

Abstract
An 8-year-old female Persian cat was brought in for evaluation of chronic vomiting. The presence of opaque enteric foreign bodies and intestinal obstruction along with azotaemia, hyperphosphataemia, moderate anaemia and peritoneal fluid were revealed following appropriate diagnostic work-up. Exploratory laparotomy confirmed jejunoileal dilation, ileocaecal stenosis, and numerous foreign objects in the jejunoileum. These foreign objects and ileocaecal stenosis were surgically removed, and intestinal resection and anastomosis was performed. The patient recovered favourably. Analysis revealed that the foreign objects were composed of calcium phosphate and calcium carbonate. Intestinal inflammation and stenosis secondary to enterolithiasis may have developed following ingestion of cat litter or a previous unrelated surgical intervention. We were unable to delineate the inciting pathogenesis in this particular case.
In humans, enterolithiasis is associated with ileal diverticulitis, duodenal diverticulitis, Meckel diverticulitis, Crohn's disease and secondary small bowel obstruction (Bruni et al 2002). In veterinary medicine, enterolithiasis is fairly common in horses (Lloyd et al 1987, Hassel et al 1999, Cohen et al 2000, Hassel et al 2004), but is considered rare in dogs and cats (Pitcher 1994). To the best of our knowledge, there is no description of enterolithiasis in a cat. Few reports have described trichobezoars and trichophytobezoars in cats. Barrs et al (1999) reported intestinal obstruction due to trichobezoars and trichophytobezoars caused by ingestion of non-digestible plant material, inflammatory bowel disease, flea allergy dermatitis and a long-hair coat; Frye (1972) documented that trichobezoars were caused by diaphragmatic hiatal hernia. None of these reports included analysis of the composition of the bezoar. Trichobezoars and trichophytobezoars represent concretions resulting from hair and plant ingestion; enterolithiasis concretions result from mineral ingestion. Herein, we present the case of a cat with enterolithiasis that underwent ovariohysterectomy because of pyometra 1 year earlier and propose a potential aetiology.
An 8-year-old female Persian cat with a 2-month history of chronic vomiting was brought to our institution. The diet for the cat had been Hairball Care Formula for adult cats (IAMS Japan, Tokyo, Japan) for several years. No history of pica was reported. The cat had previously undergone ovariohysterectomy because of pyometra 1 year earlier, and had been evaluated 6 months before this presentation due to vomiting. Plain abdominal radiography at that time suggested the presence of jejunoileal distension and intestinal foreign objects (Fig 1). More thorough testing was recommended, but declined by the owner.
Fig 1.

Lateral (A) and ventral–dorsal (B) abdominal radiography taken 6 months earlier, showing jejunoileal distension and radio-opaque foreign objects.
On physical examination, the cat was subdued, very thin and dehydrated, and had a bloated abdomen. At the time of admission, tests indicated moderate anaemia (packed cell volume, 22%; normal: 32–45%), an increased white blood cell count (wbc) (60,100/μl, bands 1202/μl, neutrophils 56,494/μl, monocytes 2404/μl; normal total wbc: 5500–19,500/μl), elevated urea nitrogen (84.2 mg/dl; normal: 17.0–36.0 mg/dl), mildly increased phosphorous (10.0 mg/ml; normal: 1.7–7.2 mg/ml) and mildly increased creatinine (2.0 mg/ml; normal: 0.7–1.8 mg/ml). The urine specific gravity was 1.050 (normal: 1.015–1.050) indicating that the elevations in creatinine and urea nitrogen were prerenal in origin. The rest of the urinalysis was normal. Serum enzyme-linked immunosorbent assay yielded negative results for both feline leukaemia virus and feline immunodeficiency virus. Faecal testing likewise yielded negative results for internal parasites. Plain abdominal radiography showed severe gas retention in the jejunoileum, jejunoileal distension and several pebble-sized (15×10×10 mm) radio-opaque lesions in the jejunoileum and colon (Fig 2). Abdominal ultrasonography revealed gas retention and several pebble-sized (15×10×10 mm) shadowy and highly echogenic foreign objects in the jejunoileum and colon. No uroliths were identified in the kidney or bladder on ultrasonography, and these and other abdominal organs appeared normal.
Fig 2.

Lateral (A) and ventral–dorsal (B) abdominal radiography showing severe jejunoileal distension. Numerous radio-opaque foreign objects are also apparent.
Intravenous fluids were administered to correct dehydration and an exploratory laparotomy was performed the next day. The abdominal cavity contained a moderate amount of fluid and the jejunoileum was severely distended (Fig 3). Moderate ileocaecal stenosis and mesenteric adhesion were noted (Fig 4). In addition, swollen sentinel lymph nodes and dilated jejunal and ileal veins were confirmed (Fig 3). Numerous foreign objects were palpable in the distended jejunoileum. The distal end of the dilated jejunoileum, ileocaecal section and proximal end of the colon were resected and end-to-end anastomosis was performed after removing all foreign objects (Fig 5). Swollen mesenteric lymph nodes were also excised. Although the excised intestinal canal exhibited stenosis because of moderate thickening of the intestinal wall, no regions of complete obstruction were present.
Fig 3.
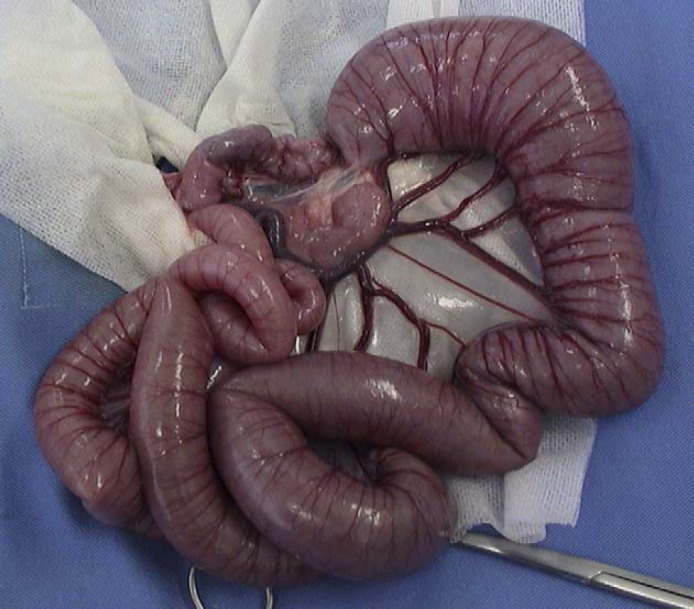
Exploratory laparotomy showing severe jejunoileal distension. Moderate ileocaecal stenosis is also apparent.
Fig 4.
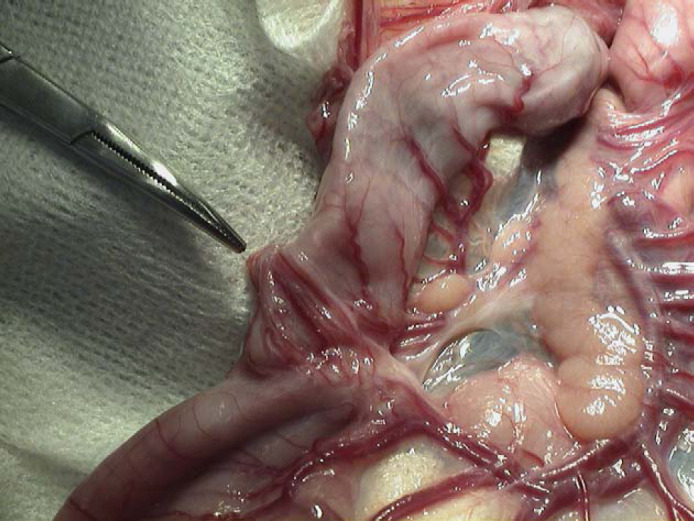
Exploratory laparotomy revealing mild mesenteric adhesion in the ileocaecal region.
Fig 5.

Numerous hairball- and stone-like foreign objects were retrieved.
Histopathological analysis of the excised intestinal tract showed wide mucosal detachment in one area and ulceration accompanied by necrosis and purulent inflammation. On the serosal membrane, oedema, dilated lymphatic vessels, bleeding and haemosiderin deposition were noted; submucosal tissue displayed broad focal lymphocytic infiltration. Infiltration of numerous plasmacytes and lymphocytes was observed in the lamina propria mucosae, and the tips of intestinal villi were oedematous. Lymphocytic infiltration accompanied by mild fibrosis was present in the slightly stenosed ileocaecal submucosal tissue and tunica muscularis. Furthermore, in the connective tissue of the mesenteric adhesion, similar infiltration of lymphocytes and plasmacytes was seen. Although mildly enlarged lymphoid follicles were noted in the cortices of lymph nodes, no atypical cells were present. Lymphatic sinuses were mildly dilated, and numerous macrophages were seen. The entire resected specimen was carefully examined and no evidence of neoplasia was identified. Analysis of the foreign objects revealed a composition of 61% calcium phosphate and 39% calcium carbonate (SRL Laboratory, Tokyo, Japan).
The general condition of the cat continued to improve, and the animal was discharged. Although mild anaemia remained on day 25 after presentation, other abnormal values returned to normal. Radiographs taken 5 months postoperatively revealed no signs of further enterolithiasis.
Few studies on trichobezoars in cats have been reported (Frye 1972, Barrs et al 1999), and to the best of our knowledge, none have described enterolithiasis diagnosed with component analysis. In the present case, jejunoileal foreign objects were diagnosed as lithiasis by component analysis. In addition, based on past medical history and present surgery, a plausible cause of enterolithiasis was hypothesised.
The results of exploratory laparotomy showed that the severe jejunoileal dilatation was caused by ileocaecal stenosis. Furthermore, the jejunoileal dilation appeared to have caused dilation of the mesenteric vein. Peritoneal fluid was likely attributable to elevated mesenteric vein pressure and recent fluid therapy, as no fluid had been detected prior to surgery 1 year before. Because the peritoneal fluid was not examined cytologically, the pathophysiological cause could not be substantiated.
Histology showed that the ends of the excised intestinal tract were normal, suggesting that enterolithiasis was not the result of primary intestinal disease. About 1 year previously, the cat had undergone ovariohysterectomy for pyometra. Several cases of colonic stenosis due to mesenteric adhesion have been reported previously (Muir et al 1991, Smith and Davies 1996, Coolman et al 1999). In this case, ileocaecal stenosis was accompanied by mild mesenteric adhesion, and fibrosis in the ileocaecal tunica muscularis and submucosal tissue. These findings suggest that ileocaecal stenosis developed as a postoperative complication of ovariohysterectomy.
Pitcher (1994) reported the case of a cocker spaniel with enterolithiasis. In that report, the composition was described as being primarily granular calcified material and hairs. However, the pathogenesis of enterolithiasis in that case was not explained. In this current case, abdominal radiography 6 months previously had shown jejunoileal distension and several radio-opaque densities. The numerous foreign objects removed in surgery from the cat contained hair and stone-like material, suggesting that enterolithiasis resulted from reduced intestinal peristalsis due to partial ileocaecal obstruction by hairballs. However, as in the report by Pitcher (1994), the underlying pathogenesis for enterolithiasis remained unclear. No disease causing abnormalities of calcium phosphate or calcium carbonate metabolism were present in this case. In horses, direct ingestion of nitrogen, magnesium and phosphorus can be a risk factor of developing struvite enterolithiasis (Lloyd et al 1987). As in horses, the causes of developing enterolithiasis in the present case could include direct ingestion of substances containing component of the enterolithiasis, however, the pathogenesis is not certain. Some cat litter has a high calcium phosphate or calcium carbonate content. Ingestion of cat litter would result in higher concentrations of calcium phosphate or calcium carbonate in intestinal contents, possibly contributing to the development of enterolithiasis. However, there was no history of pica to confirm this theory in this case. Unfortunately, therefore, we were not able to clarify the actual pathogenesis of the enterolith development in this patient.
References
- Barrs V.R., Beatty J.A., Tisdall P.L., Hunt G.B., Gunew M., Nicoll R.G., Malik R. Intestinal obstruction by trichobezoars in five cats, Journal of Feline Medicine and Surgery 1, 1999, 199–207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bruni R., Chirco L., Lemeni A.R., Petrocca S. Intermittent small bowel obstruction by jejunal enteroliths in a patient with a Crohn's disease stricture, Chirurgia Italiana 54, 2002, 903–905. [PubMed] [Google Scholar]
- Cohen N.D., Vontour C.A., Rakestraw P.C. Risk factors for enterolithiasis among horses in Texas, Journal of the American Veterinary Medical Association 216, 2000, 1787–1794. [DOI] [PubMed] [Google Scholar]
- Coolman B.R., Marretta S.M., Dudley M.B., Averill S.M. Partial colonic obstruction following ovariohysterectomy: a report of three cases, Journal of the American Hospital Association 35, 1999, 169–172. [DOI] [PubMed] [Google Scholar]
- Frye F.L. Hiatal diaphragmatic hernia and tricholithiasis in a Golden cat (a case history), Veterinary Medicine, Small Animal Clinician 67, 1972, 391–392. [PubMed] [Google Scholar]
- Hassel D.M., Langer D.L., Snyder J.R., Drake C.M., Goodell M.L., Wyle A. Evaluation of enterolithiasis in equids: 900 cases (1973–1996), Journal of the American Veterinary Medical Association 214, 1999, 233–237. [PubMed] [Google Scholar]
- Hassel D.M., Rakestraw P.C., Gardner I.A., Spier S.J., Snyder J.R. Dietary risk factors and colonic pH and mineral concentrations in horses with enterolithiasis, Journal of Veterinary Internal Medicine 18, 2004, 346–349. [DOI] [PubMed] [Google Scholar]
- Lloyd K., Hintz H.F., Wheat J.D. Enteroliths in horses, Cornell Veterinarian 77, 1987, 172–186. [PubMed] [Google Scholar]
- Muir P., Goldsmid S.E., Bellengerm C.R. Megacolon in a cat following ovariohysterectomy, Veterinary Record 129, 1991, 512–513. [PubMed] [Google Scholar]
- Pitcher G.D. Partial ileocaecocolic obstruction due to suspected enterolithiasis in a dog, Veterinary Record 135, 1994, 579. [PubMed] [Google Scholar]
- Smith M.C., Davies N.L. Obstipation following ovariohysterectomy in a cat, Veterinary Record 138, 1996, 163. [DOI] [PubMed] [Google Scholar]