

Abstract
Workplace supportive supervisor interventions offer an effective, though underutilized mechanism to bolster employee well-being, which may have important benefits particularly for understudied groups such as military veterans in the civilian workforce. The present study employed a two-wave daily diary study to test the effectiveness of a supportive supervisor training on positive and negative emotions of veteran employees. Daily diaries are instrumental to understanding well-being, in that they accurately capture emotions as they are experienced without retrospective biases that reflect more global emotional assessments. Each wave (baseline and 6 months later) comprised emotion reports over 32-day periods. Thirty-five organizations were randomized into intervention and control groups; 144 veterans (91% men) participated in the daily diaries at baseline. The training significantly improved well-being facets including improvements in unactivated positive (i.e., calm) emotions at follow-up. Two significant moderation effects were also revealed for PTSD screening. For veteran employees with positive PTSD screens, the intervention functioned to reduce negative emotions. For those employees with negative PTSD screens, the intervention enhanced positive emotions. Our work highlights the benefit of workplace supervisor support to positive and negative employee mood.
Military veterans comprise nearly 6% of the U.S. civilian workforce (Bureau of Labor Statistics, 2020). Over four million people have served in the U.S. military since Operation Enduring Freedom and Operation Iraqi Freedom (OEF/OIF, or post-9/11); the number of transitioning service members is estimated to continue to grow, with current numbers reaching 200,000 per year (Ainspan, Penk, & Kearney, 2018). Veterans are well-qualified for many workplace roles, bringing diverse experiences and perspectives, along with strong skills (Hammer, Brockwood, & Haverly, 2021; Hardison & Shanley, 2016). Successful integration into the civilian workforce is an important opportunity for organizations. Furthermore, successful integration is critical to the well-being of service members who have sacrificed for the benefit of the country (Elnitsky, Blevins, Fisher, & Magruder, 2017). According to Elnitsky et al., too little research has focused on community-level factors (such as workplaces) that play a critical role in successful societal reintegration; research fails to acknowledge the interplay between community- and individual-level factors (e.g., how supportive work environments can promote individual veteran psychological health). This coincides with recent calls for more research on this underserved population of employees (e.g., Colella, Hebl, & King, 2017). Although many veterans make the transition seamlessly, some need greater support, and the workplace is an effective context for interventions demonstrated to improve psychological health (Hammer, Wan, Brockwood, Bodner, & Mohr, 2019) and the work–family interface, especially for higher-stressed employees (Hammer, Kossek, Anger, Bodner, & Zimmerman, 2011). Indeed, a subset of post-9/11 veterans experience post-traumatic stress disorder (PTSD; about 13.5%; Dursa, Reinhard, Barth, & Schneiderman, 2014) and thus may have particular support needs. The aim of the present study is to examine the effectiveness of one such intervention – a supervisor support training (SST) intervention tailored to support military veterans who have transitioned to the civilian workplace.
With increased interest in the improvement of health and well-being of workers among occupational health scholars and organizational practitioners, more efforts have been focused on developing and evaluating the effects of workplace interventions (Hammer & Perry, 2019). Positive effects have been demonstrated for training interventions targeting supervisor supportive behaviours on worker outcomes including sleep (e.g., Crain et al., 2019) and psychological health (e.g., psychological distress; Kossek et al., 2019). Such trainings draw on the rich and voluminous literature on social support to provide supervisors with evidence-based tools to enrich employees’ positive resources and mitigate negative stress-related outcomes. Based on evidence of the value of supporting employee health and well-being, as well as theoretical and empirical support for the importance of emotional well-being, interventions that target reductions in employee stress and enhance resources by increasing supervisor support should benefit both employees and the workplace. However, evaluating the effectiveness of such interventions on employees’ emotional well-being may require different strategies from traditional longitudinal multi-wave surveys.
Although SSTs provide benefits to workplace organizations and their employees as a whole, research has documented the tailored benefits that can be afforded to employees confronting particular challenges, such as employees managing work–family conflicts (e.g., Hammer et al., 2011), or those experiencing a period of high stress or mental health difficulties (e.g., Dimoff & Kelloway, 2019). For veterans and non-veterans alike, generational demographic changes in the workforce have led to a burgeoning interest in the work–family interface with the evolution in work and domestic roles (e.g., women working outside the home; Halpern, 2005), along with interventions designed to maximize the benefits of flexibility, while reducing conflicts between work and family domains (e.g., Hammer et al., 2011). Social support may be particularly beneficial to people in greater need, such as members of disadvantaged groups (Bavik, Shaw, & Wang, 2020). One such disadvantaged group is that of military veteran employees, as this is a group of employees who are likely to face stigma in the workplace (Stone & Colella, 1996; Stone & Stone, 2015) due to perceptions of being ‘damaged’ or of ‘poorer’ mental health than the general population (Britt, Black, Cheung, Pury, & Zinzow, 2018).
Workplace social support
Social support theory provides the foundation for understanding supervisor support mechanisms and provides guidance for tools and strategies supervisors can use to bolster employee well-being. Generally speaking, the social support we receive from others in our social networks, including the people with whom we work, is vital to our health and well-being (e.g., Cohen & Wills, 1985) including emotions (Pierce & Quiroz, 2019). Perceptions of workplace social support involve the perception that one is a valued employee and the access to resources that help meet role demands (e.g., Kossek, Pichler, Bodner, & Hammer, 2011); such resources include emotional and instrumental or tangible assistance (e.g.,Cutrona, 1989).According to a recent comprehensive meta-analysis of the multidisciplinary social support literature, social support plays multiple distinct roles in shaping well-being (Bavik et al., 2020). Of most relevance to our investigation is the role of social support as positivity catalyst and negativity buffer (Bavik et al., 2020).
Positivity catalyst describes how the exchange of resources over time fosters high quality social relationships and is built on the social norm of reciprocity that governs all relationships (e.g., Gouldner, 1960). When social support acts as a positivity catalyst, an employee provided with a supportive benefit engenders their own positive behaviour (e.g., employee engagement). While this role of social support as a positivity catalyst is consistent with social exchange theory (Blau, 1964), it also suggests that the provision of support serves as a resource, as described in the conservation of resources (COR) theory (Hobfoll, 1989) and the job demands-resources (JD-R) model (Demerouti, Bakker, Nachreiner, & Schaufeli, 2001). COR theory and the JD-R model articulate how employees are motivated to accumulate and maintain highly valued resources, yielding work and well-being benefits. This view of social support most closely aligns with the direct effect model of social support (Cohen & Wills, 1985), in which positive benefits are derived directly from one’s socially rewarding social roles and embeddedness in a larger social network, and not necessarily in response to a real or potential stressor.
The most dominant perspective of social support roles is that of the negativity buffer (Bavik et al., 2020). In this role, the potential impact of a stressor on one’s health and well-being is a function of one’s appraisal of a perceived stressor and one’s adequacy (or inadequacy) of resources to meet the needs of that stressor (Lazarus & Folkman, 1984). In the workplace context, support can also be viewed as a resource, which can reduce the negative effects of stressors and job demands on well-being, consistent with the JD-R model (Demerouti et al., 2001). This support role is most consistent with the stress-buffering function of social support (Cohen & Wills, 1985). Although received support can be miscarried, support that is given when needed is associated with positive perceptions of support and mental well-being (Melrose, Brown, & Wood, 2015). As a negativity (or stress) buffer, social support can influence the appraisal of a potential stressor, thereby preventing a stress response. Similarly, a key benefit of resource accumulation, as described above, is that it prevents the occurrence of many stressors.
Supervisors are particularly valuable source of support for employees in the workplace, as the support they give can serve as both a positivity catalyst and negativity buffer. Supervisors are able to cultivate a culture of support for employees; for example, workplace programmes encouraging family supportive supervisor behaviours (FSSB) lead to improved employee health, well-being, and work outcomes (Hammer & Perry, 2019). Supervisors also hold positions enabling them to provide critical resources to offset work-related stress (Hammer,Kossek,Zimmerman,& Daniels, 2007). They provide direction on performing the job, provide rewards for performance, and are gatekeepers to top organizational leaders and to accessing organizational programmes and policies that can support employees both in times of need and normalcy.
Consequently, supervisor support benefits employee health and well-being (for reviews, see Crain & Stevens, 2018; Kelloway & Barling, 2010), impacting both positive and negative psychological health outcomes, including stress and strain (Kelloway & Barling, 2010). During times of high need (e.g., organizational crisis), employee positive and negative emotions mediate the relationship between perceptions of supervisor support and cynicism (Cole, Bruch, & Vogel, 2006). Daily supervisor support protects against work–family conflict-associated declines in negative affect (Almeida et al., 2016). Further, FSSB training, which is conceptually related to the present study intervention, has been shown to improve job satisfaction among employees experiencing significant work–family conflict (Hammer et al., 2011); job satisfaction being a facet of subjective well-being, along with emotions (e.g., Diener, 2009; Judge & Locke, 1993). Despite evidence on the benefits of supervisor support (e.g., Hammer et al., 2011; Odle-Dusseau, Hammer, Crain, & Bodner, 2016), little information in the literature instructs supervisors on how to enact supportive behaviours. Recently, research has begun to demonstrate the positive effects of SST interventions that target enactment of supportive behaviours on worker health and well-being outcomes (e.g., Crain et al., 2019; Kossek et al., 2019).
Workplace SST for veterans
The workplace SST developed for this study targets support provisions that are relevant to all employees, while also incorporating veteran-specific support that targets the civilian workplace reintegration of veterans and active reservists (e.g., National Guard service members). Our approach helps address the call for the inclusion of more diversity of employees in organizational research, including current and former service members (i.e., veterans; Colella et al., 2017), in order to better understand the workplace context for that segment of the workforce. Evidence suggests that challenges in work and family domains may be particularly concerning for reintegrating veterans who report difficulty adjusting to civilian life post-military deployment (44%) and experience strains in family life (48%; Tanielian, Batka, & Meredith, 2017). In addition, veterans face many potential work-related difficulties, including a lack of positive support interactions and stigma in the workplace (Keeling, Kintzle, & Castro, 2018). Many veterans face additional stressors, such as cynicism that carry over from military deployment and issues affecting work and family functioning (Smith, Weisenbach, & Jones, 2018). Thus, workplace supports developed to address work–family issues may be especially beneficial to military veterans’ emotional well-being.
The SST examined in the present study (Hammer et al., 2019) is based on evidence-based FSSB training (Hammer, Demsky, Kossek & Bray, 2016) and targets four types of support behaviours, defined as (1) emotional, or behaviours that demonstrate a worker is cared for and their feelings are being considered; (2) instrumental, or behaviours that help workers manage schedules and solve schedule conflicts; (3) role modelling, or behaviours that show how a supervisor is taking care of their own work/life challenges; and (4) creative work–family management, or behaviours aimed at redesigning work to support conflicting employee work-life demands in a manner that is a ‘win-win’ for both employees and employers. Job performance support training was also included covering topics associated with general supervisor skills that address task accomplishment, including measurement, direction, feedback, coaching, providing resources, and health protection, to complement the FSSB training (Hammer et al., 2016). Our intervention also included information regarding mental and physical health effects that could result from military combat, including clarifying that the incidence of PTSD in the military is lower than public perceptions (Mahar et al., 2017), while offering tips on warning signs, thereby educating civilian supervisors and destigmatizing such experiences.
Thus, we aimed to cultivate greater resources for the veterans through SST leading to improved well-being. The intervention also includes information that contributes to a supportive military culture by highlighting the contributions of service members such as high levels of dedication and strong leadership skills and abilities. Accordingly, the positive emotional enhancement brought about by the SST serves as a positivity catalyst and negativity buffer.
Emotional well-being and intervention assessment
Positive and negative emotions are characterized as feeling pleasant or unpleasant across lay and academic perspectives (e.g., Beedie, Terry, & Lane, 2005; Davidson, 1994; Russell & Barrett, 1999) and comprise core components of subjective well-being, with the understanding that optimal well-being is represented by a high positive emotion to negative emotion ratio (Diener, 2000). Positive and negative emotions ebb and flow with everyday positive and negative events (Gable, Reis, & Elliot, 2000) including work stressors (e.g., Bolger, DeLongis, Kessler, & Schilling, 1989). Emotions and cognitions are thought to be primary responses to contextual factors (Lazarus, 1982; Zajonc, 1980), preceding behavioural outcomes. Positive and negative emotions function independently (Diener & Emmons, 1984), meaning individuals can experience both low negative and positive emotions simultaneously. Emotional well-being has most often been represented by a summary or composite of positive and of negative emotion scores to represent a general sense of pleasant or unpleasant emotional experience (e.g., Diener, 2000).
Because emotional states are dynamic and changeable (e.g., Larsen & Kasimatis, 1990), as are the relationships between day-to-day stressors and emotions, it is critical to capture these variables as they are experienced, as opposed to retrospectively (e.g., Tennen, Affleck, Armeli, & Carney, 2000). Importantly, a recent rigorous evaluation of global perceptions of well-being (as in traditional self-report surveys) revealed that global perceptions overestimate daily experiences of well-being when compared to daily reports of well-being (Newman, Schwarz, & Stone, 2020). Beyond reflecting recent experience, global reports also incorporate peak experiences and frequently occurring experiences. Newman et al. (2020) highlight the benefits of assessing well-being via aggregated daily emotions or ‘momentary averages’ of emotions as a more accurate means for assessing well-being as it is experienced in one’s daily life. We propose that this more accurate methodological approach should be incorporated into the context of measuring SST effectiveness. Thus, using a randomized controlled trial (RCT) design with 35 organizations, where organization was the unit of randomization, we examined the effects of an SST intervention on employee emotions experienced during the 32-day pre-intervention period and then again 6 months later (post-intervention) in a second 32-day diary. Our study offers a beneficial method for assessing training effectiveness on employee’s daily emotional experience.
One additional benefit to employing daily emotion reports is that it facilitates the differentiation of positive and negative emotions into discrete emotions based on the pleasant/unpleasant dimension and also the physiological arousal or activation associated with each, as described by the Circumplex Model of Emotion (Larsen & Diener, 1992). Bored emotion, for example, is considered the opposite of enthusiastic or lively emotions. Similarly, unactivated (or deactivated) unpleasant is considered the opposite of activated pleasant emotion, wherein each emotion type (e.g., unactivated pleasant, activated pleasant, unactivated negative, activated negative) is theoretically associated with distinct behavioural effects. FMRI research has provided evidence that valence, or the positive–negative dimension of emotion, is associated with a distinct neural substrate in the brain from the arousal dimension (Posner et al., 2009). Weiss and Cropanzano (1996) noted the potential value for considering discrete emotional states in workplace studies. A recent study demonstrated clear relationships between perceived supervisor support and both positive and negative emotions in the expected directions (Cole et al., 2006). Further, Lazarus (2006) articulated the importance of examining discrete emotions, which can hinder or enhance our interpersonal relationships and are a central feature of our ongoing relationships, in addition to general summaries (composite scores) of positive and negative emotions via daily diary reports. We proposed to examine emotions from both a dimensional view, which presumes there is an underlying commonality according to valence (i.e., positive vs. negative), as well as a discrete emotions view, whereby emotions ‘are assumed to be psychologically meaningful units that have unique organizational significance’ (Diener, Thapa, & Tay, 2020, p. 453).
Despite previous work demonstrating the beneficial effects of SST on employee health and work outcomes (Hammer et al., 2019) there is no published research establishing the effects of such an intervention on daily emotions. Considering that emotion is a core component of well-being, and the above literature ties supportive supervision to emotional well-being, we hypothesized that:
H 1. The SST would have a significant effect on veteran employee emotions, specifically improving positive emotions and decreasing negative emotions 6 months post-intervention both in terms of composite (average) and discrete positive and negative emotions.
Post-traumatic stress (PTSD)
Negative affective disturbance (e.g., loneliness, irritability) is a defining feature of PTSD, as are difficulties enjoying positive experiences (APA; American Psychiatric Association, 2013). According to the DSM-V, those with PTSD can experience ‘persistent negative emotional states’ as wellas ‘persistent inability to experience positive emotions’ (pp. 271–272). Consequently, veterans who are experiencing greater PTSD may experience greater negative emotions in their daily lives than those who do not have PTSD and thus may be in particular need of supportive intervention to help reduce such distress. Experimental research has shown that following exposure to emotion words in the laboratory, combat veterans with PTSD experienced less positive emotion (i.e., calm, pleased) and greater negative emotion than combat veterans without PTSD (Amdur, Larsen, & Liberzon, 2000). Yet, social support should buffer the effects of negative stimuli on individual well-being (Cohen& Wills, 1985). Correspondingly, post-deployment social support has been shown to reduce PTSD severity for veterans (Han et al., 2014). We proposed that although PTSD screening would have a positive relationship with daily negative emotions, the intervention would buffer the relationship between PTSD and daily negative emotions. It is less clear whether the intervention would boost positive emotions among those with PTSD, given the evidence of anhedonia or emotional numbing reported in (male) veterans with PTSD in terms of positive emotion (e.g., Kashdan, Elhai, & Frueh, 2007). Consequently, we did not propose a directional hypothesis for this test.
As previously reported (McCabe, Mohr, Hammer & Carlson, 2019), the estimate of positive PTSD screens from our survey sample was 17%. Such PTSD screening and cutoffs are defined based on empirically based levels that identify those veterans who are likely to be experiencing PTSD symptoms and in need of early intervention (Bliese et al., 2008). The use of screening tools with empirically validated cutoff values, such as the PTSD screening, has been widely encouraged as a way of reaching more members of the general public who may need support or intervention. Researchers have noted this as a significant development for public mental health, as these tools can be quickly and easily administered without a clinician and have been instituted broadly including in the military (e.g., Bliese, Adler, & Castro, 2011). The present study affords the opportunity to consider whether those above the PTSD screening cutoff receive particular benefit from the supervisor support intervention, relative to those below the PTSD screening cutoff.
H 2. PTSD scores would moderate the effects of the SST on employee negative emotions such that the intervention has a stronger (decreasing) effect on negative emotions among veteran employees with positive screens for PTSD, compared to those with negative PTSD screens.
RQ1: Do PTSD scores moderate the effect of the SST on employee positive emotions such that the intervention has a stronger (increasing) effect on positive emotions among veteran employees with negative screens for PTSD, compared to those with positive PTSD screens?
Method
Study design overview
Using a randomized controlled trial (RCT) design with 35 organizations where workplace was the unit of randomization, we examined the effects of a supervisor training and self-monitoring intervention on employee emotions at 6-months post-baseline (i.e., post-intervention), controlling for baseline emotions using daily diary data aggregated across two 32-day diary waves (see Figure 1). Daily diary data were collected as part of veteran couples’ study, which was developed as a multi-wave daily Internet study in which National Guard members, reservists, and separated (former) service members (termed veterans) and married or cohabiting partners (referred to as spouses) were invited to participate in a 32-day Internet survey at baseline and again 6 months later. The Daily Internet Study (DIS) was designed as a complementary study to the veteran employee study which developed and scientifically evaluated SST to enhance retention of veterans, with the goal of improving workplace culture and general well-being of veterans. At the start of the DIS study screening, veterans indicated their interest in participating in a couples’ study with their spouse or cohabiting partner (i.e., living together for 6+ months) by providing their spouse’s name and contact information. To be eligible to begin the DIS study, both veteran and spouse were required to consent and complete the baseline survey questionnaire. Veterans who completed at least 7 + daily surveys in the baseline DIS (along with spouses) were invited to participate in a second 32-day survey wave 6 months post-baseline, after the supervisor intervention. Although data were obtained from both members of each couple, the current study focuses only on veteran employees.
Figure 1.
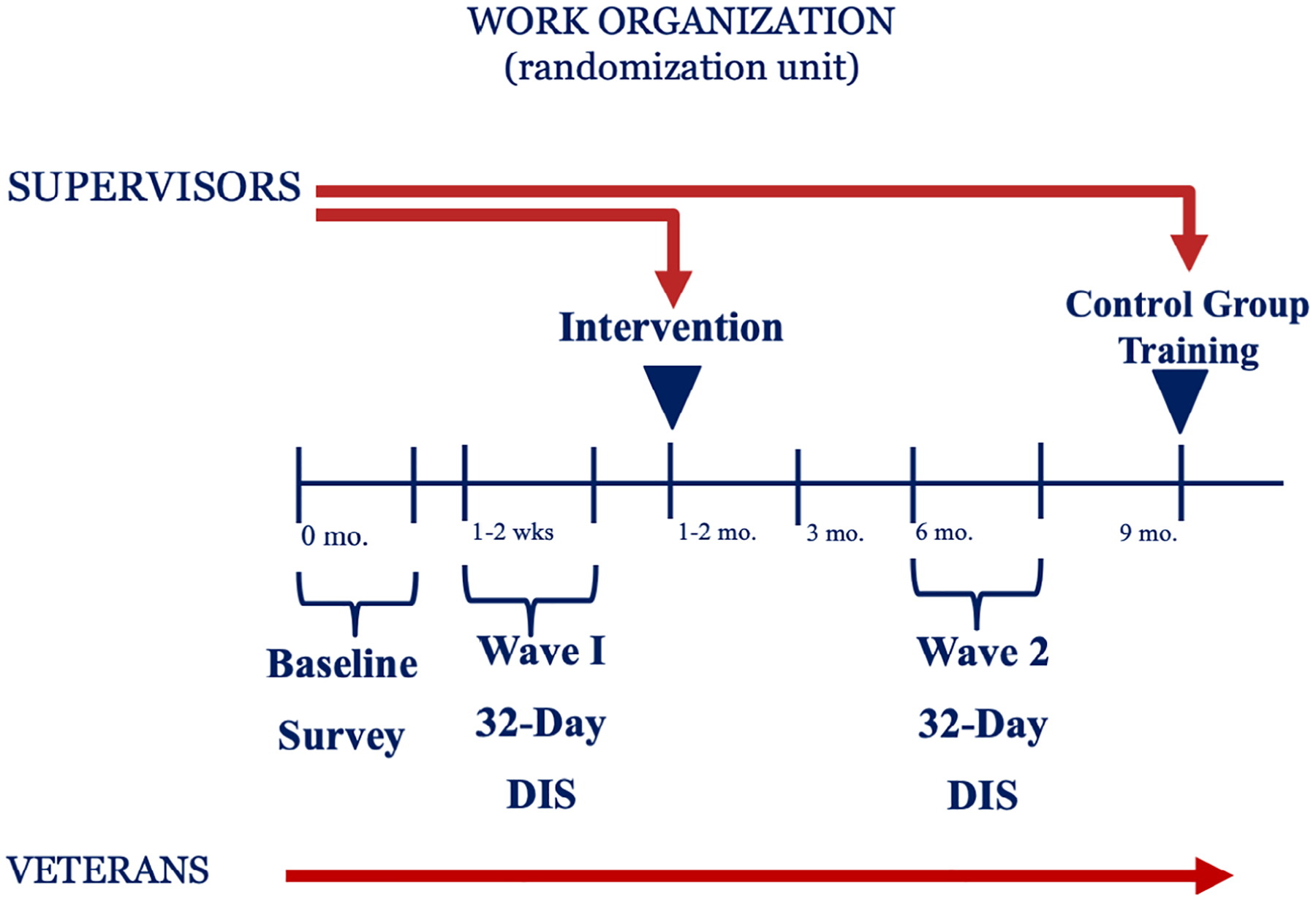
Intervention study protocol in which 35 workplace organizations were randomized to receive supervisor support intervention or wait-list control. DIS = Daily Internet Study.
Study recruitment was conducted through workplaces throughout the U.S. States of Oregon and Southwest Washington. Each organization was invited to participate in a randomized study of the supervisor intervention or wait-list control condition; veterans were recruited primarily through emails once the organization agreed to participate. Overall, 35 workplace organizations enrolled in the two-group RCT, with 19 randomized to the wait-list control condition and 16 randomized to the intervention. Eligibility requirements for the larger study included employment at least 20 hr/week at a participating organization and post-9/11 service in the U.S. military. Survey data were collected from veterans at baseline (pre-intervention) and then post-intervention at both 3 and 9 months following baseline. For a description of the baseline sample, as well as work, family, and health characteristics of the veterans involved in the larger study, see Hammer, Wan, Brockwood, Mohr, and Carlson (2017). All research activities in the current study were approved and overseen by [Portland State University’s] IRB, and the U.S. Army Medical Research and Materiel Command, Human Research Protection Office.
Participants
Of 509 veteran employee study participants, 395 were eligible for the DIS (i.e., were married or cohabiting), from which 191 veterans consented and enrolled. However, 16 of those veterans completed an early version of the DIS that did not include the survey items of interest in the current study, leaving a potential 175. An additional eight veterans were randomized but excluded from intervention analyses because they were either no longer at the participating organization or were considered supervisors. Thus, 167 veterans completed at least 1 day of the daily baseline survey and were potentially appropriate for inclusion in the intervention study. We were able to contact 161 veterans at 6-month follow-up of which 120 indicated interest in completing the follow-up survey; 116 completed at least one daily survey; 72% response rate. Of those, 11 were excluded as they were no longer at the participating organization or were considered supervisors. Participants were paid up to $90 in exchange for their participation in each daily diary wave based on number of completed surveys.
Consistent with daily process methodology practices, those with fewer than 5 completed surveys/days were deemed as having poor daily study compliance and removed from study analyses (e.g., Armeli, Conner, Todd, & Tennen, 2008). This resulted in an analysis sample of 144 participants (72 Intervention, 72 control) at baseline and 92 participants at 6-month follow-up (48 Intervention, 44 control). Comparing those who completed the DIS 6-month follow-up to those who completed only the baseline DIS revealed no significant differences in study variables. Demographically, those who completed the 6-month follow-up were similar to those who did not, with no differences in terms of gender, age, dependent children at home, work tenure, educational status, military status (active reservists vs. separated active duty), work shift (regular hours vs. alternate schedule), or work hours. To examine study attrition, we created a dichotomous variable differentiating study stayers (1) from study leavers (0), which was then regressed on baseline levels of outcome variables, individual differences/moderator variables, and treatment (see Goodman & Blum, 1996). Logistic regression analyses revealed no significant differences in completion status as a function of any study variable. Thus, we found no evidence that non-random sampling effects of subject attrition were responsible for our results in either set of analyses for emotions variables (ps range = .11 to .79), PTSD (p = .08) and treatment condition (p = .53). Finally, we compared baseline participants on whether they complied with the baseline daily survey using the Goodman and Blum (1996) procedures (i.e., 0 = non-compliant at 1–4 surveys vs. 1 = compliant); none of the variables we considered in logistic regression analysis were significant predictors of poor study compliance, including basic demographics such as gender, race, or employer type, PTSD symptoms and other individual difference items (e.g., personality), and military characteristics (length of deployment; ps range = .16 to .97).
The present study sample comprised 144 veterans (91% men) at baseline who were on average 38.4 years old (SD = 9.2) and mostly white (86%). The typical daily study male was married (89%) and in the relationship for on average 12 years (SD = 8.7); 7% completed high school, 26% completed some college, 47% graduated with a college degree, and 20% had started or completed graduate school. The majority were parents (77%), with 67% having at least one dependent child living in the home 3+ days per week. The majority were separated service members (84%), on average 5.9 years (SD = 3.4) post-separation, with 16% currently serving in active reserves. The typical DIS veteran was deployed at least once (89%), and 83% reported 1 + combat-related experience. Veterans worked on average 42.4 hr (SD = 6.4) per week, mostly in public sector organizations (66%). Mean job tenure was 5.9 years (SD = 5.8). Those veterans who consented to participate in the baseline DIS were not significantly different from married/partnered veterans who did not participate in the DIS in terms of PTSD symptoms (M = 1.88 vs. 1.90, respectively), p = .813. They were comparable on all other baseline individual difference indicators of well-being (e.g., loneliness, satisfaction with life, perceived stress). For more information about the veteran employee sample, please consult (Hammer et al., 2017; 2019).
Supportive supervisor (SST) intervention
The intervention comprised three components (Hammer et al., 2019): (1) 1-hr computer-based intervention to teach supportive behaviours in three modules: creating a culture of support for military (and non-military) employees, defining and identifying supportive supervisor behaviours in the areas of veteran and family support as well as performance support, and putting the supportive supervisor behaviours into practice; (2) 2-week behaviour-tracking exercise to practice enacting the supportive behaviours learned in the computer-based intervention. Supervisors set goals for the total number of behaviours they would enact in the 2-week tracking period and were reminded daily via email to track their behaviours. The tracking activity required about 5 min/day throughout the 2-week tracking period; and (3) the intervention included supplementary activities called ‘Above and Beyond’, providing additional information through three short intervention modules, as well as the opportunity for supervisors to engage in online discussion of the intervention and its material. Supervisors who participated in Above and Beyond activities received a higher level of certification than those who completed the core computer-based training intervention. Supervisors received the intervention through email links to the secure intervention page 1–2 months following the baseline survey and were given approximately 1 month to complete the intervention.
Measures and assessment procedures
Baseline surveys
Prior to the intervention, veteran participants were given approximately 2 weeks to complete an online survey of work-, family-, and health-related characteristics hosted through Qualtrics©2013. Informed consent was obtained from all participants prior to the start of data collection. Each participant received $25 in exchange for the baseline survey completion. In addition to demographic information of relevance to the present study, participants completed the following:
Post-traumatic stress disorder (PTSD)
We employed a four-item abbreviated version of the PTSD Checklist-Military Version (PCL-M; Bliese et al., 2008). Participants indicate how bothered they were over the previous 30 days by each symptom on a 5-point Likert-type scale. The instrument is designed to assess symptoms related to experiences while serving in the military and has been used in studies of service members (Cacioppo et al., 2016). Based on Bliese et al. (2008), the values for the four items are summed to create a symptom score; those indicating scores of 12 or higher were coded as having a positive screen for PTSD (scored as 1). All other participants received a negative for the screening (0). Note that positive scores from this measure should not be interpreted as a diagnosis but rather a greater likelihood that the individual is experiencing PTSD symptoms – and as a means for identifying those who may need early intervention (Bliese et al., 2008) and consequently derive the most benefit in terms of emotions from a supervisor intervention.
Daily internet study (DIS)
Each day for 32 (calendar) days veteran participants received an automatically generated email reminder including a unique link to the Internet survey at both baseline and 6 months later(Figure 1).The link was activated between the hours of 5 p.m. and 11 p.m.; participants were blocked from accessing the survey at other times. They were provided up to three missed surveys they could complete. This reporting window was selected to capture the transition from daytime activities (typically work) and beginning of evening activities; participants were encouraged to complete the survey at the end of the work-day. The approximately 10-min daily survey recorded a range of experiences including work, family, and child interactions, activities and stressors, daily emotions, and health behaviours.
Because the study comprised a broad range of work organizations, work schedules were highly varied with some employees working non-regular shifts (e.g., night shift, swing shift; 18%). In order to facilitate participation among all employed veterans, we created an alternate-shift survey timeframe, in which employees who chose this option responded to questions between 5 a.m. and 11 a.m. (consistently throughout the study).
Regarding study compliance, at baseline, the mean number of completed surveys was 25.2 (SD = 7.7), or 3634 out of a possible 4608 (32 surveys × 144 people) surveys was completed for a compliance rate of 78.9%. The follow-up analysis sample comprised 92 individuals who completed a mean of 27 (SD = 5.5) surveys, or 84.6% (2492/2944) of surveys.
Positive and negative emotion measures
Discrete emotion items were taken from the PANAS-X(extended Positive and Negative Affect Schedule; Watson, Clark, & Tellegen, 1988) and Larsen and Diener’s (1992) emotion circumplex model, classifying emotions as pleasant or unpleasant, high or low activation, or as a combination of these dimensions. Negative emotions included sad, angry, lonely, ashamed, and guilty. Positive emotion items included happy, active, quiet, and relaxed. For each emotion, participants rated the extent to which they felt this way right now on a scale of 1 (Not at all) to 5 (Extremely). Research has demonstrated that emotions can be reliability assessed with single items (e.g., Burisch, 1984; Myers & Diener, 1995), while offering advantages in terms of face validity and brevity, there by reducing participant fatigue (Larsen & Fredrickson, 1999). For the negative emotion composite score, we took the mean of negative emotion items for each day the participant completed at least 4 of 5 items. Similarly, for positive emotion items, we took the mean for days with at least three of the four emotion items completed.Day-level internal consistencies for the negative emotion summary scores ranged from α = .69 on day 3 to α = .81 on day 26; alphas for positive emotion summary scores ranged from α = .61 on day 3 to α = .76 on day 26. As a basis of comparison, reliability estimates averaged across days were of a similar magnitude (i.e., α = .79 and .82 for positive and α = .78 and .81 for negative emotions at baseline and 6 months, respectively).1
Data analysis
The study was designed as a two-condition cluster-randomized controlled trial (cRCT), in which workplace organizations were randomized to the SST intervention condition or wait-list control group. The intervention effects were evaluated using an intent-to-treat (ITT) approach whereby follow-up emotion reports from the DIS are compared for those in the supervisor intervention condition (Condition = 1) versus those in the control condition (Condition = 0). Although this approach is conservative, because it does not adjust for whether the supervisors actually received the intervention, it is considered the ‘gold standard’ as it affords the benefit of reducing biases, such as selection effects, that would potentially undermine or negate the benefit of the randomized controlled trial in terms of ruling out alternative explanations for findings (Little, Long, & Lin, 2009; see also McCoy, 2017 for further detail).
We employed a linear mixed model statistical approach using MPlus 8.4 (Muthén & Muthen, 1998–2017) to test for intervention effects with group randomized designs (e.g., Murray, 1998), which accounted for the nesting of employees within randomized workplace organizations by specifying that participants were clustered by employer. Baseline values for a given outcome measure were modelled as grand-mean centred covariates, based on Bodner and Bliese (2018) who advise analysis of covariance as the appropriate analysis method for testing intervention effects with power. We specified organization level as the between-cluster level and employee level as the within-cluster level to account for the nesting of employees within organizations. This approach adjusts the model parameters and their standard errors accounting for the degree of nonindependence of employee observations within organizations.
There were no significant differences between control and treatment condition participants at baseline as a function of condition, according to a series of one-way ANOVAs. The observed number of positive PTSD screens was not significantly different from expected as a function of condition, Χ2 (1) = 2.97, p = .085, with 8.3% positive screens in the control and 18.1% in the intervention condition. Likewise, the number of PTSD symptoms upon which the screen is scored were not significantly different (M = 7.17 vs. 8.00, for control vs. intervention) at F (1, 142) = 1.53, p = .213. Given this lack of findings, and Spector and Brannick’s (2011) caution against overinclusion of control variables, and when strong theoretical justification is absent (Bernerth & Aguinis, 2016), we did not include additional covariates in our models.2 The analysis sample size for the linear mixed models was 92 (44 Intervention/48 Control). Descriptive statistics for study variables at baseline and follow-up are presented in Table 1.
Table 1.
Descriptive statistics for variables at DIS baseline and follow-up by condition
| Variable | Control condition | Training condition | ||
|---|---|---|---|---|
| Baseline n = 72 M (SD) |
Follow-up n = 48 M (SD) |
Baseline n = 72 M (SD) |
Follow-up n = 44 M (SD) |
|
| PTSD screening | 0.08 (0.28) | – | 0.18 (0.39) | – |
| Negative emotion composite | 1.40 (0.22) | 1.39 (0.28) | 1.43 (0.22) | 1.40 (0.26) |
| Positive emotion composite | 2.52 (0.67) | 2.38 (0.52) | 2.48 (0.72) | 2.47 (0.71) |
| Happy | 2.95 (0.80) | 2.88 (0.83) | 2.82 (0.79) | 2.85 (0.93) |
| Active | 1.57 (0.55) | 1.60 (0.55) | 1.68 (0.73) | 1.71 (0.82) |
| Relaxed | 2.78 (0.68) | 2.68 (0.75) | 2.72 (0.73) | 2.78 (0.82) |
| Quiet | 2.58 (0.74) | 2.35 (0.64) | 2.59 (0.65) | 2.55 (0.79) |
| Sad | 1.21 (0.28) | 1.23 (0.38) | 1.28 (0.46) | 1.22 (0.40) |
| Lonely | 1.22 (0.41) | 1.26 (0.52) | 1.26 (0.39) | 1.25 (0.46) |
| Angry | 1.24 (0.35) | 1.30 (0.56) | 1.25 (0.50) | 1.23 (0.47) |
| Guilty | 1.11 (0.22) | 1.13 (0.27) | 1.10 (0.21) | 1.09 (0.22) |
| Ashamed | 1.06 (0.12) | 1.08 (0.22) | 1.09 (0.19) | 1.08 (0.22) |
Note. Follow-up data were collected 6 months after baseline. For the PTSD screening variable, 0 = negative and 1 = positive PTSD screen.
Results
Tests of intervention effects
There were no significant intervention effects observed in composite positive emotions (Table 2), nor for activated positive emotions (happy, active). However, for unactivated positive emotions, the intervention effect on relaxed at 6 months was significantly positive (b = .05, SE = .01, 95% CI [0.03, 0.08], p < .001, pseudo ΔR2 < .01). Similarly, the intervention effect on quiet at 6 months was significantly positive (b = .11, SE = .01, 95% CI [0.09, 0.14], p < .001, pseudo ΔR2 = .015).
Table 2.
Model results of intervention effects on positive emotions at 6-month follow-up
| DV: Composite Positive Est. (95% CI) |
DV: Activated | DV: Unactivated | |||
|---|---|---|---|---|---|
| Happy Est. (95% CI) |
Active Est. (95% CI) |
Relaxed Est. (95% CI) |
Quiet Est. (95% CI) |
||
| Intercept | 2.34*** (2.27, 2.42) | 2.80*** (2.73, 2.86) | 1.65*** (1.50, 1.80) | 2.66*** (2.59, 2.73) | 2.44*** (2.30, 2.58) |
| Intervention | .09 (−0.02, 0.20) | .04 (−0.08, 0.16) | −.10 (−0.37, 0.17) | .05*** (0.03, 0.08) | .11*** (0.09, 0.14) |
| Baseline of DV | .68*** (0.57, 0.79) | .95*** (0.85, 1.04) | .81*** (0.67, 0.96) | .94*** (0.84, 1.04) | .79*** (0.60, 0.97) |
| Residual variance | .13*** (0.11,0.16) | .17*** (0.13, 0.21) | .14** (0.05,0.22) | .12*** (0.09, 0.14) | .20*** (0.14, 0.26) |
| Intercept variance | .00 (−0.003, 0.003) | .00 (−0.003, 0.003) | .01 (−0.05,0.08) | .00 (−0.06, 0.06) | .00 (−0.06, 0.06) |
| Model R2 (within cluster/org.) | .65*** | .78*** | .70*** | .81*** | .61*** |
| Model R2 (between clusters/orgs.) | .94 | .67 | .16 | .84 | .88 |
Note.DV = Dependent variable. Models controlled for baseline levels of outcome variable. All estimates listed represent unstandardized values. For the intervention variable, 1 = intervention condition and 0 = control condition. Intercept variances represent variability in the outcome variables due to the clustering of employees in the randomized organizations. All continuous predictors and the PTSD predictor are grand-mean centred. For the centred PTSD screening variable, −.13 = negative and .87 = positive PTSD screen. Ns = 92.
p < .05;
p < .01;
p < .001.
Next, analyses revealed no significant effects for negative emotion items (Table 3). Thus, Hypothesis 1 was partially supported, wherein the SST intervention had a significant effect on improving veteran employees’ unactivated positive emotions 6 months post-intervention.
Table 3.
Model results of intervention effects on negative emotions at 6-month follow-up
| DV: Composite Negative Est. (95% CI) |
DV: Activated | DV: Unactivated | ||||
|---|---|---|---|---|---|---|
| Angry Est. (95% CI) |
Ashamed Est. (95% CI) |
Guilty Est. (95% CI) |
Sad Est. (95% CI) |
Lonely Est. (95% CI) |
||
| Intercept | 1.41*** (1.35, 1.47) | 1.30*** (1.13, 1.46) | 1.09*** (1.05, 1.13) | l.l 1*** (1.06, 1.17) | 1.24*** (1.17, 1.30) | 1.29*** (1.01, 1.57) |
| Intervention | −.01 (−0.09,0.07) | −.09 (−0.25, 0.08) | −.01 (−0.08,0.06) | −.01 (−0.002,0.003) | −.02 (−0.15,0.10) | −.04 (−0.51, 0.43) |
| Baseline of DV | .77*** (0.51, 1.04) | .84*** (0.55, 1.13) | .57** (0.19, 0.95) | .59*** (0.38, 0.80) | .67*** (0.50, 0.85) | .80*** (0.56, 1.04) |
| Residual variance | .04** (0.02,0.07) | .11*** (0.06,0.16) | .04** (0.01,0.06) | .04** (0.01,0.07) | .09** (0.03, 0.14) | .14* (0.010, 0.28) |
| Intercept variance | .00 (−0.01, 0.01) | .00 (−0.14, 0.14) | .00 (−0.02, 0.02) | .00 (−0.002, 0.003) | .00 (−0.01,0.01) | .00 (−0.19,0.19) |
| Model R2 (within cluster/org.) | .43*** | .59*** | .18* | .31** | .43*** | .39** |
| Model R2 (between clusters/orgs.) | .23 | .95 | .49 | .13 | .52 | .60 |
Note.DV = Dependent variable. Models controlled for baseline levels of outcome variable. All estimates listed represent unstandardized values. For the intervention variable, 1 = intervention condition and 0 = control condition. Intercept variances represent variability in the outcome variables due to the clustering of employees in the randomized organizations. All continuous predictors and the PTSD predictor are grand-mean centred. For the centred PTSD screening variable, −.13 = negative and .87 = positive PTSD screen. Ns = 92.
p < .05;
p < .01;
p < .001.
Moderated intervention effects
Consistent with Hypothesis 2, our analyses revealed a significant moderation effect (PTSD x Intervention) predicting composite 6-month negative emotion (b = −.43, SE = .08, p < .001, pseudo ΔR2 = .10), as shown in Table 4. The specific form of the interaction is depicted in Figure 2. Simple slope tests revealed a significant effect of the intervention on negative emotion for those above the positive screening cutoff for PTSD (b = −.17, SE = .07, p = .016). There was no significant influence of the intervention on negative emotions for those below the PTSD cutoff (b = .13, SE = .19, p = .49).3
Table 4.
Model results of intervention effects on mean emotions
| DV: Negative emotion (6-month) w/ Moderator | DV: Positive Emotion (6-month) w/ Moderator | |||
|---|---|---|---|---|
| Est. | 95% CI | Est. | 95% CI | |
| Intercept | 1.42*** | (1.36, 1.49) | 2.35*** | (2.28, 2.42) |
| Intervention | −.02 | (−0.17, 0.12) | .08 | (−0.01,0.17) |
| Baseline of DV | 72*** | (0.56, 0.89) | .68*** | (0.57, 0.78) |
| PTSD | .33* | (0.02, 0.64) | .12 | (−0.05, 0.29) |
| Intervention × PTSD | −.43*** | (−0.59, −0.27) | −.42** | (−0.72, −0.12) |
| Residual variance | .04** | (0.02, 0.06) | .13*** | (0.11,0.15) |
| Intercept variance | .00 | (−0.04, 0.04) | .00 | (−0.002, 0.003) |
| Model R2 (within cluster or organization) | .49*** | .67*** | ||
| Model R2 (between clusters or organizations) | .76 | .95 | ||
Note. DV = Dependent variable. Models controlled for baseline levels of outcome variable. All estimates listed represent unstandardized values. For the intervention variable, 1 = intervention condition and 0 = control condition. Intercept variances represent variability in the outcome variables due to the clustering of employees in the randomized organizations. All continuous predictors and the PTSD predictor are grand-mean centred. For the centred PTSD screening variable, −.13 = negative and .87 = positive PTSD screen. Ns = 92.
p < .05;
p < .01;
p < .001.
Figure 2.
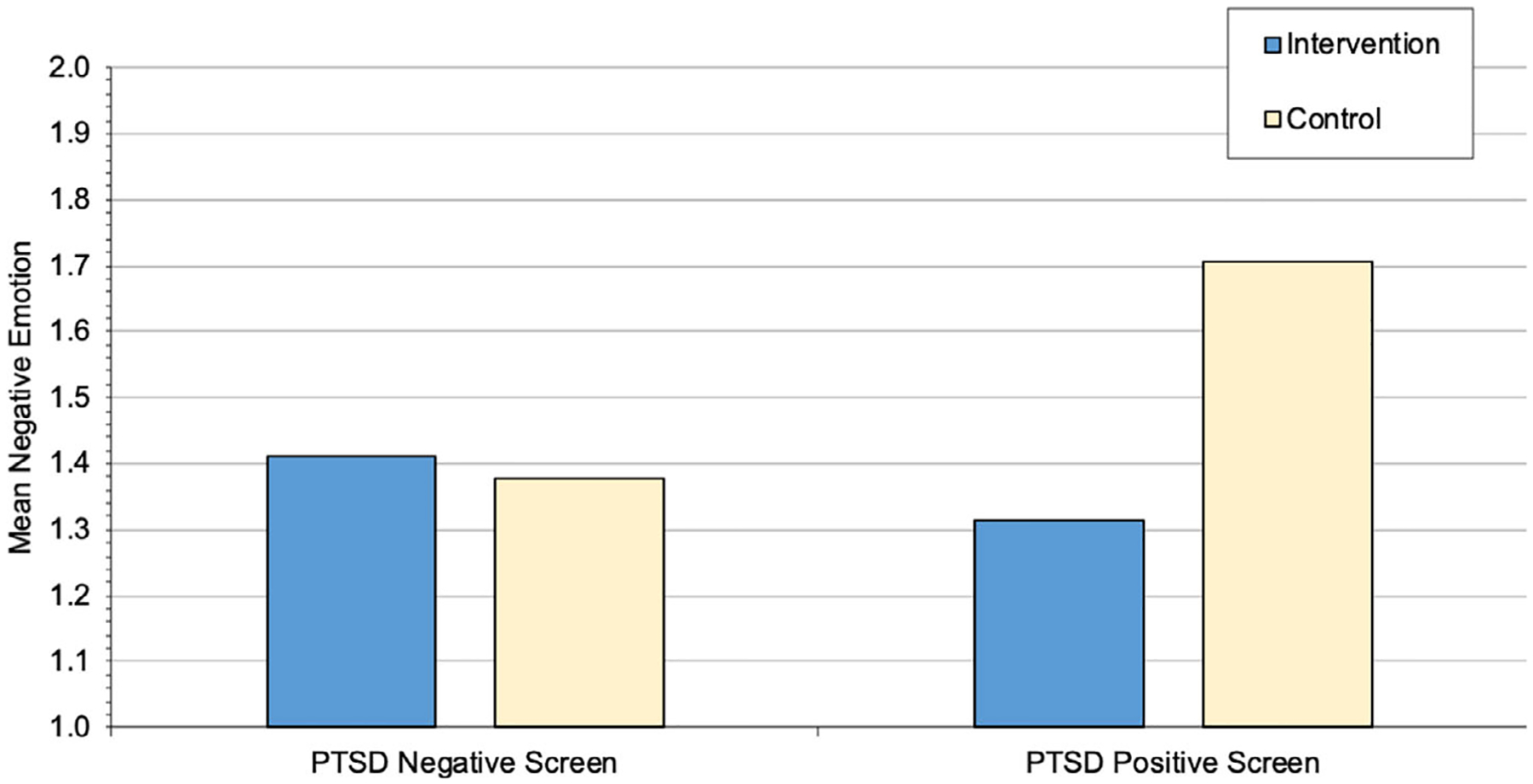
Interaction between condition and PTSD screening on composite negative emotions at 6 months. Intervention = Intervention condition; Control = wait-list control condition.
To address Research Question 1, we tested the moderation effect of PTSD screening on 6-month positive emotions (Table 4), revealing a significant effect (b = −.42, SE = .15, p = .006, pseudo ΔR2= .038), as depicted in Figure 3. Simple slope tests revealed that for those with a positive PTSD screen, there was no significant effect of the intervention on positive emotion (b = −.27, SE = .18, p = .128). For those who did not screen positive for PTSD, the intervention significantly increased positive emotion (b = .15, SE = .06, p = .010).
Figure 3.
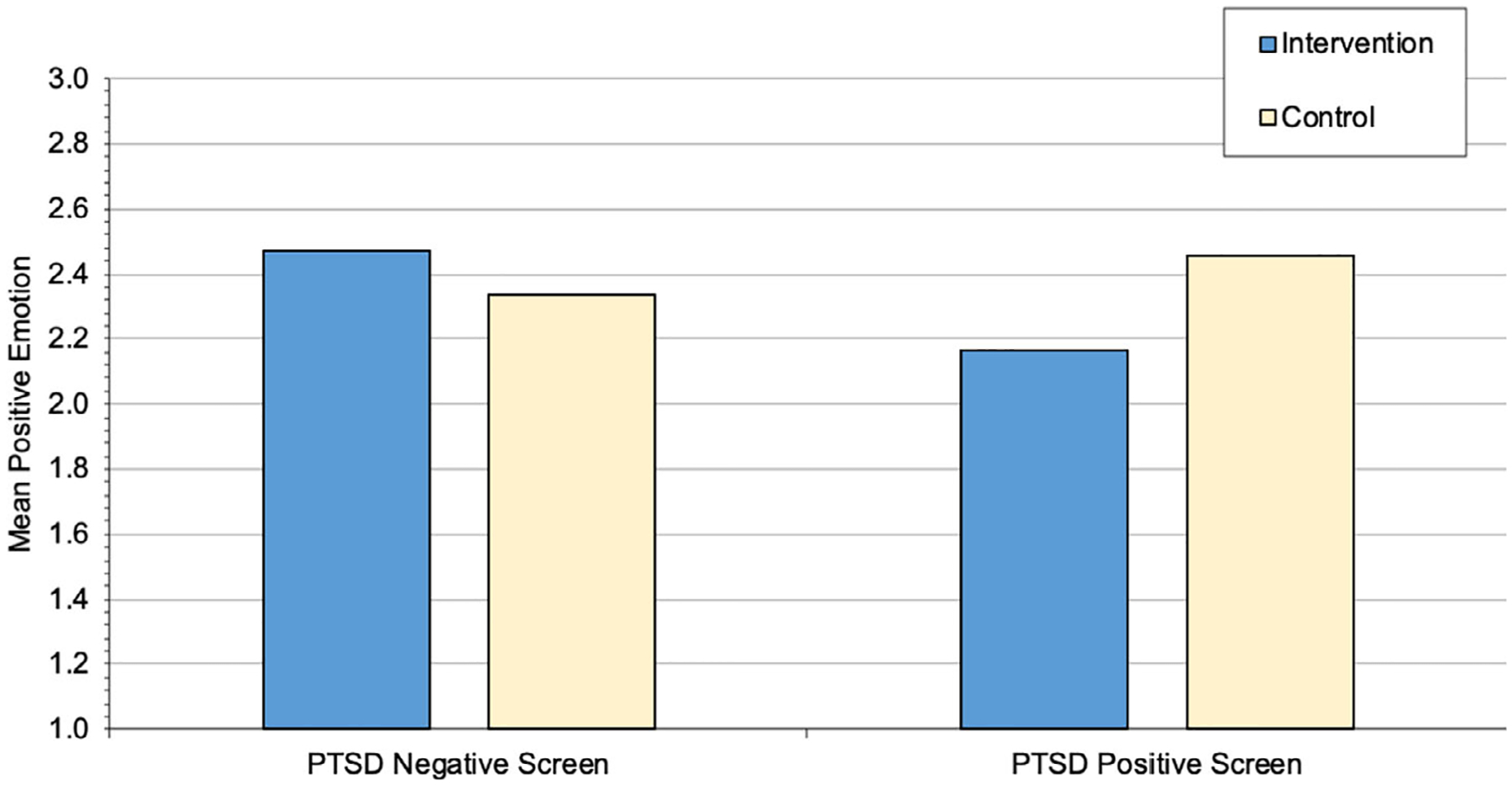
Interaction between condition and PTSD screening on composite positive emotions at 6 months. Intervention = Intervention condition; Control = wait-list control condition.
Discussion
This study affirms the importance of workplace supervisor support provision to boost veteran affective experiences. The study contributes to workplace positive psychology intervention research by considering the effect of an SST on employees’ well-being in the form of daily emotions, which can shed light on positive shifts in one’s emotions in the immediate periods pre- to post-supervisor support intervention. Such information is qualitatively different from the information gleaned from global assessments of well-being (e.g., Newman et al., 2020). This study extends evidence on the effectiveness of SST to the domain of veteran emotional well-being as they transition into and thrive in the civilian workplace.
The SST intervention was demonstrated to have a significant effect on facets of emotional well-being. Although there were no direct effects of the intervention on composite positive and negative emotion averages across the 32-day diaries, pre- and post-intervention, the intervention improved relaxed and quiet emotions, whereby veterans in the intervention condition reported significantly higher 6-month relaxed and quiet emotions than those in the control condition, which represents greater calmness or ‘serenity’ (Watson et al., 1988) or lower arousal (e.g., Feldman, 1995). An inspection of condition means suggests the intervention may have stabilized or increased those emotions for intervention condition veterans (relative to the control condition which appeared to show decrements over time). The significant moderating effect of positive PTSD screening suggests that the intervention improved composite positive emotion at 6 months among those who were screened as PTSD negative (i.e., most participants). For those screened positive for PTSD, results suggest the intervention was effective at reducing composite negative emotion at 6-month follow-up. Because of the small sample of PTSD-positive participants, these results should be interpreted with caution.
Our results revealed the insight gleaned from studying discrete emotions, whereby the supervisor intervention was effective for all veterans in promoting calm and quiet emotions, but not necessarily the more activated positive emotions such as happy emotion. Such findings may have important health outcomes, given meta-analysis reports showing that unactivated positive emotion induction (e.g., calm, relaxed) was related to improved immune and neuroendocrine functioning (Pressman & Cohen, 2005). There is also evidence of work performance-related outcomes, whereby Bissing-Olson, Iyer, Fielding, and Zacher (2013) found that unactivated emotions (i.e., calm, relaxed and content) were uniquely linked to a greater likelihood that employees engaged in work tasks in an environmentally friendly way.
Composite positive emotion, which includes activated positive emotions like happy, was increased among veterans who did not screen positive for PTSD (i.e., most veterans). According to Seo, Barrett, and Bartunek (2004), positive affect is associated with greater focus on goal attainment, generativity, and intensity and persistence towards goal attainment. Seo et al. also argue that activated, but not deactivated (unactivated) affect enhances effort, though they do not differentiate deactivated positive (e.g., relaxed) from negative (e.g., lonely, bored), which our results indicate would be important. We encourage future work on the influence of employee emotional well-being, in terms of activated and unactivated positive and negative emotions and work-related outcomes. Researchers may also consider differentiating emotions at work from emotions at home (e.g., Sonnentag & Grant, 2012) to better capture affective experiences in work and non-work (family) domains.
For veterans who screened positive for PTSD, SST was associated with a reduction in negative emotions, but activated positive emotions like happiness did not increase. These results need to be replicated with a larger sample of veterans with positive PTSD screens before conclusions can be drawn. A preliminary interpretation could suggest a particular challenge for them in fully enjoying the benefits of the supervisor intervention – potentially due to consequences of PTSD, which impairs the ability to enjoy positive experiences (APA, 2013). Conversely, our intervention did not reduce negative emotions, except for among the PTSD-positive-screening veterans. Given that individuals who experience PTSD are more likely to have stronger associations with negative affect (e.g., downward spirals of emotions; for overview see Garland et al., 2010), this finding may indicate that those downward spirals were weakened by the SST. This outcome is consistent with the negativity buffering model of social support (Bavik et al., 2020), in which veterans with positive PTSD screens may benefit from enhanced supervisor support resulting in a reduction of negative emotions. Veterans without PTSD experienced lower rates of negative emotions in our study (e.g., mean negative emotion ranged from 1.39 to 1.43 depending on condition, on a 1-to-5 scale), as with other non-clinical populations (e.g., Crawford & Henry, 2004), wherein negative emotion may be too low to necessitate intervention.
Observed increases in positive emotions resulting from the SST are consistent with the positivity catalyst role of social support (Bavik et al., 2020), in which support leads to generation of resources. Theoretically, the positive emotions engendered by the intervention may reflect improved relationships with the supervisor, which should lead to positive employee behaviour (e.g., employee engagement) via reciprocity (Bavik et al., 2020). Accordingly, positive emotions as a component of employee well-being are fundamental to employee engagement (Robertson & Cooper, 2010). The intervention was also designed to alleviate or buffer employee stress, described as a negativity buffer (Bavik et al., 2020). To probe further, future work should examine how supervisor social support influences responses to employee stress in daily work interactions, for example as described in the JD-R model (Demerouti et al., 2001). As employees perceive stressor demands exceeding capacity or resources, supervisor support should enhance resources or offset demands to alleviate stress. Future work should also consider the potential for supervisor support to alter the appraisal of a potential stressor, intervening early in the stress response, which would also be consistent with stress and negativity buffering models. This study presents a methodological contribution to the literature by demonstrating the value of daily diary methods to capture ecological momentary emotion assessments before and after the intervention to facilitate the assessment of intervention effectiveness. The combination of multi-wave daily assessment and RCTs is rare. Although the length of time between daily diary intervals (6 months) might seem too long to detect intervention effects, other non-daily intervention analyses emerging from our larger study reveal that effects not present at a 3-month interval were significant at 9-month follow-up (Hammer et al., 2019). As static surveys, the 3- and 9-month surveys were not designed to measure the everyday emotions captured in the 6-month daily diaries. The 6-month daily diary, then, may have captured an emerging effect on emotions of the SST that was building over time. One potential explanation for the delayed treatment effect is that supervisors need time to practice in order to provide effective support.
Our study was robust in the length of the daily surveys, spanning up to 32 days of reports in each wave for a total of 64 possible reports. Daily diaries are particularly useful in measuring the ebb and flow of emotions as they occur while minimizing concerns about retrospective bias (e.g., Newman et al., 2020; Reis & Gable, 2000). Our approach provides a solid foundation for launching more complex and sophisticated inquiries into employee emotional experiences. We look forward to future work examining more complex within-person changes over time as a function of the intervention, modelling processes specified by positivity catalyst and negativity buffer models (Bavik et al., 2020).
Limitations
Despite study strengths, there are limitations that warrant discussion. First, the DIS recruited married/cohabiting veterans, but not single veterans. As such, our results may not generalize to single veterans or reservists. Most of our larger veteran study participants were married (70.6%), as are the majority of service members more generally. We also note that our sample of veteran employees may not generalize to the larger employee population, but may extend to other underserved populations of employees. The SST was based on general social support theory; similar workplace social support interventions have shown positive benefits to employee well-being (e.g., Kossek et al., 2019). Support provisions are especially important to employees from disadvantaged groups, who face unique demands and stressors (Bavik et al., 2020) – our findings may be particularly relevant to those employee groups. Intervention effectiveness may also be dependent on existing programmes in place; organizations that are familiar with supporting veterans in the workplace may achieve higher SST benefits.
Despite efforts to recruit as many supervisors as possible, not all supervisors participated in the intervention, and supervisors and employees were recruited separately, limiting the ability to match supervisors and employees. If all supervisors received the intervention, the potential for detecting intervention effects would be magnified. Yet, examining whether the intervention is effective when followed as prescribed (i.e., treatment efficacy; Little et al., 2009; or treatment on the treated; Shadish & Cook, 2009) comes with a distinct downside in that the estimates can contain selection bias. The intent-to-treat (ITT) approach we employed is considered the gold standard in preserving the benefits of randomization and is also the preferred approach in many cases, because it facilitates policy-making or dissemination effort (Shadish & Cook, 2009). Namely, when informing policy, those implementing the recommended training frequently cannot guarantee adherence or require people to complete the training, and thus, ITT provides the most realistic assessment of effectiveness.
Practical implications
Our results provide compelling evidence that supervisors’ supportive behaviours and interactions with veteran employees can make a significant difference in improving employee emotional well-being, which in turn can have significant positive effects on their workplace behaviour and attitudes (Cropanzano, Dasborough, & Weiss, 2017; Weiss & Cropanzano, 1996). These intervention benefits potentially generalize beyond veteran employees to the broader workforce because the intervention was worksite-based in that all supervisors were encouraged to participate and it included more general aspects of FSSB training in addition to veteran-specific support. The SST represents an evidence-based programme that improves employee calm emotions by enhancing supervisor support for veterans. We see significant value in providing this vehicle for enhancing support for veterans in the civilian workforce and believe this should go hand-in-hand with veteran hiring initiatives.
Our findings regarding employees who screen positive for PTSD point to potential benefits of supervisor support for individuals who may have clinically significant mental health challenges. Dimoff and Kelloway (2019) recently demonstrated the effectiveness of a supervisor training focused on mental health awareness, which improved employees’ willingness to seek out and use mental health resources. Thus, training supervisors to support veterans may also improve psychological resources, leading to improved veteran emotional well-being, especially for those in need. Veterans who screened PTSD-positive may have uniquely benefitted from the intervention in terms of reduction of negative emotions, though the small sample size in our study necessitates additional replication. This finding is comparable to other moderation results that have been documented with a similar supportive supervisor intervention focused on family support to reduce work–family conflict, whereby the intervention was effective for those who particularly needed it – those with higher work–family conflict (Hammer et al., 2011). These results complement our findings from the broader study that included all of the veterans who completed the baseline survey (Hammer et al., 2019). Using ITT analyses the intervention was found to improve work and health outcomes for those employees who reported higher levels of supervisor and coworker support at baseline. Thus, while the daily diary study provided us with a more accurate assessment of positive and negative emotions before and after the supervisor intervention, with less retrospective bias than is present in global affect assessments, the larger study demonstrated the workplace contextual factors that were important for examining the broader stress– and strain–outcome relationship.
Conclusion
In combining the benefits of an RCT testing supervisor effectiveness with multi-wave daily diary reports, this study forged new methodological contributions to the testing of supervisor support training, while also providing substantive contributions to the literature in demonstrating the importance of workplace supervisor support to employee well-being. Our work highlighted the benefit of workplace supervisor support interventions in improving veteran employee emotions, including among those who screen positive for an affect-related disorder (i.e., PTSD). Our results underscore the importance of considering momentary emotion averages taken from daily emotion reports, in order to detect intervention effects, providing a practical method for improving the well-being of veteran employees, who are usually underserved.
Practitioner points.
Our supervisor support training represents an evidence-based programme that improves employee positive emotions.
Positive emotions were increased among veterans who did not screen positive for PTSD (i.e., most veterans).
Veterans with positive PTSD screens may benefit from enhanced supervisor support resulting in a reduction of negative emotions, providing supportive evidence for supervisor mental health awareness training.
Acknowledgements
The U.S. Army Medical Research Acquisition Activity, 820 Chandler Street, Fort Detrick MD 21702-5014 is the awarding and administering acquisition office. This work was supported by the Office of the Assistant Secretary of Defense for Health Affairs, through the USAMRMC Broad Agency Announcement under Award No. W81XWH-13-2-0020. Portions of this research were supported by the Grant # T03OH008435. Opinions, interpretations, conclusions and recommendations are those of the author and are not necessarily endorsed by the Department of Defense. Special thanks to Luke Mahoney, Sheila Umemoto, Philip Bouleh, and AnnaMarie O’Neill for their assistance with the paper.
Footnotes
Conflicts of interest
All authors declare no conflict of interest.
Multilevel reliabilities were also estimated using the multilevel reliability analysis function in the psych package created for R (Revelle, 2020), in which the average of emotion measures (by valence) is taken over K fixed days (Cranford et al., 2006; see Equation 4, p. 925), with resulting values of RKF = .99 (both baseline & follow-up) for positive emotion and RKF = .98 and .99 (baseline & follow-up, respectively) for negative emotion.
We examined General Supervisor Support (GSS; Yoon & Lim, 1999) as a control variable in hypothesized models. GSS was not a significant predictor of emotion outcomes in our models; including GSS did not change study findings.
Test of moderation effects was re-estimated using the continuous PTSD symptom measure. Interaction effects were statistically significant for both positive and negative emotions. Simple slope tests (estimating effects at±1 SD on PTSD) were largely similar, except that for those 1 SD higher on PTSD, the intervention effect on negative emotion was marginal (b = −.08, SE = .05, p = .09).
Data availability statement
The data utilized in the current study are available from the second author upon reasonable request.
References
- Ainspan ND, Penk W, & Kearney LK (2018). Psychosocial approaches to improving the military-to-civilian transition process. Psychological Services, 15, 129–134. 10.1037/ser0000259 [DOI] [PubMed] [Google Scholar]
- Almeida DM, Davis KD, Lee S, Lawson KM, Walter KN, & Moen P (2016). Supervisor support buffers daily psychological and physiological reactivity to work-to-family conflict. Journal of Marriage and Family, 78, 165–179. 10.1111/jomf.12252 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amdur RL, Larsen R, & Liberzon I (2000). Emotional processing in combat-related posttraumatic stress disorder: A comparison with traumatized and normal controls. Journal of Anxiety Disorders, 14, 219–238. 10.1016/S0887-6185(99)00035-3 [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association (APA) (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author. [Google Scholar]
- Armeli S, Conner T, Todd M, & Tennen H (2008). Mean levels and yearly changes in coping and enhancement motives as moderators of the negative affect-drinking association among college students. Alcoholism-Clinical and Experimental Research, 69, 313–322. 10.15288/jsad.2008.69.313 [DOI] [Google Scholar]
- Bavik YL, Shaw JD, & Wang XH (2020). Social support: Multi-disciplinary review, synthesis, and future agenda. Academy of Management Annals, 14, 726–758. 10.5465/annals.2016.0148 [DOI] [Google Scholar]
- Beedie C, Terry P, & Lane A (2005). Distinctions between emotion and mood. Cognition & Emotion, 19, 847–878. 10.1080/02699930541000057 [DOI] [Google Scholar]
- Bernerth JB, & Aguinis H (2016). Acritical review and best-practice recommendations for control variable usage. Personnel Psychology, 69, 229–283. 10.1111/peps.12103 [DOI] [Google Scholar]
- Bissing-Olson MJ, Iyer A, Fielding KS, & Zacher H (2013). Relationships between daily affect and pro-environmental behavior at work: The moderating role of pro-environmental attitude. Journal of Organizational Behavior, 34, 156–175. 10.1002/job.1788 [DOI] [Google Scholar]
- Blau PM(1964). Justice in social exchange. Sociological Inquiry,34,193–206. 10.1111/j.1475-682X.1964.tb00583.x [DOI] [Google Scholar]
- Bliese PD, Adler AB, & Castro CA (2011). Research-based preventive mental health care strategies in the military. In Adler AB, Bliese PD & Castro CA (Eds.), Deployment psychology: Evidence-based strategies to promote mental health in the military (pp. 103–124). Washington, DC: American Psychological Association. 10.1037/12300004 [DOI] [Google Scholar]
- Bliese PD, Wright KM, Adler AB, Cabrera O, Castro CA, & Hoge CW (2008). Validating the primary care posttraumatic stress disorder screen and the posttraumatic stress disorder checklist with soldiers returning from combat. Journal of Consulting and Clinical Psychology, 76, 272–281. 10.1037/0022-006X.76.2.272 [DOI] [PubMed] [Google Scholar]
- Bodner T, & Bliese P (2018). Detecting and differentiating the direction of change and intervention effects in randomized trials. The Journal of Applied Psychology, 103, 37–53. 10.1037/apl0000251 [DOI] [PubMed] [Google Scholar]
- Bolger N, DeLongis A, Kessler RC, & Schilling EA (1989). Effects of daily stress on negative mood. Journal of Personality and Social Psychology, 57, 808–818. 10.1037/0022-3514.57.5.808 [DOI] [PubMed] [Google Scholar]
- Britt T, Black K, Cheung J, Pury C, & Zinzow H (2018). Unit training to increase support for military personnel with mental health problems. Work & Stress, 32, 281–296. 10.1080/02678373.2018.1445671 [DOI] [Google Scholar]
- Bureau of Labor Statistics. (2020). Employment situation of veterans–2019. https://www.bls.gov/news.release/pdf/vet.pdf.
- Burisch M (1984). You don’t always get what you pay for: Measuring depression with short and simple versus long and sophisticated scales. Journal of Research in Personality, 18(1), 81–98. 10.1016/0092-6566(84)90040-0 [DOI] [Google Scholar]
- Cacioppo JT, Cacioppo S, Adler AB, Lester PB, McGurk D, Thomas JL, & Chen HY (2016). The cultural context of loneliness: Risk factors in active duty soldiers. Journal of Social and Clinical Psychology, 35, 865–882. 10.1521/jscp.2016.35.10.865 [DOI] [Google Scholar]
- Cohen S, & Wills T (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98, 310–357. 10.1037/0033-2909.98.2.310 [DOI] [PubMed] [Google Scholar]
- Cole MS, Bruch H, & Vogel B (2006). Emotion as mediators of the relations between perceived supervisor support and psychological hardiness on employee cynicism. Journal of Organizational Behavior: The International Journal of Industrial, Occupational and Organizational Psychology and Behavior, 27, 463–484. 10.1002/job.381 [DOI] [Google Scholar]
- Colella A, Hebl M, & King E (2017). One hundred years of discrimination research in the Journal of Applied Psychology: A sobering synopsis. Journal of Applied Psychology, 102, 500–513. 10.1037/apl0000084 [DOI] [PubMed] [Google Scholar]
- Crain TL, Hammer LB, Bodner T, Olson R, Kossek EE, Moen P, & Buxton OM (2019). Sustaining sleep: Results from the randomized controlled Work, Family, and Health Study. Journal of Occupational Health Psychology, 24, 180–197. 10.1037/ocp0000122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crain T, & Stevens S (2018). Family-supportive supervisor behaviors: A review and recommendations for research and practice. Journal of Organizational Behavior, 39, 869–888. 10.1002/job.2320 [DOI] [Google Scholar]
- Cranford JA, Shrout PE, Iida M, Rafaeli E, Yip T, & Bolger N (2006). A procedure for evaluating sensitivity to within-person change: Can mood measures in diary studies detect change reliably? Personality and Social Psychology Bulletin, 32, 917–929. 10.1177/0146167206287721 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crawford JR, & Henry JD (2004). The Positive and Negative Affect Schedule (PANAS): Construct validity, measurement properties and normative data in a large non-clinical sample. British Journal of Clinical Psychology, 43, 245–265. 10.1348/0144665031752934 [DOI] [PubMed] [Google Scholar]
- Cropanzano R, Dasborough MT, & Weiss HM (2017). Affective events and the development of leader-member exchange. Academy of Management Review, 42, 233–258. 10.5465/amr.2014.0384 [DOI] [Google Scholar]
- Cutrona CE (1989). Ratings of social support by adolescents and adult informants: Degree of correspondence and prediction of depressive symptoms. Journal of Personality and Social Psychology, 57, 723–730. 10.1037/0022-3514.57.4.723 [DOI] [PubMed] [Google Scholar]
- Davidson RJ (1994). How are emotions distinguished from moods, temperament, and other related affective constructs? In Ekman P & Davidson RJ (Eds.), The nature of emotion: Fundamental questions. Series in affective science (pp. 49–96). New York, NY: Oxford University Press. [Google Scholar]
- Demerouti E, Bakker AB, Nachreiner F, & Schaufeli WB (2001). The job demands-resources model of burnout. Journal of Applied Psychology, 86, 499–512. 10.1037/00219010.86.3.499 [DOI] [PubMed] [Google Scholar]
- Diener E (2000). Subjective well-being: The science of happiness and a proposal for a national index. American Psychologist, 55, 34–43. 10.1037/0003-066X.55.1.34 [DOI] [PubMed] [Google Scholar]
- Diener E (2009). Assessing subjective well-being: Progress and opportunities. In Diener E (Ed.), Assessing well-being. Social indicators research series, Vol. 39 (pp. 25–65). Dordrecht: Springer. [Google Scholar]
- Diener E, & Emmons RA (1984). The independence of positive and negative affect. Journal of Personality and Social Psychology, 47, 1105–1117. 10.1037/0022-3514.47.5.1105 [DOI] [PubMed] [Google Scholar]
- Diener E, Thapa S, & Tay L (2020). Positive emotions at work. Annual Review of Organizational Psychology and Organizational Behavior, 7, 451–477. 10.1146/annurevorgpsych-012119-044908 [DOI] [Google Scholar]
- Dimoff JK, & Kelloway EK (2019). With a little help from my boss: The impact of workplace mental health training on leader behaviors and employee resource utilization. Journal of Occupational Health Psychology, 24, 4–19. 10.1037/ocp0000126 [DOI] [PubMed] [Google Scholar]
- Dursa EK, Reinhard MJ, Barth SK, & Schneiderman AI (2014). Prevalence of a positive screen for PTSD among OEF/OIF and OEF/OIF-era veterans in a large population-based cohort. Journal of Traumatic Stress, 27, 542–549. 10.1002/jts.21956 [DOI] [PubMed] [Google Scholar]
- Elnitsky CA, Blevins CL, Fisher MP, & Magruder K (2017). Military service member and veteran reintegration: A critical review and adapted ecological model. American Journal of Orthopsychiatry, 87, 114–128. 10.1037/ort0000244 [DOI] [PubMed] [Google Scholar]
- Feldman LA (1995). Variations in the circumplex structure of mood. Personality and Social Psychology Bulletin, 21, 806–817. 10.1177/0146167295218003 [DOI] [Google Scholar]
- Gable SL, Reis HT, & Elliot AJ (2000). Behavioral activation and inhibition in everyday life. Journal of Personality and Social Psychology, 78, 1135–1149. 10.1037/00223514.78.6.1135 [DOI] [PubMed] [Google Scholar]
- Garland EL, Fredrickson B, Kring AM,Johnson DP, Meyer PS, & Penn DL (2010). Upward spirals of positive emotions counter downward spirals of negativity: Insights from the broaden-and-build theory and affective neuroscience on the treatment of emotion dysfunctions and deficits in psychopathology. Clinical Psychology Review, 30, 849–864. 10.1016/j.cpr.2010.03.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goodman JS, & Blum TC (1996). Assessing the non-random sampling effects of subject attrition in longitudinal research. Journal of Management, 22, 627–652. 10.1177/014920639602200405 [DOI] [Google Scholar]
- Gouldner AW (1960). The norm of reciprocity: A preliminary statement. American Sociological Review, 25, 161–178. 10.2307/2092623 [DOI] [Google Scholar]
- Halpern DF (2005). Psychology at the intersection of work and family: Recommendations for employers, working families, and policymakers. American Psychologist, 60, 397–409. 10.1037/0003-066X.60.5.397 [DOI] [PubMed] [Google Scholar]
- Hammer LB, Brockwood K, & Haverly SN (2021). Supporting veterans in the workplace – The key role of supervisors. In Ainspan ND & Saboe KN (Eds.), How to hire and retain military veterans: A guidebook for business leaders and human resources professionals. Oxford University Press. [Google Scholar]
- Hammer LB, Demsky CA, Kossek EE, & Bray JW (2016). Work-family intervention research. In Allen TD & Eby LT (Eds.), The oxford handbook of work and family (pp. 349–361). NewYork, NY: Oxford University Press. 10.1093/oxfordhb/9780199337538.013.27 [DOI] [Google Scholar]
- Hammer LB, Kossek EE, Anger WK, Bodner T, & Zimmerman KL (2011). Clarifying work–family intervention processes: The roles of work–family conflict and family-supportive supervisor behaviors. Journal of Applied Psychology, 96, 134–150. 10.1037/a0020927 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hammer LB, Kossek EE, Zimmerman K, & Daniels R (2007). Clarifying the construct of family-supportive supervisory behaviors (FSSB): A multilevel perspective. In Perrewé PL & Ganster DC (Eds.), Research in occupational stress and well-being: Exploring the work and non-work interface, Vol. 6 (pp. 165–204). Amsterdam, the Netherlands: Elsevier Science/JAI Press. 10.1016/S1479-3555(06)06005-7 [DOI] [Google Scholar]
- Hammer LB, & Perry ML (2019). Reducing work–life stress: The place for integrated interventions. In Hudson HL, Nigam JAS, Sauter SL, Chosewood LC, Schill AL & Howard J (Eds.), Total worker health (pp. 263–278). Washington, DC: American Psychological Association. 10.1037/0000149-016 [DOI] [Google Scholar]
- Hammer LB, Wan WH, Brockwood K, Bodner T, & Mohr CD (2019). Supervisor support training effects on veterans in the workplace: Effects on health and work outcomes. Journal of Applied Psychology, 104, 52–69. https://psycnet.apa.org/doi/10.1037/apl0000354. [DOI] [PubMed] [Google Scholar]
- Hammer LB, Wan WH, Brockwood KJ, Mohr CD, & Carlson KF (2017). Military, work, and health characteristics of separated and active service members from the Study for Employment Retention of Veterans (SERVe). Military Psychology, 29(6), 491–512. [Google Scholar]
- Han SC, Castro F, Lee LO, Charney ME, Marx BP, Brailey K, … Vasterling JJ (2014). Military unit support, post deployment social support, and PTSD symptoms among active duty and National Guard soldiers deployed to Iraq. Journal of Anxiety Disorders, 28, 446–453. 10.1016/j.janxdis.2014.04.004 [DOI] [PubMed] [Google Scholar]
- Hardison CM, & Shanley MG (2016). Essential skills veterans gain during professional military training: A resource for veterans and transitioning service members. Santa Monica, CA: RAND Corporation. 10.7249/TL160.3-1 [DOI] [Google Scholar]
- Hobfoll SE (1989). Conservation of resources: A new attempt at conceptualizing stress. American Psychologist, 44, 513–524. 10.1037/0003-066X.44.3.513 [DOI] [PubMed] [Google Scholar]
- Judge TA, & Locke EA(1993). Effect of dysfunctional thought processes on subjective wellbeing and job satisfaction. Journal of Applied Psychology, 78, 475–490. 10.1037/0021-9010.78.3.475 [DOI] [Google Scholar]
- Kashdan TB, Elhai JD, & Frueh BC (2007). Anhedonia, emotional numbing, and symptom overreporting in male veterans with PTSD. Personality and Individual Differences, 43, 725–735. 10.1016/j.paid.2007.01.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keeling M, Kintzle S, & Castro CA (2018). Exploring US veterans’ post-service employment experiences. Military Psychology, 30(1), 63–69. 10.1080/08995605.2017.1420976 [DOI] [Google Scholar]
- Kelloway EK, & Barling J (2010). Leadership development as an intervention in occupational health psychology. Work & Stress, 24, 260–279. 10.1080/02678373.2010.518441 [DOI] [Google Scholar]
- Kossek E, Pichler S, Bodner T, & Hammer L (2011). Workplace social support and work–family conflict: A meta-analysis clarifying the influence of general and work–family-specific supervisor and organizational support. Personnel Psychology, 64, 289–313. 10.1111/j.1744-6570.2011.01211.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kossek EE, Thompson RJ, Lawson KM, Bodner T, Perrigino MB, Hammer LB, … Bray JW (2019). Caring for the elderly at work and home: Can a randomized organizational intervention improve psychological health? Journal of Occupational Health Psychology, 24, 36–54. 10.1037/ocp0000104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larsen RJ, & Diener E (1992). Promises and problems with the circumplex model of emotion. In Clark MS (Ed.), Review of personality and social psychology, Vol. 13 Emotion (pp. 25–59). Thousand Oaks, CA: Sage Publications Inc. [Google Scholar]
- Larsen RJ, & Fredrickson BL (1999). Measurement issues in emotion research. In Kahneman D, Diener E & Schwarz N (Eds.), Well-being: The foundations of hedonic psychology (pp. 40–60). New York, NY: Russell Sage Foundation. [Google Scholar]
- Larsen RJ, & Kasimatis M (1990). Individual difference in entrainment of mood to the weekly calendar. Journal of Personality and Social Psychology, 58(1), 164–171. 10.1037/0022-3514.58.1.164 [DOI] [PubMed] [Google Scholar]
- Lazarus RL (1982). Thoughts on the relations between emotion and cognition. American Psychologist, 37, 1019–1024. 10.1037/0003-066X.37.9.1019 [DOI] [Google Scholar]
- Lazarus RS (2006). Emotions and interpersonal relationships: Toward a person-centered conceptualization of emotions and coping. Journal of Personality, 74(1), 9–46. 10.1111/j.1467-6494.2005.00368.x [DOI] [PubMed] [Google Scholar]
- Lazarus RS, & Folkman S (1984). Stress, appraisal, and coping. New York, NY: Springer Publishing Company Inc. [Google Scholar]
- Little RJ, Long Q, & Lin X (2009). A comparison of methods for estimating the causal effect of a treatment in randomized clinical trials subject to noncompliance. Biometrics, 65, 640–649. 10.1111/j.1541-0420.2008.01066.x [DOI] [PubMed] [Google Scholar]
- Mahar AL, Gribble R, Aiken AB, Dandeker C, Duffy B, Gottfried G, … Fear NT (2017). Public opinion of the armed forces in Canada, UK and the US. Journal of Military, Veteran and Family Health, 3, 2–3. 10.3138/jmvfh.3.2.002 [DOI] [Google Scholar]
- McCabe CT, Mohr CD, Hammer LB, & Carlson KC (2019). PTSD symptomology and motivated alcohol use among military service members: Testing a conditional indirect effect model of social support. Substance Use and Misuse, 54(2), 257–270. 10.1080/10826084.2018.1517176. [DOI] [PubMed] [Google Scholar]
- McCoy CE (2017). Understanding the intention-to-treat principle in randomized controlled trials. Western Journal of Emergency Medicine, 18, 1075–1078. 10.5811/westjem.2017.8.35985 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Melrose KL, Brown GD, & Wood AM (2015). When is received social support related to perceived support and well-being? When it is needed. Personality and Individual Differences, 77, 97–105. 10.1016/j.paid.2014.12.047 [DOI] [Google Scholar]
- Murray D (1998). Design and analysis of group-randomized trials: Monographs in epidemiology and biostatistics, Vol. 29. New York, NY: Oxford University Press Inc. [Google Scholar]
- Muthén LK, & Muthén BO (1998–2017). Mplus user’s guide (8th ed.). Los Angeles, CA: Author. [Google Scholar]
- Myers D, & Diener E (1995). Who is happy? Psychological Science, 6(1), 10–19. 10.1111/j.1467-9280.1995.tb00298.x [DOI] [Google Scholar]
- Newman DB, Schwarz N, & Stone AA (2020). Global reports of well-being overestimate aggregated daily states of well-being. The Journal of Positive Psychology, 1–10. 10.1080/17439760.2020.1725608. Advanced Online Publication. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Odle-Dusseau HN, Hammer LB, Crain TL, & Bodner TE (2016). The influence of family-supportive supervisor training on employee job performance and attitudes: An organizational work–family intervention. Journal of Occupational Health Psychology, 21, 296–308. 10.1037/a0039961 [DOI] [PubMed] [Google Scholar]
- Pierce KD, & Quiroz CS (2019). Who matters most? Social support, social strain, and emotions. Journal of Social and Personal Relationships, 36, 3273–3292. 10.1177/0265407518817400 [DOI] [Google Scholar]
- Posner J, Russell JA, Gerber A, Gorman D, Colibazzi T, Yu S, … Peterson BS (2009). The neurophysiological bases of emotion: An fMRI study of the affective circumplex using emotiondenoting words. Human Brain Mapping, 30, 883–895. 10.1002/hbm.20553 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pressman SD, & Cohen S (2005). Does positive affect influence health? Psychological Bulletin, 131, 925–971. 10.1037/0033-2909.131.6.925 [DOI] [PubMed] [Google Scholar]
- Reis HT, & Gable SL (2000). Event-sampling methods. In Reis HT & Judd C (Eds.), Handbook of research methods in social psychology (pp. 190–222). New York, NY: Cambridge University Press. [Google Scholar]
- Revelle W (2020). Psych: Procedures for Psychological, Psychometric, and Personality Research. Northwestern University, Evanston, Illinois. R package version 2.0.7. https://CRAN.R-project.org/package=psych [Google Scholar]
- Robertson IT, & Cooper CL (2010). Full engagement: The integration of employee engagement and psychological well-being. Leadership & Organization Development Journal, 31, 324–336. 10.1108/01437731011043348 [DOI] [Google Scholar]
- Russell JA, & Barrett LF (1999). Core affect, prototypical emotional episodes, and other things called emotion: Dissecting the elephant. Journal of Personality and Social Psychology, 76, 805–819. 10.1037/0022-3514.76.5.805 [DOI] [PubMed] [Google Scholar]
- Seo MG, Barrett LF, & Bartunek JM (2004). The role of affective experience in work motivation. Academy of Management Review, 29, 423–439. 10.5465/amr.2004.13670972 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shadish WR, & Cook TD (2009). The renaissance of field experimentation in evaluating interventions. Annual Review of Psychology, 60, 607–629. 10.1146/annurev.psych.60.110707.163544 [DOI] [PubMed] [Google Scholar]
- Smith AJ, Weisenbach SL, & Jones RT (2018). Cynicism among veterans who struggle to adapt to life after combat: Towards an understanding of adaptive functions and maladaptive consequences. Traumatology, 24, 17–26. 10.1037/trm0000127 [DOI] [Google Scholar]
- Sonnentag S, & Grant AM (2012). Doing good at work feels good at home, but not right away: When and why perceived prosocial impact predicts positive affect. Personnel Psychology, 65, 495–530. 10.1111/j.1744-6570.2012.01251.x [DOI] [Google Scholar]
- Spector PE, & Brannick MT (2011). Methodological urban legends: The misuse of statistical control variables. Organizational Research Methods, 14, 287–305. 10.1177/1094428110369842 [DOI] [Google Scholar]
- Stone C, & Stone DL (2015). Factors affecting hiring decisions about veterans. Human Resource Management Review, 25, 68–79. 10.1016/j.hrmr.2014.06.003 [DOI] [Google Scholar]
- Stone D, & Colella A (1996). A model of factors affecting the treatment of disabled individuals in organizations. The Academy of Management Review, 21, 352–401. 10.5465/amr.1996.9605060216 [DOI] [Google Scholar]
- Tanielian T, Batka C, & Meredith LS (2017). The changing landscape for Veterans’ Mental Health Care. Santa Monica, CA: RAND Corporation. https://www.rand.org/pubs/research_briefs/RB9981z2.html [Google Scholar]
- Tennen H, Affleck G, Armeli S, & Carney MA (2000). A daily process approach to coping: Linking theory, research, and practice. American Psychologist, 55,626–636. 10.1037/0003-066X.55.6.626 [DOI] [PubMed] [Google Scholar]
- Watson D, Clark LA, & Tellegen A (1988). Development and validation of brief measures of positive and negative affect: The PANAS Scales. Journal of Personality and Social Psychology, 54, 1063–1070. 10.1037/0022-3514.54.6.1063 [DOI] [PubMed] [Google Scholar]
- Weiss HM, & Cropanzano R (1996). Affective events theory: A theoretical discussion of the structure, causes and consequences of affective experiences at work. In Staw BM & Cummings LL (Eds.), Research in organizational behavior: An annual series of analytical essays and critical reviews, Vol. 18 (pp. 1–74). Greenwich, CT: Elsevier Science/JAI Press. [Google Scholar]
- Yoon J, & Lim JC (1999). Organizational support in the workplace: The case of Korean hospital employees. Human Relations, 52, 923–945. 10.1023/A:1016923306099 [DOI] [Google Scholar]
- Zajonc RB (1980). Feeling and thinking: Preferences need no inferences. American Psychologist, 35, 151–175. 10.1037/0003-066X.35.2.151 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data utilized in the current study are available from the second author upon reasonable request.