

Abstract
Over the past two decades, China has become a distinctive and increasingly important donor of development assistance for health (DAH). However, little is known about what factors influence China’s priority-setting for DAH. In this study, we provide an updated analysis of trends in the priorities of Chinese DAH and compare them to comparable trends among OECD Development Assistance Committee (DAC) donors using data from the AidData’s Global Chinese Development Finance Dataset (2000–2017, version 2.0) and the Creditor Reporting System (CRS) database (2000–2017). We also analyse Chinese medical aid exports before and after the start of the COVID-19 pandemic using a Chinese Aid Exports Database. We further explore the potential factors influencing China’s shifting priority-setting processes by reviewing Chinese official documents following Walt and Gilson’s policy analysis framework (context–actors–process–content) and by testing our conjectures empirically. We find that China has become an important DAH donor to most regions if measured using project value, including but not limited to Africa. China has prioritized aid to African and Asian countries as well as to CRS subsectors that are not prioritized by DAC donors, such as medical services and basic health infrastructure. Chinese quarterly medical aid exports almost quintupled after the start of the COVID-19 pandemic. Noticeably, China has allocated more attention to Asia, eye diseases and infectious disease outbreaks over time. In contrast, the priority given to malaria has declined over the same period. Regarding factors affecting priority shifts, the outbreaks of SARS and Ebola, the launch of the Belt and Road Initiative and the COVID-19 pandemic appear to be important milestones in the timeline of Chinese DAH. Unlike stereotypes of China as a ‘lone wolf’ donor, our analysis suggests multilateral processes are influential in informing and setting Chinese DAH priorities.
Keywords: China, overseas development assistance, politics, health systems research, malaria, ophthalmology, infectious diseases
Key messages.
We found that China has become a significant development assistance for health (DAH) donor in most regions, rather than only in Africa. China has prioritized Africa and Asia, as well as Creditor Reporting System (CRS) subsectors, such as medical services and basic health infrastructure, that are not priorities for Development Assistance Committee (DAC) donors.
Chinese quarterly medical aid exports almost quintupled after the start of COVID-19 pandemic.
Over time, China has focused more on Asia, eye diseases and infectious disease outbreaks. In contrast, the priority given to malaria has greatly declined.
The outbreaks of SARS and Ebola, the launch of the Belt and Road Initiative and the COVID-19 pandemic have influenced the allocation patterns of Chinese DAH. Interestingly, our analysis suggests that multilateral processes are very influential in influencing Chinese DAH priorities.
Introduction
China’s role in global health is growing (Liu et al., 2014; Wu et al., 2020), and its role as a global health donor has been increasingly recognized (Tang et al., 2017). There is thus increased interest and need to better understand Chinese health aid flows, but doing so requires careful and accurate measurement which is challenging for several reasons (Fan et al., 2014). First, unlike ‘traditional’ aid donors, China does not report its overseas development finance to the Creditor Reporting System (CRS), the primary database of global aid flows used by the Organization for Economic Co-Operation and Development (OECD)- Development Assistance Committee (DAC) members but also open to non-OECD entities. Second, the modalities of Chinese aid flows tend to be different from more ‘traditional’ donors, including a greater focus on in-kind donations rather than cash disbursements, and increasingly heavy use of loans relative to grants.
Studies that estimated Chinese development assistance for health (DAH) have generally agreed that China is a large and growing global health donor. Using AidData’s Chinese Official Finance to Africa Dataset, which mainly sourced data from media and government websites, an early study found that China’s health aid to African countries had increased substantially from 2000 to 2012 and estimated that China would have ranked among the top 10 bilateral donors of DAH to Africa at that time. It also found that, in contrast to more ‘traditional’ donors, Chinese aid was more likely to be directed at infrastructure, human resources and malaria projects, with little funding for other global health priorities (Grépin et al., 2014). Using a different data source and methodology, Micah et al. (2019) estimated China’s bilateral and multilateral aid flows over a decade through 2017. It found that China’s DAH contributions nearly doubled to over US$650 million a year in 2017 relative to 2007 and that approximately 8.2% of the aid disbursed over this time was provided via multilateral channels. These estimates excluded aid provided by sub-national entities, even though sub-national units are believed to play important roles in providing Chinese development assistance. More recently, using a newer and larger dataset from AidData, McDade et al. (2022) found that Chinese DAH had continued to increase through 2017, that Africa remained the top destination of Chinese aid and that the top priorities for Chinese DAH were medical services, malaria control and infrastructure projects. It also estimated that China’s ranking as a DAH donor to African countries had increased over time.
Researchers generally agree that many events have played a role in shaping China’s global health agenda over the past two decades; however, there has been little evaluation of the impact of these events on Chinese DAH flows. First, following the SARS outbreak in 2003, China made important investments to improve domestic infectious disease surveillance and response and has engaged in numerous multilateral initiatives to improve global health security both regionally and internationally. Second, in 2013, shortly after taking office as the Chinese head of state, Xi Jinping launched what would become known as the Belt and Road Initiative (BRI), his signature foreign policy initiative. The BRI entails massive investments in infrastructure across over 150 countries, including many countries in Asia and Eastern Europe. Although not a foreign aid programme per se, due to the inclusion of many low- and middle-income countries (LMICs), as well as its focus on infrastructure, the BRI has been seen by many as a platform through which China is increasingly advancing its global development agenda (Zhang, 2021). Health has explicitly been linked to the BRI with specific goals to promote health along the ‘Health Silk Route’ (Huang, 2022). In 2018, China established the China International Development Cooperation Agency (CIDCA), a new agency designed to oversee many of the development activities that had previously been run through the Ministry of Commerce, perhaps due to the desire to distinguish its more development focused activities from its more commercial foreign activities (Zhang, 2021). Finally, during the COVID-19 pandemic, China became an important donor of vaccines and medical supplies to the world.
Given these events, there is a need to understand the changing policy priorities for Chinese health aid flows over time as well as China’s DAH in developing regions beyond Africa. In addition, studies to date on similar topics have largely been descriptive. Although solid studies have been done to empirically explore the determinants of Chinese DAH (Zhao et al., 2018; Guillon and Mathonnat, 2019) and development assistance to other sectors (Guillon and Mathonnat, 2020), they generally only covered the period from 2000 to 2014 and were heavily focused on Africa. Moreover, existing literature has not shed light on the aforementioned important events that might help to explain the shifting priorities of Chinese DAH, a gap that this article helps to fill.
Materials and methods
Data
We utilized four main sources of data to systematically explore the shifting priorities of Chinese DAH over the past two decades. The primary data source was AidData’s Global Chinese Development Finance Dataset (2000–2017, version 2.0) (AidData 2.0) (Custer et al., 2021; Dreher et al., 2022). The Chinese government does not systematically publish the project-level details of its foreign aid or other forms of development finance, nor does it report this information to primary international repositories such as the CRS. AidData’s datasets are the most comprehensive source of data for empirical analysis of China’s development assistance activities at present. AidData 2.0 was constructed using the Tracking Underreported Financial Flows (TUFF) 2.0 methodology, the details of which have been described elsewhere (Custer et al., 2021; Dreher et al., 2022). Briefly, AidData first identifies potential projects and sources, often through official government sources and publicly available media reports, then searches for additional information on each record in detail and finally conducts several layers of data quality assurance to ensure accuracy (Custer et al., 2021; Van Grieken and Kantorowicz, 2021). AidData 2.0 includes 13 427 projects across six major regions. It captures projects committed from 2000 to 2017, with implementation status updated to August 2021. Projects are mapped onto CRS sector-level purpose codes.
We defined health-related projects as those in the health (CRS purpose code 120) and population (CRS purpose code 130) sectors. We also included 10 projects related to HIV/AIDS mitigation (CRS purpose code 160.64). Collectively, to better align with the literature, we refer to these projects as health and population (HP) projects in this study. We further conducted a project selection process according to flow class, implementation status and other variables, following a widely used approach (see Annexe 1 Figure S1) (Grépin et al., 2014; McDade et al., 2022). In total, we used 7567 projects in the analysis, of which 1349, or 17.83%, were HP projects. All dollar amounts were reported in constant 2017 US$ million, unless otherwise specified.
Second, to compare China with ‘traditional’ donors, namely DAC reporting donors, we used data from the CRS datasets (2000–2017). From the CRS, we sourced data on 259 973 bilateral projects in the sector of health (120), population (130) and social mitigation of HIV/AIDS (160.64) into the analysis (see Annexe 1 Figure S2). Project values were converted to constant 2017 US$ using OECD DAC deflators (Custer et al., 2021). The deflators were retrieved from the OECD GeoBook (OECD.Stat., 2022). Values of 435 (or 0.17%) projects were set to missing due to deflator unavailability.
Third, we used the Chinese Aid Exports Database, which was retrieved from the University of Göttingen database repository. As of January 2023, this database contained data on China’s medical and non-medical aid exports to 195 countries between January 2017 and September 2022. It is a balanced panel dataset aggregated at the recipient country and month levels. The original data source is China’s General Administration of Customs (Fuchs et al., 2022). This dataset defined aid exports as exports in ‘Aid or Donation between Governments and International Organizations’ (code for Chinese customs statistical trade mode: 11) and ‘Other Donation’ (code: 12) sectors (Fuchs et al., 2022). Further, the dataset defined medical aid exports according to the World Trade Organization (WTO)’s definition whose full lists have been provided elsewhere (Helble, 2012; WTO, 2020). Briefly, medical aid exports include inputs specific to the pharmaceutical industry, chemical inputs of general-purpose, hospital and laboratory inputs, medical technology equipment, medical supplies, medical equipment and personal protective products. We note that the medical aid exports are not directly comparable with HP projects in AidData’s dataset 2.0 for a number of reasons. First, AidData records often focus on the underlying activity purpose, but the Chinese Aid Exports Database emphasizes the nature of the goods. For example, donating computers to a hospital could be defined as a HP project since it aims to improve the health system. However, it could not be defined as medical aid export since computers are not medical goods. Second, AidData’s data collection methodology utilized a broader definition regarding health-related projects and activities. However, the Chinese Aid Exports Database mainly restricts its scope to medical goods (WTO, 2020). Third, the Chinese Aid Exports Database only tracks physical goods, whereas AidData’s dataset also captures intangible assistance (i.e. training) (Helble, 2012). Therefore, in this study, we do not directly compare the Chinese Aid Exports Database with AidData’s but rather use it as a signal of China’s DAH after the onset of the COVID-19 pandemic.
Fourth, documents on Chinese aid activities were collected from official government sources. The documents include policy documents, press releases, white papers, reports on the work of the government, reports to the national congress of the Communist Party of China (CPC) and speech transcripts of Chinese leaders (for analysed documents, see Annexe 2 Table S1). These documents were retrieved from Chinese government websites, CPC websites and significant official Chinese media outlets, such as People’s Daily (Central Committee of CPC’s organ), Xinhua News Agency (China’s state news agency) and China Central Television (China’s state television).
Finally, data on China’s malaria cases were derived from the surveillance reports on China’s notifiable infectious diseases (2003–17) (National Health Commission of China, 2022).
Methods
Labelling projects with OECD CRS purpose codes
AidData’s 2.0 dataset maps projects onto the CRS sector-level purpose codes (i.e. health, population, etc.), which limits the ability to compare it to subsector-level data from the CRS database. Thus, we labelled the HP projects with subsector purpose codes according to the CRS classification system, which includes purpose codes for such activities as basic health care, as well as population statistics and data. Annexe 3 Table S2 provides the full list (OECD, 2022). We followed the coding process used by a related study (McDade et al., 2022). Two researchers independently reviewed all HP project titles and descriptions and then applied the closest purpose codes to each project. If insufficient information was available, we would retrieve additional information online. One project can only be mapped onto one subsector purpose code, its primary focus. When there were disagreements between the two researchers, project information was provided to a third researcher to break the tie.
Content analysis
To further explore Chinese DAH priorities in depth, we conducted a content analysis. In the first stage, we developed two keyword lists to better understand the content of the DAH projects (see Annexe 3 Table S3). List 1 was used to capture the specific health problem a project focused on, such as eye disease or Ebola. List 2 was used to define a project’s activities, for example, infrastructure construction or workforce dispatch. To develop keyword lists, we first manually inspected each project’s title and description and then extracted words related to specific health problems or activities. Then, we categorized similar words and generated a standard keyword for them. For example, we extracted the words of ‘anti-malaria’ and ‘artemisinin’ from projects and generated the standard keyword of ‘malaria’. We also considered the taxonomies adopted in previous studies (Ravishankar et al., 2009; Liu et al., 2014; Dieleman et al., 2016). In the second stage, two researchers independently manually reviewed all HP projects’ titles and descriptions and then applied the keywords as appropriate. We read original web pages in English or Chinese. One project could have multiple keyword labels assigned. For instance, one project could be labelled with ‘eye disease’, ‘workforce dispatch’ and ‘training’ if a project dispatched a medical team to a country to treat eye disease patients and to train local ophthalmologists. Two researchers then cross-checked and discussed the labels. When there were disagreements, a third researcher reviewed the data to arrive at a consensus.
Estimating missing project values
Of the 1349 HP projects in the AidData 2.0 database, 802 (59.45%) projects are missing a project financial value. To impute them, we first calculated median project values for 37 combinations of subsector and flow type (i.e. loans). We then filled in missing project values with the corresponding combination median values, except for 10 combinations wherein all project values were missing. In these cases, we used the median value for a similar flow type within the subsector. For example, the value of all free-standing technical assistance projects in the basic health infrastructure subsector was missing; so, we used the median value of grant projects in the same subsector. For three combinations, project values were unavailable for entire subsectors; so, we used the median value of each flow type instead. For example, there were no financial data for population statistics and data subsector. We filled missing values with the median value of either grant or free-standing technical assistance projects depending on the project type. This approach has been previously used by McDade et al. (2022). As the imputation method we used is difficult to validate, we also adopted a regression-based imputation method, which has also been used by McDade et al. (2022). As the results with two imputation methods were highly consistent, we present only the median-based results and report methods and results of regression imputation in Annexe 4.
Priority-setting analysis
This analysis used Walt and Gilson’s policy analysis framework (context–actors–process–content) (Walt and Gilson, 1994) to explore factors of China’s DAH priorities. We selected this framework because it provides both a comprehensive and dynamic perspective (Lyra et al., 2022). Moreover, it has been proven to perform well in LMIC settings (Hercot et al., 2011). The ‘context’ category focuses on economic, political, cultural and other sector-specific factors. The ‘actor’ category focuses on the role of influential individuals, groups and organizations during the policy process (Walt and Gilson, 1994; Lyra et al., 2022). The ‘process’ category refers to activities that could be seen to be part of the policy process—from agenda setting to policy implementation. The ‘content’ category captures elements of policy design, for instance, the stated objectives and the expression of a given policy. To identify factors and key events, we conducted a review process as follows: First, one researcher who can read Chinese reviewed Chinese DAH documents (i.e. white paper) narratively to understand the policy language, the document scope and sentiments of the government and CPC about specific topics. Second, while reading, the researcher took notes following the Walt and Gilson’s policy analysis framework. During this process, the researcher paid particular attention to any mentions of Chinese DAH priorities and key events related to Chinese DAH. If any were mentioned, third, the researcher further searched for additional documents related to the mentioned information and reviewed them. Fourth, two researchers discussed the notes together in English and reached a consensus on factors and key events that probably affected Chinese DAH priorities. All other authors reviewed and commented on the findings. When conflicting statements were found, all authors discussed them in person or in writing to reach a consensus. Fifth, for identified key events, two researchers identified their accurate timing and processes to prepare for the econometric analysis.
Econometric analysis
We conducted several econometric analyses to empirically test our conjectures regarding key events identified in our policy analysis. First, we utilized Interrupted Time Series Analysis (ITSA) to investigate the effects of key events (i.e. the launch of BRI) on the count and value of HP projects as well as the medical aid exports from China to 192 United Nations Member States (for details, see Annexe 5 and Annexe 6) (Guillon and Mathonnat, 2019). Second, we calculated Herfindahl-Hirschman concentration indices of medical aid exports around the COVID-19 pandemic onset (for details, see Annexe 7) (Ansari, 2012; Guillon and Mathonnat, 2020). It is worth noting that they are not the main analysis but are supplementary analyses to our qualitative priority-setting analysis and should be interpreted cautiously.
Results
From 2000 to 2017, China committed, implemented or completed 7567 Official Development Assistance (ODA)-like projects. Of these projects, 1349 (or 17.83%) were deemed HP projects using the above approach. When aggregating only non-imputed commitments, HP projects accounted for 2975.15 US$ million (or 2.96% of all project commitments value), and the average project value was 5.44 US$ million (for summary, see Annexe 7 Table S14). Figure 1 shows that, on average, between 2000 and 2017, HP projects accounted for 17.18% of all Chinese aid projects without substantial changes over time. Figure 1 illustrates that the non-imputed and imputed project commitments show a similar overall shape over time, although imputation was used to fill in the value of around half of the projects in our database (for comparison details, see Annexe 4 Table S5 and Figure S3). The yearly difference between the non-imputed and imputed commitments was 54.76 US$ million, accounting for 33.13% of non-imputed commitments.
Figure 1.
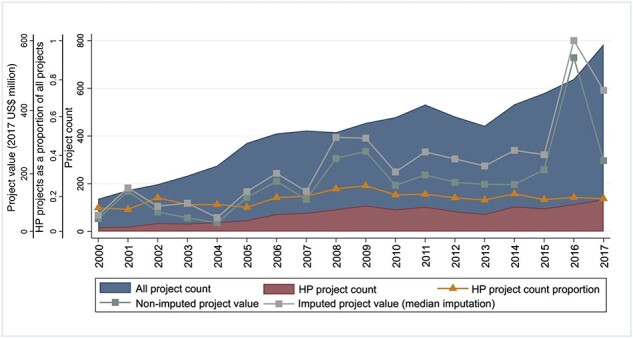
HP project count, value, and HP projects as a share of all Chinese development assistance projects from 2000 to 2017. Data source: AidData 2.0.
Financial comparison between China and DAC donors
Figure 2 shows that regarding project value, China’s role in global DAH has steadily increased since 2000 in most regions of the world. We split data into three time periods (2000–3, 2004–13 and 2014–17) to correspond with key events, namely the SARS outbreak (2003) and the launch of the BRI (2013). Figure 2 illustrates that China became Africa’s seventh largest DAH donor during the 2004–2013 period and has remained at this rank between 2014 and 2017 (711.07 US$ million). By 2014–2017, China ranked one of the top five donors in Asia (fifth, or 593.10 US$ million), America (third, or 171.25 US$ million), Oceania (third, or 84.76 US$ million) and Europe (fifth, or 23.19 US$ million). Only in the Middle East (7.00 US$ million) did China not rank among one of the top 10 donors from 2014 to 2017. The regressions imputation method generated analogous rankings (see Annexe 4 Figure S4). Unlike the rankings by project value, Figure 3 shows China was not among the top 10 donors in most regions in terms of project count 2000–2017 (except for Oceania). One interpretation is that the mean value of Chinese HP projects is higher than for most DAC donors (the mean value of Chinese projects was 2.90 US$ million vs. 0.99 for DAC donors).
Figure 2.
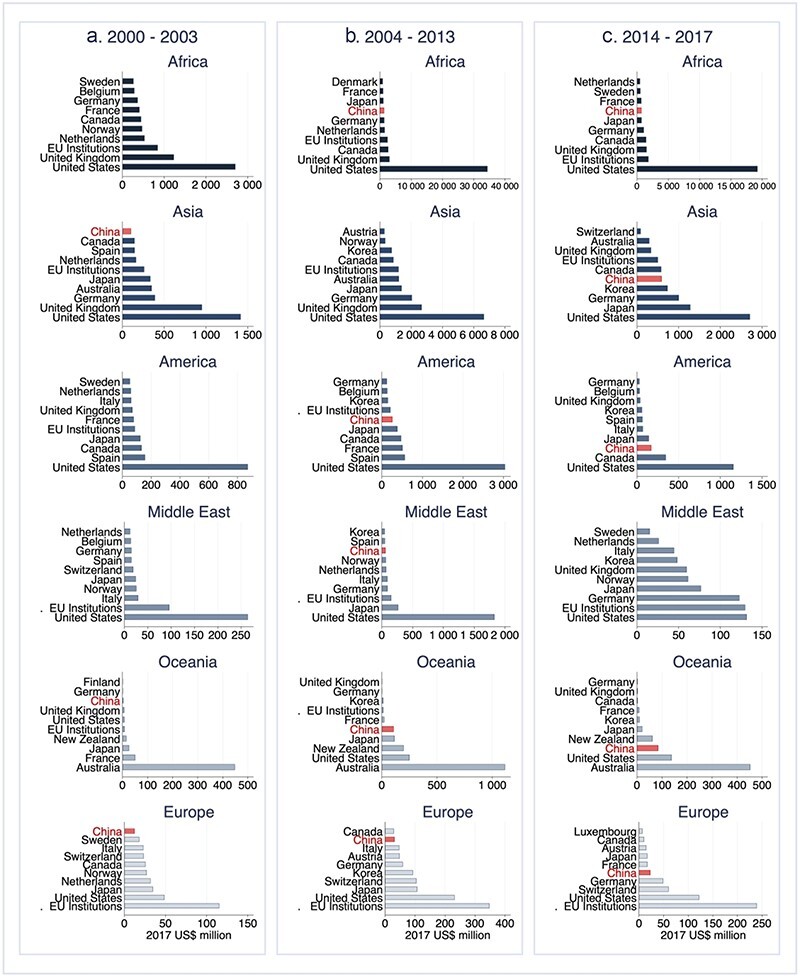
Top 10 bilateral donors of HP commitments in each region from (a) 2000 to 2003; (b) 2004 to 2013; (c) 2014 to 2017. Ranked from bottom to top by the HP project value (median imputation). Datasource: AidData 2.0 and CRS datasets.
Figure 3.
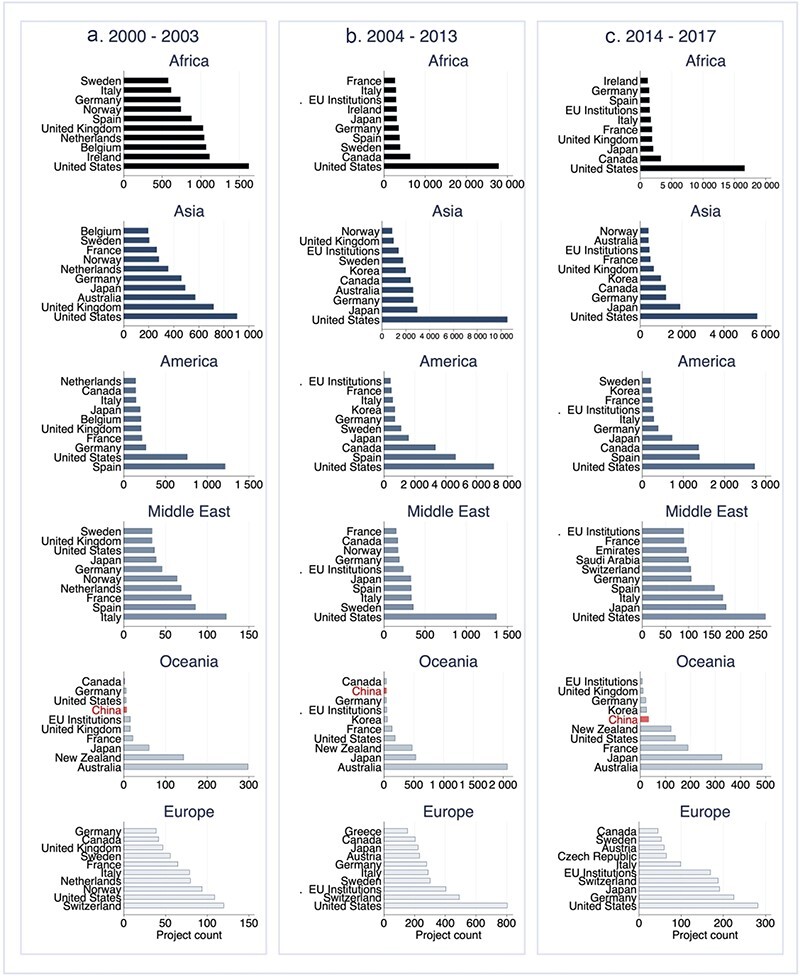
Top 10 bilateral donors of HP commitments in each region from (a) 2000 to 2003; (b) 2004 to 2013; (c) 2014 to 2017. Ranked from the bottom to the top by the HP project count. Data source: AidData 2.0 and CRS datasets.
Figure 4a and b compares China and the DAC donors regarding the regional distribution of their HP commitments, measured by project value. Figure 4a shows that, in 2000, Africa accounted for 100% (or 53.09 US$ million) of all Chinese HP commitments. From 2001 to 2017, China also distributed commitments to other regions but continued to prioritize Africa, accounting for 31.11% (or 73.28 US$ million) to 92.13% (or 279.10 US$ million) of all commitments (60.74% or 129 US$ million, on average between 2001 and 2017). Since 2014, or following the launch of the BRI, Asia has become the second-largest recipient region of Chinese DAH, accounting for average of 34.31% (or 148.29 US$ million) of total commitments from 2014 to 2017. Sri Lanka (151.71 US$ million), Cambodia (132.35 US$ million) and Laos (121.24 US$ million) were the largest Asian recipients between 2014 and 2017 (for full list, see Annexe 7 Table S15). DAC donors also prioritized Africa, accounting for 46.52% (or 5 191.03 US$ million) of all commitments on average from 2000 to 2017. Asia used to be the second highest priority of DAC donors’ DAH; however, as of 2001, it had been replaced by the category of others. Moreover, Chinese DAH showed a less consistent regional distribution over time as compared to DAC donors. Results with regression imputation were highly consistent with those reported here (Annexe 4 Figure S5).
Figure 4.
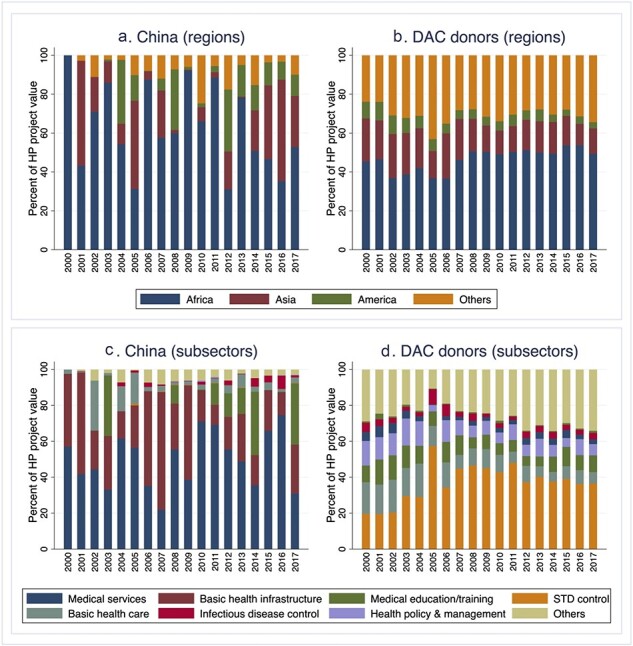
Distribution of HP commitments across regions ((a) China and (b) DAC donors) and CRS subsectors ((c) China and (d) DAC donors) by year from 2000 to 2017, measured by the HP project value (median imputation). Data source: AidData 2.0 and CRS datasets.
Figure 4c and d depicts the distribution of Chinese and DAC donors’ HP commitments among CRS subsectors from 2000 to 2017, measured by project value. There was minimal overlap between the top priorities of China and DAC donors. China prioritized medical services (49.87% or 113.99 US$ million, on average, between 2000 and 2017) and basic health infrastructure (29.78% or 59.55 US$ million, on average, between 2000 and 2017). Basic health infrastructure accounted for a higher proportion of Chinese HP commitments between 2006 and 2009 (49.09% or 105.55 US$ million, on average) than in other years. However, DAC donors prioritized Sexually Transmitted Diseases (STD) control (36.85% or 4 166.43 US$ million, on average between 2000 and 2017) the most, followed by basic health care (10.97% or 1 039.08 US$ million, on average between 2000 and 2017). There were no significant priority changes for DAC donors, but the proportion of STD control commitments increased from 19.62% (or 927.60 US$ million) in 2000 to 36.47% (or 5512.17 US$ million) in 2017, and peaked at 57.38% (or 2502.06 US$ million) in 2005. Similarly, regarding CRS subsectors, Chinese DAH also showed a less consistent distribution. Results with regression imputation were consistent on most years (see Annexe 4 Figure S5).
Figure 5 compares the distribution of Chinese and DAC donors’ HP commitments among regions and CRS subsectors from 2000 to 2017, measured by the project count. The results largely reinforce those highlighted in Figure 4, with a few additional insights. For example, for China, malaria control became the highest priority from 2006 to 2009, accounting for 30.75 (or 34.91%) projects on average. However, it decreased dramatically and constantly since then and has not been among the top two priorities since 2014
Figure 5.
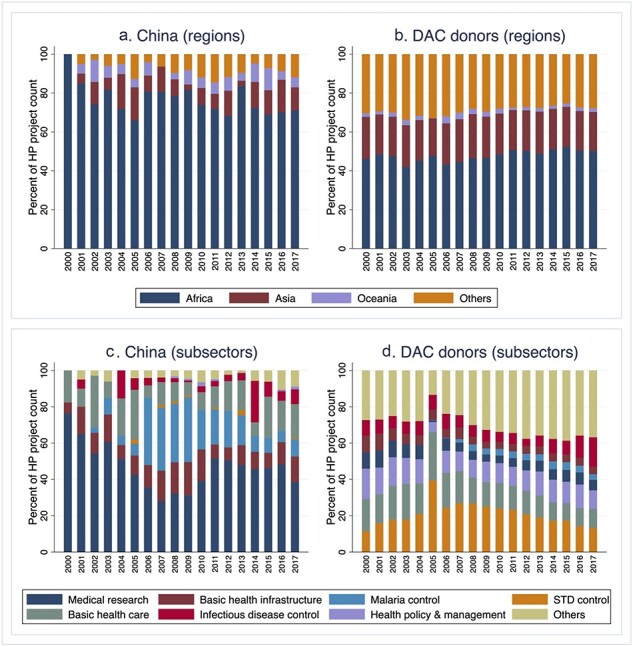
Distribution of HP commitments across regions ((a) China and (b) DAC) and CRS subsectors ((c) China and (d) DAC) by year from 2000 to 2017, measured by the HP project count. Data source: AidData 2.0 and CRS datasets.
Chinese shifting priorities in specific health problems
Figure 6a and b illustrates the count and value of the Chinese HP projects by major specific health problems from 2000 to 2017. Of Chinese HP projects, 412 (or 31.21%) were targeted to specific health problems. The results highlight the following findings. First, communicable diseases are a significant priority for Chinese HP projects. Regarding project count, the communicable disease category was the absolute priority from 2000 to 2017 except for 2016, and its count peaked in 2009 and 2014. Second, interestingly, the count and value of eye disease projects have risen considerably since 2010 and have become the second-highest priority regarding project count. The count and value of eye disease projects significantly jumped in 2014 and 2013, respectively. Among 56 eye disease projects, 29 (or 51.79%) included dispatching medical teams or training professionals to improve local cataract treatment (for examples, see Annexe 7 Table S16). Annexe 4 Figure S6 shows that the highlighted trends basically still hold with the regression imputation.
Figure 6.
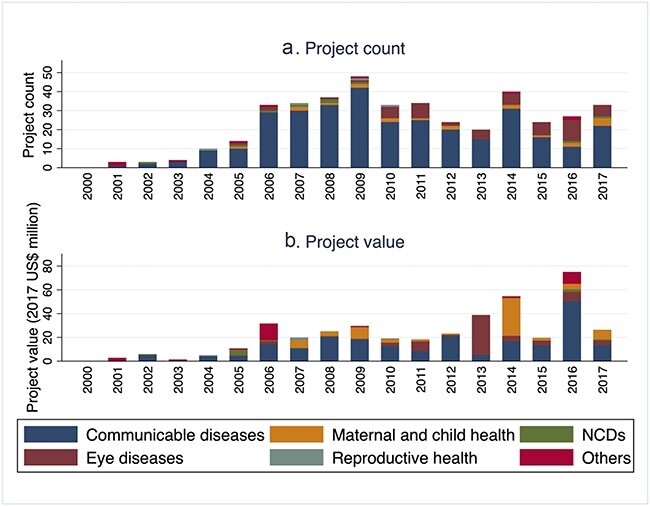
Chinese HP projects by specific health issue and by year from 2000 to 2017, measured by (a) Project count and (b) Project value (median imputation). NCDs= non-communicable diseases. Data source: AidData 2.0.
Figure 7a and b illustrates the count and value of communicable disease-related projects by specific disease and year from 2000 to 2017. The results highlight the following findings. First, malaria-related projects were the top priority between 2006 and 2013. However, its priority has significantly faded since then, which reinforced the finding in Figure 5c. Second, in 2014 and 2015, during the West African outbreak, Ebola was one of the top two priorities among communicable diseases, regardless whether considered by project count or value. Annexe 4 Figure S7 shows that the regression imputation generated a consistent trend for most years.
Figure 7.
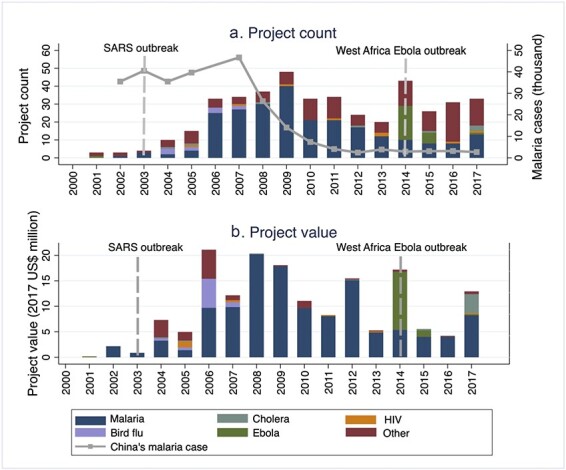
Chinese HP projects by specific communicable disease, by year (2000 to 2017), measured by (a) Project count and (b) Project value (median imputation). Two reference lines correspond to the outbreak of SARS in China and Ebola in West Africa. The line graphs illustrated new malaria cases number in China overtime. Data sources: AidData 2.0 and surveillance reports on China’s notifiable infectious diseases of National Health Commission of China (2003-2017).
Chinese medical aid export changes around the COVID-19 pandemic
Figure 8 turns to quarterly Chinese aid exports from January 2017 to September 2022. Noticeably, Chinese medical aid exports increased to a high level at the onset of the COVID-19 pandemic in early 2020, but non-medical aid exports only increased slightly around this time. For example, from quarter one (Q1) to Q2 of 2020, medical aid export increased by 140.05 current US$ million (from 116.58 to 256.62, current US$ million), while non-medical aid export increase by just 10.65 current US$ million (from 142.22 to 152.87, current US$ million). During the COVID-19 pandemic, the average level of Chinese medical aid exports per quarter was 143.31 current US$ million, which was around five times higher than before (28.22 current US$ million). This finding was also supported by the ITSA results (Annexe 6 Table S13).
Figure 8.
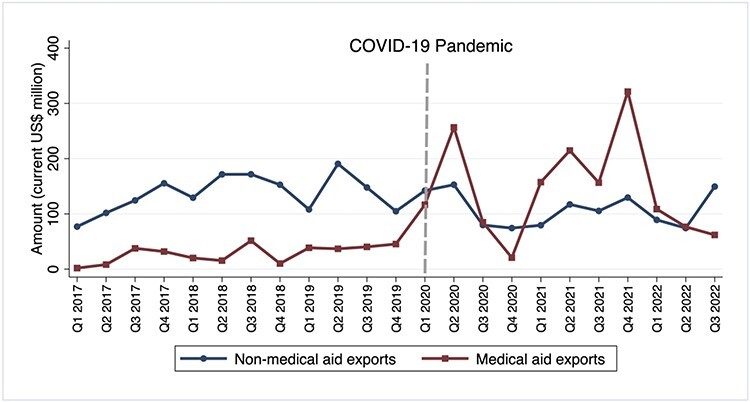
Chinese aid exports by quarter from January 2017 to September 2022. The reference line divides the period into pre- COVID-19 and post- COVID-19. Data source: Chinese Aid Exports Database.
Figure 9 shows the regional distribution of Chinese medical aid exports from January 2017 to September 2022, by year. Compared with the pre-pandemic period, China directed a higher proportion of its medical aid exports to Asia and these even exceeded exports to Africa during 2020, 2021 and the first three quarters of 2022. Surprisingly, Europe received a considerable proportion of Chinese medical aid exports during 2020. The declines in Herfindahl-Hirschman concentration indices upon the COVID-19 pandemic onset also suggest that Chinese medical aid exports became more dispersed after the pandemic (Annexe 7 Table S17 and Figure S8).
Figure 9.
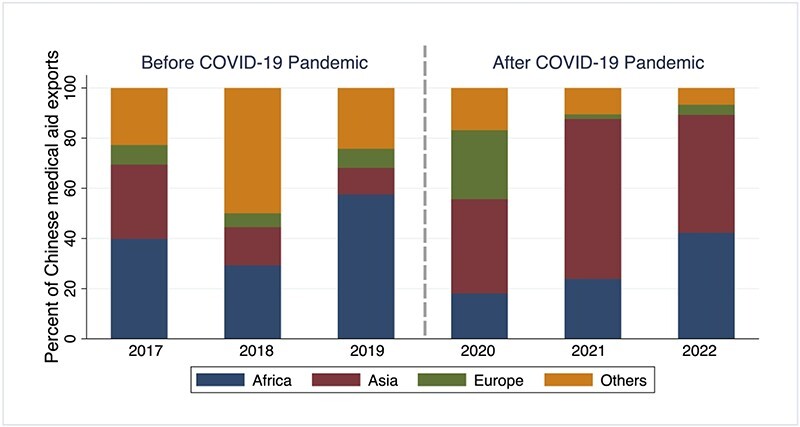
Distribution of Chinese medical aid exports across regions by quarter from January 2017 to September 2022, measured by the amount in current US$. The reference line divides the period into pre- COVID-19 and post- COVID-19. Data source: Chinese Aid Exports Database.
Factors affecting priority shifts in Chinese DAH
Our analysis highlights several important trends in the priorities of Chinese DAH. We now turn to Chinese policy documents to analyse whether there were important shifts in any of the ‘context’, ‘actors’, ‘process’ and ‘content’ categories which could help to explain some of these trends.
Since 2014, China has sharply increased its prioritization of DAH to Asia. Chinese documents suggest that factors of the ‘actors’, ‘context’ and ‘content’ categories probably drove this shift. First, Xi Jinping (actor) began serving as China’s president in 2013. Xi has allocated significant attention to making China more active in its foreign affairs, even more so than his two most recent predecessors, Jiang Zemin and Hu Jintao. This is reflected in ‘Xi Jinping’s Thought on Socialism with Chinese Characteristics for a New Era’, which places heavy emphasis on issues of diplomacy. Existing literature suggests Chinese diplomacy strategy has shifted away from Deng Xiaoping’s ‘“Tao Guang Yang Hui” (keeping a low profile)’ to ‘major country diplomacy’ during Xi’s tenure (Wang, 2019). Second, the BRI has become a major Chinese foreign policy over the past decade. After being proposed by Xi in Kazakhstan and Indonesia in 2013 (context), it was upgraded to a national strategy at the third Plenary Session of the 18th Central Committee of the CPC in December 2013. As mentioned in the Vision and Actions on Jointly Building Silk Road Economic Belt and 21st-Century Maritime Silk Road, the BRI emphasizes enhancing cooperation in public health with countries along the route, which might explain why China has given the second highest priority to Asia, the geographically closest and most important target region of the BRI. The ITSA results in Annexe 5 Table S8 also support our conjectures regarding BRI. The BRI was incorporated into the Constitution of China in 2018, and thus, it remains a major Chinese foreign policy though it received less official mention during the 20th CPC Congress in October 2022 relative to five years earlier.
China has substantially increased its support for infectious diseases since 2003. During the Ebola outbreak that started in 2014, China provided considerable DAH to the affected countries. This shift might be driven by the outbreak of SARS in 2003 (context) and World Health Organization (WHO)’s attitude towards Chinese health system (actor) then. In early 2003, China’s failure in the early stage of the SARS outbreak greatly damaged its international image and harmed its goal of becoming ‘a responsible state’ (Liu et al., 2014). To redeem its fast-fading image, China removed two high-level officials in charge of the SARS response, namely the Chinese health minister and Beijing mayor, from their posts. Also, China declared to strengthen its cooperation with WHO. In March 2003, China joined the global virtual laboratory network established by the WHO (Luo, 2011). In May 2003, Chinese Vice Premier Wu Yi attended the 56th World Health Assembly, promising that China would significantly contribute to SARS and other communicable diseases containment in the future. The COVID-19 pandemic may be another milestone of China’s emphasis on communicable diseases. It is unsurprising that Chinese quarterly medical aid exports quintupled after the COVID-19 pandemic. ITSA results also support our conjectures regarding the SARS outbreak (Annexe 5 Table S9) and the COVID-19 pandemic (Annexe 6 Table S13).
Surprisingly, while China’s malaria control projects increased rapidly between 2006 and 2009, they have sharply declined since then. This shift might be influenced by the interaction of key actors’ attitudes and policy implementation costs. In 2019, the Chairman of the China International Development Cooperation Agency (actor) re-emphasized that China was still a developing country and China had always adhered the principle of “Liang Li Er Xing, Jin Li Er Wei” (doing no more than we can, doing everything we can) in foreign aid. He also emphasized that China would pay attention to foreign aid’s cost, outcome and efficiency. From 2006 to 2017, the implementation cost of malaria projects (policy process) fluctuated greatly. In 2005, the WHO (actor) held the International Artemisinin Conference in Tanzania, calling on China, whose artemisinin production accounts for around 90% of the world’s, to develop processing enterprises and to reduce the price of artemisinin. This news triggered a binge of purchases of ‘Artemisia annua’ in China and a dramatic increase in its price, which greatly encouraged the planting and production of compound artemisinin in China. For instance, as reported by the Economic Information Daily, a media outlet run by the Xinhua News Agency, from 2004 to 2006, China’s artemisinin ingredient manufacturers increased from 3 to 100, four times larger than the market demand. However, after the WHO lowered its demand forecast in 2005, the price of ‘Artemisia annua’ in China dropped considerably. This meant that China had excess production capacity and could donate anti-malarial drugs to countries at an affordable cost. However, due to the long-term sluggishness of the industry and the entry of Indian pharmaceutical companies into the market, there had already been a shortage of ‘Artemisia annua’ in China by 2009. As of 2015, most small- and medium-sized manufacturers in China had quit the anti-malarial drug market. These market dynamics might have limited China’s ability to sustain its large-scale donations of anti-malarial drugs to other countries. Besides, malaria was once widespread in China, especially in the early 1970s (Dieleman et al., 2016). However, since Chinese domestic malaria cases had dropped significantly (Figure 7), China announced it entered the malaria elimination stage in 2010. Thus, the financial support for domestic anti-malarial affairs vastly decreased (Xian et al., 2017), which probably reduced the attention of Chinese officials (actor) to anti-malaria projects in DAH as well. The ITSA results support our conjectures about the WHO International Artemisinin Conference (Annexe 5 Table S10). In 2021, China was certified as malaria-free by the WHO. This may have further reduced China’s attention on malaria, or conversely, encouraged China to share its successful experience with other countries through anti-malaria assistance, which can be a model of ‘telling China’s stories’, rather than using market surplus as a form of DAH.
Noticeably, eye disease projects, especially cataract-related projects, became a higher priority with the decline of malaria control projects. We suggest that WHO (actor) also played an essential role in this shifting process. In 1999, the WHO and the International Agency for the Prevention of Blindness jointly launched the ‘Global Initiative for the Elimination of Avoidable Blindness’. China participated in this initiative very early. In 2013, WHO decided to revise the action plan as ‘Universal Eye Health: A global Action Plan (2014–2019)’. This plan urged the WHO member states to include the action in national priorities, including universal and equitable access to services (WHO, 2013). It also incorporated accessibility of cataract surgery as one of the three indicators of progress monitoring for member states (WHO, 2013). This probably means many countries, especially those whose health systems do not have enough capacity, had high demand for cataract surgery-related DAH. Also, China may have had a greater willingness to assist in this field since this plan also encouraged international partnerships in funding and health system capacity building (WHO, 2013).
Discussion
To the best of our knowledge, this study provides the first in-depth exploration of China’s DAH from 2000 to 2017 based on multiple data sources, including AidData 2.0, the CRS and the Chinese Aid Exports Database. It is also the first policy analysis to understand factors explaining prior shifts based on documents from Chinese official sources.
We found that China has become a significant donor of DAH in most regions, rather than only in Africa. China prioritizes both the African and Asian regions as well as CRS subsectors that have not been prioritized by ‘traditional’ donors, such as medical services, basic health infrastructure and malaria control. The existence of a more significant financial gap in these subsectors may explain this phenomenon. As an emerging donor, China faces limited competition from ‘traditional’ donors in these areas; thus, it may have presented an opportunity for China to rapidly build its image at a lower cost. Noticeably, China has increased its prioritization of Asian countries, eye disease and infectious disease control over time. In contrast, the priority given to malaria has greatly declined. Regarding factors affecting these priority shifts, the outbreaks of SARS and Ebola, the launch of the BRI and the COVID-19 pandemic appear to be important milestones in the timeline of Chinese DAH. Previously, Chinese DAH was seen as being a ‘lone wolf’ because its priority-setting is more shaped by its own political and economic interests and its preference for bilateral channels (Brautigam, 2011; Tang et al., 2017), but our analysis suggests that multilateral processes to address global health problems, such as the WHO initiative’s role in incentivizing its eye projects, were likely influential in informing and setting Chinese aid priorities.
Our findings are also relevant for larger debates about geopolitical implications in Africa, Asia and other developing regions. Geopolitical competition has been a feature of development finance since the inception of modern foreign aid after World War II (Meernik et al., 1998; Fleck and Kilby, 2010), and it is well known that donors and lenders use aid to pursue a wide range of security, political and economic interests (Burnside and Dollar, 2000; de Mesquita and Smith, 2007; Dreher et al., 2009). The rise of ‘emerging’ donors and lenders such as China, India, various Middle Eastern countries and Russia raises questions about the changing influence of these new players and ‘traditional’ donors and creditors (Woods, 2008). Public health has typically been a more cooperative, multilateral area of international development—even amidst donor competition (Manela, 2010)—but appears to be increasingly shaped by competition rather than coordination, as epitomized by the international response to the COVID-19 pandemic (Fazal, 2020). Our findings show that the Chinese government is a growing DAH provider in regions long dominated by the United States, particularly Africa, and is also now a major player in Asia, where the United States accounts for a less dominant share of DAH, and where regional ‘traditional’ donors such as Japan and Korea play a larger role. In aggregate, China’s government is still not close to approaching the scale of the United States DAH in these regions. However, many of its DAH activities are high-visibility initiatives, such as health infrastructure construction and pandemic aid, that arguably have outsized relevance for influence-seeking. Perhaps the best example is the newly completed headquarters for Africa Centres for Disease Control and Prevention (Africa CDC), which China’s government-financed and built in Addis Ababa. Probably another example is the more dispersive regional distribution of aid after the COVID-19 pandemic, namely the motivation to expand its influence in more countries, especially Europe and Asia. For China, it would be helpful to evaluate the affordability of its increasing DAH and to find the most effective approach of providing DAH, especially facing the downward economic pressure after the COVID-19 pandemic. To predict Chinese DAH in the future, an event should be noted that China promulgated the ‘Administrative Measures for Foreign Aid’ in 2021. It was the first time China formulated a comprehensive departmental regulation for foreign aid, demonstrating an emphasis on aid activities. We may expect more DAH efforts from China.
There are limitations in this study worth mentioning. First, 802 (or 59.45%) HP projects in AidData 2.0 were missing a project value. Our estimation of project values, therefore, might be inaccurate or biased, particularly if project values are systematically and not randomly missing, for example, if projects with larger value tend to be missing in reported values, or other potential factors that might explain the presence of missing project values. Thus, the results should be interpreted cautiously. However, we followed a justified estimation approach proposed by a previous study (McDade et al., 2022). We also reported results measured by project count and project value with regression imputation. There are other limitations of the AidData 2.0 dataset, such as its potential underreporting of projects (i.e. projects that may not have been reported in the media), etc. In short, the world would benefit if China could publicize project-level details systematically and comprehensively while also establishing itself as a multilateral partner with OECD DAC.
Second, while our analysis has allowed us to speculate about the factors that help to explain China’s shift in DAH priorities, this study is not causal or exhaustive. We cannot be sure that these were the main or only factors influencing these shifts in priority for DAH. Nevertheless, our study offers new insights by unpacking shifts seen through quantitative analysis and by applying a priority-setting framework to examine influential events qualitatively. Chinese official documents generally only recorded facts rather than opinions of Chinese DAH policymakers or the policy formulation process. Thus, although we attempted to do a narrative policy analysis, we acknowledge we could only provide conjectures based on data from official documents rather than from official actors directly. Future research would benefit from in-depth interviews with key informants in China and multilateral agencies, such as the WHO, as well as with local country policymakers consistent with the principle of country ownership. In particular, the rationale for China’s emphasis and priority on medical services and basic health infrastructure may offer other lessons to DAC donors and emerging donors, such as India.
Third, although we attempted to provide empirical evidence for our conjectures using econometric analyses, we acknowledge that they are imperfect. Specifically, the dataset only covers 18 years, and for several events of interest, there were only four or five data points before or after the events. Although it meets the minimum requirement of three data points, they are only straightforward analyses and can only supplement our qualitative policy review. The ITSA results should be interpreted very cautiously.
Finally, this study was not comprehensive in its analysis of other factors that may drive priority. For example, past research has indicated that China’s role as a donor depends on Chinese provinces working with assigned partner nations (Shen and Fan, 2014), but due to limited data availability, specific province-to-country relationships were not analysed in this study. While this study contributes to examining the changes in medical aid exports by China before and during the COVID-19 pandemic, future comparative analysis of Chinese medical aid exports compared to DAC medical aid exports may help to benchmark China’s 5-fold growth in medical aid exports as well as understand the disaggregated types of goods comprising medical aid exports.
Conclusion
In conclusion, our study has demonstrated that China has become an increasingly important DAH donor in various regions, including Africa, Asia, Europe, Oceania and America. Unlike ‘traditional’ donors, China prioritizes different CRS subsectors such as medical services, basic health infrastructure and malaria control. Recently, eye disease projects have become a new priority, while malaria control has faded in importance. Chinese DAH has been shaped by significant events such as the SARS and Ebola outbreaks, the launch of the BRI and the COVID-19 pandemic. Despite the stereotype of China being a ‘lone wolf’ (Brautigam, 2011; Tang et al., 2017), we anticipate greater participation of China in multilateral DAH. However, further research is required to understand the opinions of Chinese senior officials regarding priority setting for DAH and to examine causal inferences further.
Supplementary Material
Acknowledgements
We wish to thank Yanyan Wu and Duan Zhao for their help in AidData 2.0 project coding. The authors would also like to thank Anas Ismail and Amanda Karapici from the Alliance for Health Policy and Systems Research, WHO for their help with proofreading the paper.
Contributor Information
Bingqing Guo, School of Public Health, Li Ka Shing Faculty of Medicine, The University of Hong Kong, 7 Sassoon Road, Pok Fu Lam, Hong Kong SAR, Peoples’ Republic of China.
Victoria Fan, Senior Fellow, Center for Global Development, Washington, DC 20036, The United States.
Austin Strange, Assistant Professor, Department of Politics and Public Administration, Faculty of Social Sciences, The University of Hong Kong, Hong Kong SAR, Peoples’ Republic of China.
Karen Ann Grépin, School of Public Health, Li Ka Shing Faculty of Medicine, The University of Hong Kong, 7 Sassoon Road, Pok Fu Lam, Hong Kong SAR, Peoples’ Republic of China.
Supplementary data
Supplementary data are available at Health Policy and Planning Journal online.
Data availability
The data that support the findings of this study are openly available from multiple sources. AidData’s Global Chinese Development Finance Dataset (2000–2017, version 2.0) is available in GitHub at https://github.com/aiddata/china-osm-geodata/tree/master/input_data/2.0release. Creditor Reporting System datasets (2000–2017) were derived from the following resources available in the public domain: OECD Stat, https://stats.oecd.org/Index.aspx?DataSetCode=crs1. Chinese Aid Exports Database is available in GRO.data at https://doi.org/10.25625/KOS7KX. Documents on Chinese aid activities were retrieved from Chinese official websites, and weblinks can be seen in the supplementary materials. The surveillance reports on China’s notifiable infectious diseases of the National Health Commission of China (2003–2017) were retrieved from website of National Health Commission of China at http://www.nhc.gov.cn/jkj/s2907/new_list.shtml. OECD deflators is available in OECD Stat, https://stats.oecd.org/Index.aspx?DataSetCode=DACDEFL. Data used in the supplementary materials are detailed in supplementary materials.
Funding
No funding was provided for this project.
Author contributions
B.G. conducted the data analysis and interpretation as well as drafted the article. V.F. participated in the research design, critically reviewed the data analysis and revised the article. A.S. drafted the article as well as critically reviewed and revised the article. K.G. conceptualized the work, drafted the article, critically reviewed the data analysis and critically revised the article. All authors read and approved the final manuscript.
Reflexivity Statement
This paper’s authors’ group is considered inclusive. Regarding seniority, this group contains two senior experts in global health, an assistant professor and a PhD student. Regarding regional location, one author is located in The United States, and three authors are located in the People’s Republic of China, the country this paper studies. We also include female and male authors.
Ethical approval
As the study involved the analysis of existing data, ethical approval for this type of study is not required by our institute.
Conflict of interest statement
None declared.
Why all authors come from HICs
Three authors are located in Hong Kong (High Income Country (HIC)). Hong Kong is a special administrative region of China (Low- and Middle-Income Country (LMIC)). The first author Bingqing Guo’s family has lived in mainland China for generations. Bingqing Guo was born and raised in mainland China and earned her bachelor’s and master’s degrees from universities in mainland China. She came to Hong Kong only 2 years ago to pursue her PhD. Both Bingqing Guo, Victoria Fan and Austin Strange can read Chinese documents.
Abbreviations
DAH, Development Assistance for Health; CRS, Creditor Reporting System; DAC, Development Assistance Committee; AidData 2.0, AidData’s Global Chinese Development Finance Dataset (2000–2017, version 2.0); CPC, Communist Party of China; ODA, Official Development Assistance; BRI, Belt and Road Initiative; ITSA, Interrupted Time Series Analysis.
References
- Ansari MR. 2012. HHI: Stata module to compute Herfindahl index.
- Brautigam D. 2011. The Dragon’s Gift: The Real Story of China in Africa. Oxford, UK: Oxford University Press. [Google Scholar]
- Burnside C, Dollar D. 2000. Aid, policies, and growth. The American Economic Review 90: 847–68. [Google Scholar]
- Custer S, Dreher A, Elston TB et al. 2021. Tracking Chinese Development Finance: An Application of AidData’s TUFF 2.0 Methodology. Williamsburg, VA: AidData at William and Mary. [Google Scholar]
- de Mesquita BB, Smith A. 2007. Foreign aid and policy concessions. The Journal of Conflict Resolution 51: 251–84. [Google Scholar]
- Dieleman JL, Schneider MT, Haakenstad A et al. 2016. Development assistance for health: past trends, associations, and the future of international financial flows for health. The Lancet 387: 2536–44. [DOI] [PubMed] [Google Scholar]
- Dreher A, Fuchs A, Parks BC, Strange A, Tierney MJ. 2022. Banking on Beijing: The Aims and Impacts of China’s Overseas Development Program. Cambridge University Press: Cambridge, UK. [Google Scholar]
- Dreher A, Sturm J-E, Vreeland JR. 2009. Development aid and international politics: does membership on the UN Security Council influence World Bank decisions? Journal of Development Economics 88: 1–18. [Google Scholar]
- Fan VY, Grépin KA, Shen GC, Chen L. 2014. Tracking the flow of health aid from BRICS countries. Bulletin of the World Health Organization 92: 457–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fazal TM. 2020. Health diplomacy in pandemical times. International Organization 74: E78–E97. [Google Scholar]
- Fleck RK, Kilby C. 2010. Changing aid regimes? U.S. foreign aid from the Cold War to the War on Terror. Journal of Development Economics 91: 185–97. [Google Scholar]
- Fuchs A, Kaplan L, Kis-Katos K et al. 2022. GRO.data Chinese Aid Exports Database (V1).
- Grépin KA, Fan VY, Shen GC, Chen L. 2014. China’s role as a global health donor in Africa: what can we learn from studying under reported resource flows? Globalization and Health 10: 84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guillon M, Mathonnat J. 2019. Is there a strategy in China’s health official development assistance to African countries? Revue D Economie Politique 129: 619–60. [Google Scholar]
- Guillon M, Mathonnat J. 2020. What can we learn on Chinese aid allocation motivations from available data? A sectorial analysis of Chinese aid to African countries. China Economic Review 60: 1–21. [Google Scholar]
- Helble M 2012. More trade for better health? International trade and tariffs on health products. Staff Working Paper. Geneva, Switzerland: World Trade Organization. [Google Scholar]
- Hercot D, Meessen B, Ridde V, Gilson L. 2011. Removing user fees for health services in low-income countries: a multi-country review framework for assessing the process of policy change. Health Policy and Planning 26: ii5–15. [DOI] [PubMed] [Google Scholar]
- Huang YZ. 2022. The Health Silk Road: how China adapts the Belt and Road Initiative to the COVID-19 pandemic. American Journal of Public Health 112: 567–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu PL, Guo Y, Qian X et al. 2014. China’s distinctive engagement in global health. The Lancet 384: 793–804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo YH. 2011. Discussion on the effects and challenges of ‘Global Health Diplomacy’ on China. The Journal of International Studies 2: 45–61. [Google Scholar]
- Lyra TM, Albuquerque MSV, Oliveira RS et al. 2022. The National Health Policy for people with disabilities in Brazil: an analysis of the content, context and the performance of social actors. Health Policy and Planning 37: 1086–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manela E. 2010. A pox on your narrative: writing disease control into Cold War history. Diplomatic History 34: 299–323. [Google Scholar]
- McDade KK, Kleidermacher P, Yamey G, Mao W. 2022. Estimating Chinese bilateral aid for health: an analysis of AidData’s Global Chinese Official Finance Dataset Version 2.0. BMJ Global Health 7: 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meernik J, Krueger EL, Poe SC. 1998. Testing models of U.S. Foreign Policy: foreign aid during and after the Cold War. The Journal of Politics 60: 63–85. [Google Scholar]
- Micah AE, Zhao Y, Chen CS et al. 2019. Tracking development assistance for health from China, 2007–2017. BMJ Global Health 4: e001513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Health Commission of China . 2022. Surveillance reports on China’s notifiable infectious diseases of the National Health Commission of China.
- OECD . 2022. DAC and CRS code lists.
- OECD.Stat . 2022. GeoBook: Deflators.
- Ravishankar N, Gubbins P, Cooley RJ et al. 2009. Financing of global health: tracking development assistance for health from 1990 to 2007. The Lancet 373: 2113–24. [DOI] [PubMed] [Google Scholar]
- Shen GC, Fan VY. 2014. China’s provincial diplomacy to Africa: applications to health cooperation. Contemporary Politics 20: 182–208. [Google Scholar]
- Tang K, Li ZH, Li WK, Chen L. 2017. China’s Silk Road and global health. The Lancet 390: 2595–601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Grieken BJ, Kantorowicz J. 2021. Debunking myths about China: the determinants of China’s official financing to the pacific. Geopolitics 26: 861–88. [Google Scholar]
- Walt G, Gilson L. 1994. Reforming the health sector in developing countries: the central role of policy analysis. Health Policy and Planning 9: 353–70. [DOI] [PubMed] [Google Scholar]
- Wang JW. 2019. Xi Jinping’s ‘Major Country Diplomacy’: a paradigm shift? Journal of Contemporary China 28: 15–30. [Google Scholar]
- WHO . 2013. Universal eye health: a global action plan 2014-2019. [DOI] [PubMed]
- Woods N. 2008. Whose aid? Whose influence? China, emerging donors and the silent revolution in development assistance. International Affairs 84: 1205–21. [Google Scholar]
- WTO . 2020. Trade in medical goods in the context of tackling COVID-19. COVID-19 Reports. World Trade Organization: Geneva, Switzerland. [Google Scholar]
- Wu J, Bhuyan SS, Fu X. 2020. Enhancing global health engagement in 21st century China. BMJ Global Health 5: 1–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xian Y, Wang ML, Shao T et al. 2017. Analysis on the evolution and trend of malaria prevention and control policies in China. Chinese Journal of Health Policy 10: 70–4. [Google Scholar]
- Zhang M. 2021. The Belt and Road Initiative: implications for China’s foreign aid. China-an International Journal 19: 75–99. [Google Scholar]
- Zhao YX, Kennedy K, Tang K. 2018. Factors influencing the allocation of China’s development assistance for health. Journal of Global Health 8: 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data that support the findings of this study are openly available from multiple sources. AidData’s Global Chinese Development Finance Dataset (2000–2017, version 2.0) is available in GitHub at https://github.com/aiddata/china-osm-geodata/tree/master/input_data/2.0release. Creditor Reporting System datasets (2000–2017) were derived from the following resources available in the public domain: OECD Stat, https://stats.oecd.org/Index.aspx?DataSetCode=crs1. Chinese Aid Exports Database is available in GRO.data at https://doi.org/10.25625/KOS7KX. Documents on Chinese aid activities were retrieved from Chinese official websites, and weblinks can be seen in the supplementary materials. The surveillance reports on China’s notifiable infectious diseases of the National Health Commission of China (2003–2017) were retrieved from website of National Health Commission of China at http://www.nhc.gov.cn/jkj/s2907/new_list.shtml. OECD deflators is available in OECD Stat, https://stats.oecd.org/Index.aspx?DataSetCode=DACDEFL. Data used in the supplementary materials are detailed in supplementary materials.