

Abstract
Background
The emigration of skilled professionals from low‐ and middle‐income countries (LMICs) to high‐income countries (HICs) is a general phenomenon but poses particular challenges in health care, where it contributes to human resource shortages in the health systems of poorer countries. However, little is known about the effects of strategies to help regulate this movement.
Objectives
To assess the effects of policy interventions to regulate emigration of health professionals from LMICs.
Search methods
We searched the Cochrane Effective Practice and Organisation of Care (EPOC) Group Specialised Register (searched 15 March 2011), the Cochrane Register of Controlled Trials (CENTRAL) (searched 2 March 2011), MEDLINE (searched 5 March 2011), EMBASE (searched 2 March 2011), CINAHL (searched 5 March 2011), LILACS (searched 7 March 2011), WHOLIS (searched 20 March 2011), SocINDEX (searched 11 March 2011), EconLit (searched 8 March 2011), Science and Social Science Citation Index (searched 8 March 2011), NLM Gateway (searched 31 March 2011) and ERIC (searched March 3 2011). We reviewed reference lists of included studies and selected reviews on the topic, contacted authors of included studies and experts on the field, and reviewed relevant websites.
Selection criteria
Randomised controlled trials (RCT), non‐randomised controlled trials (NRCT), controlled before‐and‐after studies (CBA) and interrupted time series (ITS) studies assessing any intervention in the source, the recipient or both countries that could have an impact on the number of professionals that emigrate from a LMIC. Health professionals, such as physicians, dentists, nurses or midwives, should be nationals of a LMIC whose graduate training was in a LMIC.
Data collection and analysis
One review author extracted data onto a standard form and a second review author checked data. Two review authors assessed risk of bias.
Main results
Only one study was included. This time series study assessed the migration of Philippine nurses to the United States of America (USA) from 1954 to 1990. We re‐analysed it as an interrupted time series study. The intervention was a modification of migratory law in the US, called the 'Act of October 1965', which decreased the restrictions on Eastern hemisphere immigrants to the USA. The analysis showed a significant immediate increase of 807.6 (95% confidence interval (CI) 480.9 to 1134.3) in the number of nurses migrating to the USA annually after the intervention. This represents a relative increase of 5000% over the underlying pre‐intervention trend. There were no significant differences in the slopes of the underlying trends for the number of nurses migrating between the pre‐ and postintervention periods.
Authors' conclusions
There is an important gap in knowledge about the effectiveness of policy interventions in either HICs or LMICs that could regulate positively the movement of health professionals from LMICs. The only evidence found was from an intervention in a HIC that increased the movement of health professionals from a LMIC.
New initiatives to improve records on the migration of health professionals from LMICs should be implemented, as a prerequisite to conducting more rigorous research in the field. This research should focus on whether the range of interventions outlined in the literature could be effective in retaining health professionals in LMICs. Such interventions include financial rewards, career development and continuing education, improving hospital infrastructure, resource availability, better hospital management and improved recognition of health professionals.
Keywords: Humans, Developed Countries, Developed Countries/statistics & numerical data, Developing Countries, Developing Countries/statistics & numerical data, Emigration and Immigration, Emigration and Immigration/legislation & jurisprudence, Emigration and Immigration/statistics & numerical data, Health Personnel, Nurses, Nurses/statistics & numerical data, Philippines, United States
Plain language summary
Interventions for controlling emigration of health professionals from low‐ and middle‐income countries
Researchers in the Cochrane Collaboration conducted a review of the effect of interventions to control the emigration of health professionals from low‐ and middle‐income countries. After searching for all relevant studies, they found only one study that met their requirements. The findings of this study are summarised below.
Controlling the emigration of health professionals Difficult living and working conditions and better opportunities abroad often lead health professionals from poorer countries to migrate to wealthier countries. This is one of several reasons why poorer countries often suffer from a severe shortage of health workers. Governments in these countries have tried a number of approaches to stop this migration, for instance by improving health workers’ working conditions; offering better training, more pay and better career prospects; or by introducing compulsory service for certain periods of time. Governments in a few wealthy countries have also tried to prevent this migration by introducing ethical guidelines for the recruitment of foreign health professionals. In other wealthy countries, however, governments have tried to solve their own health worker shortage by attracting foreign health workers, for instance through active recruitment or special immigration regulations.
What happens when efforts are made to regulate the emigration of health professionals? In most cases, efforts to regulate health worker migration have not been properly evaluated. The review authors found only one study that met their stated requirements for types of study designs. This study looked at the impact of United States (US) immigration law on the number of nurses emigrating from the Philippines to the USA. US government immigration laws were changed in the 1960s, giving equal access to European and non‐European immigrants. The study measured the number of nurses migrating from the Philippines to the USA in the years before and after the law had changed. The study showed that:
‐ The change in US immigration laws probably increased the number of nurses migrating from the Philippines to the USA. The quality of this evidence is moderate.
The review shows that there is a huge gap in our knowledge about the effectiveness of policy interventions that attempt to regulate the movement of health professionals from low‐ and middle‐income countries.
Summary of findings
for the main comparison.
| Interventions to reduce the emigration of health professionals from LMICs to HICs | ||||
|
Patient or population: Nurses in The Philippines Settings: USA and The Phillipines Intervention: Modification in US immigration law ('The Act of 1965') Comparison: No comparison group (uncontrolled ITS study) | ||||
| Outcomes | Impact | No of Participants (studies) | Quality of the evidence (GRADE) | Comments |
| Yearly number of Philippine nurses migrating to the USA | First data point after intervention: +807.6 nurses, (95% CI 480.9 to 1134.3). 5 years after the intervention the absolute difference between the number of nurses that migrated annually to the USA, compared with the number predicted by the underlying trend before the intervention, was 982 (95% CI 205 to 1758). |
1 study | ⊕⊕⊕⊝ moderate | The quality of the evidence was upgraded from low to moderate because of the magnitude of the effect size. |
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect. Very low quality: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||
Background
Description of the condition
International migration has been a growing phenomenon in recent decades (Global Forum 2007). In 2005, 191 million people, representing 3% of world population, lived outside their country of birth (United Nations 2006) and 45% of them were workers (Handbook 2006).
It is possible to distinguish two types of worker migration: temporary and permanent. In the first case, workers transfer for a limited time from their countries to another country and go back after a period of time (WHO 2006). In the case of permanent migration, workers emigrate from their countries and remain where they have moved.
In this review we will focus on policies that aim to reduce the permanent emigration of health professionals from low‐ or middle‐income countries (LMICs) and the undesirable effects of such emigration on the health system in LMICs. According to the framework proposed by Dal Poz to classify health workers (Dal Poz 2006), we will define 'health professionals' as those professionals directly in charge of the provision of health services, such as physicians, nurses or midwives. Other professionals in support and management roles in the health system and other non‐professional health providers (e.g. associate nurses or community health workers) will not be considered in this review.
Magnitude and impact of the problem
Permanent migration can produce positive effects for the source country through migrant investments, remittances, networking and knowledge transfer. However, this type of migration can also have negative consequences, especially when there is large‐scale emigration from a LMIC, which contributes to a shortage of professionals in the country's health system.
The World Health Report 2006 (WHO 2006) identified the migration of health professionals as a relevant concern in the healthcare systems of LMICs and high income countries (HICs). However, it is known that there are considerable difficulties in getting complete and reliable statistics for health professional migration, so the real situation is not fully known (Diallo 2004; Dovlo 2004). Moreover, available information is generally limited to registered doctors and nurses. Data on the migration of other health professionals, such as dentists, pharmacists and others, are virtually non‐existent (Stilwell 2003).
As an example of the magnitude of the problem, data reported in the World Health Report 2006 (WHO 2006) for country members of the Organization for Economic Co‐operation and Development (OECD) indicate that doctors and nurses trained abroad represent an important percentage of all the professionals registered, especially in English‐speaking countries. This has been confirmed by other authors in numerous publications (Bach 2007; Buchan 2004a; Connell 2007). From the perspective of source countries, available information indicates that doctors trained in Sub‐Saharan Africa and working in OECD countries represent around a quarter of the current workforce in those source countries, ranging from 3% in Cameroon to 37% in South Africa (OECD/WHO).
The emigration of health professionals from many LMICs has contributed to shortages of human resources in their health systems, exacerbating inequalities in health. Regions particularly affected include Sub‐Saharan Africa and South Asia (Dovlo 2004; Dovlo 2007). When a large number of health professionals remain abroad, the source country that has financed their education loses a return on their investment, giving a 'perverse subsidy' to the high‐income country where the professionals remain. On the other hand, such staff may be more willing to work (at a lower salary rate) in remote or unattractive locations in the recipient country (Martineau 2004). In a recently published study on the origins of migrant primary care physicians in the USA, Starfield et al established that “The United States disproportionately uses graduates of foreign medical schools from the poorest and most deprived countries to maintain its primary care physician supply.” (Starfield 2007).
In the case of nurses, there is evidence that there is an important flow of these professionals from LMICs to upper‐income destinations such as the United Kingdom, the United States and Ireland (Buchan 2003; Buchan 2004b; Dovlo 2007). In this case, the shortfall of these professionals in the recipient country acts as the main driver for international recruitment of these cadres, mainly from the Philippines, India and Sub‐Saharan Africa. The case of the Philippines is remarkable. It is estimated that close to 15,000 nurses migrate overseas each year to 30 different countries, resulting in an estimated 30,000 unfilled nursing positions in the source country (WHO 2006). This situation has been worsened by the policy of the Philippines to train nurses for overseas work (Muncada 1995).
Causes of the phenomenon
Although the decision to migrate is ultimately a personal choice, it is influenced by the migrant’s economic and social context in the country of origin and the conditions offered in the possible recipient country. Most of the time it is a difficult and complex choice marked by complicated social situations which we detail in the following paragraphs.
Conditions in the source country that can influence a decision to emigrate are: limited opportunities for professional development, training and promotion, in contrast to perceived opportunities abroad. Other conditions include poor remuneration and employment opportunities, such as differentials in salary levels between source and destination countries, and better prospects of securing a job abroad; constraints in health budgets in LMICs resulting in limited recruitment and unemployment; and poor working environments with lack of equipment, supplies and drugs to diagnose and treat patients (WHO 2006). Additional factors in the source country are political instability, ethnic and religious tensions resulting in civil war, human rights abuses, economic collapse, extreme poverty and excess workload for the few available health workers, as a result of a high disease burden, compounded by, in some settings, the HIV/AIDS pandemic. Finally, the intention to contribute to family wealth through sending a portion of their wages back to their families has been also mentioned by other authors (Stilwell 2004).
Conditions in the recipient country that may encourage a decision to emigrate include: increased demand for health professionals due to demographic conditions, such as an ageing population requiring more care, and economic changes that make work less attractive for local professionals; better working conditions; and better security as a result of economic and political stability in the recipient country (Dovlo 2003). Additionally, the use of aggressive international recruitment strategies in source countries by recipient countries, such as the UK and Canada, have also been mentioned (Bach 2003).
These conditions are intertwined in complex and variable ways from case to case, but always result in an imbalance favouring conditions in the recipient country.
Description of the intervention
The complex combination of factors that drives the migration flow of health professionals contributes to the complexity of the strategies to manage this flow. Actions to decrease imbalances between health systems of low, middle and high‐income countries have been described at three levels: in source countries, in recipient countries and at the international level.
A recent systematic review found seven major motivational themes that affect in and out of country migration: financial rewards, career development, continuing education, hospital infrastructure, resource availability, hospital management and recognition, but suggested that there was no good quality evidence on whether interventions that aim to address these factors are effective (Willis‐Shattuck 2008). The 2006 World Health Report suggests that education and training interventions for health professionals, which adjust training to the needs and demands of the local health system, could help to decrease emigration, but notes that there is no evidence to support this (WHO 2006).
It has also been suggested that, in recipient countries, strategies such as improving staff retention may decrease shortages of health professionals, resulting in fewer opportunities for migrants and, in consequence, in fewer incentives to migrate (Stilwell 2004). Regulation of visas and work permits to admit foreign health professionals may also help (Martineau 2004).
Interventions at the international level have been reviewed by Willets and Martineau (Willets 2004). They have analysed international codes which regulate the unethical recruitment of health professionals. The authors found at least 15 different codes and instruments, but only 12 had statements related to the protection of low‐ or middle‐income country health systems. None of the instruments analysed clearly contributed to achieving the defined objective.
Why it is important to do this review
We are not aware of any other systematic reviews of the evidence in this complex policy area that has important implications for health systems in LMICs. Therefore, this review aims to evaluate the effects of different strategies to regulate health professional emigration from LMICs.
Objectives
To assess the effects of policy interventions to regulate emigration of health professionals from LMICs.
Methods
Criteria for considering studies for this review
Types of studies
1. Randomised controlled trials (RCTs). 2. Non‐randomised controlled trials (NRCTs). 3. Controlled before‐after studies (CBAs), provided that:
pre‐ and postintervention periods for the study and control groups are the same;
the choice of control site is appropriate (comparable with respect to main characteristics); and
they have at least two clusters in each comparison group.
4. Interrupted time series (ITS) studies provided that:
the point in time when the intervention occurred is clearly defined and there are at least three data points before and three after the intervention.
Types of participants
Any group of health professionals who are nationals of a LMIC and whose graduate training was in a LMIC.
We defined a health professional as any professional directly in charge of the provision of health services, such as physicians, dentists, nurses or midwives. We used the World Bank definition of LMICs (World Bank).
We excluded all other health personnel without health professional training, such as lay health workers, managers or policy makers. Likewise, we excluded those health professionals from LMICs whose graduate training was in a high‐income country.
Types of interventions
Any intervention in the source, the recipient or both countries that could have an impact on the outcomes relevant to this review. Examples of interventions proposed in the literature include the following (Bach 2003; Buchan 2004b; Dal Poz 2006; Diallo 2004; Dovlo 2003; Stilwell 2004).
Source country
Strategies to improve work conditions and career prospects of health professionals (financial and non financial).
Interventions for the education and training of health professionals, which adjust training to the needs and demands of the local health system (e.g. teaching methods, use of local language training, community‐based curricula, etc.).
Use of compulsory service schemes for health professionals.
Strategies to facilitate and support the return of health professionals working abroad.
Recipient country
Strategies to improve the retention of native health professionals: financial and non‐financial incentives.
National migration regulation (e.g. visas, ethical guidelines for recruitment of foreign health professionals).
National (or regional) regulation of professional licensing.
Strategies to facilitate and support the return of foreign health professionals to their country of origin.
International agreements
Bilateral or multilateral agreements that regulate the flow of health professionals from LMICs to HICs.
Types of outcome measures
We included studies measuring at least one of the outcomes listed below.
Primary outcomes
Proportion of health professionals that emigrate from a LMIC (source country) or any measurement of change in the number of professionals that emigrate from a LMIC.
Secondary outcomes
Intention to emigrate abroad among health professionals from LMICs.
Any measurement of the number of emigrant (low‐ or middle‐income country) health professionals with professional licensing in recipient countries (high‐income countries).
Any other outcome reported.
Search methods for identification of studies
Electronic searches
We based our electronic search strategies on a combination of the Cochrane Effective Practice and Organisation of Care (EPOC) Group search strategy related to the study design (using the EPOC definitions ‐ RCT, NRCT, CBA, ITS) with terms related to health professionals and migration, expressed as controlled vocabulary terms (i.e. MeSH) and free‐text terms.
We searched the following electronic databases (with no language or publication restrictions) and the full search strategies are provided in the appendices listed.
Cochrane EPOC Group Specialised Register. Details of the search strategy used by the Group for the identification of studies for the Register, and the procedure used to code references, are outlined in the Group's module (http://onlinelibrary.wiley.com/o/cochrane/clabout/articles/EPOC/frame.html) (host: BiblioWeb; date of search 15 March 2011) (Appendix 1).
Cochrane Central Register of Controlled Trials Register (CENTRAL); (host: Wiley; date of search 2 March 2011)(Appendix 2).
MEDLINE (host: PubMed; date of search 5 March 2011)(Appendix 3).
EMBASE (host: OVID; date of search 2 March 2011)(Appendix 4).
CINAHL (host: EBSCO; date of search 5 March 2011)(Appendix 5).
LILACS (host: BIREME; date of search 7 March 2011)(Appendix 6).
ERIC (host: OCLC First search; date of search 3 March 2011) (Appendix 7).
Science and Social Science Citation Index (host: ISI web of science; date of search 8 March 2011)(Appendix 8).
SocINDEX (host: EBSCO; date of search 11 March 2011)(Appendix 9).
EconLit (host: EBSCO; date of search 8 March 2011)(Appendix 10).
WHOLIS (host: WHO; date of search 20 March 2011)(Appendix 11).
NLM Gateway (meeting abstracts, HSRProj) (host: National Library of Medicine, USA; date of search 31 March 2011)(Appendix 12).
Searching other resources
We used the following strategies to identify articles that may have been missed by the electronic searches:
handsearching of reference lists of all included studies;
handsearching of reference lists of selected reviews found through the electronic searches and that addressed the review topic;
search of 'Related articles' in PubMed for all included studies;
contact with authors to ask for any further published or unpublished work;
contact with experts; and
review of two relevant websites on the topic: International Centre on Nurse Migration (http://www.intlnursemigration.org) and EQUINET AFRICA (http://www.equinetafrica.org).
Data collection and analysis
We performed the analysis in accordance with the guidelines published in the Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 (Cochrane Handbook).
Selection of studies
Two review authors (TP, GR, BP,GB or CH) independently screened the titles and abstracts of all articles obtained from the search. We retrieved full copies of all reports deemed eligible by either of the review authors for closer inspection to determine if these studies met the inclusion criteria. Studies that initially appeared to meet the inclusion criteria but were later excluded are described in the table 'Characteristics of excluded studies' with the reasons for their exclusion. We settled disagreements through discussion with a third review author.
Data extraction and management
Data extraction was done by one review author (BP) and reviewed by a second (TP).
Assessment of risk of bias in included studies
Two authors (BP, TP) assessed the risk of bias of the only eligible study using the EPOC Group's risk of bias criteria for ITS studies.
Measures of treatment effect
As only one study was included in the review, we were not able to conduct any meta‐analysis (see Appendix 13 for review methods reported in the protocol).
Dealing with missing data
The only study included in the review needed to be re‐analysed as an ITS study. To accomplish this, we contacted the author of the study to obtain missing data. We then carried out a new statistical analysis using a segmented regression model adjusted for first order autocorrelation.
Data synthesis
As only one study was included in the review, data are presented in a narrative format (see Appendix 13 for review methods reported in the protocol).
Sensitivity analysis
We performed no sensitivity analysis.
Results
Description of studies
Results of the search
The comprehensive literature search retrieved 11,842 references that we subsequently screened. We considered 299 as potentially eligible and retrieved and evaluated the full text. Sixty‐two references corresponded to articles about a topic unrelated to emigration; 111 were not primary studies (this group included narrative reviews, letters, etc.); 34 described issues related to emigration in non health professions; and 70 described some aspect of emigration in health professionals, but not the effects of a specific intervention. Twenty‐one studies evaluated an intervention for controlling emigration, but did not fulfil our study design criteria. These studies are described in more detail under Characteristics of excluded studies. Only one study fulfilled our inclusion criteria (see Characteristics of included studies). The study selection process is summarised in Figure 1.
1.
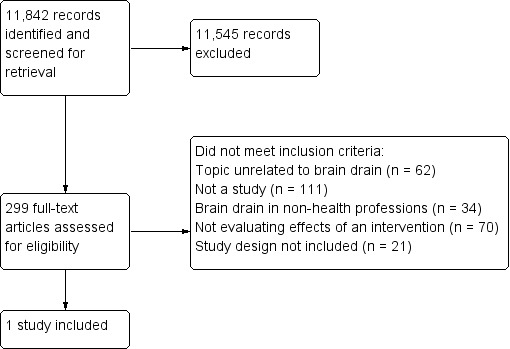
Flow diagram of study selection process.
Included studies
Only one study fulfilled the inclusion criteria for this review (Muncada 1995). This was a time series study examining the migration of nurses from the Philippines to the USA from 1954 to 1990. Although the author did not analyse the data as an interrupted time series, the information provided (published and unpublished) allowed us to do so. The intervention analysed was a modification in immigration laws in the USA in the 1960s, called the 'Act of October 1965'. This law modified the previous legislation in terms of decreasing the restrictions on Eastern hemisphere immigrants to the USA. Details of this intervention are provided in the Characteristics of included studies table. The outcome assessed was the number of Philippine nurses migrating to the USA per year. There were insufficient data to estimate the rate of nurse emigration.
Excluded studies
The vast majority of studies were excluded for reasons that were not obvious in the initial screening (which in many cases was based on the title only), as summarised in Figure 1. Twenty‐one studies evaluated an intervention to control the emigration of health professionals from LMICs, but their study designs did not match our inclusion criteria. These studies are described under Characteristics of excluded studies. Four studies had some data before and after the intervention, but did not have enough points before and after to fulfil our definition (Bach 2007; Bhagwati 1976; Buchan 2002; Wiwanitkit 2011). We contacted authors in order to be sure that there were no additional unreported data available.
Risk of bias in included studies
We carried out a risk of bias assessment of the included study using the EPOC criteria for ITS studies ('Risk of bias' table). The study presented a low risk of bias: the intervention assessed was independent of other changes over time and it was unlikely to affect data collection. The outcome was objective and missing outcome measures were unlikely to bias the results; there is no evidence that outcomes were selectively reported and there is no evidence of other sources of bias. The only criterion that was not accomplished was that the authors did not pre‐specify the shape of the intervention effect.
Effects of interventions
See: Table 1
We performed a formal ITS analysis with published and unpublished data provided by the author of the included study (Muncada 1995). Data used were a time series of the number of nurses per year that had emigrated from the Philippines to the USA from 1954 to 1990 (Table 2). We considered 1968 as the year of introduction of the intervention (a new migration law in the USA). The number of points used to carry out the analysis was 13 before and 23 after the intervention. No transition time was considered. Each point provided corresponded to the number of nurses that emigrated from the Philippines to the USA per year.
1. Number of Filipino nurses that migrated to the USA 1955 to 1990.
| Observation | Time (year) | Number of Philippine nurse immigrants to the USA |
| 1 | 1955 | 13 |
| 2 | 1956 | 22 |
| 3 | 1957 | 23 |
| 4 | 1958 | 54 |
| 5 | 1959 | 44 |
| 6 | 1960 | 64 |
| 7 | 1961 | 45 |
| 8 | 1962 | 58 |
| 9 | 1963 | 79 |
| 10 | 1964 | 43 |
| 11 | 1965 | 41 |
| 12 | 1966 | 137 |
| 13 | 1967 | 435 |
| 14 | 1968 | 884 |
| 15 | 1969 | 784 |
| 16 | 1970 | 951 |
| 17 | 1971 | 1549 |
| 18 | 1972 | 1273 |
| 19 | 1973 | 997 |
| 20 | 1974 | 1245 |
| 21 | 1975 | 1748 |
| 22 | 1976 | 1529 |
| 23 | 1977 | 1680 |
| 24 | 1978 | 1680 |
| 25 | 1979 | 1462 |
| 26 | 1980 | 1536 |
| 27 | 1981 | 1611 |
| 28 | 1982 | 1685 |
| 29 | 1983 | 1539 |
| 30 | 1984 | 1393 |
| 31 | 1985 | 1698 |
| 32 | 1986 | 1903 |
| 33 | 1987 | 1899 |
| 34 | 1988 | 1537 |
| 35 | 1989 | 1704 |
| 36 | 1990 | 1500 |
The segmented regression analysis of the time series showed a significant immediate increase of 807.6 (95% confidence interval (CI) 480.9 to 1134.3) more nurses migrating to the USA annually after the intervention. This represents a relative increase of 5000% over the underlying pre‐intervention trend (Figure 2). We did not find any differences between the year‐to‐year variations (slope of the underlying trends) between the pre‐ and post‐interventions periods.
2.
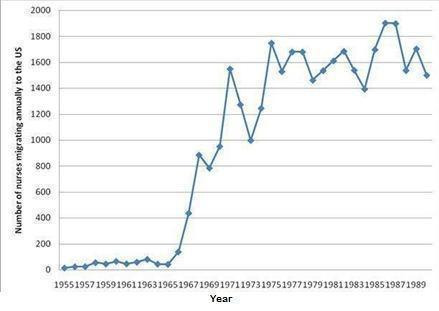
Source: graph based on published and unpublished data from the author of Muncada 1995 (Felipe Muncada)
At five years after introducing the intervention, the absolute difference between the number of nurses that migrated annually to the USA compared with the number predicted by the underlying trend before the intervention was 982 (95% CI 205 to 1758). Summing up, the introduction of law regulating migration increased the number of nurses migrating to USA without a significant change in the year‐to‐year variation in migration.
Discussion
Summary of main results
After a comprehensive search of electronic databases and other sources, we found only one study evaluating an intervention to control emigration of health professionals from LMICs.
Although the included study was not published as an interrupted time series, it provided sufficient data to allow re‐analysis to assess the effects of a modification in immigration law in the USA on the number of Philippine nurses that emigrated to that country. The study indicates that the implementation of this law produced a significant increase in the number of these professionals emigrating to the USA.
Our search strategy identified a number of non‐randomised studies of strategies implemented in some countries to regulate the emigration of health professionals from LMICs (see Excluded studies). We divided the interventions identified into two main groups: regulatory interventions for the recruitment of health professionals in high‐income countries (HICs) and incentives to retain professionals in LMICs. Information from these excluded studies is presented below in order to illustrate the range of interventions that might be used to regulate the emigration of health professionals from LMICs. Such interventions should be evaluated in the future using more rigorous designs.
Regulatory interventions
Buchan 2002 reported a number of regulatory interventions. Two initiatives were implemented in the United Kingdom to regulate the recruitment of health workers from LMICs: firstly, guidelines published in 1999 indicated specifically that National Health Service (NHS) employers should avoid direct recruitment from South Africa and the Caribbean, and set out good practice guidelines for international recruitment. The guidelines did not cover non‐NHS employers and recruitment agencies. In 2001, a Code of Practice established that “NHS employers should not target developing countries for recruitment of healthcare personnel unless the government of that country formally agrees via the Department of Health”.
Other initiatives identified were: visa requirements for foreign health professionals; labour market tests and other regulations necessary to justify the need for employment of foreign professionals (including language requirements); and pre‐employment confirmation by a professional body (e.g. a local Medical Council or Nursing Board) of the applicant’s qualifications and skills (Manning 2007).
Bach 2007 describes several interventions to regulate nurse migration to the UK. It tries to answer to what extent have forms of ‘soft regulation’, notably codes of practice on international recruitment, been effective measures in regulating the movement of nurses. Some of these regulations are referred as the “'NHS Plan”, implemented in 2000.
Bhagwati 1976 evaluates the effects of the modification of migratory law in the USA, called "'Act of 1965"'. It evaluates the situation of all high‐level, skilled or professional, technical and similar workers, and provides some separate data on physicians and surgeons.
Rao 2003 evaluates the impact of current graduate medical education and immigration policies among psychiatry residents during the 1990s in the USA. The study compares the roles played by international medical graduates in contrast to medical graduates from the USA.
Mejía 2004 describes actions taken by countries to regulate migration. The study is part of the WHO's Multinational Study of the International Migration of Physicians and Nurses. It includes a statistical report on stocks and flows of migrant physicians and nurses for 137 countries.
Xu 2005 analyses the theoretical effects of overseas recruitment and international recruitment agencies. It makes special mention of interventions in China with contradictory effects. On the one hand, the authorities have implemented and publicised improvements in the socioeconomic status of nurses (ineffectively, according to the authors) but, on the other hand, the authorities have opened a new center providing the certification test needed to work abroad.
Martineau 2006 describes the potential impact of eight national level and international codes of practice or similar instruments that were introduced to encourage ethical recruitment of health professionals, in order to protect source countries.
Herfs 2007 examines both national and university policies in ten European Economic Area (EEA) countries, including foreign medical degrees and the development of additional programmes for non‐EEA doctor (diploma evaluation, medical‐knowledge tests, language requirements, length of additional programmes, etc.).
Masselink 2009 and Masselink 2010 explore the expansion and commercialisation of nursing education and the role of nursing schools as "migrant institutions" in promoting the link between nursing education and migration.
Financial and non financial incentives
Chimbari 2008 reported a number of financial and non financial incentives for health professionals that were implemented in Zimbabwe. These incentives included the following.
Regular reviews of salaries and allowances, and rewards/incentives for high performers.
Staff with medical qualifications, technical or professional, could receive a medical payment at a rate of 70% of their basic salary, as additional payment while non‐medical staff working within health institutions or in hazardous environments, such as mortuary attendants and ambulance drivers, could receive a payment at a rate of 20% additional to their basic salary.
Study opportunities and low‐interest student loans to those who have served in the public sector for more than two years.
Implementation of (regulated) private consulting during their normal working days.
Accommodation and reliable transport, with vehicle purchase schemes for critical members of staff.
Some incentives that address social needs, such as the need for housing, staff transport, childcare facilities and assistance in procuring basic food items, for example, by providing a canteen.
Developing human resource information systems (HRIS).
Offering better management, implementing worker loss‐abatement strategies and accelerating staff appointments to vacant positions.
Lorenzo 2005 reports incentives implemented by the Government of the Philippines to promote responsible emigration. These included better employment opportunities and modes of engagement in overseas labour markets, as well as promoting the reintegration of migrants upon their return. Instruments developed to this end included: pre‐departure orientation seminars on the laws, customs and practices of destination countries; model employment contracts ensuring that the prevailing market conditions are respected and protecting the welfare of overseas workers; a system of accreditation of foreign employers; the establishment of overseas labour offices (POLOs) that provide legal, medical and psycho‐social assistance to Filipino overseas workers; a network of resource centres for the protection and promotion of workers’ welfare and interests; and reintegration programmes that provide skills training and assist returning migrants to invest their remittances and develop entrepreneurship.
Kugler 2003 evaluates re‐licensing requirements for Soviet trained physicians that immigrated to Israel. An immigrant re‐training assignment rule used by the Ministry of Health in Israel provided an exogenous source of variation in re‐licensing outcomes (including the wages of high‐skilled immigrant physicians and the quality of service).
Mufunda 2007 describes an innovative curriculum oriented to increase the retention of trained human resources in a School of Medicine in Zimbabwe. Several curricular innovations were incorporated. However, early patient contact and community attachment were the main changes sustained during the course of the study.
Kaushik 2008 assesses different types of admission and awards to medical students, and the relationship of these interventions with performance and the probability of emigrating in India.
Masango 2008 assesses the impact of non‐financial incentives on the retention of health sector workforce in Swaziland. These incentives included training and professional development, supervision schemes (supportive supervision and feedback) and staff welfare support (medical aid).
Barnighausen 2009 describes a health care education scholarship that is conditional on the recipient committing to work for several years after graduation in the area of delivering ART in sub‐Saharan Africa.
Moullan 2009 analyses the effects of foreign aid in the health sector on the medical brain drain using a database of physicians from 192 source countries to 17 destination countries. It also analyses whether the effects of foreign aid for health differs in a context of good governance (in relation to corruption, inflation).
Bourgain 2010 compares scenarios with and without substitution strategies (replacing highly‐qualified by less‐qualified health personnel) through a simulation method based on data from Ghana's medical sector.
Wiwanitkit 2011 evaluates Thailand's mandatory health service. Since 1989 all early‐career health workers from public professional schools serve in rural areas as government employees in order to maintain the rural health workforce. In the context of recent changes that streamed healthcare workers from mandatory rural service to urban private hospitals, a number of strategies have been implemented in an attempt to solve the shortage of rural healthcare workers. These strategies included a one‐year rural service prerequisite for specialist training for all new medical graduates; a special programme in medical schools to produce rural physicians; setting a special salary rate for rural physicians; and founding new medical schools in rural areas.
Overall completeness and applicability of evidence
As already mentioned, the only study included in this review was an ITS that assessed one of many possible interventions to regulate the emigration of health professionals from LMICs to HICs. Indeed, we did not identify any randomised studies that were eligible for inclusion in this review. Major issues precluding randomisation may include that some of the interventions (such as regulation) can only be implemented at national level; there may be resistance from professional groups to randomisation; and the complexity of the interventions may pose practical difficulties for trials. While the complexity of these interventions may make using rigorous designs more difficult, it also means that such designs are needed, since other study designs may not be at higher risk of bias. We believe our decision to focus on randomised controlled trials (RCTs), non‐RCTs, controlled before‐and‐after (CBA) and interrupted time series (ITS) studies is therefore justified.
Within the topic of the regulation of emigration, there are a number of relevant questions other than effectiveness that could be addressed using other forms of evidence. Although beyond the scope of this review, these questions include motivational factors behind decisions to emigrate, and the preferences of health professionals in LMICs regarding incentives to remain in their country of origin.
Some specific considerations should be mentioned regarding the peculiar conditions related to the emigration of Philippine nurses. As was described previously (Muncada 1995; WHO 2006), the Philippines has a public policy of encouraging the emigration of nurses to other countries. This is not the case in most LMICs (Buchan 2004b) ‐ a situation that should be considered when applying findings from the Philippines to other settings.
Quality of the evidence
Although the included study had a low risk of bias, it is difficult to draw robust conclusions from only one study.
Potential biases in the review process
This review did not formally explore publication bias because of the limited number of studies included. However the comprehensiveness of the search strategy makes it is unlikely that eligible studies were missed.
Agreements and disagreements with other studies or reviews
As far as we know, this is the first systematic review focusing on this type of evidence for this topic. We found one systematic review that assessed motivational factors and retention of health workers in LMICs and which included a wider range of study designs, from quantitative to qualitative methods (Willis‐Shattuck 2008). This review identified several factors that probably influence the intention of health professionals to emigrate. However, it did not identify studies that rigorously assessed the effects of interventions to control emigration.
Given the similarities between strategies to retain health professionals in their countries and interventions to increase the proportion of health professionals practising in underserved communities or in rural areas, it is relevant to mention that a recent Cochrane Review on the latter topic (Gobler 2009) did not identify any studies assessing such interventions.
Another recent document from the World health Organization (WHO) (WHO 2010) that summarises evidence and recommendations about strategies to increase access to health workers in remote and rural areas found only observational studies for most relevant educational, regulatory and financial strategies. This highlights again the lack of rigorous evidence in this area.
Authors' conclusions
Implications for practice.
The review identified only one study of the effectiveness of an intervention to modify emigration of health professionals from low‐ and middle‐income countries (LMIC) to high‐income countries (HICs). This regulatory intervention, implemented in a HIC, increased the movement of health professionals from a LMIC. This evidence highlights the role and responsibility of HICs on this issue. These countries could use regulatory policies to help reduce (rather than increase) the deleterious effects on LMICs' health systems of the massive emigration of health professionals to richer countries.
Available evidence does not provide guidance on which interventions to control emigration are effective and therefore rigorous evaluation is needed of any interventions that are implemented.
Implications for research.
There is an important knowledge gap about the effects of policy interventions in HICs and LMICs that could regulate the movement of health professionals from LMICs. The range of interventions reported from different countries, such as financial rewards, career development, continuing education, hospital infrastructure, resource availability, hospital management and recognition of health professionals, need to be assessed from the perspective of LMICs and with adequate study methodologies.
Another relevant issue is the lack of good data from LMICs regarding the emigration of their health workers. New initiatives to improve data collection need to be implemented, as a prerequisite for conducting more informative research in the field. A good example of this is the database of health professionals' emigration from Africa that has been published by Clemens and Petterson (Clemens 2006). This could be reproduced in other regions.
Finally, it would be very useful for future research to consider regional differences in the migration of health professionals, taking into account the specific features of Sub‐Sahara Africa, the Caribbean or the South East Asian regions (Chikanda 2005; Dal Poz 2006; Hawkes 2009).
Feedback
Comment from Jih‐I Yeh, 6 October 2013
Summary
The title of this review is "Interventions to reduce emigration of health care professionals from low‐ and middle‐income countries". The included references should study total number of emigrated health care professionals or representative indicators of that number in low‐ and middle‐income countries. The number of Philippines nurses emigrated to the US was not equivalent to nor correlated well with the total number of emigrated Philippines nurses after the oil crisis in the 1970s[1]. This was particularly clear again after 1995[2]. While the number of nurses emigrated to US was limited by US law at around 1,700 per year, the number of land‐based Filipino workers moved overseas increased from 12,051 in 1975 to 355,346 in 1989[3] and more nurse worked in other countries so Saudi Arabia surpassed US to become the largest employer of Filipino nurses overseas[1,2].
Muncada did not analyze his data using interrupted time series analysis. The US "Immigration and Nationality Act of 1965" was a well recognized factor that had great impact on Philippine emigration to US, but other well known factors during the same period that might potentially be more important in sending Philippines workers overseas. For example, the declaration of martial law in 1972, oil crisis in 1973, a national policy to deploy Filipino workers overseas[1], and the number of nursing schools increased from 16 in 1950 to around 470 in 2010[4,5]. All but the oil crisis were domestic policies impacting Filipino nurse migration, therefore, more pertinent interventions to consider for this review. The interrupted time series analysis should be on the total number of Filipino nurse working overseas and competing factors be tested before proposing an interpretation. I think the interrupted time series analysis was not appropriate here. Considering the original goal of this review, the Muncada study should also be excluded from this review.
References:
1. Ball RE. Divergent development, racialised rights: globalised labour markets and the trade of nurses—The case of the Philippines. Women’s Studies International Forum 27 (2004) 119– 133.
2. Lorenzo FM, Dela FRJ, Paraso GR, Villegas S, Isaac C, Yabes J, Trinidad F, Fernando G, Atienza J. “Migration of Health Workers: Country Case Study” The Institute of Health Policy and Development Studies, National Institute of Health, September 2005.
3. Asis MMB. How International Migration Can Support Development: A Challenge for The Philippines. Segundo Semestre, 2006, pp. 96‐122. ISSN 1946‐4037. Available at: http://www.redalyc.org/articulo.oa?id=6600070
4. Masselink LE, Lee DSY. Nurses, Inc.: Expansion and commercialization of nursing education in the Philippines. Social Science & Medicine 71(2010):166‐172.
5. Choo V. Philippines losing its nurses, and now maybe its doctors. The Lancet • 361(2003):1356
Reply
Thank you very much for your comments. Although Muncada 1995 did not report an interrupted time series analysis, they did report time series data and it was possible for us to reanalyze those data. The reanalysis adhered to guidance provided by the Cochrane Effective Practice and Organisation of Care group (EPOC 2013) and the reanalyzed results met our inclusion criteria, as per the protocol for this review (Peñaloza 2009).
The points you make about other explanatory factors besides the USA Immigration Law of 1965 that could affect the emigration of Philippine nurses to USA are correct and we thank you for pointing these out. We acknowledge we should have mentioned these in our discussion and will do so when we update this review, by the end of this year. We also agree that it is important to consider the findings of this analysis in relation to emigration to other countries besides the USA, both in the discussion and implications for practice. Although the analysis supports our conclusion that the decrease in restrictions on immigration to the USA probably led to an increase in Philippine nurses emigrating to the USA, this might not have had a measurable impact on the total number of Philippine nurses emigrating to the USA and other countries.
It seems unlikely that those other factors could explain the immediate increase in the number of nurses migrating from the Philippines to the USA, but they might have contributed to subsequent trends. Consequently, we believe that our conclusion that the reduction in restriction on immigration probably led to an immediate increase (GRADE: moderate quality of evidence) is justified. However, we agree that the longer‐term effects of that change are less certain, since other factors including those you identified might have affected subsequent trends.
References
(EPOC 2013) Effective Practice and Organisation of Care (EPOC). Interrupted time series (ITS) analyses. EPOC Resources for review authors. Oslo: Norwegian Knowledge Centre for the Health Services; 2013. Available at: http://epocoslo.cochrane.org/epoc‐specific‐resources‐review‐authors
(Peñaloza 2009) Peñaloza B, Rada G, Pantoja T, Bastías G, Herrera C. Interventions for controlling emigration of health professionals from low and middle‐income countries (Protocol). Cochrane Database of Systematic Reviews 2009, Issue 1. Art. No.: CD007673. DOI: 10.1002/14651858.CD007673.
Contributors
Feedback (comment) from:
Jih‐I Yeh, Department of Family Medicine, Buddhist Tzu‐Chi General Hospital and Tzu‐Chi University, Hualien, Taiwan
Response to feedback (comment) from:
Dr Blanca Peñaloza, Department of Family Medicine, Faculty of Medicine, Pontificia Universidad Católica de Chile, Santiago
What's new
| Date | Event | Description |
|---|---|---|
| 4 July 2014 | Feedback has been incorporated | The review authors have replied to feedback received via The Cochrane Library |
Acknowledgements
We would like to thank the Alliance for Health Policy and Systems Research (WHO) for providing funds to support this review. The following people have also contributed from different perspectives: Andy Oxman (technical advice), Delanyo Dovlo (provision of original manuscripts), Stephen Bach and James Buchan, (provision of additional information about new resources to search for potentially included studies), Craig M. Ramsay (help with the statistical analysis) and Philip Muncada who provided us with the raw data from the included study for the ITS re‐analysis.
Appendices
Appendix 1. EPOC Register search strategy
| EPOC Register Date of search: 15 March 2011 |
| Brain drain* or immigr* or emigra* or migrat* or migrant or diáspora? or (border* and crossing) AND health manpower or human resources or human resource or foreign professional personnel* |
Appendix 2. CENTRAL search strategy
| Host: Wiley 1898 to 2 March 2011 |
| 1. brain drain* 2. immigr* 3. emigra* 4. migrat* 5. migrant* 6. diaspora* 7. (Border* AND Crossing*) 8. "Emigration and Immigration"[Mesh] 9. "Transients and Migrants"[Mesh] 10. "Emigrants and Immigrants"[Mesh] 11. "Foreign Professional Personnel"[Mesh] 12. #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 13. (health* OR medical) AND (profession* OR personnel OR staff OR worker* OR manpower OR workforce) 14. "Health Personnel"[Mesh] 15. "Health Manpower"[Mesh] 16. nurse*:ti,ab,kw 17. physician*:ti,ab,kw 18. doctor*:ti,ab,kw 19. dentist*:ti,ab,kw 20. midwife*:ti,ab,kw 21. midwive*:ti,ab,kw 22. pharmacist*:ti,ab,kw 23. #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 24. #12 AND #23 |
Appendix 3. MEDLINE search strategy
| Host: PubMed 1809 to 5 March 2011 |
| 1. brain drain [All Fields] 2. immigr* [All Fields] 3. emigra* [All Fields] 4. migrat* [All Fields] 5. migrant* [All Fields] 6. diaspora* [All Fields] 7. Border*[All Fields] AND Crossing[All Fields] 8. "Emigration and Immigration"[Mesh] 9. "Transients and Migrants"[Mesh] 10. "Emigrants and Immigrants"[Mesh] 11. "Foreign Professional Personnel"[Mesh] 12. #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 13. (health* OR medical) AND (profession* OR personnel OR staff OR worker* OR manpower OR workforce) 14. "Health Personnel"[Mesh] 15. "Health Manpower"[Mesh] 16. nurse* [All Fields] 17. physician* [Title/Abstract] 18. doctor* [Title/Abstract] 19. dentist* [Title/Abstract] 20. midwife* [Title/Abstract] OR midwiv* [Title/Abstract] 21. pharmaceu* [Title/Abstract] 22.#13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 23. randomized controlled trial[pt] 24. random* [All Fields] 25. intervention* [All Fields] 26. control[Title/Abstract] or controlled[Title/Abstract] 27. effect* [All Fields] 28. evaluat* [All Fields] 29. #23 OR #24 OR #25 OR #26 OR #28 30. #12 AND # 22 AND #29 |
Appendix 4. EMBASE search strategy
| Host: OVID 1986 to 26 March 2011 |
| 1. brain drain.tw. 2. immigr$.tw. 3. emigra$.tw. 4. migrat$.tw 5. migrant$.tw 6. diaspora$.tw 7. (border and crossing).tw. 8. immigration/ 9. migration/ 10. immigrant/ 11. population migration/ 12. Foreign Worker/ 13. OR / 1‐12 14. ((health$ or medical) and (profession$ or personnel or staff or worker$ or manpower or workforce)).tw. 15. exp Health Care Personnel/ 16. Health Care Manpower/ 17. Health Practitioner/ 18. nurse$.ti. or nurse$.ab. 19. physician$.ti. or physician$.ab. 20. doctor$.ti. or doctor$.ab. 21. dentist$.ti. or dentist$.ab. 22. midwife$.ti. or midwife$.ab. 23. midwive$.ti. or midwive$.ab. 24. pharmacist$.ti. or pharmacist$.ab. 25. OR / 14‐24 26. randomized controlled trial/ 27. intervention study/ 28. control group/ 29. control$.tw. 30. intervention$.tw. 31. effect$.tw. 32. evaluat$.tw. 33. random$.tw. 34. OR /25‐32 35. 13 AND 25 AND 34 |
Appendix 5. CINAHL search strategy
| Host: EBSCO 1981 to 5 March 2011 |
| 1. MH "Experimental Studies+" 2. MH "Quasi‐Experimental Studies+" 3. MH "Repeated Measures" 4. controlled N4 study 5. controlled N4 trial 6. TX random* 7. TX time serie 8. TX controlled before 9. TX (pre‐test or pretest or post‐test) and control* 10. S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 11. TX brain drain* 12. TX immigr* 13. TX emigra* 14. TX migrat* 15. TX migrant* 16. TX diaspora* 17. TX out‐migrants* 18. (TI border* OR AB border*) and (TI crossing* OR AB crossing*) 19. MH "Emigration and Immigration" 20. MH "Immigrants" 21. MH "Foreign Nurses" 22. MH "Foreign Professional Personnel" 23. MH "Career Mobility, International" 24. S11 or S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22 or S23 25. (health* or medical) and (profession* or personnel or staff or worker* or manpower or workforce) 26. MH "Health Personnel+" 27. MH "Health Manpower+" 28. TI nurse* or AB nurse* or MW nurse* 29. TI physician* or AB physician* or MW physician* 30. TI doctor* or AB doctor* or MW doctor* 31. TI dentist* or AB dentist* or MW dentist* 32. TI midwife* or AB midwife* or MW midwife* 33. TI midwive* or AB midwive* or MW midwive* 34. TI pharmacist* or AB pharmacist* or MW pharmacist* 35. S25 or S26 or S27 or S28 or S29 or S30 or S31 or S32 or S33 or S34 36. S10 and S24 and S35 |
Appendix 6. LILACS search strategy
| Host: BIREME, iAH form (Spanish interface) 1980 to 7 March 2011 |
| CT COMPARATIVE STUDY or random$ or intervention$ or intervencion or intervenção or control$ or efect$ or effect$ or efet$ or evaluat$ or evaluac$ or Avaliaç$ [Palabras] AND (brain and drain) or (immigr$ or inmigr$ or imigra$) or emigr$ or (migrat$ or migrac$ or Migraç$) or (migrant$) or diaspora$ or ((Border$ and crossing) or (frontera and cruzar) or (fronteira and passar)) or [MH]"Migración Internacional" or [MH]"Migrantes" or [MH]"Personal Profesional Extranjero" [Palabras] AND (((health$ or medic$) and profession$) or (profesion$ and (salud or sanitari$)) or (profissi$ and saude)) or (nurse$ or enfermer$ or enfermeir$) or (physician$ or medico$) or (doctor$ or doutor$) or hospitalist$ or dentist$ or (midwi$ or matrona$ or obstetriz) or (pharmacist$ or farmaceutico$) or [MH]"Personal de Salud" or [MH]"Recursos Humanos en Salud" [Palabras] |
Appendix 7. ERIC search strategy
| Host: OCLC First search 1985 to 3 March 2011 |
| 1. ab: RANDOM* or ti: RANDOM* 2. ab: intervent* or ti: intervent* 3. ab: COMPAR* or ti: COMPAR* 4. ab: CONTROL* or ti: CONTROL* 5. ab: EXPERIMENT* or ti: EXPERIMENT* 6. ab: effect* or ti: effect* 7. ab: evaluat* or ti: evaluat* 8. or/1‐7 9. su:immigrant or su:immigrants or su:immigration 10. su:migrant or su:migrants or su:migration or su:migratory 11. su:emigrants or su:emigration 12. su: diaspora* 13. ti:immigr* or ab:immigr* 14. ti:emigra* or ab:emigra* 15. ti:migrat* or ab:migrat* 16. (ab:brain or ti:brain) and (ti:drain or ab:drain) 17. (ab:border or ti:border) and (ti:crossing or ab:crossing) 18. or/9‐17 19. (ti:health* or ab:health* or ti:medical* or ab:medical*) and ((ti:profession* or ab:profession*) or (ti:personn* or ab:personn*) or (ti:manpower or ab:manpower)) 20. su:nurse or su:nurses 21. su:physician or su:physicians 22. su:dentists 23. su:pharmacist or su:pharmacists 24. ti:nurse* or ab:nurse* 25. ti:physician* or ab:physician* 26. ti:dentist* or ab:dentist* 27. ti:midwi?e* or ab:midwi?e* 28. ti:pharmacist* or ab:pharmacist* 29. or/19‐28 30. 8 and 18 and 29 |
Appendix 8. Social and Science Citation Index search strategy
| Host: ISI web of science 1988 to 8 March 2011 |
| 1. TS=random* 2. TS=intervention* 3. TS=control* 4. TS=effect* 5. TS=evaluat* 6. #1 OR #2 OR #3 OR #4 OR #5 7. TS=migrat* 8. TS=migrant* 9. TS=diaspora* 10. TS=immigr* 11. TS=emigra* 12. (TS=brain) and (TS=drain) 13. (TS=border) and (TS=cross*) 14.#7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 15. (TS=health* or TS=medical) and (TS=profession* or TS=personn* or TS=staff or TS=worker* or TS=workforce or TS=manpower) 16. TS=nurse* 17. TS=physician* 18. TS=doctor* 19. TS=dentist* 20. TS=midwife* 21. TS=midwive* 22. TS=pharmacist* 23. #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 24. #6 AND #14 AND #23 |
Appendix 9. SocINDEX search strategy
| Host: EBSCO 1908 to 11 March 2011 |
| 1. ab RANDOM* or ti RANDOM* 2. ab intervent* or ti intervent* 3. ab COMPAR* or ti COMPAR* 4. ab CONTROL* or ti CONTROL* 5. ab EXPERIMENT* or ti EXPERIMENT* 6. ab effect* or ti effect* 7. ab evaluat* or ti evaluat* 8. S1 or S2 or S3 or S4 or S5 or S6 or S7 9. SU migration 10. DE "MIGRANT labor" 11. DE "EMIGRATION & immigration" 12. DE "IMMIGRANTS" 13. DE "BRAIN drain" 14. DE "SKILLED labor" 15. AB migrat* or TI migrat* 16. AB migrant* or TI migrant* 17. AB diaspora* or TI diaspora* 18. AB immigr* or TI immigr* 19. AB emigra* or TI emigra* 20. (AB brain or TI brain) and (AB drain or TI drain) 21. (AB border or TI border) and (AB cross* or TI cross*) 22. S9 or S10 or S11 or S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 23. DE "MEDICAL personnel" 24. DE "NURSES" 25. DE "PHARMACISTS" 26. DE "PHYSICIANS" 27. DE "MEDICINE" 28. (TI health* or AB health* or TI medical or AB medical) and (TI profession* or AB profession* or TI personn* or AB personn* or TI manpower or AB manpower) 29. TI nurse* or AB nurse* 30. TI physician* or AB physician* 31. TI hospitalist* or AB hospitalist* 32. TI dentist* or AB dentist* 33. TI midwi?e* or AB midwi?e* 34. TI pharmacist* or AB pharmacist* 35. S23 or S24 or S25 or S26 or S27 or S28 or S29 or S30 or S31 or S32 or S33 or S34 36. S8 and S22 and S35 |
Appendix 10. Search strategy EconLit
| Host: EBSCO 1981 to 8 March 2011 |
| 1. DE "Economic Development: Human Resources; Human Development; Income Distribution; Migration" 2. DE "Geographic Labor Mobility; Immigrant Workers" 3. DE "International Migration" 4. DE "Demographic Trends and Forecasts; General Migration" 5. TX (brain N3 drain*) 6. TX immigr* 7. TX emigra* 8. TX migrat* 9. TX migrant* 10. TX diaspora* 11. TX out‐migrants* 12. (border* N4 crossing*) 13. S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10 or S11 or S12 14. DE "health production" 15. DE "health, education, and welfare: general" 16. DE "health: general" 17. DE "health: government policy; regulation; public health" 18. DE "health: other" 19. (health* or medical) and (profession* or personnel or staff or worker* or manpower or workforce) 20. TX nurse* 21. TX physician* 22. TX doctor* 23. TX dentist* 24. TX midwife* or midwiv* 25. TX pharmacist* 26. S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22 or S23 or S24 or S25 27. TX random* or intervention* or control* or compar* or evaluat* or time or pretest or posttest or pre test or post test or impact* or chang* or effect* or experiment* 28. S13 and S26 and S27 |
Appendix 11. Search strategy WHOLIS
| WHOLIS Date of search: 20 March 2011 |
| subject ""BRAIN DRAIN" or "FUGA DE CEREBROS" or "EXODE DES COMPETENCES" or "TRANSIENTS AND MIGRANTS" or "TRANSEUNTES Y MIGRANTES" or "POPULATION PASSAGE ET IMMIGRANTS" or EMIGRATION AND IMMIGRATION or "EMIGRATION ET IMMIGRATION" or "MIGRACION INTERNACIONAL"" OR words or phrase "EMIGRATION or IMMIGRATION or MIGRATION or DIASPORA or EMIGRACION or INMIGRACION or MIGRACION" AND words or phrase "HEALTH or MEDICAL or NURSE$ or DOCTOR$ or DENTIST$ or MIDWIVE$ or PHARMACIST$ or SALUD or MEDIC$ or ENFERMER$ or MATRON$ or FARMACEUTIC$" |
Appendix 12. NLM Gateway search strategy
| NLM Gateway (HSRProj) Date of search: 31 March 2011 |
| migration OR (Brain AND drain) OR Emigration OR immigration |
Appendix 13. Methods issues reported in the protocol of this review
Data analysis
Reporting
For each study, we will report data in natural units. Where baseline results are available, we will report pre‐intervention and postintervention means or proportions for both study and control groups and the unadjusted and adjusted (for any baseline imbalance) absolute change from baseline will be calculated with 95% confidence limits.
Primary analyses will be based upon consideration of the primary outcome: the proportion of health professionals of a LMIC that emigrate.
We will present the results for all comparisons using a standard method of presentation where possible. For comparisons of RCTs, NRCTs, CBAs we will report (separately for each study design):
median effect size across included studies;
inter‐quartile ranges of effect sizes across included studies; and
range of effect sizes across included studies.
When a summary measure of effect cannot be computed we will use a random‐effects model, anticipating important heterogeneity across studies.
Exploring heterogeneity
If possible and relevant, we will prepare tables and box plots comparing effect sizes of included studies grouped according to potential effect modifiers. The main factors to consider will be the targeted professionals, type of intervention, conditions in the source and the recipient country and study quality. If a sufficient number of studies are available (a minimum of 10) we will use funnel plots to assess publication bias.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Muncada 1995.
| Methods | Univariate time series. We used published and unpublished data to develop an interrupted time series study. We carried out reanalysis using a segmented regression model that also adjusted for first order autocorrelation. | |
| Participants | Annual register of Philippine nurses that emigrated from the Philippines to the USA during the time period 1955 to 1990 | |
| Interventions | Regulatory intervention: modification of migratory law in the USA, called the 'Act of October 1965'. Implementation of this law was completed in 1968, considered the year of the intervention. This law modified the previous legislation by decreasing the restrictions on Eastern hemisphere immigrants to the USA. The law established an “annual limitation of 170,000 immigrants from Eastern Hemisphere, with no more than 20,000 immigrants from any country”. The abolition of the National Origins system gave an equal chance to persons from every country within each hemisphere to immigrate to the USA. | |
| Outcomes | Annual number of Philippine nurses that emigrated from the Philippines to the USA | |
| Notes | Reanalysed as an ITS study by the review team | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Was the intervention independent of other changes? | Low risk | The intervention occurred independently of other changes over time and the outcome was not influenced by other confounding variables during the study period |
| Was the shape of the intervention effect pre‐specified? | High risk | The author did not provide any explanation for the shape of the intervention effect because this was not part of the primary question of the original study |
| Was the intervention unlikely to affect data collection? | Low risk | Sources and methods of data collection were the same before and after the intervention |
| Was knowledge of the allocated interventions adequately prevented during the study? | Low risk | The outcomes were objective |
| Were incomplete outcome data adequately addressed? | Low risk | The type of outcome meant that there were no missing data (register of number of Philippine nurses that entered USA) |
| Was the study free from selective outcome reporting? | Low risk | There is no evidence that outcomes were selectively reported |
| Was the study free from other risk of bias? | Low risk | There is no evidence of other risks of bias |
ITS: interrupted time series
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Bach 2007 | Uncontrolled study evaluating different interventions to regulate nurse migration to the UK. Insufficient data to analyse as an ITS. It is not clear which is the principal intervention (they mentioned many). If we take one of the more identifiable interventions (the 'NHS Plan') that was implemented in the year 2000, it only has 2 pre intervention points and 3 post. |
| Barnighausen 2009 | Cost‐benefit analysis of a healthcare education scholarship that is conditional on the recipient committing to work for several years after graduation delivering ART in sub‐Saharan Africa |
| Bhagwati 1976 | Study evaluating the effects of the modification of migratory law in the USA, called 'Act of 1965'. Insufficient data to analyse as an ITS |
| Bourgain 2010 | Simulation study which compared scenarios with and without substitution strategies by using data from Ghana's medical sector |
| Buchan 2002 | Study evaluating the impact of the 1999 ethical recruitment guidelines in the UK. Uncontrolled study. Insufficient data to analyse as an ITS: it had a total of 4 points in the time series with only one of them previous to the intervention. |
| Buchan 2004a | Case study. Literature data and interviews with key informants, international recruitment agencies and international organisations in the UK, Ghana and Barbados. Evaluates some interventions, but using qualitative methodology |
| Herfs 2007 | Study on regulatory strategies to deal with doctors from non European Economic Area (EEA) in EEA countries. Qualitative methodology. |
| Kaushik 2008 | Retrospective cohort study assessing the relationship between medical students' performance and probability of emigrating in India. Type of admission and awards can be assumed as an intervention, but it does not have any time series data. |
| Kugler 2003 | Observational study evaluating an occupational license using novel data on Soviet‐trained physicians that immigrated to Israel. It does not have any time series data. |
| Lorenzo 2005 | Country case study of the Philippines. Evaluates some interventions, but using qualitative methodology. |
| Manning 2007 | Uncontrolled study evaluating different interventions to regulate migration of health professionals in 10 South East Asian countries. It does not have any time series data. |
| Martineau 2006 | Study about codes of practice for international recruitment of health professionals. Qualitative methodology. |
| Masango 2008 | Study evaluating the impact of non financial incentives in retention of health sector workforce in Swaziland |
| Masselink 2009 | Study exploring the expansion and commercialisation of nursing education and the role of nursing schools as "migrant institutions" in promoting the link between nursing education and migration. Qualitative methodology. |
| Masselink 2010 | Study exploring the expansion and commercialisation of nursing education and the role of nursing schools as "migrant institutions" in promoting the link between nursing education and migration. Qualitative methodology. |
| Mejía 2004 | Observational study about the actions taken by countries to regulate migration. It does not have any time series data. |
| Moullan 2009 | Econometric study that analyses the effects of foreign aid in the health sector on the medical brain drain. The intervention "foreign health aid" does not allow us to ask the authors for data to carry out an ITS analysis. |
| Mufunda 2007 | Uncontrolled study about an innovative curricula, oriented to increase the retention of trained manpower in Zimbabwe. There is no evaluation of emigration data of health professionals in this study. |
| Rao 2003 | Study evaluating the impact of current graduate medical education (GME) and immigration policies in the USA. It does not have any time series data. |
| Wiwanitkit 2011 | Study evaluating Thailand's mandatory health service. Insufficient data to analyse as an ITS. |
| Xu 2005 | Theoretical study that examines the ethics of international nurse recruitment. |
ART: antiretroviral treatment ITS: interrupted time series
Differences between protocol and review
We did not search in the Sociological Abstracts database.
Contributions of authors
Blanca Peñaloza (BP) led the writing of the review with contributions from Gabriel Rada (GR) and Tomas Pantoja (TP). Gabriel Bastias (GB) and Cristian Herrera (CH) reviewed the draft version. Gabriel Rada designed and ran the search strategy and co‐ordinated the screening and selection process. Blanca Peñaloza, Gabriel Rada, Gabriel Bastias, Tomas Pantoja and Cristian Herrera reviewed the references and selected studies. Blanca Peñaloza and Tomas Pantoja assessed the risk of bias of the included studies.
Sources of support
Internal sources
Faculty of Medicine, Pontificia Universidad Catolica de Chile, Chile.
External sources
Alliance for Health Policy and Systems Research (WHO), Other.
Declarations of interest
The authors of the review do not have any conflicts of interest to declare.
Edited (no change to conclusions), comment added to review
References
References to studies included in this review
Muncada 1995 {published and unpublished data}
- Muncada FL. The labor migration of Philippine nurses to the United States. The labor migration of Philippine nurses to the United States. Catholic University of America, 1995. [Google Scholar]
References to studies excluded from this review
Bach 2007 {published data only}
- Bach S. Going global? The regulation of nurse migration in the UK. British Journal of Industrial Relations 2007;45(2):383‐403. [Google Scholar]
Barnighausen 2009 {published data only}
- Barnighausen T, Bloom DE. "Conditional scholarships" for HIV/AIDS health workers: educating and retaining the workforce to provide antiretroviral treatment in sub‐Saharan Africa. Social Science & Medicine 2009;68(3):544‐51. [DOI] [PubMed] [Google Scholar]
Bhagwati 1976 {published data only}
- Bhagwati J. The brain drain. International Social Science Journal 1976;28(4):691. [Google Scholar]
Bourgain 2010 {published data only}
- Bourgain A, Pieretti P, Zou B. The migration of medical workers in Sub‐Saharan Africa and substitution policy [Migration des professionnels de sante de pays d'Afrique subsaharienne et politique de substitution]. Revue Economique 2010;61(6):1011‐22. [Google Scholar]
Buchan 2002 {published data only}
- Buchan J. International recruitment of nurses: United Kingdom case study. London, Royal College of Nursing; World Health Organization; International Council of Nurses 2002.
Buchan 2004a {published data only}
- Buchan J, Dovlo D. International Recruitment of Health Workers to the UK: A Report for DFID. DFID Health Systems Resource Centre (www.healthsystemsrc.org) 2004.
Herfs 2007 {published data only}
- Herfs PG, Kater L, Haalboom JR. Non‐EEA doctors in EEA countries: doctors or cleaners?. Medical Teacher 2007;29(4):383‐9. [DOI] [PubMed] [Google Scholar]
Kaushik 2008 {published data only}
- Kaushik M, Jaiswal A, Shah N, Mahal A. High‐end physician migration from India. Bulletin of the World Health Organization 2008;86(1):40‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kugler 2003 {published data only}
- Kugler A, Sauer RM. Doctors without Borders: The Returns to an Occupational License for Soviet Immigrant Physicians in Israel. RePEc Project 2003.
Lorenzo 2005 {published data only}
- Lorenzo F. Migration of health workers: country case study Philippines. Institute of Health Policy and Development Studies, Geneva, International Labour Office 2005.
Manning 2007 {published data only}
- Manning C, Sidorenko A. The regulation of professional migration: insights from the health and IT sectors in ASEAN. World Economy 2007;30(7):1084‐113. [Google Scholar]
Martineau 2006 {published data only}
- Martineau T, Willetts A. The health workforce: managing the crisis ethical international recruitment of health professionals: will codes of practice protect developing country health systems?. Health Policy 2006;75(3):358‐67. [DOI] [PubMed] [Google Scholar]
Masango 2008 {published data only}
- Masango S, Gathu K, Sibandze S. Retention strategies for Swaziland's health sector workforce: assessing the impact of non‐financial incentives. Harare, Ministry of Health Swaziland, EQUINET, ECSA‐HC. EQUINET. Discussion Paper Series N° 68. 2008.
Masselink 2009 {published data only}
- Masselink L, Lee SY. Title: Nurses, Inc.: Philippine nursing schools as migrant institutions. Conference Papers ‐ American Sociological Association. 2009.
Masselink 2010 {published data only}
- Masselink L, Lee SY. Nurses, Inc.: expansion and commercialization of nursing education in the Philippines. Social Science & Medicine 2010;71(1):166‐72. [DOI] [PubMed] [Google Scholar]
Mejía 2004 {published data only}
- Mejía A. Migration of physicians and nurses: a world wide picture: public health classics. Bulletin of the World Health Organization 2004;82(8):626‐30. [PMC free article] [PubMed] [Google Scholar]
Moullan 2009 {published data only}
- Moullan Y. Can Foreign Health Assistance Reduce the Medical Brain Drain?. IRES ‐ Institut de Recherches Economiques et Sociales 2009.
Mufunda 2007 {published data only}
- Mufunda J, Chatora R, Ndambakuwa Y, Samkange C, Sigola L, Vengesa P. Challenges in training the ideal doctor for Africa: lessons learned from Zimbabwe. Medical Teacher 2007;29(9):878‐81. [DOI] [PubMed] [Google Scholar]
Rao 2003 {published data only}
- Rao NR. Recent trends in psychiatry residency workforce with special reference to international medical graduates. Academic Psychiatry 2003;27(4):269‐76. [DOI] [PubMed] [Google Scholar]
Wiwanitkit 2011 {published data only}
- Wiwanitkit V. Mandatory rural service for health care workers in Thailand. Rural Remote Health 2011;11(1):1583. [PubMed] [Google Scholar]
Xu 2005 {published data only}
- Xu Y, Zhang J. One size doesn't fit all: ethics of international nurse recruitment from the conceptual framework of stakeholder interests. Nursing Ethics 2005;12(6):571‐81. [DOI] [PubMed] [Google Scholar]
Additional references
Bach 2003
- Bach S. International migration of health workers: labor and social issues (Working paper #209). Sectoral Activities Programme, International Labour Office 2003.
Buchan 2003
- Buchan J, Parkin T, Sochalski J. International nurse mobility: trends and policy implications. http://www.who/EIP/OSD/2003.3 (accessed July 2007).
Buchan 2004b
- Buchan J, Sochalski J. The migration of nurses: trends and policies. Bulletin of the World Health Organization 2004;82:587‐94. [PMC free article] [PubMed] [Google Scholar]
Chikanda 2005
- Chikanda A. Nurse migration from Zimbabwe: analysis of recent trends and impact. Nursing Inquiry 2005;12(3):162‐74. [DOI] [PubMed] [Google Scholar]
Chimbari 2008
- Chimbari MJ, Madhina D, Nyamangara F, Mtandwa H, Damba V. An assessment of the Zimbabwe government strategy for retention of health professionals. EQUINET Discussion Paper. Series 65.
Clemens 2006
- Clemens M, Petterson G. A New Database of Health Professional Emigration from Africa (Working Paper 95). Centre for Global Development(http://www.cgdev.org) August 2006. [http://www.queensu.ca/samp/migrationresources/Documents/DB_HealthProfessional_Emigration.pdf]
Cochrane Handbook
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 [September 2008]. The Cochrane Collaboration 2008. Available from www.cochrane‐handbook.org.
Connell 2007
- Connell J, Zurn P, Stilwell B, Awases M, Braichet JM. Sub‐Saharan Africa: Beyond the health worker migration crisis?. Social Science & Medicine 2007;64:1876‐91. [DOI] [PubMed] [Google Scholar]
Dal Poz 2006
- Dal Poz MR, Kinfu Y, Drager S, Kunyumen T, Diallo K. Counting health workers: definitions, data, methods and global results. Background paper for The World Health Report 2006. http://www.who.int/hrh/documents/en (accessed January 2008).
Diallo 2004
- Diallo K. Data on the migration of health care workers: sources, use and challenges. Bulletin of the World Health Organization 2004;82:601‐7. [PMC free article] [PubMed] [Google Scholar]
Dovlo 2003
- Dovlo D. The brain drain and retention of health professionals in Africa. A case study prepared for a regional training conference. Improving tertiary education in Sub‐Saharan Africa: things that work! 2003.
Dovlo 2004
- Dovlo D, Martineau T. A Joint Learning Initiative: Human Resources for Health and Development. A Review of the Migration of Africa's Health Professionals.. JLI Working Paper 4‐4 2004.
Dovlo 2007
- Dovlo D. Migration of nurses from Sub‐Saharan Africa: a review of issues and challenges. Health Services Research 2007;42:1373‐88. [DOI] [PMC free article] [PubMed] [Google Scholar]
Global Forum 2007
- Global forum on migration and development. http://www.gfmd.com (accessed October 2007).
Gobler 2009
- Grobler L, Marais BJ, Mabunda S, Marindi P, Reuter H, Volmink J. Interventions for increasing the proportion of health professionals practising in rural and other underserved areas. Cochrane Database of Systematic Reviews 2009, Issue 1. [DOI: 10.1002/14651858.CD005314.pub2] [DOI] [PubMed] [Google Scholar]
Handbook 2006
- Handbook on establishing effective labour migration policies in countries of origin and destination. www.gfmd‐fmmd.org/en/document‐library‐en/42 (accessed December 2007).
Hawkes 2009
- Hawkes M, Kolenko M, Shockness M, Diwaker K. Nursing brain drain from India. Human Resources for Health 2009;12(1):5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Martineau 2004
- Martineau T, Decker K, Bundred P. "Brain drain" of health professionals: from rhetoric to responsible action. Health Policy 2004;70(1):1‐10. [DOI] [PubMed] [Google Scholar]
OECD/WHO
- OECD/WHO. Policy Brief. International Migration of Health Workers. Improving International Cooperation to Address the Global Health Workforce Crisis. OECD Observer February 2010 (available in: http://www.oecd.org/document/47/0,3343,en_2649_33929_36506543_1_1_1_37407,00.html) (accessed April 2010).
Starfield 2007
- Starfield B, Fryer G. The primary care physician workforce: ethical and policy implications. Annals of Family Medicine 2007;5:486‐91. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stilwell 2003
- Stilwell B, Diallo K, Zurn P, Dal Poz MR, Adams O, Buchan J. Developing evidence‐based ethical policies on the migration of health workers: conceptual and practical challenges. Human Resources for Health 2003;1:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stilwell 2004
- Stilwell B, Diallo K, Zurn P, Vujicic M, Adams O, Dal Poz M. Migration of health care workers from developing countries: strategic approaches to its management. Bulletin of the World Health Organization 2004; Vol. 82:595‐600. [PMC free article] [PubMed]
United Nations 2006
- United Nations. International migration 2006, wall chart. www.un.org/esa/population/publications/2006migration_chart/migration2006.pdf (accessed October 2007).
WHO 2006
- Working together for health. World Health Report. World Health Organization 2006.
WHO 2010
- WHO's Global Policy Recommendations: increasing access to health workers in remote and rural areas through improved retention. World Health Organization 2010. [PubMed]
Willets 2004
Willis‐Shattuck 2008
- Willis‐ Shattuck M, Bidwell P, Thomas S, Wyness L, Blaauw D, Ditlopo P. Improving motivation and retention of health professionals in developing countries: a systematic review. BMC Health Service Research 2008;8:247. [DOI] [PMC free article] [PubMed] [Google Scholar]
World Bank
- The World Bank. Country Classification. http://data.worldbank.org/about/country‐classifications (accessed January 2008).