

Abstract
AIM
To describe the clinical, electrophysiological, and genetic features of an unusual case with an RDH12 homozygous pathogenic variant and reviewed the characteristics of the patients reported with the same variant.
METHODS
The patient underwent a complete ophthalmologic examination including best-corrected visual acuity, anterior segment and dilated fundus, visual field, spectral-domain optical coherence tomography (OCT) and electroretinogram (ERG). The retinal disease panel genes were sequenced through chip capture high-throughput sequencing and Sanger sequencing was used to confirm the result. Then we reviewed the characteristics of the patients reported with the same variant.
RESULTS
A 30-year male presented with severe early retinal degeneration who complained night blindness, decreased visual acuity, vitreous floaters and amaurosis fugax. The best corrected vision was 0.04 OD and 0.12 OS, respectively. The fundus photo and OCT showed bilateral macular atrophy but larger areas of macular atrophy in the left eye. Autofluorescence shows bilateral symmetrical hypo-autofluorescence. ERG revealed that the amplitudes of a- and b-wave were severely decreased. Multifocal ERG showed decreased amplitudes in the local macular area. A homozygous missense variant c.146C>T (chr14:68191267) was found. The clinical characteristics of a total of 13 patients reported with the same pathologic variant varied.
CONCLUSION
An unusual patient with a homozygous pathogenic variant in the c.146C>T of RDH12 which causes late-onset and asymmetric retinal degeneration are reported. The clinical manifestations of the patient with multimodal retinal imaging and functional examinations have enriched our understanding of this disease.
Keywords: RDH12 gene, inherited retinal degeneration, homozygous pathogenic variant, clinical feature, multi-mode imaging
INTRODUCTION
Retinol dehydrogenase 12 (RDH12) is a nicotinamide adenine dinucleotide phosphate hydrogen (NADPH)-dependent retinaldehyde reductase that is specifically expressed in photoreceptor cells and participates in the visual cycle[1]–[2]. In the visual cycle, a series of reactions are involved in the transport mechanisms between the retinal pigment epithelium (RPE) and photoreceptor cells, in which different members of retinol dehydrogenase play important roles[3]–[4]. It has the highest activity with all-trans retinal production. In the presence of nicotinamide adenine dinucleotide phosphate (NADP) or NADPH as a cofactor, RDH12 acts on the inner segments of the cone and rod photoreceptor cells to catalyze the conversion of all-trans retinal into all-trans retinol[5]–[7]. The RDH12 gene consists of 7 exons and encodes a protein with 316 amino acids. Gene variants in RDH12 that interfere with the activity of this protein will cause a disruption of the visual cycle[8], leading to early and progressive retinopathy[9]–[10]. RDH12 variant-related retinal degeneration usually presents early vision loss in infancy or childhood[11]. It is an autosomal recessive progressive retinal degenerative disease characterized by several types of retinopathy including Leber congenital amaurosis (LCA)[12]–[18] or/and early-onset severe retinal dystrophy (EOSRD)[13]–[14],[16]–[17],[19]–[20], autosomal recessive retinitis (RP)[13]–[14],[19],[21]–[22], cone-rod dystrophy (CORD)[13]–[14],[19]–[20],[23] and macular dystrophy[19]–[20], which leads to severe visual impairment or even blindness. Here we reported an unusual patient with predominant macular dystrophy caused by an RDH12 homozygous pathogenic variant [c.146C>T (p.T49M)] and reviewed clinical characteristics of a series of reported cases with the same pathologic variant.
SUBJECTS AND METHODS
Ethical Approval
The Ethics Committee of Shenzhen Eye Hospital approved this study and the approved number is 20210603-11. The informed consent was obtained from the patient.
The patient underwent a complete ophthalmologic examination including best-corrected visual acuity assessment, anterior segment and dilated fundus examination, visual field test, spectral-domain optical coherence tomography and electroretinogram (ERG). We extracted genomic DNA from 2 mL peripheral blood and screened protein coding sequences of targeted retinal disease gene panels by chip capture high-throughput sequencing and confirmed by Sanger sequencing.
DNA Extraction and Targeted Next Generation Sequencing
Genomic DNA (gDNA) was isolated using TIANamp Blood DNA kit (Tiangen, Shanghai, China) from ethylene diamine tetraacetic acid (EDTA) anticoagulated peripheral blood. Targeted next generation sequencing and annotation of variants were proceeded in Shanghai WeHealth Biomedical Technology Co, Ltd. (Shanghai, China). Briefly, genome libraries were constructed using the Hieff NGS OnePot DNA Library Prep Kit (YEASEN, Shanghai, China). Probes were synthesized by Integrated DNA Technologies, Inc. (Iowa, USA) to capture exons of 386 genes related to vitreoretinal diseases. Paired-end sequencing were performed by MGISEQ-T7 (BGI Genomics Co., Ltd., Shenzhen, China) to generate sequencing data of 150× depth. The quality of raw data was checked by FASTQC software. After removing the low-quality reads, the adaptor reads were mapped to the reference genome (GRCh37/hg19) with Burrows-Wheeler Aligner (BWA), Picard, and SAMtools. Genome Analysis Toolkit (GATK) was also used for insertion and deletion realignment, quality recalibration, and variant calling. Detected variants were annotated using ANNOVAR. Variants were filtered with minor allele frequencies, deleterious predictions by bioinformatic tools, gene functions and multiple databases. Then we reviewed the characteristics of the patients reported with the same homozygous variant.
RESULTS
A 30-year-old man came to our hospital for the first time, and he complained that he had night blindness since he was a child, and his vision began to decline at the age of 13, and worsen in recent 3y. He also had obvious vitreous floaters in the past 6y and occasionally metamorphopsia in the past 4y. Recently, he experienced transient vision loss in the last 4mo and both eyes suddenly darkens with dizziness. He has a family history of intermarriage that his grandfather and grandmother were siblings. The standard logarithm visual acuity chart was used to measure the visual acuity. The best corrected vision in his left and right eye was 0.04 and 0.12, respectively. The fundus photo showed bilateral macular atrophy, but larger areas of macular atrophy in the left eye. Punctate pigmentation was found at the posterior pole in the right eye, whereas few pigments around macula in the left eye. Autofluorescence showed roughly symmetrical hypofluorescence, especially in the macular area, the nasal side of the optic disc, the horizontal line between the optic disc and the macula, but in the temporal side of the optic disc it showed a crescent-shaped hyperfluorescence area. The peripheral retina is scattered with small patches of hypofluorescence, and streak-like hyperfluorescence appears in the border area of hypofluorescence (Figure 1C, 1D). Optical coherence tomography showed obvious macular atrophy, and the central macular thickness was significantly decreased in both eyes, but the severity of macular atrophy was inconsistent. The outer retina of the right eye was obviously thinned, the structure of each layer was blurred, and the RPE layer was atrophied with scattered hyper-reflective foci. The macular area of the left eye showed macular excavation changes, with RPE layer rupture and the outer retina was markedly thinned. But relatively normal retinal structures were preserved in some areas between optic nerve head and macula (Figure 2). ERG revealed that the amplitudes of a- and b-wave were extinguished during photopic and scotopic conditions. Multifocal electroretinogram (mf-ERG) showed decreased amplitudes in the local macular area. Visual evoked potential showed significantly reduced amplitudes and 24-2 visual field tests showed severely central visual field defects in both eyes (Figure 2). Toxoplasma or other microorganisms infection tests were negative. We extracted genomic DNA from 2 mL peripheral blood and screened protein coding sequences of targeted retinal disease gene panels by chip capture high-throughput sequencing and confirmed by Sanger sequencing. A homozygous missense pathologic variant c.146C>T (chr14:68191267) was found, and the corresponding amino acid change was p.Thr49Met (Figure 3). In genomAD (Genome Aggregation Database), the frequency of this allele in all humans is 0.00003286, and it is 0.0003848 in east Asian populations.
Figure 1. The fundus photo showed macular atrophy of both eyes, but the left eye was more pronounced.
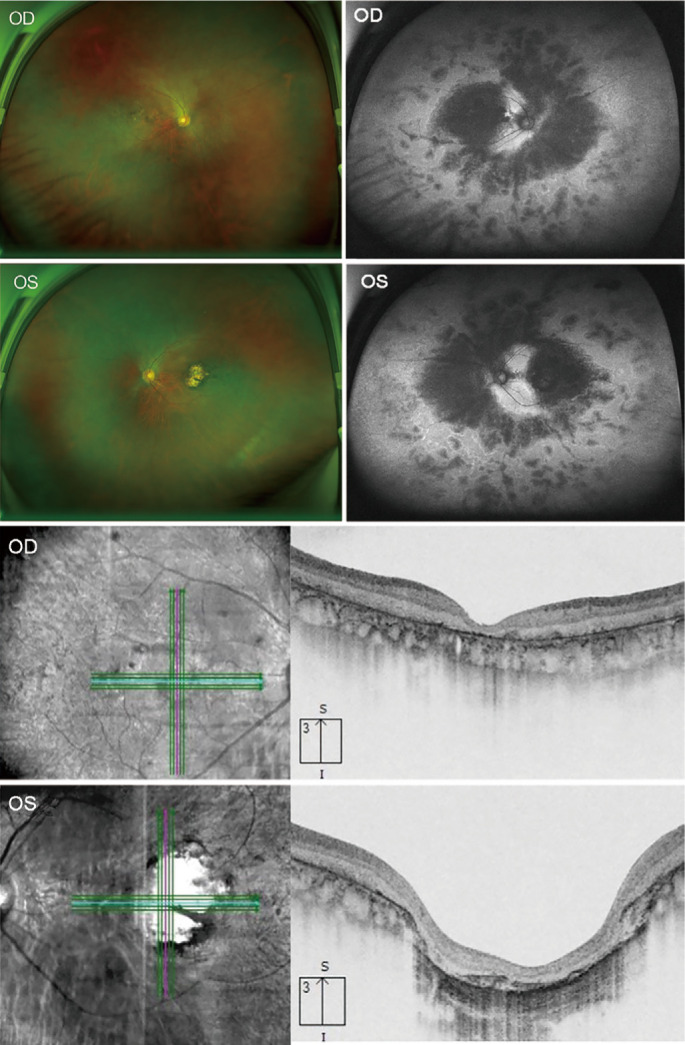
Autofluorescence shows roughly symmetrical hypofluorescence, especially in the macular area, the nasal side of the optic disc, the horizontal line between the optic disc and the macula, but in the temporal side of the optic disc it showed a crescent-shaped hyperfluorescence area. The peripheral retina is scattered with small patches of hypofluorescence, and streak-like hyperfluorescence appears in the border area of hypofluorescence. Optical coherence tomography showed obvious macular atrophy, and the central macular thickness was significantly decreased in both eyes, but the severity of macular atrophy was inconsistent. The outer retina of the right eye was obviously thinned, the structure of each layer was blurred, and the RPE layer was atrophied with scattered hyper-reflective foci. The macular area of the left eye showed macular excavation changes, with RPE layer rupture and the outer retina was markedly thinned. But relatively normal retinal structures were preserved in some areas between optic nerve head and macula. RPE: Retinal pigment epithelium.
Figure 2. Visual functional changes in the patient.

Electroretinogram (ERG) revealed that the amplitudes of a- and b-wave were extinguished during photopic and scotopic conditions (A); Multifocal electroretinogram (mf-ERG) showed abnormal changes in the local function of the macular area (B). Visual field showed that the patient only had a very limited central field, and the peripheral field disappeared (C) and visual evoked potential showed significantly reduced amplitudes (D).
Figure 3. A homozygous missense pathologic variant c.146C>T in RDH12 in the patient.

Then we reviewed the articles with the same RDH12 pathogenic variant from PubMed, GeenMedical and Embase and found a total of 3 articles including 12 patients with RDH12 pathologic homozygous variant (c.146C>T) (Table 1). Based on these data and our case, this study summarizes general information, visual acuity, ERG, fundus phenotypic characteristics, and the diagnosis of the 13 patients, as shown in Table 1. We concluded that 6 patients were female, 6 patients were male, and 1 patients had unrecorded gender. The age distribution ranged from 4 to 30 years old, and all had visual impairment. Among them, 5 patients had best corrected visual acuity equal to or less than 0.05 (convert to new national standard visual acuity chart) in one or both eyes. But in two patients, the vision acuity was not available. The onset age of disease was recorded in 6 patients, most of whom were younger than 10 years of age, and whose initial symptoms included night blindness, visual impairment, and poor school performance. The ocular examination included fundus photography and ERG. The ERG showed decreased amplitudes in 6 patients, and extinguished waveform in the remaining 7 patients[1],[23]–[25]. However, the age of onset and clinical manifestations of these patients were different, and the decline in visual acuity varied, and the pathological morphological changes of their posterior retina and macular area were also different. Among the other 12 patients, 7 patients had fundus examination records, including one with typical RP and five with bilateral coloboma-like atrophic macular chorioretinal scars and scattered areas of RPE hyperplasia. Although there are the same variants among the patients, there are different clinical diagnoses, including CORD (6/13), LCA (5/13) and autosomal recessive RP (1/13), and our patient was diagnosed with late-onset retinal degeneration. In patients with same family (No. 2-7 in one family; No. 8-12 in one family), they have the same retinal phenotypes.
Table 1. Clinical features of RDH12-induced retinal degeneration caused by the mutation of 146C>T (p.T49M) from the published literatures.
| Patient No. | Age (y) | Onset age (y) | Gender | Visual acuity | ERG | Fundus | Diagnosis | Author&year |
| 1 | 28 | 3 | NA | OD:0.15 OS: 0.10 | Extinguished | Typical RP | RP | Valverde, 2009 |
| 2 | 13 | NA | F | 0.1 | Diminished | NA | CORD | Beryozkin, 2014 |
| 3 | 12 | NA | F | NA | Diminished | NA | CORD | Beryozkin, 2014 |
| 4 | 11 | NA | F | 0.05 | Diminished | NA | CORD | Beryozkin, 2014 |
| 5 | 9 | NA | F | 0.1 | Diminished | NA | CORD | Beryozkin, 2014 |
| 6 | 7 | NA | M | 0.05 | Diminished | NA | CORD | Beryozkin, 2014 |
| 7 | 4 | NA | F | NA | Diminished | NA | CORD | Beryozkin, 2014 |
| 8 | 22 | 10 | M | OD: 0.1, OS:0.1 | Extinguished | Bilateral coloboma-like atrophic macular chorioretinal scars with RPE hyperplasia | LCA | Yücel-Yılmaz, 2014 |
| 9 | 20 | 8 | M | OD: 0.05, OS: 0.05 | Extinguished | Bilateral coloboma-like atrophic macular chorioretinal scars with RPE hyperplasia | LCA | Yücel-Yılmaz, 2014 |
| 10 | 18 | 6 | M | OD: 0.1, OS: 0.5 | Extinguished | Bilateral coloboma-like atrophic macular chorioretinal scars with RPE hyperplasia | LCA | Yücel-Yılmaz, 2014 |
| 11 | 11 | 5 | F | OD: 0.1, OS: 0.5 | Extinguished | Bilateral coloboma-like atrophic macular chorioretinal scars with RPE hyperplasia | LCA | Yücel-Yılmaz, 2014 |
| 12 | 5 | 2 | M | OD:HM, OS: 0.32 | Extinguished | Bilateral coloboma-like atrophic macular chorioretinal scars with RPE hyperplasia | LCA | Yücel-Yılmaz, 2014 |
| 13 | 30 | NA | M | OD: 0.04, OS: 0.12 | Extinguished | Details in Results | Late onset RD | Current study |
Patient No.8-12 used the logMAR vision chart (already converted), and the visual acuity chart used for the remaining patients was not mentioned in the original articles. M: Male; F: Female; OD: Right eye; OS: Left eye; NA: Not available; RPE: Retinal pigment epithelium; RP: Retinitis pigmentosa; LCA: Leber's congenital amaurosis; CORD: Cone-rod dystrophy; ERG: Electroretinogram; RD: Late-onset and asymmetric retinal degeneration; HM: Hand motion.
DISCUSSION
Genetic testing is usually used to identify the potential cause of congeneital eye diseases[26]. RDH12-related retinopathy should also be confirmed by genetic testing. It is characterized by severely impaired visual function in early life, which begins in 2 to 4y. The vision gradually deteriorated and most patients had significant vision loss before the age of 30[25]. The most severe condition may be obvious visual impairment in the first six months of life[13]. There are different clinical diagnoses in the reported cases with RDH12 pathologic variants, including EOSRD/LCA, CORD, RP, and macular dystrophy. In RDH12-related retinopathy, there are four types of pathological retinal morphological changes, including macular coloboma (mostly petal-like) with dense bone spicule pigmentation in the mid-peripheral retina, macular discoloration and wide-spread bone spicule and/or salt-pepper pigmentation, heavy and confluent pigment proliferation in the mid-peripheral region involving the macular region, and retinal posterior pole atrophy with a relatively normal peripheral retina[14]. In our patient, macular dystrophy was found similar to the reported cases, but the it is still different from the four retinal phenotypes. Specifically, macular atrophy with sparse pigmentation was found in both eyes but without dense bone spicule pigmentation. The diameter of the retinal arteries and veins on the nasal side of both eyes is significantly thinner, but there was no obvious abnormality in the mid-peripheral part of the temporal retinal vessels, which is associated with the preservation of crescent-shaped hyperfluorescence in the temporal side from fundus autofluorescence (FAF) images. Peripapillary sparing was also found in the patient, which was also reported in another case[27]. The pattern of macular dystrophy between two eyes are not consistent.
In addition, the progression of our patient's visual function also differs from other patients reported with the same variant. In our study, the patient had night blindness since childhood, but his vision declined later until 13 years old. At the age of 18, he gave up the driver's license test since his corrected visual acuity was only 0.5 in both eyes. In the past 20y, the visual acuity has been gradually declining, and his visual acuity is severely reduced now. However, a previous study showed that that RDH12 T49M substitution is related to an overall better visual acuity and milder phenotype[28]. In this study, most patients were younger, and the mean age is 18y, so the severity of retinal degeneration could be relatively milder in these patients. Another study also supported this point of more severe visual acuity decline in older age compared to younger age based on two patients with the homozygous variants[28]. The homozygous variant of 146C>T (p.T49M) seems to be the most frequent homozygous genotypes (24/252) in RDH12[13]. But in another study included 57 patients with RDH12 variants, only two patients have the same homozygous variants[16]. Therefore, it is still unclear if the homozygous variant of 146C>T (p.T49M) is a hot mutation of RDH12. Compared with the clinical symptoms of 18 other reported patients, this patient showed later retinal degeneration than other patients. It is manifested as night blindness from an early age, and a significant decrease in vision occurs during adolescence, and the vision is poorly corrected. After that, it declined slowly for a long time, until it accelerated three years ago. Compared with the reported cases of poor vision since childhood, this has a longer course of disease progression. In this patient, he has a family history of intermarriage between his father and mother. The variant could be due to a geographic isolate. Patients with the same pathogenic variant may show different clinical phenotypes, and the phenotypic differences may be due to different genetic background, gene-environment interaction or possible presence of additional pathogenic variants in different genes. From the Table 1, several patients are from the same family and they had a common genetic background, but they are from different places and the differences in clinical manifestations may be due to geographic isolation.
At present, a suitable animal model of RDH12-related retinal disease is not available, as there are very weak retinal phenotypes in Rdh12 knockout mice. Therefore, there are still huge challenges to develop novel treatment for RDH12-related retinopathy. In the future, RDH12-knockout monkeys should be tried to develop new animal disease model of the disease. It has been reported that adeno-associated virus (AVV)-mediated RDH12 gene replacement therapy has promising results in mice. Human RDH12 cDNA packaged in AAV2/5 vector was delivered to Rdh12 knockout mice by subretinal injection, resulting in correct expression positioning and maintain the structural integrity of the retina. Retinal homogenates from the injected knockout mice showed increased all-trans retinol formation and reduced sensitivity to light damage, but without visual cycle disruption[14]–[15]. This study shows promise for future gene therapy of this disease. In addition, there have been many recent studies on new treatments for retinal damage, such as studies on the protection of the retina by human umbilical cord mesenchymal stem cells modified by the leukemia inhibitory factor, which have provided us with some inspiration for further treatment[29]. A large number of previous studies have shown that the application of international, multi-center, retrospective cohort studies and accurate genetic testing technology will bring new insights into the construction of genotype-phenotype correlation databases and retinal treatments[30]–[31].
In summary, we reported an unusual patient with a homozygous pathogenic variant in the c.146C>T of RDH12 who presents late-onset and asymmetric retinal degeneration. However, among the reported patients, the age of onset, clinical characteristics and the rate of disease progression vary. The clinical manifestations of our patient with a comprehensive ophthalmological examination have increased the overall knowledge of this rare disease.
Footnotes
Authors' contributions: Conceived and designed the experiments: Yan XH; Performed the experiments: Li J, Hu YQ, Wang T, Kuang LH, Huang T and Yan XH; Analyzed the data: Li J, Hu YQ, Cheng HB, Yan XH; Contributed reagents/material/analysis tools: Yan XH, Cheng HB; Wrote the manuscript: Li J, Yan XH; All authors reviewed the manuscript.
Foundations: Supported by Shenzhen Science and Technology Program, Shenzhen, China (No.JCYJ20200109145001814; No.SGDX20211123120001001); the National Natural Science Foundation of China (No.81970790); Sanming Project of Medicine in Shenzhen (No.SZSM202011015).
Conflicts of Interest: Li J, None; Hu YQ, None; Cheng HB, None; Wang T, None; Kuang LH, None; Huang T, None; Yan XH, None.
REFERENCES
- 1.Valverde D, Pereiro I, Vallespín E, Ayuso C, Borrego S, Baiget M. Complexity of phenotype-genotype correlations in Spanish patients with RDH12 mutations. Invest Ophthalmol Vis Sci. 2009;50(3):1065–1068. doi: 10.1167/iovs.08-2083. [DOI] [PubMed] [Google Scholar]
- 2.Lee SA, Belyaeva OV, Popov IK, Kedishvili NY. Overproduction of bioactive retinoic acid in cells expressing disease-associated mutants of retinol dehydrogenase 12. J Biol Chem. 2007;282(49):35621–35628. doi: 10.1074/jbc.M706372200. [DOI] [PubMed] [Google Scholar]
- 3.Mao YM, Lan CJ, Tan QQ, et al. All-trans retinoic acid regulates the expression of MMP-2 and TGF-β2 via RDH5 in retinal pigment epithelium cells. Int J Ophthalmol. 2023;16(6):849–854. doi: 10.18240/ijo.2023.06.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kiser PD, Golczak M, Palczewski K. Chemistry of the retinoid (visual) cycle. Chem Rev. 2014;114(1):194–232. doi: 10.1021/cr400107q. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Perrault I, Hanein S, Gerber S, et al. Retinal dehydrogenase 12 (RDH12) mutations in leber congenital amaurosis. Am J Hum Genet. 2004;75(4):639–646. doi: 10.1086/424889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chen CH, Thompson DA, Koutalos Y. Reduction of all-trans-retinal in vertebrate rod photoreceptors requires the combined action of RDH8 and RDH12. J Biol Chem. 2012;287(29):24662–24670. doi: 10.1074/jbc.M112.354514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Parker RO, Crouch RK. Retinol dehydrogenases (RDHs) in the visual cycle. Exp Eye Res. 2010;91(6):788–792. doi: 10.1016/j.exer.2010.08.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Moradi P, MacKay D, Hunt DM, Moore AT. Focus on molecules: retinol dehydrogenase 12 (RDH12) Exp Eye Res. 2008;87(3):160–161. doi: 10.1016/j.exer.2008.05.013. [DOI] [PubMed] [Google Scholar]
- 9.Haeseleer F, Jang GF, Imanishi Y, et al. Dual-substrate specificity short chain retinol dehydrogenases from the vertebrate retina. J Biol Chem. 2002;277(47):45537–45546. doi: 10.1074/jbc.M208882200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Scott HA, Place EM, Ferenchak K, et al. Expanding the phenotypic spectrum in RDH12-associated retinal disease. Cold Spring Harb Mol Case Stud. 2020;6(1):a004754. doi: 10.1101/mcs.a004754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Aleman TS, Uyhazi KE, Serrano LW, Vasireddy V, Bowman SJ, Ammar MJ, Pearson DJ, Maguire AM, Bennett J. RDH12 mutations cause a severe retinal degeneration with relatively spared rod function. Invest Ophthalmol Vis Sci. 2018;59(12):5225–5236. doi: 10.1167/iovs.18-24708. [DOI] [PubMed] [Google Scholar]
- 12.Yzer S, van den Born LI, Cremers FP, den Hollander AI. Van gen naar ziekte; amaurosis congenita van Leber [From gene to disease; Leber congenital amaurosis (LCA)] Ned Tijdschr Geneeskd. 2005;149(42):2334–2337. [PubMed] [Google Scholar]
- 13.Zou X, Fu Q, Fang S, Li H, Ge ZQ, Yang LZ, Xu MC, Sun ZX, Li HJ, Li YM, Dong FT, Chen R, Sui RF. Phenotypic variability of recessive rdh12-associated retinal dystrophy. Retina. 2019;39(10):2040–2052. doi: 10.1097/IAE.0000000000002242. [DOI] [PubMed] [Google Scholar]
- 14.Sarkar H, Moosajee M. Retinol dehydrogenase 12 (RDH12): role in vision, retinal disease and future perspectives. Exp Eye Res. 2019;188:107793. doi: 10.1016/j.exer.2019.107793. [DOI] [PubMed] [Google Scholar]
- 15.Feathers KL, Jia L, Perera ND, Chen A, Presswalla FK, Khan NW, Fahim AT, Smith AJ, Ali RR, Thompson DA. Development of a gene therapy vector for RDH12-associated retinal dystrophy. Hum Gene Ther. 2019;30(11):1325–1335. doi: 10.1089/hum.2019.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fahim AT, Bouzia Z, Branham KH, et al. Detailed clinical characterisation, unique features and natural history of autosomal recessive RDH12-associated retinal degeneration. Br J Ophthalmol. 2019;103(12):1789–1796. doi: 10.1136/bjophthalmol-2018-313580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kumaran N, Pennesi ME, Yang P, et al. Leber Congenital Amaurosis /Early-Onset Severe Retinal Dystrophy Overview. 2018. updated 2023. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Bean LJH, Gripp KW, Amemiya A, editors. GeneReviews®. Seattle (WA): University of Washington, Seattle; 1993–2023. [PubMed] [Google Scholar]
- 18.Zobor D, Brühwiler B, Zrenner E, Weisschuh N, Kohl S. Genetic and clinical profile of retinopathies due to disease-causing variants in leber congenital amaurosis (LCA)-associated genes in a large German cohort. Int J Mol Sci. 2023;24(10):8915. doi: 10.3390/ijms24108915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wang JW, Wang YW, Li SQ, et al. Clinical and genetic analysis of RDH12-associated retinopathy in 27 Chinese families: a hypomorphic allele leads to cone-rod dystrophy. Invest Ophthalmol Vis Sci. 2022;63(9):24. doi: 10.1167/iovs.63.9.24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Daich Varela M, Michaelides M. RDH12 retinopathy: clinical features, biology, genetics and future directions. Ophthalmic Genet. 2022;43(3):1–6. doi: 10.1080/13816810.2022.2062392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Muthiah MN, Kalitzeos A, Oprych K, Singh N, Georgiou M, Wright GA, Robson AG, Arno G, Khan K, Michaelides M. Novel disease-causing variant in RDH12 presenting with autosomal dominant retinitis pigmentosa. Br J Ophthalmol. 2022;106(9):1274–1281. doi: 10.1136/bjophthalmol-2020-318034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Xiao YS, He WJ, Jiang HC, Tan L, Ma J, Zhang Z. Clinical and whole exome sequencing findings in children from Yunnan Yi minority ethnic group with retinitis pigmentosa: two case reports. J Med Case Rep. 2023;17(1):226. doi: 10.1186/s13256-023-03830-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Beryozkin A, Zelinger L, Bandah-Rozenfeld D, et al. Identification of mutations causing inherited retinal degenerations in the Israeli and Palestinian populations using homozygosity mapping. Invest Ophthalmol Vis Sci. 2014;55(2):1149–1160. doi: 10.1167/iovs.13-13625. [DOI] [PubMed] [Google Scholar]
- 24.Yücel-Yılmaz D, Tarlan B, Kıratlı H, Ozgül RK. Genome-wide homozygosity mapping in families with leber congenital amaurosis identifies mutations in AIPL1 and RDH12 genes. DNA Cell Biol. 2014;33(12):876–883. doi: 10.1089/dna.2014.2554. [DOI] [PubMed] [Google Scholar]
- 25.Janecke AR, Thompson DA, Utermann G, et al. Mutations in RDH12 encoding a photoreceptor cell retinol dehydrogenase cause childhood-onset severe retinal dystrophy. Nat Genet. 2004;36(8):850–854. doi: 10.1038/ng1394. [DOI] [PubMed] [Google Scholar]
- 26.Yan YC, Zhou L, Fan JC. Identification and functional analyses of a novel FOXL2 pathogenic variant causing blepharophimosis, ptosis, and epicanthus inversus syndrome. Int J Ophthalmol. 2023;16(5):680–686. doi: 10.18240/ijo.2023.05.02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Garg A, Lee W, Sengillo JD, Allikmets R, Garg K, Tsang SH. Peripapillary sparing in RDH12-associated Leber congenital amaurosis. Ophthalmic Genet. 2017;38(6):575–579. doi: 10.1080/13816810.2017.1323339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Fahim AT, Thompson DA. Natural history and genotype-phenotype correlations in RDH12-associated retinal degeneration. Adv Exp Med Biol. 2019;1185:209–213. doi: 10.1007/978-3-030-27378-1_34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Chen SN, Xu ZG, Ma YX, Chen S, He GH, Han M, Gao X, Wang JH, Wu B, Wang J. Protective effect of LIF-huMSCs on the retina of diabetic model rats. Int J Ophthalmol. 2021;14(10):1508–1517. doi: 10.18240/ijo.2021.10.06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hao XD, Liu Y, Li BW, Wu W, Zhao XW. Exome sequencing analysis identifies novel homozygous mutation in ABCA4 in a Chinese family with Stargardt disease. Int J Ophthalmol. 2020;13(4):671–676. doi: 10.18240/ijo.2020.04.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hahn LC, Georgiou M, Almushattat H, et al. The natural history of leber congenital amaurosis and cone-rod dystrophy associated with variants in the GUCY2D gene. Ophthalmol Retina. 2022;6(8):711–722. doi: 10.1016/j.oret.2022.03.008. [DOI] [PubMed] [Google Scholar]