

Abstract
Objectives
This study was conducted to validate the dorsal approach for femoral nerve (FN) blockade in cats and to verify the efficacy of the sole use of peripheral nerve electrolocation (PNE) or ultrasound (US)-guided technique to achieve the block.
Methods
This study was carried out in two phases. In phase 1, five adult experimental cats were used to validate the approach. In each cat, one FN was located by US and the accuracy of this location confirmed by PNE. Then, 2 mg/kg lidocaine 2% (diluted in saline to a final volume of 1 ml) was injected around the target nerve and the success of the blockade was evaluated. In phase 2, four adult experimental cats were included in two groups to verify the reliability of this approach to block eight FNs by the sole use of PNE (group 1) or US-guided technique (group 2). Evidence of motor blockade, time required to perform the blockade, onset time and duration of the blockades were determined.
Results
The FN was successfully located by US in all cats enrolled in phase 1, as confirmed by PNE in all cases. The success rate was clinically higher in group 2 (87.5%) than in group 1 (75.0%). The US-guided technique required less time to perform and produced blocks of longer duration. Recovery was uneventful in all cases.
Conclusions and relevance
The combined use of PNE and US-guided technique enabled validation of the dorsal approach for the FN blockade as it provided a successful FN blockade in all cases. The sole use of a US-guided technique may offer some advantages over the use of a sole PNE-guided technique to perform these blocks.
Introduction
Peripheral nerve blockade (PNB) techniques are being incorporated in veterinary anesthesia to provide analgesia of the pelvic limb.1–8 A combined femoral (FN) and sciatic (ScN) nerve blockade has been reported to be at least equally effective as the epidural administration of local anesthetics (LA) in dogs, with potentially fewer side effects. 9 A single FN block is recommended in humans as an analgesic adjunct for a variety of surgical procedures in the pelvic limb, such as fracture repair of the neck and shaft of the femur, hip replacement, total knee arthroplasty, cranial cruciate ligament repair, skin grafts and muscle biopsy of the cranial aspect of the thigh. 10
An ultrasound (US)-guided technique for the blockade of the ScN in cats has been previously described and validated in experimental cats. 11 In previous work, a FN blockade using a dorsal approach was described in feline cadavers, 12 but its clinical efficacy has not yet been documented in live cats.
Peripheral nerve electrolocation (PNE) is considered the gold standard for performing PNBs. 13 However, US-guided techniques offer important advantages such as the ability to visualize the structures of interest in real time thus reducing the need for intraneural or intravascular injections.14,15 There is an ongoing debate on which of these techniques is the most suitable in practice. The study of the efficacy and clinical reliability of a dorsal block of the FN in cats, by the use of either guiding technique, could be of clinical interest.
The aims of this study were to validate, in experimental cats, the efficacy of a dorsal approach to achieve a FN block by the combined use of US and PNE locating techniques, and then to verify the reliability of the sole use of PNE or US-guided techniques to achieve the blockade.
Materials and methods
This experimental study was approved by the Animal Care and Ethics Committee of the University of Murcia. It was conducted in two phases: phase 1 was developed to validate the dorsal approach to achieve a FN block in experimental cats by the combined use of US and PNE. Phase 2 was carried out to verify the clinical efficacy and reliability of this approach in achieving the block by the sole use of PNE or US-guiding techniques.
Animals
Five healthy experimental male cats with a mean ± SD weight of 3.99 ± 0.41 kg were employed. Before each study, cats were fasted overnight for 12 h with free access to water. All cats were sedated by intramuscular administration of 30 μg/kg medetomidine (Domitor; Pfizer) and 0.2 mg/kg butorphanol (Turbogesic; Fort Dodge). Once sedation was achieved, animals were placed in lateral recumbency with the limb to be blocked facing upwards. The lumbar area was clipped and the skin aseptically prepared. One FN was located and blocked in each trial. The procedures were performed with a resting period of at least 7 days between procedures. The animals were handled following the Guide for the Care and Use of Laboratory Animals (8th ed).
Phase 1: validation of the dorsal approach for the FN block in experimental cats
A total of five FNs were approached and then blocked by the use of a dorsal approach described in a previous cadaveric study carried out in cats (Figure 1a). 12 The target nerve was located with US guidance, employing a 4–13 MHz linear transducer (MyLab 70; Esaote). The location of the FN was considered positive when a single, well-differentiated, rounded hypoechogenic structure surrounded by a hyperechogenic rim was identified within the iliopsoas muscle (Figure 1b). 12 The US-guided location of the FN was confirmed by the use of a PNE. A #11 surgical blade (Sovereign) was used to make a skin incision of 2 mm over the dorsal skin surface, approximately 1 cm lateral to the spinous processes. Then, a peripheral 50 mm nerve block needle (Stimuplex; Braun) connected to a PNE was inserted and advanced to the FN. Initially, the current delivered by the PNE was set at 2 Hz, 0.1 ms, and at an intensity of 1 mA. Evidence of positive quadriceps contractions at a stimulating current of 0.4 mA was used to confirm the correct location of the FN by US. The US and PNE location techniques were always performed by the same investigators (AA and PH). The administration of LA was performed by a single operator (PH). Once the nerve location was confirmed, lidocaine 2% (2 mg/kg) diluted in saline (total volume of 1 ml) was infiltrated around the FN. Multiple small volume injections were made to obtain a circumferential distribution of the LA around the nerve producing the ‘doughnut’ sign (Figure 1c). Negative pressure was applied to the syringe before each injection. Injections were discontinued if increased resistance was detected during the injection. After the administration of LA, sedation was immediately antagonized (atipamezole 75 µg/kg IM) and the success of the blockade was evaluated. The cats were observed for 72 h to determine the presence of complications such as hematomas, infection, pain or signs of nerve injury.
Figure 1.
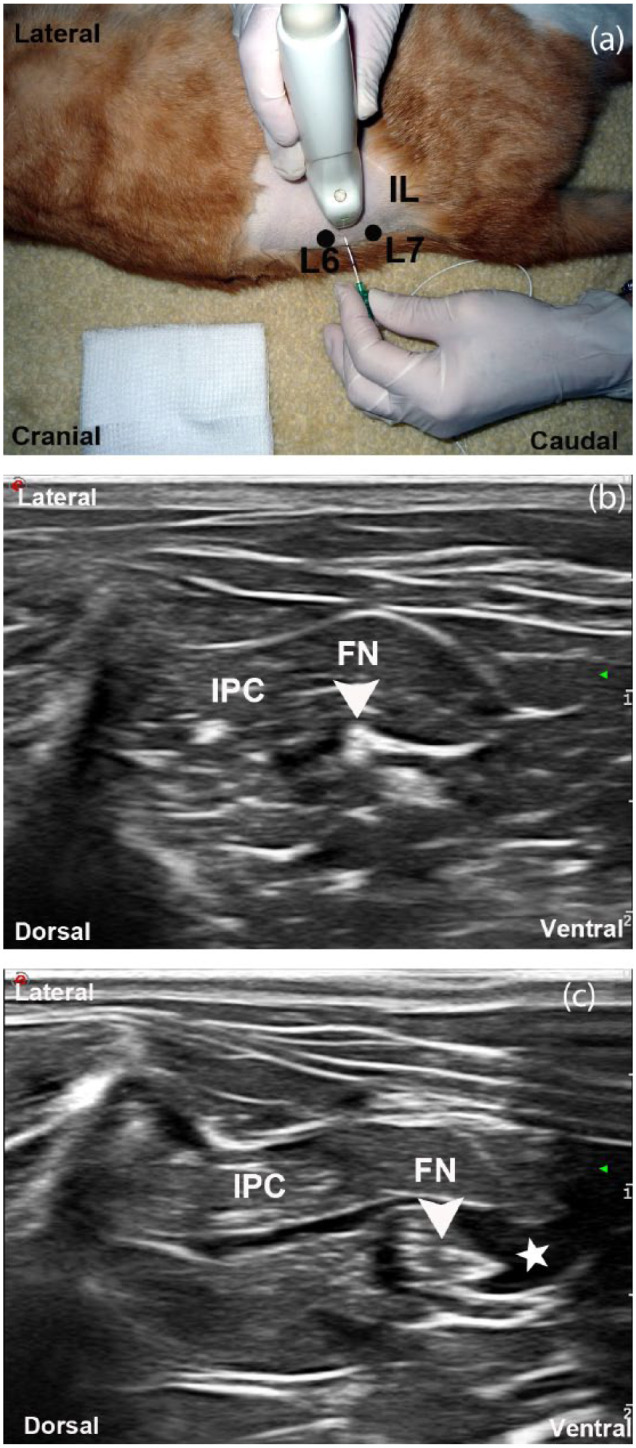
Ultrasound (US)-guided technique for the femoral nerve (FN) location and block using the dorsal approach. (a) Anatomic landmarks for the dorsal approach to the FN. The transducer was positioned lateral to the abdominal wall, perpendicular to the spine and cranial to the iliac crest (IL) at the level of sixth (L6) and seventh (L7) lumbar spinous processes. (b) Transverse ultrasonographic image of the FN (arrowhead) at this level. The FN is observed within the iliopsoas muscle complex (IPC). (c) Ultrasonographic image during the US-guided injection of local anesthetic (LA) around the FN. The circumferential spreading of the LA (star) around the FN (arrowhead) is observed
Phase 2: verification of the sole use of PNE or US-guided technique to block the FN by a dorsal approach in experimental cats
Four experimental male cats with a mean ± SD weight of 4 ± 0.40 SD were employed in this part of the study. In each group, a total of eight FNs (four on the right and four on the left side) were blocked. Only one FN was blocked in each experiment.
Group 1: PNE-guided FN block
Eight FNs were located and then blocked by the use of PNE. The anatomic landmarks employed to locate the FN were the spinous processes of L6 and L7 and the cranial border of the iliac crest. These bone structures were palpated and marked over the skin. A dotted line connecting L6–L7 was drawn, then a second dotted line was traced perpendicular to the spine, starting at mid-distance between L6 and L7, and finishing over the limits of the lateral abdominal wall. The second line was divided into thirds. Over the first third, another line parallel to the spine was drawn. The crossing point between the second and the third lines was considered to be the puncture site (Figure 2). A stab skin incision of 2 mm was performed over this point using a #11 surgical blade (Sovereign). A peripheral nerve block needle was inserted and the PNE turned on using the same settings described for phase 1. The needle was slowly advanced in a ventral direction. The location of the FN was considered successful when muscular contractions of the quadriceps muscle were observed at a current intensity of 0.4 mA. LA was administered and sedation antagonized as previously described. Then, the success of the blockade was evaluated. The time required to perform the block, defined as the time elapsed between the first needle to skin contact until the end of the injection, was recorded. Onset time and duration of the blockade were also recorded. Cats were evaluated over the following 72 h to determine the presence of complications.
Figure 2.
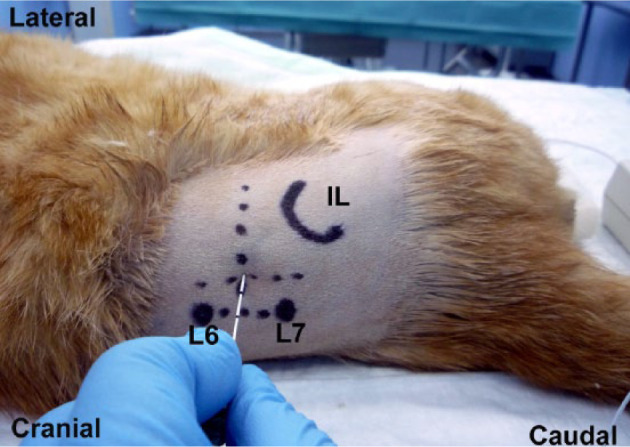
Peripheral nerve electrolocation technique for the femoral nerve location and block using the dorsal approach. The anatomic landmarks were the spinous processes of the sixth (L6) and seventh (L7) lumbar vertebrae. A dotted line was drawn connecting them. Then, a second dotted line was traced at mid-distance between these points and perpendicular to the spine to the limits of the lateral abdominal wall. The second line was divided into thirds. At the first third, another line was traced parallel to the spine line. The crossing point between the second and the third lines was considered the puncture site. IL = iliac crest
Group 2: US-guided FN block
Eight FNs were located and blocked by the sole use of a US-guided technique employing the methodology described in phase 1 of the study. The time required to perform the FN block, defined as the time elapsed between the first transducer to skin contact until the end of the injection, was recorded. Onset time and duration of the blockade were also recorded. Cats were evaluated for the next 72 h to determine the presence of complications.
Evaluation of the FN blockade
Once sedation was effectively reversed, the motor function of the blocked limb was assessed every 2 mins for the first 10 mins, then every 5 mins for the following 90 mins and thereafter every 15 mins. The last assessment was made 30 mins after normal motor function had returned. All assessments were performed by the same researcher (PH). The evaluation of the block was conducted by observing the position of the blocked leg while the cat was standing and walking. A three-point rating scale was employed: 0 = normal motor response (normal ability to walk or stand); 1 = partial motor blockade (incomplete ability to bear weight, incomplete flexion of the stifle, muscle tone weaker than in the contralateral limb); 2 = complete motor blockade (inability to stand and walk with the blocked limb, knee in extension touching the floor, limb paralyzed). The blockade of the FN block was considered to be clinically effective when a score of 2 was reached (Figure 3).
Figure 3.

Evaluation of the femoral nerve block using a dorsal approach. Inability to bear weight and knee in extension touching the floor is observed
Onset time
Onset time was defined as the time elapsed from the injection to the time when a score of 1 or 2 was noticeable.
Duration of the blockade
Duration was defined as the length of time that partial or complete motor blockade was observed.
Data analysis
Descriptive statistics (mean ± SD) were calculated from the tabulated measurements. Student’s t-test was used to compare success rate, time to perform the blocks, onset of action and duration of motor blockade between groups. The level of significance was set at P <0.05.
Results
Phase 1: validation of the dorsal approach for the FN block in experimental cats
The FN was successfully located by US in all cases. The accuracy of this location was confirmed by PNE in all cats. The US appearance of the FN was that of a single, well-differentiated rounded hypoechogenic structure encircled by a hyperechogenic rim. The FN was located within the iliopsoas muscle complex. The spreading of LA solution around the FN could be observed in real time in all cases. The doughnut sign was not observed in 3/5 cats. There was no resistance to injection, and negative blood aspiration was obtained in all cases. As a score of 2 was noted in all trials, the FN blockade was considered to be successful in all cases. No adverse effects were observed.
Phase 2: verification of the sole use of PNE or US-guided technique to block the FN by a dorsal approach in experimental cats
Group 1: PNE-guided FN block
The FN was successfully located by the sole use of PNE in all cases. Contractions of the quadriceps femoris muscles were easily elicited at 0.4 mA in all cats. The needle was inserted at a depth range of 3.0–3.5 cm. In those cats weighing <4 kg, it was necessary to tilt the needle in a medial direction to obtain quadriceps contractions of a better quality. Muscle contractions were abolished once the administration of LA commenced (Table 1).
Table 1.
Results of verification of the sole use of peripheral nerve electrolocation (PNE) and ultrasound (US)-guided technique to block the femoral nerve (FN) by a dorsal approach in experimental cats
| Verification of the FN block | Group 1 PNE | Group 2 US |
|---|---|---|
| Evaluation of the motor blockade | ||
| Score 2 | 6/8 | 7/8 |
| Score 1 | 1/8 | 1/8 |
| Score 0 | 1/8 | 0/8 |
| Time required (mins) | ||
| Time to perform the block | 6.3 ± 4.4 (1–10) | 2.7 ± 0.9 (2.0–4.1) |
| Onset time | 6.0 ± 2.0 (4–10) | 7.0 ± 2.0 (4–10) |
| Duration time of block | 47.0 ± 10.0 (35–64) | 59.0 ± 18.0 (35–95) |
Data presented as mean ± SD (range) (n = 8)
Score 2 = complete motor blockade (inability to stand and walk, knee in extension touching the floor, limb paralyzed); score 1 = partial motor blockade (incomplete ability to bear weight, incomplete flexion of the stifle, muscle tone weaker than in the contralateral limb); score 0 = normal motor response (normal ability to walk or stand)
Group 2: US-guided FN blockade
The US-guided technique enabled localization and blockade of the FN in all cases. A circumferential spread of LA was produced in all cats. The needle was inserted at a depth range of 3.0–3.5 cm to reach the FN (Table 1). There was no resistance to injection and a negative blood aspiration was obtained in all cases. No adverse effects were recorded after any injection.
There were no statistical differences in terms of time to perform the blocks (P = 0.16), onset of action (P = 0.44) or duration of motor blockade (P = 0.09) between groups.
Discussion
The main aim of the present study was to validate in live cats the efficacy of a dorsal approach to block the FN by the combined use of US- and PNE-guided techniques. This approach was previously reported in a feline cadaver study. 12
This approach was selected because it has been reported to be the most suitable way of accessing the main trunk of the FN in cats, ensuring the inclusion of all the motor and sensory FN branches. 12 The clinical reliability of this approach was verified in phase 1 of the study by the combined use of US and PNE techniques to locate the target nerve. These techniques allowed us to determine the correct location of the FN, resulting in a successful blockade in all cases, even in those cats where the doughnut sign was not observed by US (3/5). These findings support other studies, which described that the presence of the doughnut sign is not mandatory to predict a successful nerve blockade.11,16
To our knowledge, this is the first report of a technique to block the FN in live cats. In dogs, this block has been performed using a femoral triangle,1,3,6,17 preiliac, 2 iliopsoas 18 and suprainguinal approaches. 8 The femoral triangle approach only had a 50% success rate in dogs. 1 In contrast, the preiliac, 2 iliopsoas 18 and suprainguinal 8 approaches to the FN in dogs had a 100% success rate, which is similar to that obtained using the dorsal approach proposed in this study. These results could be explained by the similar characteristics of these approaches, as they intend to reach the FN near the main trunk, within the iliopsoas muscle complex, before the FN bifurcates. The US appearance of the FN found in this study was similar to previous descriptions in feline cadavers and also in live dogs.8,12 The ultrasonographic appearance of the FN seems to be enhanced at this level owing to a better contrast obtained between the nerve structure and the surrounding more echogenic muscle fibers. 8
PNB can be performed using anatomic landmarks, PNE or US to guide the blocks. PNE is a blind technique as it is not possible to determine the exact location of the needle in relation to the target nerve. The location of the needle is indirectly inferred by the motor response elicited by this technique. Another limitation is that PNE-guided techniques are not useful in locating sensory nerves. In comparison, US-guided techniques are extremely useful for locating the target nerve, needle and other relevant surrounding anatomical structures. This technique provides images of the pattern of distribution of the LA around the target nerve, allowing repositioning of the needle if necessary. It also permits the use of small volumes, allowing a reduction in the total dose of LA administered when multiple nerve blockades have to be performed in comparison to PNE techniques. 15 This could be particularly important in cats as they are more susceptible to toxicity of LA.19,20
In a veterinary clinical setting, deciding between the use of US or PNE techniques to conduct PNB depends on the availability of the equipment and also on operator preference. For this reason, the efficacy and clinical reliability of the described FN block carried out by the exclusive use of a sole PNE- or US-guided technique were assessed in phase 2 of this study.
In our study, the location of the FN was 100% successful using either PNE- or US-guided techniques. However, the sole use of US resulted in a slightly higher FN block success rate (87.5%) than the PNE technique (75.0%). These results could be biased by the low number of nerves blocked in our study and also by the expertise in the use of US-guided techniques of our operator.
A case of partial motor blockade was obtained in both groups (1/8). In this study, an even and circumferential distribution of LA around the FN was observed using US guidance but the longitudinal spreading of LA was not determined. It has been pointed out that the length of nerve in contact with the LA solution is the main factor determining the clinical success of a PNB. 21 A longitudinal distribution of LA ⩾2 cm has been classically considered as sufficient to produce an effective nerve block.7,21 A previous study conducted in feline cadavers showed that injection of 1 ml of ink by the dorsal approach produced a longitudinal spreading of ink within a range of 3.0 to 4.6 cm. 12 Differences in the longitudinal distribution of injectate along a nerve between cadavers and live specimens has already been reported. This could be owing to different factors such as the uptake of the solution by the lymphoid system and also by blood circulation. 22 The intensity of a nerve block is also dependent on the concentration of the LA administered. The concentration injected determines the sequence of blockade of motor and sensory function. As a consequence, it requires a higher concentration of a LA to block motor fibers than it does to block sensory fibers. 23 In the present study the mean concentration of LA administered was 0.80% (range 0.68–0.88%). To our knowledge, the critical concentration to achieve a motor level block has not yet been determined in cats. Further investigations studying these factors are necessary to increase the reliability of the described techniques in a clinical setting.
Only one cat showed no signs of motor blockade (score 0) in the PNE group. This cat received the highest concentration of LA administered (0.88%) in the present study. It is possible that this finding could be related to a misdistribution of LA around the FN during the injection. The success rate might have been higher in the PNE group if a lower stimulating current of 0.3 mA had been selected. 24 However, some authors do not recommend the use of currents lower than 0.4 mA because of the increased risk of intraneural injection. 25
To our knowledge, this is the first study to verify the efficacy of the PNE- and US-guided techniques to perform PNB in veterinary medicine. An obvious limitation of this study was the low number of nerves finally blocked. This could be the reason for the lack of statistical differences found. Therefore, further studies, using more animals and, ideally, performed in a clinical setting are still necessary to determine differences between US- and PNE-guided techniques to perform the blockade of the FN in cats.
Conclusions
The dorsal approach to blocking the FN in experimental cats is clinically effective. This nerve can be successfully located and blocked by the combined use of US and PNE techniques, as well as by the sole use of US or PNE locating techniques. The sole use of a US-guided technique may offer some advantages over the use of a sole PNE-guided technique.
Footnotes
The authors do not have any potential conflicts of interest to declare.
Funding: Part of this research was supported by the National Council of Science and Technology (CONACYT), Mexico (grant number 179403).
Accepted: 18 May 2015
References
- 1. Echeverry DF, Gil F, Laredo F, et al. Ultrasound-guided block of the sciatic and femoral nerves in dogs: a descriptive study. Vet J 2010; 186: 210–215. [DOI] [PubMed] [Google Scholar]
- 2. Portela DA, Otero PE, Tarragona L, et al. Combined paravertebral plexus block and parasacral sciatic block in healthy dogs. Vet Anaesth Analg 2010; 37: 531–541. [DOI] [PubMed] [Google Scholar]
- 3. Shilo Y, Pascoe PJ, Cissell D, et al. Ultrasound-guided nerve blocks of the pelvic limb in dogs. Vet Anaesth Analg 2010; 37: 460–470. [DOI] [PubMed] [Google Scholar]
- 4. Costa-Farre C, Blanch XS, Cruz JI, et al. Ultrasound guidance for the performance of sciatic and saphenous nerve blocks in dogs. Vet J 2011; 187: 221–224. [DOI] [PubMed] [Google Scholar]
- 5. Echeverry DF, Laredo FG, Gil F, et al. Ultrasound-guided ‘two-in-one’ femoral and obturator nerve block in the dog: an anatomical study. Vet Anaesth Analg 2012; 39: 611–617. [DOI] [PubMed] [Google Scholar]
- 6. Campoy L. Fundamentals of regional anesthesia using a peripheral nerve stimulator. In: Gleed RD, Ludders JW. (eds). Recent advances in veterinary anesthesia and analgesia: companion animals. http://www.ivis.org/advances/Anesthesia_Gleed/campoy/chapter.asp?LA=1) (2005, accessed October 22, 2014).
- 7. Campoy L, Martin-Flores M, Looney AL, et al. Distribution of a lidocaine-methylene blue solution staining in brachial plexus, lumbar plexus and sciatic nerve blocks in the dog. Vet Anaesth Analg 2008; 35: 348–354. [DOI] [PubMed] [Google Scholar]
- 8. Echeverry DF, Laredo FG, Gil F, et al. Ventral ultrasound-guided suprainguinal approach to block the femoral nerve in the dog. Vet J 2012; 192: 333–337. [DOI] [PubMed] [Google Scholar]
- 9. Campoy L, Martin-Flores M, Ludders JW, et al. Procedural sedation combined with locoregional anesthesia for orthopedic surgery of the pelvic limb in 10 dogs: case series. Vet Anaesth Analg 2012; 39: 91–98. [DOI] [PubMed] [Google Scholar]
- 10. Szucs S, Morau D, Iohom G. Femoral nerve blockade. Med Ultrason 2010; 12: 139–144. [PubMed] [Google Scholar]
- 11. Haro P, Laredo F, Gil F, et al. Ultrasound-guided block of the feline sciatic nerve. J Feline Med Surg 2012; 14: 545–552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Haro P, Laredo F, Gil F, et al. Ultrasound-guided dorsal approach for femoral nerve blockade in cats: an imaging study. J Feline Med Surg 2013; 15: 91–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Abrahams MS, Aziz MF, Fu RF, et al. Ultrasound guidance compared with electrical neurostimulation for peripheral nerve block: a systematic review and meta-analysis of randomized controlled trials. Br J Anaesth 2009; 102: 408–417. [DOI] [PubMed] [Google Scholar]
- 14. Marhofer P, Greher M, Kapral S. Ultrasound guidance in regional anaesthesia. Br J Anaesth 2005; 94: 7–17. [DOI] [PubMed] [Google Scholar]
- 15. Kumar PA, Gentry WB, Arora H. Ultrasound guidance in regional anaesthesia. J Anaesth Clinical Pharmacol 2007; 23: 121–128. [Google Scholar]
- 16. Eichenberger U, Stockli S, Marhofer P, et al. Minimal local anesthetic volume for peripheral nerve block: a new ultrasound-guided, nerve dimension-based method. Reg Anesth and Pain Med 2009; 34: 242–246. [DOI] [PubMed] [Google Scholar]
- 17. Mahler SP, Adogwa AO. Anatomical and experimental studies of brachial plexus, sciatic, and femoral nerve-location using peripheral nerve stimulation in the dog. Vet Anaesth Analg 2008; 35: 80–89. [DOI] [PubMed] [Google Scholar]
- 18. Mahler SP. Ultrasound guidance to approach the femoral nerve in the iliopsoas muscle: a preliminary study in the dog. Vet Anaesth Analg 2012; 39: 550–554. [DOI] [PubMed] [Google Scholar]
- 19. Court MH, Grenblatt DJ. Molecular basis for deficient acetaminophen glucuronidation in cats. Biochem Pharmacol 1997; 53: 1041–1047. [DOI] [PubMed] [Google Scholar]
- 20. Robertson SA, Taylor PM. Pain management in cats – past, present and future. Part 2. Treatment of pain – clinical pharmacology. J Feline Med Surg 2004; 6: 321–333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Raymond SA, Steffensen SC, Gugino LD, et al. The role of length of nerve exposed to local anesthetics in impulse blocking action. Anesth Analg 1989; 68: 563–570. [PubMed] [Google Scholar]
- 22. Kull K, Baer GA, Samarutel J, et al. Distribution of local anesthetic solution in retromediastinal block: preliminary experimental results. Reg Anesth 1997; 22: 308–312. [PubMed] [Google Scholar]
- 23. Winnie AP, Chen-Hin T, Kanchan PP. Pharmacokinetics of local anesthetics in plexus blocks. Anaesth Analg 1977; 56: 852–861. [DOI] [PubMed] [Google Scholar]
- 24. Neuburger M, Rotzinger M, Kaiser H. Electric nerve stimulation in relation to impulse strength. A qualitative study of the distance of the electrode point to the nerve. Anaesthesist 2001; 50: 181–186. [DOI] [PubMed] [Google Scholar]
- 25. Chan VWS, Brull R, McCartney CJL, et al. An ultrasonographic and histological study of intraneural injection and electrical stimulation in pigs. Anaesth Analg 2007: 104: 1281–1284. [DOI] [PubMed] [Google Scholar]