

Abstract
A 2-year-old female mixed-breed cat weighing 2.7 kg presented with recurrent rectal prolapse. The following report describes its treatment by laparoscopic-assisted incisional colopexy using two portals. The procedure was effective and without trans- or postoperative complications. Recurrent prolapses did not recur in the 2 months of postoperative observation.
Short Communication
Rectal prolapse is the protrusion of the rectum mucosa through the anus. 1 Colopexy is a treatment used in animals with viable tissue and where manual reduction of the prolapse is difficult, even after two or three unsuccessful attempts to apply a purse-string suture. 2
There are a few reports of laparoscopic procedures in cats. 3 Video-assisted laparoscopic colopexy in dogs demonstrated that the absence of sutures associated with the total laparoscopic colopexy allowed effective fixation of organs and reduced the operation time. 4 The authors were not aware of any published reports of this procedure in cats.
A 2-year-old female cat, of undefined breed, weighing 2.7 kg, presented with diarrhea and hyporexia of approximately 3 weeks duration. It showed cachexia, dehydration, abdominal distress and rectal prolapse. The total blood count revealed leukocytosis with neutrophilia and eosinophilia. The blood serum chemistry showed a decrease of all plasma proteins and hypoalbuminaemia. Further, Toxocara species was detected on fecal examination.
Based on the laboratory results and clinical signs, therapy with antibiotics (cephalotin 20 mg/kg, SC, q8h, for 20 days and metronidazole 30 mg/kg, PO, q12h for 7 days), anti-inflammatories (meloxicam 0.2 mg/kg, IV, q24h, 3 days), laxatives (lactulose 370 mg/kg, PO, q12h, 20 days) and anti-parasitics (pyrantel pamoate 63 mg/kg, PO; praziquantel 5.5 mg/kg, PO, repeated after 15 and 21 days) was prescribed. Conservative treatments proved inefficient. After the third recurrence, we opted for a video-assisted incisional colopexy.
The animal was kept in a supine position and CO2 pneumoperitoneum (12 mmHg) was obtained from a portal of 5 mm placed in the midline (by open technic, without Veress needle) between the xiphoid process and umbilicus. Another similar portal was positioned on the left inguinal region (Figure 1). The colon was grasped with Kelly forceps, and the lateral portal was removed and the wound was enlarged approximately 0.5 cm allowing the exteriorization of the descendent colon next to the rectum; a seromuscular incision was made on its antimesenteric surface (about 11 mm). A simple, continuous suture pattern was applied covering the muscular, serosal and intestinal submucosa layers using 4-0 polypropylene, keeping the colon slightly traced on the cranial position. The surgery was carried out in 40 min. Antibiotic therapy was prescribed and feeding with paste food was indicated. There were no recurrences within the 2 months of postoperative observation. After this period, the animal showed weight gain, 3.4 kg (± 200 g per month).
Figure 1.
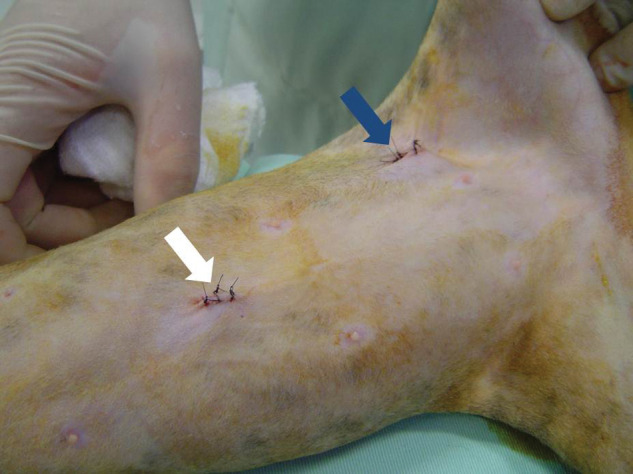
Surgical wounds (arrows) after skin sutures showing the position of the portals. The blue arrow shows the region where the descendent colon was fixed
The most common causes of rectal prolapse are dyschezia associated with severe colitis or secondary proctitis owing to parasitic infection. 2 Our patient fell into the risk group.
The combination of laparoscopic and conventional accesses was undertaken to aid the attachment of the colon in a short operation time. 4 Given that video-assisted surgery procedures demonstrated viability for dogs 5 and the colon fixation by laparoscopic route promotes permanent adhesions,3,4 the minimally-invasive approach was chosen over the abdominal cavity approach, as the video-surgery could minimize some drawbacks associated with conventional surgery. 6
Colopexy permits a permanent adherence between the serosal surface of the organ and the abdominal wall, in order to prevent caudal movement of the colon and rectum. There are several methods for fixing the large intestine, incisional and non-incisional. 1 In this case, the incisional method, with laparoscopic access, was adopted because it promotes consistent surgical adhesions with deep infiltration of conjunctive tissue. 4
The video-assisted incisional colopexy was effective for the treatment of recurrent rectal prolapse, without postoperative complications or recurrences for at least 2 months after the surgery.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- 1. Hedlund CS, Fossum TW. Surgery of the digestive system. In: Fossum TW, ed. Small animal surgery, 3rd edn. St Louis, MO: Mosby, 2007: 339–530. [Google Scholar]
- 2. Aronson L. Rectum and anus. In: Slatter D, ed. Textbook of small animal surgery, 3rd edn. Philadelphia, PA: Saunders, 2003: 682–707. [Google Scholar]
- 3. Brun MV, Pippi NL, Beck CAC, et al. Avaliação de dois diferentes fios de sutura para colopexia incisional laparoscopia em cães. Estudo experimental. Braz J Vet Res Anim Sci 2004; 41: 154–61 [in Portuguese]. [Google Scholar]
- 4. Brun MV, Pippi NL, Beck CAC, et al. Colopexia incisional por celiotomia ou transparietal auxiliada por videolaparoscopia em cães. Ciênc Rural 2004; 34: 829–37 [in Portuguese]. [Google Scholar]
- 5. Rawlings CA, Foutz TL, Mahaffey MB, et al. A rapid and strong laparoscopic-assisted gastropexy in dogs. Am J Vet Res 2001; 62: 871–5. [DOI] [PubMed] [Google Scholar]
- 6. Wickham JEA. The development of the concept of minimally invasive therapy. In: Gomella LG, Kozminski M, Winfield HN, eds. Laparoscopic urologic surgery. New York, NY: Raven Press, 1994: 3–8. [Google Scholar]