

Abstract
Background Polypharmacy may affect outcomes in patients with atrial fibrillation (AF) using non-vitamin K antagonist oral anticoagulants (NOACs) or vitamin K antagonists (VKAs) due to interactions or reduced adherence, but comparative data are lacking. Therefore, the impact of polypharmacy on AF-related outcomes and benefit–risk profiles of NOACs in patients with polypharmacy were investigated.
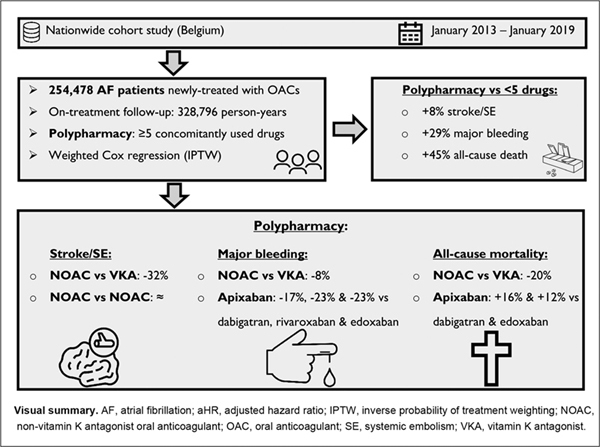
Methods AF patients initiating anticoagulation between 2013 and 2019 were included using Belgian nationwide data. Inverse probability of treatment weighted Cox regression was used to investigate outcomes.
Results Among 254,478 AF patients, 167,847 (66.0%) used ≥5 drugs. Polypharmacy was associated with higher stroke or systemic embolism (stroke/SE) (adjusted hazard ratio [aHR]: 1.08, 95% confidence interval [CI]: 1.02–1.15), all-cause mortality (aHR: 1.45, 95% CI: 1.40–1.50), and major bleeding risks (aHR: 1.29, 95% CI: 1.23–1.35). Among patients with polypharmacy, NOACs were associated with lower stroke/SE (aHR: 0.68, 95% CI: 0.63–0.73), all-cause mortality (aHR: 0.80, 95% CI: 0.77–0.84), major bleeding (aHR: 0.92, 95% CI: 0.87–0.97), and intracranial bleeding risks (aHR: 0.77, 95% CI: 0.69–0.85), but higher gastrointestinal bleeding risks (aHR: 1.10, 95% CI: 1.01–1.19) compared to VKAs. Major bleeding risks were lower with apixaban (aHR: 0.79, 95% CI: 0.74–0.85), but nonsignificantly different with other NOACs compared to VKAs. Lower major bleeding risks were observed with dabigatran (aHR: 0.91, 95% CI: 0.85–0.97) and apixaban (aHR: 0.77, 95% CI: 0.73–0.81) compared to rivaroxaban, and with apixaban compared to dabigatran (HR: 0.83, 95% CI: 0.77–0.90) and edoxaban (HR: 0.77, 95% CI: 0.70–0.85).
Conclusion Polypharmacy was associated with increased thromboembolic, bleeding, and mortality risks in AF patients. NOACs had better benefit–risk profiles than VKAs in patients with polypharmacy.
Keywords: atrial fibrillation, polypharmacy, NOAC, thromboembolism
NOACs in Atrial Fibrillation Patients with Polypharmacy
Introduction
Polypharmacy, often defined as the use of ≥5 concomitant drugs, 1 is frequently seen in patients with atrial fibrillation (AF) and has been associated with increasing age, multimorbidity, falls, frailty, and dementia. 2 3 4 5 More importantly, worse outcomes have been observed in AF patients with polypharmacy compared to those without, such as higher risks of bleeding and death. 3 4 5 6 7 8 9 However, the impact of polypharmacy on thromboembolic risks in anticoagulated AF patients is less established, as prior studies 3 4 5 6 7 rendered conflicting results. These studies were often limited by small sample sizes and short follow-up durations.
Furthermore, choosing an appropriate oral anticoagulant (OAC) treatment in patients with AF and polypharmacy is complex and difficult for clinicians, due to the potential impact of multiple comorbidities, adverse drug reactions, and especially drug–drug interactions, which may result in underuse, underdosing, or discontinuation of OACs. 3 4 5 8 9 10 11 12 13 14 15 Vitamin K antagonists (VKAs) are indeed limited by multiple drug and food interactions due to hepatic metabolism by cytochrome P450 (CYP) isoenzymes such as CYP1A2, CYP2C9, CYP2C19 and CYP3A4. 11 16 17 Likewise, pharmacokinetic interactions with non-vitamin K antagonist oral anticoagulants (NOACs) are present as well, given their excretion by P-glycoprotein (P-gp) efflux transporters and, for apixaban and rivaroxaban, hepatic metabolism mostly by CYP3A4. 10 11 17 In addition, several pharmacodynamic interactions may increase OAC-related bleeding risks (e.g., concomitant use of antiplatelets or corticosteroids). 17 18 19 Following the rapid transition of VKAs to NOACs for stroke prevention in AF 20 21 based on international guidelines 17 22 23 24 recommending the use of NOACs in preference to VKAs in the general AF population, concerns have risen whether the benefit–risk profile of NOACs is preserved in AF patients with polypharmacy in real-life clinical practice. While three posthoc analyses of randomized controlled trials (RCTs) 4 5 6 and five observational studies 12 25 26 27 28 explored the effectiveness and safety of NOACs compared to VKAs in AF patients with polypharmacy, studies were at the same time limited by small sample sizes, short follow-up durations, and heterogeneous polypharmacy measures based on various numerical definitions without specifying a minimal duration of concomitant use. So far, only two observational studies 12 26 investigated outcomes between three different NOACs (i.e., not including edoxaban yet). Consequently, there is an urgent need for a critical appraisal of the long-term benefit–risk profile of all marketed NOACs in patients with polypharmacy to further guide physicians in their choice of (N)OAC.
Therefore, we aimed to investigate (1) the impact of polypharmacy on clinical outcomes in anticoagulated AF patients, and (2) the long-term comparative effectiveness and safety of dabigatran, rivaroxaban, apixaban, and edoxaban in direct head-to-head comparisons with VKAs and between individual NOACs in AF patients with polypharmacy.
Methods
Source Population
Details on the study methodology have been published before and are provided in the Supplementary Materials (available in the online version) . 13 20 In brief, two nationwide databases provided the source population, namely the InterMutualistic Agency (IMA) database and Minimal Hospital Dataset (MHD). The IMA centralizes all claims data from Belgian health insurance funds on reimbursed ambulatory and hospital care, including demographic characteristics (e.g., age, sex, date of death), medical procedures, and drug prescription claims (e.g., dispensing date, Anatomical Therapeutic Chemical [ATC] classification code, package size, …), and represents all legal residents in Belgium. 29 The MHD aggregates hospital discharge diagnoses of every hospital admission (hospitalizations, day-care stays, and emergency room contacts), coded in International Classification of Diseases (ICD) codes (ICD-9 up to 2014, ICD-10 from 2015 onwards). 30 All single cases of the study population could be identified in both databases. This study was approved by the Belgian Commission for the Protection of Privacy (approval code IVC/KSZG/20/344). 31 The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline was followed ( Supplementary Table S1 , available in the online version>). 32
Study Population
From January 1, 2013 to January 1, 2019, persons aged ≥45 years old with ≥1 year coverage by health insurance funds were included from the IMA database on the first date of filling an OAC prescription (= index date) ( Supplementary Fig. S1 , available in the online version). NOAC users, namely dabigatran (approved in Belgium since August 2012), rivaroxaban (approved since September 2012), apixaban (approved since September 2013), and edoxaban (approved since October 2016), and VKA users (warfarin, acenocoumarol, phenprocoumon) were included. 20 Only OAC-naïve subjects were considered, excluding subjects with an OAC prescription filled up to 1 year before the index date.
Persons were excluded in case of (1) total hip or knee replacement, or diagnosis of deep vein thrombosis or pulmonary embolism up to 6 months before the index date, (2) mechanical prosthetic heart valve or moderate/severe mitral stenosis, (3) end-stage renal disease (chronic kidney disease stage V and/or dialysis), (4) ≥2 prescription claims of different OAC types or doses on the index date, or (5) use of NOAC doses not approved for stroke prevention in AF (e.g., rivaroxaban 10 mg) ( Supplementary Table S2 , Supplementary Fig. S1 [available in the online version]).
Polypharmacy
Medication history was identified with ATC-coded prescription claims in ambulatory and hospital care, considering recent use up to 6 months before the index date. Based on the total number of previously dispensed drugs, baseline polypharmacy was defined as the dispensing of ≥5 concomitant drugs during ≥30 days (30 defined daily doses of each concomitant drug, consecutive or not) 33 in the last 6 months. 1 8 Drugs were classified according to the fourth level of the ATC classification 33 to avoid considering two drug types of the same drug class as two different drugs (e.g., in case of switching between drug types). 8
Outcomes
Effectiveness outcomes included stroke or systemic embolism (stroke/SE), ischemic stroke, and all-cause mortality. Safety outcomes included major, intracranial, and gastrointestinal bleeding. Major bleeding was defined as a hospitalized bleeding event in a critical area or organ (e.g., intracranial), fatal bleeding, or bleeding event with a medical procedure code for blood transfusion up to 10 days after admission. 34 This definition is adapted from the International Society on Thrombosis and Haemostasis, 35 considering that no data on hemoglobin levels or number of blood transfusion units were available. 34 35 Outcomes were identified using ICD-coded hospital discharge diagnoses and medical procedure codes ( Supplementary Table S3 , available in the online version>). 13 The incident date of outcomes was defined as the date of hospital admission for ICD codes and date of registration for medical procedure codes, whichever occurred first. Mortality dates were identified in the IMA database.
Follow-Up
Subjects were followed from OAC initiation until the first occurrence of the investigated outcome, discontinuation (>60-day gap of drug supply) or switch of treatment, death, emigration, or end of the study period (January 1, 2019), whichever came first (on-treatment analysis). 13
Covariates
Baseline characteristics were assessed on the index date and included age, sex, comorbidities, medication history, and clinical risk scores. Comorbidities were identified with specific ICD-coded diagnoses, medical procedure codes, and/or medication prescription claims up to 1 year before the index date ( Supplementary Table S2 , available in the online version>). The CHA 2 DS 2 -VASc score, modified HAS-BLED score (without the “labile INR” [international normalized ratio] criterion), and age-adjusted Charlson Comorbidity Index were calculated. 17 36
Statistical Analyses
Mean and standard deviation and counts and percentages were presented for continuous and categorical variables, respectively. Crude event rates per outcome were calculated as the total number of events per 100 person-years at risk. Outcomes were compared between AF patients initiating anticoagulation with versus without baseline polypharmacy (≥5 vs. <5 concomitantly used drugs) using Cox proportional hazard regression models. Additionally, models were adjusted for age and sex (age- and sex-adjusted model), and for age, sex, type of OAC used, baseline comorbidities, and cardiovascular or potential bleeding-related drugs (multivariable adjusted model with covariates described in Table 1 , except risk scores to avoid multicollinearity issues). Only statistically significant factors using a two-sided p -value of <0.05 were retained in the multivariable adjusted model with backward elimination.
Table 1. Baseline characteristics of OAC-naïve AF patients with and without polypharmacy at baseline (≥5 and <5 concomitantly used drugs, respectively).
| Patient characteristics | No polypharmacy (<5 drugs) ( n = 86,631) |
Polypharmacy (≥5 drugs) | SMD a | |||
|---|---|---|---|---|---|---|
| Overall (≥5 drugs) ( n = 167,847) |
VKA ( n = 40,127) |
NOAC ( n = 127,720) |
Before IPTW | After IPTW | ||
| Age (y) | 72.5+/−11.6 | 76.3+/−10.2 | 72.8+/−11.5 | 77.4+/−9.6 | 0.43 | 0.016 |
| Female | 37,312 (43.1%) | 83,462 (49.7%) | 19,200 (47.8%) | 64,262 (50.3%) | 0.049 | 0.008 |
| Follow-up (y) | 1.3+/−1.5 | 1.3+/−1.5 | 0.9+/−1.3 | 1.4+/−1.5 | NA | NA |
| Comorbidities | ||||||
| Hypertension | 35,282 (40.7%) | 129,594 (77.2%) | 29,915 (74.5%) | 99,679 (78.0%) | 0.084 | 0.001 |
| Coronary artery disease | 7,211 (8.3%) | 40,632 (24.2%) | 12,068 (30.1%) | 28,564 (22.4%) | 0.172 | 0.002 |
| Congestive heart failure | 6,196 (7.2%) | 33,697 (20.1%) | 8,508 (21.2%) | 25,189 (19.7%) | 0.033 | 0.014 |
| Valvular heart disease | 7,457 (8.6%) | 28,705 (17.1%) | 9,706 (24.2%) | 18,998 (14.9%) | 0.241 | 0.013 |
| Peripheral artery disease | 2,740 (3.2%) | 18,196 (10.8%) | 5,906 (14.7%) | 12,290 (9.6%) | 0.144 | 0.003 |
| Dyslipidemia | 32,085 (37.0%) | 111,830 (66.6%) | 27,026 (67.4%) | 84,804 (66.4%) | 0.02 | 0.006 |
| Chronic kidney disease | 3,218 (3.7%) | 26,277 (15.7%) | 7,795 (19.4%) | 18,482 (14.5%) | 0.121 | 0.002 |
| Chronic liver disease | 1,265 (1.5%) | 7,192 (4.3%) | 2,204 (5.5%) | 4,988 (3.9%) | 0.065 | 0.005 |
| Chronic lung disease | 3,833 (4.4%) | 28,212 (16.8%) | 7,423 (18.5%) | 20,789 (16.3%) | 0.048 | 0.010 |
| Obstructive sleep apnea | 1,712 (2.0%) | 7,061 (4.2%) | 1,875 (4.7%) | 5,186 (4.1%) | 0.023 | 0.014 |
| Cancer | 4,678 (5.4%) | 20,509 (12.2%) | 4,882 (12.2%) | 15,627 (12.2%) | 0.01 | 0.017 |
| Upper GI tract disorder b | 2,681 (3.1%) | 16,497 (9.8%) | 4,470 (11.1%) | 12,027 (9.4%) | 0.047 | 0.005 |
| Lower GI tract disorder b | 3,840 (4.4%) | 13,817 (8.2%) | 3,290 (8.2%) | 10,527 (8.2%) | 0.014 | 0.004 |
| Diabetes mellitus | 11,062 (12.8%) | 71,641 (42.7%) | 19,083 (47.6%) | 52,558 (41.2%) | 0.126 | 0.047 |
| Anemia | 2,227 (2.6%) | 18,886 (11.3%) | 5,777 (14.4%) | 13,109 (10.3%) | 0.112 | 0.013 |
| Thyroid disease | 6,596 (7.6%) | 30,313 (18.1%) | 7,333 (18.3%) | 22,980 (18.0%) | 0.004 | 0.011 |
| Depression | 8,983 (10.4%) | 48,253 (28.7%) | 12,359 (30.8%) | 35,894 (28.1%) | 0.059 | 0.012 |
| Dementia | 2,485 (2.9%) | 11,077 (6.6%) | 2,301 (5.7%) | 8,776 (6.9%) | 0.055 | 0.014 |
| Parkinson's disease | 1,030 (1.2%) | 6,526 (3.9%) | 1,363 (3.4%) | 5,163 (4.0%) | 0.034 | 0.001 |
| History of falling | 2,986 (3.4%) | 17,187 (10.2%) | 3,418 (8.5%) | 13,769 (10.8%) | 0.089 | 0.049 |
| Frailty | 14,002 (16.2%) | 58,483 (34.8%) | 11,398 (28.4%) | 47,085 (36.9%) | 0.187 | 0.017 |
| Prior stroke/SE | 7,691 (8.9%) | 27,704 (16.5%) | 6,986 (17.4%) | 20,718 (16.2%) | 0.019 | 0.006 |
| Prior MB/CRNMB | 2,030 (2.3%) | 12,249 (7.3%) | 3,463 (8.6%) | 8,786 (6.9%) | 0.051 | 0.015 |
| Medication history | ||||||
| Number of concomitant drugs | 2.7+/−1.2 | 8.7+/−3.7 | 9.1+/−4.0 | 8.6+/−3.6 | 0.127 | 0.013 |
| Cardioselective beta blockers | 38,894 (44.9%) | 112,923 (67.3%) | 24,887 (62.0%) | 88,036 (68.9%) | 0.146 | 0.012 |
| Verapamil, diltiazem | 1,647 (1.9%) | 8,256 (4.9%) | 1,852 (4.6%) | 6,404 (5.0%) | 0.019 | 0.016 |
| Digoxin | 4,358 (5.0%) | 18,173 (10.8%) | 3,060 (7.6%) | 15,113 (11.8%) | 0.142 | 0.011 |
| Class I AAD | 6,912 (8.0%) | 16,389 (9.8%) | 2,552 (6.4%) | 13,837 (10.8%) | 0.160 | 0.005 |
| Class III AAD | 13,061 (15.1%) | 48,390 (28.8%) | 9,602 (23.9%) | 38,788 (30.4%) | 0.145 | 0.024 |
| Acetylsalicylic acid | 17,728 (20.5%) | 82,253 (49.0%) | 18,378 (45.8%) | 63,875 (50.0%) | 0.084 | 0.003 |
| P2Y12 inhibitor | 1,028 (1.2%) | 13,653 (8.1%) | 3,212 (8.0%) | 10,441 (8.2%) | 0.006 | 0.015 |
| Proton pump inhibitor | 16,244 (18.8%) | 86,004 (51.2%) | 21,468 (53.5%) | 64,536 (50.5%) | 0.059 | 0.030 |
| NSAID | 15,692 (18.1%) | 47,290 (28.2%) | 12,032 (30.0%) | 35,258 (27.6%) | 0.053 | 0.001 |
| Oral corticosteroids | 8,196 (9.5%) | 43,943 (26.2%) | 11,553 (28.8%) | 32,390 (25.4%) | 0.077 | 0.006 |
| SSRI/SNRI | 3,912 (4.5%) | 27,415 (16.3%) | 7,056 (17.6%) | 20,359 (15.9%) | 0.044 | 0.012 |
| Clinical risk score | ||||||
| CHA 2 DS 2 -VASc score | 2.5+/−1.6 | 4.0+/−1.7 | 3.8+/−1.9 | 4.0+/−1.7 | 0.122 | 0.001 |
| HAS-BLED score | 1.7+/−1.0 | 2.9+/−1.2 | 2.8+/−1.4 | 2.9+/−1.1 | 0.106 | 0.005 |
| Charlson Comorbidity Index | 3.3+/−1.8 | 4.8+/−2.3 | 4.7+/−2.5 | 4.9+/−2.3 | 0.117 | 0.012 |
Abbreviations: AAD, antiarrhythmic drug; AF, atrial fibrillation; CRNMB, clinically relevant nonmajor bleeding; GI, gastrointestinal; MB, major bleeding; NA, not applicable; NOAC, non-vitamin K antagonist oral anticoagulant; NSAID, nonsteroidal anti-inflammatory drug; OAC, oral anticoagulant; SE, systemic embolism; SMD, standardized mean difference; SNRI, serotonin and norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; VKA, vitamin K antagonist.
Note: Data shown as mean +/− standard deviation or counts and percentages. NOAC users without polypharmacy (30.0% reduced dose) included 10,167 dabigatran, 25,581 rivaroxaban, 20,894 apixaban, and 8,710 edoxaban users; NOAC users with polypharmacy (40.9% reduced dose) included 17,977 dabigatran, 48,840 rivaroxaban, 46,031 apixaban, and 14,872 edoxaban users. VKA users without polypharmacy included 9,170 acenocoumarol, 6,798 warfarin, and 5,311 phenprocoumon users; VKA users with polypharmacy included 20,480 acenocoumarol, 10,061 warfarin, and 9,586 phenprocoumon users.
Absolute SMDs illustrated for comparison of NOACs versus VKAs in patients with polypharmacy before and after stabilized inverse probability of treatment weighting.
Upper and lower gastrointestinal tract disorders were defined as gastroesophageal reflux disease or peptic ulcer disease; and diverticulosis, angiodysplasia, colorectal polyposis, or hemorrhoids, respectively.
Moreover, outcomes were compared between NOACs and VKAs, and between individual NOACs in patients with AF and polypharmacy using stabilized inverse probability of treatment weighting (IPTW). In comparisons with apixaban and edoxaban, the study population was restricted to subjects having initiated treatment from September 2013 and from October 2016 onwards respectively, to avoid violations of the positivity assumption. 37 Propensity scores (PS) were calculated with logistic regression models including the 40 confounding covariates described in Table 1 (demographics, comorbidities, medication history, risk scores), stratified by calendar year. Based on the PS, stabilized weights were calculated and truncated at the 0.5th and 99.5th percentile. Covariate balance before and after weighting was checked using standardized mean differences with a ≥0.1 threshold to indicate imbalance. Weighted Cox proportional hazard regression models were used to calculate adjusted hazard ratios (aHRs) with 95% confidence intervals (CIs). The proportional hazard assumption was assessed using scaled Schoenfeld residuals. A two-sided p -value of <0.05 was considered statistically significant. All analyses were performed in R (R version 3.6.0).
Subgroup and Sensitivity Analyses
Analyses were repeated in the subgroup of subjects with baseline hyperpolypharmacy, defined as ≥10 concomitantly used drugs. Moreover, sensitivity analyses were performed to check the robustness of results on the effectiveness and safety of OACs in AF patients with polypharmacy. First, to examine whether estimates were affected by differential censoring between treatment groups (e.g., due to differences in discontinuation or switching rates), analyses were repeated using an intention-to-treat approach, defining the end of follow-up as the first occurrence of an outcome, death, emigration, or end of study period, whichever occurred first. Second, only subjects with an ICD-coded hospital discharge diagnosis of AF before or up to 90 days after the index date were investigated, although this approach resulted in the exclusion of AF subjects treated exclusively in primary or ambulatory care. 38 Lastly, the study population was restricted to subjects having initiated treatment between October 1, 2016 and January 1, 2019, when all NOACs were commercially available in Belgium.
Results
Baseline Characteristics
A total of 254,478 newly treated AF patients were included ( Fig. 1 , Table 1 ). The mean number of concomitantly used drugs at baseline was 6.7 +/− 4.2 (range: 0–41), with drugs acting on the cardiovascular system, blood and blood-forming organs, and alimentary tract and metabolism being most frequently used ( Table 2 ). Only 5,580 (2.2%) subjects used no drugs at baseline. Baseline characteristics of the 167,847 (66.0%) subjects with polypharmacy (mean number of concomitantly used drugs 8.7 +/− 3.7 with 53,418 (21.0%) subjects using ≥10 drugs) and 86,631 (34.0%) subjects without polypharmacy are summarized in Table 1 . Subjects with polypharmacy were older (76.3+/−10.2 vs. 72.5+/−11.6 years) and more frequently female (49.7 vs. 43.1%), had a higher prevalence of cardiovascular comorbidities, and had higher CHA 2 DS 2 -VASc (4.0+/−1.7 vs. 2.5+/−1.6) and HAS-BLED scores (2.9+/−1.2 vs. 1.7+/−1.0) than subjects without polypharmacy. Likewise, P-gp and/or CYP3A4 inhibitors (44.4 vs. 19.9%) or inducers (2.8 vs. 0.8%) and pharmacodynamically interacting drugs (76.5 vs. 35.4%) were more frequently used by patients with polypharmacy than without ( Table 2 ).
Fig. 1.

Flowchart of study population. AF, atrial fibrillation; CKD, chronic kidney disease; DVT, deep vein thrombosis; IMA, InterMutualistic Agency; NOAC, non-vitamin K antagonist oral anticoagulant; OAC, oral anticoagulant; PE, pulmonary embolism; VKA, vitamin K antagonist.
Table 2. Distribution of drug classes based on the WHO ATC classification 29 and pharmacokinetically and -dynamically interacting drugs concomitantly used during ≥30 days in the last 6 months before OAC initiation among anticoagulated AF patients with versus without polypharmacy (≥5 vs. <5 concomitantly used drugs) .
| Drug class | 0–4 drugs ( n = 86,631) |
≥5 drugs ( n = 167,847) |
|---|---|---|
| Alimentary tract and metabolism | 21,499 (26.4%) | 126,138 (75.2%) |
| Blood and blood-forming organs (excluding NOACs and VKAs) | 30,661 (37.7%) | 126,119 (75.1%) |
| Cardiovascular system | 65,450 (80.4%) | 162,600 (96.9%) |
| Dermatological drugs | 1,521 (1.9%) | 12,179 (7.3%) |
| Genitourinary system and sex hormones | 2,446 (3.0%) | 16,645 (9.9%) |
| Systemic hormonal preparations, excluding sex hormones and insulins | 6,123 (7.5%) | 42,579 (25.4%) |
| Anti-infective drugs for systemic use | 3,553 (4.4%) | 28,549 (17.0%) |
| Antineoplastic and immunomodulating agents | 1,567 (1.9%) | 11,275 (6.7%) |
| Musculoskeletal system | 11,959 (14.7%) | 54,849 (32.7%) |
| Nervous system | 16,332 (20.1%) | 100,910 (60.1%) |
| Antiparasitic products, insecticides, and repellents | 47 (0.1%) | 399 (0.2%) |
| Respiratory system | 11,471 (14.1%) | 68,531 (40.8%) |
| Sensory organs | 3,910 (4.8%) | 20,957 (12.5%) |
| Various | 190 (0.2%) | 2,307 (1.4%) |
| Interacting drug use | ||
| ≥1 mild–moderate–strong P-gp and/or CYP3A4 inhibitor | 17,237 (19.9%) | 74,476 (44.4%) |
| ≥1 mild–moderate–strong P-gp and/or CYP3A4 inducer | 695 (0.8%) | 4,765 (2.8%) |
| ≥1 PD DDI (antiplatelet, NSAID, corticosteroid, SSRI/SNRI) | 30,710 (35.4%) | 128,390 (76.5%) |
Abbreviations: AF, atrial fibrillation; CYP3A4, cytochrome P450 enzyme 3A4; NOAC, non-vitamin K antagonist oral anticoagulant; NSAID, nonsteroidal anti-inflammatory drug; OAC, oral anticoagulant; P-gp, P-glycoprotein; SNRI, serotonin and norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; VKA, vitamin K antagonist.
Among subjects with polypharmacy, the 127,720 NOAC and 40,127 VKA users were on average 77.4+/−9.6 and 72.8+/−11.5 years old and had a mean CHA 2 DS 2 -VASc score of 4.0+/−1.7 and 3.8+/−1.9 before weighting, respectively ( Table 1 ). Baseline characteristics of the 17,977 dabigatran, 48,840 rivaroxaban, 46,031 apixaban, and 14,872 edoxaban users with polypharmacy are summarized in Supplementary Table S4 (available in the online version). After weighting, covariate balance was achieved ( Table 1 , Supplementary Fig. S2 , available in the online version).
Polypharmacy versus No Polypharmacy
During a mean follow-up of 1.3+/−1.5 years among both anticoagulated patients with (217,362 person-years) and without polypharmacy (111,434 person-years), 7,380 subjects had an event of stroke/SE (event rates 2.6 vs. 1.8 per 100 person-years), 24,853 subjects died (9.3 vs. 4.1 per 100 person-years), and 14,716 subjects had a major bleeding (5.5 vs. 3.1 per 100 person-years) ( Table 3 ). Crude, age- and sex-adjusted, and multivariable aHRs of outcomes are summarized in Table 4 . After multivariable adjustment, baseline polypharmacy compared to no polypharmacy in AF patients initiating anticoagulation was associated with significantly higher risks of stroke/SE (aHR: 1.08, 95% CI: 1.02–1.15), all-cause mortality (aHR: 1.45, 95% CI: 1.40–1.50), and major bleeding (aHR: 1.29, 95% CI: 1.23–1.35).
Table 3. The number of events and crude event rates per 100 person-years of outcomes in anticoagulated patients with AF.
| Outcome | No polypharmacy (<5 drugs) | Polypharmacy (≥5 drugs) | ||||||
|---|---|---|---|---|---|---|---|---|
| Overall polypharmacy | VKA | NOAC | Dabigatran | Rivaroxaban | Apixaban | Edoxaban | ||
| Events (per 100 PY) | Events (per 100 PY) | Events (per 100 PY) | Events (per 100 PY) | Events (per 100 PY) | Events (per 100 PY) | Events (per 100 PY) | Events (per 100 PY) | |
| Effectiveness | ||||||||
| Stroke/SE | 1,953 (1.78) | 5,427 (2.55) | 1,276 (3.71) | 4,151 (2.33) | 658 (2.34) | 1,770 (2.25) | 1,447 (2.38) | 276 (2.61) |
| Ischemic stroke | 1,008 (0.91) | 2,887 (1.34) | 643 (1.84) | 2,244 (1.25) | 403 (1.42) | 963 (1.21) | 748 (1.22) | 130 (1.22) |
| All-cause mortality | 4,555 (4.09) | 20,298 (9.34) | 3,584 (10.11) | 16,714 (9.19) | 2,098 (7.28) | 6,995 (8.71) | 6,474 (10.42) | 1,147 (10.74) |
| Safety | ||||||||
| Major bleeding | 3,306 (3.05) | 11,410 (5.48) | 2,119 (6.27) | 9,291 (5.32) | 1,352 (4.89) | 4,318 (5.65) | 2,819 (4.69) | 802 (7.74) |
| Intracranial bleeding | 945 (0.86) | 2,857 (1.33) | 593 (1.70) | 2,264 (1.26) | 366 (1.29) | 1,057 (1.34) | 694 (1.13) | 147 (1.38) |
| Gastrointestinal bleeding | 1,684 (1.53) | 5,969 (2.80) | 936 (2.69) | 5,033 (2.82) | 750 (2.65) | 2,424 (3.09) | 1,403 (2.30) | 456 (4.34) |
Abbreviations: NOAC, non-vitamin K antagonist oral anticoagulant; PY, person-year; SE, systemic embolism; VKA, vitamin K antagonist.
Table 4. Crude, age- and sex-adjusted, and multivariable adjusted hazard ratios with 95% confidence intervals of outcomes compared between anticoagulated AF patients with versus without polypharmacy (≥5 vs. <5 concomitantly used drugs) using cox proportional hazard regression models.
| Polypharmacy vs. no polypharmacy (≥5 vs. <5 drugs) | |||
|---|---|---|---|
| Crude HR (95% CI) | Age- and sex-adjusted HR (95% CI) a | Multivariable-adjusted HR (95% CI) b | |
| Effectiveness | |||
| Stroke/SE | 1.42 (1.35–1.50) | 1.37 (1.30–1.44) | 1.08 (1.02–1.15) |
| Ischemic stroke | 1.47 (1.36–1.57) | 1.36 (1.27–1.47) | 1.09 (1.01–1.18) |
| All-cause mortality | 2.27 (2.20–2.35) | 2.00 (1.94–2.07) | 1.45 (1.40–1.50) |
| Safety | |||
| Major bleeding | 1.79 (1.72–1.86) | 1.72 (1.66–1.79) | 1.29 (1.23–1.35) |
| Intracranial bleeding | 1.54 (1.43–1.66) | 1.54 (1.43–1.66) | 1.23 (1.14–1.33) |
| Gastrointestinal bleeding | 1.82 (1.73–1.93) | 1.73 (1.64–1.83) | 1.32 (1.24–1.40) |
Abbreviations: AF, atrial fibrillation; CI, confidence interval; HR, hazard ratio; OAC, oral anticoagulant; SE, systemic embolism.
Adjusted for age and sex.
Adjusted for age, sex, OAC type, baseline comorbidities, and medication history with backward elimination.
NOAC versus VKA Comparison in Patients with Polypharmacy
The unadjusted number of events and event rates among subjects with AF and polypharmacy are summarized in Table 3 . After multivariable adjustment, NOAC use in AF patients with polypharmacy was associated with significantly lower risks of stroke/SE (aHR: 0.68, 95% CI: 0.63–0.73), ischemic stroke (aHR: 0.68, 95% CI: 0.61–0.75), all-cause mortality (aHR: 0.80, 95% CI: 0.77–0.84), major bleeding (aHR: 0.92, 95% CI: 0.87–0.97), and intracranial bleeding (aHR: 0.77, 95% CI: 0.69–0.85) compared to VKAs, but higher risk of gastrointestinal bleeding (aHR: 1.10, 95% CI: 1.01–1.19) ( Supplementary Table S5 , available in the online version>).
Dabigatran, rivaroxaban, apixaban, and edoxaban were associated with significantly lower risks of stroke/SE and all-cause mortality compared to VKAs. For dabigatran, rivaroxaban, and apixaban, lower risks of ischemic stroke were observed, but with edoxaban the risk was not significantly different compared to VKAs (aHR: 0.73, 95% CI: 0.51–1.03) ( Fig. 2 ).
Fig. 2.

The ( A ) effectiveness and ( B ) safety of NOACs versus VKAs in AF patients with polypharmacy (≥5 concomitantly used drugs) after IPTW. The weighted number of subjects at risk in the pseudo-population, weighted number of events, weighted event rates per 100 PY, and adjusted HRs with 95% CIs after IPTW are illustrated. aHR, adjusted hazard ratio; CI, confidence interval; HR, hazard ratio; IPTW, inverse probability of treatment weighting; NOAC, non-vitamin K antagonist oral anticoagulant; PY, person-years; Ref. reference category; SE, systemic embolism; VKA, vitamin K antagonist.
The risk of major bleeding was significantly lower with apixaban (aHR: 0.79, 95% CI: 0.74–0.85) compared to VKAs, while nonsignificantly different with dabigatran (aHR: 0.95, 95% CI: 0.88–1.03), rivaroxaban (aHR: 1.03, 95% CI: 0.97–1.09), and edoxaban (aHR: 0.95, 95% CI: 0.81–1.11). Lower risks of intracranial bleeding were observed with rivaroxaban (aHR: 0.89, 95% CI: 0.80–0.99) and apixaban (aHR: 0.75, 95% CI: 0.65–0.86) compared to VKAs, whereas risks were not significantly different with dabigatran (aHR: 0.90, 95% CI: 0.78–1.04) or edoxaban (aHR: 1.06, 95% CI: 0.71–1.58). Compared to VKAs, dabigatran (aHR: 1.16, 95% CI: 1.04–1.29) and rivaroxaban (aHR: 1.26, 95% CI: 1.16–1.37) were associated with significantly higher risks of gastrointestinal bleeding, edoxaban with a nonsignificantly different risk (aHR: 1.10, 95% CI: 0.87–1.38), while apixaban with a significantly lower risk (aHR: 0.84, 95% CI: 0.76–0.93).
NOAC versus NOAC Comparison in Patients with Polypharmacy
No significant differences in the risks of stroke/SE and ischemic stroke were observed between individual NOACs in patients with polypharmacy ( Supplementary Table S6 [available in the online version], Fig. 3 ). Dabigatran (aHR: 0.90, 95% CI: 0.85–0.94) and edoxaban (aHR: 0.90, 95% CI: 0.83–0.98) were associated with significantly lower risks of all-cause mortality compared to rivaroxaban, while higher mortality risks were observed with apixaban compared to dabigatran (aHR: 1.16, 95% CI: 1.09–1.22) and edoxaban (aHR: 1.12, 95% CI: 1.05–1.21). No significant differences in the risk of death were observed between dabigatran and edoxaban, or apixaban and rivaroxaban.
Fig. 3.

The ( A ) effectiveness and ( B ) safety compared between individual NOAC types in AF patients with polypharmacy (≥5 concomitantly used drugs) after IPTW. The weighted number of subjects at risk in the pseudo-population, weighted number of events, weighted event rates per 100 PY, and adjusted HRs with 95% CIs after IPTW are illustrated. aHR, adjusted hazard ratio; CI, confidence interval; HR, hazard ratio; IPTW, inverse probability of treatment weighting; NOAC, non-vitamin K antagonist oral anticoagulant; PY, person-years; Ref, reference category; SE, systemic embolism.
Dabigatran (aHR: 0.91, 95% CI: 0.85–0.97) and apixaban (aHR: 0.77, 95% CI: 0.73–0.81) were associated with significantly lower risks of major bleeding in AF patients with polypharmacy compared to rivaroxaban, driven by significantly lower risks of gastrointestinal bleeding (aHR: 0.90, 95% CI: 0.83–0.98 and aHR: 0.66, 95% CI: 0.62-0.71, respectively). Major and gastrointestinal bleeding risks were also significantly lower with apixaban compared to dabigatran (HR: 0.83, 95% CI: 0.77–0.90 and aHR: 0.72, 95% CI: 0.65–0.79, respectively) and edoxaban (HR: 0.77, 95% CI: 0.70–0.85 and aHR: 0.68, 95% CI: 0.60–0.77, respectively). No significant differences in the risks of major or gastrointestinal bleeding were observed between dabigatran and edoxaban, or rivaroxaban and edoxaban, except for a significantly lower gastrointestinal bleeding risk with edoxaban compared to rivaroxaban (aHR: 0.86, 95% CI: 0.76–0.99). The risk of intracranial bleeding was similar between individual NOACs.
Hyperpolypharmacy
Hyperpolypharmacy (≥10 drugs) was identified in 53,418 (21.0%) subjects (mean follow-up: 1.1+/−1.3 years; 57,748 person-years) ( Supplementary Table S7 , available in the online version). Event rates are summarized in Supplementary Table S8 (available in the online version). After multivariable adjustment, hyperpolypharmacy was associated with significantly higher risks of stroke/SE (aHR: 1.17, 95% CI: 1.07–1.27), all-cause mortality (aHR: 1.92, 95% CI: 1.82–2.02), and major bleeding (aHR: 1.49, 95% CI: 1.39–1.60) compared to AF patients without polypharmacy (<5 drugs) ( Supplementary Table S9 , available in the online version>).
In AF patients with hyperpolypharmacy, NOACs were associated with significantly lower risks of stroke/SE (aHR: 0.73, 95% CI: 0.65–0.82), ischemic stroke (aHR: 0.75, 95% CI: 0.64–0.87), and all-cause mortality (aHR: 0.93, 95% CI: 0.87–0.98) compared to VKAs, while no significant differences in the risks of major, intracranial, or gastrointestinal bleeding were observed ( Supplementary Table S10 , Supplementary Fig. S3 [available in the online version]). Results on the comparative effectiveness and safety of individual NOACs in AF patients with hyperpolypharmacy were consistent with the main analysis ( Supplementary Table S11 , Supplementary Fig. S3 [available in the online version]).
Sensitivity Analyses
Trends on the risk–benefit profile of NOACs in patients with polypharmacy were consistent with an intention-to-treat approach (mean follow-up: 2.5+/−1.7 years; 419,122 person-years), although the risk of gastrointestinal bleeding was significantly higher with edoxaban compared to VKAs (aHR: 1.28, 95% CI: 1.08–1.51) ( Supplementary Table S12 , Supplementary Fig. S4 [available in the online version]). Likewise, results were consistent when restricting the study population to subjects with an ICD-coded hospital discharge diagnosis of AF ( n = 90,476) ( Supplementary Table S13 , Supplementary Fig. S5 [available in the online version]) or to subjects having initiated treatment between October 2016 and January 2019 ( n = 61,266) ( Supplementary Table S14 , Supplementary Fig. S6 [available in the online version]). However, no significant differences in the risk of intracranial bleeding were observed between individual NOACs and VKAs in the latter analysis.
Discussion
In the present nationwide cohort study including more than 250,000 AF patients during 328,796 person-years of on-treatment follow-up, 66% and 21% of patients concomitantly used ≥5 and ≥10 drugs when initiating anticoagulation, respectively. Baseline polypharmacy was an independent risk factor for thromboembolism, major bleeding, and all-cause mortality. Among AF patients with polypharmacy, NOACs were associated with significantly lower risks of stroke/SE, major bleeding, and all-cause mortality compared to VKAs. Although the effectiveness was similar, apixaban appeared to be associated with the most favorable safety profile across NOACs in patients with polypharmacy due to a lower gastrointestinal bleeding risk. However, caution should be warranted, given the higher observed mortality risk with apixaban compared to dabigatran and edoxaban.
In clinical practice, polypharmacy is highly prevalent in AF patients (e.g., 64–77% of patients included in phase III RCTs used ≥5 drugs). 4 5 6 Polypharmacy has been associated with worse health outcomes irrespective of AF, such as hospitalization, institutionalization, falls, frailty, and death. 4 8 Among AF patients initiating anticoagulation in the present study, polypharmacy was an independent risk factor of thromboembolism, bleeding, and death (8%, 29% and 45% significantly increased risk, respectively), which was even more pronounced among subjects concomitantly using ≥10 drugs (17%, 49% and 92% higher risks, respectively), suggestive of an incremental risk of adverse outcomes by increasing pill burden. Although the observed relationship between polypharmacy and increased risks of bleeding and death is in line with prior research, 3 4 5 6 7 results are more conflicting on thromboembolic risks. Regarding the latter, a posthoc analysis of the ARISTOTLE trial 4 also observed higher stroke/SE risks in AF patients with polypharmacy, while other studies 3 5 6 7 did not. However, these studies may have been limited in power due to small sample sizes, short follow-up durations, and low number of events. 5 Nevertheless, these findings highlight the increased vulnerability of AF patients concomitantly using multiple drugs at the time of OAC initiation.
Proposed mechanisms for the increased thromboembolic, bleeding, and mortality risks in case of polypharmacy include the influence of underlying multimorbidity, disease severity, and frailty; reduced therapy adherence or persistence due to drug regimen complexity, intake errors, and adverse drug reactions; and drug–drug interactions. 3 4 5 7 8 10 11 12 13 26 39 Potential drug–drug interactions were more frequently observed in patients with polypharmacy (e.g., 44% used ≥1 P-gp and/or CYP3A4 inhibitor and 2.8% ≥1 P-gp and/or CYP3A4 inducer) as compared to patients without polypharmacy (20% and 0.8%, respectively). Higher bleeding and mortality risks have indeed been demonstrated in NOAC-treated AF patients with versus without concomitant use of P-gp and/or CYP3A4 inhibitors (pharmacokinetic interaction), which may have contributed to the worse outcomes in patients with polypharmacy. 10 Likewise, higher bleeding risks have been reported in NOAC-treated patients concomitantly using antiplatelets, nonsteroidal anti-inflammatory drugs (NSAIDs), selective serotonin reuptake inhibitors, or corticosteroids (pharmacodynamic interaction), which were also more frequently used by patients with polypharmacy (76% vs. 35%). 17 18 19
The benefit–risk profile of NOACs is preserved in AF patients with polypharmacy, as demonstrated by the 32%, 8%, 23% and 20% reduced risk of stroke/SE, major bleeding, intracranial bleeding, and all-cause mortality, respectively, compared to VKAs, although the risk of gastrointestinal bleeding was 10% higher. However, differences in safety between NOACs were observed, as apixaban was the only NOAC associated with a significantly lower risk of major bleeding compared to VKAs in patients with polypharmacy, and only apixaban and rivaroxaban were associated with significantly lower risks of intracranial bleeding compared to VKAs. Likewise, lower risks of major and gastrointestinal bleeding were observed with dabigatran and apixaban compared to rivaroxaban, and with apixaban compared to dabigatran and edoxaban.
Comparable findings have been observed in the general AF population, 40 41 as well as in patients with polypharmacy. Posthoc analyses of RCTs and observational studies have indeed demonstrated that NOACs were associated with similar 4 5 26 27 to lower 3 6 12 25 28 39 risks of stroke/SE, similar 4 5 26 to lower 3 6 39 risks of all-cause mortality, and similar 3 39 to lower 27 risks of major bleeding compared to VKAs in patients with polypharmacy.
Potential differences in safety across NOACs were also observed, as the risk of major bleeding was similar 26 to lower 4 12 27 with apixaban, similar 6 27 to lower 12 with dabigatran, and similar 12 25 26 28 to higher 5 27 with rivaroxaban compared to VKAs in patients with polypharmacy, driven by differential gastrointestinal bleeding risks.
To the best of our knowledge, only two observational studies 12 26 compared outcomes between NOACs (however not including edoxaban) in patients with polypharmacy. In the ARISTOPHANES study, Lip et al. have demonstrated that the risks of major and gastrointestinal bleeding were significantly lower with dabigatran and apixaban compared to rivaroxaban, and with apixaban compared to dabigatran in patients using ≥6 drugs, as also observed in our study. 12 However, this observation was not confirmed by the study of Mentias et al. investigating 723 PS-matched apixaban and rivaroxaban users using ≥9 drugs, showing similar risks of major bleeding and gastrointestinal bleeding. 26
Although in the study by Mentias et al 26 and the present study, the effectiveness between NOACs was comparable, Lip et al. 12 illustrated that apixaban was associated with lower risks of stroke/SE compared to dabigatran and rivaroxaban.
In the present study, we observed significantly higher risks of all-cause mortality with apixaban compared to dabigatran and edoxaban, which is in line with the higher mortality risks with apixaban compared to rivaroxaban observed by Mentias et al. 26 However, the impact of unmeasured confounding (e.g., underweight or renal dysfunction) or selective prescribing of apixaban to the oldest and sickest AF patients using multiple drugs cannot be excluded, despite using IPTW to adjust for confounding by indication. Exemplary, apixaban users with polypharmacy were older, had more comorbidities, and had higher risk scores than other NOAC users ( Supplementary Table S4 [available in the online version]). More studies are needed to replicate these exploratory findings, including cause-specific mortality, while in the meantime, caution should be warranted.
Based on this study, NOACs should still be preferred over VKAs in case of (hyper)polypharmacy. However, a thorough medication review as a part of comprehensive geriatric assessment 42 to switch or discontinue unnecessary, interacting, or contraindicated comedication (e.g., nonindicated use of antiplatelets or NSAIDs) 10 11 43 44 should be performed in a multidisciplinary, patient-centered approach. 2 3 7 Judicious “deprescribing” may reduce the pill burden, adverse drug reactions, and drug–drug interactions. 3 7 Moreover, given that polypharmacy was independently associated with a 29% higher risk of major bleeding, clinicians should identify and tackle modifiable bleeding risk factors (e.g., uncontrolled hypertension, excessive alcohol consumption, …) and more regularly monitor patients with polypharmacy initiating anticoagulation. 43 44 Furthermore, clinicians should initialize fall prevention, 45 optimize therapy adherence, 13 and perform an individualized benefit–risk assessment with shared decision making in each AF patient with (hyper)polypharmacy. 2 Lastly, as endorsed by international guidelines, 22 24 patients with AF should be treated according the Atrial fibrillation Better Care (ABC) pathway, an integrated holistic approach which has been associated with improved clinical outcomes. 46
Strengths and Limitations
Strengths of this nationwide cohort study include the large sample size, long-term follow-up, use of an on-treatment analysis to reduce exposure misclassification, specifying a minimal duration of concomitant use to define polypharmacy, and adjustment for several confounders using stabilized IPTW.
The present study has also several limitations. First, coding errors and misclassification bias may be present due to the observational design using health care databases. However, by identifying comorbidities based on ICD, medical procedure codes and/or medication prescription claims assessed in ambulatory and hospital care, missing data, and misclassification of characteristics were reduced. Second, polypharmacy was based on drug prescription claims up to 6 months months before OAC initiation, without accounting for initiation, discontinuation, or switching of drugs during follow-up. 3 4 5 26 Likewise, a cut-off of ≥5 concomitantly used drugs during ≥30 days to define polypharmacy, remains arbitrary although widely accepted. 1 3 4 8 Moreover, use of over-the-counter drugs could not be identified. Third, although we thoroughly adjusted for confounders, there is a risk of unmeasured confounding due to missing lifestyle characteristics (e.g., body weight, smoking) and laboratory values (e.g., renal function, INR). In line, (in)appropriate NOAC dosing and time in therapeutic range of VKA users could not be assessed. Fourth, although persons with competing treatment indications were excluded (e.g., pulmonary embolism), subjects were not required to have an ICD-coded hospital discharge diagnosis of AF to be included, as this would have limited the study population to hospitalized AF subjects and excluded AF subjects treated exclusively in primary or ambulatory care. 38 Nevertheless, trends were consistent when specifically investigating subjects with an ICD-coded diagnosis of AF within 1 year before or up to 90 days the index date (to reduce misclassification bias while potentially introducing selection bias). Fifth, the follow-up duration of edoxaban users was considerably shorter than that of other NOACs due to variable approval dates. Nevertheless, effect estimates were consistent when restricting the study population to subjects having initiated treatment since October 2016. Sixth, data were lacking on the cause of death, which would have been of interest to explore why differences in the risk of all-cause mortality between individual NOACs were observed. Lastly, anticoagulant use was assessed based on dispensing data to account for discontinuation or switch of treatment. However, findings were consistent using an intention-to-treat approach.
Conclusion
In the present study, polypharmacy was an independent risk factor for thromboembolism, bleeding, and death in anticoagulated patients with AF. NOACs were associated with significantly lower thromboembolic, bleeding, and mortality risks in patients with polypharmacy compared to VKAs. The effectiveness of individual NOACs was comparable, but safety outcomes differed with apixaban being associated with the most favorable safety profile across NOACs, driven by lower gastrointestinal bleeding risks. However, more research is needed on the potentially increased risk of all-cause mortality with apixaban compared to dabigatran and edoxaban.
Acknowledgment
We would like to thank the administrators, data managers, statisticians, and other staff of the InterMutualistic Agency (IMA) and Minimal Hospital Dataset (MHD) for providing the data, especially Birgit Gielen (IMA), David Jaminé (IMA), Iris Grant (IMA), Dirk De Kesel (IMA), Sarah Bel (IMA), Jérôme Paque (IMA), Remi Vandereyd (IMA), Xavier Rygaert (IMA), Delfien Verhelst (MHD), Karin Smets (MHD), and Francis Windey (MHD). Moreover, we would like to thank eHealth for the deterministic linkage of both databases. Lastly, we would like to thank Stephan Devriese (Belgian Health Care Knowledge Centre, KCE) for performing the small cell risk analysis.
Funding Statement
Funding This work was supported by grants from the Research Foundation Flanders (FWO) (grant number 11C0820N to Maxim Grymonprez).
Conflict of Interest Outside this manuscript, T.D.B. has served as a chairperson during a lecture for Bayer and Daiichi Sankyo and participated in an expert meeting for Pfizer. Outside this manuscript, L.L. has been consulted as an expert for AstraZeneca. Outside this manuscript, M.P. and S.S. have given a lecture sponsored by BMS, L.L. a lecture sponsored by Chiesi, and S.S., L.L., and M.G. lectures sponsored by IPSA vzw, a nonprofit organization facilitating lifelong learning for health care providers. None of the authors has received any fees personally.
Data Availability Statement
Requests for the data underlying this article should be directed to the administrators of the Inter Mutualistic Agency (IMA) database or Minimal Hospital Dataset and is subject to approval.
Authors' Contribution
M.G. and L.L. contributed to the concept and design of the study. M.G. performed the statistical analysis, interpretation, and writing under the supervision of L.L. M.P., T.D.B., S.S., and L.L. revised the manuscript critically. All authors contributed to the article and approved the final version of the manuscript.
What is known about this topic?
Although non-vitamin K antagonist oral anticoagulants (NOACs) are recommended over vitamin K antagonists (VKAs) in atrial fibrillation (AF) management, polypharmacy may affect their effectiveness and safety due to underlying comorbidities, reduced therapy adherence, adverse drug reactions, and especially drug–drug interactions.
However, long-term comparative data are lacking in AF patients with polypharmacy to guide physicians in their choice of NOAC.
What does this paper add?
Among 254,478 AF patients during 328,796 person-years of follow-up, baseline polypharmacy, identified in 66% of patients, was an independent risk factor for thromboembolism, major bleeding, and all-cause mortality.
Among AF patients with polypharmacy, NOACs were associated with significantly lower risks of stroke/SE, major bleeding, and all-cause mortality compared to VKAs.
While effectiveness was comparable between individual NOACs, apixaban was overall associated with a more favorable safety profile in patients with polypharmacy due to a lower gastrointestinal bleeding risk. However, higher mortality risks were observed with apixaban compared to dabigatran and edoxaban.
Supplementary Material
References
- 1.Masnoon N, Shakib S, Kalisch-Ellett L, Caughey G E. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017;17(01):230. doi: 10.1186/s12877-017-0621-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Grymonprez M, Steurbaut S, De Backer T L, Petrovic M, Lahousse L. Effectiveness and safety of oral anticoagulants in older patients with atrial fibrillation: a systematic review and meta-analysis. Front Pharmacol. 2020;11:583311. doi: 10.3389/fphar.2020.583311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Harskamp R E, Teichert M, Lucassen W AM, van Weert H CPM, Lopes R D. Impact of polypharmacy and P-glycoprotein- and CYP3A4-modulating drugs on safety and efficacy of oral anticoagulation therapy in patients with atrial fibrillation. Cardiovasc Drugs Ther. 2019;33(05):615–623. doi: 10.1007/s10557-019-06907-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jaspers Focks J, Brouwer M A, Wojdyla D M et al. Polypharmacy and effects of apixaban versus warfarin in patients with atrial fibrillation: post hoc analysis of the ARISTOTLE trial. BMJ. 2016;353:i2868. doi: 10.1136/bmj.i2868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Piccini J P, Hellkamp A S, Washam J B et al. Polypharmacy and the efficacy and safety of rivaroxaban versus warfarin in the prevention of stroke in patients with nonvalvular atrial fibrillation. Circulation. 2016;133(04):352–360. doi: 10.1161/CIRCULATIONAHA.115.018544. [DOI] [PubMed] [Google Scholar]
- 6.Millenaar D, Schumacher H, Brueckmann M et al. Cardiovascular outcomes according to polypharmacy and drug adherence in patients with atrial fibrillation on long-term anticoagulation (from the RE-LY trial) Am J Cardiol. 2021;149:27–35. doi: 10.1016/j.amjcard.2021.03.024. [DOI] [PubMed] [Google Scholar]
- 7.Proietti M, Raparelli V, Olshansky B, Lip G Y. Polypharmacy and major adverse events in atrial fibrillation: observations from the AFFIRM trial. Clin Res Cardiol. 2016;105(05):412–420. doi: 10.1007/s00392-015-0936-y. [DOI] [PubMed] [Google Scholar]
- 8.Franchi C, Marcucci M, Mannucci P M et al. Changes in clinical outcomes for community-dwelling older people exposed to incident chronic polypharmacy: a comparison between 2001 and 2009. Pharmacoepidemiol Drug Saf. 2016;25(02):204–211. doi: 10.1002/pds.3938. [DOI] [PubMed] [Google Scholar]
- 9.GLORIA-AF Investigators . Romiti G F, Proietti M, Bonini N et al. Clinical complexity domains, anticoagulation, and outcomes in patients with atrial fibrillation: a report from the GLORIA-AF registry phase II and III. Thromb Haemost. 2022;122(12):2030–2041. doi: 10.1055/s-0042-1756355. [DOI] [PubMed] [Google Scholar]
- 10.Grymonprez M, Vanspranghe K, Capiau A, Boussery K, Steurbaut S, Lahousse L. Impact of P-glycoprotein and/or CYP3A4-interacting drugs on effectiveness and safety of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation: a meta-analysis. Br J Clin Pharmacol. 2022;88(07):3039–3051. doi: 10.1111/bcp.15265. [DOI] [PubMed] [Google Scholar]
- 11.Grymonprez M, Vanspranghe K, Steurbaut S, De Backer T L, Lahousse L. Non-vitamin K antagonist oral anticoagulants (NOACs) versus warfarin in patients with atrial fibrillation using P-gp and/or CYP450-interacting drugs: a systematic review and meta-analysis. Cardiovasc Drugs Ther. 2023;37:781–791. doi: 10.1007/s10557-021-07279-8. [DOI] [PubMed] [Google Scholar]
- 12.Lip G YH, Keshishian A, Kang A et al. Effectiveness and safety of oral anticoagulants among non-valvular atrial fibrillation patients with polypharmacy. Eur Heart J Cardiovasc Pharmacother. 2021;7(05):405–414. doi: 10.1093/ehjcvp/pvaa117. [DOI] [PubMed] [Google Scholar]
- 13.Grymonprez M, Capiau A, Steurbaut S et al. Adherence and persistence to oral anticoagulants in patients with atrial fibrillation: a Belgian nationwide cohort study. Front Cardiovasc Med. 2022;9:994085. doi: 10.3389/fcvm.2022.994085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rose A J, Hylek E M, Ozonoff A, Ash A S, Reisman J I, Berlowitz D R. Patient characteristics associated with oral anticoagulation control: results of the Veterans AffaiRs Study to Improve Anticoagulation (VARIA) J Thromb Haemost. 2010;8(10):2182–2191. doi: 10.1111/j.1538-7836.2010.03996.x. [DOI] [PubMed] [Google Scholar]
- 15.Mazzone A, Bo M, Lucenti A, Galimberti S, Bellelli G, Annoni G. The role of comprehensive geriatric assessment and functional status in evaluating the patterns of antithrombotic use among older people with atrial fibrillation. Arch Gerontol Geriatr. 2016;65:248–254. doi: 10.1016/j.archger.2016.04.008. [DOI] [PubMed] [Google Scholar]
- 16.Vazquez S R. Drug-drug interactions in an era of multiple anticoagulants: a focus on clinically relevant drug interactions. Blood. 2018;132(21):2230–2239. doi: 10.1182/blood-2018-06-848747. [DOI] [PubMed] [Google Scholar]
- 17.External reviewers . Steffel J, Collins R, Antz M et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Europace. 2021;23(10):1612–1676. doi: 10.1093/europace/euab065. [DOI] [PubMed] [Google Scholar]
- 18.Holm J, Mannheimer B, Malmström R E, Eliasson E, Lindh J D. Bleeding and thromboembolism due to drug-drug interactions with non-vitamin K antagonist oral anticoagulants-a Swedish, register-based cohort study in atrial fibrillation outpatients. Eur J Clin Pharmacol. 2021;77(03):409–419. doi: 10.1007/s00228-020-03015-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zhang Y, Souverein P C, Gardarsdottir H, van den Ham H A, Maitland-van der Zee A H, de Boer A. Risk of major bleeding among users of direct oral anticoagulants combined with interacting drugs: a population-based nested case-control study. Br J Clin Pharmacol. 2020;86(06):1150–1164. doi: 10.1111/bcp.14227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Grymonprez M, De Backer T L, Capiau A et al. Trends in oral anticoagulant use in patients with atrial fibrillation in Belgium from 2013 to 2019: a nationwide cohort study. Br J Clin Pharmacol. 2023;89(04):1360–1373. doi: 10.1111/bcp.15582. [DOI] [PubMed] [Google Scholar]
- 21.Grymonprez M, Simoens C, Steurbaut S, De Backer T L, Lahousse L. Worldwide trends in oral anticoagulant use in patients with atrial fibrillation from 2010 to 2018: a systematic review and meta-analysis. Europace. 2022;24(06):887–898. doi: 10.1093/europace/euab303. [DOI] [PubMed] [Google Scholar]
- 22.ESC Scientific Document Group . Hindricks G, Potpara T, Dagres N et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(05):373–498. doi: 10.1093/eurheartj/ehaa612. [DOI] [PubMed] [Google Scholar]
- 23.Writing Group Members . January C T, Wann L S, Calkins H et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm. 2019;16(08):e66–e93. doi: 10.1016/j.hrthm.2019.01.024. [DOI] [PubMed] [Google Scholar]
- 24.Chao T F, Joung B, Takahashi Y et al. 2021 Focused Update Consensus Guidelines of the Asia Pacific Heart Rhythm Society on Stroke Prevention in Atrial Fibrillation: Executive Summary. Thromb Haemost. 2022;122(01):20–47. doi: 10.1055/s-0041-1739411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Martinez B K, Baker W L, Sood N A et al. Influence of polypharmacy on the effectiveness and safety of rivaroxaban versus warfarin in patients with nonvalvular atrial fibrillation. Pharmacotherapy. 2019;39(02):196–203. doi: 10.1002/phar.2213. [DOI] [PubMed] [Google Scholar]
- 26.Mentias A, Heller E, Vaughan Sarrazin M. Comparative effectiveness of rivaroxaban, apixaban, and warfarin in atrial fibrillation patients with polypharmacy. Stroke. 2020;51(07):2076–2086. doi: 10.1161/STROKEAHA.120.029541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hohmann C, Hohnloser S H, Jacob J, Walker J, Baldus S, Pfister R. Non-vitamin K oral anticoagulants in comparison to phenprocoumon in geriatric and non-geriatric patients with non-valvular atrial fibrillation. Thromb Haemost. 2019;119(06):971–980. doi: 10.1055/s-0039-1683422. [DOI] [PubMed] [Google Scholar]
- 28.Alberts M J, He J, Kharat A, Ashton V. Effectiveness and safety of rivaroxaban versus warfarin among nonvalvular atrial fibrillation patients with obesity and polypharmacy. Am J Cardiovasc Drugs. 2022;22(04):425–436. doi: 10.1007/s40256-021-00520-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.InterMutualistic Agency (IMA/AIM) . Accessed November 25, 2021 at:https://ima-aim.be/
- 30.The Minimal Hospital Dataset . Accessed November 25, 2021 at:https://www.health.belgium.be/en/node/23607
- 31.The Sectoral Committee of Social Security and Health Section Health ('Informatieveiligheidscomité')Accessed November 25, 2021 athttps://www.ehealth.fgov.be/ehealthplatform/nl/informatieveiligheidscomite
- 32.STROBE Initiative von Elm E, Altman D G, Egger M, Pocock S J, Gøtzsche P C, Vandenbroucke J P.The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies Lancet 2007370(9596):1453–1457. [DOI] [PubMed] [Google Scholar]
- 33.WHO Collaborating Centre for Drug Statistics Methodology . Accessed November 25, 2021 at:https://www.whocc.no/
- 34.Halvorsen S, Ghanima W, Fride Tvete I et al. A nationwide registry study to compare bleeding rates in patients with atrial fibrillation being prescribed oral anticoagulants. Eur Heart J Cardiovasc Pharmacother. 2017;3(01):28–36. doi: 10.1093/ehjcvp/pvw031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Subcommittee on Control of Anticoagulation . Kaatz S, Ahmad D, Spyropoulos A C, Schulman S. Definition of clinically relevant non-major bleeding in studies of anticoagulants in atrial fibrillation and venous thromboembolic disease in non-surgical patients: communication from the SSC of the ISTH. J Thromb Haemost. 2015;13(11):2119–2126. doi: 10.1111/jth.13140. [DOI] [PubMed] [Google Scholar]
- 36.Quan H, Li B, Couris C M et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(06):676–682. doi: 10.1093/aje/kwq433. [DOI] [PubMed] [Google Scholar]
- 37.Austin P C, Stuart E A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med. 2015;34(28):3661–3679. doi: 10.1002/sim.6607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Hellfritzsch M, Pottegård A, Haastrup S B, Rasmussen L, Grove E L. Cohort selection in register-based studies of direct oral anticoagulant users with atrial fibrillation: an inevitable trade-off between selection bias and misclassification. Basic Clin Pharmacol Toxicol. 2020;127(01):3–5. doi: 10.1111/bcpt.13423. [DOI] [PubMed] [Google Scholar]
- 39.Kim I S, Kim H J, Yu H T et al. Non-vitamin K antagonist oral anticoagulants with amiodarone, P-glycoprotein inhibitors, or polypharmacy in patients with atrial fibrillation: systematic review and meta-analysis. J Cardiol. 2019;73(06):515–521. doi: 10.1016/j.jjcc.2018.12.018. [DOI] [PubMed] [Google Scholar]
- 40.Ray W A, Chung C P, Stein C M et al. Association of rivaroxaban vs apixaban with major ischemic or hemorrhagic events in patients with atrial fibrillation. JAMA. 2021;326(23):2395–2404. doi: 10.1001/jama.2021.21222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Rutherford O W, Jonasson C, Ghanima W, Söderdahl F, Halvorsen S. Comparison of dabigatran, rivaroxaban, and apixaban for effectiveness and safety in atrial fibrillation: a nationwide cohort study. Eur Heart J Cardiovasc Pharmacother. 2020;6(02):75–85. doi: 10.1093/ehjcvp/pvz086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ellis G, Whitehead M A, O'Neill D, Langhorne P, Robinson D. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev. 2011;(07):CD006211. doi: 10.1002/14651858.CD006211.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.ESC Scientific Document Group . Steffel J, Verhamme P, Potpara T S et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J. 2018;39(16):1330–1393. doi: 10.1093/eurheartj/ehy136. [DOI] [PubMed] [Google Scholar]
- 44.Gorog D A, Gue Y X, Chao T F et al. Assessment and mitigation of bleeding risk in atrial fibrillation and venous thromboembolism: executive summary of a European and Asia-Pacific Expert Consensus Paper. Thromb Haemost. 2022;122(10):1625–1652. doi: 10.1055/s-0042-1750385. [DOI] [PubMed] [Google Scholar]
- 45.Academy of Geriatric Physical Therapy of the American Physical Therapy Association . Avin K G, Hanke T A, Kirk-Sanchez N et al. Management of falls in community-dwelling older adults: clinical guidance statement from the Academy of Geriatric Physical Therapy of the American Physical Therapy Association. Phys Ther. 2015;95(06):815–834. doi: 10.2522/ptj.20140415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Romiti G F, Pastori D, Rivera-Caravaca J M et al. Adherence to the 'Atrial Fibrillation Better Care' pathway in patients with atrial fibrillation: impact on clinical outcomes-a systematic review and meta-analysis of 285,000 patients. Thromb Haemost. 2022;122(03):406–414. doi: 10.1055/a-1515-9630. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Requests for the data underlying this article should be directed to the administrators of the Inter Mutualistic Agency (IMA) database or Minimal Hospital Dataset and is subject to approval.