

Abstract
Introduction: Groin hernia literature often uses the terms light- and heavyweight and small or large pores to describe meshes. There is no universal definition of these terms, and the aim of this scoping review was to assess how mesh weight and pore sizes are defined in the groin hernia literature.
Methods: In this systematic scoping review, we searched PubMed, Embase, and Cochrane CENTRAL. We included randomised controlled trials with adults undergoing groin hernia repair with the Lichtenstein or laparoscopic techniques using a flat permanent polypropylene or polyester mesh. Studies had to use the terms lightweight, mediumweight, or heavyweight to be included, and the outcome was to report how researchers defined these terms as well as pore sizes.
Results: We included 48 studies with unique populations. The weight of lightweight meshes ranged from 28 to 60 g/m2 with a median of 39 g/m2, and the pore size ranged from 1.0 to 4.0 mm with a median of 1.6 mm. The weight of heavyweight meshes ranged from 72 to 116 g/m2 with a median of 88 g/m2, and the pore size ranged from 0.08 to 1.8 mm with a median of 1.0 mm. Only one mediumweight mesh was used weighing 55 g/m2 with a pore size of 0.75 mm.
Conclusion: There seems to be a consensus that meshes weighing less than 60 g/m2 are defined as lightweight and meshes weighing more than 70 g/m2 are defined as heavyweight. The weight terms were used independently of pore sizes, which slightly overlapped between lightweight and heavyweight meshes.
Keywords: inguinal hernia, groin hernia, femoral hernia, lightweight mesh, heavyweight mesh
Introduction
The standard treatment for symptomatic groin hernia is mesh repair (1). The rationale for using a mesh is the lower risk of recurrence compared with non-mesh repair (1), and the long-term reoperation rate is reported to be around 5% for mesh repairs (2). Despite the concern that meshes might introduce groin pain, a systematic review has shown that there is no difference in the risk of chronic pain regardless of repairing inguinal hernias with or without mesh (3). Therefore, the recommended and most used techniques are the Lichtenstein repair and the laparoscopic transabdominal preperitoneal (TAPP) and total extraperitoneal (TEP) techniques (1).
Today, there are many different meshes on the market, but the most used is a permanent flat polypropylene mesh (1). The terms lightweight, mediumweight, and heavyweight together with large and small porous have been used for many years to describe a mesh. Generally, a lightweight mesh has large pore size with less weight, whereas a heavyweight mesh has small pore size with more weight (1). Interestingly, systematic reviews have shown a lower risk of chronic pain when using a lightweight mesh in Lichtenstein repair (4) and a lower risk of recurrence when using a heavyweight mesh in laparoscopic repair (5). However, there is no clear definition of what the definition of a lightweight and heavyweight mesh is (1).
Due to the lack of agreement on mesh weight definitions, this systematic scoping review aimed to map how researchers conducting randomised controlled trials (RCT) on patients with groin hernias have defined lightweight, mediumweight, and heavyweight meshes in terms of areal weight and pore sizes.
Methods
This systematic scoping review was reported using the Preferred Reporting Items for Systematic reviews and Meta-Analysis extension for Scoping Review (PRISMA-ScR) guideline (6). The protocol was registered at Open Science Framework (OSF) before data extraction was initiated (7).
The eligibility criteria were studies including participants minimum 18 years old undergoing groin hernia repair with a mesh using the Lichtenstein, TAPP, or TEP techniques. The mesh had to be flat and made of permanent polypropylene or polyester, and simple flat meshes are the most commonly used mesh type (1). And the studies had to use the terms lightweight, mediumweight, or heavyweight when describing the mesh. The outcome of this systematic scoping review was to report researchers’ definitions of light-, medium-, and heavyweight meshes. To define the mesh weight, we focused on areal weight in g/m2, but other definitions of weight were also considered. Furthermore, pore sizes were also included in studies where the weight was defined. An additional outcome was to report how many studies had used light-, medium-, and heavyweight meshes when repairing with the Lichtenstein, TAPP, or TEP techniques. We excluded studies that used meshes of other shapes than simple flat, such as special firm borders, 3D shapes, and self-gripping or adhesive meshes. If studies only mentioned using a light-, medium-, or heavyweight mesh but without further specifying the weight, the manufacturer’s website was searched to retrieve these data. We excluded studies if they failed to mention the term “weight.” We also excluded studies if the areal weight was insufficiently described in the study and it could not be found on the website of the manufacturer, regardless of whether they had reported the pore size or not. Studies that included other repairs than inguinal- or femoral hernia repairs or other meshes than flat polypropylene or polyester meshes were included if the results were separately presented for the eligible patients. Finally, only published randomised controlled trials written in English were included.
A search strategy was first created in PubMed with the help of an information specialist. This search strategy was later converted to the databases Embase and Cochrane CENTRAL. All searches were conducted on 19 August 2022. We also performed a snowball search by studying the reference lists of the included studies (8), and studies that seemed relevant were full text screened according to the eligibility criteria. The search strategy in PubMed was: “(femoral OR inguinal OR groin OR lateral OR medial OR pantaloon OR indirect OR direct) AND (hernia OR hernia [MeSH Terms]) AND (“randomized control trial” [Title/Abstract] OR “controlled clinical trial” [Title/Abstract] OR “randomized” [Title/Abstract] OR “randomised” [Title/Abstract] OR “RCT” [Title/Abstract] OR “trial” [Title/Abstract]).” After conducting the searches, studies were imported to the reference software Mendeley 1 where duplicates were removed. The studies were screened using the software Covidence 2 , which also removed further duplicates. Both the screening of titles and abstracts and of full text papers were done by two authors independently. If there were any disagreement, it was resolved by discussion within the author group. If needed, study authors were contacted by e-mail twice for data clarity.
Data were first extracted for five studies to a pilot Excel spreadsheet by the first author. The pilot sheet was discussed within the author group, and after agreement on the final spreadsheet, the first author extracted data uniformly for all studies. The extracted data were first author, year of publication, number of eligible patients, type of groin hernia repair, type of groin hernia (inguinal or femoral), whether the mesh was defined as light-, medium-, or heavyweight, and mesh details such as weight in g/m2, pore size, and mesh size. Categorical data were presented with numbers and percentages, and continuous data were reported as median and interquartile range (IQR) and range. Pore sizes reported in mm2 were calculated to diameter in mm based on the formula to calculate the area of a circle and isolation of radius; “A = π·r2”.
Results
Study selection is illustrated in the PRISMA flowchart (Figure 1). We identified 8,059 records, and 1,054 of these were full text screened. Finally, 59 studies fulfilled the eligibility criteria (9–67). Of these studies, 11 had reused the patient population (57–67), which resulted in 48 studies with a unique population (9–56). Thus, only data from these 48 studies are presented in the following.
FIGURE 1.
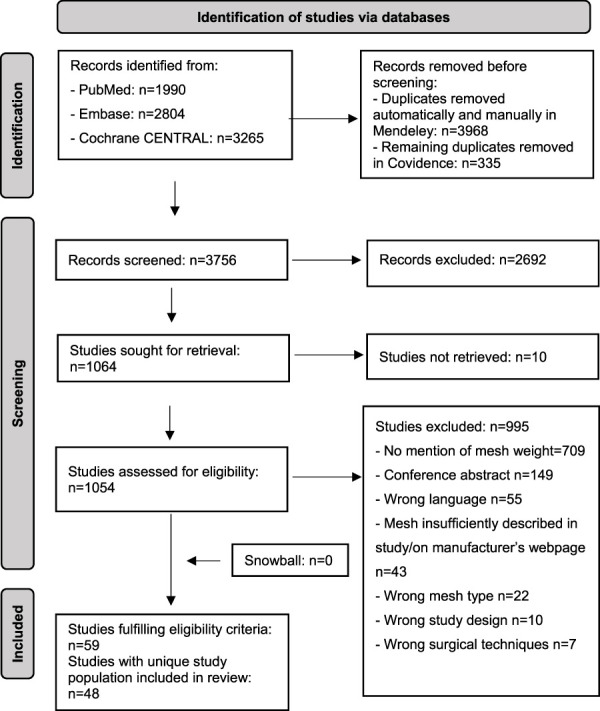
Preferred Reporting Items for Systematic reviews and Meta-Analysis extension for Scoping Review (PRISMA) flow diagram. n: number.
Study characteristics are presented in Table 1. The 48 randomised controlled trials (9–67) were published between 2003 and 2021. Thirty-seven studies used the Lichtenstein repair (10–29, 31, 32, 34–39, 43–46, 50–53, 55) and 12 studies used laparoscopic repairs (9, 28, 30, 33, 40–42, 48–49, 54, 56). Of these 12 studies, six used TEP repair (28, 33, 40–42, 54), four used TAPP repair (30, 48, 49, 56), and two studies used TEP and TAPP repairs (10, 47). Two of the 48 studies included patients with groin hernias (17, 41), and the remaining studies only included inguinal hernias. One study used a polyester mesh (13) while the remaining 47 studies used meshes made of polypropylene. Nine of the studies used two meshes (48–56), resulting in 48 studies mentioning mesh weight for 57 meshes. Of these 58 meshes, 26 were by the authors defined as lightweight meshes (9–28, 50–55), 30 as heavyweight meshes (29–56), and one as a mediumweight mesh (56). Even though three studies did not use the term heavyweight, we interpreted it as heavyweight since two studies described the mesh as conventional densely woven (46, 50) and one as non-lightweight with a high areal weight (42). The one study that defined their mesh as mediumweight had a weight of 55 g/m2 and a pore size of 0.75 mm (56).
TABLE 1.
Study characteristics and mesh properties.
| Ref | Study characteristics | Mesh characteristics | Brand | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Year | Patients a | Hernia | Repair type | Mesh | Weight (g/m2) | Pore (mm) | Size (cm) | ||
| (9) | 2016 | 140 | Inguinal | TEP/TAPP | LW | 30–45 | > 2 | 10 x 15 | Prolene soft |
| (10) | 2021 | 20 | Inguinal | Lichtenstein | LW | 44 | NR | NR | Prolene |
| (11) | 2017 | 70 | Inguinal | Lichtenstein | LW | 36 | 1 | NR | Optilene LP |
| (12) | 2017 | 170 | Inguinal | Lichtenstein | LW | 46 | NR | NR | Parietex |
| (13) | 2017 | 370 | Inguinal | Lichtenstein | LW | 60 | NR | 7.5 x 15 | Optilene |
| (14) | 2016 | 63 | Inguinal | Lichtenstein | LW | 36 | 3.0–4 | 4.5 x 10 | Optilene LP |
| (15) | 2016 | 258 | Inguinal | Lichtenstein | LW | 38 | NR | NR | Parietene Light |
| (16) | 2016 | 151 | Groin | Lichtenstein | LW | 53.7 | NR | NR | Parietene Light |
| (17) | 2015 | 216 | Inguinal | Lichtenstein | LW | 60 | NR | 9 x 13 | Optilene |
| (18) | 2015 | 75 | Inguinal | Lichtenstein | LW | 36 | 1 | 6 x 14 | Optilene LP |
| (19) | 2014 | 287 | Inguinal | Lichtenstein | LW | 38 | NR | NR | Parietene Light |
| (20) | 2014 | 70 | Inguinal | Lichtenstein | LW | 36 | 1 | 4.5 x 10 | Optilene LP |
| (21) | 2013 | 159 | Inguinal | Lichtenstein | LW | NR | NR | 6 x 13.7 | Soft mesh, Bard |
| (22) | 2013 | 80 | Inguinal | Lichtenstein | LW | 48 | NR | NR | Evolution P3EM |
| (23) | 2012 | 196 | Inguinal | Lichtenstein | LW | 35 | 1.6 | 10 x 15 | Prolene |
| (24) | 2012 | 153 | Inguinal | Lichtenstein | LW | <40 | NR | NR | Parietene Light |
| (25) | 2012 | 110 | Inguinal | Lichtenstein | LW | 52 | NR | 7.5 x 15 | ProLite-Ultra |
| (26) | 2011 | 302 | Inguinal | Lichtenstein | LW | 60 | NR | 9 x 13 | Optilene |
| (27) | 2011 | 110 | Inguinal | Lichtenstein | LW | 38 | NR | NR | Surgimesh WN |
| (28) | 2020 | 176 | Inguinal | Lichtenstein/TEP | LW | 38 | 1.6 | 10 x 15 | Parietene Light |
| (29) | 2020 | 43 | Inguinal | Lichtenstein | HW | 80–85 | NR | 6 x 12 | Prolene |
| (30) | 2020 | 54 | Inguinal | TAPP | HW | >75 | NR | 10 x 15 | NR |
| (31) | 2018 | 197 | Inguinal | Lichtenstein | HW | 90 | NR | NR | Bard Flatmesh |
| (32) | 2017 | 25 | Inguinal | Lichtenstein | HW | 100 | NR | NR | Marlex |
| (33) | 2015 | 454 | Inguinal | TEP | HW | 80 | 0.8–1.2 | 10 x 15 | Prolene |
| (34) | 2014 | 113 | Inguinal | Lichtenstein | HW | 82 | 0.8 | 8 x 12 | Prolene |
| (35) | 2014 | 25 | Inguinal | Lichtenstein | HW | 85 | NR | 10 x 15 | Prolene |
| (36) | 2013 | 76 | Inguinal | Lichtenstein | HW | 100 | 1 | NR | NR |
| (37) | 2012 | 300 | Inguinal | Lichtenstein | HW | >80 | NR | NR | Prolene |
| (38) | 2011 | 34 | Inguinal | Lichtenstein | HW | 100 | 1 | 8 x 15 | NR |
| (39) | 2011 | 16 | Inguinal | Lichtenstein | HW | 105 | 0.82 | NR | Prolene |
| (40) | 2010 | 20 | Inguinal | TEP | HW | 95 | 1 | 13 x 15 | Marlex |
| (41) | 2010 | 211 | Groin | TEP | HW | 105 | 0.8-1 | 12 x 15 | Prolene |
| (42) | 2010 | 40 | Inguinal | TEP | HW | 80 | NR | 10 x 15 | Hi-Trex |
| (43) | 2008 | 161 | Inguinal | Lichtenstein | HW | >80 | NR | 10 x 15 | Prolene |
| (44) | 2006 | 301 | Inguinal | Lichtenstein | HW | >80 | NR | 7.5 x 15 | Prolene |
| (45) | 2005 | 159 | Inguinal | Lichtenstein | HW | 85 | 1 | NR | Prolene |
| (46) | 2004 | 48 | Inguinal | Lichtenstein | HW | 100–110 | NR | 8 x 13 | Atrium |
| (47) | 2013 | 149 | Inguinal | TEP/TAPP | HW | 80–85 | NR | 10 x 15 | Prolene |
| (48) | 2008 | 120 | Inguinal | TAPP | HW | 108 | 1.0–1.6 | 10 x 15 | Prolene |
| HW | 116 | 0.08–0.1 | 10 x 15 | Serapen | |||||
| (49) | 2003 | 40 | Inguinal | TAPP | HW | 108 | 1.0–1.6 | NR | Prolene |
| HW | 116 | 0.8–1.0 | Serapen | ||||||
| (50) | 2007 | 153 | Inguinal | Lichtenstein | LW | 55 | NR | NR | Premilene Mesh LP |
| HW | 82 | Premilene | |||||||
| (51) | 2017 | 58 | Inguinal | Lichtenstein | LW | 43.7 | 2.8 | 7 x 15 | Bard Davol |
| HW | 105.4 | 0.84 | 7 x 15 | Bard Davol | |||||
| (52) | 2013 | 110 | Inguinal | Lichtenstein | LW | 36 | 2.6 | 7.5 x 15 | Dynamesh |
| HW | 72 | 1.8 | 7.5 x 15 | Dynamesh | |||||
| (53) | 2010 | 135 | Inguinal | Lichtenstein | LW | 36 | 1 | 4.5 x 10 | Optilene |
| HW | 82 | 0.8 | 4.5 x 10 | Premilene | |||||
| (54) | 2009 | 50 | Inguinal | TEP | LW | <50 | >1 | 12 x 15 | NR |
| HW | ≈100 | <1 | 12 x 15 | NR | |||||
| (55) | 2009 | 25 | Inguinal | Lichtenstein | LW | 43 | NR | NR | Surgimesh WN |
| HW | 80 | Surgipro | |||||||
| (56) | 2011 | 300 | Inguinal | TAPP | MW | 55 | 0.75 | 10 x 15 | Premilene LP |
| HW | 90 | 1.2 | 10 x 15 | Prolene | |||||
Only the numbers of eligible patients are presented; ref, reference; NR, not reported; TEP, total extraperitoneal; TAPP, transabdominal preperitoneal; LW, lightweight; HW, heavyweight; MW, mediumweight.
In the 37 studies where the Lichtenstein technique was used, 30 lightweight and 18 heavyweight meshes were used (Table 2). In 12 studies where laparoscopic techniques were used, 3 lightweight, 12 heavyweight, and 1 mediumweight mesh were used (Table 2).
TABLE 2.
Summary of groin hernia repairs and type of meshes used.
| Operation and mesh type | Number of studies (%) |
|---|---|
| Lichtenstein repair | 37 |
| lightweight | 19 (51) |
| heavyweight | 13 (35) |
| mediumweight | 0 (0) |
| light- and heavyweight | 5 (14) |
| Laparoscopic repair | 12 |
| lightweight | 2 (17) |
| heavyweight | 8 (67) |
| mediumweight | 0 (0) |
| light- and heavyweight | 1 (8) |
| medium- and heavyweight | 1 (8) |
Lightweight Mesh
A total of 26 lightweight meshes were reported in 25 studies (9–28, 50–55) (Table 1). The areal weight was reported in all but one study (21), with a median of 39 g/m2, an IQR of 36–50 g/m2, and a range of 35–60 g/m2 (Figure 2A). The only study that did not report the weight in g/m2 described the weight as “approximately 60% lighter weight than traditional polypropylene mesh” (21). The pore size was reported in 13 studies (9–11, 14, 18, 20, 22, 23, 28, 50–53) (Figure 2B). Two studies described that the lightweight mesh had large pore size without specifying the size in mm (10, 22), while the remaining ten studies either reported the pore diameter in mm or in µm, which was converted to mm (one study informed the size by email (23)) (9, 11, 14, 18, 20, 23, 50–53). Two studies had unspecified pore sizes (9, 53) and two studies used a range (14, 28). Nevertheless, the median of all lightweight meshes was 1.6 mm with an IQR of 1.0–2.3 mm and a range of 1.0–4.0 mm.
FIGURE 2.
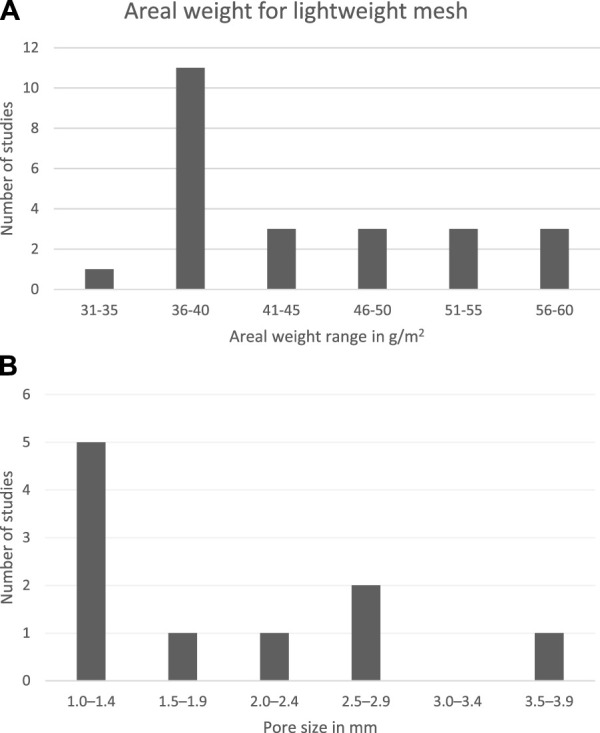
Definition of lightweight meshes regarding (A) areal weight and (B) pore size diameter in mm. For studies that provided a range, the mean of this range was calculated and used in the figure. Some areal weight and pore sizes were reported in an unspecified manner, and these were categorised in the range closest to the minimum estimate (i.e., >1 was classified in the range closest to 1 but also greater than 1).
The mesh size was reported in cm in 15 studies (9, 13, 14, 17, 19, 20, 21, 23, 25, 26, 28, 51–54). There were many variations, which are presented in Table 1.
Heavyweight Mesh
A total of 30 heavyweight meshes were reported in 28 studies (29–56) (Table 1). For all heavyweight meshes, the areal weight was reported in g/m2 with a median areal weight of 88 g/m2, an IQR of 81–104 g/m2, and a range of 72–116 g/m2 (Figure 3A).
FIGURE 3.
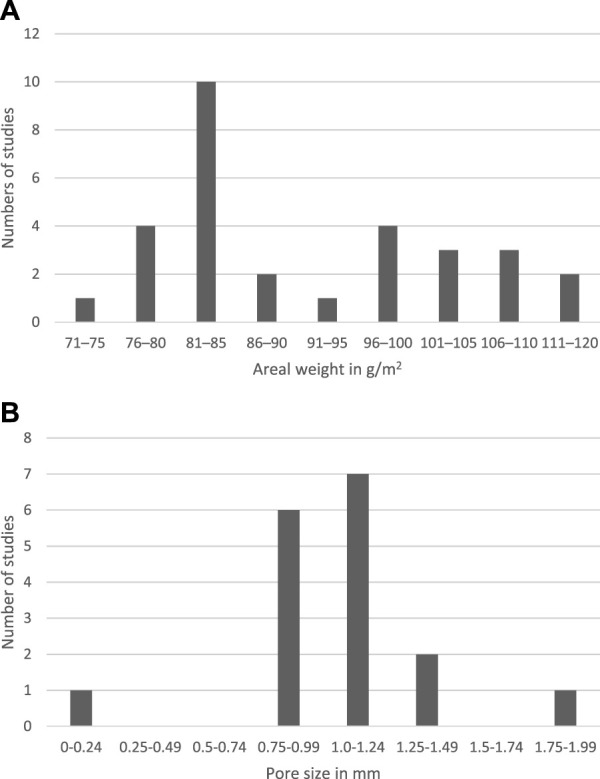
Definition of heavyweight meshes regarding areal weight (A). Pore size for heavyweight meshes in mm (B). For studies that provided a range, the mean of this range was calculated and used in the figure. Both for areal weight and for pore sizes reported in greater-than x were categorised in the closest ranging group.
The pore size was reported in mm for 15 studies (33, 34, 36, 38–41, 45, 48, 49, 51–54, 56), with a median of 1.0 mm, an IQR of 0.84–1.0 mm, and a range of 0.08–1.8 mm (Figure 3B). One study that reported the mesh having 0.8–1.2 mm pores also described the mesh as having small pores (33), while another study only mentioned that the mesh was microporous without specifying the size in mm (28).
The mesh size was reported in 19 studies for 20 heavyweight meshes (29, 30, 33–35, 38, 40–44, 46, 47, 48, 51–54, 56). Nine of the meshes measured 10 × 15 cm (30, 33, 35, 42, 43, 47, 48, 56), but there were many variations (Table 1).
Discussion
In this systematic scoping review, we reported how mesh weight was defined in randomised controlled trials on groin hernia repair. There seemed to be a distinct definition in the areal weight, where lightweight had an areal weight of ≤60 g/m2 and heavyweight had an areal weight of >70 g/m2. Pore sizes overlapped between lightweight and heavyweight meshes.
This study has several strengths. It is reported according to the PRISMA-ScR (6), and the protocol was registered in a public database before data extraction to increase transparency (7). We conducted a broad search using various databases with assistance from an information specialist, and two authors screened the titles and abstracts and the full text studies. Our study also has limitations. Only one author extracted data, but all data were reviewed for accuracy. Another limitation is that we only included English language studies. However, only including English language rarely compromises the review quality (68). Thirdly, ten studies could not be retrieved. Lastly, since this study’s main focus was on mesh weight and pore sizes it does not include other technical aspects of mesh properties such as elasticity, tensile strength, and other design properties of the mesh.
We need a universal classification based on the specific properties of the mesh as proposed by an international guideline on inguinal hernia management (1). However, this guideline (1) also points out that a universal classification is hard to achieve. In this study, we have investigated how RCTs have defined light–, medium–, and heavyweight mesh terms for flat polypropylene or polyester meshes. Only one study used a mediumweight mesh, and the nomenclature should therefore probably only comprise lightweight and heavyweight mesh. Even though there was some consensus regarding the areal mesh weight in g/m2, there was no general agreement of what small pores and large pores are and if lightweight and heavyweight meshes have characteristic pore sizes. Earlier studies have tried to categorise mesh weight classes. A study from 2008 proposed a classification as follows (69): ultralight weight <35 g/m2, lightweight 35–50 g/m2, mediumweight 51–90 g/m2, and heavyweight >90 g/m2. Another proposed classification from 2012 (70) emphasised that in the previous classification (69), a heavyweight mesh weighing 91 g/m2 would be in the same category as a heavyweight mesh weighing almost three times the weight. Thus, they proposed a classification that doubles the next limit: ultra-light <35 g/m2, light ≥35 <70 g/m2, standard ≥70 < 140 g/m2, and heavy ≥140 g/m2. Recently, meta-analyses comparing light- and heavyweight meshes in patients undergoing laparoscopic repair (5) or Lichtenstein repair (4) for uncomplicated inguinal hernia have defined lightweight meshes as ≤ 50 g/m2 and heavyweight meshes as >70 g/m2. Some of the lightweight meshes in this scoping review were over 50 g/m2, but the heavyweight meshes were in the same category as the proposed definition by the meta-analyses (4, 5). This underlines the problem with the classifications as mesh types fall under different categories. It is important to achieve a common technical language so that surgeons with different backgrounds and educational systems agree upon and utilise a common language. This would ease comparison in meta-analyses, thereby guiding clinical practice. However, the mesh market is in constant development, and with the current data presented here, we propose a simplified definition where lightweight could be all meshes with an areal weight ≤60 g/m2 and heavyweight meshes would be all meshes with an areal weight >70 g/m2.
In conclusion, the areal weight for lightweight and heavyweight meshes had a wide range, but all studies have defined lightweight as being ≤60 g/m2 and heavyweight as being >70 g/m2. There was an overlap between light- and heavyweight meshes’ pore sizes with a tendency that lightweight meshes had larger pore sizes.
Footnotes
Mendeley (2022). Available from: https://www.mendeley.com (Accessed November 2, 2022).
Covidence (2022). Available from: https://www.covidence.org (Accessed November 2, 2022).
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
- 1. The HerniaSurge Group. International Guidelines for Groin Hernia Management. Hernia (2018) 22:1–165. 10.1007/s10029-017-1668-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Kehlet H, Bay-Nielsen M, Danish Hernia Database Collaboration. Nationwide Quality Improvement of Groin Hernia Repair from the Danish Hernia Database of 87,840 Patients from 1998 to 2005. Hernia (2008) 12:1–7. 10.1007/S10029-007-0285-5 [DOI] [PubMed] [Google Scholar]
- 3. Öberg S, Andresen K, Klausen TW, Rosenberg J. Chronic Pain after Mesh versus Nonmesh Repair of Inguinal Hernias: a Systematic Review and a Network Meta-Analysis of Randomized Controlled Trials. Surgery (2018) 163:1151–9. 10.1016/j.surg.2017.12.017 [DOI] [PubMed] [Google Scholar]
- 4. Bakker WJ, Aufenacker TJ, Boschman JS, Burgmans JPJ. Lightweight Mesh Is Recommended in Open Inguinal (Lichtenstein) Hernia Repair: a Systematic Review and Meta-Analysis. Surgery (2020) 167:581–9. 10.1016/j.surg.2019.08.021 [DOI] [PubMed] [Google Scholar]
- 5. Bakker WJ, Aufenacker TJ, Boschman JS, Burgmans JPJ. Heavyweight Mesh Is superior to Lightweight Mesh in Laparo-Endoscopic Inguinal Hernia Repair: a Meta-Analysis and Trial Sequential Analysis of Randomized Controlled Trials. Ann Surg (2021) 273:890–9. 10.1097/SLA.0000000000003831 [DOI] [PubMed] [Google Scholar]
- 6. Tricco AC, Lillie E, Zarin W, O’Brian KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med (2018) 169:467–73. 10.7326/M18-0850 [DOI] [PubMed] [Google Scholar]
- 7. OSF Protocol. OSF Registration of a Scoping Review (2022). Available from: https://osf.io/rhm8n (Accessed October 30, 2022). [Google Scholar]
- 8. Greenhalgh T, Peacock R. Effectiveness and Efficiency of Search Methods in Systematic Reviews of Complex Evidence: Audit of Primary Sources. BMJ (2005) 331:1064–5. 10.1136/BMJ.38636.593461.68 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Prakash P, Bansal V, Misra M, Babu D, Sagar R, Krishna A, et al. A Prospective Randomised Controlled Trial Comparing Chronic Groin Pain and Quality of Life in Lightweight versus Heavyweight Polypropylene Mesh in Laparoscopic Inguinal Hernia Repair. J Minim Access Surg (2016) 12:154–61. 10.4103/0972-9941.170018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Aguilar-García J, Villafuerte-Fernandez R, Ntezes-Hidalgo PI, Meade-Aguilar JA, Ramirez-GarciaLuna JL, Martinez-Jimenez MA. Postoperative Inguinal Pain and Disability after Lichtenstein versus ONSTEP Hernia Repair: Analysis of Responses to the Inguinal Pain Questionnaire in Spanish. Surg Today (2021) 51:703–12. 10.1007/s00595-020-02155-8 [DOI] [PubMed] [Google Scholar]
- 11. Nikkolo C, Vaasna T, Murruste M, Suumann J, Ü K, Seepter H, et al. Three-year Results of a Randomized Study Comparing Self-Gripping Mesh with Sutured Mesh in Open Inguinal Hernia Repair. J Surg Res (2017) 209:139–44. 10.1016/j.jss.2016.10.010 [DOI] [PubMed] [Google Scholar]
- 12. Molegraaf MJ, Grotenhuis B, Torensma B, de Ridder V, Lange JF, Swank DJ, et al. The HIPPO Trial, a Randomized Double-Blind Trial Comparing Self-Gripping Parietex Progrip Mesh and Sutured Parietex Mesh in Lichtenstein Hernioplasty: A Long-Term Follow-Up Study. Ann Surg (2017) 266:939–45. 10.1097/SLA.0000000000002169 [DOI] [PubMed] [Google Scholar]
- 13. Hoyuela C, Juvany M, Carvajal F, Veres A, Troyano D, Trias M, et al. Randomized Clinical Trial of Mesh Fixation with Glue or Sutures for Lichtenstein Hernia Repair. Br J Surg (2017) 104:688–94. 10.1002/bjs.10488 [DOI] [PubMed] [Google Scholar]
- 14. Nikkolo C, Vaasna T, Murruste M, Seepter H, Kirsimägi Ü, Lepner U. Three-year Results of a Single-centre Single-Blinded Randomised Study Evaluating the Impact of Mesh Pore Size on Chronic Pain after Lichtenstein Hernioplasty. Scand J Surg (2016) 105:141–6. 10.1177/1457496915620311 [DOI] [PubMed] [Google Scholar]
- 15. Smeds S, Nienhuijs S, Kullman E, Sanders DL, Lehnert T, Ziprin P, et al. Identification and Management of the Ilio-Inguinal and Ilio-Hypogastric Nerves in Open Inguinal Hernia Repair: Benefits of Self-Gripping Mesh. Hernia (2016) 20:33–41. 10.1007/s10029-015-1372-7 [DOI] [PubMed] [Google Scholar]
- 16. Löfgren J, Nordin P, Ibingira C, Matovu A, Galiwango E, Wladis A. A Randomized Trial of Low-Cost Mesh in Groin Hernia Repair. N Engl J Med (2016) 374:146–53. 10.1056/NEJMoa1505126 [DOI] [PubMed] [Google Scholar]
- 17. Rönkä K, Vironen J, Kössi J, Hulmi T, Silvester S, Hakal T, et al. Randomized Multicenter Trial Comparing Glue Fixation, Self-Gripping Mesh, and Suture Fixation of Mesh in Lichtenstein Hernia Repair (FinnMesh Study). Ann Surg (2015) 262:714–9. 10.1097/SLA.0000000000001458 [DOI] [PubMed] [Google Scholar]
- 18. Nikkolo C, Vaasna T, Murruste M, Seepter H, Suumann J, Tein A, et al. Single-center, Single-Blinded, Randomized Study of Self-Gripping versus Sutured Mesh in Open Inguinal Hernia Repair. J Surg Res (2015) 194:77–82. 10.1016/j.jss.2014.09.017 [DOI] [PubMed] [Google Scholar]
- 19. Sanders DL, Nienhuijs S, Ziprin P, Miserez M, Gingell-Littlejohn M, Smeds S. Randomized Clinical Trial Comparing Self-Gripping Mesh with Suture Fixation of Lightweight Polypropylene Mesh in Open Inguinal Hernia Repair. Br J Surg (2014) 101:1373–82. 10.1002/bjs.9598 [DOI] [PubMed] [Google Scholar]
- 20. Nikkolo C, Vaasna T, Murruste M, Seepter H, Kirsimägi Ü, Lepner U. Randomized Clinical Study Evaluating the Impact of Mesh Pore Size on Chronic Pain after Lichtenstein Hernioplasty. J Surg Res (2014) 191:311–7. 10.1016/j.jss.2014.04.022 [DOI] [PubMed] [Google Scholar]
- 21. Koning GG, de Vries J, Borm GF, Koeslag L, Vriens PW, van Laarhoven CJ, et al. Health Status One Year after Transinguinal Preperitoneal Inguinal Hernia Repair and Lichtenstein’s Method: an Analysis Alongside a Randomized Clinical Study. Hernia (2013) 17:299–306. 10.1007/s10029-012-0963-9 [DOI] [PubMed] [Google Scholar]
- 22. Canonico S, Benevento R, Perna G, Guerniero R, Sciaudone G, Pellino G, et al. Sutureless Fixation with Fibrin Glue of Lightweight Mesh in Open Inguinal Hernia Repair: Effect on Postoperative Pain: a Double-Blind, Randomized Trial versus Standard Heavyweight Mesh. Surgery (2013) 153:126–30. 10.1016/j.surg.2012.06.024 [DOI] [PubMed] [Google Scholar]
- 23. Pierides G, Scheinin T, Remes V, Hermunen K, Vironen J. Randomized Comparison of Self-Fixating and Sutured Mesh in Open Inguinal Hernia Repair. Br J Surg (2012) 99:630–6. 10.1002/bjs.8705 [DOI] [PubMed] [Google Scholar]
- 24. Kingsnorth A, Gingell-Littlejohn M, Nienhuijs S, Schüle S, Appel P, Ziprin P, et al. Randomized Controlled Multicenter International Clinical Trial of Self-Gripping ParietexTM ProGripTM Polyester Mesh versus Lightweight Polypropylene Mesh in Open Inguinal Hernia Repair: Interim Results at 3 Months. Hernia (2012) 16:287–94. 10.1007/s10029-012-0900-y [DOI] [PubMed] [Google Scholar]
- 25. Shen Y, Sun W, Chen J, Liu S, Wang M. NBCA Medical Adhesive (N-butyl-2-cyanoacrylate) versus Suture for Patch Fixation in Lichtenstein Inguinal Herniorrhaphy: a Randomized Controlled Trial. Surgery (2012) 151:550–5. 10.1016/j.surg.2011.09.031 [DOI] [PubMed] [Google Scholar]
- 26. Paajanen H, Kössi J, Silvasti S, Hulmi T, Hakal T, Sanders DL, et al. Randomized Clinical Trial of Tissue Glue versus Absorbable Sutures for Mesh Fixation in Local Anaesthetic Lichtenstein Hernia Repair. Br J Surg (2011) 98:1245–51. 10.1002/bjs.7598 [DOI] [PubMed] [Google Scholar]
- 27. Śmietański M, Bury K, Śmietańska IA, Owczuk R, Paradowski T, Polish Hernia Study Group. Five-year Results of a Randomised Controlled Multi-centre Study Comparing Heavy-Weight Knitted versus Low-Weight, Non-woven Polypropylene Implants in Lichtenstein Hernioplasty. Hernia (2011) 15:495–501. 10.1007/s10029-011-0808-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Isil RG, Avlanmis O. Effects of Totally Extraperitoneal and Lichtenstein Hernia Repair on Men's Sexual Function and Quality of Life. Surg Endosc (2020) 34:1103–11. 10.1007/s00464-019-06857-0 [DOI] [PubMed] [Google Scholar]
- 29. Fouda E, Thabet W, Elsaid M, Emile S, Elbaz S. A Randomized Clinical Trial of Mesh Fixation with Cyanoacrylate Glue Compared to Sutures in Inguinal Hernia Repair. Int J Abdom Wall Hernia Surg (2020) 3:56. 10.4103/ijawhs.ijawhs_4_20 [DOI] [Google Scholar]
- 30. Prabhu AS, Carbonell A, Hope W, Warren J, Higgins R, Jacob B, et al. Robotic Inguinal vs Transabdominal Laparoscopic Inguinal Hernia Repair: The RIVAL Randomized Clinical Trial. JAMA Surg (2020) 155:380–7. 10.1001/jamasurg.2020.0034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Rutegård M, Gümüsçü R, Stylianidis G, Nordin P, Nilsson E, Haapamäki MM. Chronic Pain, Discomfort, Quality of Life and Impact on Sex Life after Open Inguinal Hernia Mesh Repair: an Expertise-Based Randomized Clinical Trial Comparing Lightweight and Heavyweight Mesh. Hernia (2018) 22:411–8. 10.1007/s10029-018-1734-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Lee SD, Son T, Lee J-B, Chang YS. Comparison of Partially-Absorbable Lightweight Mesh with Heavyweight Mesh for Inguinal Hernia Repair: Multicenter Randomized Study. Ann Surg Treat Res (2017) 93:322–30. 10.4174/astr.2017.93.6.322 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Burgmans JPJ, Voorbrood CEH, Schouten N, Smakman N, Elias S, Clevers GJ, et al. Three-month Results of the Effect of Ultrapro or Prolene Mesh on post-operative Pain and Well-Being Following Endoscopic Totally Extraperitoneal Hernia Repair (TULP Trial). Surg Endosc (2015) 29:3171–8. 10.1007/s00464-014-4049-x [DOI] [PubMed] [Google Scholar]
- 34. Demetrashvili Z, Khutsishvili K, Pipia I, Kenchadze G, Ekaladze E. Standard Polypropylene Mesh vs Lightweight Mesh for Lichtenstein Repair of Primary Inguinal Hernia: a Randomized Controlled Trial. Int J Surg (2014) 12:1380–4. 10.1016/j.ijsu.2014.10.025 [DOI] [PubMed] [Google Scholar]
- 35. Chatzimavroudis G, Papaziogas B, Koutelidakis I, Galanis I, Atmatzidis S, Christopoulos P, et al. Lichtenstein Technique for Inguinal Hernia Repair Using Polypropylene Mesh Fixed with Sutures vs. Self-Fixating Polypropylene Mesh: a Prospective Randomized Comparative Study. Hernia (2014) 18:193–8. 10.1007/s10029-013-1211-7 [DOI] [PubMed] [Google Scholar]
- 36. Pielacinski K, Szczepanik AB, Wroblewski T. Effect of Mesh Type, Surgeon and Selected Patients’ Characteristics on the Treatment of Inguinal Hernia with the Lichtenstein Technique. Randomized Trial. Wideochirurgia Inne Tech Maloinwazyjne (2013) 8:99–106. 10.5114/wiitm.2011.32824 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Bury K, Śmietański M, Polish Hernia Study Group. Five-year Results of a Randomized Clinical Trial Comparing a Polypropylene Mesh with a Poliglecaprone and Polypropylene Composite Mesh for Inguinal Hernioplasty. Hernia (2012) 16:549–53. 10.1007/s10029-012-0916-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Pielaciński K, Szczepanik AB, Misiak A, Wróblewski T. Randomized Clinical Trial Comparing Inguinal Hernia Repair with Lichtenstein Technique Using Non-absorbable or Partially Absorbable Mesh. Preliminary Report. Wideochirurgia Inne Tech Maloinwazyjne (2011) 6:190–206. 10.5114/wiitm.2011.26253 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Silvestre AC, de Mathia GB, Fagundes DJ, Medeiros LR, Rosa MI. Shrinkage Evaluation of Heavyweight and Lightweight Polypropylene Meshes in Inguinal Hernia Repair: a Randomized Controlled Trial. Hernia (2011) 15:629–34. 10.1007/s10029-011-0853-6 [DOI] [PubMed] [Google Scholar]
- 40. Peeters E, Spiessens C, Oyen R, De Wever L, Vanderschueren D, Penninckx F, et al. Laparoscopic Inguinal Hernia Repair in Men with Lightweight Meshes May Significantly Impair Sperm Motility: a Randomized Controlled Trial. Ann Surg (2010) 252:240–6. 10.1097/SLA.0b013e3181e8fac5 [DOI] [PubMed] [Google Scholar]
- 41. Chowbey PK, Garg N, Sharma A, Khullar R, Soni V, Baijal M, et al. Prospective Randomized Clinical Trial Comparing Lightweight Mesh and Heavyweight Polypropylene Mesh in Endoscopic Totally Extraperitoneal Groin Hernia Repair. Surg Endosc (2010) 24:3073–9. 10.1007/s00464-010-1092-0 [DOI] [PubMed] [Google Scholar]
- 42. Abbas MH, Hamade A, Choudhry MN, Hamza N, Nadeem R, Ammori BJ. Infiltration of Wounds and Extraperitoneal Space with Local Anesthetic in Patients Undergoing Laparoscopic Totally Extraperitoneal Repair of Unilateral Inguinal Hernias: a Randomized Double-Blind Placebo-Controlled Trial. Scand J Surg (2010) 99:18–23. 10.1177/145749691009900105 [DOI] [PubMed] [Google Scholar]
- 43. Koch A, Bringman S, Myrelid P, Smeds S, Kald A. Randomized Clinical Trial of Groin Hernia Repair with Titanium-Coated Lightweight Mesh Compared with Standard Polypropylene Mesh. Br J Surg (2008) 95:1226–31. 10.1002/bjs.6325 [DOI] [PubMed] [Google Scholar]
- 44. Bringman S, Wollert S, Österberg J, Smedberg S, Granlund H, Heikkinen T-J. Three-year Results of a Randomized Clinical Trial of Lightweight or Standard Polypropylene Mesh in Lichtenstein Repair of Primary Inguinal Hernia. Br J Surg (2006) 93:1056–9. 10.1002/bjs.5403 [DOI] [PubMed] [Google Scholar]
- 45. O’Dwyer PJ, Kingsnorth AN, Molloy RG, Small PK, Lammers B, Horeyseck G. Randomized Clinical Trial Assessing Impact of a Lightweight or Heavyweight Mesh on Chronic Pain after Inguinal Hernia Repair. Br J Surg (2005) 92:166–70. 10.1002/bjs.4833 [DOI] [PubMed] [Google Scholar]
- 46. Post S, Weiss B, Willer M, Neufang T, Lorenz D. Randomized Clinical Trial of Lightweight Composite Mesh for Lichtenstein Inguinal Hernia Repair. Br J Surg (2004) 91:44–8. 10.1002/bjs.4387 [DOI] [PubMed] [Google Scholar]
- 47. Bansal VK, Misra MC, Babu D, Victor J, Kumar S, Sagar R, et al. A Prospective, Randomized Comparison of Long-Term Outcomes: Chronic Groin Pain and Quality of Life Following Totally Extraperitoneal (TEP) and Transabdominal Preperitoneal (TAPP) Laparoscopic Inguinal Hernia Repair. Surg Endosc (2013) 27:2373–82. 10.1007/s00464-013-2797-7 [DOI] [PubMed] [Google Scholar]
- 48. Langenbach MR, Schmidt J, Ubrig B, Zirngibl H. Sixty-month Follow-Up after Endoscopic Inguinal Hernia Repair with Three Types of Mesh: a Prospective Randomized Trial. Surg Endosc (2008) 22:1790–7. 10.1007/s00464-008-9863-6 [DOI] [PubMed] [Google Scholar]
- 49. Langenbach MR, Schmidt J, Zirngibl H. Comparison of Biomaterials in the Early Postoperative Period: Polypropylene Meshes in Laparoscopic Inguinal Hernia Repair. Surg Endosc (2003) 17:1105–9. 10.1007/s00464-002-9167-1 [DOI] [PubMed] [Google Scholar]
- 50. Paajanen H. A Single-Surgeon Randomized Trial Comparing Three Composite Meshes on Chronic Pain after Lichtenstein Hernia Repair in Local Anesthesia. Hernia (2007) 11:335–9. 10.1007/s10029-007-0236-1 [DOI] [PubMed] [Google Scholar]
- 51. Carro JLP, Riu SV, Lojo BR, Latorre L, Garcia MTA, Pardo BA, et al. Randomized Clinical Trial Comparing Low Density versus High Density Meshes in Patients with Bilateral Inguinal Hernia. Am Surg (2017) 83:1352–6. 10.1177/000313481708301217 [DOI] [PubMed] [Google Scholar]
- 52. Yazdankhah Kenary A, Afshin SN, Ahmadi Amoli H, Yagoobi NA, Borjian A, Yagoobi N, et al. Randomized Clinical Trial Comparing Lightweight Mesh with Heavyweight Mesh for Primary Inguinal Hernia Repair. Hernia (2013) 17:471–7. 10.1007/s10029-012-1009-z [DOI] [PubMed] [Google Scholar]
- 53. Nikkolo C, Lepner U, Murruste M, Vaasna T, Seepter H, Tikk T, et al. Randomised Clinical Trial Comparing Lightweight Mesh with Heavyweight Mesh for Inguinal Hernioplasty. Hernia (2010) 14:253–8. 10.1007/s10029-010-0630-y [DOI] [PubMed] [Google Scholar]
- 54. Agarwal BB, Agarwal KA, Mahajan KC. Prospective Double-Blind Randomized Controlled Study Comparing Heavy- and Lightweight Polypropylene Mesh in Totally Extraperitoneal Repair of Inguinal Hernia: Early Results. Surg Endosc (2009) 23:242–7. 10.1007/s00464-008-0188-2 [DOI] [PubMed] [Google Scholar]
- 55. Paradowski T, Olejarz A, Kontny T, Lukasiewicz J, Sledzinski Z, Smietanska I. Polypropylene vs. ePTFE vs. WN Mesh for Lichtenstein Inguinal Hernia Repair—A Prospective Randomized, Double Blind Pilotstudy of One-Year Follow-Up. Wideochirurgia Inne Tech Maloinwazyjne (2009) 4:6–9. [Google Scholar]
- 56. Bittner R, Leibl BJ, Kraft B, Schwarz J. One-year Results of a Prospective, Randomised Clinical Trial Comparing Four Meshes in Laparoscopic Inguinal Hernia Repair (TAPP). Hernia (2011) 15:503–10. 10.1007/s10029-011-0810-4 [DOI] [PubMed] [Google Scholar]
- 57. Paajanen H, Rönkä K, Laurema A. A Single-Surgeon Randomized Trial Comparing Three Meshes in Lichtenstein Hernia Repair: 2- and 5-year Outcome of Recurrences and Chronic Pain. Int J Surg (2013) 11:81–4. 10.1016/j.ijsu.2012.11.020 [DOI] [PubMed] [Google Scholar]
- 58. Rutegård M, Lindqvist M, Svensson J, Nordin P, Haapamäki MM. Chronic Pain after Open Inguinal Hernia Repair: Expertise-Based Randomized Clinical Trial of Heavyweight or Lightweight Mesh. Br J Surg (2021) 108:138–44. 10.1093/bjs/znaa049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Bittner R, Schmedt C-G, Leibl BJ, Schwarz J. Early Postoperative and One Year Results of a Randomized Controlled Trial Comparing the Impact of Extralight Titanized Polypropylene Mesh and Traditional Heavyweight Polypropylene Mesh on Pain and Seroma Production in Laparoscopic Hernia Repair (TAPP). World J Surg (2011) 35:1791–7. 10.1007/s00268-011-1148-x [DOI] [PubMed] [Google Scholar]
- 60. Bakker WJ, Roos MM, Kerkman T, Burgmans JPJ. Experience with the PINQ-PHONE Telephone Questionnaire for Detection of Recurrences after Endoscopic Inguinal Hernia Repair. Hernia (2019) 23:685–91. 10.1007/s10029-019-01909-9 [DOI] [PubMed] [Google Scholar]
- 61. Matikainen M, Aro E, Vironen J, Kössi J, Hulmi T, Silvasti S, et al. Factors Predicting Chronic Pain after Open Inguinal Hernia Repair: a Regression Analysis of Randomized Trial Comparing Three Different Meshes with Three Fixation Methods (FinnMesh Study). Hernia (2018) 22:813–8. 10.1007/s10029-018-1772-6 [DOI] [PubMed] [Google Scholar]
- 62. Roos M, Bakker WJ, Schouten N, Voorbrood C, Clevers GJ, Verleisdonk EJ, et al. Higher Recurrence Rate after Endoscopic Totally Extraperitoneal (TEP) Inguinal Hernia Repair with Ultrapro Lightweight Mesh: 5-year Results of a Randomized Controlled Trial (TULP-Trial). Ann Surg (2018) 268:241–6. 10.1097/SLA.0000000000002649 [DOI] [PubMed] [Google Scholar]
- 63. Matikainen M, Vironen J, Kössi J, Hulmi T, Hertsi M, Rantanen T, et al. Impact of Mesh and Fixation on Chronic Inguinal Pain in Lichtenstein Hernia Repair: 5-year Outcomes from the Finn Mesh Study. World J Surg (2021) 45:459–64. 10.1007/s00268-020-05835-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Miller BT, Prabhu AS, Petro CC, Beffa LRA, Carbonell AM, Hope W, et al. Laparoscopic versus Robotic Inguinal Hernia Repair: 1- and 2-year Outcomes from the RIVAL Trial. Surg Endosc (2022) 37:723–8. 10.1007/s00464-022-09320-9 [DOI] [PubMed] [Google Scholar]
- 65. Burgmans JPJ, Voorbrood CEH, Simmermacher RKJ, Schouten N, Smakman N, Clevers G, et al. Long-term Results of a Randomized Double-Blinded Prospective Trial of a Lightweight (Ultrapro) versus a Heavyweight Mesh (Prolene) in Laparoscopic Total Extraperitoneal Inguinal Hernia Repair (TULP-Trial). Ann Surg (2016) 263:862–6. 10.1097/SLA.0000000000001579 [DOI] [PubMed] [Google Scholar]
- 66. Peeters E, Spiessens C, Oyen R, De Wever L, Vanderschueren D, Pennickx F, et al. Sperm Motility after Laparoscopic Inguinal Hernia Repair with Lightweight Meshes: 3-year Follow-Up of a Randomised Clinical Trial. Hernia (2014) 18:361–7. 10.1007/s10029-012-1028-9 [DOI] [PubMed] [Google Scholar]
- 67. Nikkolo C, Murruste M, Vaasna T, Seepter H, Tikk T, Lepner U. Three-year Results of Randomised Clinical Trial Comparing Lightweight Mesh with Heavyweight Mesh for Inguinal Hernioplasty. Hernia (2012) 16:555–9. 10.1007/s10029-012-0951-0 [DOI] [PubMed] [Google Scholar]
- 68. Morrison A, Polisena J, Husereau D, Moulton K, Clark M, Fiander M, et al. The Effect of English-language Restriction on Systematic Review-Based Meta-Analyses: a Systematic Review of Empirical Studies. Int J Technol Assess Health Care (2012) 28:138–44. 10.1017/S0266462312000086 [DOI] [PubMed] [Google Scholar]
- 69. Earle DB, Mark LA. Prosthetic Material in Inguinal Hernia Repair: How Do I Choose? Surg Clin North Am (2008) 88:179–201. 10.1016/J.SUC.2007.11.002 [DOI] [PubMed] [Google Scholar]
- 70. Coda A, Lamberti R, Martorana S. Classification of Prosthetics Used in Hernia Repair Based on Weight and Biomaterial. Hernia (2012) 16:9–20. 10.1007/S10029-011-0868-Z [DOI] [PubMed] [Google Scholar]