

Abstract
Tracheal diameter can be assessed from a thoracic radiograph, with assessment of tracheal diameter in dogs based on ratios between tracheal diameter and a skeletal measurement. Reference intervals are not, however, available for the cat. Tracheal narrowing may cause significant clinical problems, although tracheal hypoplasia in dogs may be clinically silent, and is rarely reported in cats (both mesati- and brachycephalic). The tracheal diameter and trachea:thoracic inlet and trachea:rib ratios were calculated for populations of domestic shorthair (DSH) (n = 68) and Persian (n = 40) cats. This gave reference intervals for radiographic tracheal measurements in these breeds. It is proposed that the tracheal diameter in a normal DSH cat should be 18% of the diameter of the thoracic inlet, and compared to 20% in Persian cats.
Tracheal hypoplasia is an underdevelopment of the trachea resulting in a significantly narrowed tracheal diameter, which is commonly found in brachycephalic dog breeds, most notably the English Bulldog and Boxer. 1 Changes that may be seen include close apposition or overlapping of the ends of the tracheal cartilage rings and absence of the dorsal tracheal membrane. Hypoplastic tracheas have a stable diameter that does not vary with the phase of respiration. 1 Tracheal hypoplasia may be regarded as a component of brachycephalic syndrome (along with stenotic nares, everted laryngeal saccules and an elongated soft palate). 2 Although the condition may frequently be clinically silent, the narrowing of the trachea may cause exacerbation of cardiovascular or respiratory disease.1,2 Clinical presentations and conditions associated with tracheal hypoplasia may include chronic coughing and recurrent tracheitis. 1
In the cat dynamic tracheal collapse has been reported, both due to a congenital malformation of the tracheal cartilages 3 and as an acquired condition associated with upper airway obstruction and neoplasms of the tracheal wall and lumen.3–7 Acquired narrowing of the tracheal lumen may be seen following trauma or associated with extraluminal compression or in association with thickening of the wall of the trachea.5,7 However, tracheal hypoplasia has been seldom reported in cats, where it has been reported in association with mucopolysaccharoidosis. 8
Diagnosis of tracheal narrowing (eg, associated with collapse or hypoplasia) is most easily made through radiography. In dogs, the most commonly used technique is to calculate the ratio between the diameter of the trachea at the level of the thoracic inlet and the inner diameter of the thoracic inlet. 9 In most dogs, this ratio will be greater than 0.2:1 — ie, the tracheal diameter will be at least 20% of the diameter of the thoracic inlet. In most brachycephalic breeds, this ratio has been calculated as normal if it is greater than 0.16:1, whilst in the English Bulldog, this measurement has been calculated to be normal for the breed if greater than 11% of the diameter of the thoracic inlet. Other ratios that have also been described for assessing tracheal diameter in the dog include comparing the diameter of the midthoracic trachea to the width of the third rib, with normal ratios of trachea:third rib being reported as >2.0 and >3.0, with tracheal hypoplasia being defined as a ratio of less than 1.0. 10 Although the diameter of the trachea can be assessed endoscopically, this technique is potentially hazardous due to the risk of obstruction of the already narrowed airway.
Radiographic assessment of the tracheal diameter and calculation of ratios to skeletal structures has not been reported in either domestic shorthair (DSH) or Persian cats. This study establishes reference intervals for these ratios in DSH and Persians, and investigates for differences in these ratios between the two breeds.
Materials and methods
The radiographic archives at the Small Animal Hospitals of the Royal (Dick) School of Veterinary Studies, University of Edinburgh and the Faculty of Veterinary Medicine, University of Glasgow were searched for thoracic radiographs of DSH and Persian cats and the associated medical records. For inclusion in the study, the patients had to be at least 1 year old and to have no history of respiratory or cardiovascular disease, and had to have right lateral thoracic radiographs of good diagnostic quality, including the entire thorax and thoracic inlet in the collimated area, with the neck in a neutral position (ie, not excessively hyperextended or flexed), with the forelimbs extended cranially and not superimposed on the thoracic cavity and with no axial rotation of the thorax. Cases with radiographic evidence of thoracic disease were excluded. In addition, cases with an endotracheal tube extending beyond the mid-cervical vertebrae were also excluded.
Once the films were collected, measurements (in millimetres) were taken from the films as follows (Fig 1):
Fig 1.
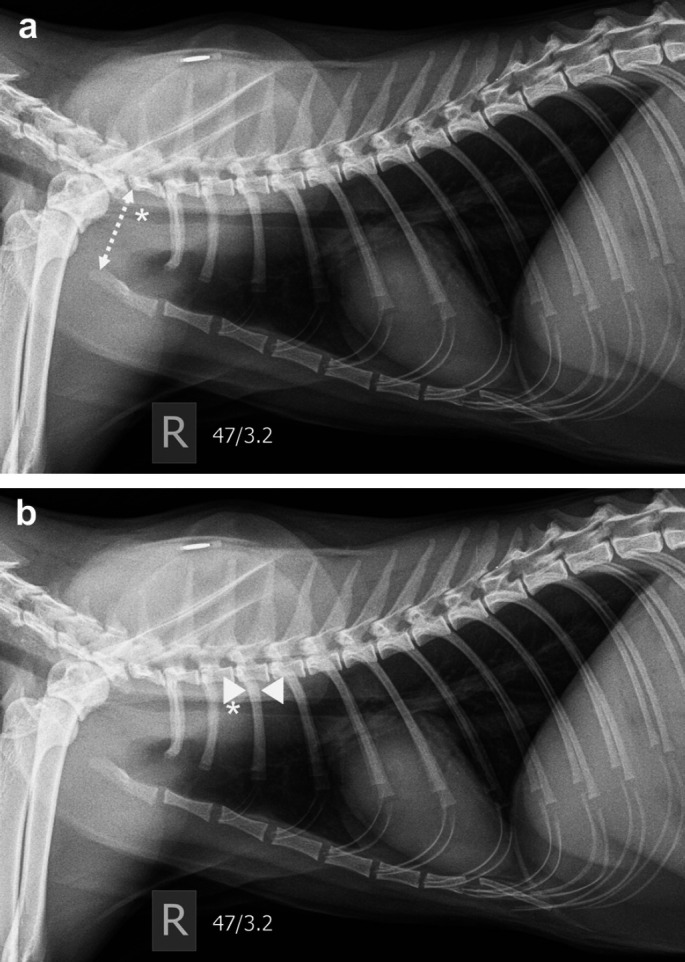
a. Lateral feline thoracic radiograph showing measurement points for trachea:thoracic inlet ratio: * = level to measure tracheal diameter (mm) at thoracic inlet (TDinlet);  = thoracic inlet diameter (mm) (TInlet). b. Lateral feline thoracic radiograph showing measurement points for trachea:third rib ratio: * = point to measure tracheal diameter (mm) in second intercostal space (TDintercostal);
= thoracic inlet diameter (mm) (TInlet). b. Lateral feline thoracic radiograph showing measurement points for trachea:third rib ratio: * = point to measure tracheal diameter (mm) in second intercostal space (TDintercostal);  = point to measure width of proximal one third of the third rib (mm) (between arrow heads) (Rib).
= point to measure width of proximal one third of the third rib (mm) (between arrow heads) (Rib).
Tracheal diameter at the level of the thoracic inlet (TDinlet) (Fig 1a)
Thoracic inletdiameter, from the dorsocranial aspect of the manubrium to the caudoventral aspect of the body of the seventh cervical vertebra (TInlet) (Fig 1a)
Tracheal diameter at the level of the second intercostal space (TDintercostal) (Fig 1b)
Width of the proximal third of the third rib (Rib) (Fig 1b).
The means were calculated for each group of measurements. Ratios were calculated between:
TDinlet divided by TInlet (measurement points from Fig 1a)
TDintercostal divided by Rib (measurement points from Fig 1b).
The mean measurements and ratios were compared between the populations (DSH and Persians) using a two-tailed t-test.
Results
Radiographs from 68 DSH and 40 Persians were included in the study. The majority had undergone thoracic radiography for either oncological staging or investigation of systemic disease. Measurements were subjectively simple to obtain using a standard ruler. The mean measurements are presented in Table 1. The mean ratios and P values are presented in Table 2.
Table 1.
Mean measurements and P values for DSH and Persian study populations.
| Mean measurements | P value | ||
|---|---|---|---|
|
|
|||
| DSH | Persian | ||
|
| |||
| Trachea—thoracic inlet | 5.4 mm | 5.6 mm | 0.37 |
| Trachea—mid-thoracic | 5.4 mm | 5.6 mm | 0.42 |
| Thoracic inlet | 32.5 mm | 28.7 mm | <0.005 |
| Proximal third rib | 3.5 mm | 3.3 mm | 0.05 |
Table 2.
Mean ratios and P values for DSH and Persian study populations
| Mean ratios | P value | ||
|---|---|---|---|
|
|
|||
| DSH | Persian | ||
|
| |||
| Trachea:thoracic inlet | 0.18 (range 0.13–0.23) | 0.20 (range 0.13–0.28) | <0.005 |
| Trachea:third rib | 1.59 (range 1.20–2.33) | 1.71 (range 1.25–2.33) | <0.05 |
There was no significant difference in the mean tracheal diameter at either the thoracic inlet or intercostal space locations, nor in the width of the third rib between the two populations. However there was a significant difference in the measurements of the thoracic inlet, with the Persian cat population showing a significantly narrowed thoracic inlet compared to the DSH population. There was a significant difference in both of the ratios calculated, with the Persian population showing significantly greater trachea:thoracic inlet and trachea:-third rib ratios than the DSH population.
Discussion
Given the potential significance of tracheal hypoplasia or other causes of tracheal narrowing, coupled with the lack of reference intervals for normal radiographic tracheal measurements in the cat, the authors felt it valuable to establish reference intervals for the trachea in mesaticephalic (DSH) and brachycephalic (Persian) cat breeds.
When comparing the absolute size of the trachea between the DSH and Persian populations, there was no significant difference between the mean tracheal diameters (Table 1). However, when the trachea: thoracic inlet is compared, that of the Persian population is significantly greater than that of the DSH population. This is believed to be due to a proportional dorsoventral compression of the thoracic inlet of the Persian cat when compared to that of the DSH (demonstrated by the significant difference in absolute measurements of the thoracic inlet shown in Table 1). This anatomic conformational difference is likely of no clinical significance, but results in the alteration in the trachea:thoracic ratio, and should be considered when assessing other structures using the thoracic skeletal structure as a comparison (eg, the height of the cardiac silhouette) as this apparent flattening could result in a misinterpretation of the structure or organ in question. The authors propose that the trachea in a DSH should be considered of normal diameter if it is 18% of the diameter of the thoracic inlet, and that of the Persian cat should be considered normal if it is 20% of the thoracic inlet.
The trachea:rib ratios demonstrated a similar (although less significant) variation between the populations. Given the similarity in absolute size of the tracheas, this is most suggestive of thicker ribs in the DSH population demonstrated by the absolute measurements (although this was not statistically significant). Although the weights and sizes of the patients included in the study was not always available, subjectively there was no significant discrepancy in body size between the two populations of adult cats (skeletally immature cats were excluded from the study) and so this is not thought to be an influence on the skeletal measurements. However, it was felt that the trachea:thoracic inlet ratio was considerably easier to obtain, and it would be the authors' advice that the trachea:thoracic ratio is used for assessing trachea diameter in preference to the trachea:rib ratio.
In addition, given the fairly uniform nature of the body sizes in the study population, it may be argued that a tracheal diameter of around 5.5 mm is normal for a cat (DSH or Persian) of average size, and this would forego the requirement to calculate a ratio with a set skeletal measurement. However, it cannot be guaranteed that the body sizes of the study population are typical of the population as a whole, and in addition some cats will lie at the extremes of the population range. It is, therefore, the authors' recommendation that the tracheal diameter is assessed using a ratio with a skeletal measurement (such as those described above) as this should minimise variations due to absolute body size.
Tracheal hypoplasia in the dog is frequently clinically silent, but as it can significantly worsen the clinical effect of a respiratory disorder such as pneumonia prior knowledge of its presence in a patient can be valuable. 1 Detection is most commonly through thoracic radiography, although computed tomography or endoscopy may also be indicative of tracheal hypoplasia.1,11 On the basis of the results of the study, it can be shown that there was no evidence of clinically silent tracheal hypoplasia in the population of Persian cats studied. It is possible that tracheal hypoplasia does exist in the Persian cat, but always results in clinically significant respiratory disease (and as a result, such cases would have been excluded from the population used in this study). However, this is thought unlikely by the authors, considering the frequently silent nature of tracheal hypoplasia in the dog. This would suggest that the brachycephalic anatomic changes seen in Persian cats are restricted to the skull and upper respiratory tract, such as the nasopharyngeal turbinates reported to be seen in about 20% of brachycephalic cats. 11 There is the question of whether the study population of Persian cats was truly representative of the population as a whole — unfortunately, in part due to this being a retrospective study, the possibility of a skewed population cannot be excluded. However, the authors feel that the wide range of presentations, and the inclusion of cases from two different referral hospitals reduces this possibility.
In conclusion, this study establishes reference intervals for the assessment of tracheal diameter in Persian and DSH cats: for DSH cats with no evidence of cardiorespiratory disease, the tracheal diameter should be 18% of the internal diameter of the thoracic inlet, and this measurement should increase to 20% in normal Persian cats.
References
- 1.Coyne BE, Fingland RB. Hypoplasia of the trachea in dogs: 103 cases (1974–1990). J Am Vet Med Assoc 1992; 201: 768–72. [PubMed] [Google Scholar]
- 2.Rieks TW, Birchard SJ, Stephens JA. Surgical correction of brachycephalic syndrome in dogs: 62 cases (1991–2004). J Am Vet Med Assoc 2007; 230: 1324–8. [DOI] [PubMed] [Google Scholar]
- 3.Hendricks JC, O'Brien JA. Tracheal collapse in two cats. J Am Vet Med Assoc 1985; 187: 418–9. [PubMed] [Google Scholar]
- 4.Fujita M, Miura H, Yasuda D, Hasegawa D, Orima H. Tracheal narrowing secondary to airway obstruction in two cats. J Small Anim Pract 2004; 45: 29–31. [DOI] [PubMed] [Google Scholar]
- 5.Kim DY, Kim JR, Taylor HW, Lee YS. Primary extranodal lymphosarcoma of the trachea in a cat. J Vet Med Sci 1996; 58: 703–6. [DOI] [PubMed] [Google Scholar]
- 6.Mims HL, Hancock RB, Leib MS, Waldron DR. Primary tracheal collapse in a cat. J Am Anim Hosp Assoc 2008; 44: 149–53. [DOI] [PubMed] [Google Scholar]
- 7.Bell R, Philbey AW, Martineau H, Nielsen L, Pawson P, Dukes-McEwan J. Dynamic tracheal collapse associated with disseminated histiocytic sarcoma in a cat. J Small Anim Pract 2006; 47: 461–4. [DOI] [PubMed] [Google Scholar]
- 8.Schultheiss PC, Gardner SA, Owens JM, Wenger DA, Thrall MA. Mucopolysaccharidosis VII in a cat. Vet Pathol 2000; 37: 502–5. [DOI] [PubMed] [Google Scholar]
- 9.Harvey CE, Fink EA. Tracheal diameter, analysis of radiographic measurements in brachycephalic and nonbrachycephalic dogs. J Am Anim Hosp Assoc 1982; 18: 570–6. [Google Scholar]
- 10.Suter PF. A text atlas of thoracic diseases of the dog and cat. Wettswil, Switzerland: Peter Suter, 1984: 238–40. [Google Scholar]
- 11.Schlueter C, Budras KD, Ludewig E, et al. CT and anatomical study of the relationship between head confirmation and the nasolacrimal drainage system. J Feline Med Surg 2009; 11: 891–900. [DOI] [PMC free article] [PubMed] [Google Scholar]