

Abstract
There have been few investigations on the epidemiology, etiology, and medical management of acute unilateral vestibulopathy (AUV). Short-term pharmaceutical resolutions include vestibular symptomatic suppressants, anti-emetics, and some cause-based therapies. Anticholinergics, phenothiazines, antihistamines, antidopaminergics, benzodiazepines, and calcium channel antagonists are examples of vestibular suppressants. Some of these medications may show their effects through multiple mechanisms. In contrast, N-acetyl-L-leucine, Ginkgo biloba, and betahistine improve central vestibular compensation. Currently, AUV pathophysiology is poorly understood. Diverse hypotheses have previously been identified which have brought about some causal treatments presently used. According to some publications, acute administration of anti-inflammatory medications may have a deleterious impact on both post-lesional functional recovery and endogenous adaptive plasticity processes. Thus, some authors do not recommend the use of corticosteroids in AUV. Antivirals are even more contentious in the context of AUV treatment. Although vascular theories have been presented, no verified investigations employing anti-clotting or vasodilator medications have been conducted. There are no standardized treatment protocols for AUV to date, and the pharmacological treatment of AUV is still questionable. This review addresses the most current developments and controversies in AUV medical treatment.
Keywords: Acute unilateral vestibulopathy, Vestibular neuritis, Treatment, Review, Vestibular suppressants
Introduction
Acute unilateral vestibulopathy (AUV) has replaced “vestibular neuritis” as the preferred term in the International Classification of Vestibular Disorders. AUV is distinguished by an acute onset of spinning sensation, which is usually accompanied by nausea, vomiting, and gait instability, with symptoms lasting at least 24 hours [1]. It has an estimated frequency of 3.5 instances per 100,000 persons, generally affecting adults between the ages of 30 and 60 years, and both genders are equally affected [2].
Management of AUV is usually multi-stepped, involving symptomatic and causal treatment followed by central compensation enhancement, with antivertiginous drugs, corticosteroids, and physical therapy being frequently used [3]. Despite this approach, there are currently no treatment protocols established for AUV. Therefore, the goal of this review was to synthesize current information on AUV care to aid physicians in selecting the best treatment choice for their patients.
Vestibular suppressants not only reduce subjective symptoms but also the nystagmus induced by AUV. However, it is generally accepted that all symptomatic therapies should be reduced in a short time, in order to avoid impairment of the central compensatory mechanisms [3]. According to the actual knowledge, we here describe the most relevant vestibular suppressants drugs and causal therapies amenable to be used in AUV. It is important to note that the commercially available drugs widely vary depending on world regions and are dependent on national medicines policies.
A literature search of articles relevant to AUV pharmacological treatment options was conducted using the PubMed and Cochrane databases, with “vestibular neuritis” and/or “acute unilateral vestibulopathy” as search terms. Articles published over the last 5 years were preferred and references from the main review papers were also used to detect other relevant articles. A narrative condensed review format was employed with the goal of providing a brief and concise tool for readers searching for an updated summary regarding the state-of-the-art drugs used in the management of AUV.
Symptomatic Treatment
The use of vestibular suppressants may be an important step to alleviate the patient’s symptoms during the first 2–3 days after AUV onset. Albeit the restoration of peripheral function may help in some cases, final recovery of static and dynamic symptoms is largely dependent on the compensation/habituation/adaption of the vestibular, visual and somatosensory pathways [4-6]. Hence, evidence suggests that the goals of pharmacotherapy in AUV should be carefully assessed before prescription as symptomatic therapy often decreases the vestibular tone imbalance that acts as the main central compensation driver. This fact likely has a negative impact on central compensation and long-term outcomes, further supporting the use of vestibular exercises to increase vestibular tone imbalance, particularly by head movements, increasing central compensation and adequate return to a full functional state [3,7,8]. Table 1 summarizes the vestibular suppressive compounds denoted in this review.
Table 1.
Vestibular suppressants for acute unilateral vestibulopathy
| Class | Activity | Drugs | Dosage | Contraindications and side-effects |
|---|---|---|---|---|
| Anticholinergics | Central inhibition, aborting vegetative symptoms (nausea and vomiting) | Scopolamine [24] | 1 Patch in the mastoid area each 3 days (1 mg/3 days), remove once symptoms resume | Sedation (less than benzodiazepines) |
| Be aware not to use: | ||||
| - Glaucoma | ||||
| - Bladder retention | ||||
| - Prostate enlargement | ||||
| - Tachyarrhythmias | ||||
| - Psychiatric disorders | ||||
| Antihistamines | Central vertigo inhibition by antihistaminergic effects | Meclizine [32] | 25-50 mg each 4-6 hours | |
| Dimenhydrinate [51] | 50 mg each 4-6 hours | |||
| Cyclizine [51] | 50-150 mg/day | |||
| Diphenhydramine [51] | 25-50 mg/day | |||
| Betahistine [38] | 48 mg/day | Contraindicated in phaeochromocytoma | ||
| SENS-111 [40] | 100-200 mg/day | |||
| Serotonin inhibitor | Ondansetron [44,45] | 4-8 mg each 4-6 hours | Fatigue, diarrhea, QT prolongation | |
| Phenothiazines | Sedative and anti-emetic due to activity on chemoreceptor trigger zone (CTZ) | Promethazine [42,51] | 12.5 mg each 6-8 hours | Dose dependent sedation and lower seizure threshold |
| Prochlorperazine [53] | 10-20 mg each 6-8 hours | |||
| Thiethylperazine [54] | 10-30 mg daily | |||
| Antidopaminergics | Anti-emetics | Metoclopramide [45] | 10 mg each 8 hours | Extrapiramidal syndrome |
| QT prolongation | ||||
| Domperidone [60] | 10 mg daily 8 mg each 8 hours | |||
| Diazepam [51] | 2-5 mg each 6-8 hours | Dose dependent sedation and respiratory depression | ||
| Benzodiazepines | Anxiolytics, cerebellar suppressant activity | Lorazepam [51] | 0.5-2 mg each 8-12 hours | |
| Clonazepam [51] | 0.25-1 mg each 8-12 hours | |||
| Cinnarizine [51] | 15 mg each 8 hours | Weight gain, somnolence, depression, rhinitis | ||
| Calcium channel antagonists | Reducing depolarization that could lead to vertigo (±concomitant anti-histaminic or antidopaminergic effects) | Flunarizine [51] | 10 mg/day | |
| Aminoacids/metabolites | Restoring membrane potential in hyperpolarized/depolarized vestibular neurons | N-acetyl-L-leucine [74] | 1.5-2 g each 12 hours | Allergy to wheat (excludes celiac disease) |
| 4-aminopyridine [77] | 5 mg each 8 hours | QT prolongation, cardiac arrhythmias |
Symptomatic agents
Anticholinergics
Anticholinergic medicines are hypothesized to function in the vestibular system by inhibiting the activity of vestibular nuclei or cerebellar pathways [4,9,10], and are classified as solely anticholinergic or mixed anticholinergic+antihistamin ergic drugs [4,9,10]. Scopolamine, an alkaloid, is an example of a pure anticholinergic medication that acts as a non-specific muscarinic receptor antagonist [11-14]. Scopolamine blocks muscarinic receptors competitively, resulting in peripheral antimuscarinic effects as well as central sedative, antiemetic, and amnestic qualities. It is most typically used in vestibulopathies to reduce neuro-vegetative symptoms caused by parasympathetic activation by motion [12]. Because pure anticholinergic medications tend to be less effective after symptom onset, they are mostly used as a prophylactic [15], with a transdermal application of 0.5 mg scopolamine 4 to 6 hours before the commencement of a travel being recommended in motion sickness [16]. Scopolamine can also be taken orally, although its usage is limited due to the short average life of scopolamine in the plasma and its side effects [10,12], the most common of which are impaired vision and dry mouth [10]. Migraine episodes are another potential side effect of scopolamine use [17], and overdosage can cause mental symptoms such as hallucinations and impaired awareness [18-20].
Scopolamine administration in AUV is the subject of few investigations, and its late start of effect (90 minutes) and limited duration when given orally may restrict its use in AUV [21]. Nonetheless, scopolamine has been shown to be effective in the treatment of vertigo in a caloric induced vertiginous state, with one study proving the use of a transdermal patch releasing 0.17 mg/day for 7 days to be effective in acute vertigo from multiple causes [22,23]. Additional research addressing the usefulness of scopolamine patches in alleviating AUV symptoms is required [23]. Current commercial transdermal formulations release around 1 mg of scopolamine over a 72-hour period [24].
On the other hand, combined anticholinergic and antihistaminergic agents, although primarily designed for motion sickness avoidance, are more widely employed in AUV [25]. Common examples of this kind of drug are meclizine, dimenhydrinate, cyclizine, and diphenhydramine [3,22,26-28]. The antihistaminic component may cause tiredness and long-term weight gain when used regularly [29]. Meclizine and dimenhydrinate have been demonstrated to be equivalent to diazepam in the treatment of vertigo in AUV, but entail less sedation than benzodiazepines and should therefore be favored as a first therapy, particularly in the elderly [30-32]. As a result, unlike scopolamine, which is virtually exclusively used to combat motion sickness, these medicines are also utilized in AUV [3,22,26,27].
Addiction may occur from anticholinergic use, and cautious withdrawal is suggested [31]. Commonly used anticholinergic doses are displayed on Table 1.
Antihistamines
Despite a lack of robust evidence to support their efficacy, antihistamines have played a notorious role in vertigo management throughout the last decades [31], being the most often used medicines in the treatment of vestibular vertigo [33-35]. The presence of all four types of histamine receptors (H1R, H2R, H3R, and H4R) in the inner ear indicates the relevance of histamine in proper ear function [33,34]. H1 and H3 antagonists are the most commonly used antihistamines. Many antihistamines have simultaneous anticholinergic (e.g., meclinizine, cyclizine, dimenhydrinate, diphenhydramine, promethazine) or calcium blocker (e.g., cinnarizine, flunarizine) effects, thus belonging in different drug classes [33]. Hence, only pure antihistaminergic drugs will be considered in this section to facilitate systematization.
Betahistine, an H1R agonist and H3R antagonist, is the most regularly used antihistamine in Europe; however, the drug is not licensed in the United States, where meclizine, cyclizine, and diphenhydramine prevail [33,36]. Histamine has been shown in various in vitro and in vivo studies to play a role in the modulation of vestibular plasticity during the process of vestibular central compensation [33]. Indeed, betahistine reduced the time required to reach compensation by 1 month in the setting of neurectomy for Meniére’s disease [37]. The authors of the the VIRTUOSO (Effectiveness of Betaserc® [Betahistine Dihydrochloride] in Patients With Vestibular Vertigo in Routine Practice) study study suggest that using betahistine for 2 months could improve compensation in patients with vestibular vertigo [38]. However, the variability in methodology and patient selection has prevented a definitive conclusion on the efficacy of betahistine in vestibular compensation in AUV patients [4]. The major disadvantage of antihistamines is their sedative effect, which has a significant influence on optimal central compensation and everyday functioning, in addition to their direct modulation of central vestibular signaling [33]. While betahistine may not be a viable alternative for the management of acute vertigo symptoms, its H1R agonism qualities and consequent augmentation of central compensation provide for a possible application in the recovery phase of vertigo through the decrease of chronic symptoms [33,37].
SENS-111 is an H4R antagonist undergoing clinical trials [39]. In both in vitro and ex vivo experiments, selective H4R antagonists inhibited vestibular neuron activity, relieving vertigo symptoms in rats with AUV [39,40]. Despite being associated with less sedation than other antihistamine classes and being suggested to be safe and tolerable [33,40], this medication failed to meet the primary endpoint in a phase 2 study [39].
Serotonin inhibitor
Ondansetron is a 5-HT3 receptor antagonist, interacting with these receptors in both the central and peripheral nervous systems [41]. Ondansetron has traditionally been regarded as an anti-emetic, and its usage in peripheral vestibulopathies is intended to alleviate associated neuro-vegetative symptoms [42,43]. However, it has also been demonstrated to improve vertigo [44,45]. Indeed, early treatment with a combination of ondansetron, corticosteroids, and antivirals has been linked with a decrease in the vestibular deficit in acutephase AUV when compared to the standard H1R antagonists [45]. Ondansetron is often provided orally since it is readily absorbed and produces a comparable anti-emetic effect as intravenous dosing, which is more suited when individuals present with excessive vomiting [46-48]. Because ondansetron has no impact on dopamine receptors, it is not associated with extrapyramidal symptoms [49,50].
Phenothiazines
Phenothiazines are a subclass of neuroleptics known for their antipsychotic properties due to their anti-dopaminergic effect [4,50], blocking muscarinic, histaminergic H1, and serotonergic 5-hydroxytryptamine type 2 (5-HT 2) receptors as well [4,50].
Relevant compounds for the treatment of vertigo include promethazine [42], prochlorperazine [51-53], and thiethylperazine [54], all of which have anticholinergic properties that result in sedative and anti-emetic effects by acting on the chemoreceptor trigger zone (CTZ) [4,51]. Low-dose promethazine (6.25 mg) has been shown to have anti-emetic effects comparable to 4 mg ondansetron but superior vertigo suppression abilities [42,55]. Phenothiazides are also linked to peripheral adrenergic receptor blockade and quinidine-like cardiac effects, along with lowering seizure thresholds [56]. Sedation, coma, hypotension, extrapyramidal symptoms, and cardiac arrhythmias are the most prevalent clinical indicators of toxicity, in addition to anticholinergic side effects [56].
Antidopaminergics
Despite the fact that previously mentioned drugs such as meclizine and promethazine have anti-emetic activities, administration of dopaminergic antagonists may also be beneficial [57]. Metoclopramide, domperidone, and droperidol are anti-emetic medications that can be used to alleviate neurovegetative symptoms in AUV [58-61], although they can cause extrapyramidal signs and QT prolongation [56]. While metoclopramide and domperidone do not appear to be true vestibular suppressants, droperidol’s nervous system activity was revealed through its use in anesthesia [59,61], with both droperidol and droperidol+fentanyl suppressing vestibular symptoms and being effective in the management of vestibular disease [59,61].
Benzodiazepines
Gamma-aminobutyric acid (GABA) is a primary neuroinhibitory transmitter for vestibular neurons [27]. Benzodiazepines decrease the electrical activity of vestibular nuclei through their GABA agonist characteristics, leading to their therapeutic impact in vertiginous disorders [10].
Patients may benefit from the sedative and anxiolytic characteristics of benzodiazepines in addition to their inhibitory impact on vertigo [10], with diazepam, lorazepam, and clonazepam being the most often used benzodiazepines for vestibular suppression [10]. Diazepam is associated with a significant reduction in the spontaneous electrical activity of neurons in the medial vestibular nuclei, modulating both preand post-synaptic actions of diverse groups on neurons [10,62- 64]. Clonazepam on the other hand is especially useful in the treatment of migraine-related vertigo and postural vertigo [65,66]. One should be aware that the long-term use of these drugs prolongs or even prevent central compensation of vestibular tone imbalance [27].
Calcium channel antagonists
Calcium is present in the endolymph [67], flowing into the cells of the crista ampullaris in response to its movement [68] and triggering an action potential that is transmitted centrally [10,51]. Calcium channel blockers are postulated to inhibit this calcium flow, reducing the depolarization that could lead to vertigo [10,51]. Flunarizine and cinnarizine are the two major calcium channel blockers used in clinical practice [51,69]. Flunarizine is also a dopamine blocker and cinnarizine exhibits concomitant anti-histaminergic effects and blocks pressure sensitive potassium channels. The latter possibly provides a separate mechanism for the treatment of hydrops [69].
Flunarizine has been shown to be a powerful peripherally acting labyrinthine suppressant without the characteristic side effects of antihistamines and anticholinergics. Flunarizine has applications in the prevention of motion sickness, vertigo, and migraine, which constitutes an advantage in migraineurs [51,70,71]. Cinnarizine is less potent than flunarizine [72]. A fixed combination of cinnarizine 20 mg and dimenhydrinate 40 mg is available in Europe for patients with AUV. Studies confirm the benefit of this association on the management of AUV symptoms [72].
Neither drug is selective for a particular calcium channel subtype [51,70], thus exerting effects throughout the central nervous system. This can lead to potential toxicity, including weight gain, depression, sedation, or even parkinsonian symptoms, and while both drugs have been used in Europe, their use is rarer elsewhere [51].
Amino acids/metabolites
The exact role of N-acetyl-L-leucine in vertigo is unknown [73,74]. Its primary mode of action is thought to be its influence on vestibular nucleus networks, with restoration of membrane potential of hyperpolarized/depolarized vestibular neurons. N-acetyl-L-leucine improves postural symptom compensation in a dose-dependent manner [75], possibly by activating the vestibulocerebellum and deactivating the posterolateral thalamus. This molecule is suggested to have a rapid antivertiginous effect when administered intravenously or orally in humans [73,75]. N-acetyl-L-leucine is currently not used to treat vertigo in the United States.
4-Aminopyridine (4-AP) is a non-selective potassium channel blocker [76-78] that seems to restore the pacemaking function of malfunctioning Purkinje cells by extending and enhancing their action potential following hyperpolarization [79]. 4-AP may thereby augment the cerebellum’s physiological inhibitory influence on the vestibular nuclei [78]. Treatment with 4-AP has been reported to transiently ameliorate postural imbalance in AUV patients via vestibulocerebellum activation [76-78].
Unlike previous medications used to treat vertigo symptoms, compounds in this class do not have sedative effects [76-79]. These two novel agents showed promising outcomes in the treatment of cerebellar ataxias and downbeat nystagmus [77,80-82].
Causal Treatment
Immune system, inflammation, and glucocorticoids
Since Hiyoshi and Sekitani [83] discovered a possible association between the onset of AUV and influenza vaccination, immunological mechanisms have been formally implicated in the etiology of AUV [84]. Bumm and Schlimok [85] later identified similarities between lymphocyte subpopulations and HLA-DR determinations in diseases of the inner ear and Bell’s palsy. A recent study employing gene expression profiling and bioinformatics analysis discovered a difference in expressed immune system genes in AUV patients when compared to controls [86]. According to the same study, neutrophil degranulation is one of the most prominent immunological pathways in AUV, leading not only to inflammation but also to a pro-thrombotic state in the vestibular end organ [86]. These findings support Kassner, et al’s [87] discovery of proinflammatory activation of peripheral mononuclear cells in AUV patients, and explain the widespread use of endovenous glucocorticoids, such as dexamethasone, methylprednisone, and prednisone (Table 2), in AUV in both Europe and the United States [88,89]. Nonetheless, their usage is contentious, with no established standards for dosing or therapy length. Contrary to abrupt idiopathic hearing loss, intra-tympanic administration of corticoids in AUV has received less attention. Although the majority of authors endorse a brief course of high-dose glucocorticoids, a recent systematic review and meta-analysis determined that there is insufficient evidence to support their usage [90]. These medications appear to offer short-term advantages in canal paresis but no long-term benefits in canal paresis or symptomatic recovery, with a small number of patients reporting adverse effects [90]. Additionally, it was recently established from AUV rat models that acute anti-inflammatory modulators alter the post-lesional functional recovery and the endogenous adaptive plasticity pathways, which may eventually cause exacerbated and sustained vestibular and postural impairments instead [91].
Table 2.
Causal treatments for acute unilateral vestibulopathy
| Class | Activity | Drugs | Dosage | Contraindications and side-effects |
|---|---|---|---|---|
| Glucocorticoids | Suppresses immune response by inhibition of the two main products of inflammation: prostaglandins and leukotrienes | Prednisone, oral [89] | 50 mg/day, for 5-7 days, with 7 days tappering | Hyperglycemia, hypertension, insomnia, mania, fatigue, acne. |
| Contraindicated in uncontrolled hyperglycemia, uncontrolled bipolar disease, diabetes mellitus, glaucoma, hypertension, and in herpes simplex and varicella infection, peptic ulcer disease, congestive heart failure. | ||||
| Antivirals | Inhibitor of viral DNA replication thought inhibition and inactivation of the viral DNA polymerase | Methylprednisone, intravenous or oral [89] | 1 mg/kg, for 5 days, with 5 days tappering | |
| Dexamethasone, intravenous [89] | 12-24 mg/day for 7 days, with 7 days tappering | |||
| Valacyclovir [88] | 1,000 mg/ 3 times a day for 7 days | Kidney failure, hallucination/confusion, seizure, headache, nausea | ||
| Contraindicated in kidney disease and immunosuppressive states | ||||
| Vasodilators | Antiplatelet | Ginkgo biloba extract [97] | 120 mg/ twice a day for 12 weeks | Diarrhea,dizziness,headache, stomachache |
| Vasodilator | Contra-indicated with the concomitant use of antiplatelet or anticoagulant drugs and/or haemorrhagic diseases | |||
| Neuromodulator |
Vascular mechanisms and blood related treatments
Vascular changes, as an epiphenomenon mediated by inflammation, have been linked to AUV by significant increases in plasma fibrinogen concentrations and decreased lipoprotein (a) levels [92]. D-dimers, other marker of coronary artery disease, was also found to be higher in patients with AUV [93]. However, whether vascular processes represent a causal cause of AUV remains unknown [93,94]. Evidence suggests an epidemiologic link between cardiovascular risk factors and the prevalence of AUV, with comorbidities such as diabetes, dyslipidemia, hypertension, obesity, ischemic heart disease, and cigarette smoking being higher among AUV patients compared to the general population [95].
Inner ear infarctions cannot currently be seen using current imaging modalities [96]. Nonetheless, Liqun, et al. [96] stated in a recent study that selective labyrinth embolism should be addressed in patients with AUV or auditory symptoms in the presence of concomitant acute infarctions, even if in nonanterior inferior cerebellar artery territories. To date, peripheral vestibular histology does not support vascular occlusion as an etiology of AUV, and there is no significant evidence supporting the use of anticoagulants or antiplatelet medications.
Ginkgo biloba extract (Table 2), a mild antiplatelet compound, has been shown to reduce vascular resistance and improve peripheral blood circulation. However, its use has been mainly studied as a central neuro-modulator in vestibular compensation [97,98]. Preliminary animal model studies indicate this agent as efficient in vestibular compensation through modulation of cerebral vestibular networks [99-101].
Infection hypothesis and the use of antivirals
A viral etiology has long been suspected as being involved in AUV pathogenesis. The epidemiologic timing association between AUV onset and recent upper respiratory tract infections, the detection of herpes virus in the vestibular ganglia, and the similarities found in postmortem histopathological findings in the vestibular nerve/vestibular sensory epithelium and other known viral disorders all lend support to this hypothesis [84,102-104]. Aside from the aforementioned data, there are very few trials utilizing antivirals in AUV, with Strupp, et al. [88] describing that valacyclovir (Table 2) did not enhance vestibular recovery in the setting of AUV. Hence, there are no available standardized guidelines for the use of antivirals.
Table 2 shows some examples of common causal treatments used in AUV, and Fig. 1 summarizes the proposed mechanisms and causal treatments in AUV.
Fig. 1.
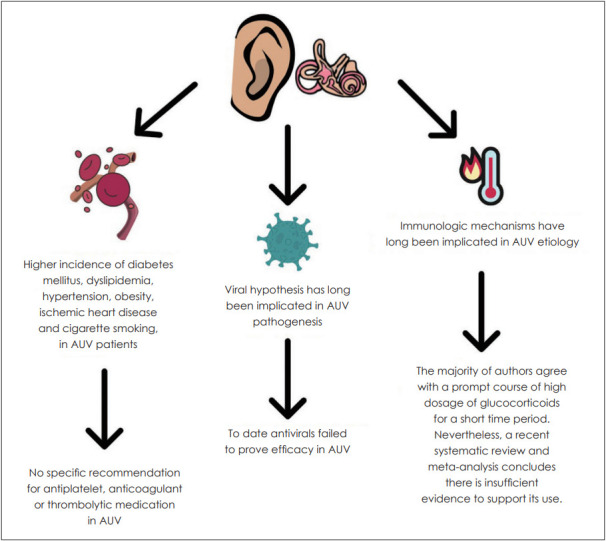
Potential causal mechanisms and therapies for acute unilateral vestibulopathy (AUV).
Conclusion
AUV may have an undefined etiology, but its clinical presentation follows a common pattern for most patients, making it possible to design a comprehensive approach for treatment. Most times, impending vertigo lasting for days ensues and therefore, the first thing to do after diagnosis is to provide symptomatic relief to the patient, which is generally very symptomatic. Vestibular suppressants are almost always in the equation, in order to rapidly alleviate the patient’s neuro-vegetative symptoms (predominantly nausea and vomiting) and intense rotatory vertigo. Pharmacological treatment of AUV is a mainstay in the management of this pathology, allowing for symptomatic relief of truly diseased patients. The clinician should be familiar with the vast and valuable arsenal of vestibular suppressant drugs, in order to be able to use them as wisely and quickly as possible, keeping in mind that central compensation can be compromised if the drugs are used inadvertently for long periods.
On the other hand, prognostic changing treatments to halt the “vestibular shutdown” progression in an early phase are still lacking. This probably reflects the same lack of consensus about AUV causal mechanisms, hindering the development of specific therapeutic targets, with corticosteroids being widely used, although not incontestably. This review ultimately aims to summarize the evidence and guide the clinician towards the best suitable solution in the treatment of AUV.
The topographic diagnosis in AUV is becoming a reality with the advent of video head impulse test [105]. Topography of the involved segments may point to a vascular event in a specific arterial territory as the cause of the AUV, undermining the chance for an inflammatory cause. One example is the suggested selective ischemia at the area of the common cochlear artery when there is an abrupt functional loss of cochlear epithelium, saccular macula and posterior canal ampulla [105]. Furthermore, plasma biomarkers may play a role in separating causative pathways [93].
Thus, and parting from a focus on more efficient diagnostic exams, we believe that the future of the management of AUV may be a more tailored approach to its causal mechanism, as each AUV is unique, and a single case may be one of the multiple subtypes of AUV yet to be described.
Along with the advances in diagnosis, it is also vital to have full confidence when planning a course of treatment [106]. Choosing an adequate treatment may become increasingly difficult as a lot of research is being conducted on AUV symptomatic treatment [39,75], causal treatment [93,94], and vestibular rehabilitation [107]. Furthermore, and despite some debate on the subject [108], there is reasonable evidence that, whereas AUV affects the whole vestibular nerve, vestibular neuritis frequently spares a portion of the nerve [109,110]. As a result, breakthroughs in physical and pharmacological therapy aimed at restoring residual vestibular function and speeding vestibular functioning are expected in AUV [111]. Fig. 2 summarizes future perspectives in AUV diagnosis and treatment.
Fig. 2.
Acute unilateral vestibulopathy (AUV) treatment future perspectives: using video head impulse test towards topographic diagnosis, laboratorial data and imaging towards the causal diagnosis and scientific advancement towards targeted therapy and rehabilitation.
Summary recommendations
In general, there is insufficient evidence to support the effectiveness of anti-vertiginous drugs for AUV. However, betahistine may be effective for peripheral vertigo and may be considered (grade of recommendation: C) [112]. A combination of cinnarizine and dimenhydrinate may be used for improving symptoms in the acute stage of vestibular neuritis (grade of recommendation: B) and can be used for a short period [112]. Betahistine, ondansetron, cinnarizine, flunarizine, dimenhydrinate, and diazepam are among the most widely studied vestibular supressants and should be preferred. Corticosteroids resulted in a statistically significant improvement in vestibular neuritis [113], so that the authors recommend their routine use in AUV. Despite the multitude of therapeutic options, there is a lack for larger, higher quality studies regarding the pharmacological treatment of AUV.
Acknowledgments
We want to thank Dr. Mariline Santos and Dr. João Lino for their support of this work.
Footnotes
Conflicts of Interest
The authors have no financial conflicts of interest.
Author Contributions
Conceptualization: Francisco Alves de Sousa, Ângela Reis Rego. Data curation: Francisco Alves de Sousa, Ângela Reis Rego. Investigation: Francisco Alves de Sousa, Ângela Reis Rego, Clara Serdoura Alves. Methodology: Francisco Alves de Sousa, Ângela Reis Rego. Project administration: Ângela Reis Rego, Ana Nóbrega Pinto, Luís Meireles. Resources: Francisco Alves de Sousa, Ângela Reis Rego. Software: Francisco Alves de Sousa, Ângela Reis Rego. Supervision: Ângela Reis Rego, Luís Meireles. Validation: Ângela Reis Rego, Ana Nóbrega Pinto, Luís Meireles. Writing—original draft: Francisco Alves de Sousa, Ângela Reis Rego. Writing—review & editing: Francisco Alves de Sousa, Ângela Reis Rego, Clara Serdoura Alves, Ana Nóbrega Pinto. Approval of final manuscript: all authors.
REFERENCES
- 1.Strupp M, Dlugaiczyk J, Ertl-Wagner BB, Rujescu D, Westhofen M, Dieterich M. Vestibular disorders. Dtsch Arztebl Int. 2020;117:300–10. doi: 10.3238/arztebl.2020.0300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sekitani T, Imate Y, Noguchi T, Inokuma T. Vestibular neuronitis: epidemiological survey by questionnaire in Japan. Acta Otolaryngol Suppl. 1993;503:9–12. doi: 10.3109/00016489309128061. [DOI] [PubMed] [Google Scholar]
- 3.Strupp M, Magnusson M. Acute unilateral vestibulopathy. Neurol Clin. 2015;33:669–85. doi: 10.1016/j.ncl.2015.04.012. [DOI] [PubMed] [Google Scholar]
- 4.Casani AP, Gufoni M, Capobianco S. Current insights into treating vertigo in older adults. Drugs Aging. 2021;38:655–70. doi: 10.1007/s40266-021-00877-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Curthoys IS. Vestibular compensation and substitution. Curr Opin Neurol. 2000;13:27–30. doi: 10.1097/00019052-200002000-00006. [DOI] [PubMed] [Google Scholar]
- 6.Lacour M, Helmchen C, Vidal PP. Vestibular compensation: the neuro-otologist’s best friend. J Neurol. 2016;263(Suppl 1):S54–64. doi: 10.1007/s00415-015-7903-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Swamy Suman N, Kumar Rajasekaran A, Yuvaraj P, Pruthi N, Thennarasu K. Measure of central vestibular compensation: a review. J Int Adv Otol. 2022;18:441–6. doi: 10.5152/iao.2022.21207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Komazec Z, Lemajić S. [Specific vestibular exercises in the treatment of vestibular neuritis] Med Pregl. 2004;57:269–74. doi: 10.2298/mpns0406269k. Serbian. [DOI] [PubMed] [Google Scholar]
- 9.Low KJY, Phillips M, Pervushin K. Anticholinergic drugs interact with neuroprotective chaperone L-PGDS and modulate cytotoxicity of Aβ amyloids. Front Pharmacol. 2020;11:862. doi: 10.3389/fphar.2020.00862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Soto E, Vega R. Neuropharmacology of vestibular system disorders. Curr Neuropharmacol. 2010;8:26–40. doi: 10.2174/157015910790909511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Svoboda J, Popelikova A, Stuchlik A. Drugs interfering with muscarinic acetylcholine receptors and their effects on place navigation. Front Psychiatry. 2017;8:215. doi: 10.3389/fpsyt.2017.00215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Renner UD, Oertel R, Kirch W. Pharmacokinetics and pharmacodynamics in clinical use of scopolamine. Ther Drug Monit. 2005;27:655–65. doi: 10.1097/01.ftd.0000168293.48226.57. [DOI] [PubMed] [Google Scholar]
- 13.Bajo R, Pusil S, López ME, Canuet L, Pereda E, Osipova D, et al. Scopolamine effects on functional brain connectivity: a pharmacological model of Alzheimer’s disease. Sci Rep. 2015;5:9748. doi: 10.1038/srep09748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Winter J, Hart LL. Transdermal scopolamine in nausea and vomiting. Drug Intell Clin Pharm. 1987;21:712–4. [Google Scholar]
- 15.Antor MA, Uribe AA, Erminy-Falcon N, Werner JG, Candiotti KA, Pergolizzi JV, et al. The effect of transdermal scopolamine for the prevention of postoperative nausea and vomiting. Front Pharmacol. 2014;5:55. doi: 10.3389/fphar.2014.00055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Nachum Z, Shupak A, Gordon CR. Transdermal scopolamine for prevention of motion sickness: clinical pharmacokinetics and therapeutic applications. Clin Pharmacokinet. 2006;45:543–66. doi: 10.2165/00003088-200645060-00001. [DOI] [PubMed] [Google Scholar]
- 17.Gordon CR, Mankuta D, Shupak A, Spitzer O, Doweck I. Recurrent classic migraine attacks following transdermal scopolamine intoxication. Headache. 1991;31:172–4. doi: 10.1111/j.1526-4610.1991.hed3103172.x. [DOI] [PubMed] [Google Scholar]
- 18.Barceló B, Gomila I, de-Castro-Ríos A, Perez-Barcena J, Jimenez C, Lendoiro E, et al. Diminished consciousness in a woman following an unsuspected scopolamine overdose. J Anal Toxicol. 2021;45:e7–14. doi: 10.1093/jat/bkaa135. [DOI] [PubMed] [Google Scholar]
- 19.Castaño Pérez GA, Calderón Vallejo GA, Berbesi Fernández DY. [Use of emerging drugs in Medellín, Colombia] Rev Colomb Psiquiatr. 2013;42:248–56. doi: 10.1016/S0034-7450(13)70017-9. Spanish. [DOI] [PubMed] [Google Scholar]
- 20.Müller J, Wanke K. [Toxic psychoses from atropine and scopolamine] Fortschr Neurol Psychiatr. 1998;66:289–95. doi: 10.1055/s-2007-995265. German. [DOI] [PubMed] [Google Scholar]
- 21.Zabirowicz ES, Gan TJ. In: Pharmacology and Physiology for Anesthesia. 2nd ed. Hemmings HC, Egan TD, editors. Philadelphia, PA: Elsevier; 2019. Pharmacology of postoperative nausea and vomiting; pp. 671–92. [Google Scholar]
- 22.Babin RW, Balkany TJ, Fee WE. Transdermal scopolamine in the treatment of acute vertigo. Ann Otol Rhinol Laryngol. 1984;93(1 Pt 1):25–7. doi: 10.1177/000348948409300106. [DOI] [PubMed] [Google Scholar]
- 23.Schmitt LG, Shaw JE. Alleviation of induced vertigo. Therapy with transdermal scopolamine and oral meclizine. Arch Otolaryngol Head Neck Surg. 1986;112:88–91. doi: 10.1001/archotol.1986.03780010090017. [DOI] [PubMed] [Google Scholar]
- 24.Lau SH, Vaneaton C. Scopolamine patch withdrawal syndrome. Hosp Pharm. 2014;49:218–20. doi: 10.1310/hpj4903-218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Scholtz AW, Schwarz M, Baumann W, Kleinfeldt D, Scholtz HJ. Treatment of vertigo due to acute unilateral vestibular loss with a fixed combination of cinnarizine and dimenhydrinate: a double-blind, randomized, parallel-group clinical study. Clin Ther. 2004;26:866–77. doi: 10.1016/s0149-2918(04)90130-0. [DOI] [PubMed] [Google Scholar]
- 26.Cohen B, DeJong JM. Meclizine and placebo in treating vertigo of vestibular origin. Relative efficacy in a double-blind study. Arch Neurol. 1972;27:129–35. doi: 10.1001/archneur.1972.00490140033006. [DOI] [PubMed] [Google Scholar]
- 27.Huppert D, Strupp M, Mückter H, Brandt T. Which medication do I need to manage dizzy patients? Acta Otolaryngol. 2011;131:228–41. doi: 10.3109/00016489.2010.531052. [DOI] [PubMed] [Google Scholar]
- 28.Sherman CR. Motion sickness: review of causes and preventive strategies. J Travel Med. 2002;9:251–6. doi: 10.2310/7060.2002.24145. [DOI] [PubMed] [Google Scholar]
- 29.Jørgensen EA, Knigge U, Warberg J, Kjaer A. Histamine and the regulation of body weight. Neuroendocrinology. 2007;86:210–4. doi: 10.1159/000108341. [DOI] [PubMed] [Google Scholar]
- 30.Shih RD, Walsh B, Eskin B, Allegra J, Fiesseler FW, Salo D, et al. Diazepam and meclizine are equally effective in the treatment of vertigo: an emergency department randomized double-blind placebo-controlled trial. J Emerg Med. 2017;52:23–7. doi: 10.1016/j.jemermed.2016.09.016. [DOI] [PubMed] [Google Scholar]
- 31.Marken PA, Stoner SC, Bunker MT. Anticholinergic drug abuse and misuse. CNS Drugs. 1996;5:190–9. [Google Scholar]
- 32.Patel PN, Ambizas EM. Meclizine: safety and efficacy in the treatment and prevention of motion sickness. Clin Med Insights Ther. 2011;3:CMT.S6237. [Google Scholar]
- 33.Dyhrfjeld-Johnsen J, Attali P. Management of peripheral vertigo with antihistamines: new options on the horizon. Br J Clin Pharmacol. 2019;85:2255–63. doi: 10.1111/bcp.14046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Takumida M, Takumida H, Anniko M. Localization of histamine (H1, H2, H3 and H4) receptors in mouse inner ear. Acta Otolaryngol. 2016;136:537–44. doi: 10.3109/00016489.2015.1136433. [DOI] [PubMed] [Google Scholar]
- 35.Amini A, Heidari K, Kariman H, Taghizadeh M, Hatamabadi H, Shahrami A, et al. Histamine antagonists for treatment of peripheral vertigo: a meta-analysis. J Int Adv Otol. 2015;11:138–42. doi: 10.5152/iao.2015.1169. [DOI] [PubMed] [Google Scholar]
- 36.Adrion C, Fischer CS, Wagner J, Gürkov R, Mansmann U, Strupp M, BEMED Study Group Efficacy and safety of betahistine treatment in patients with Meniere’s disease: primary results of a long term, multicentre, double blind, randomised, placebo controlled, dose defining trial (BEMED trial) BMJ. 2016;352:h6816. doi: 10.1136/bmj.h6816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Redon C, Lopez C, Bernard-Demanze L, Dumitrescu M, Magnan J, Lacour M, et al. Betahistine treatment improves the recovery of static symptoms in patients with unilateral vestibular loss. J Clin Pharmacol. 2011;51:538–48. doi: 10.1177/0091270010369241. [DOI] [PubMed] [Google Scholar]
- 38.Parfenov VA, Golyk VA, Matsnev EI, Morozova SV, Melnikov OA, Antonenko LM, et al. Effectiveness of betahistine (48 mg/day) in patients with vestibular vertigo during routine practice: the VIRTUOSO study. PLoS One. 2017;12:e0174114. doi: 10.1371/journal.pone.0174114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Petremann M, Gueguen C, Delgado Betancourt V, Wersinger E, Dyhrfjeld-Johnsen J. Effect of the novel histamine H4 receptor antagonist SENS-111 on spontaneous nystagmus in a rat model of acute unilateral vestibular loss. Br J Pharmacol. 2020;177:623–33. doi: 10.1111/bph.14803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Venail F, Attali P, Wersinger E, Gomeni R, Poli S, Schmerber S. Safety, tolerability, pharmacokinetics and pharmacokinetic-pharmacodynamic modelling of the novel H4 receptor inhibitor SENS-111 using a modified caloric test in healthy subjects. Br J Clin Pharmacol. 2018;84:2836–48. doi: 10.1111/bcp.13744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Christofaki M, Papaioannou A. Ondansetron: a review of pharmacokinetics and clinical experience in postoperative nausea and vomiting. Expert Opin Drug Metab Toxicol. 2014;10:437–44. doi: 10.1517/17425255.2014.882317. [DOI] [PubMed] [Google Scholar]
- 42.Saberi A, Pourshafie SH, Kazemnejad-Leili E, Nemati S, Sutohian S, Sayad-Fathi S. Ondansetron or promethazine: which one is better for the treatment of acute peripheral vertigo? Am J Otolaryngol. 2019;40:10–5. doi: 10.1016/j.amjoto.2018.09.010. [DOI] [PubMed] [Google Scholar]
- 43.Braude D, Crandall C. Ondansetron versus promethazine to treat acute undifferentiated nausea in the emergency department: a randomized, double-blind, noninferiority trial. Acad Emerg Med. 2008;15:209–15. doi: 10.1111/j.1553-2712.2008.00060.x. [DOI] [PubMed] [Google Scholar]
- 44.Dyhrfjeld-Johnsen J, Gaboyard-Niay S, Broussy A, Saleur A, Brugeaud A, Chabbert C. Ondansetron reduces lasting vestibular deficits in a model of severe peripheral excitotoxic injury. J Vestib Res. 2013;23:177–86. doi: 10.3233/VES-130483. [DOI] [PubMed] [Google Scholar]
- 45.Venail F, Biboulet R, Mondain M, Uziel A. A protective effect of 5-HT3 antagonist against vestibular deficit? Metoclopramide versus ondansetron at the early stage of vestibular neuritis: a pilot study. Eur Ann Otorhinolaryngol Head Neck Dis. 2012;129:65–8. doi: 10.1016/j.anorl.2011.10.006. [DOI] [PubMed] [Google Scholar]
- 46.Sadawarte P, Bhure A, Deshmukh S, Parate S. Comparative study of oral vs IV ondansetron for reducing PONV in patients undergoing laparoscopic surgery under general anesthesia. Int J Pharm Sci Invent. 2015;4:1–6. [Google Scholar]
- 47.Roila F, Del Favero A. Ondansetron clinical pharmacokinetics. Clin Pharmacokinet. 1995;29:95–109. doi: 10.2165/00003088-199529020-00004. [DOI] [PubMed] [Google Scholar]
- 48.Butcher ME. Global experience with ondansetron and future potential. Oncology. 1993;50:191–7. doi: 10.1159/000227176. [DOI] [PubMed] [Google Scholar]
- 49.Montgomery AM, Rose IC, Herberg LJ. The effect of a 5-HT3 receptor antagonist, ondansetron, on brain stimulation reward, and its interaction with direct and indirect stimulants of central dopaminergic transmission. J Neural Transm Gen Sect. 1993;91:1–11. doi: 10.1007/BF01244914. [DOI] [PubMed] [Google Scholar]
- 50.Tyers MB. Pharmacology and preclinical antiemetic properties of ondansetron. Semin Oncol. 1992;19(4 Suppl 10):1–8. [PubMed] [Google Scholar]
- 51.Zajonc TP, Roland PS. Vertigo and motion sickness. Part II: pharmacologic treatment. Ear Nose Throat J. 2006;85:25–35. [PubMed] [Google Scholar]
- 52.Jagdale SC, Randhave AB. Hydroxyl ethyl cellulose HHX and polymethyl methacrylate based site specific floating delivery of prochlorperazine maleate. Open Pharm Sci J. 2016;3:149–63. [Google Scholar]
- 53.Singh AK, Chaturvedi VN. Prochlorperazine versus cinnarizine in cases of vertigo. Indian J Otolaryngol Head Neck Surg. 1998;50:392–7. doi: 10.1007/BF03000698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Johnson WH, Ireland PE. The control of vertigo by thiethylperazine. Arch Otolaryngol. 1965;82:261–6. doi: 10.1001/archotol.1965.00760010263008. [DOI] [PubMed] [Google Scholar]
- 55.Moser JD, Caldwell JB, Rhule FJ. No more than necessary: safety and efficacy of low-dose promethazine. Ann Pharmacother. 2006;40:45–8. doi: 10.1345/aph.1G282. [DOI] [PubMed] [Google Scholar]
- 56.Dougherty MM, Marraffa JM. In: Encyclopedia of Toxicology. 3rd ed. Wexler P, editor. Oxford: Academic Press; 2014. Phenothiazines; pp. 881–3. [Google Scholar]
- 57.Smith HS, Cox LR, Smith BR. Dopamine receptor antagonists. Ann Palliat Med. 2012;1:137–42. doi: 10.3978/j.issn.2224-5820.2012.07.09. [DOI] [PubMed] [Google Scholar]
- 58.Ercin D, Erdur B, Turkcuer I, Seyit M, Ozen M, Yilmaz A, et al. Comparison of efficacy dimenhydrinate and metoclopramide in the treatment of nausea due to vertigo; a randomized study. Am J Emerg Med. 2021;40:77–82. doi: 10.1016/j.ajem.2020.12.010. [DOI] [PubMed] [Google Scholar]
- 59.Johnson WH, Fenton RS, Evans A. Effects of droperidol in management of vestibular disorders. Laryngoscope. 1976;86:946–54. doi: 10.1288/00005537-197607000-00007. [DOI] [PubMed] [Google Scholar]
- 60.Oosterveld WJ. The combined effect of cinnarizine and domperidone on vestibular susceptibility. Aviat Space Environ Med. 1987;58:218–23. [PubMed] [Google Scholar]
- 61.Irving C, Richman PB, Kaiafas C, Eskin B, Ritter A, Allegra J. Droperidol for the treatment of acute peripheral vertigo. Am J Emerg Med. 1999;17:109–10. doi: 10.1016/s0735-6757(99)90037-2. [DOI] [PubMed] [Google Scholar]
- 62.Holstein GR, Martinelli GP, Cohen B. The ultrastructure of GABA-immunoreactive vestibular commissural neurons related to velocity storage in the monkey. Neuroscience. 1999;93:171–81. doi: 10.1016/s0306-4522(99)00141-4. [DOI] [PubMed] [Google Scholar]
- 63.Holstein GR, Martinelli GP, Boyle R, Rabbitt RD, Highstein SM. Ultrastructural observations of efferent terminals in the crista ampullaris of the toadfish, opsanus tau. Exp Brain Res. 2004;155:265–73. doi: 10.1007/s00221-003-1734-8. [DOI] [PubMed] [Google Scholar]
- 64.Sekitani T, McCabe BF, Ryu JH. Drug effects on the medial vestibular nucleus. Arch Otolaryngol. 1971;93:581–9. doi: 10.1001/archotol.1971.00770060883007. [DOI] [PubMed] [Google Scholar]
- 65.Ganança MM, Caovilla HH, Ganança FF, Ganança CF, Munhoz MS, da Silva ML, et al. Clonazepam in the pharmacological treatment of vertigo and tinnitus. Int Tinnitus J. 2002;8:50–3. [PubMed] [Google Scholar]
- 66.Stensrud P, Sjaastad O. Clonazepam (rivotril) in migraine prophylaxis. Headache. 1979;19:333–4. doi: 10.1111/j.1526-4610.1979.hed1906333.x. [DOI] [PubMed] [Google Scholar]
- 67.Ferrary E, Tran Ba Huy P, Roinel N, Bernard C, Amiel C. Calcium and the inner ear fluids. Acta Otolaryngol Suppl. 1988;460:13–7. doi: 10.3109/00016488809125130. [DOI] [PubMed] [Google Scholar]
- 68.Mammano F, Bortolozzi M, Ortolano S, Anselmi F. Ca2+ signaling in the inner ear. Physiology (Bethesda) 2007;22:131–44. doi: 10.1152/physiol.00040.2006. [DOI] [PubMed] [Google Scholar]
- 69.Soto E, Vega R, Seseña E. Neuropharmacological basis of vestibular system disorder treatment. J Vestib Res. 2013;23:119–37. doi: 10.3233/VES-130494. [DOI] [PubMed] [Google Scholar]
- 70.Lee JA, Watson LA, Boothby G. Calcium antagonists in the prevention of motion sickness. Aviat Space Environ Med. 1986;57:45–8. [PubMed] [Google Scholar]
- 71.Lepcha A, Amalanathan S, Augustine AM, Tyagi AK, Balraj A. Flunarizine in the prophylaxis of migrainous vertigo: a randomized controlled trial. Eur Arch Otorhinolaryngol. 2014;271:2931–6. doi: 10.1007/s00405-013-2786-4. [DOI] [PubMed] [Google Scholar]
- 72.Oosterveld WJ. Vestibular pharmacology of flunarizine compared to that of cinnarizine. ORL J Otorhinolaryngol Relat Spec. 1974;36:157–64. doi: 10.1159/000275168. [DOI] [PubMed] [Google Scholar]
- 73.Fields T, Patterson M, Bremova-Ertl T, Belcher G, Billington I, Churchill GC, et al. A master protocol to investigate a novel therapy acetyl-L-leucine for three ultra-rare neurodegenerative diseases: NiemannPick type C, the GM2 gangliosidoses, and ataxia telangiectasia. Trials. 2021;22:84. doi: 10.1186/s13063-020-05009-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Churchill GC, Strupp M, Galione A, Platt FM. Unexpected differences in the pharmacokinetics of N-acetyl-DL-leucine enantiomers after oral dosing and their clinical relevance. PLoS One. 2020;15:e0229585. doi: 10.1371/journal.pone.0229585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Günther L, Beck R, Xiong G, Potschka H, Jahn K, Bartenstein P, et al. N-acetyl-L-leucine accelerates vestibular compensation after unilateral labyrinthectomy by action in the cerebellum and thalamus. PLoS One. 2015;10:e0120891. doi: 10.1371/journal.pone.0120891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Beck R, Günther L, Xiong G, Potschka H, Böning G, Bartenstein P, et al. The mixed blessing of treating symptoms in acute vestibular failure--evidence from a 4-aminopyridine experiment. Exp Neurol. 2014;261:638–45. doi: 10.1016/j.expneurol.2014.08.013. [DOI] [PubMed] [Google Scholar]
- 77.Strupp M, Teufel J, Zwergal A, Schniepp R, Khodakhah K, Feil K. Aminopyridines for the treatment of neurologic disorders. Neurol Clin Pract. 2017;7:65–76. doi: 10.1212/CPJ.0000000000000321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Alviña K, Khodakhah K. The therapeutic mode of action of 4-aminopyridine in cerebellar ataxia. J Neurosci. 2010;30:7258–68. doi: 10.1523/JNEUROSCI.3582-09.2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Etzion Y, Grossman Y. Highly 4-aminopyridine sensitive delayed rectifier current modulates the excitability of guinea pig cerebellar Purkinje cells. Exp Brain Res. 2001;139:419–25. doi: 10.1007/s002210100788. [DOI] [PubMed] [Google Scholar]
- 80.Jen JC, Graves TD, Hess EJ, Hanna MG, Griggs RC, Baloh RW, CINCH investigators Primary episodic ataxias: diagnosis, pathogenesis and treatment. Brain. 2007;130(Pt 10):2484–93. doi: 10.1093/brain/awm126. [DOI] [PubMed] [Google Scholar]
- 81.Kalla R, Strupp M. Aminopyridines and acetyl-DL-leucine: new therapies in cerebellar disorders. Curr Neuropharmacol. 2019;17:7–13. doi: 10.2174/1570159X16666180905093535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Mitoma H, Manto M. The physiological basis of therapies for cerebellar ataxias. Ther Adv Neurol Disord. 2016;9:396–413. doi: 10.1177/1756285616648940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Hiyoshi M, Sekitani T. Vertigo consistent with the so-called vestibular neuronitis after influenza vaccination. Pract Oto-Rhino-Laryngol. 1982;75(supplement 1):260–5. [Google Scholar]
- 84.Davis LE. Viruses and vestibular neuritis: review of human and animal studies. Acta Otolaryngol Suppl. 1993;113(sup503):70–3. doi: 10.3109/00016489309128077. [DOI] [PubMed] [Google Scholar]
- 85.Bumm P, Schlimok G. [Lymphocyte subpopulations and HLA-DR determinations in diseases of the inner ear and Bell’s palsy] HNO. 1986;34:525–7. German. [PubMed] [Google Scholar]
- 86.Oh EH, Rhee JK, Shin JH, Cho JW, Kim DS, Park JY, et al. Neutrophil-mediated immune response as a possible mechanism of acute unilateral vestibulopathy. J Vestib Res. 2020;30:363–74. doi: 10.3233/VES-200044. [DOI] [PubMed] [Google Scholar]
- 87.Kassner SS, Schöttler S, Bonaterra GA, Stern-Straeter J, Hormann K, Kinscherf R, et al. Proinflammatory activation of peripheral blood mononuclear cells in patients with vestibular neuritis. Audiol Neurootol. 2011;16:242–7. doi: 10.1159/000320839. [DOI] [PubMed] [Google Scholar]
- 88.Strupp M, Zingler VC, Arbusow V, Niklas D, Maag KP, Dieterich M, et al. Methylprednisolone, valacyclovir, or the combination for vestibular neuritis. N Engl J Med. 2004;351:354–61. doi: 10.1056/NEJMoa033280. [DOI] [PubMed] [Google Scholar]
- 89.Hegemann SCA, Wenzel A. Diagnosis and treatment of vestibular neuritis/neuronitis or peripheral vestibulopathy (PVP)? Open questions and possible answers. Otol Neurotol. 2017;38:626–31. doi: 10.1097/MAO.0000000000001396. [DOI] [PubMed] [Google Scholar]
- 90.Leong KJ, Lau T, Stewart V, Canetti EFD. Systematic review and meta-analysis: effectiveness of corticosteroids in treating adults with acute vestibular neuritis. Otolaryngol Head Neck Surg. 2021;165:255–66. doi: 10.1177/0194599820982910. [DOI] [PubMed] [Google Scholar]
- 91.El Mahmoudi N, Rastoldo G, Marouane E, Péricat D, Watabe I, Tonetto A, et al. Breaking a dogma: acute anti-inflammatory treatment alters both post-lesional functional recovery and endogenous adaptive plasticity mechanisms in a rodent model of acute peripheral vestibulopathy. J Neuroinflammation. 2021;18:183. doi: 10.1186/s12974-021-02222-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Milionis HJ, Mittari V, Exarchakos G, Kalaitzidis R, Skevas AT, Elisaf MS. Lipoprotein (a) and acute-phase response in patients with vestibular neuronitis. Eur J Clin Invest. 2003;33:1045–50. doi: 10.1111/j.1365-2362.2003.01275.x. [DOI] [PubMed] [Google Scholar]
- 93.Fattori B, Ursino F, Cristofani R, Galetta F, Nacci A. Relevance of plasma D-dimer measurement in patients with acute peripheral vertigo. J Laryngol Otol. 2003;117:467–72. doi: 10.1258/002221503321892316. [DOI] [PubMed] [Google Scholar]
- 94.Bartual-Pastor J. Vestibular neuritis: etiopathogenesis. Rev Laryngol Otol Rhinol (Bord) 2005;126:279–81. [PubMed] [Google Scholar]
- 95.Oron Y, Shemesh S, Shushan S, Cinamon U, Goldfarb A, Dabby R, et al. Cardiovascular risk factors among patients with vestibular neuritis. Ann Otol Rhinol Laryngol. 2017;126:597–601. doi: 10.1177/0003489417718846. [DOI] [PubMed] [Google Scholar]
- 96.Liqun Z, Park KH, Kim HJ, Lee SU, Choi JY, Kim JS. Acute unilateral audiovestibulopathy due to embolic labyrinthine infarction. Front Neurol. 2018;9:311. doi: 10.3389/fneur.2018.00311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Sokolova L, Hoerr R, Mishchenko T. Treatment of vertigo: a randomized, double-blind trial comparing efficacy and safety of Ginkgo biloba extract EGb 761 and betahistine. Int J Otolaryngol. 2014;2014:682439. doi: 10.1155/2014/682439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Mehlsen J, Drabaek H, Wiinberg N, Winther K. Effects of a Ginkgo biloba extract on forearm haemodynamics in healthy volunteers. Clin Physiol Funct Imaging. 2002;22:375–8. doi: 10.1046/j.1475-097x.2002.00445.x. [DOI] [PubMed] [Google Scholar]
- 99.Lindner M, Gosewisch A, Eilles E, Branner C, Krämer A, Oos R, et al. Ginkgo biloba extract EGb 761 improves vestibular compensation and modulates cerebral vestibular networks in the rat. Front Neurol. 2019;10:147. doi: 10.3389/fneur.2019.00147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Duverger D, DeFeudis FV, Drieu K. Effects of repeated treatments with an extract of Ginkgo biloba (EGb 761) on cerebral glucose utilization in the rat: an autoradiographic study. Gen Pharmacol. 1995;26:1375–83. doi: 10.1016/0306-3623(94)00309-b. [DOI] [PubMed] [Google Scholar]
- 101.Lacour M, Ez-Zaher L, Raymond J. Plasticity mechanisms in vestibular compensation in the cat are improved by an extract of Ginkgo biloba (EGb 761) Pharmacol Biochem Behav. 1991;40:367–79. doi: 10.1016/0091-3057(91)90568-m. [DOI] [PubMed] [Google Scholar]
- 102.Dix MR, Hallpike CS. The pathology symptomatology and diagnosis of certain common disorders of the vestibular system. Proc R Soc Med. 1952;45:341–54. [PMC free article] [PubMed] [Google Scholar]
- 103.Schuknecht HF, Kitamura K. Second Louis H. Clerf lecture. Vestibular neuritis. Ann Otol Rhinol Laryngol Suppl. 1981;90(1 Pt 2):1–19. [PubMed] [Google Scholar]
- 104.Arbusow V, Schulz P, Strupp M, Dieterich M, von Reinhardstoettner A, Rauch E, et al. Distribution of herpes simplex virus type 1 in human geniculate and vestibular ganglia: implications for vestibular neuritis. Ann Neurol. 1999;46:416–9. doi: 10.1002/1531-8249(199909)46:3<416::aid-ana20>3.0.co;2-w. [DOI] [PubMed] [Google Scholar]
- 105.Castellucci A, Pepponi E, Bertellini A, Senesi C, Bettini M, Botti C, et al. Case report: filling defect in posterior semicircular canal on MRI with balanced steady-state gradient-echo sequences after labyrinthine ischemia in the common cochlear artery territory as an early sign of fibrosis. Front Neurol. 2021;11:608838. doi: 10.3389/fneur.2020.608838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Ardıç FN, Tümkaya F. Evidence-based medical treatment in peripheral vestibular diseases. Turk Arch Otolaryngol. 2014;52:61–6. [Google Scholar]
- 107.Heffernan A, Abdelmalek M, Nunez DA. Virtual and augmented reality in the vestibular rehabilitation of peripheral vestibular disorders: systematic review and meta-analysis. Sci Rep. 2021;11:17843. doi: 10.1038/s41598-021-97370-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Lu YC, Young YH. Vertigo from herpes zoster oticus: superior or inferior vestibular nerve origin? Laryngoscope. 2003;113:307–11. doi: 10.1097/00005537-200302000-00020. [DOI] [PubMed] [Google Scholar]
- 109.Fetter M, Dichgans J. Vestibular neuritis spares the inferior division of the vestibular nerve. Brain. 1996;119(Pt 3):755–63. doi: 10.1093/brain/119.3.755. [DOI] [PubMed] [Google Scholar]
- 110.Gianoli G, Goebel J, Mowry S, Poomipannit P. Anatomic differences in the lateral vestibular nerve channels and their implications in vestibular neuritis. Otol Neurotol. 2005;26:489–94. doi: 10.1097/01.mao.0000169787.99835.9f. [DOI] [PubMed] [Google Scholar]
- 111.Fawzy M, Khater A. Bilateral vestibulopathy treatment: update and future directions. Egypt J Otolaryngol. 2016;32:83–92. [Google Scholar]
- 112.Hashimoto M, Koizuka I, Yamashita H, Suzuki M, Omori K, Origasa H, et al. Diagnostic and therapeutic strategies for vestibular neuritis of the Japan society for equilibrium research. Auris Nasus Larynx. 2022 Dec 27; doi: 10.1016/j.anl.2022.12.005. [Epub]. Available from: [DOI] [PubMed] [Google Scholar]
- 113.Bogdanova A, Dlugaiczyk J, Heckmann JG, Schwab S. Corticosteroids in patients with vestibular neuritis: an updated meta-analysis. Acta Neurol Scand. 2022;146:429–39. doi: 10.1111/ane.13676. [DOI] [PubMed] [Google Scholar]