

Abstract
The biplanar mesenteric vein portovenograms of 10 cats with left divisional intrahepatic portosystemic shunts consistent with a patent ductus venosus (PDV) were reviewed. A corrosion cast of the hepatic portal vasculature was made post mortem from one individual that died post operatively following surgical attenuation of the shunting vessel. On the basis of the combined surgical, post mortem and imaging data, these left divisional shunts were found to have consistent anatomy, each having a straight vessel which drained into a venous ampulla before draining into the caudal vena cava at the level of the diaphragm. The left phrenic vein and left hepatic vein both entered the ampulla independently of the shunting vessel. The anatomical similarity between these findings in the cat and the PDV in the dog suggest that it is appropriate to describe this particular portosystemic shunt as a PDV.
The embryological origin of the congenital intrahepatic portosystemic shunts that are recognised in the dog and cat remain unclear. Similar to the dog, intrahepatic porto-systemic shunts in the cat may be classified with regards to hepatic divisions according to which branch of the portal vein the shunting vessel arises from (White et al 1996, Lamb & White 1998).
In newborn puppies, the course of the ductus venosus has been shown to be consistent (Tisdall et al 1997, Burton & White 1999). The vessel was found to arise from the left branch of the portal vein, and continue between the left lateral lobe and papillary process of the caudate lobe of the liver before entering a venous ampulla and then the caudal vena cava. The venous ampulla represented the confluence of the ductus venosus, the left hepatic vein and the left phrenic vein (Burton & White 1999). A recent study has confirmed that a commonly recognised left divisional intrahepatic shunt in the dog represented persistence of the fetal ductus venosus (White & Burton 2000).
Although the patent ductus venosus (PDV) intrahepatic portosystemic shunt has been recognised in the cat (Parker 1982, Gandolfi 1984, White et al 1996), its anatomy has been poorly described and it has previously been defined as a left divisional shunt which drains into the left hepatic vein before entering the caudal vena cava (Payne et al 1990, White et al 1996, Lamb & White 1998). The purpose of this study was define the anatomy of the PDV in the cat more fully using the angiographic and gross anatomical findings of a series of clinical cases with left divisional intrahepatic shunts which were consistent with the previous definition of a PDV.
Materials and methods
The surgical records of clinical cases treated for the attenuation of a left divisional intrahepatic shunt consistent with a PDV, which had been examined by the authors between June 1993 and December 2000 were reviewed, retrospectively.
Mesenteric portovenography was carried out during surgery by using a mobile image intensification unit to obtain lateral and ventrodorsal images of the cranial abdomen (White et al 1996, Lamb & White 1998). Images were obtained before manipulation of the shunt and during the temporary full ligation of the shunting vessel. Angiograms were recorded on videotape and all the diagnostic images were reviewed by both authors.
In one clinical case, a five-month-old Siamese, the surgical management of the portosystemic shunt was complicated by the presence of a full thickness duodenal ulcer and peritonitis. This cat died 4 h after the surgical procedure and permission was given for a post mortem examination. Mesenteric portovenography was performed and representative lateral and ventrodorsal radiographs were obtained to illustrate the morphological features of the left divisional portosystemic shunt. Subsequently, a corrosion cast of this cat's hepatic portal system was made using polyester casting resin (Alec Tiranti) as previously described (White & Burton 2000).
On the basis of the combined imaging data, the gross findings during surgery and the findings of the corrosion cast, the anatomy of the intrahepatic portosystemic shunts were reviewed and evaluated.
Results
Diagnostic images of 10 cats were reviewed. The breeds represented were five Siamese, two Havannahs, two domestic shorthairs and a Persian. All of these cats had a left divisional shunt consistent with a PDV (White et al 1996, Lamb & White 1998). Portovenography consistently demonstrated a straight shunt vessel draining into a venous dilatation that drained into the caudal vena cava at the level of the diaphragm (Figs 1 and 2). In each case, two other vessels were seen to enter the venous dilatation; the left phrenic vein entered the lateral region of the dilatation and the left hepatic vein entered the caudoventral region of the dilatation. In all cases, the shunting vessel was exposed between the left medial and lateral lobes of the liver towards the midline, as described by White and others (1996) (Fig 3). These vessels and their orientations were clearly revealed on the corrosion cast of the hepatic portal system obtained post mortem from the Siamese cat that died post operatively (Figs 4 and 5).
Fig 3.
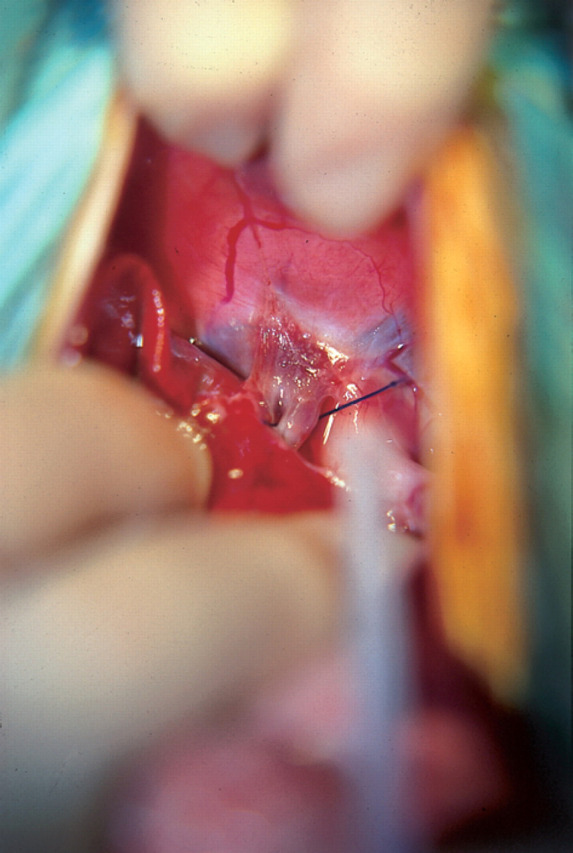
Intraoperative view of a cat with a left divisional shunt consistent with a PDV. A, ampulla; D, diaphragm; LH, left hepatic vein; L Ph, left phrenic vein; PDV, patent ductus venosus; S, ligature placed around the PDV allowing shunt attenuation.
Fig 1.

(a) Ventrodorsal portovenogram of a cat with a left divisional shunt consistent with a PDV. (b) The radiographic findings are also represented as a line diagram. A, ampulla; L Ph, left phrenic vein; P, portal vein; PDV, patent ductus venosus; Pre VC, prehepatic vena cava; Post VC, post hepatic vena cava.
Fig 2.

(a) Lateral portovenogram of a cat with a left divisional shunt consistent with a PDV. (b) The radiographic findings are also represented as a line diagram. The same annotations apply as to Fig 1. LH, left hepatic vein.
Fig 4.

(a) A painted corrosion cast of the hepatic vasculature from a cat with a left divisional shunt consistent with a PDV, photographed from the cranial direction. (b) The cast is also represented as a line diagram. Blue-portal vein vasculature; red-patent ductus venosus; yellow-venous ampulla. LH, left hepatic vein; L Ph, left phrenic vein; P, portal vein; Pre VC, prehepatic vena cava; Post VC, post hepatic vena cava; RH, right medial lobe hepatic vein.
Fig 5.

(a) A painted corrosion cast of the hepatic vasculature from a cat with a left divisional shunt consistent with a PDV, photographed from the left lateral apsect. (b) The cast is also represented as a line diagram. The same colour codings and annotations apply as to Fig 4.
The surgical records indicated that in all cases, the shunt ligation was performed on the shunting vessel itself, before it entered the venous dilatation. The left hepatic vein was never included in the ligated vessel.
Discussion
In this study, the angiographic and surgical anatomy of the intrahepatic portosystemic shunt that has been classified as a PDV was found to be consistent. The anatomical findings were considered similar to the anatomy of the PDV recently described in the dog (White & Burton 2000). As with the dog, the shunting vessel was found to enter a venous ampulla prior to its drainage into the caudal vena cava. Angiographic and surgical findings confirmed that the left hepatic and left phrenic veins also entered the ampulla prior to its subsequent caval drainage. Previously, reports of PDV anatomy in the dog and cat have suggested that the shunting vessel enters directly into the left hepatic vein (Payne et al 1990, Swalec Tobias & Rawlings 1996, Lamb & White 1998). Similar to the dog, the findings of this study confirm that this is not the case and that the shunting vessel and the left hepatic vein enter the venous ampulla as independent vessels.
Although this study has not investigated the anatomy of the portal venous system in the neonatal cat, the anatomical similarities of the hepatic portal system found in the juvenile cat and those of the PDV in the juvenile dog suggest that it is appropriate to describe this particular portosystemic shunt as a persistent PDV.
The corrosion cast obtained from the Siamese cat that died did not demonstrate evidence of an intrahepatic portal vasculature. In the dog, it is well recognised that a number of individuals with intrahepatic portosystemic shunts demonstrate, radiographically, very little evidence of further intrahepatic portal vasculature development at the time of surgical intervention (White et al 1998). This condition has been described as portal atresia, but as demonstrated by White and others (1998), the majority of these individuals develop a well-formed intrahepatic portal vasculature following shunt attenuation. Swalec & Smeak (1990) suggested that an absence of aborising intrahepatic vasculature is correlated with more postoperative complications. The portovenography findings in the remaining nine cats in the study were similar to those found in the Siamese that died. It was, therefore, not considered possible to make further conclusions regarding this lack of portal vasculature found in the corrosion cast.
In cats, intrahepatic shunts are considered to occur less commonly than extrahepatic shunts; less than 10% of the 78 cases of feline portosystemic shunts reviewed by Levy and others (1995) were intrahepatic. Possibly, as a consequence of this, there are few reports describing the surgical management of intrahepatic portosystemic shunts in the cat (Berger et al 1986, White et al 1996). In six of the seven cases described, the left divisional shunts consistent with a PDV were surgically managed by the post hepatic direct shunt attenuation. In the remaining case, the shunt was managed by segmental isolation and obstruction of the specific branch of the portal vein supplying the intrahepatic shunt (Berger et al 1986). A number of authors have described attenuation of the left hepatic vein for the treatment of the PDV in the dog (Martin et al 1986, Swalec Tobias & Rawlings 1996). White and others (1998) concluded that, in the dog, the direct attenuation of the PDV before it enters the venous ampulla was technically the least complicated or demanding of the surgical procedures that have been described for the attenuation of this form of intrahepatic shunt. In this study, in each case, the portosystemic shunt was also attenuated by the direct manipulation of the shunting vessel prior to its entrance into the ampulla.
In conclusion, the PDV in the cat consistently courses craniolaterally between the left lateral lobe and the papillary process of the caudate lobe of the liver, before terminating in a venous ampulla which drains into the left lateral region of the caudal vena cava at the level of the diaphragm. The left hepatic vein and the left phrenic vein both enter the ampulla independently of the shunting vessel. Surgically, the PDV can be attenuated directly prior to its entrance into the ampulla.
References
- Berger B, Whiting PG, Breznock EM, et al. (1986) Congenital feline portosystemic shunts. Journal of the American Veterinary Medical Association 188, 517–521. [PubMed] [Google Scholar]
- Burton CA, White RN. (1999) The angiographic anatomy of the portal venous system in the neonatal dog. Research in Veterinary Science 66, 211–217. [DOI] [PubMed] [Google Scholar]
- Gandolfi RC. (1984) Hepatoencephalopathy associated with patent ductus venosus in a cat. Journal of the American Veterinary Medical Association 185, 301–302. [PubMed] [Google Scholar]
- Lamb CR, White RN. (1998) Morphology of congenital intrahepatic portacaval shunts in dogs and cats. Veterinary Record 142, 55–60. [DOI] [PubMed] [Google Scholar]
- Levy JK, Bunch SE, Komtebedde J. (1995) Feline portosystemic vascular shunts. In: Kirk's Current Veterinary Therapy XII. Small Animal Practice Bonagura JD, ed. Philadelphia: WB Saunders, pp. 743–749. [Google Scholar]
- Martin RA, August JR, Barber DL, et al. (1986) Left hepatic vein attenuation for treatment of patent ductus venosus in a dog. Journal of the American Veterinary Medical Association 189, 1465–1468. [PubMed] [Google Scholar]
- Parker AJ. (1982) Differential diagnosis of brain disease. Modern Veterinary Practice 63, 711–715. [PubMed] [Google Scholar]
- Payne JT, Martin RA, Constantinescu GM. (1990) The anatomy and embryology of portosystemic shunts in dogs and cats. Seminars in Veterinary Medicine and Surgery (Small Animal Practice) 5, 76–82. [PubMed] [Google Scholar]
- Swalec KM, Smeak DD. (1990) Partial versus complete attenuation of single portosystemic shunts. Veterinary Surgery 19, 406–411. [DOI] [PubMed] [Google Scholar]
- Tobias KM Swalec, Rawlings CA. (1996) Surgical techniques for extravascular occlusion of intrahepatic shunts. Compendium on Continuing Education for the Practicing Veterinarian 18, 745–754. [Google Scholar]
- Tisdall PLC, Hunt GB, Borg RP, et al. (1997) Anatomy of the ductus venosus in neonatal dogs (Canis familiaris). Anatomy Histology and Embryology 26, 35–38. [DOI] [PubMed] [Google Scholar]
- White RN, Burton CA. (2000) Anatomy of the patent ductus venosus in the dog. Veterinary Record 146, 425–429. [DOI] [PubMed] [Google Scholar]
- White RN, Burton CA, McEvoy FJ. (1998) Surgical treatment of intrahepatic portosystemic shunts in 45 dogs. Veterinary Record 142, 358–365. [DOI] [PubMed] [Google Scholar]
- White RN, Forster-van Hijfte MA, Petrie G, et al. (1996) Surgical treatment of intrahepatic portosystemic shunts in six cats. Veterinary Record 139, 314–317. [DOI] [PubMed] [Google Scholar]