

Abstract
Indirect blood pressure measurements were compared in 28 conscious cats using Doppler and oscillometric blood pressure-measuring devices. Ten cats were used to compare Doppler measurements between two examiners and 18 cats were used to compare Doppler and oscillometric measurements. The Doppler machine obtained systolic and diastolic blood pressure readings in 100% and 51% of attempts, respectively. With the oscillometric machine, systolic and diastolic blood pressure readings were obtained in 52% of the attempts. With the Doppler, measures of mean systolic blood pressure between two examiners were positively correlated, but there was no correlation for diastolic blood pressure measures. When comparing the results obtained by Doppler and oscillometric machines there was no significant difference between mean systolic blood pressure readings, but the oscillometric machine produced significantly higher estimates of diastolic blood pressure. In both cases, the standard deviations for the oscillometric machine were considerably larger than those for the Doppler machine. The first reading of systolic blood pressure obtained with the Doppler machine was an excellent predictor of the mean of five readings, but this was not so for the oscillometric machine. It took less than 5 min to obtain five readings in 37.5% of cases with the Doppler machine but this was true for only 5% of cases with the oscillometric machine. Two cats with ophthalmological lesions consistent with systemic hypertension were identified. In these two patients, systolic blood pressure measurements were between 200 and 225 mmHg when measured by Doppler, and between 140 and 150 mmHg when measured by the oscillometric machine. This suggests that a lower reference range for normal systolic blood pressure values should be used for the oscillometric device.
The clinical importance of feline systemic hypertension is increasingly recognised in veterinary practice. Target organs of systemic hypertension include the kidney, heart, brain and eye. The pathological expression of systemic hypertension within these structures can be considerable and irreversible, and includes glomerular sclerosis and interstitial fibrosis, hypertrophy of the left ventricle, intracranial haemorrhage and retinal detachment. Because of these potentially irreversible effects, it is important that systemic hypertension is diagnosed early in the course of the disease.
Most cases of feline hypertension are thought to be secondary. Chronic renal failure followed by hyperthyroidism currently represents the most common cause of hypertension in published studies (Kobayashi et al 1990, Littman 1994, Sansom et al 1994, Stiles et al 1994, Maggio et al 2000, Syme et al 2002, Chetboul et al 2003) but other diseases associated with hypertension include primary hyperaldosteronism (Flood et al 1999, Maggio et al 2000), hyperadrenocorticism (Hoenig 2002), chronic anaemia (Morgan 1986), diabetes mellitus (Littman 1994, Maggio et al 2000, Chetboul et al 2003) and erythropoietin therapy (Cowgill et al 1998). Prevalence figures for systemic hypertension vary in published studies, ranging from 20 to 65% of cats with chronic renal failure (Kobayashi et al 1990, Stiles et al 1994, Syme et al 2002).
Important requirements of a blood pressure (BP) measuring device for routine use in conscious cats are the accuracy of the machine and its ease of use. Most devices available for use in veterinary practice are non-invasive and indirect, measuring BP by means of a cuff placed on a limb or base of the tail. Classes of non-invasive indirect BP devices that are currently available are Doppler ultrasonographic, oscillometric sphygnomanometric and photoplethysmographic machines (Grandy et al 1992, Binns et al 1995, Branson et al 1997, Caulkett et al 1998, Pedersen et al 2002).
We compared Doppler and oscillometric machines in a clinical setting using two veterinary models that are currently available in the UK. As direct BP measurements could not be performed as a control we could not measure the accuracy of either machine. However, we aimed to determine the ease of use of each machine, in particular the repeatability of consecutive readings, inter-operator variability of readings, the time required to obtain a BP measurement and the ability of the patient to tolerate the device.
Materials and methods
The study was carried out at the Small Animal Hospital, Department of Clinical Veterinary Science, University of Bristol. In total, 28 cats were used in the study. These comprised hospital in-patient cats and healthy cats belonging to members of staff. Any cat that had been anaesthetised or sedated within a 12-h period and any cat on medication that is known to affect blood pressure was excluded. All BP measurements were performed in the same room and by the same two examiners. Prior to commencement of BP measurements, each cat was given a 10-min ‘acclimatisation period’ with the aim of reducing stress-induced hypertension (the ‘white coat effect’) (Belew et al 1999, Sparkes et al 1999). Heart rate was measured at the end of the acclimatisation period and again at the end of the period of BP measurement.
Indirect BP measurements were taken using Doppler (CAT Doppler, Thames Medical, UK) and oscillometric (Memoprint, S+B medVET, GmbH, Germany) machines. A single Doppler machine and a single oscillometric machine were used throughout the study. Doppler and oscillometric cuffs were placed on the forelimb according to the manufacturer's instructions (beneath the elbow for Doppler measurements and above the elbow for oscillometric measurements). For each cat, a cuff width of between 30 and 40% of the limb circumference was chosen (Grandy et al 1992, Henik 1997, Sparkes et al 1999).
Initially, 10 cats were used to determine whether mean Doppler readings were comparable between two different examiners. For each of the 10 cats, five consecutive BP measurements (systolic and diastolic) were recorded in quick succession by one of the two examiners. The Doppler probe was placed over the common digital branch of the radial artery on the palmar aspect of the foot. The hair was not clipped before placement of the probe. Aqueous gel (Ultrasonic free conductivity gel, Pharmaceutical Innovations Inc) was placed between the probe and the skin to improve ultrasonic contact, and the volume of the Doppler machine was adjusted to obtain a clearly audible signal. The cuff was inflated until flow sounds were no longer audible, and then gradually deflated until clear flow sounds became audible. The manometer reading at the reappearance of flow sounds was recorded as the systolic BP. The cuff was deflated further until a change in tone of the flow sound was noted, becoming lower pitched or ‘muffled’. The manometer reading at the change in tone of flow sounds was recorded as the diastolic BP (Binns et al 1995).
The second examiner, who was ‘blinded’ to the results of the first examiner, then repeated the procedure following a 5-min rest period. For each cat, the order of the first and second examiner was decided randomly.
In the second part of the study, 18 cats were used to directly compare Doppler and oscillometric machines. The order in which Doppler and oscillometric measures were taken was decided randomly for each cat. Doppler measurements were performed as described above. The time taken to obtain five consecutive BP readings was recorded. If five readings could not be obtained over 10 attempts, the procedure was abandoned and the reason for failure was recorded. Following a 5-min rest period the procedure was repeated, this time by the second examiner. Again, the order of the first and second examiner was decided randomly.
The oscillometric machine gives automated systolic and diastolic pressure readings that do not require subjective interpretation by the operator. Following cuff placement, five systolic and diastolic BP measurements were attempted. As with the Doppler machine, if five readings could not be obtained over 10 attempts, the procedure was abandoned and the reason for failure was recorded.
Ocular fundus examination was performed on all cats. At the start of the acclimatisation period, a single drop of tropicamide 1% (Mydriacyl; Alcon, UK) was placed in both eyes of the cat under study. Indirect and direct ophthalmoscopy was performed between 30 and 60 min later. One examiner performed all fundus examinations.
Wilcoxon's signed rank test was used to compare Doppler systolic and diastolic BP measurements taken by the two examiners on the same cats, and also to compare the same examiner's readings on the same cat using both types of machine. Spearman rank correlation coefficients were calculated to examine the correlation between the examiners' measurements of systolic and diastolic BP in both the sample of 10 cats and the sample of 18 cats using the Doppler machine. They were also used to compare the examiners' measurements using the Doppler machine with those made by the oscillometric machine, and to evaluate the correlation between the first measure made by each machine and the mean of five measures.
Results
Consistency of Doppler measurements between examiners
Ten cats were used to investigate whether Doppler readings were comparable between examiners. There was no significant difference between mean systolic BP measurements obtained by the two examiners (Wilcoxon's T=38.0, n=10, P=0.308), and these measures were significantly positively correlated across the 10 cats (Spearman rs=0.673, n=10, P=0.033). There was a significant difference between mean diastolic BP measurements (Wilcoxon's T=0, n=10, P=0.014). One examiner recorded a consistently higher diastolic BP than the other. Furthermore, there was no significant correlation between the examiners' measurement of diastolic BP across the 10 cats (Spearman rs=0.521, n=10, P=0.186).
Comparison of Doppler and oscillometric machines
BP measurements were performed on 18 cats using both Doppler and oscillometric machines. For each cat, the order of the Doppler and oscillometric examination was decided randomly. Sample sizes vary in the following analyses according to the number of cats for which data were successfully collected on each measure.
Effectiveness of Doppler and oscillometric machines
Combining the data from both examiners, with five attempts each for all 28 cats in the study, the Doppler machine gave a systolic BP reading in 280/280 attempts (100%). Diastolic BP readings were determined in 144/280 attempts (51.4%). It was not possible to obtain diastolic BP readings in the remaining attempts because the examiners were unable to detect a clear change from systolic to diastolic tone.
The oscillometric machine is automated and gives both systolic and diastolic readings simultaneously. A maximum of 10 attempts were allowed for the oscillometric machine to obtain five results. However, the machine did not always require the full 10 attempts and once five readings had been obtained the procedure was terminated. Thus, systolic and diastolic readings were obtained in 115/223 attempts (52%).
Comparison of mean systolic and diastolic BP values between Doppler and oscillometric machines
There was no significant difference in the mean systolic BP between the Doppler and oscillometric machines (examiner 1: Wilcoxon's T=86, n=16, P=0.3755; examiner 2: Wilcoxon's T=62, n=16, P=0.782). However, the standard deviation for the oscillometric machine was considerably larger than those for both operators using the Doppler machine (Fig 1). Both examiners showed good agreement in their Doppler estimates of systolic BP (rs=0.553, n=16, P=0.017), as they did in the initial study of 10 cats. However, only one examiner's Doppler measurements of systolic BP correlated with the oscillometric measurements across cats (rs=0.516, n=16, P=0.041), while the other examiner's Doppler measurements were not correlated with the oscillometric measurements (rs=0.352, n=16, P=0.181).
Fig 1.
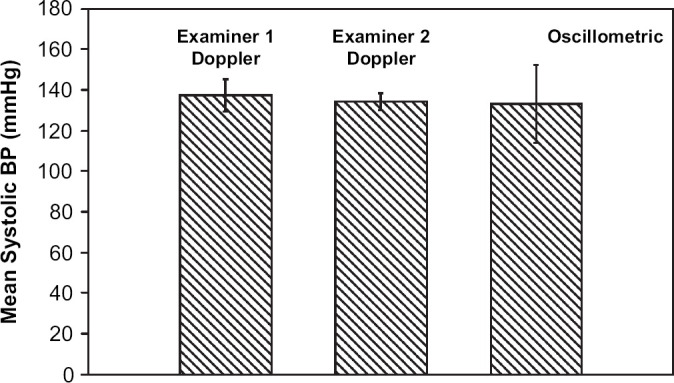
Graph showing mean systolic BP and standard deviation for examiners 1 and 2 and oscillometric machine.
When the same analysis was performed for mean diastolic BP there was a significant difference between the Doppler and oscillometric machines (examiner 1: Wilcoxon's T=1, n=11, P=0.002; examiner 2: Wilcoxon's T=2, n=14, P=0.0004). The oscillometric machine tended to measure a higher diastolic BP (Fig 2). Again, the standard deviations for the oscillometric machine were considerably larger than those for both operators using the Doppler machine (Fig 2). Furthermore, the Doppler measures of diastolic BP were not correlated with the oscillometric measures across cats for either examiner (examiner 1: rs=−0.200, n=11, P=0.533; examiner 2: rs=0.120, n=14, P=0.671), and neither were the Doppler measures of the two examiners (rs=0.053, n=14, P=0.856).
Fig 2.

Graph showing mean diastolic BP and standard deviation for examiners 1 and 2 and oscillometric machine.
Use of first reading as a predictor of mean systolic and diastolic BP
We aimed to determine whether the first BP measurement was an accurate predictor of the mean of five BP readings. For systolic BP measurement using the Doppler machine, there was a strong correlation between the first reading and the mean of five readings, for both operators (Fig 3a and b) (examiner 1: rs=0.939, n=18, P<0.001; examiner 2: rs=0.938, n=18, P<0.001). There was also no overall difference between the estimated systolic BP from the first measurement and from the mean of five measurements (examiner 1: Wilcoxon's T=114.5, n=18, P=0.228; examiner 2: Wilcoxon's T=113, n=18, P=0.2462). For diastolic BP insufficient data were available for the comparison of the first reading and mean of five. For the oscillometric machine there was no significant correlation between the first reading of systolic BP and the mean of five (rs=0.409, n=11, P=0.212; Fig 4), and there was no overall difference between these two measurements (Wilcoxon's T=41, n=11, P=0.5195).
Fig 3.

(a) Graph comparing first systolic BP reading with the mean of five systolic BP readings for examiner 1 (Doppler machine). (b) Graph comparing first systolic BP reading with the mean of five systolic BP readings for examiner 2 (Doppler machine).
Fig 4.

Graph comparing first systolic BP reading with the mean of five systolic BP readings (oscillometric machine).
Time taken to perform five BP measurements
Using the Doppler machine, examiners 1 and 2 were able to perform five readings within 5 min in 35.7% and 39.3% of cases, respectively. The oscillometric machine performed five readings within 5 min in only 5% of cases, and in 55% of cases it took greater than 10 min.
Ocular fundus examination
Two of the 28 cats had lesions consistent with active hypertensive chorioretinopathy (multiple bullous retinal detachments, intra-retinal haemorrhage, superficial retinal blood vessel tortuosity). Both these cats had mean systolic blood pressure measurements greater than 200 mmHg when measured by Doppler by both examiners (examiner 1 recorded mean systolic BP values of 212 mmHg and 207 mmHg, respectively; examiner 2 recorded values of 201 mmHg and 224 mmHg, respectively). In contrast, the oscillometric machine measured mean systolic BP in these two cats as 141 mmHg and 149 mmHg, respectively.
Discussion
We were able to record a systolic BP reading in 100% of attempts using the Doppler machine. Although the technique required some user skill this was learned quickly, and the systolic BP measurements could thereafter be obtained efficiently. Interestingly, the first systolic BP measurement was not significantly different from the mean of five readings, indicating that a single systolic BP reading obtained by the Doppler machine may be as reliable as the mean of a series of readings (Fig 3a, b). Furthermore, there was no significant difference between mean systolic BP readings recorded by two different examiners. Diastolic BP readings using the Doppler machine were less easily obtained and we were only able to obtain a reading in 51.4% of attempts. Furthermore, mean diastolic BP readings between two examiners were statistically different, implying that the diastolic BP measurement may not be reliable. Identification of diastolic BP using the Doppler device is more subjective than detection of systolic BP, because it relies on determination of a shift in audible tone. In contrast, systolic BP measurement relies on the appearance of an audible tone, which is easier to identify.
Using the oscillometric machine, which records systolic and diastolic BP simultaneously, we were successful in 52% of attempts. The oscillometric device required cuff placement above the elbow, and some cats tolerated this poorly. In addition, the oscillometric machine required that the cat remain still throughout the procedure, which in more than half of all attempts took longer than 10 min to complete. This could influence the choice of machines in a clinical setting. An advantage of the oscillometric device compared to the Doppler was that it required minimal skill and did not rely on interpretation of sounds by the operator.
Comparing results obtained between Doppler and oscillometric machines, we found no significant difference between mean systolic BP readings. However, plots of the data showed that the standard deviation for the oscillometric machine was considerably higher than that for the Doppler machine (Fig 1). Thus, despite mean values being comparable between machines, there was a greater variability in the individual oscillometric data points. Therefore, it is recommended that when using the oscillometric method an average of five readings should be obtained. With regards to the diastolic BP measurements, there was a statistically significant difference between the two devices, with the oscillometric machine giving higher readings (Fig 2). Again, the standard deviation for the oscillometric machine was considerably higher than that for the Doppler machine (Fig 2).
All cats underwent ocular fundus examination using direct and indirect ophthalmoscopy. Two of the cats showed ocular fundus changes consistent with systemic hypertensive disease (bilateral, multifocal bullous retinal detachments and superficial retinal blood vessel tortuosity (Crispin and Mould 2001)). In each case (and for both examiners, who were unaware of the ocular fundus abnormalities) the Doppler machine measured systolic BP as greater than 200 mmHg, whereas the oscillometric device measured systolic BP as between 140 mmHg and 150 mmHg for each cat. Although direct BP measurements were not performed on these two cats, the characteristic ophthalmological changes were highly suggestive of systemic hypertension. This suggests that a lower reference range for normal systolic blood pressure values in cats should be used for the Memoprint oscillometric device. This finding is in agreement with another study that suggested a normal reference range of 109–137 mmHg in cats when using the Memoprint device (Curtet et al 2001).
There were a number of limitations to our study including the small population size and the possibility of an improvement over time in both taking the measurements and in cat handling ability. Another major limitation was the use of a single machine for evaluating each method. Ideally, we would have tested a number of Doppler machines against a number of oscillometric machines, but for practical reasons this was beyond the limitations of our study.
Our sample contained many cats undergoing treatment at the hospital. We had no control over such treatments or the procedures that were performed before our investigation and these factors may have influenced BP, although we took care to exclude cats that were on medication known to affect blood pressure, and cats that had been sedated or anaesthetised within the previous 12 h. Most importantly, we were unable to undertake direct BP readings and, therefore, cannot qualify the accuracy of our results throughout this study.
In conclusion, we found the Doppler machine superior to the oscillometric machine for measuring systolic BP in cats, in terms of ease of use and repeatability of results, and speed of use and diagnosis of systemic hypertension.
Acknowledgements
The authors would like to acknowledge the help of Dr S. H. Binns and the staff of the Small Animal Hospital, Department of Clinical Veterinary Science, University of Bristol, in particular Ms Maud van de Stadt. We are grateful to the manufacturers of the blood pressure devices for the loan of their machines.
References
- Belew A.M., Barlett T., Brown S.A. Evaluation of the white coat effect in cats, Journal of Veterinary Internal Medicine 13, 1999, 134–142. [DOI] [PubMed] [Google Scholar]
- Binns S.H., Sisson D., Buoscio D.A., Schaeffer D.J. Doppler ultrasonographic, oscillometric sphygmomanometric and photoplethysmographic techniques for non-invasive blood pressure measurement in anaesthetised cats, Journal of Veterinary Internal Medicine 9 (6), 1995, 405–414. [DOI] [PubMed] [Google Scholar]
- Branson K.R., Wagner-Mann C.C., Mann F.A. Evaluation of an oscillometric blood pressure monitor on anaesthetised cats and the effect of cuff placement and fur on accuracy, Veterinary Anaesthesia 26, 1997, 347–353. [DOI] [PubMed] [Google Scholar]
- Caulkett N.A., Cantwell S.L., Houston D.M. A comparison of indirect blood pressure monitoring techniques in the anaesthetised cat, Veterinary Anaesthesia 27, 1998, 370–377. [DOI] [PubMed] [Google Scholar]
- Chetboul V., Lefebvre H.P., Pinhas C., Clerc B., Boussouf M., Pouchelon J.L. Spontaneous feline hypertension: clinical and echocardiographic abnormalities, and survival rate, Journal of Veterinary Internal Medicine 17 (1), 2003, 89–95. [DOI] [PubMed] [Google Scholar]
- Cowgill L.D., James K.M., Levy J.K., Browne J.K., Miller A., Lobingier R.T., Egrie J.C. Use of recombinant human erythropoietin for management of anemia in dogs and cats with renal failure, Journal of the American Veterinary Medical Association 212 (4), 1998, 521–528. [PubMed] [Google Scholar]
- Crispin S.M., Mould J.R.B. Systemic hypertensive disease and the feline fundus, Veterinary Ophthalmology 4 (2), 2001, 131–140. [DOI] [PubMed] [Google Scholar]
- Curtet J.D., Busato A., Lombard C.W. The use of memoprint in the cat, Schweizer Archiv fur Tierheilkunde 143, 2001, 241–247. [PubMed] [Google Scholar]
- Flood S.M., Randolph J.F., Gelzer A.R., Refsal K. Primary hyperaldosteronism in two cats, Journal of the American Animal Hospital Association 35 (5), 1999, 411–416. [DOI] [PubMed] [Google Scholar]
- Grandy J.L., Dunlop C.I., Hodgson D.S., Curtis C.R., Chapman P.L. Evaluation of the Doppler ultrasonic method of measuring systolic arterial blood pressure in cats, American Journal of Veterinary Research 53 (7), 1992, 1166–1169. [PubMed] [Google Scholar]
- Henik R.A. Diagnosis and treatment of feline systemic hypertension, Compendium of Continuing Education in Veterinary Practice 19, 1997, 163–178. [Google Scholar]
- Hoenig M. Feline hyperadrenocorticism – where are we now?, Journal of Feline Medicine and Surgery 4, 2002, 171–174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kobayashi D.L., Peterson M.E., Graves T.K., Lesser M., Nichols C.E. Hypertension in cats with chronic renal failure or hyperthyroidism, Journal of Veterinary Internal Medicine 4 (2), 1990, 58–61. [DOI] [PubMed] [Google Scholar]
- Littman M.P. Spontaneous systemic hypertension in 24 cats, Journal of Veterinary Internal Medicine 8 (2), 1994, 79–86. [DOI] [PubMed] [Google Scholar]
- Maggio F., Defrancesco T.C., Atkins C.E., Pizzirani S., Gilger B.V., Davidson M.G. Ocular lesions associated with systemic hypertension in cats: 69 cases (1985–1998), Journal of American Veterinary Medical Association 217, 2000, 695–702. [DOI] [PubMed] [Google Scholar]
- Morgan R.V. Systemic hypertension in four cats: ocular and medical findings, Journal of American Animal Hospital Association 22, 1986, 615–621. [Google Scholar]
- Pedersen K.M., Butler M.A., Ersboll A.K., Pedersen H.D. Evaluation of an oscillometric blood pressure monitor for use in anaesthetised cats, Journal of American Veterinary Medical Association 221, 2002, 646–650. [DOI] [PubMed] [Google Scholar]
- Sansom J., Barnett K.C., Dunn K.A., Smith K.C., Dennis R. Ocular disease associated with hypertension in 16 cats, Journal of Small Animal Practice 35, 1994, 604–611. [Google Scholar]
- Sparkes A.H., Caney S.M.A., King M.K.A., Gruffydd-Jones T.J. Inter- and intraindividual variability in indirect (Doppler) systolic blood pressure measurements in cats, Journal of Veterinary Internal Medicine 13, 1999, 314–318. [DOI] [PubMed] [Google Scholar]
- Stiles J., Polzin D.J., Bistner S.I. The prevalence of retinopathy in cats with systemic hypertension and chronic renal failure or hyperthyroidism, Journal of the American Animal Hospital Association 30, 1994, 564–572. [Google Scholar]
- Syme H.M., Barber P.J., Markwell P.J., Elliott J. Prevalence of systolic hypertension in cats with chronic renal failure at initial evaluation, Journal of the American Veterinary Medical Association 220 (12), 2002, 1799–1804. [DOI] [PubMed] [Google Scholar]