

Abstract
Background
Studies investigating the effectiveness of acupuncture therapies in alleviating pain in pelvic inflammatory disease (PID) have gained increasing attention. However, to date, there have been no systematic reviews and meta-analyses providing high-quality evidence regarding the efficacy and safety of acupuncture therapies in this context.
Objective
The objective of this review was to assess the efficacy and safety of acupuncture therapies as complementary or alternative treatments for pain relief in patients with PID.
Method
A comprehensive search was conducted in eight databases from inception to February 20, 2023: PubMed, Embase, Web of Science, the Cochrane Library, China National Knowledge Infrastructure, Wanfang Database, VIP Database, and Chinese Biomedical Literature Database. Randomized controlled trials (RCTs) investigating acupuncture therapies as complementary or additional treatments to routine care were identified. Primary outcomes were pain intensity scores for abdominal or lumbosacral pain. The Cochrane risk of bias criteria was applied to assess the methodological quality of the included trials. The Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) system was used to evaluate the quality of evidence. Data processing was performed using RevMan 5.4.
Result
This systematic review included twelve trials comprising a total of 1,165 patients. Among these, nine trials examined acupuncture therapies as adjunctive therapy, while the remaining three did not. Meta-analyses demonstrated that acupuncture therapies, whether used alone or in combination with routine treatment, exhibited greater efficacy in relieving abdominal pain compared to routine treatment alone immediately after the intervention (MD: -1.32; 95% CI: -1.60 to -1.05; P < 0.00001). The advantage of acupuncture therapies alone persisted for up to one month after the treatment (MD: -1.44; 95% CI: -2.15 to -0.72; P < 0.0001). Additionally, acupuncture therapies combined with routine treatment had a more pronounced effect in relieving lumbosacral pain after the intervention (MD: -1.14; 95% CI: -2.12 to -0.17; P < 0.00001) in patients with PID. The incidence of adverse events did not increase with the addition of acupuncture therapies (OR: 0.56; 95% CI: 0.21 to 1.51; P = 0.25). The findings also indicated that acupuncture therapies, as a complementary treatment, could induce anti-inflammatory cytokines, reduce pro-inflammatory cytokines, alleviate anxiety, and improve the quality of life in patients with PID.
Conclusion
Our findings suggest that acupuncture therapies may effectively reduce pain intensity in the abdomen and lumbosacral region as complementary or alternative treatments, induce anti-inflammatory cytokines, decrease pro-inflammatory cytokines, alleviate anxiety, and enhance the quality of life in patients with PID, without increasing the occurrence of adverse events. However, due to the low quality of the included trials, the conclusion should be interpreted with caution, highlighting the need for further high-quality trials to establish more reliable conclusions.
1. Introduction
Pelvic inflammatory disease (PID) is a condition characterized by inflammation in the upper reproductive tract of females caused by infection, affecting vital structures such as the endometrium, fallopian tubes, ovaries, or pelvic peritoneum [1]. Although international variations in the incidence and prevalence of PID are not well understood [2], a report indicates that approximately 4.4% of sexually experienced women and 10% of women with a previously diagnosed sexually transmitted infection in the United States have received a lifetime diagnosis of PID [3]. The annual healthcare cost for managing this condition exceeds $4 billion, highlighting its significant health burden [2].
The primary symptom of PID is a sudden onset of lower abdominal or pelvic pain in sexually active women [4]. However, these symptoms are often subtle, nonspecific, or asymptomatic, potentially leading to delayed diagnosis and treatment, and contributing to inflammatory complications in the upper genital tract [5]. Although guidelines for treating PID recommend broad-spectrum combination regimens of antimicrobial agents to cover likely pathogens [5], the long-term effectiveness is still suboptimal. Consequently, patients with PID face a higher risk of long-term reproductive complications, including infertility, ectopic pregnancy, recurrent PID, and most commonly, chronic pelvic pain (CPP) [2].
The pelvis contains visceral structures such as the uterus, bowel, and bladder, as well as somatic structures including the skin, muscles, fascia, and bones, which share neural pathways. Consequently, inflammatory complications in the upper reproductive tract of females can lead to hypersensitivity of other pelvic organs, resulting in persistent nociceptive stimuli and noxious somatic stimulation [6]. This complexity adds to the challenges in managing CPP, which is frequently associated with negative cognitive, behavioral, sexual, and emotional consequences, and can lead to comorbid chronic pain and psychiatric disorders [7].
Due to the multifactorial nature of CPP, its treatment requires a multimodal and interdisciplinary approach that includes pharmacotherapy (analgesics, muscle relaxants, hormone therapy, etc.), nonpharmacological or interventional therapies (neuromodulation, trigger point injections, surgery, etc.), physical therapies (physical therapy, massage, etc.), psychological therapies, and self-care. It often involves multiple appointments, extended monitoring periods, and collaboration among healthcare providers [7].
Hence, there is an urgent need to find a practical, relatively safe, and widely accepted intervention. Acupuncture is a traditional Chinese medical technique that has been used for centuries to stimulate specific acupoints and meridian channels, providing relief from pain and various other symptoms. Evidence suggests that acupuncture may be an effective and safe treatment for various types of chronic pain [8]. Moreover, studies have indicated that acupuncture might be a promising treatment option for reducing menstrual pain [9]. Therefore, it holds potential as a treatment modality for pain in PID.
Several systematic reviews and meta-analyses have been published in Chinese, discussing the association of acupuncture and moxibustion with PID [10–16]. Among them, only one published in 2017 mentioned pain relief [14], but it included only two studies that compared acupuncture therapies plus Chinese medicine with Chinese medicine alone, both assessing pain intensity scores. Furthermore, since 2016, twelve new trials focusing on pain relief in PID have been conducted [17–28]. As a result, we conducted a systematic review and meta-analysis, synthesizing data from previous trials to evaluate the safety and effectiveness of acupuncture therapies as therapeutic interventions for pain relief in individuals diagnosed with PID.
2. Methods
2.1. Type of studies
This study included randomized controlled trials that examined the role of acupuncture therapies as interventions for pain relief in individuals diagnosed with PID. There were no language limitations, and no restrictions were placed on blinding or allocation concealment. However, case reports, reviews, animal studies, clinical research studies comparing different types of acupuncture therapies or acupuncture therapies with Chinese medicine, and combination treatments involving non-acupuncture-related therapies were excluded. The study protocol was registered in PROSPERO before the study was conducted (CRD42023407399). The study was conducted in accordance with the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement [29].
2.2. Type of participants
The study included participants diagnosed with PID, including both acute and chronic types, based on internationally accepted diagnostic criteria [5]. The inclusion criteria did not depend on age, duration, or source of cases, and individuals with any comorbidities were excluded from the study.
2.3. Type of interventions
Acupuncture therapies were provided as complementary or alternative treatments in addition to routine treatment (RT). The included therapies were manual acupuncture (MA), electroacupuncture (EA), warm needling (WN), fire needle (FN), scalp acupuncture (SA), abdominal acupuncture (AA), auricular acupuncture (AA), acupoint catgut embedding (AE), acupoint injection (AJ), or acupuncture combined with other treatments such as Chinese medicine (CM). The acupuncture interventions in this study were reported in accordance with the Standards for Reporting Interventions in Clinical Trials of Acupuncture, providing clear and explicit descriptions of needle selection, acupoints, manipulations, and treatment protocols [30]. The control intervention consisted of RT, sham acupuncture, or no treatment.
2.4. Type of outcome measures
The original study investigated the efficacy of acupuncture therapies as therapeutic interventions for reducing abdominal or lumbosacral pain in individuals diagnosed with PID. The effectiveness was assessed using outcome indicators as measures. The primary outcomes included pain intensity scores for abdominal or lumbosacral pain, such as the visual analogue scale (VAS). The secondary outcomes included levels of inflammatory cytokines, anxiety or depression scores, life quality scores, and adverse reactions.
2.5. Search strategy
A comprehensive search was conducted across four English databases (PubMed, Embase, Web of Science, the Cochrane Library) and four Chinese databases (China National Knowledge Infrastructure, Wanfang Database, VIP Database, and Chinese Biomedical Literature Database) from the inception of the databases to February 20, 2023. The keywords used for the search were acupuncture, pelvic inflammatory disease, and RCT. The details of the search strategy are provided in the S1 Appendix. Obtaining gray literature was challenging. All eligible studies were evaluated by experts in the relevant field and subsequently analyzed.
2.6. Selection of studies
The screening process was conducted by two reviewers (Yi LC and Huang BY) following the established retrieval strategy. Duplicate studies were removed using EndNote X9 (Clarivate Analytics, Philadelphia, PA, USA). Non-qualifying studies were excluded based on the title and abstract, and eligible trials were selected for further evaluation based on the inclusion criteria and a full-text review. All researchers worked independently, and any discrepancies were resolved between the two reviewers. If any disagreements remained unresolved, a third reviewer (Zhou LL) was consulted to reach a consensus.
2.7. Data extraction
Data from the included studies were extracted and recorded in an Excel template. The extracted information included the year of publication, lead author, language, sample size, age range, disease duration, intervention details, acupoint selection, treatment duration and frequency, as well as primary and secondary outcome measures. Two independent evaluators conducted the data extraction process and resolved any discrepancies through discussion. The consistency of the extracted data was confirmed by a third party.
2.8. Quality assessment
The Cochrane Collaboration risk of bias (ROB) tool [31] was used to assess the methodological quality of each included study across seven domains, including random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. The ROB of each domain was classified as low, high, or unclear. The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach [32] was used to rate the overall quality of evidence across five domains, including the risk of bias, inconsistency, indirectness, imprecision, and potential publication bias. The quality of evidence was classified as high, moderate, low, or very low. We used GRADEpro GDT to conduct the Summary of Findings (SoF) table.
2.9. Statistical analysis
Statistical analyses were conducted using the RevMan 5.4 version. The effect size of dichotomous and continuous data was presented as odds ratio (OR) and mean difference (MD) or standard mean difference (SMD), all with a 95% confidence interval (CI). Heterogeneity among trials was identified using the I-squared and Chi2 test. Acceptable heterogeneity was defined as P > 0.1 or I2 < 50%, while significant heterogeneity was defined as P ≤ 0.1 or I2 ≥ 50%. The decision between the fixed-effect model and the random-effects model is still a subject of controversy [31]. Considering that studies may differ in different kinds of covariates, leading to different effect sizes across studies, we decided to conduct a random-effects model regardless of I-squared and Chi2 test. This choice is more appropriate and is more likely to fit the actual sampling distribution [33]. Subgroup analyses were conducted to discover the source of heterogeneity, and sensitivity analyses were performed to assess the robustness of the synthesized results. Missing data were obtained by contacting the study authors via email. In case of unavailable data, statistical analyses were performed using only studies in which relevant outcomes were reported. Pooled effects were calculated, and a two-sided P-value < 0.05 was considered statistically significant.
2.10. Assessment of reporting biases
If the number of included trials exceeded ten, visual funnel plots were employed to evaluate publication bias.
3. Results
3.1. Trial characteristics
Based on the search strategy, an initial screening was conducted on 2,068 trials retrieved from the eight aforementioned databases. Ultimately, twelve trials [17–28], involving a total of 1,165 participants, were included in this meta-analysis (Fig 1). All included trials were published between 2016 and 2023 and conducted in China. The sample sizes in the included studies ranged from 60 to 144 participants, and the treatment duration varied from 7 to 60 sessions. Among these trials, three [19, 26, 27] (25%) compared acupuncture therapies with RT, while nine [17, 18, 20–25, 28] (75%) investigated the use of acupuncture therapies in combination with RT versus RT alone. Specifically, three trials [21, 23, 24] compared the use of MA or EA in combination with RT against RT alone, two trials [18, 25] compared the use of WN in combination with RT against RT alone, two trials [17, 28] compared the use of MA in combination with CM and RT against RT alone, and two trials [20, 22] compared the use of MA in combination with MB or WN and CM and RT against RT alone. Adverse events were mentioned in five studies [17, 19, 20, 23, 24]. The characteristics of the included trials are presented in Table 1.
Fig 1. Study flow diagram.

Table 1. Characteristics of included trials.
| References | Country | Sample size (E/C) | Mean Age[y,(SD)] (E/C) | Course of disease[mean(SD)] (E/C) | Experimental treatment | Control treatment | Acupuncture points | Outcome |
|---|---|---|---|---|---|---|---|---|
| Acupuncture vs. Routine treatment | ||||||||
| Peng P 2022 [19] | China | 33/33 | 35.61±6.781/34.58±6.495 | 25.39±9.982/24.58±11.610(months) | MA+BL | Antimicrobial agent | Guanyuan(CV4) Zhongji(CV3) Zusanli(ST36) Xuehai(SP10) Sanyinjiao(SP6) Zigong(EX-CA1) |
①, ⑩ |
| Jiang X 2020 [27] | China | 30/31 | 33.47±6.91/32.16±6.35 | 20.47±9.80/19.19±10.12(months) | MA+WN | Antimicrobial agent+Analgesic | Guanyuan(CV4) Qihai(CV6) Guilai(ST29) Sanyinjiao(SP6) Shenshu(BL23) Yangbai(GB14) Yintang(GV24+) Sishencong(EX-HN3) |
①, ③, ⑦ |
| Xiao JY 2021 [26] | China | 30;30/30 | 33.37±5.629;31.90±6.666/33.73±7.565 | 3.020±1.480;2.967±1.811/3.283±1.770(years) | MA+TDP;MA+TDP | Antimicrobial agent | E1: Baliao(BL31, 32, 33, 34) Shenshu(BL23) Zhibian(BL54) Mingmen(GV4) Yaoyangguan(GV3) Sanyinjiao(SP6) E2: Zhongji(CV3) Guanyuan(CV4) Qihai(CV6) Sanyinjiao(SP6) Zigong(EX-CA1) |
①, ③ |
| Acupuncture plus routine treatment vs. Routine treatment | ||||||||
| Huang XQ 2023 [17] | China | 61/61 | 42.37±4.54/41.61±4.52 | 9.21±1.31/9.12±1.22(years) | MA+CM | Antimicrobial agent | Guanyuan(CV4) Qihai(CV6) Shenque(CV8) Sanyinjiao(SP6) |
①, ⑤, ⑥, ⑦, ⑧, ⑩ |
| Lin L 2022 [20] | China | 42/42 | 36.4±9.5/34.9±8.4 | 16.9±4.5/17.2±4.9(months) | MA+MB+CM | Analgesic | Guanyuan(CV4) Qihai(CV6) Zigong(EX-CA1) Tianshu(ST25) Zusanli(ST36) Sanyinjiao(SP6) Diji(SP8) Taixi(KI3) Hegu(LI4) |
①, ②, ⑨, ⑩ |
| Liu XT 2021 [23] | China | 30/30 | 28(22,49)/30(48,24) | 23.5(12,86)/24(7,39)(months) | MA | Analgesic | Guanyuan(CV4) Shuidao(ST28) Guilai(ST29) Shenshu(BL23) Ciliao(BL32) |
①, ⑩ |
| Liu YH 2021 [21] | China | 72/72 | 35±8/36±8 | 2.13±1.59/2.59±2.25(years) | EA | Analgesic | Guanyuan(CV4) Shuidao(ST28) Guilai(ST29) Shenshu(BL23) Ciliao(BL32) |
①, ②, ⑨ |
| Lu XH 2016 [28] | China | 45/45 | 33.1±5.3/32.3±4.9 | 19.2±5.7/18.7±5.3(months) | MA+CM+TDP | Antimicrobial agent | Guanyuan(CV4) Qihai(CV6) Xiawan(CV10) Zhongwan(CV12) Shuidao(ST28) Daheng(SP15) Qixue(KI13) |
① |
| Tian L 2020 [24] | China | 72/72 | 36.38±5.62/36.17±5.31 | 8.36±1.12/8.13±1.07(months) | EA | Analgesic | Guanyuan(CV4) Shuidao(ST28) Guilai(ST29) Shenshu(BL23) Ciliao(BL32) |
①, ②, ④, ⑥, ⑦, ⑨, ⑩ |
| Wang LN 2020 [25] | China | 42/42 | 36.96±5.19/38.25±6.31 | 7.84±3.79/7.20±4.57(months) | MA+WN | Antimicrobial agent+Analgesic | Qihai(CV6) Guilai(ST29) Ciliao(BL32) Xialiao(BL34) Sanyinjiao(SP6) Taichong(LR3) |
①, ⑧ |
| Wang Y 2022 [18] | China | 49/49 | 37.93±3.57/37.93±2.57 | 11.72±4.45/12.04±4.82(months) | MA+WN | Antimicrobial agent+Analgesic | Zhongji(CV3) Qihai(CV6) Shuidao(ST28) Guilai(ST29) Ganshu(BL18) Shenshu(BL23) Sanyinjiao(SP6) Xuehai(SP10) Taichong(LR3) |
①, ④, ⑤, ⑥ |
| Zhi XF 2021 [22] | China | 46/46 | 31.72±5.60/31.30±5.71 | 3.71±0.89/3.53±0.92(months) | WN+CM | Antimicrobial agent | Guanyuan(CV4) Qihai(CV6) Sanyinjiao(SP6) Xuehai(SP10) Zigong(EX-CA1) |
①, ⑦ |
①VAS score for abdominal pain; ②VAS score for lumbosacral pain; ③VAS score for long-term effect of abdominal pain; ④IL-2; ⑤IL-6; ⑥TNF-α; ⑦CRP; ⑧SAS score; ⑨WHOQOL-BREF score; ⑩Adverse events.
E/C, experimental group/control group; MA, manual acupuncture; WN, warm needling; EA, electroacupuncture; BL, blood letting; CM, Chinese medicine; TDP, specific electromagnetic spectrum therapy instrument; E1, experiment group 1; E2, experiment group 2.
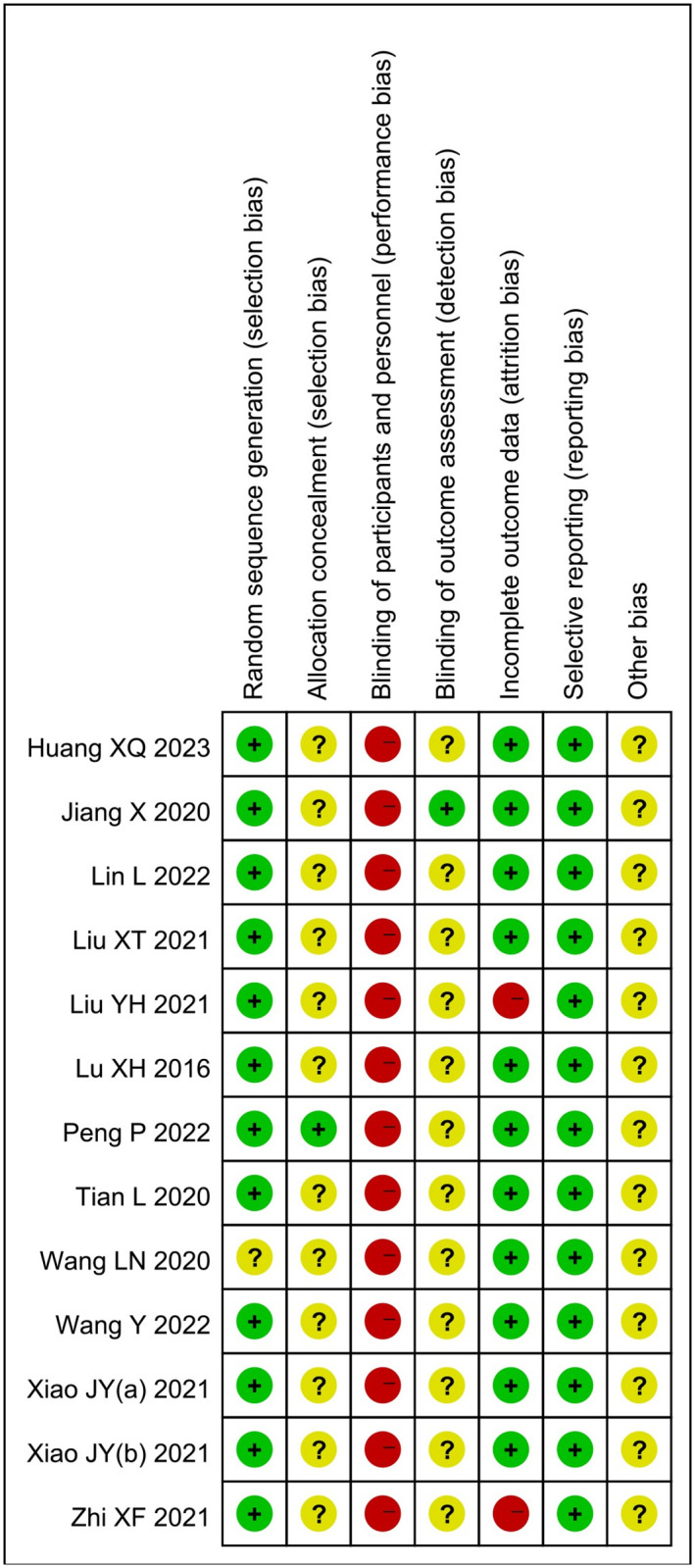
3.2. Risk of bias
All twelve trials were assessed for the risk of bias [17–28] (Fig 2). Eleven trials [17, 18, 20–24, 26–28] demonstrated a low risk of bias in the generation of random sequences. One trial [25] did not provide clear information regarding the method used for random sequence generation and was, therefore, deemed to have an unclear risk of bias. Regarding allocation concealment, eleven trials [17, 18, 20–28] had an unclear risk of bias due to insufficient details provided, while one trial [19] was considered to have a low risk of bias for providing adequate information. Blinding of the acupuncture practitioner was not feasible, resulting in a high risk of performance bias. However, one trial [27] reported blinding of the outcome assessor and was classified as having a low risk of bias, while the remaining trials had an unclear risk of bias due to insufficient reporting. Two trials [21, 22] had a high risk of bias in incomplete outcomes data due to participant withdrawal. All trials reported the predetermined outcome measures, indicating a low risk of bias in selective reporting. Due to insufficient registration information, all trials were judged to have an unclear risk of bias for other sources.
Fig 2. Risk of bias assessment.
3.3. Primary outcomes
3.3.1. VAS score for abdominal pain
The twelve trials [17–28], involving a total of 1,165 patients, provided data on the VAS score for abdominal pain. The results indicated that the application of acupuncture therapies resulted in a significant decrease in the VAS score associated with abdominal pain in individuals with PID (MD: -1.32; 95%CI: -1.60 to -1.05; P < 0.00001) (Fig 3). Heterogeneity was significant (I2 = 91%, P < 0.00001). Consequently, a subgroup analysis was conducted based on different intervention types. The data for subgroup 1 (acupuncture therapies alone) yielded an MD of -1.47; 95%CI: -1.83 to 1.11; P < 0.00001. For subgroup 2 (MA or EA plus RT), the MD was -1.55; 95%CI: -1.60 to -1.49; P < 0.00001. The data for subgroup 3 (WN plus RT) yielded an MD of -2.09; 95%CI: -2.43 to -1.74. The data for subgroup 4 (MA plus CM and RT) yielded an MD of -1.20; 95%CI: -1.36 to -1.04; P < 0.00001. Finally, the data for subgroup 5 (MA plus MB or WN plus CM and RT) resulted in an MD of -0.49; 95%CI: -0.69 to -0.30. These findings indicate that the acupuncture group exhibited significantly lower VAS scores for abdominal pain compared to the control group. No significant heterogeneity was observed among all subgroups (I2 = 27%, P = 0.25; I2 = 0%, P = 0.48; I2 = 0%, P = 0.87; I2 = 0%, P = 0.97; I2 = 0%, P = 0.44). The analysis revealed that the observed heterogeneity could be explained by the subgroup based on intervention type. To explore potential sources of heterogeneity, a sensitivity analysis was conducted, which revealed that the exclusion of each individual study in a successive manner did not significantly impact the overall pooled analysis.
Fig 3. Forest plot and meta-analysis of VAS score for abdominal pain.

3.3.2. VAS score for lumbosacral pain
Three trials [20, 21, 24] involving 372 patients reported that acupuncture reduced the VAS score for lumbosacral pain (MD: -1.14; 95%CI: -2.12 to -0.17; P < 0.00001) (Fig 4). Heterogeneity was significant (I2 = 98%, P < 0.00001). The influence of each study on the VAS score for lumbosacral pain was investigated by excluding one study at a time. The sensitivity analysis revealed that the study conducted by Tian L [24] was the primary contributor to the observed heterogeneity, as its exclusion resulted in an I2 value of 2% for the outcome.
Fig 4. Forest plot and meta-analysis of VAS score for lumbosacral pain.

3.3.3. VAS score for abdominal pain after one month
Two trials [26, 27] involving 181 patients demonstrated that acupuncture had a long-lasting effect on alleviating abdominal pain for at least one month (MD: -1.44; 95%CI: -2.15 to -0.72; P < 0.0001) (Fig 5). Heterogeneity was significant (I2 = 50%, P = 0.10). Notably, experiment group 1 in the study conducted by Xiao JY [26] was identified as the source of heterogeneity, as its exclusion resulted in an I2 value of 0% for the outcome.
Fig 5. Forest plot and meta-analysis of VAS score for abdominal pain after one month.

3.4. Secondary outcomes
3.4.1. IL-2
A total of two trials [18, 24] involving 242 patients reported the effect of acupuncture combination therapy on IL-2 levels. Overall, acupuncture treatment significantly increased IL-2 levels (SMD: 1.60; 95%CI: 1.31 to 1.89; P < 0.00001) (Fig 6). Heterogeneity was not significant (I2 = 0%, P = 0.40).
Fig 6. Forest plot and meta-analysis of IL-2 level.

3.4.2. IL-6
Two trials [17, 18], involving 220 patients, reported the effects of acupuncture on IL-6 levels. The results showed a significant reduction in IL-6 levels after acupuncture treatment (SMD: -2.59, 95%CI: -3.61 to -1.57; P < 0.00001) (Fig 7). Heterogeneity was significant (I2 = 87%, P = 0.02).
Fig 7. Forest plot and meta-analysis of IL-6 level.

3.4.3. TNF-α
Three trials [17, 18, 20], involving 364 patients, reported the effects of acupuncture on TNF-α levels. The results demonstrated a significant reduction in TNF-α levels following acupuncture treatment (SMD: -2.21, 95%CI: -2.47 to -1.95; P < 0.00001) (Fig 8). Heterogeneity was not significant (I2 = 0%, P = 0.60). Sensitivity analysis indicated that the result was stable.
Fig 8. Forest plot and meta-analysis of TNF-α level.

3.4.4. CRP
Four trials [17, 22, 24, 27] assessed the effect of acupuncture on CRP levels. Among them, one trial [27] compared acupuncture therapies alone with RT, while the other three trials [17, 22, 24] compared acupuncture therapies plus RT with RT. The results showed that acupuncture therapies alone significantly reduced CRP levels (MD: -4.01; 95%CI: -5.27 to -2.75; P < 0.00001), and acupuncture therapies as an adjunctive treatment, involving a total of 358 patients, also demonstrated higher effectiveness (MD: -3.85; 95%CI: -5.50 to -2.20; P < 0.00001) (Fig 9). Heterogeneity was significant (I2 = 90%, P = 0.0001). Sensitivity analysis revealed that the study conducted by Huang XQ [17] was the primary contributor to heterogeneity, as its exclusion resulted in an I2 value of 4% for the outcome.
Fig 9. Forest plot and meta-analysis of CRP level.

3.4.5. SAS
Only two trials [17, 25], comprising 206 patients, reported the effects of acupuncture on the SAS scores. The results showed that acupuncture significantly reduced the SAS scores in patients with PID (MD: -10.82; 95%CI: -16.60 to -5.04; P = 0.0002) (Fig 10). Heterogeneity was significant (I2 = 93%, P = 0.0001).
Fig 10. Forest plot and meta-analysis of SAS level.

3.4.6. Quality of life
Three trials [20, 21, 24] evaluated the patients’ quality of life using the WHOQOL-BREF. However, one trial [21] reported the four items of the scale separately, while the other two trials [20, 24] reported only the total score. The study by Liu YH [21] showed that the combination of acupuncture significantly improved all four domains (physical, psychological, environment, and social relationship), but only the physical domain showed a significant difference compared to RT. The meta-analysis of the other two studies, involving 228 patients, indicated that acupuncture increased the WHOQOL-BREF scores in patients with PID (MD: 8.29; 95%CI: 3.48 to 13.10; P = 0.0007) (Fig 11). Heterogeneity was significant (I2 = 87%, P = 0.006).
Fig 11. Forest plot and meta-analysis of WHOQOL-BREF score.

3.4.7. Adverse events
Among the twelve trials, one study [23] reported no adverse effects, and four studies [17, 19, 20, 24] reported the occurrence of adverse events. Among these, one study [19] compared acupuncture therapies alone with RT, while the other three studies [17, 20, 24] compared acupuncture therapies plus RT with RT. The results showed that the incidence of adverse events was lower in the acupuncture therapies group (0%) compared to the RT group (6%), and there was no significant difference between acupuncture therapies plus RT and RT (OR: 0.56; 95%CI: 0.21 to 1.51; P = 0.10) (Fig 12). Heterogeneity was not significant (I2 = 31%, P = 0.23). These findings indicate that acupuncture therapies do not increase the risk of adverse events and may have higher safety compared to RT.
Fig 12. Forest plot and meta-analysis of adverse events.

3.5. Publication bias
Funnel plots were used to assess the possibility of publication bias. The distribution of studies appeared to be asymmetric, with some studies lying outside the 95% confidence intervals, suggesting potential publication bias (Fig 13).
Fig 13. Funnel plots illustrating meta-analysis of VAS score for abdominal pain.

3.6. Assessment of evidence
The GRADEpro GDT was employed to assess the quality of evidence for the outcomes. The quality of evidence was downgraded due to a high risk of bias in the included studies, inadequate sample size, unexplained high heterogeneity, and asymmetry in the funnel plots. The VAS score for abdominal pain, IL-6, SAS, and WHOQOL-BREF outcomes demonstrated very low quality of evidence. The VAS score for lumbosacral pain, VAS score for abdominal pain after one month, IL-2, TNF-α, CRP, and adverse events showed a low quality of evidence. Further details are provided in the S2 Appendix.
4. Discussion
4.1. Main findings
This systematic review and meta-analysis, conducted in accordance with the Cochrane Collaboration Guidelines and following the PRISMA reporting checklist, is the first to investigate the efficacy and safety of acupuncture for relieving pain in PID. The results suggest that acupuncture therapies alone or in combination with RT are associated with higher therapeutic efficiency than RT alone. Acupuncture therapies, as complementary or alternative treatments, improve the effectiveness of reducing abdominal pain in patients with PID, and this effect persists for at least one month after treatment. Additionally, the effectiveness of reducing lumbosacral pain also demonstrates significant improvement. Our findings indicate a significant decrease in pro-inflammatory cytokines, particularly IL-6 and TNF-α, in response to acupuncture. Conversely, we observed an increase in the levels of anti-inflammatory cytokines, such as IL-2. This suggests that acupuncture may be effective in reducing inflammation by upregulating anti-inflammatory cytokines while downregulating pro-inflammatory ones. Furthermore, our results suggest the potential efficacy of acupuncture in relieving anxiety and improving the quality of life.
4.2. Investigation of heterogeneity
The heterogeneity was high across several outcomes. Subgroup analysis was conducted, which resulted in insignificant heterogeneity within each subgroup (I2 = 27%, P = 0.25; I2 = 0%, P = 0.48; I2 = 0%, P = 0.87; I2 = 0%, P = 0.97; I2 = 0%, P = 0.44). Therefore, we consider the use of different types of acupuncture therapies or their combination with CM as a possible explanation for the significant heterogeneity in the VAS score for abdominal pain. Sensitivity analyses were also conducted, suggesting that a shorter duration of the disease could explain the heterogeneity in the VAS score for lumbosacral pain, as the heterogeneity decreased to I2 = 2% after removing the trial of Tian L [24]. Furthermore, differences in acupoint selection could partially explain the heterogeneity in the VAS score for abdominal pain after one month, as the heterogeneity decreased to I2 = 0% after excluding the experimental group 1 of Xiao JY [26], which mainly focused on acupoints located in the lumbosacral region compared to the others, which were primarily in the lower abdomen. Additionally, a longer duration of the disease or older age could partly explain the heterogeneity in the CRP level results, as the heterogeneity decreased to I2 = 4% after excluding the trial of Huang XQ [17].
4.3. Mechanisms of acupuncture
Acupuncture therapies have been found to alleviate pain through peripheral, spinal, and supraspinal mechanisms [34]. Previous studies on acupuncture analgesia have demonstrated that acupuncture stimulation can increase the release of various opioid peptides in the central nervous system (CNS) [35] and inhibit the transmission of noxious inputs at the spinal level [34, 36, 37]. Recent studies have also demonstrated the anti-inflammatory effect of acupuncture by activating the vagal-adrenal anti-inflammatory axis [38–40], which can alleviate peripheral stimulation. Furthermore, the co-occurrence of chronic pain and psychiatric disorders, such as anxiety and depression [41], is well-documented and significantly impacts patients’ quality of life. Chronic pain patients are more susceptible to experiencing depression or anxiety [41], and these psychological stressors can contribute to hyperalgesia, an increase in the perception of visceral pain. Recent studies have also indicated the clinical efficacy of acupuncture in addressing emotional pain and anxiety disorders [42], which can contribute to pain management by improving psychological well-being.
4.4. Limitations
Several limitations should be acknowledged in this systematic review. Firstly, significant heterogeneity existed among the analyzed studies, partly due to the different types of interventions. Acupuncture therapies encompass various treatments, including manual acupuncture, electroacupuncture, scalp acupuncture, abdominal acupuncture, warm needling, and others. While our aim was to evaluate the overall effectiveness of acupuncture therapies, the strength of evidence for individual therapies may be diminished. Secondly, all the included trials were conducted and published in China, with publications in the Chinese language. This introduces a potential selection bias and limits the generalizability of the findings. Additionally, databases in languages such as Japanese and Korean were not searched, which means that some trials published in other languages may have been missed. Furthermore, it should be noted that the absence of trials with negative results, as indicated by the funnel plot analysis, suggests potential publication bias, which could impact the overall findings of this meta-analysis. Thirdly, the sample sizes of the included studies were relatively small (n = 60–144), and the methodological quality of each study was not high, resulting in low to very low-quality evidence. This likely reduces the precision of the outcomes and may lead to misleading results.
4.5. Implications for research
We recommend conducting rigorously designed studies with large sample sizes in different countries or regions to validate the efficacy of acupuncture therapies in relieving pain in PID. Furthermore, future studies could focus on comparing different acupuncture therapies and acupoint selections to determine the optimal treatment for pain in PID, which would have significant clinical implications.
5. Conclusion
Based on our findings, acupuncture therapies, either alone or as adjunctive therapies, may offer sustained clinical benefits in reducing abdominal and lumbosacral pain for at least one month. Acupuncture also demonstrates potential anti-inflammatory effects by promoting anti-inflammatory cytokines while reducing pro-inflammatory cytokines. Additionally, it may alleviate anxiety and improve the quality of life in patients with PID. The occurrence of adverse events was infrequent, with most events being mild and self-limiting, requiring no intervention for recovery. However, caution is advised when interpreting the results of our review due to the methodological limitations of the included trials. High-quality trials are essential to draw more reliable conclusions.
Supporting information
(DOCX)
(DOCX)
(PDF)
Data Availability
All relevant data are within the paper and its Supporting information files.
Funding Statement
The author(s) received no specific funding for this work.
References
- 1.Wihlfahrt K, Günther V, Mendling W, Westermann A, Willer D, Gitas G, et al. Sexually Transmitted Diseases-An Update and Overview of Current Research. Diagnostics (Basel). 2023;13(9). doi: 10.3390/diagnostics13091656 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Greydanus DE, Cabral MD, Patel DR. Pelvic inflammatory disease in the adolescent and young adult: An update. Dis Mon. 2022;68(3):101287. doi: 10.1016/j.disamonth.2021.101287 [DOI] [PubMed] [Google Scholar]
- 3.Hillier SL, Bernstein KT, Aral S. A Review of the Challenges and Complexities in the Diagnosis, Etiology, Epidemiology, and Pathogenesis of Pelvic Inflammatory Disease. J Infect Dis. 2021;224(12 Suppl 2):S23–s8. doi: 10.1093/infdis/jiab116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Curry A, Williams T, Penny ML. Pelvic Inflammatory Disease: Diagnosis, Management, and Prevention. Am Fam Physician. 2019;100(6):357–64. [PubMed] [Google Scholar]
- 5.Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1–187. doi: 10.15585/mmwr.rr7004a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pacheco-Carroza EA. Visceral pain, mechanisms, and implications in musculoskeletal clinical practice. Med Hypotheses. 2021;153:110624. doi: 10.1016/j.mehy.2021.110624 [DOI] [PubMed] [Google Scholar]
- 7.Lamvu G, Carrillo J, Ouyang C, Rapkin A. Chronic Pelvic Pain in Women: A Review. Jama. 2021;325(23):2381–91. doi: 10.1001/jama.2021.2631 [DOI] [PubMed] [Google Scholar]
- 8.Patel M, Urits I, Kaye AD, Viswanath O. The role of acupuncture in the treatment of chronic pain. Best Pract Res Clin Anaesthesiol. 2020;34(3):603–16. doi: 10.1016/j.bpa.2020.08.005 [DOI] [PubMed] [Google Scholar]
- 9.Li PS, Peng XM, Niu XX, Xu L, Hung Yu Ng E, Wang CC, et al. Efficacy of acupuncture for endometriosis-associated pain: a multicenter randomized single-blind placebo-controlled trial. Fertil Steril. 2023;119(5):815–23. doi: 10.1016/j.fertnstert.2023.01.034 [DOI] [PubMed] [Google Scholar]
- 10.Rong W, Fang W, Han W. Heat-sensitive moxibustion as adjuvant therapy for chronic pelvic inflammatory disease: a Meta-analysis. China’s Naturopathy. 2022;30(22):37–40. [Google Scholar]
- 11.Ting H, Hao C, Jie C, Youbing X, Youling G, Yanyun M. Effect of Acupuncture Therapy on Chronic Pelvic Inflammatory Disease: A Meta-analysis. Liaoning journal of traditional chinese medicine [liaoning zhong yi za zhi]. 2019;46(08):1573–8. doi: 10.13192/j.issn.1000-1719.2019.08.002 [DOI] [Google Scholar]
- 12.Ziying Z, Yanzhong W, Biya Y. Clinical Effect of Acupuncture and Moxibustion Combined with Herbal Enema in Treatment of Patients with Chronic Pelvic Inflammatory Disease:A Meta-analysis. Chinese Manipulation and Rehabilitation Medicine. 2017;8(03):45–7. doi: 10.19787/j.issn.1008-1879.2017.03.021 [DOI] [Google Scholar]
- 13.Xuan Z. Clinical Effect of Acupuncture and Moxibustion Combined with Traditional Chinese Medicine Enema in the Treatment of Patients with Chronic Pelvic Inflammatory Disease: A Meta- analysis. Journal of clinical acupuncture and moxibustion [zhen jiu lin chuang za zhi]. 2017;33(04):50–3. [Google Scholar]
- 14.Lili Z, Yang L, Danwei Z, Qin C, Yi L. Systematic Review and Meta-analysis of the Effect of Acupuncture on Chronic Pelvic Inflammation Disease. Journal of Zhejiang Chinese Medical University. 2017;41(11):928–40. doi: 10.16466/j.issn1005-5509.2017.11.021 [DOI] [Google Scholar]
- 15.Danping W. A systematic evaluation of warming needle moxibustion in treating chronic pelvic inflammatory. Master. Thesis, Guangzhou University of Chinese Medicine; 2016.
- 16.Linlin F, Wenhua Y, Xiaoqian L, Zhuang C, Jun M, Changping L. A Meta-analysis on effectiveness of Acupuncture and Moxibustion for Chronic Pelvic Inflammatory Disease. Acupuncture Research. 2014;39(02):156–63. doi: 10.13702/j.1000-0607.2014.02.013 [DOI] [PubMed] [Google Scholar]
- 17.Xiuqing H, Yan Y, Fangfang H, Zhuping W, Linyan L, Qi Y. Clinical Study on Acupuncture Combined with Xuefu Zhuyu Decoction for Chronic Pelvic Inflammatory Disease with Stasis-Toxin Internal Accumulation Syndrome. New Chinese Medicine. 2023;55(03):185–9. doi: 10.13457/j.cnki.jncm.2023.03.041 [DOI] [Google Scholar]
- 18.Yue W, Xin W. Clinical Study on Regulating Effect of Needle Warming Moxibustion on Cytokines and Th1 /Th2 Balance in Patients with Chronic Pelvic Pain after Pelvic Inflammatory Disease. Liaoning journal of traditional chinese medicine [liaoning zhong yi za zhi]. 2022;49(02):161–5. doi: 10.13192/j.issn.1000-1719.2022.02.045 [DOI] [Google Scholar]
- 19.Pan P. Clinical study of acupuncture combined with collateral prickingand cupping in the treatment of chronic pelvic pain in SPID. Master. Thesis, Guangxi University of Chinese Medicine; 2022.
- 20.Ling L, Yun J, Taofang F, Aijun W. Effect observation on the treatment of chronic pelvic pain with sequelae of pelvic inflammatory disease assisted by acupuncture and moxibustion. Chinese Journal of Rural Medicine and Pharmacy. 2022;29(19):23–5. [Google Scholar]
- 21.Yinghua L, Xin W, Zhuo L, Hui L, Dongmei Z, Ling S. Acupuncture combined with western medication on chronic pelvic pain after pelvic inflammatory disease: a multi-center randomized controlled trial. Chinese Acupuncture & Moxibustion. 2021;41(01):31–5. doi: 10.13703/j.0255-2930.20191218-k0002 [DOI] [PubMed] [Google Scholar]
- 22.Xianfeng Z, Yanxi C, Lijun R, Chongyang F, Yuanhe L. Clinical Study on Warm Acupuncture combined with Qidan Quyu Decoction for 46 cases of Chronic Pelvic Inflammatory Disease with qi stagnation and blood stasis. Global Traditional Chinese Medicine. 2021;14(10):1901–4. [Google Scholar]
- 23.Xiaotong L. Clinical Observation on Acupuncture treating sequelae of Pelvic Inflammatory Disease (Chronic Pelvic Pain). Master. Thesis, Liaoning University of Traditional Chinese Medicine; 2020.
- 24.Lu T, Xin W. Clinical Effect of Acupuncture on Pelvic Pain Caused by Chronic Pelvic Inflammatory Disease and Iits Effect on Immune Cells and Inflammatory Factors. World Journal of Integrated Traditional and Western Medicine. 2020;15(05):785–9. doi: 10.13935/j.cnki.sjzx.200501 [DOI] [Google Scholar]
- 25.Lina W, Xin W. Warming Acupuncture for Chronic Pelvic Pain Following Pelvic Infl ammatory Disease of Qi Stagnation and Blood Stasis. Jilin Journal of Chinese Medicine. 2020;40(10):1380–2. doi: 10.13463/j.cnki.jlzyy.2020.10.034 [DOI] [Google Scholar]
- 26.Jieyun X. Clinical study on the treatment of chronicpelvic pain from sequelae of pelvic inflammatory disease treated by acupuncture from drawing yang from yin combined with finch pecking and moxibustion. Master. Thesis, Guangxi University of Chinese Medicine; 2020.
- 27.Xin J. The clinical study In treating Chronic Pelvic Inflammatory Disease by Jin`s three needle. Master. Thesis, Guangzhou University of Chinese Medicine; 2019.
- 28.Xihua L, Xiaofang C, Chunhua Z, Daihong L, Jianghua Y, Xiaosheng Q, et al. Abdominal acupuncture combined with Chinese medicine fumigation in the treatment of 45 cases of chronic pelvic inflammatory disease. Practical Clinical Journal of Integrated Traditional Chinese and Western Medicine. 2016;16(01):58–9. [Google Scholar]
- 29.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J Clin Epidemiol. 2021;134:103–12. doi: 10.1016/j.jclinepi.2021.02.003 [DOI] [PubMed] [Google Scholar]
- 30.MacPherson H, Altman DG, Hammerschlag R, Youping L, Taixiang W, White A, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT statement. J Evid Based Med. 2010;3(3):140–55. doi: 10.1111/j.1756-5391.2010.01086.x [DOI] [PubMed] [Google Scholar]
- 31.Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page M, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane. 2022. www.training.cochrane.org/handbook.
- 32.Schünemann H, Brożek J, Guyatt G, Oxman A. Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach. GRADE Working Group. 2013. https://gdt.gradepro.org/app/handbook/handbook.html.
- 33.Borenstein M, Hedges LV, Higgins JP, Rothstein HR. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synth Methods. 2010;1(2):97–111. doi: 10.1002/jrsm.12 [DOI] [PubMed] [Google Scholar]
- 34.Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi: 10.1097/ALN.0000000000000101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Qiao L, Guo M, Qian J, Xu B, Gu C, Yang Y. Research Advances on Acupuncture Analgesia. Am J Chin Med. 2020;48(2):245–58. doi: 10.1142/S0192415X20500135 [DOI] [PubMed] [Google Scholar]
- 36.Lao L, Zhang RX, Zhang G, Wang X, Berman BM, Ren K. A parametric study of electroacupuncture on persistent hyperalgesia and Fos protein expression in rats. Brain Res. 2004;1020(1–2):18–29. doi: 10.1016/j.brainres.2004.01.092 [DOI] [PubMed] [Google Scholar]
- 37.Zhang YQ, Ji GC, Wu GC, Zhao ZQ. Excitatory amino acid receptor antagonists and electroacupuncture synergetically inhibit carrageenan-induced behavioral hyperalgesia and spinal fos expression in rats. Pain. 2002;99(3):525–35. doi: 10.1016/S0304-3959(02)00268-3 [DOI] [PubMed] [Google Scholar]
- 38.Liu S, Wang Z, Su Y, Qi L, Yang W, Fu M, et al. A neuroanatomical basis for electroacupuncture to drive the vagal-adrenal axis. Nature. 2021;598(7882):641–5. doi: 10.1038/s41586-021-04001-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Liu S, Wang ZF, Su YS, Ray RS, Jing XH, Wang YQ, et al. Somatotopic Organization and Intensity Dependence in Driving Distinct NPY-Expressing Sympathetic Pathways by Electroacupuncture. Neuron. 2020;108(3):436–50.e7. doi: 10.1016/j.neuron.2020.07.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Torres-Rosas R, Yehia G, Peña G, Mishra P, del Rocio Thompson-Bonilla M, Moreno-Eutimio MA, et al. Dopamine mediates vagal modulation of the immune system by electroacupuncture. Nat Med. 2014;20(3):291–5. doi: 10.1038/nm.3479 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Michaelides A, Zis P. Depression, anxiety and acute pain: links and management challenges. Postgrad Med. 2019;131(7):438–44. doi: 10.1080/00325481.2019.1663705 [DOI] [PubMed] [Google Scholar]
- 42.Patil S, Sen S, Bral M, Reddy S, Bradley KK, Cornett EM, et al. The Role of Acupuncture in Pain Management. Curr Pain Headache Rep. 2016;20(4):22. doi: 10.1007/s11916-016-0552-1 [DOI] [PubMed] [Google Scholar]