

Overweight and obesity are pressing public health problems and development of these conditions is linked to the earliest life stages. 1 These early life stages include infancy (0 through 11 months) and toddlerhood (12 through 23 months),1 collectively referred to as birth to 24 months (B-24). Systematic reviews from the Pregnancy and Birth to 24 Months (P/B-24) Project found that risk of childhood obesity is associated with the types of foods introduced during the complementary feeding period,2,3 which begins at about age six months when complementary foods and beverages are first introduced and continues to age 24 months as children transition to family foods.4 There is mounting evidence that the dietary patterns established during complementary feeding are not only associated with current and future weight status2,3,5 and health outcomes,6 but also associated with diet quality in later life stages. For example, intake of fruits, vegetables, and sugar sweetened beverages, during infancy are associated with fruit and vegetable7 and sugar sweetened beverage8 intakes at age six. Additionally, risk for childhood obesity may begin even before solid foods are introduced, as breastfeeding is also associated with childhood indicators of higher diet quality and reduced risk of obesity.9–11
In recognition that infant and toddler nutrition can influence diet quality and health outcomes throughout the lifespan, the Dietary Guidelines for Americans (DGA), 2020–2025 for the first time included comprehensive dietary recommendations for birth to 24 months of age (B-24) and established dietary patterns for the second year of life.1 This latest edition of the DGA emphasizes that “every bite counts” at every life stage. In contrast to the popular but not evidence-based rhyme, “food before one is just for fun”,12 this new and evidence-based mantra that “every bite counts” highlights the importance of every bite, especially as feeding and eating behaviors are introduced and learned during early life stages.
Since every bite counts, the field of infant and toddler nutrition now faces a challenge: How do we count (measure) every bite?
Given the need to measure the new DGA recommendations for infants and toddlers, a new dietary assessment work group, described below, was formed. The purpose of this commentary paper by National Collaborative for Childhood Obesity Research (NCCOR) colleagues is to propose a process for identifying measurement gaps and to provide research recommendations for closing those gaps.
Formation of the NCCOR B-24 Diet Assessment Work Group
The evaluation of interventions, nutrition education tools, dietetics practices, and policy changes that are designed to improve B-24 dietary patterns is contingent on precise collection and analysis of dietary data. Measurement has been a focus of the National Collaborative for Childhood Obesity Research (NCCOR) for over a decade, beginning with its emphasis on developing tools such as the NCCOR Measures Registry and Measures Registry Learning Suite.13,14 NCCOR brings together the four leading funders of childhood obesity research: the Centers for Disease Control and Prevention (CDC), the National Institutes of Health (NIH), the Robert Wood Johnson Foundation (RWJF), and the U.S. Department of Agriculture (USDA). With participation from each of these four leaders, NCCOR represents a partnership that continually assesses the needs in childhood obesity research, develops joint projects to address gaps and make strategic advancements, and works together to generate synergetic ideas to reduce childhood obesity.15
In response to the 2020–2025 DGA and the 2020–2030 Strategic Plan for NIH Nutrition Research,1,16 a new NCCOR B-24 Diet Assessment Work Group was formed in March 2021 and met bi-weekly for one year to identify existing measurement tools and methods, as well as potential gaps in these areas. The work group is comprised of thirteen members from multiple agencies, including: USDA Food and Nutrition Service (Center for Nutrition Policy and Promotion and Office of Policy Support), CDC (Division of Nutrition, Physical Activity, and Obesity), National Institutes of Health (National Cancer Institute; Eunice Kennedy Shriver National Institute of Child Health and Human Development) and was facilitated by FHI360. The work group’s long-term goal is to identify research gaps to spur innovative research for the development of new measurement tools and methods that can be used to generate data to inform future iterations of the B-24 dietary guidelines. This work is intended to complement existing federal funding initiatives focused on nutrition in young children less than five years of age.17,18
To identify the most effective ways to inform future B-24 dietary guidelines, the work group reviewed the “Future Directions” in the Scientific Report of the 2020 Dietary Guidelines Advisory Committee.4 Given work group members’ expertise in assessment methods and surveillance systems, the following Future Directions from the Committee were selected to anchor the work: “1) Improve dietary assessment methods that can more accurately estimate energy intakes feasible for use in federal surveillance and monitoring; and 2) Implement surveillance systems to gather more information about the contextual aspects of food and beverage intake, such as the frequency and/or timing of food and beverage consumption.”4
The USDA and the Department of Health and Human Services (HHS) are mandated to jointly publish the DGA every five years, based on the preponderance of current scientific and medical knowledge. Therefore, each new edition of the DGA relies on advancements made by the nutrition research community to address limitations and gaps in the research. The inclusion of infants and toddlers in the 2020–2025 DGA led the group to inventory and critically appraise existing tools to assess dietary practices of the B-24 population using one 2020–2025 DGA recommendation as a case study. The process for identifying measurement gaps from the case study is detailed next.
Process for Identifying Measurement Gaps
With a focus on measurement gaps with immediate applications for assessment methods and surveillance, the work group developed a process to identify research gaps. First, one key recommendation for the B-24 population was selected from the 2020–2025 DGA to use as a model for this case study. The guideline selected was the recommendation to exclusively feed infants human milk for about the first six months of life, or feed infants iron-fortified infant formula when human milk is unavailable.1 Next, a framework was created to characterize the full landscape of methods to measure the exclusive human milk/formula feeding dietary recommendation.
Dietary intake is both multidimensional (i.e., it is a complex, multi-layered exposure and behavior) and dynamic (i.e., it varies over time and the life course).19 To incorporate multidimensionality and dynamism into the approach, the following layers of multidimensionality were considered: who, what, when, where, why, how. These layers are important because they synergistically influence the “what” such that the overall combination of the who, what, when, where, why, and how describes infant and toddler feeding practices. For example, a daycare provider (who) might feed a child cooked vegetables (what) at the daycare’s (where) 2 PM snack time (when) based on reimbursable meal options (why). However, multidimensional information is not captured in all dietary studies, and has not been used consistently to inform dietary guidance. Nonetheless, other expert bodies have reviewed the literature and put forward evidence-based recommendations; for example, Healthy Eating Research provides recommendations for not just what but also how to feed infants and toddlers using a responsive parenting approach.20
The NCCOR B-24 Work Group identified sample research questions for all layers of multidimensionality, including who, what, when, where, why, and how. The sample research questions were mapped to existing measurement tools and methods, and measurement gaps were recorded. The work group then solicited feedback from the academic research community by consulting three experts with knowledge of: lactation/infant nutrition; dietary assessment of children in limited resource community settings; innovative technologies for dietary measurement (e.g. wearable sensors). Two of the experts are registered dietitians and all three hold PhDs in relevant fields and were identified based on their ongoing research programs. The experts were consulted to provide feedback on the research questions and measurement tools identified in Table 1.
Table 1.
Sample research questions, measurement tools, measurement gaps, and innovations to fill gap for multidimensional layers of dietary patterns for Birth to 24 Months (B-24). Case Study: For about the first 6 months of life, exclusively feed infants human milk. Continue to feed infants human milk through at least the first year of life, and longer if desired. Feed infants iron-fortified infant formula during the first year of life when human milk is unavailable.
| Sample Research Question | Measurement Tools Availablea | Measurement Gaps and Limitations | Example of Innovation to Fill Gap | |
|---|---|---|---|---|
| WHO b | Who feeds the infant human milk or infant formula? (e.g., parent, caregiver, self-feeding) | Short time periods | Context specific probes are not typically included to assess who feeds the infant. | Include probes for who feeds the infant for each food or beverage consumed. |
| Longer time periods | Can assess usual intake but lacks details about who is performing the feeding. | |||
| Novel/Innovative methods | High respondent and researcher burden possible. | Use passive video capture and face recognition software to identify who feeds the infant on each eating occasion. | ||
| Who else is present during feeding? (e.g., other children) | Short time periods | Context specific probes not typically included to assess who else is present during feeding. | Include probes for who else is present when the infant is fed | |
| Longer time periods | Can assess usual intake but lacks details about who is present during feeding. | |||
| Novel/Innovative methods | High respondent and researcher burden possible | Adapt Exposure Notification Systems (currently used to map potential COVID exposure with cell phone proximity) to identify who was present at the feeding. | ||
| WHAT c | What was the first feeding after birth? | Short time periods | There is a small window of opportunity to collect data on first feeding after birth. | Standardize use of Electronic Medical Records to integrate with data collected on birth certificate. Collect data at hospital discharge or at first postnatal pediatric appointment. |
| Longer time periods | Reporting errors may occur. This option relies on accurate recall of the first feeding after birth. | Adjust for measurement error and social desirability bias when possible. | ||
| Is there mixed feeding? If so, what is the ratio of human milk feeding to infant formula? | Short time periods | Can assess what was fed (e.g. human milk vs. formula) but volume of human milk expression is difficult to measure. | Add probes to capture mixed feeding occasions and quantities consumed. | |
| Longer time periods | Can assess usual intake but lacks details about quantities fed. | Develop apps that objectively yet passively collect this information to reduce respondent reporting burden. Conduct user-testing on smart phones apps to ensure intuitive user interface to maximize ease of use and reduce missing data. | ||
| Novel/Innovative methods | Biomarkers: Expensive, moderate risk diagnostic tools exist but few are validated for B-24 population. | Leverage carbon isotope ratios to tease apart human milk from formula intake. | ||
| WHEN d | When was the first feeding after birth? | Short time periods | Measurement error for recalling time of eating is not well characterized. | Combine multiple methods of dietary assessment to understand measurement error of time reporting. |
| Longer time periods | Not well suited to capture this type of information | |||
| Novel/Innovative methods | High respondent and researcher burden possible. | Apply Ecological Momentary Assessment or adapt/expand Electronic Medical Records to capture infant feeding behavior during birth hospitalization (i.e., hourly data collections). |
||
| What is the duration of human milk consumption? | Short time periods | Single administration not well suited to capture this type of information | ||
| Longer time periods | Not well suited to capture this type of information | |||
| Novel/Innovative methods | High respondent and researcher burden possible | Apply Ecological Momentary Assessment and develop programs to query and capture information on duration of human milk consumption. | ||
| WHERE e | Where is the infant typically fed? | Short time periods | Context specific probes not typically included for location of feeding. | For each food or beverage consumed, ask where the infant is fed. |
| Longer time periods | Can assess “usual” but can lack detail on where the food was consumed. | |||
| Novel/Innovative methods | High respondent and researcher burden possible | Use room cameras to capture where the infant is fed. Pair phone GPS of the primary feeder with infant feeding reports. |
||
| WHY f | If the infant was not exclusively fed human milk, why was formula introduced? | Short time periods | Not well suited to capture this type of information | |
| Longer time periods | Not well suited to capture this type of information | |||
| Novel/Innovative methods | Not well suited to capture this type of information | |||
| HOW g | How is the human milk fed to the infant: from the chest, bottle, or other device? | Short time periods | Context specific probes not included for how the milk or formula was administered | At each feeding, ask how human milk was fed. |
| Longer time periods | Can assess “usual” intake (what) but often lacks questions about behavioral feeding patterns (how) | Include questions to clarify how the human milk or infant formula was administered. | ||
| Novel/Innovative methods | High respondent and researcher burden possible | Use room cameras, body cameras, smart bottles or other devices to capture feeding details and pair with short-term methods. |
Measurement tools included represent tools validated for research use in the B-24 population; tools developed for consumer use could be included in the future upon further evaluation and validation for research purposes in the B-24 population. Measurement tools are categorized into tools that assess diet over short time periods (i.e. intake on a given day), such as one 24-hour recall; tools that assess diet over longer time periods (i.e. usual frequency), such as food frequency questionnaires; and new innovative methods that can assess diet over variable time periods, such as image-based devices.
Additional WHO questions:
• Who feeds the infant human milk or infant formula? (e.g., parent, caregiver, self-feeding?)
○ Additional Consideration: How is self-feeding defined?
• Who provides information to the parents regarding infant feeding decisions (prenatal and at birth)?
• Who provided support at birth and after hospital discharge (e.g., RN, IBCLC, RDN, WIC BFPC, doulas, family, social media)
• Who provided instructions on how to prepare infant formula?
• Who provided instructions on how to feed by bottle?
• Who is being fed? Are there multiples? Is an older infant also being fed?
Additional WHAT questions:
• What is the quality of human milk fed to the infant? E.g., what is the diet quality of the lactating parent? For expressed human milk, what storage practices were used?
• Was there mixed feeding?
○ Additional Consideration: How does the ratio of infant formula to human milk change in the child’s first year of life? What is the intensity, proportion, or amount of human milk consumed by mixed fed infants?
• Was human milk ever fed?
• If infant formula is consumed, what type? (e.g., iron-fortified, milk-based, soy-based, homemade – not recommended)
• Is the infant fed fresh pumped milk, or previously frozen?
• What supplement(s) is the infant consuming? What supplement(s) is the lactating parent consuming?
• Is toddler formula consumed? If so what type?
• What ways was the milk/formula fortified by the caregiver (e.g., with supplements, cereal, sugar, etc.)
Additional WHEN questions:
• What is the duration of human milk consumption?
○ Additional Consideration: Did it continue beyond 24 months of age?
• What is the duration of exclusive human milk consumption?
• When was the first time something other than human milk was introduced? When were foods introduced for taste? When
• were foods introduced for nutritive feeding that displaced energy from milk/formula?
Additional WHERE questions:
• Where does the infant receive human milk vs. infant formula?
• Where was the human milk or formula obtained? (e.g., lactating parent, milk bank, friend, social media, store, etc.)
• Where did the parent/caregiver obtain early infant feeding information and support?
• Where did the birth occur? (e.g., hospital, at home, birthing center, car)
Additional WHY questions:
• If the infant was not exclusively fed human milk, why was formula introduced?
○ Additional Considerations: Probe about source of beliefs. E.g., Why do they feel the infant was not satisfied?
Additional HOW questions:
• How does type of infant formula fed change over the first year (if it does change)?
• How do we assess responsive feeding/feeding on demand for human milk vs. formula feeding?
• How was infant formula prepared and stored?
• How was expressed human milk prepared (including warmed) and stored (including duration of storage)? Was the human milk expressed in the morning and fed later in the day? Was it frozen and fed days/weeks/months later?
• How does time impact feeding practices? Are parents trying to align with ‘chronobiology?’ What is the clinical relevance of observed chronobiological shifts in human milk composition? What are the unintended consequences of trying to align with chronobiology in terms of caregiver burden?
• Was the infant fed on demand vs. on a schedule?
• How was the infant held or positioned during feeding?
• When introducing complementary foods, in what order is human milk/complementary foods fed within the feeding session?
• How did the infant interact with the feeder during the eating occasion?
In the section below, the example of exclusive human milk/formula feeding is used to demonstrate the breadth and depth of research needed to advance the knowledge base that will inform future iterations of the DGA for the B-24 population. Other researchers may wish to replicate the case study and related table for other B-24 recommendations in the 2020–2025 DGA to identify other areas for innovation.
Case Study: Human Milk/Formula Feeding in the First Six Months of Life
The 2020–2025 DGA provide evidence-based food and beverage recommendations for what to eat, reinforced by the central theme that every bite counts. Most dietary data collection tools (e.g., 24-hour recalls, food records and dairies, food frequency questionnaires, image-based dietary assessment) capture what foods are being consumed. Consequently, most dietary assessment and analysis methods (e.g., diet quality indices) also evaluate what was consumed. These existing tools are rapidly being adapted for use in the B-24 population. For example, image-based dietary assessment has been used with infants,21 and toddler diet quality indices have been developed and evaluated to measure alignment with the 2020–2025 DGA.22–24 To characterize the full dietary landscape of B-24 nutrition, existing tools could continue to evolve to capture repeated measures of multiple constructs in order to address the multidimensionality and dynamism of dietary data.
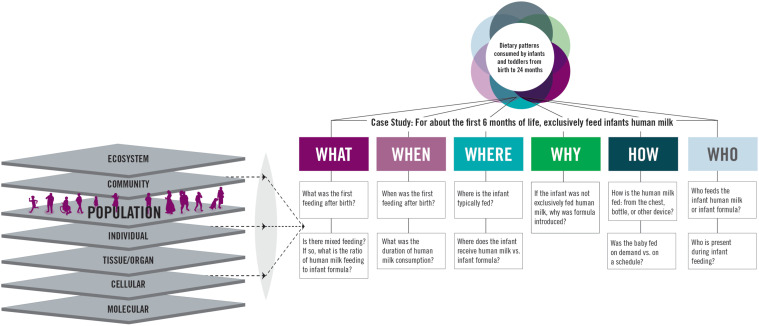
Supplementary Figure 1 represents a case study on the dietary recommendation to exclusively feed infants human milk, or formula when human milk is unavailable, for about the first six months of life. Sample research questions related to human milk/formula intake are shown for all layers of multidimensionality. Table 1 then pairs these sample research questions to existing measurement tools, and identifies measurement gaps and potential innovations to fill the gap. In the table, the column “Measurement Tools Available” refers to tools that have been validated for use in research; products developed for consumer use could be included in the future upon further evaluation for research purposes in the B-24 population. The examples provided in the table are not exhaustive across all layers of multidimensionality. Importantly, they should not be assumed to be applicable to every research question without adaptation for the population under investigation. Further, given the sensitivity associated with infant feeding choices, any research conducted should seek to embed equity, diversity, and inclusion into each step of the praxis to ensure historically omitted communities, cultures, and individuals are provided an equal voice and truthful representation in the action, theory, and reflection processes of science as we seek to fulfill the objectives of inclusive knowledge and discovery. Since the information in the table was based on a case study that used one dietary recommendation, the information is not intended to substitute for a comprehensive or systematic literature review; it is provided to spur research ideas.
In the “who” layer of multidimensionality, sample questions include: Who is feeding human milk or formula to the infant? Who is present during the feeding? (e.g., breastfeeding in private vs. in common spaces). Measurement tools available to address these questions include tools that assess diet over short time periods (i.e., intake on a given day), such as one 24-hour recall; tools that assess diet over longer time periods (i.e., usual frequency), such as food frequency questionnaires; and new innovative methods that can assess diet over variable time periods, such as image-based devices. Although it is possible to explore these questions with existing tools, there are limitations. In most 24-hour recalls, context-specific probes are not included to capture who is performing the feeding. However, flexible, web-based tools like the National Cancer Institute’s (NCI) Automated Self-Administered 24-Hour Dietary Assessment Tool (ASA24),25 have the potential to be programmed to collect such information. The ASA24 already has multiple modules that researchers can turn on or off, including modules to query where meals were eaten (where), whether meals were eaten alone or with others (who), television and computer use during meals (how), source of foods (where), and the timing of both eating and sleeping (when).26 Though possible, these additional modules have the potential to increase the length of time to complete a 24-hour dietary recall and could increase respondent burden. Innovative digital technologies have been developed to objectively yet passively collect information on dietary intake,27–29 but further innovation to address multiple layers of multidimensionality plus adaptation for use in the B-24 population is needed.
Overall, across all who, what, when, where, why, and how layers of multidimensionality, multiple research questions were identified and matched to existing measurement methods. Common measurement limitations included lack of context-specific probes, high respondent burden, and being resource (time or money) intensive. Ultimately there was overlap in the measurement gaps across several domains, meaning that innovative solutions to address one domain (e.g. who) may be transferable to other contexts (e.g. where).
Measurement Research Gaps
An important output from the review of science to inform the DGA is the identification and documentation of research gaps and methodological limitations. These gaps and limitations form the basis of research recommendations that describe the research, data, and methodological advances that are needed to strengthen the body of evidence available to inform dietary guidance. These research opportunities speak not only to what to eat for good health, but also call for more information on multidimensional layers of dietary intake. Experts have identified research gaps to inform future B-24 DGA,4,30 with complementary foods, lactation, and frequency of eating noted as research gaps that are currently being addressed by an NIH-funded project.30 To complement the existing literature, additional B-24 research opportunities that are measurement-specific are presented below.
Limitations for measuring “what” was consumed
Ample tools are available for measuring dietary intake though limitations remain. The limitations of self-reported dietary intake data are well documented,31,32 and although strategies exist to address issues such as measurement error,32–35 there are also unique considerations for the B-24 population.
Measuring Quantity: It is difficult to measure the quantity of foods consumed while adjusting for atypical sources of food waste (e.g. food thrown on floor or food stuck in hair). Methods for adjusting for this type of measurement error require further exploration.
Proxy Reporting: Children’s intakes are reported via a proxy respondent in national surveys like the National Health and Nutrition Examination Survey (NHANES).36 Proxy reporting may be particularly challenging in situations where the distribution of feeding responsibilities is spread across multiple caregivers (e.g. daycare staff, nanny, parent, and older sibling) and the impact this has on the accuracy of reported foods has not been quantified.
Biased Reporting: Social desirability bias and other factors lead to energy underreporting in dietary surveillance,31 however, both the magnitude and direction of misreporting (either under- or over-reporting) remains unknown for the B-24 population.
Usual Intake: Dietary data from national surveys can be used to estimate usual intakes.37,38 However, infancy and toddlerhood represent a period characterized by the introduction of new foods so the variety, amounts, and textures of foods and beverages fluctuate substantially. Therefore, the field would benefit from further exploration of whether statistical assumptions for usual intake hold for the B-24 population.
Human Milk Composition: Some surveillance datasets collect substantial information on human milk and formula feeding in the first year of life (e.g. WIC Infant and Toddler Feeding Practices Study-2)39 while other datasets collect considerably less detail (e.g. NHANES).36 Regardless, these databases share common limitations related to human milk composition and consumption data. Efforts are underway to better understand the biological composition of human milk and national food composition databases could be updated accordingly.18,40,41
Biomarkers: Biomarkers can be used to assess specific dietary components or used in the calibration and validation of new dietary assessment tools. In adults, urine biomarkers are commonly used to assess sodium intake.42 In the B-24 population, there is limited research on validation of biomarkers of dietary components commonly consumed by B-24 populations; for example, using carbon isotope ratios to distinguish between human milk and formula consumption.43
Data Processing: In recognition that current and future research will require large amounts of data, it is important to consider the role of data processing and advanced analytics. Artificial intelligence (AI) is part of national discussions on health and nutrition, and explicitly mentioned under Pillar 5 of the Biden-Harris Administration’s National Strategy on Hunger, Nutrition, and Health from the White House Conference on Food, Nutrition, Hunger, and Health,44 and in the 2020–2030 Strategic Plan for NIH Nutrition Research.16 As AI continues to expand, issues of algorithmic bias and social/structural impacts should be considered to ensure research progresses with a DEI lens.
Limitations for measuring other dimensions of diet
Device Limitations: Innovative device-based measurement tools could capture information on the context surrounding dietary intake. Devices for this age group are in early stages of development,21,45 but further research is needed to evaluate their safety, accuracy, and validity in diverse populations. Additionally, not all tools are publicly available.
Multidimensionality: Infant and toddler feeding practices are multidimensional. Understanding why caregivers make certain feeding decisions may require new evaluation metrics or more qualitative research that centers on the lived experiences of caregivers.
Dynamism: Infant and toddler diets change frequently and are rarely static during this time of rapid growth and development. Tools that can be easily adapted to age and developmental stage, and administered to collect repeated measures, are needed to address the dynamic nature of B-24 diets and related growth patterns.
Research Opportunities
The NCCOR B-24 Diet Assessment Work Group brought together diverse thought leaders from federal agencies (CDC, NIH, USDA) and academic research (three expert consultants), to identify opportunities to spur research in B-24 dietary assessment. In addition to the measurement research gaps listed above, the group identified five opportunities and themes:
Include and prioritize the B-24 population in research relevant to the DGA. A recent workshop and associated paper highlighted implementation of the 2020–2025 DGA, including opportunities and approaches to improve adoption of the DGA recommendations.46 However, the opportunities and approaches presented did not target B-24 caregivers,46 demonstrating the need for more implementation research for B-24 dietary recommendations. Similarly, recent reviews on the state of the science for technology tools for dietary assessment did not address the unique technological considerations for infants and toddlers,47 though new device-based measurements can add to the body of literature that informs B-24 dietary recommendations.
Develop a national research agenda to prioritize B-24 research topics. National research agendas have been successfully developed for nutrition topics like healthy food retail.48 A coordinated national plan for B-24 research could rank various measurement questions, and prioritize measurement research in the context of broader B-24 initiatives.
Collate a library of B-24 dietary assessment resources. Collating a library of survey questions, food frequency questionnaires, diet quality indices, and other tools for B-24 dietary assessment would serve as a resource to researchers. Currently, researchers can search the NCCOR Measures Registry using search filters for various ages of children including 2–5, 6–11, 12–18 years.13 Short instruments (e.g. screeners, survey questions) are available in the NCI’s Register of Validated Short Dietary Assessment Instruments.49 In the future, these registers can be expanded to include the B-24 population. Additionally, resources that provide rubrics for assessing strengths and weaknesses of tools, and guidance for selecting an appropriate tool based on the research question,33 can be similarly revised to include specific guidance for the B-24 population.
Forge diverse and interdisciplinary research collaborations. The nutrition and engineering disciplines have collaborated to engineer age-appropriate devices for studying infant feeding, such as instrumented bottles,45 and have creatively re-engineered existing tools such as image-based mobile food records to be suitable for use in infants.21 Future research at the intersection of nutrition, marketing, and behavioral sciences could conduct user-testing research on the new instruments to obtain design and usability feedback from B-24 caregivers. Nutrition, statistics, and other disciplines can collaborate to evaluate the validity and reliability of the new devices’ measurements of dietary intake across diverse populations and settings. Overall, characterizing multidimensional layers of infant and toddler dietary intakes will require continuing to break with historical research silos and collaborate across disciplines.
Recognize that everyone has a role to play. In addition to the interdisciplinary research collaborations mentioned above, it is also important to recognize the value of inter-agency and applied work. Funding agencies such as CDC, NIH, RWJF, and USDA can develop unique yet complementary funding proposals that support the research necessary to advance the knowledge base for future iterations of the B-24 DGA. Pediatric dietetic professionals can provide expertise across all layers of infant and toddler dietary intake, including not just “what” infants and toddlers should eat but also the how’s and why’s of feeding, to help overcome the logistic obstacles in measurement. End users (e.g. B-24 caregivers) can be involved in all phases of the research process to inform a more equitable approach grounded in lived experiences,50 especially as the field moves towards more multidimensional and dynamic contexts for dietary intake.
Conclusions
The development of dietary guidelines for the B-24 population emphasized recommendations based on the scientific evidence that every bite counts at every life stage and that food before one is not just for fun. However, there are many caveats for comprehensive assessment of the multidimensional and dynamic dietary intakes of infants and toddlers. Research gaps specific to B-24 dietary assessment methods were identified and summarized as: measurement error, proxy reporting, biased reporting, usual intake estimations, human milk composition, lack of biomarkers, device limitations, data processing developments, and the complexity of multidimensional and dynamic dietary patterns. The overlap in measurement gaps across several layers of multidimensionality (who, what, when, where, why, how) highlights an opportunity for innovative solutions in one area (e.g. who) to be transferable to other contexts (e.g. where). As B-24 research continues, five opportunities are: include and prioritize a diverse B-24 population in research relevant to the DGA; develop a national research agenda to prioritize and rank B-24 questions and research topics; collate a library of B-24 dietary assessment resources; forge diverse and interdisciplinary research collaborations; and recognize that everyone can help. Each stakeholder has a unique role to play in advancing B-24 dietary assessment. With widespread collaboration, it is possible to not only make every bite count, but also to count every bite.
Supplementary Material
Figure 1: The figure represents a case study focused on the Dietary Guidelines recommendation to exclusively feed infants human milk, or formula when human is unavailable, for the first six months of life. Historically, diet assessment research has focused on the ‘what’ and ‘when’ highlighted in purple, and has beet concentrated in the community, population, and individual levels of nutrition research. More research is needed across all layers and levels. Any research condu should be done through the lens of equity, diversity, and Inclusion. All of these questions can be answered using short-term methods (e.g. 24-hour recall), longf m methods (e.g. food frequency questionnaire), interviews, and novel methods (e.g. device-based assessments). The question under ‘what’ regarding mixed feed can also be answered using biomarkers.
{kind=link}
Acknowledgements
The authors thank three expert consultants - Lauren Au, Laurie Nommsen-Rivers, and Edward Sazonov - for their review of the supplementary table and for their contributions to identifying measurement gaps and research opportunities. We also acknowledge the contributions of all other members of the NCCOR B-24 Diet Assessment Work Group.
Footnotes
Financial Disclosure: none
Conflicts of Interest Disclosure: none
Written permission has been obtained from the individuals listed in the Acknowledgements section.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Heather C. Hamner, Health Scientist, Centers for Disease Control and Prevention, 4770 Buford Hwy NE, Mail-Stop S107-5, Atlanta, GA 30341-3717.
Kirsten A. Herrick, Program Director; National Cancer Institute; 9609 Medical Center Dr, Rockville, MD 20850.
Jennifer L. Lerman, Program Management Analyst; National Cancer Institute; 9609 Medical Center Dr, Rockville, MD 20850.
Jill Reedy, Branch Chief, Risk Factor Assessment Branch; National Cancer Institute; 9609 Medical Center Dr, Rockville, MD 20850.
Meghan Zimmer, At Time of Study: CRTA Research Fellow; National Cancer Institute; 9609 Medical Center Dr, Rockville, MD 20850; Current: Harvard University.
Kimberlea Gibbs, Nutrition Specialist; Eunice Kennedy Shriver National Institute of Child Health and Human Development; BG 6710 ROCKLEDGE DR. WING B RM 2415A, 6710B, ROCKLEDGE DRIVE, BETHESDA MD 20817.
Amanda Sharfman, Project Manager of Social Marketing and Communications; FHI360. 1825 Connecticut Avenue, NW |Washington, DC 20009..
Julie Obbagy, Branch Chief, Nutrition Evidence Systematic Review Branch, Center for Nutrition Policy and Promotion, Food and Nutrition Service, USDA, 1320 Braddock Place, Alexandria, Virginia 22314.
Kelley S. Scanlon, Director, Supplemental Nutrition and Safety Research and Analysis Division, Office of Policy Support, USDA Food and Nutrition Service, 1320 Braddock Place, Alexandria, Virginia 22314.
TusaRebecca E. Pannucci, Branch Chief, Nutrition and Economic Analysis Branch, Center for Nutrition Policy and Promotion, Food and Nutrition Service, USDA; 1320 Braddock Place, Alexandria, Virginia 22314.
References
- 1.US Departments of Agriculture and Health and Human Services. Dietary Guidelines for Americans, 2020–2025: Make Every Bite Count With the Dietary Guidelines. Dietary Guidelines for Americans. 2020;(9). Accessed June 9, 2022. DietaryGuidelines.gov [Google Scholar]
- 2.English LK, Obbagy JE, Wong YP, Butte NF, Dewey KG, Fox MK, Greer FR, Krebs NF, Scanlon KS, Stoody EE. Types and amounts of complementary foods and beverages consumed and growth, size, and body composition: a systematic review. Am J Clin Nutr. 2019;109(Suppl_7):956S–977S. doi: 10.1093/AJCN/NQY281 [DOI] [PubMed] [Google Scholar]
- 3.English LK, Obbagy JE, Wong YP, Butte NF, Dewey KG, Fox MK, Greer FR, Krebs NF, Scanlon KS, Stoody EE. Timing of introduction of complementary foods and beverages and growth, size, and body composition: a systematic review. Am J Clin Nutr. 2019;109(Suppl_7):935S–955S. doi: 10.1093/AJCN/NQY267 [DOI] [PubMed] [Google Scholar]
- 4.Dietary Guidelines Advisory Committee. Scientific Report of the 2020 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Agriculture and the Secretary of Health and Human Services.; 2020. [Google Scholar]
- 5.Rose CM, Birch LL, Savage JS. Dietary patterns in infancy are associated with child diet and weight outcomes at 6 years. Int J Obes (Lond). 2017;41(5):783–788. doi: 10.1038/IJO.2017.27 [DOI] [PubMed] [Google Scholar]
- 6.Golley RK, Smithers LG, Mittinty MN, Emmett P, Northstone K, Lynch JW. Diet quality of U.K. infants is associated with dietary, adiposity, cardiovascular, and cognitive outcomes measured at 7–8 years of age. J Nutr. 2013;143(10):1611–1617. doi: 10.3945/JN.112.170605 [DOI] [PubMed] [Google Scholar]
- 7.Grimm KA, Kim SA, Yaroch AL, Scanlon KS. Fruit and vegetable intake during infancy and early childhood. Pediatrics. 2014;134 Suppl 1(Suppl 1):S63–S69. doi: 10.1542/PEDS.2014-0646K [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Park S, Pan L, Sherry B, Li R. The association of sugar-sweetened beverage intake during infancy with sugar-sweetened beverage intake at 6 years of age. Pediatrics. 2014;134:S56–S62. doi: 10.1542/peds.2014-0646J [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Perrine CG, Galuska DA, Thompson FE, Scanlon KS. Breastfeeding Duration Is Associated With Child Diet at 6 Years. Pediatrics. 2014;134(Suppl 1):S50. doi: 10.1542/PEDS.2014-0646I [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dewey KG, Güngör D, Donovan SM, Madan EM, Venkatramanan S, Davis TA, Kleinman RE, Taveras EM, Bailey RL, Novotny R, et al. Breastfeeding and risk of overweight in childhood and beyond: a systematic review with emphasis on sibling-pair and intervention studies. Am J Clin Nutr. 2021;114(5):1774–1790. doi: 10.1093/AJCN/NQAB206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Thompson HR, Borger C, Paolicelli C, Whaley SE, Reat A, Ritchie L. The Relationship between Breastfeeding and Initial Vegetable Introduction with Vegetable Consumption in a National Cohort of Children Ages 1–5 Years from Low-Income Households. Nutrients. 2022;14(9). doi: 10.3390/NU14091740/S1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Belz K. Parents face a bewildering range of food advice. These tips can help. The Washington Post. April 10, 2022. [Google Scholar]
- 13.National Collaborative on Childhood Obesity Research. NCCOR Measures Registry. Accessed June 10, 2022. https://www.nccor.org/nccor-tools/measures/
- 14.McKinnon RA, Reedy J, Berrigan D, Krebs-Smith SM. The National Collaborative on Childhood Obesity Research Catalogue of Surveillance Systems and Measures Registry: New Tools to Spur Innovation and Increase Productivity in Childhood Obesity Research. Am J Prev Med. 2012;42(4):433–435. doi: 10.1016/J.AMEPRE.2012.01.004 [DOI] [PubMed] [Google Scholar]
- 15.National Collaborative on Childhood Obesity Research. Accessed June 10, 2022. https://www.nccor.org/ [Google Scholar]
- 16.National Institutes of Health Nutrition Research Task Force. 2020–2030 Strategic Plan for NIH Nutrition Research.; 2020. Accessed June 6, 2022. https://dpcpsi.nih.gov/onr/strategic-plan
- 17.NOT-CA-21–108: Notice of Special Interest (NOSI): Dietary, Physical Activity, Sedentary Behavior and Sleep Assessment Methodologies Among Infants and Young Children (Birth to 5 years) through Adults. Accessed June 10, 2022. https://grants.nih.gov/grants/guide/notice-files/NOT-CA-21-108.html [Google Scholar]
- 18.Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). Human Milk as a Biological System (R01 Clinical Trial Optional). Accessed June 9, 2022. https://grants.nih.gov/grants/guide/rfa-files/RFA-HD-22-020.html
- 19.Reedy J, Subar AF, George SM, Krebs-Smith SM. Extending Methods in Dietary Patterns Research. Nutrients. 2018;10(5). doi: 10.3390/NU10050571 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Pérez-Escamilla R, Segura-Pérez S, Lott M. Feeding Guidelines for Infants and Young Toddlers: A Responsive Parenting Approach. Healthy Eating Research. Published February 2017. Accessed June 9, 2022. https://healthyeatingresearch.org/wp-content/uploads/2017/02/her_feeding_guidelines_report_021416-1.pdf [Google Scholar]
- 21.Fialkowski MK, Kai J, Young C, Langfelder G, Ng-Osorio J, Shao Z, Zhu F, Kerr DA, Boushey CJ. An Active Image-Based Mobile Food Record Is Feasible for Capturing Eating Occasions among Infants Ages 3–12 Months Old in Hawai’i. Nutrients. 2022;14(5). doi: 10.3390/NU14051075 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kay MC, Duffy EW, Harnack LJ, Anater AS, Hampton JC, Eldridge AL, Story M. Development and Application of a Total Diet Quality Index for Toddlers. Nutrients 2021, Vol 13, Page 1943. 2021;13(6):1943. doi: 10.3390/NU13061943 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Development of the Healthy Eating Index-Toddlers-2020. J Acad Nutr Diet. [DOI] [PubMed] [Google Scholar]
- 24.Evaluation of the Healthy Eating Index-Toddlers-2020. J Acad Nutr Diet. [DOI] [PubMed] [Google Scholar]
- 25.National Cancer Institute. Automated Self-Administered 24-Hour (ASA24®) Dietary Assessment Tool. Accessed June 6, 2022. https://epi.grants.cancer.gov/asa24
- 26.Shams-White MM, O’Connor LE, O’Connor SG, Herrick KA. Development of the Sleep Module for the Automated Self-Administered 24-Hour (ASA24) Dietary Assessment Tool: New Research Opportunities. J Acad Nutr Diet. 2022;122(11):2017–2022. doi: 10.1016/J.JAND.2022.06.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Doulah A, Ghosh T, Hossain D, Imtiaz MH, Sazonov E. “Automatic Ingestion Monitor Version 2” – A Novel Wearable Device for Automatic Food Intake Detection and Passive Capture of Food Images. IEEE J Biomed Health Inform. 2021;25(2):568. doi: 10.1109/JBHI.2020.2995473 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Raju VB, Sazonov E. FOODCAM: A Novel Structured Light-Stereo Imaging System for Food Portion Size Estimation. Sensors 2022, Vol 22, Page 3300. 2022;22(9):3300. doi: 10.3390/S22093300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Raju VB, Sazonov E. A Systematic Review of Sensor-Based Methodologies for Food Portion Size Estimation. IEEE Sens J. 2021;21(11):12882–12899. doi: 10.1109/JSEN.2020.3041023 [DOI] [Google Scholar]
- 30.Landry MJ, Ruiz LD, Gibbs K, Radtke MD, Lerman J, Vargas AJ. Perspective: Early-Life Nutrition Research Supported by the US National Institutes of Health from 2018 to 2020. Advances in Nutrition. 2022;13(5):1395–1401. doi: 10.1093/ADVANCES/NMAC044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Subar AF, Freedman LS, Tooze JA, Kirkpatrick SI, Boushey C, Neuhouser ML, Thompson FE, Potischman N, Guenther PM, Tarasuk V, et al. Addressing Current Criticism Regarding the Value of Self-Report Dietary Data. J Nutr. 2015;145(12):2639–2645. doi: 10.3945/JN.115.219634 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kirkpatrick SI, Guenther PM, Subar AF, Krebs-Smith SM, Herrick KA, Freedman LS, Dodd KW. Using Short-Term Dietary Intake Data to Address Research Questions Related to Usual Dietary Intake among Populations and Subpopulations: Assumptions, Statistical Techniques, and Considerations. J Acad Nutr Diet. 2022;122(7):1246–1262. doi: 10.1016/J.JAND.2022.03.010 [DOI] [PubMed] [Google Scholar]
- 33.National Cancer Institute. Dietary Assessment Primer. Accessed June 7, 2022. https://dietassessmentprimer.cancer.gov/ [Google Scholar]
- 34.Zhang S, Midthune D, Guenther PM, Krebs-Smith SM, Kipnis, Dodd KW, Buckman DW, Tooze JA, Freedman L, Carroll RJ. A new multivariate measurement error model with zero-inflated dietary data, and its application to dietary assessment. Annals of Applied Statistics. 2011;5(2 B):1456–1487. doi: 10.1214/10-AOAS446 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Freedman LS, Schatzkin A, Midthune D, Kipnis V. Dealing With Dietary Measurement Error in Nutritional Cohort Studies. JNCI Journal of the National Cancer Institute. 2011;103(14):1086. doi: 10.1093/JNCI/DJR189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.NHANES Questionnaires, Datasets, and Related Documentation. Accessed January 18, 2023. https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/default.aspx?BeginYear=2017 [Google Scholar]
- 37.Tooze JA, Midthune D, Dodd KW, Freedman LS, Krebs-Smith SM, Subar AF, Guenther PM, Carroll RJ, Kipnis V. A new method for estimating the usual intake of episodically-consumed foods with application to their distribution. J Am Diet Assoc. 2006;106(10):1575. doi: 10.1016/J.JADA.2006.07.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.National Cancer Institute. Usual Dietary Intakes: The NCI Method. Accessed June 9, 2022. https://epi.grants.cancer.gov/diet/usualintakes/method.html [Google Scholar]
- 39.WIC Infant and Toddler Feeding Practices Study-2 (WIC ITFPS-2): Prenatal, Infant Year, Second Year, Third Year, and Fourth Year Datasets | Ag Data Commons. Accessed November 25, 2022. https://data.nal.usda.gov/dataset/wic-infant-and-toddler-feeding-practices-study-2-wic-itfps-2-prenatal-infant-year-second-year-third-year-and-fourth-year-datasets-0 [Google Scholar]
- 40.Christian P, Smith ER, Lee SE, Vargas AJ, Bremer AA, Raiten DJ. The need to study human milk as a biological system. Am J Clin Nutr. 2021;113(5):1063. doi: 10.1093/AJCN/NQAB075 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Breastmilk Ecology: Genesis of Infant Nutrition (BEGIN) Project. Accessed June 7, 2022. https://www.nichd.nih.gov/research/supported/begin#:~:text=The BEGIN Project%2C an effort,for both parent and infant [Google Scholar]
- 42.Cogswell ME, Maalouf J, Elliott P, Loria CM, Patel S, Bowman BA. Use of Urine Biomarkers to Assess Sodium Intake: Challenges and Opportunities. Annu Rev Nutr. 2015;35(1):349. doi: 10.1146/ANNUREV-NUTR-071714-034322 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.O’Brien DM. Stable Isotope Ratios as Biomarkers of Diet for Health Research. Annu Rev Nutr. 2015;35(1):565. doi: 10.1146/ANNUREV-NUTR-071714-034511 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Biden-Harris Administration National Strategy on Hunger, Nutrition, and Health. Published September 2022. Accessed January 18, 2023. https://www.whitehouse.gov/wp-content/uploads/2022/09/White-House-National-Strategy-on-Hunger-Nutrition-and-Health-FINAL.pdf [Google Scholar]
- 45.Sazonov E, Imtiaz MH, Bahorski J, Schneider CR, Chandler-Laney P. Design and Testing of an Instrumented Infant Feeding Bottle. Proceedings of IEEE Sensors. 2018;2018-October. doi: 10.1109/ICSENS.2018.8589888 [DOI] [Google Scholar]
- 46.Sanders LM, Allen JC, Blankenship J, Decker EA, Christ-Erwin M, Hentges EJ, Jones JM, Mohamedshah FY, Ohlhorst SD, Ruff J, et al. Implementing the 2020–2025 Dietary Guidelines for Americans: Recommendations for a path forward. J Food Sci. 2021;86(12):5087–5099. doi: 10.1111/1750-3841.15969 [DOI] [PubMed] [Google Scholar]
- 47.Das SK, Miki AJ, Blanchard CM, Sazonov E, Gilhooly CH, Dey S, Wolk CB, Khoo CSH, Hill JO, Shook RP. Perspective: Opportunities and Challenges of Technology Tools in Dietary and Activity Assessment: Bridging Stakeholder Viewpoints. Advances in Nutrition. 2022;13(1):1–15. doi: 10.1093/ADVANCES/NMAB103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Hecht AA, Lott MM, Arm K, Story MT, Snyder E, Wootan MG, Moran AJ. Developing a National Research Agenda to Support Healthy Food Retail. Int J Environ Res Public Health. 2020;17(21):1–17. doi: 10.3390/IJERPH17218141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.National Cancer Institute. Search the Register of Validated Short Dietary Assessment Instruments. Accessed June 10, 2022. https://epi.grants.cancer.gov/diet/shortreg/register.php [Google Scholar]
- 50.Consumer Engagement and Involvement | Cochrane. Accessed November 25, 2022. https://www.cochrane.org/about-us/consumer-engagement-and-involvement [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure 1: The figure represents a case study focused on the Dietary Guidelines recommendation to exclusively feed infants human milk, or formula when human is unavailable, for the first six months of life. Historically, diet assessment research has focused on the ‘what’ and ‘when’ highlighted in purple, and has beet concentrated in the community, population, and individual levels of nutrition research. More research is needed across all layers and levels. Any research condu should be done through the lens of equity, diversity, and Inclusion. All of these questions can be answered using short-term methods (e.g. 24-hour recall), longf m methods (e.g. food frequency questionnaire), interviews, and novel methods (e.g. device-based assessments). The question under ‘what’ regarding mixed feed can also be answered using biomarkers.