

Abstract
Background:
Randomized controlled trials (RCTs) are crucial in comparative research, and a careful approach to randomization methodology helps minimize bias. However, confounding variables like socioeconomic status (SES) and race are often underreported in orthopaedic RCTs, potentially affecting the generalizability of results. This study aimed to analyze the reporting trends of SES and race in RCTs pertaining to Achilles tendon pathology, considering 4 decades of data from top-tier orthopaedic journals.
Methods:
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and used PubMed to search 10 high–impact factor orthopaedic journals for RCTs related to the management of Achilles tendon pathology. The search encompassed all articles from the inception of each journal until July 11, 2023. Data extraction included year of publication, study type, reporting of SES and race, primary study location, and intervention details.
Results:
Of the 88 RCTs identified, 68 met the inclusion criteria. Based on decade of publication, 6 articles (8.8%) reported on SES, whereas only 2 articles (2.9%) reported on race. No RCTs reported SES in the pre-1999 period, but the frequency of reporting increased in subsequent decades. Meanwhile, all RCTs reporting race were published in the current decade (2020-2030), with a frequency of 20%. When considering the study location, RCTs conducted outside the United States were more likely to report SES compared with those within the USA.
Conclusion:
This review revealed a concerning underreporting of SES and race in Achilles tendon pathology RCTs. The reporting percentage remains low for both SES and race, indicating a need for comprehensive reporting practices in orthopaedic research. Understanding the impact of SES and race on treatment outcomes is critical for informed clinical decision making and ensuring equitable patient care. Future studies should prioritize the inclusion of these variables to enhance the generalizability and validity of RCT results.
Keywords: systematic review, Achilles tendon pathology, randomized controlled trial, socioeconomic status, race
Introduction
Randomized controlled trials (RCTs) have long been the gold standard for comparative research. 65 RCTs help minimize bias by randomly assigning patient characteristics, theoretically allowing for the possibility to attribute all study outcomes to a specific factor. 31 Although conducting an RCT involves detailed procedures geared toward effective randomization of the cohort through methods such as simple, blocked, or stratified randomization, 54 studies still fail to include all possible confounding variables when assigning groups. 60 For example, socioeconomic status (SES) is rarely reported across all medical disciplines and may have a large effect on the generalizability of the results of a particular RCT.27,60 Although certain fields, such as neuroscience, have consistently included SES metrics within the randomization process, 89 orthopaedic surgery has consistently underreported SES.29,40,56 Additionally, patient demographics, such as race, are rarely reported in orthopaedic RCTs.83,101 Race and SES have both demonstrated strong effects on outcomes after traumatic events and various orthopaedic procedures, and could potentially be large confounding variables in any orthopaedic RCT.75,106 As race and SES have shown a clear link in the quality of health care received, studying both metrics simultaneously was of great interest. 112
Across orthopaedics, there is evidence that SES and race can have an impact on outcomes of spine surgery, foot and ankle surgery, total joint arthroplasty, and follow-up metrics.29,40,44,45,64 However, the rate of reporting of these metrics is low in top orthopaedic journals. 22 Within foot and ankle orthopaedics, one previous systematic review organized SES and race reporting for RCTs encompassing all foot and ankle surgery. 64 Although this review found evidence demonstrating consistent underreporting of SEC and race within foot and ankle surgery, it was limited to only a 6-year time frame (2016-2021) and only described studies within 4 specific journals. 64 To follow up on this review, we extended the time frame to include RCTs from the last 4 decades, while also differentiating by the top 10 orthopaedic journals to better understand trends over time for each journal. Furthermore, the broad nature of this review prevented analysis of individual foot and ankle pathologies that may be more affected by SES and race. Therefore, our study only investigates SES and race reporting for Achilles tendon pathology—a condition well described in foot and ankle RCTs. Although this condition was purely chosen because of its high volume of RCTs and to address the possible confounding factors of previous reviews, 64 studies have found that race has an impact on Achilles tendon rupture in elite African American gymnasts.14,20 Although there is no sound evidence that SES and race are significantly related, one could argue that it is important to study SES and race within minority populations as a slight impact has been shown. Although no study has reported on SES directly for Achilles tendon pathology, SES is indirectly related to race and would likely have a significant impact as well. Therefore, the primary aim of this review was to evaluate SES and race reporting for foot and ankle surgery by evaluating Achilles tendon pathology RCTs over the last 4 decades to better understand reporting trends for these factors in major orthopaedic journals.
Methods
Study Creation
This systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) most recent guidelines. This study utilized PubMed to search 10 top-tier orthopaedic journals for randomized controlled trials (RCTs) related to management of Achilles tendon pathology. Journals were found by searching the Observatory of International Research (OOIR) website (https://ooir.org/journals.php?field=Clinical+Medicine&category=Orthopedics&metric=jif) for the top 5 general orthopaedic journals as well as the top 5 foot and ankle orthopaedic journals by impact factor. PubMed then was searched from database inception for each of the included journals until July 11, 2023. Search algorithm used in PubMed with the 10 top-tier orthopaedic journals with a filter of “Randomized Controlled Trials” was (“J Physiother”[journal]) OR (“Osteoarthritis Cartilage”[journal]) OR (“Am J Sports Med”[journal]) OR (“J Bone Joint Surg Am”[journal]) OR (“J Orthop Sports Phys Ther”[journal]) OR (“Foot Ankle Int.”[journal]) OR (“J Foot Ankle Res.”[journal]) OR (“Foot Ankle Surg”[journal]) OR (“Foot Ankle Clin.” [journal]) OR (“J Foot Ankle Surg”[journal]). All RCTs in the 10 top-tier orthopaedic articles by impact factor were initially retrieved for evaluation.
Inclusion and Exclusion Criteria
RCTs were included if the articles dealt primarily with Achilles tendon pathology, used human subjects, and were found in any of the 10 top-tier orthopaedic journals used for this study. Exclusion criteria were articles not primarily dealing with Achilles tendon pathology (eg, plantar fasciitis), non-English articles, non-full-text articles, and those that used nonhuman subjects (eg, cadavers or animals).
Study Definitions and Groups
For the purposes of this study, SES was broadly defined to give the most comprehensive reporting of SES in the high-level evidence in the literature. SES includes information on patient education levels, income levels, wealth, and occupation as well as any related terminology. RCTs were grouped by decade (1999 and prior, 2000-2009, 2010-2019, and 2020 and later), intervention (surgical, nonsurgical, or both), and primary study location (within the United States or outside of the United States).
Article Screening Process
After the initial search, articles were screened by abstract and title followed by full-text screening. Article screening was performed by multiple authors, with any discrepancies solved by a single author. Hand-screening of included articles’ references was also performed.
Data Extraction
Data extraction was performed by a single author. Data extracted included year of publication, type of study, reporting of SES, reporting of race, primary study location, and intervention as well as specifics about SES for further reporting.
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) version 29.0 (IBM Corp, Armonk, NY) was used for the statistical analysis of this study. As this study focused on qualitative data, only frequency reporting and descriptive statistics were needed.
Results
Initial Search Results
A total of 68 met inclusion criteria from a total of 88 RCTs found from the top-tier orthopaedic journals.1 -3,6 -8,10,12,13,16,17,19,23 -26,30,32 -34,36 -38,41 -43,46 -49,51,52,57,59,61 -63,66 -73,76 -78,80,81,84,85,87,88,90 -95,97,103 -105,107,110,113,114 Refer to Figure 1 for the PRISMA diagram for this systematic review. The RCTs in this study were taken from the top 10 orthopaedic journals by impact factor (Table 1).
Figure 1.
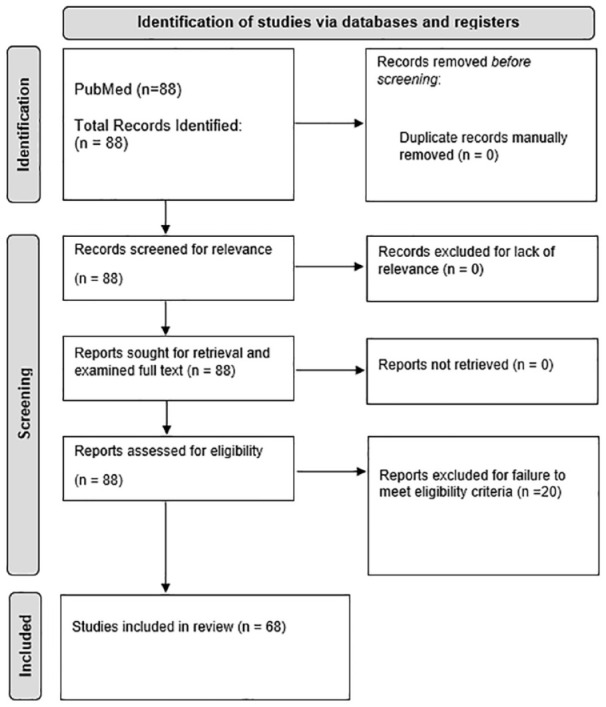
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram used for this systematic review. This diagram outlines the initial search to final article inclusion.
Table 1.
Description of the 10 orthopaedic articles searched on PubMed for randomized controlled trials (RCTs) included in this systematic review. a
| Impact Factor Ranking | Journal Name | Impact Factor | PubMed Abbreviation | PubMed Search Format |
|---|---|---|---|---|
| 1 | Journal of Physiotherapy | ca. 10.71 | J Physiother | ("J Physiother"[journal]) |
| 2 | Osteoarthritis and Cartilage | ca. 7.51 | Osteoarthritis Cartilage | ("Osteoarthritis Cartilage"[journal]) |
| 3 | American Journal of Sports Medicine | ca. 7.01 | Am J Sports Med | ("Am J Sports Med"[journal]) |
| 4 | Journal of Bone and Joint Surgery-American Volume | ca. 6.56 | J Bone Joint Surg Am | ("J Bone Joint Surg Am"[journal]) |
| 5 | Journal of Orthopaedic & Sports Physical Therapy | ca. 6.28 | J Orthop Sports Phys Ther | ("J Orthop Sports Phys Ther"[journal]) |
| 6 | Foot & Ankle International | ca. 3.57 | Foot Ankle Int | ("Foot Ankle Int."[journal]) |
| 7 | Journal of Foot and Ankle Research | ca. 3.05 | J Foot Ankle Res | ("J Foot Ankle Res."[journal]) |
| 8 | Foot and Ankle Surgery | ca. 2.84 | Foot Ankle Surg | ("Foot Ankle Surg"[journal]) |
| 9 | Foot and Ankle Clinics | ca. 2.03 | Foot Ankle Clin | ("Foot Ankle Clin. "[journal]) |
| 10 | Journal of Foot & Ankle Surgery | ca. 1.35 | J Foot Ankle Surg | ("J Foot Ankle Surg"[journal]) |
Data recorded included rank by Impact Factor (IF), name of the journal, IF, PubMed abbreviation, and PubMed search term by abbreviation.
Reporting by Decade
Based on decade, there were 4 articles published in 1999 or prior, 25 articles published between 2000 and 2009, 29 articles published between 2010 and 2019, and 10 articles published in 2020 and later. Overall, there was a total of 6 articles (8.8%) that reported SES and 2 articles (2.9%) that reported race. Based on decade, no RCTs (0.0% of RCTs within the decade) reported on SES in 1999 or prior years, 2 RCTs (8.0% of RCTs within the decade) reported on SES in 2000-2009, 3 RCTs (10.3% of RCTs within the decade) reported on SES in 2010-2019, and only 1 of the RCTs (10.0% of RCTs within the decade) reported on SES in 2020 or later years. The only 2 RCTs to report on race were in 2020 or later years as no RCTs reported on race prior to 2020. Refer to Figure 2 for a visual summary of reporting by decade.
Figure 2.
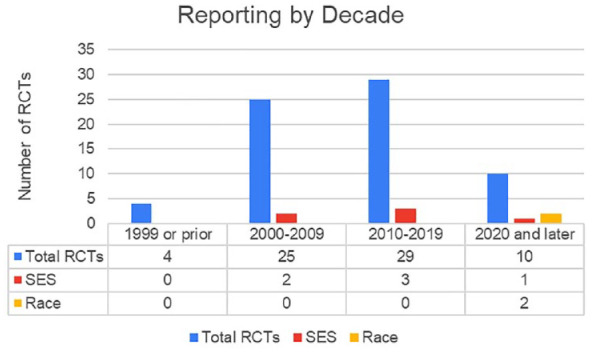
Reporting by decade for socioeconomic status (SES) and race. Decades include 1999 and prior, 2000-2009, 2010-2019, and 2020 and later. Abbreviations: RCTs, randomized controlled trials; SES, socioeconomic status.
Reporting by Surgical or Nonsurgical Intervention
From the 68 included RCTs, 45 RCTs (66.2% of RCTs) reported on nonsurgical treatment of Achilles tendon pathology, 11 RCTs (16.2% of RCTs) reported on surgical treatment of Achilles tendon pathology, and 12 RCTs (17.6% of RCTs) reported on both surgical and nonsurgical treatment of Achilles tendon pathology. Four of the RCTs (66.6% of RCTs reporting on SES) focused on nonsurgical interventions, 1 of the RCTs (16.7% of RCTs reporting on SES) focused on surgical interventions, and the remaining RCTs (16.7% of RCTs reporting on SES) focused on both surgical and nonsurgical interventions. One of the RCTs (50% of RCTs reporting on race) that reported on race focused on nonsurgical interventions whereas the other one of the RCTs (50% of RCTs reporting on race) that reported on race focused on surgical interventions. Refer to Figure 3 for a visual summary of reporting by type of intervention.
Figure 3.
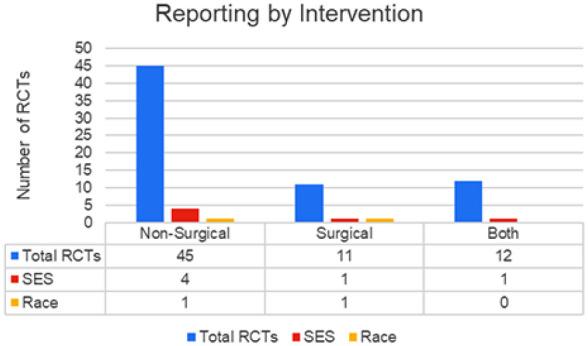
Reporting by intervention for socioeconomic status (SES) and race. Interventions included nonsurgical, surgical, or both. Abbreviations: RCTs, randomized controlled trials; SES, socioeconomic status.
Reporting by Primary Study Location
From the 68 included RCTs, 6 RCTs (8.8% of RCTs) had a primary study location within the United States, 61 RCTs (89.7% of RCTs) had a primary study location outside of the United States, and one of the RCTs (1.5% of RCTs) had an unknown primary study location. Five of the 6 RCTs (83.3% of RCTs reporting on SES) that reported on SES had a primary study location outside of the United States, with 1 of the RCTs (16.7% of RCTs reporting SES) having an unknown primary study location. However, both RCTs (100% of RCTs reporting race) had a primary study location within the United States. Refer to Figure 4 for a visual summary of reporting by study location.
Figure 4.
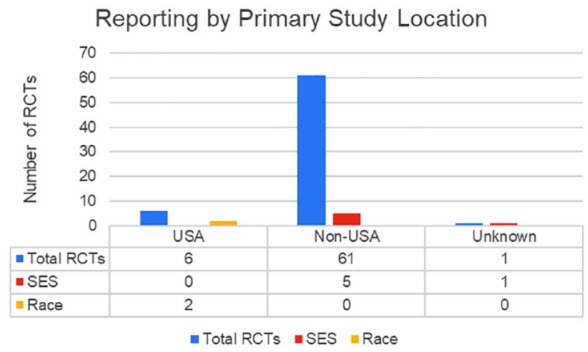
Reporting by primary study location for socioeconomic status (SES) and race. Primary study location included within the United States (USA) or outside of the United States (Non-USA). Abbreviations: RCTs, randomized controlled trials; SES, socioeconomic status.
Specifics on Socioeconomic Reporting
Of the 6 RCTs that reported on SES, all 6 RCTs (100%) reported SES as occupation level in terms of difficulty: heavy, light, sedentary, or mobile. No RCT reported on SES in terms of patient education level, wealth level, or income level.
Discussion
Given criticism within foot and ankle RCTs for lack of appropriate confounding variable reporting, RCTs pertaining to Achilles tendon pathology were studied to understand the frequency and trends of SES and race reporting by decade and by orthopaedic journal. As race and SES have been shown to be directly related, 111 this review was of high relevance. The aim of this review was to follow up on previous reviews by extending the time frame of interest while also including a broader scope of journals.
In previous reviews, such as the one by Martinazzi et al, 64 SES was studied on RCTs published from 2016 through 2021. This review found that RCTs rarely report SES, and more important, found that the frequency of reporting did not increase over time, that studied journals had no difference in frequency of reporting, and no difference in reporting for various outcome studies. 64 As this previous review focused on all RCTs encompassing foot and ankle surgery, we aimed to study a particular well-studied pathology in order to better understand reporting trends. Although studying all foot and ankle conditions may better illuminate the issue of not reporting SES within foot and ankle orthopaedics, SES reporting may have a greater impact on pathologies that frequently require surgical intervention, pathologies that require longer follow-up periods, or pathologies that require additional financial stability.11,21,82 Thus, although the previous review found no difference in reporting for various outcome studies, it may be hard to compare pain management and operative procedures of different pathologies without introducing additional confounding factors. 100 Therefore, the aim of this study was to study a particular pathology, such as Achilles tendon pathology. As this condition is widely published across the foot and ankle literature, RCTs focused on all forms of outcome studies (nonoperative, operative, or both) allowing for comparison within the same pathology. Furthermore, the studied time frame of the previous review was limited to 6 years. Although trends in reporting were assessed and found to be nonsignificant over the studied time frame, 64 expanding the time frame may better demonstrate the trends in SES reporting. Finally, in the previous review, the authors only studied reporting by 4 orthopaedic journals. Including additional top journals was of high priority within this review, as excluding journals may not fully represent the true trends in SES reporting, or more importantly, the trends across different journals.
Although Achilles tendon pathology was studied because of its high prevalence in the literature, this condition was also chosen because of the possibility that SES may have a large impact on treatment and outcomes. In a previous review that studied tendinopathy, 35 it was found that certain tendinopathic conditions led to patients taking additional sick leave to heal, decreased productivity, and most importantly, a decrease in function while performing everyday tasks such as driving, sleeping, carrying objects, and dressing.5,15,35,96,108,109 Therefore, including this condition was of great interest as foot and ankle tendinopathy was not addressed in detail in previous reviews. As SES has demonstrated impact on orthopaedic patient outcomes, clinically and subjectively, it is of great interest to understand SES reporting frequency in Achilles tendon pathology to better interpret the generality of an RCT’s results.18,39,50,53,55,58,74,79,86,98,99,102,115
In this review, we found upward trends in SES reporting for Achilles tendon pathology. Comparing decades, RCTs included from 1990 through 2000 failed to report SES, whereas RCTs from 2000 to 2010 and 2010 to 2020 included SES in 2 and 3 RCTs, respectively. Although the overall percentage of reporting was low for both decades (8% for 2000-2010, 10.3% for 2010-2020), the frequency is increasing. However, small sample sizes were included from each decade, so direct statistical comparison was difficult. But on an absolute scale, the frequency of SES reporting is increasing. Interestingly, the rate of SES reporting for the included articles from 2020 to 2023 have roughly the same frequency as the previous decade (10.3% for 2010-2020, 10% for 2020-2023). Future investigation into SES reporting by decade would be necessary to understand the trends of the current decade (2020-2030). Without grouping by decade, comparison of RCT reporting of SES by location revealed interesting results. Although the majority of our included RCTs came from outside the USA, RCTs from non-US countries were the only included RCTs to report SES. Future investigation into SES on Achilles tendon pathology RCTs from the USA would allow for statistical comparison based on location.
Another crucial aspect of this review, beyond the reporting of SES, was the frequency of reporting race in RCTs. As many studies have shown that race has an impact on intraoperative complications, postoperative success, and even perceived pain and patient satisfaction.9,53,86,98 Therefore, it was of great interest to include race as part of our analysis, particularly as race and SES are indirectly related. Our results demonstrate that until the current decade (2020-2030), race has not been reported for Achilles tendon pathology RCTs. However, in the current decade, the frequency of race reporting is higher than the frequency of SES reporting (10% for SES, 20% for race). Nevertheless, no statistical analysis was able to be performed to determine if this increase is significant compared to previous decades. This slight increase in reporting may be linked to the increase in race and SES political discussion in the last decade. Although reporting solely SES may encompass a variety of confounders, direct reporting of both race and SES is of paramount importance based on the impact race has on orthopaedic outcomes.9,53,86,98 Furthermore, as the NIH has emphasized the requirement to include women and minorities in future research, SES and race reporting should increase as a result. However, as methods such as Area Deprivation Index can account for race when SES is controlled for, reporting solely SES may be sufficient for RCTs. It is important to establish the standard for reporting race and SES in research to understand where orthopaedic ranks with respect to other specialties. To no surprise, orthopaedics is not the only specialty underreporting these metrics, with RCTs pertaining to general and internal medicine, oncology, cardiac and cardiology, obstetrics and gynecology, and infectious disease all underreporting race and SES. 28 Even in times where race and SES have been of great political discussion across the world, general medical journals consistently underreport these metrics regardless of specialty. 4
The primary limitation of our study is being unable to directly compare journals for SES and race reporting frequency. As only 8 of 68 RCTs included SES and/or race reporting, statistical comparison was not feasible. As more RCTs begin including SES and race, investigation into the frequency of reporting these factors by journal would be insightful in the future. Next, no study to date has examined why exactly race and SES are underreported in orthopaedic RCTs. Future research investigating this trend and its possible origin could be extremely impactful. As race and SES have both demonstrated strong effects on orthopaedic outcomes, their inclusion in RCTs would be completely justified.75,106 Furthermore, race and SES have both shown negative impact on the level of involvement in health-related research. Although our review found consistent underreporting on race and SES, future research should also attempt to include those of all races and SES, at least proportionally to the area of study, to potentially limit the bias that comes from recruiting for medical research.
Conclusion
In conclusion, this review focused on the reporting of SES and race in RCTs pertaining to Achilles tendon pathology. The aim was to extend previous reviews by analyzing a broader scope of journals and a longer time frame. Findings revealed an upward trend in SES reporting over the decades studied, but no statistical analysis prevented conclusive statements from being made regarding the significance of this upward trend. Interestingly, RCTs from non-USA countries were the only ones to report SES, highlighting potential regional differences in reporting practices. Moreover, race reporting has been absent until the current decade, further demonstrating the need for more comprehensive reporting practices in orthopaedic research to better understand the impact of race and SES on treatment outcomes.
Supplemental Material
Supplemental material, sj-pdf-1-fao-10.1177_24730114231225454 for Socioeconomic Status and Race Are Rarely Reported in Randomized Controlled Trials for Achilles Tendon Pathology in the Top 10 Orthopaedic Journals: A Systematic Review by Grayson M. Talaski, Anthony N. Baumann, Natasha Salmen, Deven P. Curtis, Kempland C. Walley, Albert T. Anastasio and Cesar de Cesar Netto in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval: Ethical approval was not sought for the present study because this is a systematic review.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs: Grayson M. Talaski,  https://orcid.org/0000-0002-0018-6410
https://orcid.org/0000-0002-0018-6410
Anthony N. Baumann, DPT,
https://orcid.org/0000-0002-4175-3135
Natasha Salmen, BS,
https://orcid.org/0009-0001-6527-6628
Albert T. Anastasio, MD,
https://orcid.org/0000-0001-5817-3826
Cesar de Cesar Netto, MD, PhD,
https://orcid.org/0000-0001-6037-0685
References
- 1. Abdelkader NA, Helmy MNK, Fayaz NA, Saweeres ESB. Short- and intermediate-term results of extracorporeal shockwave therapy for noninsertional Achilles tendinopathy. Foot Ankle Int. 2021;42(6):788-797. [DOI] [PubMed] [Google Scholar]
- 2. Aktas S, Kocaoglu B. Open versus minimal invasive repair with Achillon device. Foot Ankle Int. 2009;30(5):391-397. [DOI] [PubMed] [Google Scholar]
- 3. Aktas S, Kocaoglu B, Nalbantoglu U, Seyhan M, Guven O. End-to-end versus augmented repair in the treatment of acute Achilles tendon ruptures. J Foot Ankle Surg. 2007;46(5):336-340. [DOI] [PubMed] [Google Scholar]
- 4. Alegria M, Sud S, Steinberg BE, Gai N, Siddiqui A. Reporting of participant race, sex, and socioeconomic status in randomized clinical trials in general medical journals, 2015 vs 2019. JAMA Netw Open. 2021;4(5):e2111516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Alizadehkhaiyat O, Fisher AC, Kemp GJ, Frostick SP. Pain, functional disability, and psychologic status in tennis elbow. Clin J Pain. 2007;23(6):482-489. [DOI] [PubMed] [Google Scholar]
- 6. Alvarez CM, Wright JG, Chhina H, Howren A, Law P. Botulinum toxin type A versus placebo for idiopathic clubfoot: a two-center, double-blind, randomized controlled trial. J Bone Joint Surg Am. 2018;100(18):1589-1596. [DOI] [PubMed] [Google Scholar]
- 7. Barfod KW, Bencke J, Lauridsen HB, Ban I, Ebskov L, Troelsen A. Nonoperative dynamic treatment of acute Achilles tendon rupture: the influence of early weight-bearing on clinical outcome: a blinded, randomized controlled trial. J Bone Joint Surg Am. 2014;96(18):1497-1503. [DOI] [PubMed] [Google Scholar]
- 8. Barfod KW, Bencke J, Lauridsen HB, Dippmann C, Ebskov L, Troelsen A. Nonoperative, dynamic treatment of acute Achilles tendon rupture: influence of early weightbearing on biomechanical properties of the plantar flexor muscle–tendon complex—a blinded, randomized, controlled trial. J Foot Ankle Surg. 2015;54(2):220-226. [DOI] [PubMed] [Google Scholar]
- 9. Bernstein DN, Mayo K, Baumhauer JF, Dasilva C, Fear K, Houck JR. Do patient sociodemographic factors impact the PROMIS scores meeting the patient-acceptable symptom state at the initial point of care in orthopaedic foot and ankle patients? Clin Orthop Relat Res. 2019;477(11):2555-2565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Beyer R, Kongsgaard M, Kjær BH, Øhlenschlæger T, Kjær M, Magnusson SP. Heavy slow resistance versus eccentric training as treatment for Achilles tendinopathy: a randomized controlled trial. Am J Sports Med. 2015;43(7):1704-1711. [DOI] [PubMed] [Google Scholar]
- 11. Birkmeyer NJO, Gu N, Baser O, Morris AM, Birkmeyer JD. Socioeconomic status and surgical mortality in the elderly. Med Care. 2008;46(9):893-899. [DOI] [PubMed] [Google Scholar]
- 12. Boesen AP, Boesen MI, Hansen R, et al. Effect of platelet-rich plasma on nonsurgically treated acute Achilles tendon ruptures: a randomized, double-blinded prospective study. Am J Sports Med. 2020;48(9):2268-2276. [DOI] [PubMed] [Google Scholar]
- 13. Boesen AP, Hansen R, Boesen MI, Malliaras P, Langberg H. Effect of high-volume injection, platelet-rich plasma, and sham treatment in chronic midportion Achilles tendinopathy: a randomized double-blinded prospective study. Am J Sports Med. 2017;45(9):2034-2043. [DOI] [PubMed] [Google Scholar]
- 14. Bonanno J, Cheng J, Tilley D, Abutalib Z, Casey E. Factors associated with Achilles tendon rupture in women’s collegiate gymnastics. Sports Health. 2022;14(3):358-368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Bonde JP, Mikkelsen S, Andersen JH, et al. Prognosis of shoulder tendonitis in repetitive work: a follow up study in a cohort of Danish industrial and service workers. Occup Environ Med. 2003;60(9):E8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Bostick GP, Jomha NM, Suchak AA, Beaupré LA. Factors associated with calf muscle endurance recovery 1 year after Achilles tendon rupture repair. J Orthop Sports Phys Ther. 2010;40(6):345-351. [DOI] [PubMed] [Google Scholar]
- 17. Brorsson A, Silbernagel KG, Olsson N, Helander KN. Calf muscle performance deficits remain 7 years after an Achilles tendon rupture. Am J Sports Med. 2018;46(2):470-477. [DOI] [PubMed] [Google Scholar]
- 18. Butler RA, Rosenzweig S, Myers L, Barrack RL. The Frank Stinchfield Award: the impact of socioeconomic factors on outcome after THA: Hip Society Meetings 2010. Clin Orthop Relat Res. 2011;469(2):339-347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U. Operative versus nonoperative treatment of Achilles tendon rupture. A prospective randomized study and review of the literature. Am J Sports Med. 1993;21(6):791-799. [DOI] [PubMed] [Google Scholar]
- 20. Claessen FMAP, de Vos RJ, Reijman M, Meuffels DE. Predictors of primary Achilles tendon ruptures. Sports Med. 2014;44(9):1241-1259. [DOI] [PubMed] [Google Scholar]
- 21. Clement N, Muzammil A, Macdonald D, Howie C, Biant L. Socioeconomic status affects the early outcome of total hip replacement. J Bone Joint Surg Br. 2011;93(4):464-469. [DOI] [PubMed] [Google Scholar]
- 22. Crnkovic C, Quiring R, Chapple AG, Bronstone A, Krause PC, Dasa V. Low rates of reporting race, ethnicity, and socioeconomic status in studies published in top orthopaedic journals. J Bone Joint Surg Am. 2022;104(14):1244-1249. [DOI] [PubMed] [Google Scholar]
- 23. de Jonge S, de Vos RJ, Weir A, et al. One-year follow-up of platelet-rich plasma treatment in chronic Achilles tendinopathy: a double-blind randomized placebo-controlled trial. Am J Sports Med. 2011;39(8):1623-1630. [DOI] [PubMed] [Google Scholar]
- 24. de Jonge S, Tol JL, Weir A, Waarsing JH, Verhaar JA, de Vos RJ. The tendon structure returns to asymptomatic values in nonoperatively treated Achilles tendinopathy but is not associated with symptoms: a prospective study. Am J Sports Med. 2015;43(12):2950-2958. [DOI] [PubMed] [Google Scholar]
- 25. Eliasson P, Agergaard AS, Couppe C, et al. The ruptured Achilles tendon elongates for 6 months after surgical repair regardless of early or late weightbearing in combination with ankle mobilization: a randomized clinical trial. Am J Sports Med. 2018;46(10):2492-2502. [DOI] [PubMed] [Google Scholar]
- 26. Fredberg U, Bolvig L, Andersen NT. Prophylactic training in asymptomatic soccer players with ultrasonographic abnormalities in Achilles and patellar tendons: the Danish Super League Study. Am J Sports Med. 2008;36(3):451-460. [DOI] [PubMed] [Google Scholar]
- 27. Furler J, Magin P, Pirotta M, van Driel M. Participant demographics reported in “Table 1” of randomised controlled trials: a case of “inverse evidence”? Int J Equity Health. 2012;11:14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Geller SE, Koch A, Pellettieri B, Carnes M. Inclusion, analysis, and reporting of sex and race/ethnicity in clinical trials: have we made progress? J Womens Health (Larchmt). 2011;20(3):315-320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Griffin SA, Magnuson JA, Sutton RM, Krueger CA. Reporting and analyzing demographics in the journal of arthroplasty: are we making progress? J Arthroplasty. 2021;36(12):3825-3830. [DOI] [PubMed] [Google Scholar]
- 30. Hansen MS, Bencke J, Kristensen MT, Kallemose T, Hölmich P, Barfod KW. Achilles tendon gait dynamics after rupture: a three-armed randomized controlled trial comparing an individualized treatment algorithm vs. operative or non-operative treatment. Foot Ankle Surg. 2023;29(2):143-150. [DOI] [PubMed] [Google Scholar]
- 31. Hariton E, Locascio JJ. Randomised controlled trials—the gold standard for effectiveness research: study design: randomised controlled trials. BJOG. 2018;125(13):1716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Heikkinen J, Lantto I, Flinkkila T, et al. Soleus atrophy is common after the nonsurgical treatment of acute Achilles tendon ruptures: a randomized clinical trial comparing surgical and nonsurgical functional treatments. Am J Sports Med. 2017;45(6):1395-1404. [DOI] [PubMed] [Google Scholar]
- 33. Heikkinen J, Lantto I, Flinkkilä T, et al. Augmented compared with nonaugmented surgical repair after total Achilles rupture: results of a prospective randomized trial with thirteen or more years of follow-up. J Bone Joint Surg Am. 2016;98(2):85-92. [DOI] [PubMed] [Google Scholar]
- 34. Hoksrud A, Öhberg L, Alfredson H, Bahr R. Ultrasound-guided sclerosis of neovessels in painful chronic patellar tendinopathy: a randomized controlled trial. Am J Sports Med. 2006;34(11):1738-1746. [DOI] [PubMed] [Google Scholar]
- 35. Hopkins C, Fu SC, Chua E, et al. Critical review on the socio-economic impact of tendinopathy. Asia Pac J Sports Med Arthrosc Rehabil Technol. 2016;4:9-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Horstmann T, Jud HM, Fröhlich V, Mündermann A, Grau S. Whole-body vibration versus eccentric training or a wait-and-see approach for chronic Achilles tendinopathy: a randomized clinical trial. J Orthop Sports Phys Ther. 2013;43(11):794-803. [DOI] [PubMed] [Google Scholar]
- 37. Hunt KJ, Cohen BE, Davis WH, Anderson RB, Jones CP. Surgical treatment of insertional Achilles tendinopathy with or without flexor hallucis longus tendon transfer: a prospective, randomized study. Foot Ankle Int. 2015;3(9):998-1005. [DOI] [PubMed] [Google Scholar]
- 38. Hyer CF, Berlet G, Philbin T, et al. Does functional neuromuscular electrical stimulation (NMES) influence calf atrophy following Achilles tendon surgery? Prospective double-blind randomized controlled trial on the use of immediate postoperative electrical muscle stimulation to preserve muscle function and volume. J Foot Ankle Surg. 2021;60(4):683-688. [DOI] [PubMed] [Google Scholar]
- 39. Ibrahim SA, Stone RA, Han X, et al. Racial/ethnic differences in surgical outcomes in veterans following knee or hip arthroplasty. Arthritis Rheum. 2005;52(10):3143-3151. [DOI] [PubMed] [Google Scholar]
- 40. Issa TZ, Lambrechts MJ, Canseco JA, et al. Reporting demographics in randomized control trials in spine surgery—we must do better. Spine J. 2023;23(5):642-650. [DOI] [PubMed] [Google Scholar]
- 41. Kane TPC, Ismail M, Calder JDF. Topical glyceryl trinitrate and noninsertional Achilles tendinopathy: a clinical and cellular investigation. Am J Sports Med. 2008;36(6):1160-1163. [DOI] [PubMed] [Google Scholar]
- 42. Kangas J, Pajala A, Ohtonen P, Leppilahti J. Achilles tendon elongation after rupture repair: a randomized comparison of 2 postoperative regimens. Am J Sports Med. 2007;35(1):59-64. [DOI] [PubMed] [Google Scholar]
- 43. Kauranen K, Kangas J, Leppilahti J. Recovering motor performance of the foot after Achilles rupture repair: a randomized clinical study about early functional treatment vs. early immobilization of Achilles tendon in tension. Foot Ankle Int. 2002;23(7):600-605. [DOI] [PubMed] [Google Scholar]
- 44. Kirchner G, Kerbel Y, Kim A, Stein M, Ryan W, Mehta S. Looking forward: a systematic review assessing risk factors predicting orthopaedic trauma “loss to follow-up.” J Orthop Exp Innov. Published online August 28, 2022. doi: 10.60118/001c.33879 [DOI] [Google Scholar]
- 45. Kirchner GJ, Kim AH, Martinazzi BJ, Sudah SY, Lieber AM, Aynardi MC. Factors associated with amputation following ankle fracture surgery. J Foot Ankle Surg. 2023;62(5):792-796. [DOI] [PubMed] [Google Scholar]
- 46. Knobloch K, Grasemann R, Spies M, Vogt PM. Midportion Achilles tendon microcirculation after intermittent combined cryotherapy and compression compared with cryotherapy alone: a randomized trial. Am J Sports Med. 2008;36(11):2128-2138. [DOI] [PubMed] [Google Scholar]
- 47. Knobloch K, Kraemer R, Jagodzinski M, Zeichen J, Meller R, Vogt PM. Eccentric training decreases paratendon capillary blood flow and preserves paratendon oxygen saturation in chronic Achilles tendinopathy. J Orthop Sports Phys Ther. 2007;37(5):269-276. [DOI] [PubMed] [Google Scholar]
- 48. Kocaoglu B, Ulku TK, Gereli A, Karahan M, Turkmen M. Evaluation of absorbable and nonabsorbable sutures for repair of Achilles tendon rupture with a suture-guiding device. Foot Ankle Int. 2015;36(6):691-695. [DOI] [PubMed] [Google Scholar]
- 49. Krogh TP, Ellingsen T, Christensen R, Jensen P, Fredberg U. Ultrasound-guided injection therapy of Achilles tendinopathy with platelet-rich plasma or saline: a randomized, blinded, placebo-controlled trial. Am J Sports Med. 2016;44(8):1990-1997. [DOI] [PubMed] [Google Scholar]
- 50. Kugelman DN, Haglin JM, Carlock KD, Konda SR, Egol KA. The association between patient education level and economic status on outcomes following surgical management of (fracture) non-union. Injury. 2019;50(2):344-350. [DOI] [PubMed] [Google Scholar]
- 51. Lantto I, Heikkinen J, Flinkkila T, et al. Early functional treatment versus cast immobilization in tension after Achilles rupture repair: results of a prospective randomized trial with 10 or more years of follow-up. Am J Sports Med. 2015;43(9):2302-2309. [DOI] [PubMed] [Google Scholar]
- 52. Lantto I, Heikkinen J, Flinkkila T, et al. A prospective randomized trial comparing surgical and nonsurgical treatments of acute Achilles tendon ruptures. Am J Sports Med. 2016;44(9):2406-2414. [DOI] [PubMed] [Google Scholar]
- 53. Lavernia CJ, Alcerro JC, Contreras JS, Rossi MD. Ethnic and racial factors influencing well-being, perceived pain, and physical function after primary total joint arthroplasty. Clin Orthop Relat Res. 2011;469(7):1838-1845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Lee S, Kang H. Statistical and methodological considerations for reporting RCTs in medical literature. Korean J Anesthesiol. 2015;68(2):106-115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Li X, Galvin JW, Li C, Agrawal R, Curry EJ. The impact of socioeconomic status on outcomes in orthopaedic surgery. J Bone Joint Surg Am. 2020;102(5):428-444. [DOI] [PubMed] [Google Scholar]
- 56. Lim CT. Factors Influencing the Enrollment of Eligible Individuals in Orthopedic Randomized Controlled Trials. Doctoral dissertation. Harvard University; 2016. [Google Scholar]
- 57. Lim J, Dalai R, Waseem M, Percutaneous vs. open repair of the ruptured Achilles tendon—a prospective randomized controlled study. Foot Ankle Int. 2001;22(7):559-568. [DOI] [PubMed] [Google Scholar]
- 58. MacDermid JC, Donner A, Richards RS, Roth JH. Patient versus injury factors as predictors of pain and disability six months after a distal radius fracture. J Clin Epidemiol. 2002;55(9):849-854. [DOI] [PubMed] [Google Scholar]
- 59. Maempel JF, Clement ND, Duckworth AD, Keenan OJ, White TO, Biant LC. A randomized controlled trial comparing traditional plaster cast rehabilitation with functional walking boot rehabilitation for acute Achilles tendon ruptures. Am J Sports Med. 2020;48(11):2755-2764. [DOI] [PubMed] [Google Scholar]
- 60. Magin P, Victoire A, Zhen XM, et al. Under-reporting of socioeconomic status of patients in stroke trials: adherence to CONSORT principles. Stroke. 2013;44(10):2920-2922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Malmgaard-Clausen NM, Jørgensen OH, Høffner R, et al. No additive clinical or physiological effects of short-term anti-inflammatory treatment to physical rehabilitation in the early phase of human Achilles tendinopathy: a randomized controlled trial. Am J Sports Med. 2021;49(7):1711-1720. [DOI] [PubMed] [Google Scholar]
- 62. Manent A, López L, Coromina H, et al. Acute Achilles tendon ruptures: efficacy of conservative and surgical (percutaneous, open) treatment—a randomized, controlled, clinical trial. J Foot Ankle Surg. 2019;58(6):1229-1234. [DOI] [PubMed] [Google Scholar]
- 63. Mansur NSB, Matsunaga FT, Carrazzone OL, et al. Shockwave therapy plus eccentric exercises versus isolated eccentric exercises for Achilles insertional tendinopathy: a double-blinded randomized clinical trial. J Bone Joint Surg Am. 2021;103(14):1295-1302. [DOI] [PubMed] [Google Scholar]
- 64. Martinazzi BJ, Kirchner GJ, Nam HH, et al. Improving randomized-controlled trials in foot and ankle orthopaedics: the need to include sociodemographic patient data. Foot Ankle Spec. Published online May 6, 2023. doi: 10.1177/19386400231170965 [DOI] [PubMed] [Google Scholar]
- 65. Meldrum ML. A brief history of the randomized controlled trial. From oranges and lemons to the gold standard. Hematol Oncol Clin North Am. 2000;14:745-760. [DOI] [PubMed] [Google Scholar]
- 66. Metz R, Verleisdonk EJMM, van der Heijden GJMG, et al. Acute Achilles tendon rupture: minimally invasive surgery versus nonoperative treatment with immediate full weightbearing—a randomized controlled trial. Am J Sports Med. 2008;36(9):1688-1694. [DOI] [PubMed] [Google Scholar]
- 67. Milgrom C, Finestone A, Zin D, Mandel D, Novack V. Cold weather training: a risk factor for Achilles paratendinitis among recruits. Foot Ankle Int. 2003;24(5):398-401. [DOI] [PubMed] [Google Scholar]
- 68. Molund M, Husebye EE, Hellesnes J, Nilsen F, Hvaal K. Proximal medial gastrocnemius recession and stretching versus stretching as treatment of chronic plantar heel pain. Foot Ankle Int. 2018;39(12):1423-1431. [DOI] [PubMed] [Google Scholar]
- 69. Morrison RJ, Brock TM, Reed MR, Muller SD. Radiofrequency microdebridement versus surgical decompression for Achilles tendinosis: a randomized controlled trial. J Foot Ankle Surg. 2017;56(4):708-712. [DOI] [PubMed] [Google Scholar]
- 70. Mortensen HM, Skov O, Jensen PE. Early motion of the ankle after operative treatment of a rupture of the Achilles tendon. A prospective, randomized clinical and radiographic study. J Bone Joint Surg Am. 1999;81(7):983-990. [DOI] [PubMed] [Google Scholar]
- 71. Mueller MJ, Sinacore DR, Hastings MK, Strube MJ, Johnson JE. Effect of Achilles tendon lengthening on neuropathic plantar ulcers. A randomized clinical trial. J Bone Joint Surg Am. 2003;85(8):1436-1445. [PubMed] [Google Scholar]
- 72. Nilsson-Helander K, Silbernagel KG, Thomee R, et al. Acute Achilles tendon rupture: a randomized, controlled study comparing surgical and nonsurgical treatments using validated outcome measures. Am J Sports Med. 2010;38(11):2186-2193. [DOI] [PubMed] [Google Scholar]
- 73. Nistor L. Surgical and non-surgical treatment of Achilles Tendon rupture. A prospective randomized study. J Bone Joint Surg Am. 1981;63(3):394-399. [PubMed] [Google Scholar]
- 74. Nwachukwu BU, Kenny AD, Losina E, Chibnik LB, Katz JN. Complications for racial and ethnic minority groups after total hip and knee replacement: a review of the literature. J Bone Joint Surg Am. 2010;92(2):338-345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. O’Hara NN, Isaac M, Slobogean GP, Klazinga NS. The socioeconomic impact of orthopaedic trauma: a systematic review and meta-analysis. PLoS One. 2020;15(1):e0227907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. Okoroha KR, Ussef N, Jildeh TR, et al. Comparison of tendon lengthening with traditional versus accelerated rehabilitation after Achilles tendon repair: a prospective randomized controlled trial. Am J Sports Med. 2020;48(7):1720-1726. [DOI] [PubMed] [Google Scholar]
- 77. Olsson N, Silbernagel KG, Eriksson BI, et al. Stable surgical repair with accelerated rehabilitation versus nonsurgical treatment for acute Achilles tendon ruptures: a randomized controlled study. Am J Sports Med. 2013;41(12):2867-2876. [DOI] [PubMed] [Google Scholar]
- 78. Pajala A, Kangas J, Siira P, Ohtonen P, Leppilahti J. Augmented compared with nonaugmented surgical repair of a fresh total Achilles tendon rupture. A prospective randomized study. J Bone Joint Surg Am. 2009;91(5):1092-1100. [DOI] [PubMed] [Google Scholar]
- 79. Paksima N, Pahk B, Romo S, Egol KA. The association of education level on outcome after distal radius fracture. Hand (N Y). 2014;9(1):75-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Paoloni JA, Appleyard RC, Nelson J, Murrell GAC. Topical glyceryl trinitrate treatment of chronic noninsertional Achilles tendinopathy. A randomized, double-blind, placebo-controlled trial. J Bone Joint Surg Am. 2004;86(5):916-922. [DOI] [PubMed] [Google Scholar]
- 81. Paoloni JA, Murrell GA. Three-year followup study of topical glyceryl trinitrate treatment of chronic noninsertional Achilles tendinopathy. Foot Ankle Int. 2007;28(10):1064-1068. [DOI] [PubMed] [Google Scholar]
- 82. Patel AR, Sarkisova N, Smith R, Gupta K, VandenBerg CD. Socioeconomic status impacts outcomes following pediatric anterior cruciate ligament reconstruction. Medicine (Baltimore). 2019;98(17):e15361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Paul RW, Lee D, Brutico J, Tjoumakaris FP, Ciccotti MG, Freedman KB. Reporting and analyzing race and ethnicity in orthopaedic clinical trials: a systematic review. J Am Acad Orthop Surg Glob Res Rev. 2021;5(5):e21.00027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Petersen W, Welp R, Rosenbaum D. Chronic Achilles tendinopathy: a prospective randomized study comparing the therapeutic effect of eccentric training, the AirHeel brace, and a combination of both. Am J Sports Med. 2007;35(10):1659-1667. [DOI] [PubMed] [Google Scholar]
- 85. Pfeffer G, Bacchetti P, Deland J, et al. Comparison of custom and prefabricated orthoses in the initial treatment of proximal plantar fasciitis. Foot Ankle Int. 1999;20(4):214-221. [DOI] [PubMed] [Google Scholar]
- 86. Pierce TP, Elmallah RK, Lavernia CJ, et al. Racial disparities in lower extremity arthroplasty outcomes and use. Orthopedics. 2015;38(12):e1139-e1146. [DOI] [PubMed] [Google Scholar]
- 87. Pinitkwamdee S, Laohajaroensombat S, Orapin J, Woratanarat P. Effectiveness of extracorporeal shockwave therapy in the treatment of chronic insertional Achilles tendinopathy. Foot Ankle Int. 2020;41(4):403-410. [DOI] [PubMed] [Google Scholar]
- 88. Porter D, Barrill E, Oneacre K, May BD. The effects of duration and frequency of Achilles tendon stretching on dorsiflexion and outcome in painful heel syndrome: a randomized, blinded, control study. Foot Ankle Int. 2002;23(7):619-624. [DOI] [PubMed] [Google Scholar]
- 89. Putman K, De Wit L, Schoonacker M, et al. Effect of socioeconomic status on functional and motor recovery after stroke: a European multicentre study. J Neurol Neurosurg Psychiatry. 2007;78(6):593-599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Rendek Z, Bon Beckman L, Schepull T, et al. Early tensile loading in nonsurgically treated Achilles tendon ruptures leads to a larger tendon callus and a lower elastic modulus: a randomized controlled trial. Am J Sports Med. 2022;50(12):3286-3298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Rompe JD, Furia J, Maffulli N. Eccentric loading compared with shock wave treatment for chronic insertional Achilles tendinopathy. A randomized, controlled trial. J Bone Joint Surg Am. 2008;90(1):52-61. [DOI] [PubMed] [Google Scholar]
- 92. Rompe JD, Furia J, Maffulli N. Eccentric loading versus eccentric loading plus shock-wave treatment for midportion Achilles tendinopathy: a randomized controlled trial. Am J Sports Med. 2009;37(3):463-470. [DOI] [PubMed] [Google Scholar]
- 93. Rompe JD, Nafe B, Furia JP, Maffulli N. Eccentric loading, shock-wave treatment, or a wait-and-see policy for tendinopathy of the main body of tendo Achillis: a randomized controlled trial. Am J Sports Med. 2007;35(3):374-383. [DOI] [PubMed] [Google Scholar]
- 94. Schepull T, Aspenberg P. Early controlled tension improves the material properties of healing human Achilles tendons after ruptures: a randomized trial. Am J Sports Med. 2013;41(11):2550-2557. [DOI] [PubMed] [Google Scholar]
- 95. Schepull T, Kvist J, Norrman H, Trinks M, Berlin G, Aspenberg P. Autologous platelets have no effect on the healing of human Achilles tendon ruptures: a randomized single-blind study. Am J Sports Med. 2011;39(1):38-47. [DOI] [PubMed] [Google Scholar]
- 96. Sérazin C, Ha C, Bodin J, Imbernon E, Roquelaure Y. Employment and occupational outcomes of workers with musculoskeletal pain in a French region. Occup Environ Med. 2013;70(3):143-148. [DOI] [PubMed] [Google Scholar]
- 97. Silbernagel KG, Thomeé R, Eriksson BI, Karlsson J. Continued sports activity, using a pain-monitoring model, during rehabilitation in patients with Achilles tendinopathy: a randomized controlled study. Am J Sports Med. 2007;35(6):897-906. [DOI] [PubMed] [Google Scholar]
- 98. Singh JA, Cleveland JD. Age, race, comorbidity, and insurance payer type are associated with outcomes after total ankle arthroplasty. Clin Rheumatol. 2020;39(3):881-890. [DOI] [PubMed] [Google Scholar]
- 99. Singh JA, Ramachandran R. Racial disparities in total ankle arthroplasty utilization and outcomes. Arthritis Res Ther. 2015;17(1):70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100. Skelly AC, Dettori JR, Brodt ED. Assessing bias: the importance of considering confounding. Evid Based Spine Care J. 2012;3(1):9-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101. Somerson JS, Bhandari M, Vaughan CT, Smith CS, Zelle BA. Lack of diversity in orthopaedic trials conducted in the United States. J Bone Joint Surg Am. 2014;96(7):e56. [DOI] [PubMed] [Google Scholar]
- 102. SooHoo NF, Lieberman JR, Ko CY, Zingmond DS. Factors predicting complication rates following total knee replacement. J Bone Joint Surg Am. 2006;88(3):480-485. [DOI] [PubMed] [Google Scholar]
- 103. Stergioulas A, Stergioula M, Aarskog R, Lopes-Martins RA, Bjordal JM. Effects of low-level laser therapy and eccentric exercises in the treatment of recreational athletes with chronic Achilles tendinopathy. Am J Sports Med. 2008;36(5):881-887. [DOI] [PubMed] [Google Scholar]
- 104. Stevens M, Tan CW. Effectiveness of the Alfredson protocol compared with a lower repetition-volume protocol for midportion Achilles tendinopathy: a randomized controlled trial. J Orthop Sports Phys Ther. 2014;44(2):59-67. [DOI] [PubMed] [Google Scholar]
- 105. Suchak AA, Bostick GP, Beaupré LA, D’Arcy CD, Jomha NM. The influence of early weight-bearing compared with non-weight-bearing after surgical repair of the Achilles tendon. J Bone Joint Surg Am. 2008;90(9):1876-1883. [DOI] [PubMed] [Google Scholar]
- 106. Suleiman LI, Manista GC, Sherman AE, et al. The impact of race and socioeconomic status on total joint arthroplasty care. J Arthroplasty. 2021;36(8):2729-2733. [DOI] [PubMed] [Google Scholar]
- 107. Twaddle BC, Poon P. Early motion for Achilles tendon ruptures: is surgery important? A randomized, prospective study. Am J Sports Med. 2007;35(12):2033-2038. [DOI] [PubMed] [Google Scholar]
- 108. van der Worp H, van Ark M, Roerink S, Pepping GJ, van den Akker-Scheek I, Zwerver J. Risk factors for patellar tendinopathy: a systematic review of the literature. Br J Sports Med. 2011;45(5):446-452. [DOI] [PubMed] [Google Scholar]
- 109. Walker-Bone K, Palmer KT, Reading I, Coggon D, Cooper C. Occupation and epicondylitis: a population-based study. Rheumatology (Oxford). 2012;51(2):305-310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110. Wezenbeek E, De Clercq D, Mahieu N, Willems T, Witvrouw E. Activity-induced increase in Achilles tendon blood flow is age and sex dependent. Am J Sports Med. 2018;46(11):2678-2686. [DOI] [PubMed] [Google Scholar]
- 111. Williams DR. Race/ethnicity and socioeconomic status: measurement and methodological issues. Int J Health Serv. 1996;26(3):483-505. [DOI] [PubMed] [Google Scholar]
- 112. Williams DR, Priest N, Anderson NB. Understanding associations among race, socioeconomic status, and health: patterns and prospects. Health Psychol. 2016;35(4):407-411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Willits K, Amendola A, Bryant D, et al. Operative versus nonoperative treatment of acute Achilles tendon ruptures: a multicenter randomized trial using accelerated functional rehabilitation. J Bone Joint Surg Am. 2010;92(17):2767-2775. [DOI] [PubMed] [Google Scholar]
- 114. Young SW, Patel A, Zhu M, et al. Weight-bearing in the nonoperative treatment of acute Achilles tendon ruptures: a randomized controlled trial. J Bone Joint Surg Am. 2014;96(13):1073-1079. [DOI] [PubMed] [Google Scholar]
- 115. Ziedas A, Abed V, Swantek A, et al. Social determinants of health influence access to care and outcomes in patients undergoing anterior cruciate ligament reconstruction: a systematic review. Arthroscopy. 2022;38(2):583-594.e4. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-pdf-1-fao-10.1177_24730114231225454 for Socioeconomic Status and Race Are Rarely Reported in Randomized Controlled Trials for Achilles Tendon Pathology in the Top 10 Orthopaedic Journals: A Systematic Review by Grayson M. Talaski, Anthony N. Baumann, Natasha Salmen, Deven P. Curtis, Kempland C. Walley, Albert T. Anastasio and Cesar de Cesar Netto in Foot & Ankle Orthopaedics