

Abstract
Background
To compare the analgesic effect of ISB with a combination of ISB-SSNB and patients who were given opioids with PCA without block in adult patients undergoing shoulder surgery, as measured by opioid consumption and pain intensity in the first 24 hours postoperatively.
Methods
Ninety patients who underwent shoulder surgery were randomly divided into three groups. Group I in which ISB was performed and patient-controlled analgesia (PCA) was inserted, Group II with; ISB and SSNB combined, and PCA was inserted, and Group III where; only PCA was used. Visual analog scale (VAS) pain scores at the second, fourth, sixth, 12th, and 24th hours, morphine consumption, additional analgesic requirement, and patient satisfaction were evaluated.
Results
Compared with Group III, the VAS pain score was significantly lower in Group I and Group II at 2, 4, 6, 12, and 24 hours postoperatively. In Group I, the VAS score at rest at the 6th hour was found to be higher than in Group II. The 24-hour total morphine consumption was higher in the control group than in Group I and Group II. The satisfaction score of the control group was lower than Group I and Group II.
Conclusion
The combined application of ISB and SSNB block is beneficial in shoulder surgery to provide both intraoperative and postoperative analgesia and opioid consumption.
Level of Evidence
Level I; Randomized Controlled Trial; Treatment Study.
Keywords: interscalene block, suprascapular nerve block, shoulder arthroscopic surgery, postoperative analgesia
Introduction
About 30–70% of patients experience severe postoperative pain after arthroscopic shoulder surgery and may need high-dose opioid treatment. Inadequate pain control and stress can lead to chronic pain syndrome. Regional anesthesia techniques help control pain both at rest and during early mobilization in the postoperative period.1,2
Various regional blocks are used for postoperative analgesia in shoulder surgery. The most important of these are the interscalene block (ISB) and suprascapular nerve block (SSNB). Interscalene block reduces opioid consumption with effective analgesia in shoulder surgery.3 ISB affects the radial side of the shoulder and arm. The duration of analgesia may vary between 8 and 24 hours.4,5 The risk of developing phrenic nerve paralysis in patients undergoing shoulder surgery after interscalene block is due to the direct inhibitory effect of local anesthetic on the C3-C5 nerve roots. Phrenic nerve paralysis most commonly presents clinically with dyspnea and hypoxemia.6 It can be diagnosed by observing the absence of diaphragmatic movement with respiration on ultrasound.7
Wertheim and Rovenstine described suprascapular nerve block in 1941, but there are still unknowns in its use in shoulder surgery.8 The suprascapular nerve receives 70% of the sensory nerves from the glenohumeral joint and innervates the infraspinatus and supraspinatus muscles. SSNB affects the posterior and upper region of the shoulder joint, the capsule and the skin covering the shoulder joint. The suprascapular nerve is a mixed nerve that emerges from the upper brachial plexus and contains both motor and sensory fibers. The application of this block is easy, the procedure time is short, it is safe, and the complication rate is very low.9 Phrenic nerve paralysis can be prevented by reducing the volume and concentration of local anesthetic, changing the injection site or technique for interscalene block, or combining interscalene block with other regional techniques.6,10 It has been reported that reducing the volume to 10 mL in blocks performed with ultrasound guidance may decrease the risk of phrenic nerve paralysis by 60%.11
There are many studies with ISB and SSNB. However, there is no study in which ISB and SSNB are applied together, and their effects on opioid consumption are evaluated.12 In our study, we added SSNB to ISB because 50% of the suprascapular nerve originates from the C4 nerve root.
The primary aim of this study was to compare the analgesic effect of ISB-SSNB combination with ISB and patients who were given opioids with PCA without block in adult patients undergoing shoulder surgery. Opioid consumption and pain intensity were measured in the first 24 hours postoperatively. Our second aim was to compare patient satisfaction and complications. The study hypothesized that the combination of ISB and SSNB with low-dose local anesthetics would provide more effective analgesia, minimal complications, and opioid consumption.
Materials and Methods
This study was designed as a prospective randomized study consisting of 90 patients who underwent rotator cuff repair via shoulder arthroscopy between February 22 and December 29, 2021. It was conducted according to the Declaration of Helsinki and approved by the Local Ethics Committee of Erciyes University (Approval number = 2015–580). Clinical Trials number is NCT 04769570. Patients with ASA (American Society of Anesthesiology) I and II and between the ages of 18–65 who were undergoing elective shoulder arthroscopy surgery were included in the study. Patients who did not give consent for the procedure, patients who had a Body Mass İndex (BMI) of <20 or >50 mg/kg2, patients with neurological or psychiatric disease, pulmonary disease, coagulopathy, drug allergy, and patients who could not undergo VAS assessment in terms of mental capacity were excluded from the study. All the patients were informed about the study before surgery, and their written consent was obtained. The patients were randomly divided into three groups: Group I in which ISB was performed and patient-controlled analgesia (PCA) was inserted, Group II with ISB and SSNB combined and PCA inserted, and Group III (control group) where; only PCA was used (Figure 1).
Figure 1.

Flow chart of the patients studied.
Patients were taken to the block room 30 minutes prior to surgery. Routine electrocardiography (ECG), non-invasive blood pressure measurement, and pulse oximetry monitoring were performed. In Group I, the patients to receive ISB were positioned supine, with their heads turned to the opposite side of the surgical area. One milligram of midazolam and 50 microgram (μg) fentanyl were administered intravenously with 0.9% NaCl 10 mg/kg. Sterile conditions were created by cleaning the skin. An ultrasound device (MyLabTM30, Esaote, Genoa, Italy) (USG) was localized at the level of the cricoid cartilage with a linear 18 MHz transducer. Skin anesthesia was provided with 2% Lidocaine when appropriate localization was achieved. C5-6 nerve roots were identified between the anterior and the middle scalene muscles. A 22-gauge 80-millimeter (mm) needle (Braun, Stimuplex Ultra 360, Germany) was advanced in plane to the C5-6 nerve roots or the upper truncus of the brachial plexus (Figure 2). The motor response was sought by setting 1.5 mAmp, 0.1 ms, and 2 Hz, while the patient was monitored with a nerve stimulator (Stimuplex S, B, Braun, Melsungen AG, Germany). If the appropriate motor response persisted in the range of 0.3–0.5 mAmp, 15 mL of 0.5% bupivacaine and 5 mL of 0.9% NaCl, was injected after negative aspiration. If paresthesia, pain, and pressure increase developed during the injection, the injection site was changed.
Figure 2.
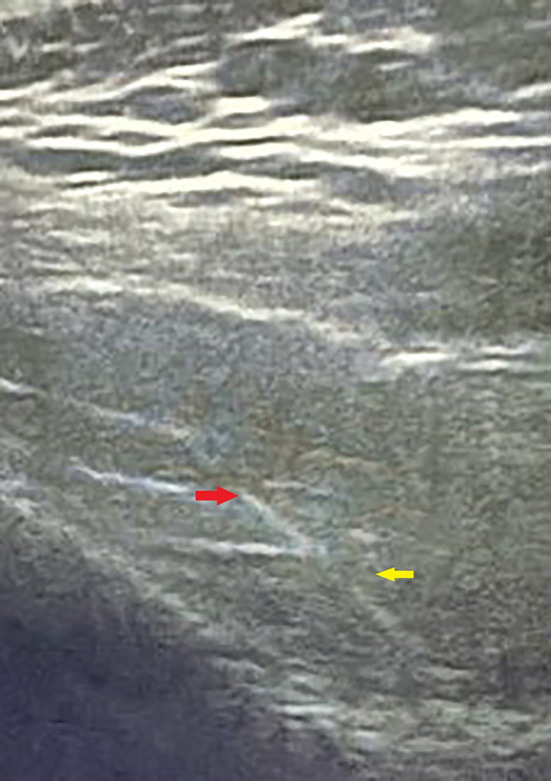
Ultrasound view of Interscalene block. (Needle (red arrow), Brachial plexus (yellow arrow).
In Group II, first ISB and then SSNB block were performed. The local dose was prepared as 15 mL of 0.5% bupivacaine and 5 mL of 0.9% NaCl. Half of this prepared solution was administered to patients who underwent ISB. Then, SSNB block was performed in a sitting position via USG and a nerve stimulator. The SSNB in-plane technique detected the scapular notch with a posterolateral approach, and the suprascapular artery was found. The suprascapular nerve was localized next to the artery, and the remaining 10 mL of local anesthesia solution was injected after negative aspiration by entering from the medial side of the probe (Figure 3). No block operations were applied to Group III.
Figure 3.
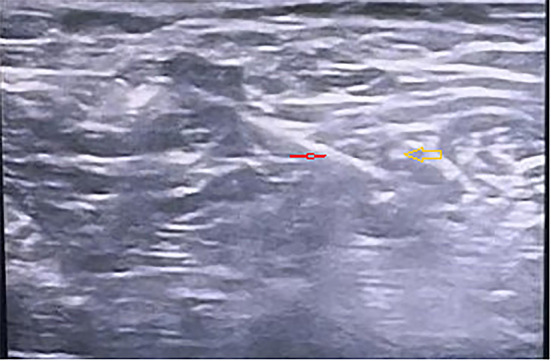
Ultrasound view of Suprascapular nerve block. (Needle (red arrow), Suprascapular Nerve (yellow arrow).
After the procedure was performed in the block room, the patients were kept under observation by anesthetists until they were taken to the operating room. The sensory block was reevaluated 30 minutes after the block was applied; it was considered an unsuccessful block in cases of insufficiency. Desaturation or other complications were noted during this period. After the block evaluation, the patients were taken to the operating room 30 minutes later, and general anesthesia was administered to the patients. In general anesthesia, muscle relaxation was achieved with 2.5 milligrams/kilogram (mg/kg) propofol, 1 μg/kg fentanyl, and 0.6 mg/kg rocuronium before intubation. 1–3% Sevoflurane and 50%/50% oxygen/air were used for anesthesia maintenance. Bispectral Index (BIS) was kept between 40 and 60. Infusion of 0.1 μg/kg Remifentanil and 0.9% NaCl (5–10 mL/kg) was continued throughout the surgery. Arthroscopy operations were performed with the same team and the same surgical method.
At the end of the surgery, patients were given 40 μg/kg neostigmine and 20 μg/kg atropine for antagonizing muscle relaxants. Patients with good muscle strength were transferred to the recovery unit. All patients were given 1 mg bolus dose of morphine at each press, and the PCA device (WYM PCA pump, Anesmed Medical, Korea) was adjusted intravenously (iv) with a 10-minute lock-in time and a 4-hour limit of 30 mg. Pain status during movement or rest was questioned with verbal number score (0: no pain, 10: severe pain, VAS). Patients with VAS 4 and above were given 0.1 mg/kg of IV bolus morphine. One anesthesiologist who was blinded to this study checked the postoperative VAS using a questionnaire and morphine consumption. If the VAS score was 4 and above despite morphine administration, 1000 milligrams of paracetamol (mgr) was administered as additional analgesia. Ondansetron IV was administered to patients with nausea and vomiting as an antiemetic. Patients with an Aldrete recovery score of ≥9 were sent to the orthopedic service.13 VAS pain scores at the 2nd, 4th, 6th, 12th, and 24th hours, morphine consumption, additional analgesic requirement and patient satisfaction (1 = very bad, 2 = poor, 3 = good; 4 = very good, 5 = excellent) were evaluated.
Demographic data, age, gender, ASA score, spO2, HR, MAP, duration of surgery, 24-hour morphine consumption, use of antiemetics and additional analgesics, VAS score and patient satisfaction score, length of hospital stay, nausea-vomiting and complications related to block were recorded.
Statistical Analysis
Data were evaluated with the statistical package program IBM SPSS Statistics for Windows, v.21 (IBM Corp., Armonk, New York, USA). The normal distribution of numerical data was examined with Shapiro–Wilk and histogram tests. One-way Anova test was used to evaluate normally distributed weight data. Since there was no difference between the groups, Post hoc Tukey was not used. Numerical data that did not show normal distribution were evaluated with Kruskal–Wallis test. If there was a difference between the groups, a comparison was made with the Post-Hoc Pairwise Comparison Test. Chi-square exact test was used to examine categorical data (e.g, ASA and sex results). If it was significant, the comparison of the groups was performed with the Pairwise Comparison test. Data were expressed as arithmetic mean±standard deviation, median or interquartile range. A p-value of <0.05 was considered significant.
Preliminary studies of 10 cases were performed to determine the sample size. In addition, average 24-hour morphine consumption was measured. Since α, β and average difference values were calculated as 0.05, 0.20, and 7.18, respectively, 14.2±7 (Group I), 7.02±4.2 (Group II), and 45.9±8.06 (Group III)) for ten patients in each group regarding the total morphine consumption, a minimum of 25 patients were calculated as necessary for each group.
Results
The study was completed with 90 patients, with 30 patients in each group. The flow chart is given in Figure 1.
When the patients were compared according to demographic characteristics, there was no statistical difference regarding age, weight, ASA status and Body Mass Index (BMI). The surgical duration was longer in Group III. The hospital stay was shorter in Group I and Group II, and there was a statistically significant difference compared to Group III (p < 0.001) (Table 1).
Table 1.
Patient Characteristics
| Group I (n=30) | Group II (n=30) | Group III (n=30) | p Value | |
|---|---|---|---|---|
| Age, y | 49.3 (14) | 54.5 (12.2) | 53.4 (12.4) | 0.269* |
| Sex (M/F) (n) | 12/18 | 12/18 | 13/17 | 0.955 |
| Weight, kg | 77.2±9.8 | 77.7±15.1 | 79.7±12.0 | 0.722 |
| ASA physical status (I/II/III) (n) | 4/20/6 | 7/21/2 | 4/21/5 | 0.520 |
| Surgical Duration, min | 96 (30) | 120 (76) | 120 (19) ab | 0.004* |
| Hospitalization time, h | 24 (12) | 24 (24) | 36 (9)a b | 0.003* |
Notes: Group I, Interscalene Block; Group II, Interscalene Block and Suprascapular Nerve Block; Group III, Control Group. Results are presented as medians and interquartile range in brackets. *Results were evaluated with Kruskal–Wallis and compared with Post-hoc pairwise comparison test. Chi-square Exact Test is used in sex and ASA, One-Way Anova test is used in weight. p < 0.001, significant difference; ap < 0.001 when compared with Group I; bp < 0.001 when compared with Group II.
The patients’ pain scores at rest were evaluated with VAS (Table 2). Accordingly, at the 2nd, 4th, 6th, 12th, and 24th hours, the resting pain score of the control group was higher than that of Groups I and II. In Group I, the VAS score at rest at the 6th hour was found to be higher than in Group II. The 24-hour total morphine consumption was higher in the control group than in Group I and Group II (Table 3).
Table 2.
VAS at Rest
| Group I (n=30) | Group II (n=30) | Group III (n=30) | p Value | |
|---|---|---|---|---|
| VAS at rest | ||||
| 2. hour | 3 (4) | 0 (2) | 4 (4) a b | <0.001 |
| 4. hour | 3 (3) | 1 (2) | 4 (2) b c | <0.001 |
| 6. hour | 3 (3) | 1 (2)d | 4 (1) b e | <0.001 |
| 12. hour | 2.5 (3) | 1 (1) | 3.5 (1) b c | <0.001 |
| 24. hour | 3 (3) | 2 (2) | 3 (1) f | p=0.001 |
Notes: Group I, Interscalene Block; Group II, Interscalene Block and Suprascapular Nerve Block; Group III, Control Group. Data are presented as medians and interquartile range in brackets, Results were evaluated with Kruskal–Wallis and compared with Post-hoc pairwise comparison test. Post hoc analysis values are indicated as a, b, c, d, e, f. ap =0.001 when compared with Group I. bp < 0.001 when compared with Group II. cp =0.002 when compared with Group I. dp =0.034 when compared with Group I. ep =0.007 when compared with Group I. fp =0.001 when compared with Group II.
Table 3.
Morphine Consumption
| Group I (n=30) | Group II (n=30) | Group III (n=30) | p Value | |
|---|---|---|---|---|
| Morphine consumption (mg) | ||||
| 0–2 hour | 1.5 (2.25) | 0 (2) | 7 (0)a b | <0.001 |
| 2–4 hour | 1 (2) | 0 (1.1) | 6 (3)a b | <0.001 |
| 4–6 hour | 2 (3.6) | 1 (2) | 6.5 (3.2)a b | <0.001 |
| 6–12 hour | 3 (6.5) | 2 (4) | 9.5 (13.2)a b | <0.001 |
| 12–24 | 2 (6.2) | 1.5 (5.1) | 12 (12.2)a b | <0.001 |
| Overall | 12 (17.3) | 7.5 (7.8) | 40 (30)a b | <0.001 |
Notes: Group I, Interscalene Block; Group II, Interscalene Block and Suprascapular Nerve Block; Group III, Control group. Data are presented as medians and interquartile range in brackets. Results were evaluated with Kruskal–Wallis and compared with Post-hoc pairwise comparison test. ap < 0.001 when compared with Group I. bp < 0.001 when compared with Group II.
When we evaluated the patients regarding patient satisfaction score, the satisfaction score of the control group was lower than Group I and Group II (Table 4).
Table 4.
Patient Satisfaction
| Group I (n=30) | Group II (n=30) | Group III (n=30) | p Value | |
|---|---|---|---|---|
| Patient Satisfaction | ||||
| 0–2 hour | 4.5 (1) | 5 (1) | 3 (2)a b | <0.001 |
| 2–4 hour | 4.5 (1) | 5 (1) | 3 (2)a b | <0.001 |
| 4–6 hour | 4 (1) | 5 (1) | 3 (2)a b | <0.001 |
| 6–12 hour | 4 (1) | 5 (1) | 3 (2)a b | <0.001 |
| 12–24 hour | 4 (1) | 4.5 (3) | 4 (2)c d | p=0.001 |
Notes: Group I, Interscalene Block; Group II, Interscalene Block and Suprascapular Nerve Block, Group III, Non-Block Group. Datas are presented as medians and interquartile range in brackets. Results were evaluated with Kruskal–Wallis and compared with Post-hoc pairwise comparison test. ap < 0.001 when compared with Group I. bp < 0.001 when compared with Group II. cp=0.004, compared with Group I and Group III. dp= 0.003, compared with Group II and Group III.
Additional analgesia was applied to the patients in the control group at the 2nd hour, but the other groups did not need additional analgesics at the 2nd hour. When compared in terms of side effects of the blocks applied, clinically symptomatic phrenic nerve involvement occurred in three patient in Group I. Hypotension developed during the surgical position in one patient each in Groups I and II. In one of the patients in Group I, a Bezold-Jarisch reflex was observed during the chaise lounge position, profound bradycardia was observed before surgery, and the patient was given atropine. There was no difference between the groups regarding antiemetic use.
Discussion
In this randomized study, the duration of analgesia and the comfort of the block were compared in shoulder arthroscopy patients who did not undergo block or patients who had ISB in one group and ISB and SSNB together in another group under the guidance of USG. We concluded that the complication development rate was low, analgesic consumption was very low, and patient satisfaction was relatively high in the ISB-SSNB combination group.
Patients experience severe pain in the postoperative period of shoulder arthroscopy. Regional nerve block combined with general anesthesia reduces the need for anesthesia in the intraoperative period, and rapid and high-quality recovery is achieved by reducing postoperative pain.2 ISB and SSNB are very effective methods in postoperative pain control.14,15 Although many studies have compared these two blocks, studies to prolong the duration of analgesia are still ongoing.1,14–18
The systematic review and meta-analysis of Hussain et al examined the studies comparing the effects of ISB and SSNB on postoperative pain.15 The results showed no difference between the groups regarding opioid-related side effects, analgesic duration, analgesic consumption in PACU and surgical comfort. Cho et al compared posterior suprascapular nerve block with placebo in their meta-analysis consisting of ten studies.19 They reported that 24-hour analgesia duration and opioid consumption were not different between the placebo and the block groups. Therefore, it is argued that the analgesic effect of ISB can be compared only if the posterior suprascapular block is supported by complementary blocks such as supraclavicular and infraclavicular blocks.19
In a study conducted in arthroscopic surgeries, much better analgesia was provided in the combination of SSNB and axillary block compared to patients who had SSNB block alone for the 12 hour period.20 Lee et al examined patients who were to undergo rotator muscle repair in two groups. They applied only ISB block to one group, first ISB, and then SSNB block to the other group arthroscopically. In the combined block, the severity of pain was decreased.21 Our study provided adequate analgesia in Group I and Group II within 24 hours.
Koga et al compared suprascapular nerve block and interscalene block in arthroscopic rotator cuff repair. According to this study, there was no difference in analgesic consumption between the two methods.18 Although ISB and SSNB are effective methods in providing analgesia, postoperative pain score and morphine consumption were lower in the ISB block group. In our study, total morphine consumption for 24 hours was 70% lower in the ISB group than the control group and 81% lower in the ISB and SSNB groups. Group II was the group with the lowest VAS score for 24 hours. The addition of additive or synergistic adjuvant blocks (two or more) to regional anesthesia for postoperative analgesia reduces pain with different mechanisms and reduces the need for postoperative analgesia. It was shown that the success rate increases by 87–100% with the addition of the supraclavicular block to the ISB.2 In arthroscopic surgery, the suprascapular nerve block or axillary block, which are applied together, is less effective than the interscalene block. The primary aim of these blocks is to provide capsular innervation of the shoulder, and phrenic nerve paralysis is very rare in these blocks.9
Diaphragmatic paralysis resulting from phrenic nerve paralysis can be temporary or persistent. Clinically, respiratory failure symptoms due to diaphragmatic paralysis can range from asymptomatic to requiring respiratory support.22 In our study, phrenic nerve palsy was developed in three patients in the interscalene block group. In a patient with a BMI of 41 mg/kg2, oxygen saturation fell below 80%. The patient was excluded from the study, intubated and followed in the intensive care unit. In the other two patients, the diagnosis of paralysis was made with the help of USG, but since they were asymptomatic and included in the study. Their operations were completed, and there was no problem in the postoperative follow-ups. Hussain et al stated that respiratory complications of ISB and undesirable conditions related to block might occur. However, they also reported that if there is no underlying respiratory disease, respiratory dysfunction caused by ISB block will be subclinical.15 In another study, a patient with chronic renal failure who was to undergo A-v fistula surgery, 30 mL of local anesthetic administered during an interscalene block. After the block, the patient’s oxygen saturation dropped below 85% due to the resulting paralysis.23
Phrenic nerve paralysis occurring in interscalene blocks is frequently seen at doses of 20 mL or higher of local anesthetic used. Paralysis can be prevented by reducing the volume and concentration of local anesthetic, changing the injection site or technique for interscalene block, or combining interscalene block with other regional techniques.6,22 Lee et al reported that reducing the volume to 10 mL in blocks performed with ultrasound guidance may decrease the risk of phrenic nerve paralysis by 60%.11 Stunder et al stated that when reducing the dose from 20 to 5 mL may decrease the risk of phrenic nerve paralysis by 27–45% and that it does not affect 24-hour post-operative analgesia.24 It has been reported that reducing the concentration of bupivacaine from 0.5% to 0.25% may decrease the risk of phrenic nerve paralysis from 100% to 17%. But it will also reduce the analgesic effect by the same amount and increase opioid consumption by 50%.20 In our study, we tried to prevent the complication of phrenic nerve palsy by reducing the dose of local anesthesia in ISB-SSNB combination group was applied. As a matter of fact, this complication was not observed in Group II, and no decrease in analgesic effectiveness and opioid consumption was observed. In randomized controlled studies, patients with pulmonary disease, obesity, and obstructive sleep apnea have been excluded from interscalene block studies in the literatüre. In addition to the analgesic efficacy of the suprascapular block, it can be preferred as a good alternative method in shoulder surgery in patients with pre-existing respiratory disease or other comorbidities (eg, obesity).6
One of the patients in Group I developed a Bezold-Jarisch reflex during the chaise-lounge position before starting the surgery, and profound bradycardia occurred. Atropine was administered, and an immediate response was achieved; the procedure was continued.
This study has some limitations. Since the patients were discharged early, the postoperative analgesia evaluation period was limited to 24 hours. Patients could not be evaluated in the long term to better understand to develop strategies for opioid consumption and prevention.
Conclusion
In this randomized prospective study, adequate intraoperative analgesia was provided since the combination of ISB and SSNB was applied preemptively in both blocks in shoulder arthroscopic surgery. It was found that the pain intensity was lower, and the opioid dose needed was lower in patients who underwent a combination of blocks. In addition to these, the dose of local anesthesia used with the combination of blocks was reduced, thus reducing the potential respiratory complications.
Funding Statement
There are no funders to report for this article.
Data Sharing Statement
The data will be available on request from the corresponding author.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Lee SM, Park SE, Nam YS, et al. Analgesic effectiveness of nerve block in shoulder arthroscopy: comparison between interscalene, suprascapular and axillary nerve blocks knee surg sports. Traumatol Arthrosc. 2012;20(12):2573–2578. doi: 10.1007/s00167-016-4198-7 [DOI] [PubMed] [Google Scholar]
- 2.C B Jr, Sripada R. Regional blockade of the shoulder: approaches and outcomes. Anesthesiol Res Pract. 2012;2012:971963. doi: 10.1155/2012/971963 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Abdallah FW, Halpern SH, Aoyama K, Brull R. Will the real benefits of single-shot interscalene block please stand up? A systematic review and meta-analysis. Anesthesia Analg. 2015;120(5):1114–1129. doi: 10.1213/ANE.0000000000000688 [DOI] [PubMed] [Google Scholar]
- 4.Nisar A, Morris MW, Freeman JV, et al. Subacromial bursa block is an effective alternative to interscalene block for postoperative pain control after arthroscopic subacromial decompression: a randomized trial. J Shoulder Elbow Surg. 2008;17(1):78–84. doi: 10.1016/j.jse.2007.05.014 [DOI] [PubMed] [Google Scholar]
- 5.Kim JH, Koh HJ, Kim DK, et al. Interscalene brachial plexus bolus block versus patient-controlled interscalene indwelling catheter analgesia for the first 48 hours after arthroscopic rotator cuff repair. J Shoulder Elbow Surg. 2018;27(7):1243–1250. doi: 10.1016/j.jse.2018.02.048 [DOI] [PubMed] [Google Scholar]
- 6.El-Boghdadly K, Chin KJ, Chan VWS. Phrenic nerve palsy and regional anesthesia for shoulder surgery: anatomical, physiologic, and clinical considerations. Anesthesiology. 2017;127(1):173–191. doi: 10.1097/ALN.0000000000001668 [DOI] [PubMed] [Google Scholar]
- 7.Boon AJ, Sekiguchi H, Harper CJ, et al. Sensitivity and specificity of diagnostic ultrasound in the diagnosis of phrenic neuropathy. Neurology. 2014;83(14):1264–1270. doi: 10.1212/WNL.0000000000000841 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chan CW, Peng PW. Suprascapular nerve block: a narrative review. Reg Anesth Pain Med. 2011;36(4):358–373. doi: 10.1097/AAP.0b013e3182204ec0 [DOI] [PubMed] [Google Scholar]
- 9.Fernandes MR, Barbosa MA, Sousa AL, Ramos GC. Suprascapular nerve block: important procedure in clinical practice. Braz J Anesthesiol. 2012;62(1):96–104. doi: 10.1016/S0034-7094(12)70108-3 [DOI] [PubMed] [Google Scholar]
- 10.Sinha SK, Abrams JH, Barnett JT, et al. Decreasing the local anesthetic volume from 20 to 10 mL for ultrasound-guided interscalene block at the cricoid level does not reduce the incidence of hemidiaphragmatic paresis. Reg Anesth Pain Med. 2011;36(1):17–20. doi: 10.1097/aap.0b013e3182030648 [DOI] [PubMed] [Google Scholar]
- 11.Lee JH, Cho SH, Kim SH, et al. Ropivacaine for ultrasound-guided interscalene block: 5 mL provides similar analgesia but less phrenic nerve paralysis than 10 mL. Can J Anaesth. 2011;58(11):1001–1006. doi: 10.1007/s12630-011-9568-5 [DOI] [PubMed] [Google Scholar]
- 12.Toma O, Persoons B, Pogatzki-Zahn E, Van de Velde M, Joshi GP; PROSPECT Working Group collaborators. PROSPECT guideline for rotator cuff repair surgery: systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2019;74(10):1320–1331. doi: 10.1111/anae.14796 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aldrete JA, Vazeery A. Is magnesium sulfate an anesthetic? Anesthesia Analg. 1989;68(2):186–187. doi: 10.1213/00000539-198902000-00024 [DOI] [PubMed] [Google Scholar]
- 14.Desroches A, Klouche S, Schlur C, et al. Suprascapular nerve block versus interscalene block as analgesia after arthroscopic rotator cuff repair: a randomized controlled noninferiority trial. Arthroscopy. 2016;32(11):2203–2209. doi: 10.1016/j.arthro.2016.03.013 [DOI] [PubMed] [Google Scholar]
- 15.Hussain N, Goldar G, Ragina N, et al. Suprascapular and interscalene nerve block for shoulder surgery: a systematic review and meta-analysis. Anesthesiology. 2017;127(6):998–1013. doi: 10.1097/ALN.0000000000001894 [DOI] [PubMed] [Google Scholar]
- 16.Aliste J, Bravo D, Fernández D, et al. A randomized comparison between interscalene and small-volume supraclavicular blocks for arthroscopic shoulder surgery. Reg Anesth Pain Med. 2018;43(6):590–595. doi: 10.1097/AAP.0000000000000767 [DOI] [PubMed] [Google Scholar]
- 17.Singelyn FJ, Lhotel L, Fabre B. Pain relief after arthroscopic shoulder surgery: a comparison of intraarticular analgesia, suprascapular nerve block, and interscalene brachial plexus block. Anesthesia Analg. 2004;99(2):589–592. doi: 10.1213/01.ANE.0000125112.83117.49 [DOI] [PubMed] [Google Scholar]
- 18.Koga R, Funakoshi T, Yamamoto Y, Kusano H. Suprascapular nerve block versus interscalene block for analgesia after arthroscopic rotator cuff repair. J Orthop. 2020;19:28–30. doi: 10.1016/j.jor.2019.11.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cho N, Kang RS, McCartney CJL, et al. Analgesic benefits and clinical role of the posterior suprascapular nerve block in shoulder surgery: a systematic review, meta-analysis and trial sequential analysis. Anaesthesia. 2020;75(3):386–394. doi: 10.1111/anae.14858 [DOI] [PubMed] [Google Scholar]
- 20.Wilson-Poe AR, Morón JA. The dynamic interaction between pain and opioid misuse. Br J Pharmacol. 2018;175(14):2770–2777. doi: 10.1111/bph.13873 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lee JJ, Hwang JT, Kim DY, et al. Effects of arthroscopy‑guided suprascapular nerve block combined with ultrasound‑guided interscalene brachial plexus block for arthroscopic rotator cuff repair: a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc. 2017;25(7):2121–2128. doi: 10.1007/s00167-016-4198-7 [DOI] [PubMed] [Google Scholar]
- 22.Riazi S, Carmichael N, Awad I, Holtby RM, McCartney CJ. Effect of local anaesthetic volume (20 vs 5 mL) on the efficacy and respiratory consequences of ultrasound-guided interscalene brachial plexus block. Br J Anaesth. 2008;101(4):549–556. doi: 10.1093/bja/aen229 [DOI] [PubMed] [Google Scholar]
- 23.Altintas F, Gumus F, Kaya G, et al. Interscalene brachial plexus block with bupivacaine and ropivacaine in patients with chronic renal failure: diaphragmatic excursion and pulmonary function changes. Anesth Analg. 2005;100(4):1166–1171. doi: 10.1213/01.ANE.0000154443.68396.70 [DOI] [PubMed] [Google Scholar]
- 24.Stundner O, Meissnitzer M, Brummett CM, et al. Comparison of tissue distribution, phrenic nerve involvement, and epidural spread in standard- vs low-volume ultrasound-guided interscalene plexus block using contrast magnetic resonance imaging: a randomized, controlled trial. Br J Anaesth. 2016;116(3):405–412. doi: 10.1093/bja/aev550 [DOI] [PubMed] [Google Scholar]