioning; GAS=Global Assessment Scale; HDRS=Flamilton Depression rating Scale; LIFE-RIFT=Range of Impaired Functioning Tool; MATRICS=Measurement and Treatment Research to Improve Cognition in Schizophrenia; MOAS= Modified Overt Aggression Scale; MoCA= Montreal Cognitive Assessment; PSS=Perceived Stress Scale; Q-LES-Q18=Quality of Life Enjoyment and Satisfaction Questionnaire; QLS=Quality of Life Scale; QOL=Quality Of Life; RBANS=RepeaTable Battery for Assessment of Neuropsychological Status; SANS=Scale for Assessment of Negative Symptoms; SAPS=Scale for Assessment of Positive Symptoms; SAS=Simpson Angus Scale; SCZ=schizophrenia; SOFAS=Social and Occupational Functioning Assessment Scale; TRS=Treatment Resistant Schizophrenia; WAIS=Wechsler Adult Intelligence Scale.
Study entering the SR portion only.
All included studies were parallel-group RCTs, except two crossover design studies 22, 68. The median number of participants was n = 60 (interquartile range, n = 40), range, n = 20–157). Most studies ranged from four to 24 weeks, except for three that lasted 26 weeks 36, 52 weeks 32, and two years 39, respectively. The latter 39 was a maintenance study involving patients who discontinued the antipsychotic treatment, undergoing randomization to omega-3 + α-lipoic acid or placebo, thus not being appropriate for the quantitative synthesis.
Most of the included studies were conducted in Asia (29 studies), followed by North America (12 studies), Europe (five studies), Africa (two studies), and Australia (two studies).
In all included studies, the efficacy of nutraceuticals or phytoceutical compounds was assessed through the score on the Positive and Negative Syndrome Scale (PANSS) 71, Scale for the Assessment of Positive Symptoms (SAPS) 72, Scale for the Assessment of Negative Symptoms (SANS) 73, and the Clinical Global Impression-Improvement module (CGI-I) 74, different cognitive batteries, and functioning scales.
Most studies were conducted on patients with chronic schizophrenia, with baseline PANSS total scores ranging from 48 60 to 114 31. The phase of illness and the setting of the study have been detailed in Table 1. Finally, the lack of corresponding data precluded a subgroup analysis for clozapine studies.
A qualitative synthesis of the results of all included RCTs is reported in Table 1. The main results are summarized in Figs. 2–4.
Figure 2.

Forest plot showing effects of nutraceuticals and phytoceuticals on change in schizophrenia-specific total symptomatology, compared to placebo+TAU.
CERLYS=Cerebrolysin; CITI=Citicoline; CURC=Curcumin; D-ALA=D-Alanine; DHA=Docosahexaenoic acid; D-SER=D-Serine; EPA=Eicosapentaenoic acid; FOL=Folate; FOLB12=Folates+Vitamin B12; GLY=Glycine; L-LYS=L-Lysine; MANG=Mangosteen; N-ACETYLCYSTEINE=N-Acetylcysteine; O3MIX=Omega-3; PBO=Placebo; WSE=Whitania Somnifera Extract; SARCO=Sarcosine; SARCO+BEN=Sarcosine+Sodium Benzoate; SARSA=Sarsasapogenin; SULFO=Sulforaphane; VitD=Vitamin D; vitdPROB=Vitamin D+Probiotics; YOKU=Yokukansan.
Note: data refers to any of the disease.
Figure 4.

Forest plot showing effects of nutraceuticals and phytoceuticals on acceptability and tolerability.
CERLYS=Cerebrolysin; CITI=Citicoline; CURC=Curcumin; D-ALA=D-Alanine; DHA=Docosahexaenoic acid; D-SER=D-Serine; EPA=Eicosapentaenoic acid; FOL=Folate; FOLB12=Folates+Vitamin B12; GINKGO=Ginkgo Biloba; GINS=Ginseng extract; GLY=Glycine; L-LYS=L-Lysine; L-THEA=L-Theanine; MANG=Mangosteen; N-ACETYLCYSTEINE=N-Acetylcysteine; O3MIX=Omega-3; PBO=Placebo; WSE=Whitania Somnifera Extract; SARCO=Sarcosine; SARCO+BEN=Sarcosine+Sodium Benzoate; SARSA=Sarsasapogenin; SULFO=Sulforaphane; VitD=Vitamin D; vitdPROB=Vitamin D+Probiotics; YOKU=Yokukansan.
Note: data refers to any phase of the disease.
Regarding the risk of bias, 11 studies (22% of the records) were rated as having some concerns, 27 studies as low-risk (54%), and 12 as high risk of bias (24%) (e-Table 1).
Network meta-analyses of nutraceuticals and phytoceuticals as an augmentation to treatment as usual
PANSS total symptomatology
Thirty-six studies with 22 treatments encompassing 2,384 patients were included in the NMA for change in total symptomatology. Specifically, the following augmentations of TAU relied on one RCT only: cerulysine, citicoline, D-alanine, DHA, folate + Vitamin B12, glycine, L-lysine, mangosteen, sarcosine + sodium benzoate, sarsapogenein, sulforaphane, vitamin D, vitamin D + probiotics, whitania somnifera, and yokukansan. The following augmentations of TAU relied on two RCTs: curcumin and folate. The following augmentations of TAU relied on three RCTs: D-serine. The following augmentations of TAU relied on four RCTs: NAC, EPA, and omega-3. Sarcosine relied on six RCTs.
As an adjunct to TAU, most nutraceutical or phytoceutical compounds failed to outperform placebo + TAU regarding total symptomatology; see the forest plot (Fig. 2 and the league Table; e-Table 2). A statistically significant difference was found only for the following supplements: citicoline (SMD=−1.05, 95%CI=−1.85; − .24), L-lysine (SMD=−1.04, 95%CI=−1.84; − .25); N-acetylcysteine (SMD=−.87, 95%CI=−1.27; − .47), sarcosine (SMD=−.5, 95%CI=−.87; − .13) (e-Figure 1). Citicoline outperformed DHA, L-lysine outperformed Vit-D and DHA, N-acetylcysteine outperformed omega-3, EPA, D-serine, mangosteen, folate + Vit.B12, Vitamin D and DHA (e-Table 2). Considerable heterogeneity was present (tau2 = .10, I2 = 55.9%) and global inconsistency (Q = 40.79, df = 18, p = .002). No publication bias was detected (Egger’s test, p = .42) (e-Figure 2).
Considering acute phase studies (k = 7, n = 422), all evaluated compounds (L-Lysine, N-acetylcysteine, withania somnifera, sarcosine, omega-3, Vitamin D, and D-serine) failed to show a significant effect on the total symptomatology, when compared to placebo augmentation (e-Figure 3 & e-Table 3; Section S5). Considering clinically stable patients (k = 12, n = 850), a significant difference was found for the following augmentation strategies vs. placebo: sarcosine (SMD=−1.26, 95%CI=−1.91; − .60), citicoline (SMD=−1.05, 95%CI=−1.65, − .44), and N-acetylcysteine (SMD=−.55, 95%CI=−.92, − .19) (e-Figure 4). Also, regarding head-to-head comparisons, sarcosine outperformed all other interventions except citicoline and N-acetylcysteine; citicoline outperformed all other active compounds except sarcosine, N-acetylcysteine, and yokukansan (e-Table 4).
No significant publication bias was found (p = .54) (e-Figure 5). Such findings were consistently supported by sensitivity analyses removing high risk-of-bias studies in all phase analyses (k = 26, n = 1,716) (e-Figure 6, e-Table 5). In contrast, the acute phase analysis without high-risk-of-bias studies (k = 6, n = 355) showed a significant effect for the following augmentations vs. placebo: N-acetylcysteine (SMD=−1.10, 95%CI=−1.75, − .45), L-lysine (SMD=−1.05, 95%CI=−1.55, − .19), omega-3 (SMD=−.83, 95%CI=−1.31; − .34) and withania somnifera (SMD=−.71, 95%CI=−1.21, − .22) (e-Figure 7 & e-Table 6). Sensitivity analysis of clinically stable patients (k = 9, n = 667) was concordant with the main analysis of studies other than high risk-of-bias (e-Figure 8 & e-Table 7).
Considering people with schizophrenia in all phases of the disease (k = 26, n = 1,542), citicoline (SMD=−1.05, 95%CI=−1.86, − .23), L-lysine (SMD=−1.04, 95%CI=−1.84, − .24), N-acetylcysteine (SMD=−.89, 95%CI=−1.35, − .43) and sarcosine (SMD=−.61, 95%CI=−1.02, − .21) outperformed placebo augmentation of TAU (e-Figure 9 & e-Table 8). In analysis of acute phase schizophrenia analysis (k = 5, n = 285), N-acetylcysteine (SMD=−1.10, 95%CI=−1.75, − .45) and L-Lysine (SMD=−1.05, 95%CI=−1.55, − .56) outperformed placebo (e-Figure 10 & e-Table 9). Considering clinically stable patients with schizophrenia (k = 8, n = 582), TAU augmentation with either sarcosine (SMD=−1.26, 95%CI=−1.83, − .68), citicoline (SMD=−1.05, 95%CI=−1.56, − .53), and N-acetylcysteine (SMD=−.41, 95%CI=−.75, − .08) outperformed placebo + TAU, supporting the main analysis findings (e-Figure 11 & e-Table 10).
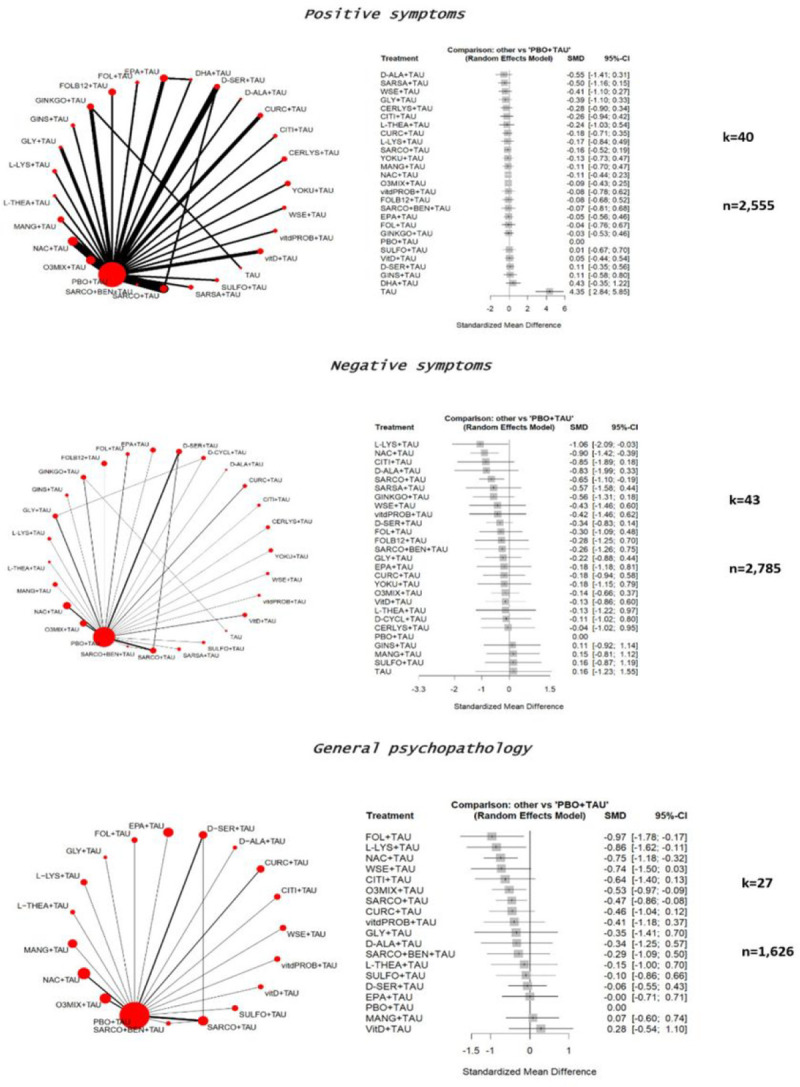
Positive symptoms
Regarding positive symptoms (measured through PANSS positive subscale or SAPS), 40 studies with 27 treatments encompassing 2,555 patients were included in the main analysis, encompassing all phases of the disease. Specifically, the following augmentations of TAU relied on one RCT only: cerulysine, citicoline, D-alanine, DHA, folate, folate + Vitamin B12, ginseng, L-lysine, L-theanine, mangosteen, sarcosine + sodium benzoate, sarsapogenein, sulforaphane, vitamin D + probiotics, whitania somnifera, and yokukansan. The following augmentations of TAU relied on two RCTs: curcumin and glycine. The following augmentations of TAU relied on three RCTs: D-serine and ginkgo biloba. The following augmentations of TAU relied on four RCTs: NAC and omega-3. Sarcosine relied on five RCTs.
Along with placebo augmentation, every compound outperformed TAU monotherapy. However, no compound outperformed placebo + TAU (e-Table 11). Moderate heterogeneity was present (tau2 = .06, I2 = 42.9%), while significant global inconsistency was found (Q = 29.77, df = 17, p = .0281). No publication bias was detected (Egger’s test, p = .85) (e-Figure 13). Considering acute phase and clinically stable studies, all compounds overlapped placebo (e-Figure 14–15 & e-Table 12–13).
Negative symptoms
The following augmentations of TAU relied on one RCT only: cerulysine, citicoline, D-alanine, D-cycloserine, EPA, folate + Vitamin B12, ginseng, L-lysine, L-theanine, mangosteen, sarcosine + sodium benzoate, sarsapogenein, sulforaphane, vitamin D + probiotics, whitania somnifera, and yokukansan. The following augmentations of TAU relied on two RCTs: curcumin and vitamin D + folate. The following augmentations of TAU relied on three RCTs: glycine. The following augmentations of TAU relied on four RCTs: NAC and omega-3. D-serine and sarcosine relied on five and six RCTs, respectively.
Regarding negative symptoms (measured through PANSS negative subscale or SANS), considering all phases of disease (k = 43, n = 2,785), among 25 treatments, a significant effect was found for the following augmentation strategies, compared to placebo: L-Lysine (SMD=−1.06, 95%CI=−2.09; − .03), N-acetylcysteine (SMD=−.90, 95%CI=−1.42; − .39), and sarcosine (SMD=−.65, 95%CI=−1.10; − .19). All other compounds did not outperform the placebo augmentation (e-Figure 16 & e-Table-14).
High heterogeneity was found (tau2 = .213, I2 = 70.8%). Global inconsistency was high (Q = 71.89, df = 21, p < .001). No publication bias was detected (Egger’s test, p = .09) (e-Figure 17).
Regarding acute phase studies (k = 7, n = 422), only N-acetylcysteine (SMD=−1.18, 95%CI=−1.83; − .52) and L-Lysine (SMD=−1.06, 95%CI=−1.55; − .56) outperformed placebo augmentation (e-Figure 18). N-acetylcysteine and L-Lysine outperformed sarcosine, Omega-3 mixture, and Vitamin D (e-Table 15).
In samples of clinically stable patients (k = 18, n = 1,190), only sarcosine (SMD=−2.30, 95%CI=−3.26; −1.34) and citicoline (SMD=−.85, 95%CI=−1.70; − .01) outperformed placebo. N-acetylcysteine overlapped with the placebo effect, while L-lysine did not enter the pertinent analysis (e-Figure 19). Sarcosine also outperformed all other compounds (e-Table 16). No publication bias was detected (Egger’s test, p = .08) (e-Figure 20).
General Psychopathology
Regarding PANSS general psychopathology (k = 27, n = 1,626), among 18 augmentation strategies, Folate (SMD=−.97, 95%CI=−1.78; − .17), L-Lysine (SMD=−.86, 95%CI=−1.62; − .11), and N-acetylcysteine (SMD=−.75, 95%CI=−1.18; − .32) outperformed placebo, while all other compound overlapped its effects (e-Figure 21 & e-Table 17). The following augmentations of TAU relied on one RCT only: citicoline, D-alanine, EPA, folate, glycine, L-lysine, L-theanine, mangosteen, sarcosine + sodium benzoate, sulforaphane, vitamin D, and whitania somnifera. Curcumin relied on two RCTs, while D-serine, NAC, and omega-3 relied on three. Sarcosine relied on five RCTs.
Moderate heterogeneity emerged (tau2 = .088, I2 = 51%), as well as significant global inconsistency (Q = 22.46, df = 11, p = .02). No publication bias was detected (Egger’s test, p = .17) (e-Figure 22).
Regarding acute phase studies (k = 6, n = 355), omega-3 (SMD=−.91, 95%CI=−1.39; − .42), L-lysine (SMD=−.86, 95%CI=−1.34; − .38), sarcosine (SMD=−.78, 95%CI=−1.43; − .12), N-acetylcysteine (SMD=−.76, 95%CI=−1.39; − .13) and withania somnifera (SMD=−.74, 95%CI=−1.24; − .24) outperformed placebo (e-Figure 23) and Vitamin D (e-Table 18). Regarding clinically stable patients’ analysis (k = 10, n = 563), sarcosine (SMD=−.97, 95%CI=−1.53; − .42), citicoline (SMD=−.64, 95%CI=−1.13; − .14), curcumin (SMD=−.47, 95%CI=−.87; − .06), and N-acetylcysteine (SMD=−.36, 95%CI=−.70; − .03) outperformed placebo (e-Figure 24 & e-Table 19). Low heterogeneity (tau2 = 0, I2 = 0%) and significant global inconsistency (Q = .37, df = 2, p = .83) emerged.
Depressive and cognitive symptoms
Regarding depressive symptoms (k = 4, n = 274), all assessed augmentation strategies (N-acetylcysteine, mangosteen, D-alanine, and ginseng) failed to differ from placebo (e-Figure 25 & e-Table 20). The following compounds relied upon one RCT only: D-alanine, ginseng, mangosteen, and NAC.
Regarding cognitive symptoms (k = 7, n = 344), N-acetylcysteine (SMD=−1.02, 95%CI=−1.56; − .49) augmentation outperformed placebo (e-Figure 26). N-acetylcysteine outperformed yokukansan, sarcosine, and D-serine (e-Table 21). Similar findings emerged in evaluating clinically stable patients (k = 3, n = 197) (e-Figure 27 & e-Table 22). The following augmentations of TAU relied on one RCT only: D-alanine, NAC, and yokukansan. D-serine relied on two RCTs, while sarcosine relied on three.
Clinical Response Rate
Regarding response rates (as per author’s definition) (k = 4, n = 274), only withania somnifera (RR = 3.00, 95%CI = 1.77; 5.09) and curcumin (RR = 9.50, 95%CI = 2.43; 37.13) augmentations outperformed placebo, while eicosatetraenoic Acid (EPA), docosahexaenoic acid (DHA), and Omega-3 failed to differ from placebo (e-Figure 28 & e-Table 23). Specifically, the appraised compounds relied on only one RCT: curcumin, DHA, EPA, omega-3, and whitania somnifera.
Acceptability and Tolerability Analysis
Regarding acceptability, 37 studies were included, accounting for 2,636 patients. None of the 24 nutraceutical or phytoceutical augmentation strategies significantly differed from the placebo regarding the RR of drop-out due to any cause (e-Figure 29 & e-Table 24). No heterogeneity was found (tau2 = 0, I2 = 0%). Global inconsistency was not statistically significant (Q = 9.33, df = 15, p = .86). No publication bias was detected (Egger’s test, p = .90) (e-Figure 30). Similar findings emerged from the sensitivity analyses without high risk-of-bias studies (e-Figure 31 & e-Table 25) and with people with schizophrenia only (e-Figure 32 & e-Table 26).
Concerning tolerability (k = 8, n = 747), none of the eight assessed augmentation strategies differed from the placebo regarding the RR of drop-out due to adverse events (e-Figure 33 & e-Table 27). Finally, there was insufficient information to compute the inefficacy (discontinuation due to lack of efficacy), set as a secondary outcome.
Confidence in evidence
The CINeMA confidence in evidence and its methods is summarized in Appendix S6. Regarding both PANSS total symptom and acceptability analyses, confidence in evidence was low/very low throughout all the comparisons (e-Tables 29–30). Likewise, meta-regression analysis consistently documented a trend for lower SMDs as the adapted AMSTAR content score increased across different outcomes (e.g., PANSS total symptoms change = β=−0.0245, 95%CI = .0.0866, −0.1943, p = .77, R2 = .34, N = 22).
Discussion
This NMA concurrently appraised 22 nutraceutical and phytoceutical interventions for adjunctive treatment of schizophrenia and related conditions, expanding the series of compounds already appraised by previous work (although a handful of compounds could nonetheless not be included in the present report due to the stringent inclusion/exclusion criteria) 14, 16. Specifically, the present NMA also included N-Methyl-D-Aspartate receptor (NMDAR) modulators, such as D-alanine, D-serine, D-cycloserine, glycine, sarcosine (N-substituted glycine), and plant-derived compounds such as curcumin, in addition to vitamins (e.g. Folate, B12, D), N-acetylcysteine, and omega-3 fatty acids, otherwise included in the WFSBP and CANMAT clinical guidelines 11.
While the NMA showed that most of the appraised nutraceutical and phytoceutical compounds failed to provide a significant benefit compared to placebo augmentation of TAU, specific compounds showed promising beneficial effects as an antipsychotic-augmentation strategy, with favorable acceptability and tolerability profiles. N-acetylcysteine and sarcosine improved total and negative symptoms. PANSS general symptomatology improved with curcumin and N-acetylcysteine. Citicoline improved total symptomatology only.
While mechanistic understanding of these nutraceutical/phytoceutical interventions is ongoing, the efficacy of select agents seen in our NMA is concordant with the currently understood mechanisms of action of these interventions.
Specifically, translational evidence suggests a relevant role of the nitric oxide (NO) signaling pathway in schizophrenia pathogenesis, affecting glutamate and dopamine storage, uptake, and release, also increasing oxidative stress 75. In this regard, L-lysine competes with L-arginine for the cationic amino-acid transporter 76 on the blood-brain barrier, thus reducing the influx of L-arginine and, consequently, the overall arginine-based NO synthesis 76. Altered regulation of oxidative stress and neuroinflammatory mechanisms may be relevant to the pathogenesis and the progression of schizophrenia and related medical and psychiatric disorders, likely due to membrane and neuronal damage 77, 78. Moreover, a protracted inflammatory state activates indoleamine 2,3-dioxygenase, producing neuroactive metabolites that influence the dopaminergic and glutamatergic neurotransmission, inducing neurotoxic stimuli 79, 80. Furthermore, an imbalance in glutamate neurotransmission is increasingly relevant in pathogenic theories of schizophrenia 81. Such neurobiological pathways may explain why the appraised beneficial compounds (i.e., L-lysine, N-acetylcysteine, citicoline, sarcosine, and curcumin) appear to be efficacious in schizophrenia, considering that they share direct/indirect antioxidant, anti-inflammatory and glutamate modulatory activity.
Curcumin exerts antioxidant, neuroprotective, and anti-inflammatory properties 82, concordant with its beneficial effects on general symptoms. Citicoline is a precursor of acetylcholine and membrane phospholipids with neuroprotective, antioxidant, and anti-excitotoxic properties 83. Moreover, citicoline may exert anti-inflammatory activity via unclear mechanisms, likely reducing blood-brain barrier permeability 84.
N-acetylcysteine is a glutathione precursor with antioxidant and anti-inflammatory properties 85 and is already recommended for adjunctive treatment in schizophrenia (primarily for negative symptoms) at 1–3 g/day 11. N-acetylcysteine influences glutamate neurotransmission by enhancing NMDAR activity 86, and several studies showed that its supplementation improved the processing speed, attention, working memory, and executive functioning of patients with schizophrenia 87–89, consistent with results from a recent umbrella review of adjunctive therapies in schizophrenia 90.
Finally, sarcosine is a glycine transporter type-I inhibitor and NMDAR allosteric modulator, directly binding to the NMDAR glycine co-agonist site, enhancing NMDAR activity, and possessing neuroprotective properties 91, 92. However, previous studies (not included in our study due to our exclusion criteria) suggested that sarcosine may not be effective when used as an augmentation agent with clozapine. This lack of efficacy is likely due to the potential glycinergic and glutamatergic activity of clozapine itself53, 93, resulting in a “ceiling” effect when additional modulation of NMDA receptors is unlikely 92.
Hypothetically, a high-inflammatory/oxidative stress subset of people with schizophrenia may benefit from such supplementations. Since oxidation, inflammatory, and genetic biomarkers could guide the stratification of people with schizophrenia 94, 95, further nutraceutical/phytoceutical RCTs may adopt biomarkers as inclusion criteria to evaluate different efficacy profiles across various subsets 90.
Limitations of the study
First, the main limitation of the present NMA is the low number of studies for each meta-analyzed agent. For example, for the primary efficacy outcome, for only five agents, more than one or two studies could be meta-analyzed, i.e., sarcosine: k = 5; and N-acetylcysteine, D-serine, EPA, and omega-3 (k = 4 each). Second, our findings rely on a limited number of comparisons, with most going via the placebo node, warranting future studies to draw firmer conclusions regarding the results. Third, high global inconsistency emerged across most comparisons, reflecting the trial duration heterogeneity and the underlying antipsychotic drugs and doses comprising TAU. Fourth, the limited number of studies also precluded feasible subgroup and sensitivity analyses to explain the observed inconsistency. Fifth, many studies lacked information regarding illness characteristics that could affect outcomes and inform subgroups, including illness phase (i.e., acute vs. clinically stable). Sixth, only 54% of the studies had a low risk of bias. Seventh, low and very low confidence in evidence emerged in the CINeMA, underscoring again that more high-quality studies are needed and that the results of this NMA need to be interpreted with caution, especially considering the trend for larger effect sizes documented by records with lower AMSTAR plus content score (adapted). Finally, caution in translating the results from this NMA to clinical care is also warranted because nutraceutical/phytoceuticals are often heterogeneous in composition, and the bioavailability and the effects of the same compound may vary across different preparations. No clear-cut guidance is often available because FDA and other regulatory agencies’ requirements for nutraceuticals and phytoceuticals differ from traditional drugs 96.
Conclusions
Among many nutraceuticals tested as an augmentation treatment for schizophrenia, sarcosine (2gr/day), citicoline (2.5gr/day), and N-acetylcysteine (1.2–3.6gr/day) consistently show a beneficial effect for total and specific symptoms, almost exclusively in stable patients, with good overall acceptability. However, multiple limitations encourage caution in interpreting and translating the results into clinical practice. Larger and high-quality RCTs with a low risk of bias should investigate the effects of nutraceuticals in schizophrenia, especially using heterogeneous daily doses and formulations.
Figure 3.
Forest plot showing effects of nutraceuticals and phytoceuticals on change in positiveand negative symptoms and symptomatology.
CERLYS=Cerebrolysin; CITI=Citicoline; CURC=Curcumin; D-ALA=D-Alanine; DHA=Docosahexaenoic acid; D-SER=D-Serine; EPA=Eicosapentaenoic acid; FOL=Folate; FOLB12=Folates+Vitamin B12; GINKGO=Ginkgo Biloba; GINS=Ginseng extract; GLY=Glycine; L-LYS=L-Lysine; L-THEA=L-Theanine; MANG=Mangosteen; N-ACETYLCYSTEINE=N-Acetylcysteine; O3MIX=Omega-3; PBO=Placebo; WSE=Whitania Somnifera Extract; SARCO=Sarcosine; SARCO+BEN=Sarcosine+Sodium Benzoate; SARSA=Sarsasapogenin; SULFO=Sulforaphane; VitD=Vitamin D; vitdPROB=Vitamin D+Probiotics; YOKU=Yokukansan.
Note: data refers to any phase of the disease.
Acknowledgments
There is nothing to state.
Funding
MB is supported by an NHMRC Senior Principal Research Fellowship and Leadership 3 Investigator grant (1156072 and 2017131).
WM is currently funded by an NHMRC Investigator Grant (#2008971).
Footnotes
Conflict of interest
MF received honoraria for his speaker activity from the American Society of Clinical Psychopharmacology (ASCP) and served as a consultant for Angelini, Otsuka, Lundbeck, Sanofi-Aventis, and Boehringer Ingelheim.
WM has previously received funding from the Cancer Council Queensland and university grants/fellowships from La Trobe University, Deakin University, University of Queensland, and Bond University. WM has received funding and/or has attended events funded by Cobram Estate Pty. Ltd and Bega Dairy and Drinks Pty Ltd. WM has received travel funding from the Nutrition Society of Australia. WM has received consultancy funding from Nutrition Research Australia and ParachuteBH. WM has received speakers honoraria from The Cancer Council Queensland and the Princess Alexandra Research Foundation.
MS has received honoraria/has been a consultant for AbbVie, Angelini, Lundbeck, and Otsuka.
VBM received honoraria from Angelini, unrelated to the present work.
CUC has been a consultant and/or advisor to or has received honoraria from: AbbVie, Acadia, Adock Ingram, Alkermes, Allergan, Angelini, Aristo, Biogen, Boehringer-Ingelheim, Bristol-Meyers Squibb, Car dio Diagnostics, Cerevel, CNX Therapeutics, Compass Pathways, Darnitsa, Delpor, Denovo, Gedeon Richter, Hikma, Holmusk, IntraCellular Therapies, Jamjoom Pharma, Janssen/J&J, Karuna, LB Pharma, Lundbeck, MedAvante-ProPhase, MedInCell, Merck, Mindpax, Mitsubishi Tanabe Pharma, Mylan, Neurocrine, Neurelis, Newron, Noven, Novo Nordisk, Otsuka, Pharmabrain, PPD Biotech, Recordati, Relmada, Reviva, Rovi, Sage, Seqirus, SK Life Science, Sumitomo Pharma America, Sunovion, Sun Pharma, Supernus, Tabuk, Takeda, Teva, Tolmar, Vertex, and Viatris. He provided expert testimony for Janssen and Otsuka. He served on a Data Safety Monitoring Board for Compass Pathways, Denovo, Lundbeck, Relmada, Reviva, Rovi, Supernus, and Teva. He has received grant support from Janssen and Takeda. He received royalties from UpToDate and is also a stock option holder of Cardio Diagnostics, Kuleon Biosciences, LB Pharma, Mindpax, and Quantic.
All other authors declare no conflicts of interest relevant to this work.
Supplementary information
The protocol was registered via PROSPERO at https://www.crd.york.ac.uk/prospero/
(CRD42022375946).
Contributor Information
Michele Fornaro, Federico II University of Naples.
Claudio Caiazza, University of Naples Federico II.
Martina Billeci, University of Naples Federico II.
Michael Berk, Deakin University, Australia.
Wolfgang Marx, Deakin University.
Vicent Balanzá-Martínez, University of Valencia.
Michele De Prisco, University of Naples Federico II.
Rosanna Pezone, University of Naples Federico II.
Giuseppe De Simone, University of Naples Federico II.
Niccolo’ Solini, APHM.
Felice iasevoli, APHM.
Fabrice Berna, APHM.
Guillaume FOND, APHM.
Laurent Boyer, Innovation in Mental and Physical Health and Clinical Treatment (IMPACT) Strategic Research Centre, School of Medicine, Barwon Health, Deakin University, Geelong, VIC, Australia.
Andre F Carvalho, Innovation in Mental and Physical Health and Clinical Treatment (IMPACT) Strategic Research Centre, School of Medicine, Barwon Health, Deakin University, Geelong, VIC, Australia.
Elena Dragioti, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell.
Jess Fiedorowicz, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell.
Andrea de Bartolomeis, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell.
Christoph Correll, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell.
Marco Solmi, uOttawa.
References
- 1.GBD 2019 MDC. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet Psychiatry 2022; 9(2): 137–150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Solmi M SG, Mavridis D, Correll CU, Dragioti E, Guimond S, et al. Incidence, prevalence, and global burden of schizophrenia - data, with critical appraisal, from the Global Burden of Disease (GBD) 2019. Molecular Psychiatry 2023. [DOI] [PubMed] [Google Scholar]
- 3.Keepers GA, Fochtmann LJ, Anzia JM, Benjamin S, Lyness JM, Mojtabai R et al. The American Psychiatric Association practice guideline for the treatment of patients with schizophrenia. American Journal of Psychiatry 2020; 177(9): 868–872. [DOI] [PubMed] [Google Scholar]
- 4.Correll CU, Howes OD. Treatment-Resistant Schizophrenia: Definition, Predictors, and Therapy Options. J Clin Psychiatry 2021; 82(5). [DOI] [PubMed] [Google Scholar]
- 5.Diniz E, Fonseca L, Rocha D, Trevizol A, Cerqueira R, Ortiz B et al. Treatment resistance in schizophrenia: a meta-analysis of prevalence and correlates. Brazilian Journal of Psychiatry 2023; 45: 448–458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Correll CU, Solmi M, Cortese S, Fava M, Højlund M, Kraemer HC et al. The future of psychopharmacology: a critical appraisal of ongoing phase 2/3 trials, and of some current trends aiming to de-risk trial programmes of novel agents. World Psychiatry 2023; 22(1): 48–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Berk Michael, Wolfgang Marx A. Nierenberg A. The aggregation of marginal gains: a pragmatic philosophy of clinical care in psychiatry. World Psychiatry; in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Correll CU, Rubio JM, Inczedy-Farkas G, Birnbaum ML, Kane JM, Leucht S. Efficacy of 42 pharmacologic cotreatment strategies added to antipsychotic monotherapy in schizophrenia: systematic overview and quality appraisal of the meta-analytic evidence. JAMA psychiatry 2017; 74(7): 675–684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Seetharaman M, Krishnan G, Schneider RH. The Future of Medicine: Frontiers in Integrative Health and Medicine. vol. 57. MDPI2021, p 1303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tsiaka T, Kritsi E, Tsiantas K, Christodoulou P, Sinanoglou VJ, Zoumpoulakis P. Design and Development of Novel Nutraceuticals: Current Trends and Methodologies. Nutraceuticals 2022; 2(2): 71–90. [Google Scholar]
- 11.Sarris J, Ravindran A, Yatham LN, Marx W, Rucklidge JJ, McIntyre RS et al. Clinician guidelines for the treatment of psychiatric disorders with nutraceuticals and phytoceuticals: The World Federation of Societies of Biological Psychiatry (WFSBP) and Canadian Network for Mood and Anxiety Treatments (CANMAT) Taskforce. World J Biol Psychiatry 2022: 1–32. [DOI] [PubMed] [Google Scholar]
- 12.DeFelice SL. The nutraceutical revolution: its impact on food industry R&D. Trends in Food Science & Technology 1995; 6(2): 59–61. [Google Scholar]
- 13.Lee SY, Shin YW, Hahm KB. Phytoceuticals: mighty but ignored weapons against Helicobacter pylori infection. J Dig Dis 2008; 9(3): 129–139. [DOI] [PubMed] [Google Scholar]
- 14.Firth J, Teasdale SB, Allott K, Siskind D, Marx W, Cotter J et al. The efficacy and safety of nutrient supplements in the treatment of mental disorders: a meta-review of meta-analyses of randomized controlled trials. World Psychiatry 2019; 18(3): 308–324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sarris J, Marx W, Ashton MM, Ng CH, Galvao-Coelho N, Ayati Z et al. Plant-based Medicines (Phytoceuticals) in the Treatment of Psychiatric Disorders: A Meta-review of Meta-analyses of Randomized Controlled Trials: Les médicaments à base de plantes (phytoceutiques) dans le traitement des troubles psychiatriques: une méta-revue des méta-analyses d’essais randomisés contrôlés. Can J Psychiatry 2021; 66(10): 849–862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Xu X, Shao G, Zhang X, Hu Y, Huang J, Su Y et al. The efficacy of nutritional supplements for the adjunctive treatment of schizophrenia in adults: A systematic review and network meta-analysis. Psychiatry Research 2022; 311: 114500. [DOI] [PubMed] [Google Scholar]
- 17.Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med 2015; 162(11): 777–784. [DOI] [PubMed] [Google Scholar]
- 18.Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. Bmj 2019; 366: l4898. [DOI] [PubMed] [Google Scholar]
- 19.Nikolakopoulou A, Higgins JP, Papakonstantinou T, Chaimani A, Del Giovane C, Egger M et al. CINeMA: an approach for assessing confidence in the results of a network meta-analysis. PLoS medicine 2020; 17(4): e1003082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Higgins JPT TJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors).. Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022), 2022.
- 21.Solmi M, Wade TD, Byrne S, Del Giovane C, Fairburn CG, Ostinelli EG et al. Comparative efficacy and acceptability of psychological interventions for the treatment of adult outpatients with anorexia nervosa: a systematic review and network meta-analysis. The lancet Psychiatry 2021; 8(3): 215–224. [DOI] [PubMed] [Google Scholar]
- 22.Levine J, Stahl Z, Sela BA, Ruderman V, Shumaico O, Babushkin I et al. Homocysteine-Reducing Strategies Improve Symptoms in Chronic Schizophrenic Patients with Hyperhomocysteinemia. Biological Psychiatry 2006; 60(3): 265–269. [DOI] [PubMed] [Google Scholar]
- 23.Hosseininasab M, Zarghami M, Mazhari S, Salehifar E, Moosazadeh M, Fariborzifar A et al. Nanocurcumin as an Add-on to Antipsychotic Drugs for Treatment of Negative Symptoms in Patients with Chronic Schizophrenia: A Randomized, Double-Blind, Placebo-Controlled Study. Journal of Clinical Psychopharmacology 2021; 41(1): 25–30. [DOI] [PubMed] [Google Scholar]
- 24.Miodownik C, Lerner V, Kudkaeva N, Lerner PP, Pashinian A, Bersudsky Y et al. Curcumin as add-on to antipsychotic treatment in patients with chronic schizophrenia: A randomized, double-blind, placebo-controlled study. Clinical Neuropharmacology 2019; 42(4): 117–122. [DOI] [PubMed] [Google Scholar]
- 25.Roffman JL, Lamberti JS, Achtyes E, Macklin EA, Galendez GC, Raeke LH et al. Randomized multicenter investigation of folate plus vitamin B12 supplementation in schizophrenia. JAMA Psychiatry 2013; 70(5): 481–489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Roffman JL, Petruzzi LJ, Tanner AS, Brown HE, Eryilmaz H, Ho NF et al. Biochemical, physiological and clinical effects of l-methylfolate in schizophrenia: A randomized controlled trial. Molecular Psychiatry 2018; 23(2): 316–322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Berk M, Copolov D, Dean O, Lu K, Jeavons S, Schapkaitz I et al. N-Acetyl Cysteine as a Glutathione Precursor for Schizophrenia-A Double-Blind, Randomized, Placebo-Controlled Trial. Biological Psychiatry 2008; 64(5): 361–368. [DOI] [PubMed] [Google Scholar]
- 28.Krivoy A, Onn R, Vilner Y, Hochman E, Weizman S, Paz A et al. Vitamin D Supplementation in Chronic Schizophrenia Patients Treated with Clozapine: A Randomized, Double-Blind, Placebo-controlled Clinical Trial. EBioMedicine 2017; 26: 138–145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sepehrmanesh Z, Heidary M, Akasheh N, Akbari H, Heidary M. Therapeutic effect of adjunctive N-acetyl cysteine (NAC) on symptoms of chronic schizophrenia: A double-blind, randomized clinical trial. Progress in Neuro-Psychopharmacology and Biological Psychiatry 2018; 82: 289–296. [DOI] [PubMed] [Google Scholar]
- 30.Sheikhmoonesi F, Zarghami M, Mamashli S, Charati JY, Hamzehpour R, Fattahi S et al. Effectiveness of vitamin d supplement therapy in chronic stable schizophrenic male patients: A randomized controlled trial. Iranian Journal of Pharmaceutical Research 2016; 15(4): 941–950. [PMC free article] [PubMed] [Google Scholar]
- 31.Farokhnia M, Azarkolah A, Adinehfar F, Khodaie-Ardakani MR, Hosseini SM, Yekehtaz H et al. N-acetylcysteine as an adjunct to risperidone for treatment of negative symptoms in patients with chronic schizophrenia: a randomized, double-blind, placebo-controlled study. Clinical neuropharmacology 2013; 36(6): 185–192. [DOI] [PubMed] [Google Scholar]
- 32.Breier A, Liffick E, Hummer TA, Vohs JL, Yang Z, Mehdiyoun NF et al. Effects of 12-month, double-blind N-acetyl cysteine on symptoms, cognition and brain morphology in early phase schizophrenia spectrum disorders. Schizophrenia Research 2018; 199: 395–402. [DOI] [PubMed] [Google Scholar]
- 33.Qiao Y, Liu CP, Han HQ, Liu FJ, Shao Y, Xie B. No Impact of Omega-3 Fatty Acid Supplementation on Symptoms or Hostility Among Patients With Schizophrenia. Frontiers in Psychiatry 2020; 11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Peet M, Brind J, Ramchand CN, Shah S, Vankar GK. Two double-blind placebo-controlled pilot studies of eicosapentaenoic acid in the treatment of schizophrenia. Research 2001; 49(3): 243–251. [DOI] [PubMed] [Google Scholar]
- 35.Peet M, Horrobin DF. A dose-ranging exploratory study of the effects of ethyl-eicosapentaenoate in patients with persistent schizophrenic symptoms. Journal of Psychiatric Research 2002; 36(1): 7–18. [DOI] [PubMed] [Google Scholar]
- 36.Pawełczyk T, Grancow-Grabka M, Kotlicka-Antczak M, Trafalska E, Pawełczyk A. A randomized controlled study of the efficacy of six-month supplementation with concentrated fish oil rich in omega-3 polyunsaturated fatty acids in first episode schizophrenia. Journal of Psychiatric Research 2016; 73: 34–44. [DOI] [PubMed] [Google Scholar]
- 37.Jamilian H, Ghaderi A. The Effects of Probiotic and Selenium Co-supplementation on Clinical and Metabolic Scales in Chronic Schizophrenia: a Randomized, Double-blind, Placebo-Controlled Trial. Biological Trace Element Research 2021; 199(12): 4430–4438. [DOI] [PubMed] [Google Scholar]
- 38.Jamilian H, Solhi H, Jamilian M. Randomized, placebo-controlled clinical trial of omega-3 as supplemental treatment in schizophrenia. Global journal of health science 2014; 6(7): 103–108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Emsley R, Chiliza B, Asmal L, du Plessis S, Phahladira L, van Niekerk E et al. A randomized, controlled trial of omega-3 fatty acids plus an antioxidant for relapse prevention after antipsychotic discontinuation in first-episode schizophrenia. Schizophrenia Research 2014; 158(1–3): 230–235. [DOI] [PubMed] [Google Scholar]
- 40.Emsley R, Myburgh C, Oosthuizen P, Van Rensburg SJ. Randomized, placebo-controlled study of ethyl-eicosapentaenoic acid as supplemental treatment in schizophrenia. American Journal of Psychiatry 2002; 159(9): 1596–1598. [DOI] [PubMed] [Google Scholar]
- 41.Tang W, Wang Y, Xu F, Fan W, Zhang Y, Fan K et al. Omega-3 fatty acids ameliorate cognitive dysfunction in schizophrenia patients with metabolic syndrome. Brain, Behavior, and Immunity 2020; 88: 529–534. [DOI] [PubMed] [Google Scholar]
- 42.Ritsner MS, Miodownik C, Ratner Y, Shleifer T, Mar I, Pintov L et al. L-theanine relieves positive, activation, and anxiety symptoms in patients with schizophrenia and schizoaffective disorder: An 8-week, randomized, double-blind, placebo-controlled, 2-center study. Journal of Clinical Psychiatry 2011; 72(1): 34–42. [DOI] [PubMed] [Google Scholar]
- 43.Ghaderi A, Banafshe HR, Mirhosseini N, Moradi M, Karimi MA, Mehrzad F et al. Clinical and metabolic response to vitamin D plus probiotic in schizophrenia patients. BMC Psychiatry 2019; 19(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Chengappa KNR, Brar JS, Gannon JM, Schlicht PJ. Adjunctive use of a standardized extract of withania somnifera (ashwagandha) to treat symptom exacerbation in schizophrenia: A randomized, double-blind, placebo-controlled study. Journal of Clinical Psychiatry 2018; 79(5). [DOI] [PubMed] [Google Scholar]
- 45.Chen EY, Hui CL. HT1001, a proprietary North American ginseng extract, improves working memory in schizophrenia: a double-blind, placebo-controlled study. Phytotherapy research: PTR 2012; 26(8): 1166–1172. [DOI] [PubMed] [Google Scholar]
- 46.Atmaca M, Tezcan E, Kuloglu M, Ustundag B, Kirtas O. The effect of extract of ginkgo biloba addition to olanzapine on therapeutic effect and antioxidant enzyme levels in patients with schizophrenia. Psychiatry and Clinical Neurosciences 2005; 59(6): 652–656. [DOI] [PubMed] [Google Scholar]
- 47.Zhang XY, Zhou DF, Su JM, Zhang PY. The effect of extract of ginkgo biloba added to haloperidol on superoxide dismutase in inpatients with chronic schizophrenia. Journal of Clinical Psychopharmacology 2001; 21(1): 85–88. [DOI] [PubMed] [Google Scholar]
- 48.Doruk A, Uzun Ö, Özşahin A. A placebo-controlled study of extract of ginkgo biloba added to clozapine in patients with treatment-resistant schizophrenia. International Clinical Psychopharmacology 2008; 23(4): 223–227. [DOI] [PubMed] [Google Scholar]
- 49.Miyaoka T, Furuya M, Horiguchi J, Wake R, Hashioka S, Tohyama M et al. Efficacy and safety of yokukansan in treatment-resistant schizophrenia: a randomized, double-blind, placebo-controlled trial (a Positive and Negative Syndrome Scale, five-factor analysis). Psychopharmacology 2015; 232(1): 155–164. [DOI] [PubMed] [Google Scholar]
- 50.Dickerson F, Origoni A, Katsafanas E, Squire A, Newman T, Fahey J et al. Randomized controlled trial of an adjunctive sulforaphane nutraceutical in schizophrenia. Schizophrenia research 2021; 231: 142–144. [DOI] [PubMed] [Google Scholar]
- 51.Xiao SF, Xue HB, Li X, Chen C, Li GJ, Yuan CM et al. A double-blind, placebo-controlled study of traditional Chinese medicine sarsasapogenin added to risperidone in patients with negative symptoms dominated schizophrenia. Neuroscience Bulletin 2011; 27(4): 258–268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Lane HY, Chang YC, Liu YC, Chiu CC, Tsai GE. Sarcosine or D-serine add-on treatment for acute exacerbation of schizophrenia: A randomized, double-blind, placebo-controlled study. Archives of General Psychiatry 2005; 62(11): 1196–1204. [DOI] [PubMed] [Google Scholar]
- 53.Lane HY, Huang CL, Wu PL, Liu YC, Chang YC, Lin PY et al. Glycine Transporter I Inhibitor, N-methylglycine (Sarcosine), Added to Clozapine for the Treatment of Schizophrenia. Biological Psychiatry 2006; 60(6): 645–649. [DOI] [PubMed] [Google Scholar]
- 54.Lane HY, Lin CH, Huang YJ, Liao CH, Chang YC, Tsai GE. A randomized, double-blind, placebo-controlled comparison study of sarcosine (N-methylglycine) and d-serine add-on treatment for schizophrenia. International Journal of Neuropsychopharmacology 2010; 13(4): 451–460. [DOI] [PubMed] [Google Scholar]
- 55.Tsai G, Lane HY, Yang P, Chong MY, Lange N. Glycine transporter I inhibitor, N-Methylglycine (sarcosine), added to antipsychotics for the treatment of schizophrenia. Biological Psychiatry 2004; 55(5): 452–456. [DOI] [PubMed] [Google Scholar]
- 56.Tsai GE, Yang P, Chung LC, Tsai IC, Tsai CW, Coyle JT. D-serine added to clozapine for the treatment of schizophrenia. American Journal of Psychiatry 1999; 156(11): 1822–1825. [DOI] [PubMed] [Google Scholar]
- 57.Zeinoddini A, Ahadi M, Farokhnia M, Rezaei F, Tabrizi M, Akhondzadeh S. L-lysine as an adjunct to risperidone in patients with chronic schizophrenia: A double-blind, placebo-controlled, randomized trial. Journal of Psychiatric Research 2014; 59: 125–131. [DOI] [PubMed] [Google Scholar]
- 58.Lin CY, Liang SY, Chang YC, Ting SY, Kao CL, Wu YH et al. Adjunctive sarcosine plus benzoate improved cognitive function in chronic schizophrenia patients with constant clinical symptoms: A randomised, double-blind, placebo-controlled trial. World Journal of Biological Psychiatry 2017; 18(5): 357–368. [DOI] [PubMed] [Google Scholar]
- 59.Strzelecki D, Urban-Kowalczyk M, Wysokiński A. Serum levels of interleukin 6 in schizophrenic patients during treatment augmentation with sarcosine (results of the PULSAR study). Human Psychopharmacology 2018; 33(2). [DOI] [PubMed] [Google Scholar]
- 60.Ghajar A, Gholamian F, Tabatabei-Motlagh M, Afarideh M, Rezaei F, Ghazizadeh-Hashemi M et al. Citicoline (CDP-choline) add-on therapy to risperidone for treatment of negative symptoms in patients with stable schizophrenia: A double-blind, randomized placebo-controlled trial. Human Psychopharmacology 2018; 33(4). [DOI] [PubMed] [Google Scholar]
- 61.Turner A, Baker A, Dean OM, Walker AJ, Dodd S, Cotton SM et al. Adjunctive Garcinia mangostana Linn. (Mangosteen) Pericarp for Schizophrenia: A 24-Week Double-blind, Randomized, Placebo Controlled Efficacy Trial: Péricarpe d’appoint Garcinia mangostana Linn (mangoustan) pour la schizophrénie: un essai d’efficacité de 24 semaines, à double insu, randomisé et contrôlé par placebo. Canadian Journal of Psychiatry 2021; 66(4): 354–366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Serrita J, Ralevski E, Yoon G, Petrakis I. A Pilot Randomized, Placebo-Controlled Trial of Glycine for Treatment of Schizophrenia and Alcohol Dependence. Journal of Dual Diagnosis 2019; 15(1): 46–55. [DOI] [PubMed] [Google Scholar]
- 63.Xiao S, Xue H, Li G, Yuan C, Li X, Chen C et al. Therapeutic effects of cerebrolysin added to risperidone in patients with schizophrenia dominated by negative symptoms. Australian and New Zealand journal of psychiatry 2012; 46(2): 153–160. [DOI] [PubMed] [Google Scholar]
- 64.D’Souza DC, Radhakrishnan R, Perry E, Bhakta SG, Singh N, Pittman B et al. Feasibility, safety and efficacy of the combination of D-serine and computerized cognitive retraining in schizophrenia: An international collaborative pilot study. Schizophrenia Bulletin 2013; 39: S326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Evins AE, Fitzgerald SM, Wine L, Rosselli R, Goff DC. Placebo-controlled trial of glycine added to clozapine in schizophrenia. American Journal of Psychiatry 2000; 157(5): 826–828. [DOI] [PubMed] [Google Scholar]
- 66.Buchanan RW, Javitt DC, Marder SR, Schooler NR, Gold JM, McMahon RP et al. The Cognitive and Negative Symptoms in Schizophrenia Trial (CONSIST): The efficacy of glutamatergic agents for negative symptoms and cognitive impairments. American Journal of Psychiatry 2007; 164(10): 1593–1602. [DOI] [PubMed] [Google Scholar]
- 67.Dakhale GN, Khanzode SD, Khanzode SS, Saoji A. Supplementation of vitamin C with atypical antipsychotics reduces oxidative stress and improves the outcome of schizophrenia. Psychopharmacology 2005; 182(4): 494–498. [DOI] [PubMed] [Google Scholar]
- 68.Heresco-Levy U, Javitt DC, Ebstein R, Vass A, Lichtenberg P, Bar G et al. D-serine efficacy as add-on pharmacotherapy to risperidone and olanzapine for treatment-refractory schizophrenia. Biological Psychiatry 2005; 57(6): 577–585. [DOI] [PubMed] [Google Scholar]
- 69.Fenton WS, Dickerson F, Boronow J, Hibbeln JR, Knable M. A placebo-controlled trial of omega-3 fatty acid (ethyl eicosapentaenoic acid) supplementation for residual symptoms and cognitive impairment in schizophrenia. American Journal of Psychiatry 2001; 158(12): 2071–2074. [DOI] [PubMed] [Google Scholar]
- 70.Hill M, Shannahan K, Jasinski S, Macklin EA, Raeke L, Roffman JL et al. Folate supplementation in schizophrenia: A possible role for MTHFR genotype. Schizophrenia Research 2011; 127(1–3): 41–45. [DOI] [PubMed] [Google Scholar]
- 71.Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophrenia bulletin 1987; 13(2): 261–276. [DOI] [PubMed] [Google Scholar]
- 72.Andreasen NC. Scale for the assessment of positive symptoms. Psychiatrie & Psychobiologie 1984. [Google Scholar]
- 73.Andreasen NC. Scale for the assessment of negative symptoms (SANS). University of Iowa Iowa City; 1981. [Google Scholar]
- 74.Guy W. Clinical global impression. Assessment manual for Psychopharmacology 1976: 217–222. [Google Scholar]
- 75.Nasyrova RF, Ivashchenko DV, Ivanov MV, Neznanov NG. Role of nitric oxide and related molecules in schizophrenia pathogenesis: biochemical, genetic and clinical aspects. Front Physiol 2015; 6: 139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Nasyrova RF, Ivashchenko DV, Ivanov MV, Neznanov NG. Role of nitric oxide and related molecules in schizophrenia pathogenesis: biochemical, genetic and clinical aspects. Frontiers in Physiology 2015; 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Ng F, Berk M, Dean O, Bush AI. Oxidative stress in psychiatric disorders: evidence base and therapeutic implications. International Journal of Neuropsychopharmacology 2008; 11(6): 851–876. [DOI] [PubMed] [Google Scholar]
- 78.Matsuzawa D, Obata T, Shirayama Y, Nonaka H, Kanazawa Y, Yoshitome E et al. Negative correlation between brain glutathione level and negative symptoms in schizophrenia: a 3T 1H-MRS study. PloS one 2008; 3(4): e1944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Müller N, Weidinger E, Leitner B, Schwarz MJ. The role of inflammation in schizophrenia. Front Neurosci 2015; 9: 372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Marx W, McGuinness AJ, Rocks T, Ruusunen A, Cleminson J, Walker AJ et al. The kynurenine pathway in major depressive disorder, bipolar disorder, and schizophrenia: a meta-analysis of 101 studies. Molecular psychiatry 2021; 26(8): 4158–4178. [DOI] [PubMed] [Google Scholar]
- 81.McCutcheon RA, Krystal JH, Howes OD. Dopamine and glutamate in schizophrenia: biology, symptoms and treatment. World Psychiatry 2020; 19(1): 15–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Cole GM, Teter B, Frautschy SA. Neuroprotective effects of curcumin. Adv Exp Med Biol 2007; 595: 197–212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Mallah K, Couch C, Borucki DM, Toutonji A, Alshareef M, Tomlinson S. Anti-inflammatory and Neuroprotective Agents in Clinical Trials for CNS Disease and Injury: Where Do We Go From Here? Front Immunol 2020; 11: 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Conant R, Schauss AG. Therapeutic applications of citicoline for stroke and cognitive dysfunction in the elderly: a review of the literature. Alternative medicine review 2004; 9(1): 17–31. [PubMed] [Google Scholar]
- 85.Skvarc DR, Dean OM, Byrne LK, Gray L, Lane S, Lewis M et al. The effect of N-acetylcysteine (NAC) on human cognition – A systematic review. Neuroscience & Biobehavioral Reviews 2017; 78: 44–56. [DOI] [PubMed] [Google Scholar]
- 86.Kumar A. NMDA Receptor Function During Senescence: Implication on Cognitive Performance. Front Neurosci 2015; 9: 473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Klauser P, Xin L, Fournier M, Griffa A, Cleusix M, Jenni R et al. N-acetylcysteine add-on treatment leads to an improvement of fornix white matter integrity in early psychosis: a double-blind randomized placebo-controlled trial. Transl Psychiatry 2018; 8(1): 220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Mullier E, Roine T, Griffa A, Xin L, Baumann PS, Klauser P et al. N-Acetyl-Cysteine Supplementation Improves Functional Connectivity Within the Cingulate Cortex in Early Psychosis: A Pilot Study. Int J Neuropsychopharmacol 2019; 22(8): 478–487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Sepehrmanesh Z, Heidary M, Akasheh N, Akbari H, Heidary M. Therapeutic effect of adjunctive N-acetyl cysteine (NAC) on symptoms of chronic schizophrenia: A double-blind, randomized clinical trial. Prog Neuropsychopharmacol Biol Psychiatry 2018; 82: 289–296. [DOI] [PubMed] [Google Scholar]
- 90.Fond G., Mallet J., Urbach M., Eriksen Benros M., Berk M., Billeci M. et al. Adjunctive agents to antipsychotics in schizophrenia: a systematic umbrella review and recommendations for amino acids, hormonal therapies and anti-inflammatory drugs. BMJ Ment Health 2023; Oct(1): e300771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Tanas A, Tozlu Ö, Gezmiş T, Hacimüftüoğlu A, Abd El-Aty AM, Ceylan O et al. In Vitro and In Vivo Neuroprotective Effects of Sarcosine. Biomed Res Int 2022; 2022: 5467498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.de Bartolomeis A, Vellucci L, Austin MC, De Simone G, Barone A. Rational and Translational Implications of D-Amino Acids for Treatment-Resistant Schizophrenia: From Neurobiology to the Clinics. Biomolecules 2022; 12(7): 909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Marchi M, Galli G, Magarini FM, Mattei G, Galeazzi GM. Sarcosine as an add-on treatment to antipsychotic medication for people with schizophrenia: a systematic review and meta-analysis of randomized controlled trials. Expert Opinion on Drug Metabolism & Toxicology 2021; 17(4): 483–493. [DOI] [PubMed] [Google Scholar]
- 94.Mitra S, Natarajan R, Ziedonis D, Fan X. Antioxidant and anti-inflammatory nutrient status, supplementation, and mechanisms in patients with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry 2017; 78: 1–11. [DOI] [PubMed] [Google Scholar]
- 95.van der Burg KP, Cribb L, Firth J, Karmacoska D, Sarris J. Nutrient and genetic biomarkers of nutraceutical treatment response in mood and psychotic disorders: a systematic review. Nutritional neuroscience 2021; 24(4): 279–295. [DOI] [PubMed] [Google Scholar]
- 96.Santini A, Cammarata SM, Capone G, Ianaro A, Tenore GC, Pani L et al. Nutraceuticals: opening the debate for a regulatory framework. British journal of clinical pharmacology 2018; 84(4): 659–672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al. The PRISMA 2020 statement: an updated guideline for reporting