

Abstract
Objectives
The aim of this study was to describe the characteristics of cases of feline dystocia presenting to a university emergency service.
Methods
The medical records of queens presenting for dystocia between January 2009 and September 2020 were reviewed. Data collected included queen signalment, presenting complaints, treatments, and maternal and neonatal outcomes. Clinicopathologic data included serum ionized calcium concentration, blood glucose level, packed cell volume and total solids. Owing to the small sample size, descriptive statistics were used and data presented as median (range).
Results
Thirty-five cases were reviewed. Dystocia was attributed to maternal factors in 69% (n = 24) and fetal factors in 31% (n = 11). Venous blood gas data from 19 queens in stage 2 labor revealed that no queens were hypocalcemic (median ionized calcium 5.4 mg/dl [range 4.9–5.8]) or hypoglycemic (median glucose 143 mg/dl [range 78–183]). Medical management was attempted in 21/35 queens. Successful medical management was achieved in 29% (n = 6/21). Thirteen queens underwent surgical management, six of these after failing medical management. Seven queens received no treatment. Fifteen queens were discharged and one queen was euthanized while still in labor. The remaining 19 queens delivered all fetuses with medical (n = 6) or surgical management (n = 13). Maternal survival was 94% (n = 33/35). A total of 136 kittens were born to all queens, with 58% (n = 79/136) born prior to initiation of treatment, 16% (n = 22/136) after medical management and 26% (n = 35/136) after surgical management. Overall neonatal survival to discharge was 66% (n = 90/136).
Conclusions and relevance
Feline dystocia is an emergent condition that can result in up to 34% neonatal mortality for kittens delivered via both medical and surgical means. Hypoglycemia and hypocalcemia were not precipitating causes of feline dystocia in this population.
Keywords: Dystocia, surgical management, serum ionized calcium, neonatal survival, blood glucose, medical management
Introduction
Feline gestation is approximately 65 days in length and culminates in three stages of labor.1–3 Normal stage 1 labor is marked by progressive uterine contractions and cervical dilation. Clinically, the queen may become tachypneic, restless or vocal, though this stage is frequently difficult to detect. 4 Stage 2 labor is characterized by active abdominal and uterine contractions, culminating in fetal delivery. This is followed by stage 3, during which the fetus’ associated placenta is expelled. 4
In queens, total duration of labor is typically short, and all neonates are often born within 6 h of the first kitten being delivered. 2 The interval between delivery times is variable, but approximately 95% of kittens are born within 100 mins of each other. 1 Additionally, there have been anecdotal reports of a phenomenon known as interrupted labor, during which the queen will pause active stage 2 labor then resume fetal expulsion, with no obvious detriment to either the dam or the remaining fetuses. 5
This is in contrast to dystocia, in which the normal progression of labor is disrupted and the health of the dam, its fetus(es) or both may be in jeopardy. 6 Causes of dystocia can be grouped according to maternal or fetal factors. 4 Dystocia represents a medical and/or surgical emergency and must be dealt with in a timely manner to ensure a favorable outcome. Despite this, there is a paucity of studies focusing on feline dystocia, in particular the biochemical data, treatment courses, neonatal survival to discharge and outcomes of dystocic queens in an emergent setting. The purpose of this retrospective study was to describe the population, including causes, clinicopathologic data, and fetal and maternal outcomes of queens presenting to a university emergency service for dystocia.
Materials and methods
Electronic medical records from January 2009 to September 2020 were searched for queens presenting to a university veterinary teaching hospital with the chief complaint terms of ‘dystocia’, ‘labor’, ‘labor complications’, ‘labor difficulties’, ‘difficulty birthing’, ‘pregnancy’, ‘abortion’, ‘c-section’ or ‘cesarean section’. Queens were included if they were described by the attending clinician to be in stage 2 labor and experiencing dystocia at the time of presentation. Stage 2 labor was defined as a queen with fetuses in utero on presentation and at least one of the following criteria: abdominal contractions; delivery of at least one neonate; a fetus or fetal membranes palpable in the vagina or visible in the vulva; or evidence of rupture of an amniotic sac (ie, reported history of fluid discharge from vulva and/or visualization of fetus without associated amniotic membrane). The diagnosis of dystocia was based on documentation of at least one of the following criteria: evidence of fetal obstruction; strong, persistent abdominal contractions with no neonate within 30 mins; >4 h between fetal expulsions; fetal heart rates (HRs) of <160 beats per min (bpm); lochia or fetal fluids noted, and >2 h without fetal expulsion; or evidence of maternal systemic illness. Queens were excluded if they were <55 days’ gestation, had aborted premature fetuses, were determined to be in normal stage 2 labor by the attending clinician and/or had delivered all fetuses prior to the time of presentation.
Data extracted from the records included age and breed of queen, purposeful vs accidental breeding, parity status and estimated litter size. Clinical data collected included presenting clinical signs, blood glucose level, serum ionized calcium (iCa) concentration, packed cell volume (PCV) and total solids (TS).
Based on the medical records, causes of dystocia were retrospectively categorized as either maternal or fetal, as previously described. 4 Maternal causes were further classified as uterine inertia, maternal systemic disease, previous pelvic fractures, obstructive cervical or vaginal masses, cervical fibrosis or presence of a vaginal septum. Uterine inertia was defined as a failure to deliver neonates despite the queen having an open birth canal and apparently normal fetus(es), with or without intermittent or weak abdominal contractions. Tocodynamometry was not performed and thus categorization of primary vs secondary inertia could not be determined. Fetal causes were further classified into malformation, fetal oversize, fetal death or cervical obstruction by the fetus in either normal presentation or malpresentation. Cause of fetal cervical obstruction was documented when known. Fetuses that were not exiting the cervical canal with both presenting legs extended in either anterior dorsal or posterior dorsal positions were considered to be malpresenting. 7 Fetal oversize was diagnosed based on evidence of fetal–pelvic disproportion on radiographs. Fetal distress was defined as fetal HRs <160 bpm using point-of-care ultrasound. In cases where evidence of both maternal and fetal factors were present, retrospective categorization of the cause of dystocia was based on the predominant factors noted in the medical record.
Additional data collected included the following: number of queens that underwent medical management with either digital manipulation of obstructed fetuses; route and dose of oxytocin (20 U/ml) administration; route and dose of 10% calcium gluconate supplementation, or a combination of those treatments; number of queens that underwent surgical management after attempted medical management; number of queens that underwent surgical management without prior medical management; number of queens that received no treatment; success of medical management, defined as no response (no fetuses delivered), partial response (neonate delivered, fetuses remaining in utero) or full response (all fetuses delivered); type of surgical management performed (cesarean section with or without ovariohysterectomy); and timing from presentation to anesthetic induction for surgically managed queens. Anesthetic protocols were not evaluated. Outcome data included the number of stillborns and live neonates delivered via medical management, surgical management or without treatment; neonatal survival to discharge; maternal survival to discharge; and the number of fetuses remaining in utero at the time of discharge. Descriptive statistics were performed and data presented as median (range) for continuous variables and frequency counts for categorical variables.
Results
A total of 16,039 queens were presented to the emergency room during the study period, and 52 records were identified for this study with presenting complaints included in the search terms. Of these, 13 were excluded because they were considered by the attending clinician to either be post-parturient (n = 5), experiencing normal stage 2 labor (n = 4), aborting premature fetuses (n = 2), still in gestation (n = 1) or in normal stage 1 labor (n = 1). Four were excluded because they had undergone a scheduled elective cesarean section.
Thirty-five records remained for data collection and analysis. The median age of the included queens was 2 years (range 0.8–4.5). Represented breeds were domestic shorthair (n = 19), Persian (n = 5), domestic longhair (n = 3), domestic mediumhair (n = 2) and one each of the following: Abyssinian, Bengal, Munchkin, Ocicat, Scottish Fold and Tonkinese. Ten queens were primiparous, eight were multiparous and the parity status of 17 queens was unknown. Ten queens were purposefully bred; the remaining 25 queens were bred accidentally. The most common presenting clinical signs included visible abdominal contractions (n = 18), kitten visible in the vulva (n = 11), >4 h between kittens (n = 11), hemorrhage (n = 8) and restlessness (n = 7). Twenty-five queens had more than one presenting clinical sign. There was a median of three kittens (range 1–9) per litter (n = 28 litters). The estimated median time in stage 2 labor for 31 queens was 7 h (range 1–84).
Dystocia was attributed to maternal factors in 24 queens (69%). Of these 24, 21 queens had uterine inertia. A single case of uterine prolapse and two cases with systemic disease comprised three other queens. One of the queens with maternal systemic disease was a bradycardic (HR 140 bpm), neurologic domestic stray whose history was unknown and, owing to staff safety considerations, a vaginal examination was not performed but fetal membranes were visible in her vulva. The other queen with maternal systemic disease was diagnosed with an acute kidney injury (blood urea nitrogen 63 mg/dl [reference interval {RI} 10–25], creatinine 4.1 mg/dl [RI 0.7–1.4]) and anemia (PCV 20% [RI 25–45%], TS 6.2 g/dl). Dystocia was attributed to fetal factors in 11 (31%) queens, including cervical obstruction with a fetus (n = 8), fetal death (n = 2) and oversized fetus (n = 1). Cervical obstruction was caused by a fetal malpresentation in five queens. In two additional queens, the cause of obstruction was documented as secondary to the fetus exiting in the normal dorsal posterior fetal position and in one queen the cause was unknown. No other maternal or fetal factors were identified as causes of dystocia in this population.
Venous blood gas data were available for 19 queens. Median iCa in these queens was 5.4 mg/dl (range 4.9–5.8 [RI 3.4–5.3]); median blood glucose was 143 mg/dl (range 78–183 [RI 66–117]). No cat was hypocalcemic; 11 queens were hypercalcemic and eight queens were normocalcemic. No cat was hypoglycemic; 13 were hyperglycemic and six were normoglycemic. PCV/TS data were available for 14/35 queens. Median PCV was 34.3% (range 20–42 [RI 25–45]) and median TS was 7.5 g/dl (range 6.2–10.1). PCV was on the low end of normal or below the RI in 70% of these 14 queens. The effect of PCV/TS, serum iCa and serum glucose levels on the success of medical management could not be evaluated owing to the small sample size.
Medical management was attempted in 21/35 queens, 14 of which were domestic breeds and seven were purebred. Medical management consisted of digital manipulation of obstructed fetuses alone (n = 8), oxytocin alone (n = 8), digital manipulation and oxytocin administration (n = 3), oxytocin and calcium gluconate (n = 1), or a combination of the three (n = 1). Total oxytocin dose per cat was known in 10 queens with a median intramuscular dose of 0.75 U/cat (range 0.5–2.5). All oxytocin was administered undiluted using a U-100 insulin syringe. The two queens administered 10% calcium gluconate received a median dose of 0.9 ml/cat (range 0.8–1); one was given intravenously and the other subcutaneously. Both queens receiving calcium gluconate were normocalcemic at 5.1 mg/dl. Calcium supplementation resulted in ineffective abdominal contractions in one queen, while the other did not have a documented response. Seven queens failed to respond to medical management, seven queens had a partial response, six queens had complete response and one was discharged before response could be documented. Overall, complete success of medical management was achieved in 29% of medically managed queens. Six queens underwent surgery after failing medical management; two of these were domestic breeds and four were purebred. Seven queens (three domestic breeds and four purebreds) were taken directly to surgery owing to fetal distress (n = 5), uterine prolapse (n = 1) and oversized fetus (n = 1). Of the 13 queens (six with and seven without prior medical management) that received surgical management, 10 had cesarean sections performed without ovariohysterectomy and three were ovariohysterectomized after cesarean section. The timing from presentation to induction of general anesthesia was known in 11/13 surgically managed queens with a median time of 2 h (range 1.5–15.5). Seven queens received no treatment, all of which were accidentally bred domestic breeds. Two of these queens received no treatment due to owner financial concerns; the other five queens did not have a reason listed for lack of treatment.
Fifteen queens were discharged and one queen euthanized while still in labor. Seven of the queens that were still in labor at the time of discharge received no treatment and nine received medical management. Of the nine that received medical management prior to discharge while still in labor, four had a partial response to medical management, four had no response to medical management and one was discharged before response could be documented. Additional treatment was declined in four of these queens (two with a partial response and two with no response to medical management) owing to the owners’ financial considerations. In one queen that partially responded to medical management, interrupted labor was listed as a differential diagnosis and therefore a justification for discharge without further treatment. The reason for lack of additional treatments in the other four queens (one with a partial response, two with no response and one without a documented response) was not documented. In total, these 15 queens were estimated to have 27 fetuses remaining in utero at the time of discharge. The remaining 19 queens delivered all fetuses with medical (n = 6) or surgical management (n = 13); all but one of these queens survived to discharge. Maternal survival was 94% (n = 33/35). Figure 1 shows the type of management, response to treatment and outcomes for all 35 dystocic queens.
Figure 1.
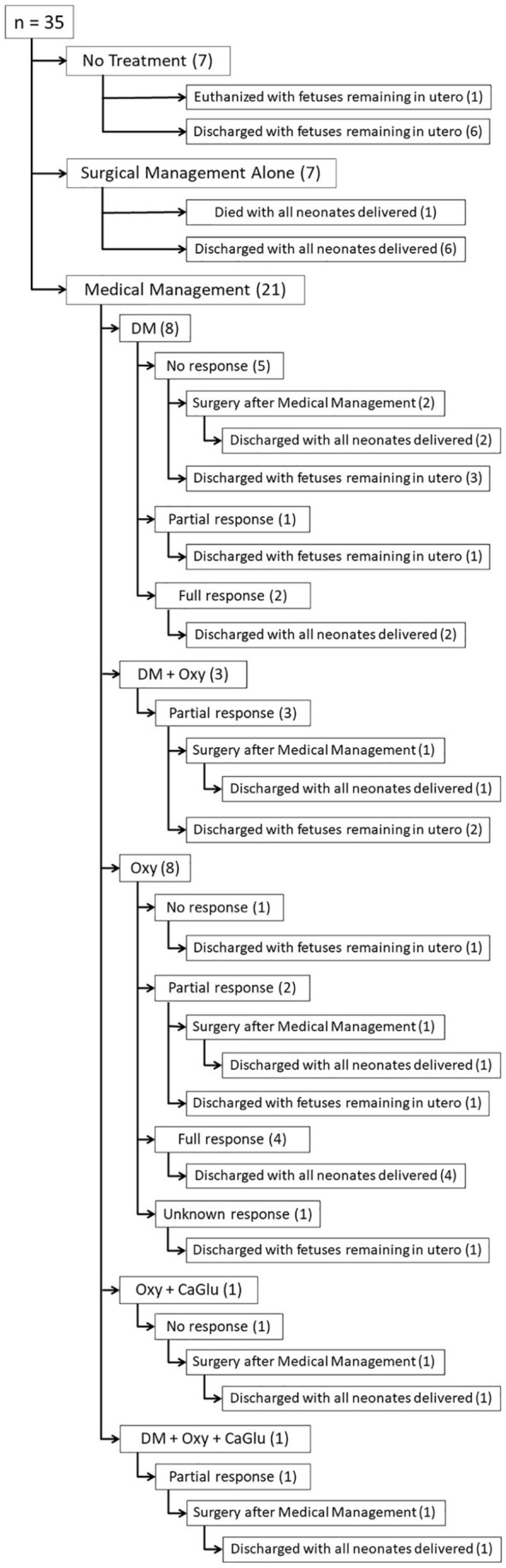
Flowchart of management types, response to treatment and outcomes for the 35 queens presenting in dystocia. Seven queens received no treatment. Seven queens were taken directly to surgery. Twenty-one queens received medical management, consisting of digital manipulation (DM), digital manipulation and oxytocin (20 U/ml) administration (DM + Oxy), oxytocin administration alone (Oxy), oxytocin and 10% calcium gluconate administration (Oxy + CaGlu), or a combination of digital manipulation and oxytocin and calcium gluconate administration (DM + Oxy + CaGlu). Medically managed queens displayed either no response, a partial response or a complete response. One medically managed queen was discharged before the response could be documented and thus her response was unknown. Six queens received surgery after displaying either no or partial response to medical management. One queen died after surgery and one was euthanized prior to treatment. All remaining queens were discharged with either all neonates delivered or fetuses remaining in utero. Numerals in parenthesis represent the number of queens in each category
Both queens that did not survive to discharge were diagnosed with dystocia secondary to maternal systemic disease. The first was the neurologic stray that was euthanized without further treatment. The second was the azotemic, anemic domestic breed queen that presented 10 h after delivering six healthy neonates. A single fetus with a heart rate of 155 bpm was noted on fetal ultrasound and the queen underwent caesarean section. The fetus was delivered stillborn; the queen underwent cardiopulmonary arrest during recovery. No necropsy was performed and the underlying diagnosis for her kidney injury and anemia was unknown.
One hundred and thirty-six kittens were born to all queens, with 58% (n = 79) born prior to the initiation of treatment, 16% (n = 22) that required medical management and 26% (n = 35) that required surgical management. Table 1 shows the number of kittens that were stillborn, live-born but died prior to discharge and live-born and survived to discharge, as well as the percentage survival to discharge for each management type.
Table 1.
Total number and percentage of neonates delivered per treatment group
| Stillborn (n) | Live born and died (n) | Live born and survived (n) | Total (n) | Survival to discharge (%) | |
|---|---|---|---|---|---|
| Prior to treatment | 17 | 4 | 58 | 79 | 73 |
| Medical management | 7 | 1 | 14 | 22 | 64 |
| Surgical management | 12 | 5 | 18 | 35 | 51 |
| Overall | 36 | 10 | 90 | 136 | 66 |
Prior to treatment = neonates born at home or in hospital prior to initiation of medical or surgical treatment; medical management = neonates delivered with medical management (digital manipulation, oxytocin and/or calcium gluconate administration); surgical management = neonates delivered via cesarean section
Discussion
To our knowledge, no previous study has evaluated serum iCa and blood glucose concentrations in dystocic queens. Calcium is required for myometrial contraction and thus calcium deficiency may predispose an animal to uterine inertia.4,8,9 However, similar to dystocic bitches, the importance of serum iCa and blood glucose levels on the myometrial strength of contraction and the etiology of dystocia and uterine inertia in dystocic queens remains unclear, as no queen in this study was hypocalcemic or hypoglycemic.8–10 Two normocalcemic queens (both iCa 5.1 mg/dl) did receive calcium gluconate supplementation as part of their medical management. Both queens ultimately underwent cesarean section. Approximately 58% of queens in this study had an iCa level above the RI, though the highest was only moderately elevated at 5.8 mg/dl. Hypercalcemia was therefore unlikely to have resulted in dystocia due to pathologic disruption of the myometrium.
PCV, when documented, was on the low end of normal or below the RI in 70% of dystocic queens. This is consistent with pregnancy-associated anemia documented in other species and is likely due to increased circulating plasma volume. 10
Stillbirth rates in queens experiencing normal parturition range from 5% to 11.8%.1–3,11 In dystocic queens, previously reported stillbirth rates for surgically managed queens was drastically higher at 58% overall. 12 Stillbirths accounted for 26% of all births in this study. However, when broken down into management categories, more stillborns were delivered medically (32%) and surgically (34%) than those delivered without assistance (22%). Given that fetal death was documented to be responsible for dystocia in only 6% of the queens in this study, these higher percentages of stillbirths suggest that dystocia is associated with significant risk to the fetus. To our knowledge, this is the first study to report neonatal survival to discharge percentages. Sixty-six percent of all neonates delivered by the queens in this study survived to discharge. Those delivered surgically had lower survival percentages (51%) and higher stillborn percentages than neonates delivered with medical management (64%) or unassisted (73%). The low survival percentage of surgically delivered neonates may reflect the fact that many were taken to surgery for evidence of fetal distress or after medical intervention was performed, thus selecting for a population of neonates that were weakened and therefore less likely to survive once delivered. However, the possibility that delays in surgical intervention contributed to lower survival rates is also considered, especially considering the prolonged time course from presentation to induction of anesthesia in queens undergoing surgical management in this study. Lastly, 15 medically managed queens were discharged with fetuses remaining in utero, so this categories’ stillbirth percentage may be falsely low, as fetuses remaining in utero were not categorized as dead or alive in this data set.
In this study, approximately 70% of all queens presenting for dystocia were domestic breeds, followed by Persian queens (14%). Robbins and Mullen similarly found that domestic breeds accounted for 70% of dystocic queens. 12 While risk analysis comparisons between domestic breeds and purebreds in this study were not performed, in other studies purebred queens had higher risks of dystocia than domestic breeds.13,14 It is possible that the skew towards domestic breeds in this study and the study by Robbins and Mullen is owing to the fact that purposefully bred queens are more likely to be followed closely by a primary veterinarian or theriogenologist, and therefore be less likely to present to an emergency clinic. 12
Our study confirmed previous findings that maternal factors are the most common causes of dystocia in queens (69% vs previously reported 67%).4,12,13,15 Regardless of the cause of dystocia, however, overall medical management success in this population was low at 29%, which is similar to previously reported medical management success rates of 31%. 13 Importantly, aside from two queens in the study by Ekstrand and Linde-Forsberg, all queens in previous studies that failed medical management received surgery. 15 In contrast, just over 40% of queens in this study were discharged while still in labor, representing seven queens that were discharged without treatment and eight queens with no response/partial response to medical management. All of the queens that received no treatment were accidentally bred domestic breeds. Domestic breeds also had medical management alone performed more often than purebreds. Given that the causes of dystocia were similar across breed groups, this difference in treatments most likely represents owner financial considerations as opposed to true factors among breeds, such as responsiveness to medical management. Additionally, one queen was discharged after partial success with medical management with a differential diagnosis of interrupted labor. Interrupted labor has been reported to occur in queens and may account for the few instances of prolonged delivery interval times of up to 48 h in queens experiencing normal parturition.2,5 However, if interrupted labor does happen, it should be regarded as a rare exception, as Musters et al showed that 63% of kittens born with delivery interval times >6 h were stillborn. 1 Thus, queens presenting with this prolonged time course should raise the suspicion for dystocia and prompt intervention.
Surgical management was performed in 37% of queens in this study. This percentage is low, compared to other studies (75% and 79.4%).13,15 This discrepancy is a logical consequence of the high numbers of queens discharged in active labor discussed above. Over 60% of surgically managed queens were purebred. Cesarean section without ovariohysterectomy was performed in the 77% of surgically managed queens, likely representing the owners’ desires for future breeding events.
Overall, maternal survival to discharge was 94%. The two queens that died prior to discharge both had dystocia due to maternal systemic disease. Two other studies have documented maternal survival to discharge for feline dystocia and found a similar maternal survival percentages of 96% and 98%, respectively.12,14
There were several limitations of this study related to its retrospective nature. Categorization of dystocia type was rarely documented in the medical records. Causes of dystocia were therefore concluded based on data included in the medical record, possibly resulting in inaccuracies within each category. This may be most apparent when evidence of both maternal and fetal factors was present, and the authors acknowledge the possibility that a combination of factors likely contributed to the dystocia in these cases. Additionally, because stringent inclusion criteria were applied in order to accurately identify dystocia, it is possible that some dystocic queens were excluded from the study population. These exclusions may have specifically affected those that may have been in stage 1 labor or experiencing uterine inertia but the queen and her fetuses were clinically normal on presentation. Another limitation of this study was the small sample size. Lastly, this study was limited by an inability to obtain follow-up data for these dystocic queens. Follow-up was attempted via telephone and email to both the queens’ owners and primary veterinarians without success. The absence of these data are particularly relevant given the high number of patients discharged with fetuses remaining in utero, as follow-up data would help determine the risk of such a practice to the queen and her fetuses.
Conclusions
Feline dystocia is an emergent condition that can result in up to 34% neonatal mortality for kittens in this study delivered via both medical and surgical means. Hypoglycemia and hypocalcemia were not precipitating causes of feline dystocia in this population.
Acknowledgments
The authors would like to acknowledge L Ari Jutkowitz, DVM, DACVECC, Erin Binagia, DVM, MS, DACVECC and Annette O’Connor, BVSC, MVSC, DVSC, FANZCVSC for their contributions to this paper.
Footnotes
Accepted: 19 May 2021
Author note: The abstract of this paper was presented, in part, at the IVECCS 2020 conference.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval: This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not specifically required for publication in JFMS.
Informed consent: Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.
ORCID iD: H Grady Bailin  https://orcid.org/0000-0003-1048-0493
https://orcid.org/0000-0003-1048-0493
Nyssa A Levy
https://orcid.org/0000-0003-4101-3767
References
- 1. Musters J, de Gier J, Kooistra HS, et al. Questionnaire-based survey of parturition in the queen. Theriogenology 2011; 75: 1596–1601. [DOI] [PubMed] [Google Scholar]
- 2. Sparkes AH, Rogers K, Henley WE, et al. A questionnaire-based study of gestation, parturition and neonatal mortality in pedigree breeding cats in the UK. J Feline Med Surg 2006; 8: 145–157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Romagnoli S, Bensaia C, Ferré-Dolcet L, et al. Fertility parameters and reproductive management of Norwegian Forest Cats, Maine Coon, Persian and Bengal cats raised in Italy: a questionnaire-based study. J Feline Med Surg 2019; 21: 1188–1197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Jutkowitz LA. Reproductive emergencies. Vet Clin North Am Small Anim Pract 2005; 35: 397–420. [DOI] [PubMed] [Google Scholar]
- 5. Little SE. The cat: clinical medicine and management. St Louis, MO: Elsevier Saunders, 2012, p xxv. [Google Scholar]
- 6. Pretzer SD. Medical management of canine and feline dystocia. Theriogenology 2008; 70: 332–336. [DOI] [PubMed] [Google Scholar]
- 7. Smith FO. Guide to emergency interception during parturition in the dog and cat. Vet Clin North Am Small Anim Pract 2012; 42: 489–499. [DOI] [PubMed] [Google Scholar]
- 8. Hollinshead FK, Hanlon DW, Gilbert RO, et al. Calcium, parathyroid hormone, oxytocin and pH profiles in the whelping bitch. Theriogenology 2010; 73: 1276–1283. [DOI] [PubMed] [Google Scholar]
- 9. Bergström A, Fransson B, Lagerstedt AS, et al. Primary uterine inertia in 27 bitches: aetiology and treatment. J Small Anim Pract 2006; 47: 456–460. [DOI] [PubMed] [Google Scholar]
- 10. Frehner BL, Reichler IM, Keller S, et al. Blood calcium, glucose and haematology profiles of parturient bitches diagnosed with uterine inertia or obstructive dystocia. Reprod Domest Anim 2018; 53: 680–687. [DOI] [PubMed] [Google Scholar]
- 11. Fournier A, Masson M, Corbière F, et al. Epidemiological analysis of reproductive performances and kitten mortality rates in 5,303 purebred queens of 45 different breeds and 28,065 kittens in France. Reprod Domest Anim 2017; 52 Suppl 2: 153–157. [DOI] [PubMed] [Google Scholar]
- 12. Robbins MA, Mullen HS. En bloc ovariohysterectomy as a treatment for dystocia in dogs and cats. Vet Surg 1994; 23: 48–52. [DOI] [PubMed] [Google Scholar]
- 13. Gunn-Moore DA, Thrusfield MV. Feline dystocia: prevalence, and association with cranial conformation and breed. Vet Rec 1995; 136: 350–353. [DOI] [PubMed] [Google Scholar]
- 14. Holst BS, Axnér E, Öhlund M, et al. Dystocia in the cat evaluated using an insurance database. J Feline Med Surg 2017; 19: 42–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Ekstrand C, Linde-Forsberg C. Dystocia in the cat: a retrospective study of 155 cases. J Small Anim Pract 1994; 35: 459–464. [Google Scholar]