

Abstract
Background
Muscle power is associated with health‐related parameters. Simple equations were validated to estimate lower extremity muscle power measures based on the time to complete the five‐repetition sit‐to‐stand test. The present study was conducted to provide lower extremity muscle power estimates and produce centile values in a large and relatively unselected population across a wide age spectrum.
Methods
Data were from the Longevity Check‐up 7+ (Lookup 7+) project, an ongoing initiative conducted in unconventional settings (e.g., exhibitions, shopping centres and health promotion campaigns) across Italy to foster adoption of healthy lifestyles. Absolute, relative, allometric and specific muscle power measures of the lower extremities were estimated using validated formulas. Cross‐sectional centile and normative values for muscle power measures from 18 to 81+ years were produced for the two sexes. Smoothed normative curves for men and women were constructed using the lambda–mu–sigma method.
Results
From 1 June 2015 to 31 October 2021, 13 515 participants were enrolled of whom 12 864 were eligible for the present study. Mean age was 55.9 years (standard deviation: 14.8 years; range: 18–98 years), and 7217 (56.%) were women. Absolute, relative, allometric and specific muscle power declined significantly with age. Specific patterns of decline were observed according to sex and muscle power parameter. Absolute muscle power peaked at 41–50 and 31–40 years in men and women, respectively. Afterwards, a decline rate of approximately 12% per decade was observed, regardless of sex. Relative muscle power showed the largest reduction with age, such that it was 40.6% and 46.4% smaller in men and women older than 80, respectively, compared with those aged 18–30 years. Age‐related changes in allometric and specific muscle power measures were similar between men and women.
Conclusions
Data from the Lookup 7+ project indicate that lower extremity muscle power estimated using simple equations is significantly associated with age. Sex‐specific patterns of decline in absolute and relative muscle power were observed with age. Allometric and specific muscle power declined at a similar rate in men and women.
Keywords: ageing, chair‐stand test, lifestyle interventions, normative curves, percentiles, physical performance
Introduction
Muscle power is the capacity to generate muscular strength as fast as possible. Although it has long been almost exclusively associated with sports performance, 1 this physical capacity is now recognized as a major determinant of functional independence in advanced age. 2 During ageing, muscle power declines earlier and faster than other physical performance parameters (e.g., muscle strength). 3 , 4 , 5 Muscle power is a strong, independent predictor of mobility disability, 5 poor functional status, 6 hospitalization and death. 7 Indeed, this physical capacity is proposed to be a better predictor of physical independence, functional performance and mobility than muscle strength. 3 , 4 , 5 , 8 As such, the maintenance of muscle power is critical to preserve functionality in advanced age. 9 , 10 These observations have led to recommend power training being included within multicomponent interventions to prevent disability and other negative health‐related events in older adults. 11 , 12 , 13
Several tools are available to assess muscle power, such as pneumatic exercise machines, linear position transducers and rotary encoders. 14 However, equipment for muscle power measurement is rarely available outside a laboratory environment. In addition, the heterogeneity of testing protocols impacts the evaluation of muscle power in everyday practice, 14 thereby hampering the identification of those at risk of negative outcomes and the assessment of effectiveness of training programmes. Recently, Alcazar et al. 15 validated simple equations to estimate lower extremity muscle power measures based on the time to complete the five‐repetition sit‐to‐stand (5STS) test, chair's height, and the test person's body weight and height. Normative values of muscle power based on these equations have been proposed. 16 , 17 , 18 However, such values were estimated for older adults only and were obtained either in small samples or in studies combining different cohorts. The availability of normative values of muscle power across ages based on 5STS equations may represent an easy‐to‐apply and cost‐effective tool to assess this physical capacity in clinical practice.
Therefore, the present study was conducted to provide lower extremity muscle power estimates using Alcazar's equations and produce centile values across a wide age spectrum. To accomplish this objective, we used data collected in a large and relatively unselected sample of community‐dwellers ranging in age between 18 and 98 years, enrolled across Italy in the Longevity Check‐up 7+ (Lookup 7+) project.
Material and methods
Data for the present investigation were gathered from the Lookup 7+ project database. Lookup 7+ is an ongoing initiative developed by the Department of Geriatrics of the Fondazione Policlinico ‘Agostino Gemelli’ IRCCS at the Università Cattolica del Sacro Cuore (Rome, Italy). The project was designed to foster healthy and active ageing by raising awareness among the general public on the importance of modifiable risk factors for chronic diseases. 19
Recruitment was conducted among people visiting public spaces (e.g., exhibitions and shopping centres) and those adhering to prevention campaigns promoted by our institution. As previously described, recruitment activities were carried out in small (<100 000 inhabitants), medium (100 000–250 000 inhabitants) and large cities (>250 000 inhabitants) to achieve a comprehensive geographic coverage of mainland Italy and major islands. 20 In large cities, participants were recruited in different locations to maximize representation of sociodemographic characteristics of inhabitants. The Lookup 7+ protocol was approved by the Ethics Committee of the Università Cattolica del Sacro Cuore (Protocol #: A.1220/CE/2011), and each participant provided written informed consent prior to enrolment. The study protocol is described in detail elsewhere. 19
The manuscript was prepared in compliance with the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines for observational studies. 21
Study participants and data collection
From 1 June 2015 to 31 October 2021, 13 515 community‐dwelling adults aged 18+ years participated to the study. Exclusion criteria were inability or unwillingness to provide written informed consent, self‐reported pregnancy and inability to perform the physical function tests as per the study protocol. For the present investigation, 12 864 participants were analysed after excluding 651 cases with missing values for the variables of interest. The general characteristics of excluded participants did not differ from those with complete data.
Each participant received a structured interview to collect information on lifestyle habits, followed by measurement of anthropometric parameters, including height, weight and calf circumference. Body height and weight were measured through a stadiometer and an analogue medical scale, respectively. The body mass index (BMI) was then calculated as the ratio between body weight (kilograms) and the square of height (square metres). Calf circumference was taken on the dominant leg by measuring the largest girth (centimetres) between ankle and knee joints using an anthropometric tape while the participant was in a seated position. Values were rounded to nearest 0.1 cm. Appendicular skeletal muscle (ASM) was estimated based on the equation developed by the COCONUT Study Group 22 :
| (1) |
where sex = 1 for men and 0 for women.
The 5STS test was performed according to a standardised protocol by trained assessors. 20 , 23 Inter‐rater and test–retest reliability, assessed during the investigator training phase, was consistent with values reported in literature. 24 Participants were instructed to completely stand up from an armless chair (43–47 cm in height) five consecutive times as fast as possible, with their arms crossed over their chest. The chair's height was chosen according to the test person's height to allow participants placing their feet comfortably on the floor. 25 A stopwatch was used to measure the total time (seconds) needed to complete the task. 20 One familiarisation trial was allowed before the actual test was conducted. Absolute muscle power values were calculated according to the equation proposed by Alcazar et al. 15 :
| (2) |
where g is gravity (e.g., 9.80352 m/s2).
Relative (adjusted by body weight), allometric (adjusted by height squared) and specific (adjusted by ASM) muscle power values were subsequently calculated as follows:
| (3) |
| (4) |
| (5) |
Statistical analysis
Demographic, anthropometric and functional characteristics of study participants according to sex and age groups are summarised as means ± standard deviation (SD). According to the Shapiro–Wilk test, data were not normally distributed. Non‐Gaussian distribution might be ignored if large sample sizes (>30–40 participants) with values representative of a ‘real population’ are analysed. 26 , 27 However, to ensure that the type of statistics did not impact results, parametric and non‐parametric analyses were conducted. To generate sex‐ and age‐specific normative values for muscle power, participants were categorised into young adult (18–30 years), adult (31–40 years), middle‐aged (41–50 years), late middle‐aged (51–60 years), young old (61–70 years), old (71–80 years) and very old (81+ years) groups. 28 , 29 One‐way analysis of variance (ANOVA), with Bonferroni's post hoc tests when appropriate, and Kruskal–Wallis H test, with Dunn's post hoc tests as needed, were used to compare participant characteristics among age groups in the whole sample and in men and women separately. Pearson's and Spearman's correlations were run to measure the strength of linear association between muscle power and age. For all tests, the level of significance was set at 5% (P < 0.05). All analyses were performed using the SPSS software Version 23.0 (SPSS Inc., Chicago, IL, USA).
Smoothed percentile curves for absolute muscle power values in men and women were constructed using the lambda–mu–sigma (LMS) method (LMS Chart Maker Pro Version 2.54, Medical Research Council, London, UK), as described elsewhere. 20
Results
The main characteristics of the 12 864 participants are shown in Table 1 . Mean age of participants was 55.9 ± 14.8 years (range: 18–98 years), and 7217 (56.1%) were women. Weight increased, while height declined significantly across age groups in the whole study sample. Calf circumference was greater in both 31–40 and 41–50 years groups compared with the 18–30 years group and declined significantly hereof up to the 81+ years group. A significant decline in ASM values was observed starting from 51 to 60 years. The performance on the 5STS test decreased from the fourth decade of life onwards. Absolute muscle power declined later, starting from the fifth decade of life. Relative muscle power decreased earlier, from the fourth decade of life, while allometric and specific muscle power values declined later, starting from 50 to 60 years. Age‐related changes in weight, calf circumference and ASM were similar in men and women. However, sex‐specific patterns of age‐related changes in muscle power measures were observed. Relative muscle power declined earlier in men, with values at 31–40 years being lower than in the 18–30 years group. Instead, absolute muscle power declined later in men, starting from the sixth decade. Women showed a later decline in relative muscle power, which was significantly reduced starting from 41−50 years. Findings did not differ when ANOVA or Kruskal–Wallis H statistics were used.
Table 1.
Main characteristics of study participants (n = 12 864)
| Variables | Age groups (years) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Whole sample | 18–30 (n = 905) | 31–40 (n = 1123) | 41–50 (n = 2214) | 51–60 (n = 3426) | 61–70 (n = 2983) | 71–80 (n = 1863) | 81+ (n = 350) | F | P value | χ 2 | P value |
| Age (years) | 24.8 ± 3.6 | 35.9 ± 2.8 | 46.2 ± 2.8 | 55.5 ± 2.7 | 65.5 ± 2.8 | 74.8 ± 2.7 | 83.9 ± 3.1 | 504 602.9 | <0.001 | 1234.6 | <0.001 |
| BMI (kg/m2) | 22.5 ± 3.6 | 24.0 ± 2.8 | 25.0 ± 4.3 | 25.5 ± 4.2 | 26.2 ± 4.1 | 26.5 ± 4.1 | 26.1 ± 3.7 | 139.4 | <0.001 | 961.3 | <0.001 |
| Weight (kg) | 65.8 ± 13.2 | 70.4 ± 14.9 a | 72.1 ± 15.2 a , b | 71.7 ± 14.6 a | 71.6 ± 13.9 a | 70.6 ± 12.6 a , c | 68.9 ± 11.9 a , c , d , e | 26.5 | <0.001 | 149.1 | <0.001 |
| Height (m) | 1.70 ± 0.9 | 1.70 ± 0.9 | 1.69 ± 0.9 b | 1.67 ± 0.9 a , b , c | 1.64 ± 0.9 a , b , c , d | 1.63 ± 0.9 a , b , c , d , e | 1.62 ± 0.9 a , b , c , d , e | 164.5 | <0.001 | 833.2 | <0.001 |
| Calf circumference (cm) | 35.5 ± 3.5 | 36.0 ± 3.4 a | 36.1 ± 3.5 a | 35.9 ± 3.6 a , b , c | 35.3 ± 3.4 a , b , c , d | 34.7 ± 3.3 a , b , c , d , e | 34.2 ± 3.2 a , b , c , d , e | 48.9 | <0.001 | 290.7 | <0.001 |
| ASM (kg) | 19.2 ± 5.1 | 19.8 ± 5.1 | 19.2 ± 5.1 | 18.7 ± 5.2 b , c | 18.0 ± 5.2 a , b , c , d | 17.5 ± 5.0 a , b , c , d | 17.3 ± 5.1 a , b , c , d | 40.2 | <0.001 | 264.1 | <0.001 |
| Sit‐to‐stand (s) | 6.4 ± 1.4 | 6.7 ± 1.6 | 7.0 ± 1.7 a , b | 7.6 ± 1.9 a , b , c | 8.3 ± 2.1 a , b , c , d | 9.5 ± 2.8 a , b , c , d , e | 10.9 ± 3.7 a , b , c , e , f | 513.3 | <0.001 | 2613.7 | <0.001 |
| Muscle power | |||||||||||
| Absolute (W) | 372.6 ± 119.0 | 384.6 ± 120.2 | 371.7 ± 124.2 b | 337.1 ± 115.1 a , b , c | 299.6 ± 103.5 a , b , c , d | 259.5 ± 92.2 a , b , c , d , e | 223.9 ± 87.1 a , b , c , d , e , f | 333.4 | <0.001 | 1864.7 | <0.001 |
| Relative (W/kg) | 5.63 ± 1.24 | 5.45 ± 1.19 a | 5.13 ± 1.22 a , b | 4.67 ± 1.17 a , b , c | 4.16 ± 1.08 a , b , c , d | 3.64 ± 1.03 a , b , c , d , e | 3.21 ± 1.04 a , b , c , d , e , f | 676.9 | <0.001 | 3258.8 | <0.001 |
| Allometric (W/m2) | 126.7 ± 32.8 | 130.5 ± 33.6 | 127.8 ± 35.4 | 118.7 ± 33.4 a , b , c | 108.5 ± 30.3 a , b , c , d | 96.1 ± 29.2 a , b , c , d , e | 83.3 ± 28.3 a , b , c , d , e , f | 307.8 | <0.001 | 1730.5 | <0.001 |
| Specific (W/kg) | 9.2 ± 2.3 | 9.3 ± 2.3 | 9.1 ± 2.4 | 8.4 ± 2.3 a , b , c | 7.6 ± 2.1 a , b , c , d | 6.6 ± 1.9 a , b , c , d , e | 5.7 ± 1.9 a , b , c , d , e , f | 398.0 | <0.001 | 2177.1 | <0.001 |
| Men | 18–30 (n = 369) | 31–40 (n = 541) | 41–50 (n = 966) | 51–60 (n = 1430) | 61–70 (n = 1282) | 71–80 (n = 875) | 81+ (n = 184) | F | P value | χ 2 | P value |
| Age (years) | 24.4 ± 3.8 | 36.1 ± 2.7 | 46.0 ± 2.8 | 55.6 ± 2.7 | 65.6 ± 2.9 | 74.8 ± 2.7 | 84.2 ± 3.3 | 24 590.2 | <0.001 | 5434.4 | <0.001 |
| BMI (kg/m2) | 23.6 ± 3.3 | 25.2 ± 3.6 | 26.1 ± 3.8 | 26.4 ± 3.7 | 27.1 ± 3.8 | 26.6 ± 3.3 | 26.2 ± 3.3 | 50.4 | <0.001 | 337.8 | <0.001 |
| Weight (kg) | 74.7 ± 11.3 | 79.4 ± 12.2 a | 82.0 ± 12.9 a , b | 81.2 ± 12.4 a | 80.5 ± 12.4 a | 77.1 ± 10.6 a , b , c , d , e | 74.9 ± 9.7 b , c , d , e | 32.3 | <0.001 | 187.8 | <0.001 |
| Height (m) | 1.77 ± 0.7 | 1.77 ± 0.6 | 1.76 ± 0.6 | 1.74 ± 0.6 a , b , c | 1.72 ± 0.6 a , b , c , d | 1.69 ± 0.6 a , b , c , d , e | 1.68 ± 0.6 a , b , c , d , e | 154.2 | <0.001 | 809.0 | <0.001 |
| Calf circumference (cm) | 36.6 ± 3.7 | 37.0 ± 3.1 | 37.2 ± 3.3 | 37.1 ± 3.3 | 36.4 ± 3.2 b , c , d | 35.5 ± 3.1 a , b , c , d , e | 35.0 ± 3.3 a , b , c , d , e | 36.0 | <0.001 | 220.1 | <0.001 |
| ASM (kg) | 24.5 ± 2.8 | 24.4 ± 2.4 | 24.3 ± 2.5 | 24.0 ± 2.5 a , b | 23.1 ± 2.4 a , b , c , d | 22.2 ± 2.4 a , b , c , d , e | 21.5 ± 2.5 a , b , c , d , e | 108.2 | <0.001 | 617.4 | <0.001 |
| Sit‐to‐stand (s) | 6.5 ± 1.4 | 6.8 ± 1.3 a | 7.0 ± 1.8 a | 7.4 ± 1.7 a , b , c | 8.1 ± 1.9 a , b , c , d | 9.0 ± 2.4 a , b , c , d , e | 10.4 ± 3.3 a , b , c , d , e , f | 198.2 | <0.001 | 1016.3 | <0.001 |
| Muscle power | |||||||||||
| Absolute (W) | 444.3 ± 119.5 | 448.5 ± 113.9 | 449.1 ± 122.4 | 414.0 ± 111.6 a , b , c | 368.3 ± 102.0 a , b , c , d | 313.7 ± 87.4 a , b , c , d , e | 267.1 ± 80.9 a , b , c , d , e , f | 221.6 | <0.001 | 1168.7 | <0.001 |
| Relative (W/kg) | 5.93 ± 1.24 | 5.64 ± 1.12 a | 5.47 ± 1.21 a | 5.10 ± 1.17 a , b , c | 4.58 ± 1.11 a , b , c , d | 4.07 ± 1.01 a , b , c , d , e | 3.57 ± 1.02 a , b , c , d , e , f | 271.0 | <0.001 | 1355.9 | <0.001 |
| Allometric (W/m2) | 140.2 ± 33.5 | 142.1 ± 32.2 | 143.1 ± 36.0 | 134.7 ± 33.5 b , c | 123.4 ± 31.4 a , b , c , d | 108.2 ± 28.9 a , b , c , d , e | 93.7 ± 28.2 a , b , c , d , e , f | 160.9 | <0.001 | 894.2 | <0.001 |
| Specific (W/kg) | 9.7 ± 2.4 | 9.8 ± 2.3 | 9.9 ± 2.5 | 9.2 ± 2.3 a , b , c | 8.3 ± 2.2 a , b , c , d | 7.2 ± 1.9 a , b , c , d , e | 6.2 ± 1.8 a , b , c , d , e , f | 183.4 | <0.001 | 994.2 | <0.001 |
| Women | 18–30 (n = 536) | 31–40 (n = 582) | 41–50 (n = 1248) | 51–60 (n = 1996) | 61–70 (n = 1701) | 71–80 (n = 988) | 81+ (n = 166) | F | P value | χ 2 | P value |
| Age (years) | 25.0 ± 3.5 | 35.7 ± 2.8 | 46.4 ± 2.7 | 55.4 ± 2.8 | 65.4 ± 2.8 | 74.7 ± 2.7 | 83.6 ± 2.9 | 30 123.6 | <0.001 | 6909.4 | <0.001 |
| BMI (kg/m2) | 21.7 ± 2.5 | 22.8 ± 4.2 | 24.1 ± 4.5 | 24.8 ± 4.4 | 25.6 ± 4.2 | 26.4 ± 4.7 | 25.9 ± 4.1 | 99.7 | <0.001 | 727.8 | <0.001 |
| Weight (kg) | 59.6 ± 10.6 | 62.0 ± 12.0 a | 64.5 ± 12.3 a , b | 64.9 ± 12.1 a , b | 64.8 ± 10.9 a , b | 64.9 ± 11.1 a , b | 62.3 ± 10.5 | 20.3 | <0.001 | 156.9 | <0.001 |
| Height (m) | 1.65 ± 0.6 | 1.64 ± 0.6 | 1.63 ± 6.6 a | 1.61 ± 0.6 a , b , c | 1.59 ± 0.6 a , b , c , d | 1.67 ± 0.6 a , b , c , d , e | 1.55 ± 0.7 a , b , c , d , e | 192.1 | <0.001 | 1006.5 | <0.001 |
| Calf circumference (cm) | 34.7 ± 3.2 | 35.1 ± 3.4 | 35.3 ± 3.5 a | 35.0 ± 3.5 | 34.5 ± 3.3 a , b , c , d | 33.9 ± 3.3 a , b , c , d , e | 33.2 ± 3.3 a , b , c , d , e | 24.1 | <0.001 | 143.5 | <0.001 |
| ASM (kg) | 15.5 ± 2.5 | 15.5 ± 2.6 | 15.3 ± 2.7 | 14.8 ± 2.7 a , b , c | 14.1 ± 2.6 a , b , c , d | 13.4 ± 2.6 a , b , c , d , e | 12.7 ± 2.5 a , b , c , d , e , f | 91.1 | <0.001 | 540.3 | <0.001 |
| Sit‐to‐stand (s) | 6.4 ± 1.4 | 6.6 ± 1.8 | 7.1 ± 1.6 a , b | 7.8 ± 2.0 a , b , c | 8.5 ± 2.2 a , b , c , d | 9.9 ± 3.0 a , b , c , d , e | 11.5 ± 4.0 a , b , c , d , e , f | 330.6 | <0.001 | 1641.0 | <0.001 |
| Muscle power | |||||||||||
| Absolute (W) | 323.3 ± 90.0 | 325.2 ± 92.2 | 311.7 ± 87.0 b | 282.0 ± 82.3 a , b , c | 247.7 ± 68.7 a , b , c , d | 211.5 ± 66.1 a , b , c , d , e | 176.0 ± 66.5 a , b , c , d , e , f | 300.6 | <0.001 | 1590.7 | <0.001 |
| Relative (W/kg) | 5.43 ± 1.19 | 5.27 ± 1.23 | 4.86 ± 1.16 a | 4.36 ± 1.07 a , b , c | 3.84 ± 0.94 a , b , c , d | 3.27 ± 0.90 a , b , c , d , e | 2.82 ± 0.92 a , b , c , d , e , f | 502.7 | <0.001 | 2232.9 | <0.001 |
| Allometric (W/m2) | 117.4 ± 28.8 | 119.6 ± 31.1 | 116.0 ± 30.1 | 107.3 ± 28.3 a , b , c | 97.3 ± 24.1 a , b , c , d | 85.5 ± 25.1 a , b , c , d , e | 71.8 ± 23.7 a , b , c , d , e , f | 225.8 | <0.001 | 1214.2 | <0.001 |
| Specific (W/kg) | 8.8 ± 2.2 | 8.9 ± 2.2 | 8.5 ± 2.1 | 7.8 ± 2.1 a , b , c | 7.0 ± 1.8 a , b , c , d | 6.1 ± 1.8 a , b , c , d , e | 5.2 ± 1.8 a , b , c , d , e , f | 263.9 | <0.001 | 1398.4 | <0.001 |
Note: Data are shown as mean ± standard deviation.
Abbreviations: ASM, appendicular skeletal muscle; BMI, body mass index.
P < 0.05 versus 18–30.
P < 0.05 versus 31–40.
P < 0.05 versus 41–50.
P < 0.05 versus 51–60.
P < 0.05 versus 61–70.
P < 0.05 versus 71–80.
Mean and percentage differences in muscle power parameters across ages compared with the 18–30 years group are shown in Table 2 . In men, absolute muscle power peaked at 41–50 years and declined thereafter at a mean rate of 12% per decade up to 70 years. Afterwards, the rate of decline per decade was approximately 34%, such that men older than 80 showed approximately 40% less muscle power compared with the 18–30 years group. In women, muscle power peaked at 31–40 years, after which it declined at a mean rate of 11.4% per decade up to 70 years. As in men, the rate of decline accelerated past the age of 70, with a mean loss of 35% per decade. In women older than 80, muscle power was approximately 40% lower than in those 18–30 years. In both sexes, the largest reduction with age was observed for relative muscle power, which was 40.6% and 46.4% lower in men and women older than 80, respectively, compared with the 18–30 years group.
Table 2.
Mean and percentage differences in muscle power parameters relative to the 18–30 years group
| Variables | Age groups (years) | |||||
|---|---|---|---|---|---|---|
| Whole sample | 31–40 (n = 1123) | 41–50 (n = 2214) | 51–60 (n = 3426) | 61–70 (n = 2983) | 71–80 (n = 1873) | 81+ (n = 340) |
| Absolute muscle power (W) | 11.9 (3.2%) | 0.9 (0.2%) | −35.5 (−9.5%) | −73.0 (−19.6%) | −113.1 (−30.3%) | −148.7 (−39.9%) |
| Relative muscle power (W/kg) | −0.2 (−3.6%) | −0.5 (−8.9%) | −1.0 (−17.9%) | −1.5 (−26.7%) | −2.0 (−35.7%) | −2.4 (−42.9%) |
| Allometric muscle power (W/m2) | 3.8 (3.0%) | 1.1 (0.9%) | −8.0 (−6.3%) | −18.1 (−14.2%) | −30.5 (−24.1%) | −43.3 (−34.2%) |
| Specific muscle power (W/kg) | 0.1 (1.1%) | −0.0 (−0.0%) | −0.8 (−8.7%) | −1.6 (−17.4%) | −2.5 (−27.1%) | −3.4 (−37.0%) |
| Men | 31–40 (n = 541) | 41–50 (n = 966) | 51–60 (n = 1430) | 61–70 (n = 1282) | 71–80 (n = 875) | 81+ (n = 184) |
| Absolute muscle power (W) | 4.2 (0.9%) | 4.8 (1.1%) | −30.3 (−6.9%) | −76.0 (−17.1%) | −130.6 (−29.3%) | −177.2 (−39.9%) |
| Relative muscle power (W/kg) | 0.3 (5.1%) | −0.5 (−8.4%) | −0.9 (−15.2%) | −1.3 (−22.0%) | −1.9 (−32.2%) | −2.4 (−40.6%) |
| Allometric muscle power (W/m2) | 1.9 (1.3%) | 3.0 (2.1%) | −5.4 (−3.9%) | −16.7 (−11.9%) | −32.0 (−22.8%) | −46.4 (−33.1%) |
| Specific muscle power (W/kg) | 0.1 (1.0%) | 0.1 (1.0%) | −0.5 (−5.1%) | −1.3 (−13.4%) | −2.4 (−24.7%) | −3.4 (−35.0%) |
| Women | 31–40 (n = 582) | 41–50 (n = 1248) | 51–60 (n = 1996) | 61–70 (n = 1701) | 71–80 (n = 988) | 81+ (n = 166) |
| Absolute muscle power (W) | 1.9 (0.5%) | −11.5 (−3.0%) | −41.3 (−11.0%) | −75.5 (−20.2%) | −111.7 (−30.0%) | −147.2 (−39.5%) |
| Relative muscle power (W/kg) | −0.2 (−2.9%) | −0.6 (−9.0%) | −1.1 (−19.6%) | −1.6 (−28.5%) | −2.1 (−37.5%) | −2.6 (−46.4%) |
| Allometric muscle power (W/m2) | 2.2 (1.7%) | −1.3 (−1.0%) | −10.1 (−7.9%) | −20.0 (−15.7%) | −32.0 (−25.2%) | −45.5 (−36.0%) |
| Specific muscle power (W/kg) | 0.0 (0.0%) | −0.3 (−0.3%) | −0.9 (−0.9%) | −1.8 (−10.5%) | −2.7 (−29.3%) | −3.6 (−39.1%) |
Figures 1, 2, 3 show the relationship between age and muscle power parameters in the whole study sample and in men and women, respectively. Age was significantly and negatively correlated with absolute, relative, allometric and specific muscle power in the whole study population and in the two sexes separately (Table S1 ). Results remained unchanged after adjustment for BMI (Table S2 ), suggesting that body size did not influence the association between age and muscle power parameters.
Figure 1.
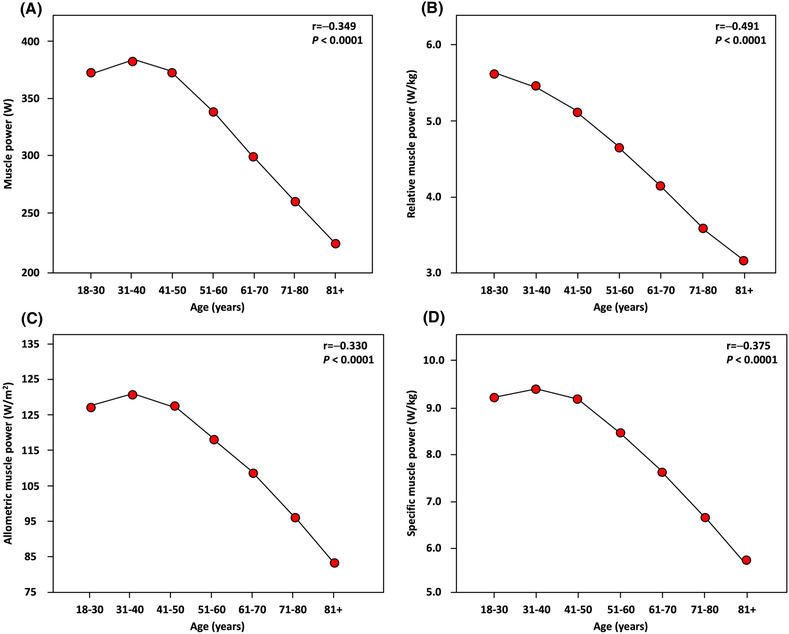
Relationship between age and lower extremity muscle power in the whole study sample as assessed by Pearson's statistics. (A) Absolute muscle power. (B) Relative muscle power. (C) Allometric muscle power. (D) Specific muscle power.
Figure 2.
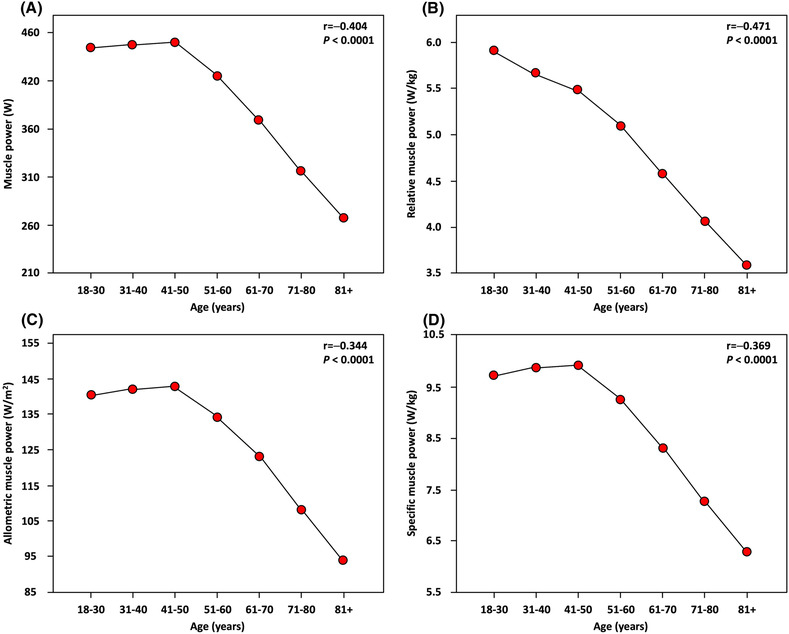
Relationship between age and lower extremity muscle power in men as assessed by Pearson's statistics. (A) Absolute muscle power. (B) Relative muscle power. (C) Allometric muscle power. (D) Specific muscle power.
Figure 3.
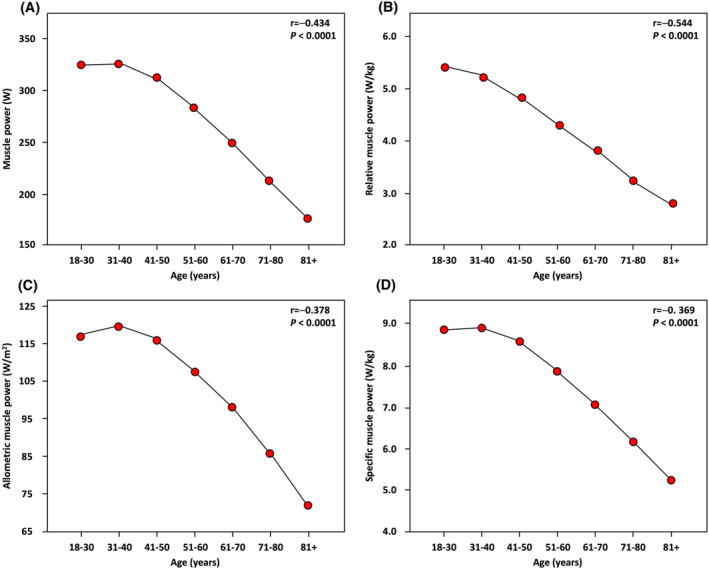
Relationship between age and lower extremity muscle power in women as assessed by Pearson's statistics. (A) Absolute muscle power. (B) Relative muscle power. (C) Allometric muscle power. (D) Specific muscle power.
Normative values for absolute muscle power in men and women, stratified by age groups, are listed in Tables 3 and 4 , respectively. Normative values for relative, allometric and specific muscle power values in men and women are shown in Tables S3–S8 . For each muscle power parameter, mean values ± SD and the 5th, 25th, 50th, 75th and 95th percentiles are reported. Reference percentiles for absolute muscle power are also depicted as charts in Figure 4 to facilitate their practical implementation.
Table 3.
Normative values for estimated absolute muscle power in men, stratified by age groups
| Age groups (years) | Observations (n) | Centiles | Mean (SD) | ||||
|---|---|---|---|---|---|---|---|
| 5th | 25th | 50th | 75th | 95th | |||
| Muscle power (W) | |||||||
| 18–30 | 369 | 265.3 | 358.3 | 441.0 | 514.3 | 665.9 | 444.3 (119.5) |
| 31–40 | 541 | 289.8 | 368.6 | 434.1 | 514.4 | 657.1 | 448.5 (113.9) |
| 41–50 | 966 | 270.0 | 360.7 | 441.7 | 524.2 | 666.7 | 449.1 (122.4) |
| 51–60 | 1430 | 256.5 | 338.3 | 398.4 | 480.6 | 605.8 | 414.0 (111.6) |
| 61–70 | 1282 | 228.2 | 296.7 | 356.2 | 428.7 | 552.5 | 368.3 (102.0) |
| 71–80 | 875 | 188.5 | 254.6 | 305.0 | 365.5 | 468.7 | 313.7 (87.4) |
| 81+ | 184 | 154.7 | 210.5 | 258.9 | 317.1 | 414.6 | 267.1 (80.9) |
Table 4.
Normative values for estimated absolute muscle power in women, stratified by age groups
| Age groups (years) | Observations (n) | Centiles | Mean (SD) | ||||
|---|---|---|---|---|---|---|---|
| 5th | 25th | 50th | 75th | 95th | |||
| Muscle power (W) | |||||||
| 18–30 | 536 | 197.8 | 267.1 | 311.7 | 369.5 | 488.9 | 323.3 (90.0) |
| 31–40 | 582 | 194.3 | 263.4 | 313.4 | 376.6 | 492.0 | 325.2 (92.2) |
| 41–50 | 1248 | 185.9 | 253.9 | 300.0 | 262.9 | 477.6 | 311.7 (87.0) |
| 51–60 | 1996 | 168.2 | 225.7 | 272.4 | 325.6 | 436.0 | 282.0 (82.3) |
| 61–70 | 1701 | 145.1 | 203.4 | 240.6 | 286.2 | 366.9 | 247.7 (68.7) |
| 71–80 | 988 | 119.1 | 134.4 | 206.2 | 249.2 | 321.7 | 211.5 (66.1) |
| 81+ | 166 | 77.3 | 125.6 | 171.2 | 214.7 | 279.1 | 176.0 (66.0) |
Figure 4.
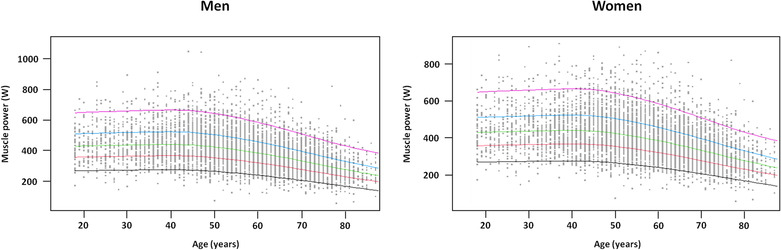
Reference percentiles for lower extremity absolute muscle power in men and women from 18 to 98 years. The 5th, 25th, 50th, 75th and 95th percentiles are depicted in black, red, green, light blue and purple, respectively.
Discussion
The present study provides normative values of lower extremity muscle power, estimated according to 5STS equations, 15 in a large and relatively unselected sample of Italian men and women across 18–98 years of age. Results of our investigation indicate that muscle power of lower extremities declines with age in men and women, with substantial losses during the last decades of life. Men displayed a significant decline in absolute, allometric and specific muscle power from the fifth decade of life. An earlier decrease, approximately in the third decade of life, was observed for relative muscle power. A similar pattern of decline was detected in women, except that relative muscle power declined significantly from the fourth decade onwards.
Our findings are in line with prior investigations. Using data from 1030 participants of the InCHIANTI study (age range 20–102 years), Lauretani et al. 5 found that lower extremity muscle power, measured through a leg extensor power rig, declined linearly from the third decade onwards. The pattern of decline was comparable between men and women. Similar findings were obtained by Suetta et al. 30 who assessed lower extremity muscle power by a leg extensor power rig in 1305 adults (age range 20–93 years) enrolled in the Copenhagen City Heart Study. In the same study population, Alcazar et al. 31 observed that lower extremity relative muscle power remained substantially unvaried between 20 and 45 years and started to decline thereafter. The authors demonstrated that, up to ~70 years, relative muscle power decreased because of both a loss of absolute power and an increase in body weight. Past the age of 70, relative muscle power declines were due to losses of absolute power only. In line with data of the present study, losses in absolute muscle power were found to be greater between 50 and 80 years in a large European cohort. 17
Only few studies analysed age‐related changes in lower extremity muscle power using 5STS‐based estimates. Baltasar‐Fernandez et al. 16 examined 1369 older adults (age range 66–97 years) from the Toledo Study for Healthy Ageing and found that muscle power‐related parameters declined significantly with age. In particular, absolute muscle power dropped by 1.2–1.4% yearly in men and up to 2.0% yearly in women. 16 In 3689 Colombian community‐dwellers, Ramírez‐Vélez et al. 18 estimated reference values for absolute muscle power from 60 to 85+ years of age. Mean values of muscle power‐related parameters across age groups were lower than those reported in the present study.
Relative, allometric and specific lower extremity muscle power measures provide information on crosstalk among different physiologic domains. Therefore, their assessment allows for exploring the influence of various parameters on absolute muscle power. As shown in this study and by others, 17 , 31 relative muscle power declines earlier than absolute muscle power, especially in men, which may reflect a combined effect of weight gain and declining neuromuscular function. Early adulthood is commonly associated with high familiar and work requirements. To optimise time, people often increase consumption of processed and takeaway foods, 32 , 33 while concomitantly quitting or drastically reducing physical activity and exercise. 34 The later decline in relative muscle power observed in women might be explained, at least partly, by the societal pressure to maintain body shape. 35
The absence of appreciable declines in specific muscle power in men and women until late middle‐age suggests that loss of muscle mass contributes marginally to absolute muscle power declines. Detriments in neuromuscular junction, 36 loss of motor neurons 37 and declines in the capacity of generating tension (i.e., muscle strength) 5 , 20 , 38 are candidate factors underpinning the age‐related decrease in absolute muscle power.
Our study has limitations that should be mentioned. First, only a limited number of participants 18–30 and 90+ years were enrolled. Second, adjusted analysis was not corrected for many covariables that may influence neuromuscular function, including physical activity levels, 39 diet quality, 40 sleep 41 and medical conditions. 42 Third, the unconventional settings (e.g., exhibitions, shopping centres and prevention campaigns) in which data collection was carried out might have selected a relatively healthy and functionally competent population. Fourth, although efforts were put forth to enrol a heterogeneous population, no detailed information was collected on the sociodemographic characteristics of participants. Hence, potential selection biases cannot be ruled out. Fifth, the study sample only included Caucasian individuals, and extrapolations of findings to other ethnic groups should be made carefully. Finally, the results shown in this work are derived from cross‐sectional observations and it is possible that differences in birth cohorts may have influenced some of the assessed parameters. For the same reason, curves and centile values should not be used to follow an individual's trajectory of muscle power over time. A deeper understanding of age‐dependent trajectories of muscle power requires the analysis of prospective data that are not available at this stage for our study.
Conclusions
Our results indicate that lower extremity muscle power estimated using simple equations is significantly associated with age in men and women. Absolute muscle power declined significantly from the fifth decade onwards in both men and women. An earlier decline was observed for relative muscle power. The normative values produced may be a useful tool to quickly examine people across a wide age spectrum and identify those who should be offered further evaluation and prescription of lifestyle interventions.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Funding
Carni Sostenibili, Danone Italia, Errekappa, Ferrarini, Italfarmaco, Italia Longeva, IVSI, Laborest, Yakult, Marche Region, Nutricia, ProAction, Serenissima and Novartis supported the Lookup 7+ project. The study was also partly supported by intramural research grants from the Università Cattolica del Sacro Cuore (D1.2020 and D1.2022), the Italian Ministry of Health (Ricerca Corrente 2023), the European Commission NextGeneration EU (Age‐IT spoke 3), and by the nonprofit research foundation ‘Centro Studi Achille e Linda Lorenzon’. The funders had no role in the design of the study; collection, analysis or interpretation of data; writing of the manuscript; or the decision to submit the results for publication. The views and opinions expressed are only those of the authors and do not necessarily reflect those of the European Union or the European Commission. Neither the European Union can be held responsible for them.
Supporting information
Table S1. Pearson's and Spearman's correlation coefficients of the relationship between age and lower‐extremity muscle power.
Table S2. Pearson's correlation coefficients of the relationship between age and lower‐extremity muscle power adjusted by body mass index.
Table S3. Normative values for estimated relative muscle power in men, stratified by age groups.
Table S4. Normative values for estimated allometric muscle power in men, stratified by age groups.
Table S5. Normative values for estimated specific muscle power in men, stratified by age groups.
Table S6. Normative values for estimated relative muscle power in women, stratified by age groups.
Table S7. Normative values for estimated allometric muscle power in women, stratified by age groups.
Table S8. Normative values for estimated specific muscle power in women, stratified by age groups.
Acknowledgements
The Lookup 7+ study group is composed as follows: Steering Committee: F. Landi and R. Bernabei; Coordination: E. Marzetti, R. Calvani and L. Mariotti; Writing Panel: A. M. Martone, E. D'Angelo, E. Serafini, A. Picca, V. Palmieri, M. Tosato, P. Abete, A. Cherubini, F. Corica and S. Salini; Field Investigators: M. Bianco, D. Biscotti, V. Brandi, M. Broccatelli, L. Catalano, F. Ciciarello, M. D'Elia, M. T. Fuga, E. Ortolani, G. Savera and M. B. Zazzara; and Participants: A. Almohani, F. Benvenuto, M. Bianchi, G. Bramato, R. Capitani, C. Celesti, G. Colloca, F. Cuccaro, L. Damato, E. Di Murru, S. Fabrizi, D. Fusco, A. Galliani, V. Galluzzo, S. Gervasi, R. Quarta, G. Modica, R. Monti, S. Orvieto, C. Pais, C. Pantanelli, S. Rocchi, D. Ronconi, E. Rota, F. Sollazzo and M. Tritto. The authors of this manuscript certify that they comply with the ethical guidelines for authorship and publishing in the Journal of Cachexia, Sarcopenia and Muscle. 43
Coelho‐Junior HJ, Marzetti E, Picca A, Tosato M, Calvani R, Landi F. Sex‐ and age‐specific normative values of lower extremity muscle power in Italian community‐dwellers. Journal of Cachexia, Sarcopenia and Muscle 2023; 10.1002/jcsm.13301
References
- 1. Kraemer WJ, Looney DP. Underlying mechanisms and physiology of muscular power. Strength Cond J 2012;34:13–19. [Google Scholar]
- 2. Reid KF, Fielding RA. Skeletal muscle power: a critical determinant of physical functioning in older adults. Exerc Sport Sci Ver 2012;40:4–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Suzuki T, Bean JF, Fielding RA. Muscle power of the ankle flexors predicts functional performance in community‐dwelling older women. J Am Geriatr Soc 2001;49:1161–1167. [DOI] [PubMed] [Google Scholar]
- 4. Bean JF, Leveille SG, Kiely DK, Bandinelli S, Guralnik JM, Ferrucci L. A comparison of leg power and leg strength within the InCHIANTI study: which influences mobility more? J Gerontol A Biol Sci Med Sci 2003;58:M728–M733. [DOI] [PubMed] [Google Scholar]
- 5. Lauretani F, Russo CR, Bandinelli S, Bartali B, Cavazzini C, Di Iorio A, et al. Age‐associated changes in skeletal muscles and their effect on mobility: an operational diagnosis of sarcopenia. J Appl Physiol 2003;95:1851–1860. [DOI] [PubMed] [Google Scholar]
- 6. Skelton DA, Greig CA, Davies JM, Young A. Strength, power and related functional ability of healthy people aged 65–89 years. Age Ageing 1994;23:371–377. [DOI] [PubMed] [Google Scholar]
- 7. Losa‐Reyna J, Alcazar J, Carnicero J, Alfaro‐Acha A, Castillo‐Gallego C, Rosado‐Artalejo C, et al. Impact of relative muscle power on hospitalization and all‐cause mortality in older adults. J Gerontol A Biol Sci Med Sci 2022;77:781–789. [DOI] [PubMed] [Google Scholar]
- 8. Hetherington‐Rauth M, Magalhães JP, Alcazar J, Rosa GB, Correia IR, Ara I, et al. Relative sit‐to‐stand muscle power predicts an older adult's physical independence at age of 90 yrs beyond that of relative handgrip strength, physical activity, and sedentary time: a cross‐sectional analysis. Am J Phys Med Rehabil 2022;101:995–1000. [DOI] [PubMed] [Google Scholar]
- 9. Alcazar J, Alegre LM, Suetta C, Pedro J, Van Roie E, González‐Gross M, et al. Threshold of relative muscle power required to rise from a chair and mobility limitations and disability in older adults. Med Sci Sports Exerc 2021;53:2217–2224. [DOI] [PubMed] [Google Scholar]
- 10. Orr R, de Vos NJ, Singh NA, Ross DA, Stavrinos TM, Fiatarone‐Singh MA. Power training improves balance in healthy older adults. J Gerontol A Biol Sci Med Sci 2006;61:78–85. [DOI] [PubMed] [Google Scholar]
- 11. Cadore EL, Izquierdo M. Muscle power training: a hallmark for muscle function retaining in frail clinical setting. J Am Med Dir Assoc 2018;19:190–192. [DOI] [PubMed] [Google Scholar]
- 12. Izquierdo M, Cadore EL. Muscle power training in the institutionalized frail: a new approach to counteracting functional declines and very late‐life disability. Curr Med Res Opin 2014;30:1385–1390. [DOI] [PubMed] [Google Scholar]
- 13. Coelho‐Júnior HJ, Uchida MC, Picca A, Bernabei R, Landi F, Calvani R, et al. Evidence‐based recommendations for resistance and power training to prevent frailty in community‐dwellers. Aging Clin Exp Res 2021;33:2069–2086. [DOI] [PubMed] [Google Scholar]
- 14. Alcazar J, Guadalupe‐Grau A, García‐García FJ, Ara I, Alegre LM. Skeletal muscle power measurement in older people: a systematic review of testing protocols and adverse events. J Gerontol A Biol Sci Med Sci 2018;73:914–924. [DOI] [PubMed] [Google Scholar]
- 15. Alcazar J, Losa‐Reyna J, Rodriguez‐Lopez C, Alfaro‐Acha A, Rodriguez‐Mañas L, Ara I, et al. The sit‐to‐stand muscle power test: an easy, inexpensive and portable procedure to assess muscle power in older people. Exp Gerontol 2018;112:38–43. [DOI] [PubMed] [Google Scholar]
- 16. Baltasar‐Fernandez I, Alcazar J, Mañas A, Alegre LM, Alfaro‐Acha A, Rodriguez‐Mañas L, et al. Relative sit‐to‐stand power cut‐off points and their association with negatives outcomes in older adults. Sci Rep 2021;11:19460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Alcazar J, Alegre LM, Van Roie E, Magalhães JP, Nielsen BR, González‐Gross M, et al. Relative sit‐to‐stand power: aging trajectories, functionally relevant cut‐off points, and normative data in a large European cohort. J Cachexia Sarcopenia Muscle 2021;12:921–932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Ramírez‐Vélez R, Izquierdo M, García‐Hermoso A, Ordoñez‐Mora LT, Cano‐Gutierrez C, Campo‐Lucumí F, et al. Sit to stand muscle power reference values and their association with adverse events in Colombian older adults. Sci Rep 2022;12:11820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Landi F, Calvani R, Picca A, Tosato M, Martone AM, Ortolani E, et al. Cardiovascular health metrics, muscle mass and function among Italian community‐dwellers: the Lookup 7+ project. Eur J Public Health 2018;28:766–772. [DOI] [PubMed] [Google Scholar]
- 20. Landi F, Calvani R, Martone AM, Salini S, Zazzara MB, Candeloro M, et al. Normative values of muscle strength across ages in a ‘real world’ population: results from the longevity check‐up 7+ project. J Cachexia Sarcopenia Muscle 2020;11:1562–1569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Kwakkenbos L, Imran M, McCall SJ, McCord KA, Fröbert O, Hemkens LG, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg 2014;12:1495–1499. [DOI] [PubMed] [Google Scholar]
- 22. Santos LP, Gonzalez MC, Orlandi SP, Bielemann RM, Barbosa‐Silva TG, Heymsfield SB, et al. New prediction equations to estimate appendicular skeletal muscle mass using calf circumference: results from NHANES 1999–2006. J Parenter Enteral Nutr 2019;43:998–1007. [DOI] [PubMed] [Google Scholar]
- 23. Patrizio E, Calvani R, Marzetti E, Cesari M. Physical functional assessment in older adults. J Frailty Aging 2021;10:141–149. [DOI] [PubMed] [Google Scholar]
- 24. Beaudart C, Rolland Y, Cruz‐Jentoft AJ, Bauer JM, Sieber C, Cooper C, et al. Assessment of muscle function and physical performance in daily clinical practice: a position paper endorsed by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Calcif Tissue Int 2019;105:1–14. [DOI] [PubMed] [Google Scholar]
- 25. Kuo Y‐L. The influence of chair seat height on the performance of community‐dwelling older adults' 30‐second chair stand test. Aging Clin Exp Res 2013;25:305–309. [DOI] [PubMed] [Google Scholar]
- 26. Ghasemi A, Zahediasl S. Normality tests for statistical analysis: a guide for non‐statisticians. Int J Endocrinol Metab 2012;10:486–489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Altman DG, Bland JM. Statistics notes: the normal distribution. BMJ 1995;310:298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Petry NM. A comparison of young, middle‐aged, and older adult treatment‐seeking pathological gamblers. Gerontologist 2002;42:92–99. [DOI] [PubMed] [Google Scholar]
- 29. Escourrou E, Laurent S, Leroux J, Oustric S, Gardette V. The shift from old age to very old age: an analysis of the perception of aging among older people. BMC Prim Care 2022;23:3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Suetta C, Haddock B, Alcazar J, Noerst T, Hansen OM, Ludvig H, et al. The Copenhagen Sarcopenia Study: lean mass, strength, power, and physical function in a Danish cohort aged 20–93 years. J Cachexia Sarcopenia Muscle 2019;10:1316–1329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Alcazar J, Aagaard P, Haddock B, Kamper RS, Hansen SK, Prescott E, et al. Age‐ and sex‐specific changes in lower‐limb muscle power throughout the lifespan. J Gerontol A Biol Sci Med Sci 2020;75:1369–1378. [DOI] [PubMed] [Google Scholar]
- 32. Pullman AW, Masters RC, Zalot LC, Carde LE, Saraiva MM, Dam YY, et al. Effect of the transition from high school to university on anthropometric and lifestyle variables in males. Appl Physiol Nutr Metab 2009;34:162–171. [DOI] [PubMed] [Google Scholar]
- 33. Sprake E, Lavin J, Grabowski P, Russell J, Featherstone M, Barker M. Eating habits associated with body weight gain in female university students. Br Food J 2017;119:2571–2582. [Google Scholar]
- 34. Allender S, Hutchinson L, Foster C. Life‐change events and participation in physical activity: a systematic review. Health Promot Int 2008;23:160–172. [DOI] [PubMed] [Google Scholar]
- 35. Hebl MR, Heatherton TF. The stigma of obesity in women: the difference is black and white. Pers Soc Psychol Bull 1998;24:417–426. [Google Scholar]
- 36. Padilla CJ, Harrigan ME, Harris H, Schwab JM, Rutkove SB, Rich MM, et al. Profiling age‐related muscle weakness and wasting: neuromuscular junction transmission as a driver of age‐related physical decline. GeroScience 2021;43:1265–1281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Tomlinson BE, Irving D. The numbers of limb motor neurons in the human lumbosacral cord throughout life. J Neurol Sci 1977;34:213–219. [DOI] [PubMed] [Google Scholar]
- 38. Coelho‐Junior HJ, Uchida MC, Gonçalves IO, Calvani R, Rodrigues B, Picca A, et al. Age‐ and gender‐related changes in physical function in community‐dwelling Brazilian adults aged 50 to 102 years. J Geriatr Phys Ther 2021;44:E123–E131. [DOI] [PubMed] [Google Scholar]
- 39. Ko YC, Chie WC, Wu TY, Ho CY, Yu WR. A cross‐sectional study about the relationship between physical activity and sarcopenia in Taiwanese older adults. Sci Rep 2021;11:11488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Coelho‐Júnior HJ, Trichopoulou A, Panza F. Cross‐sectional and longitudinal associations between adherence to Mediterranean diet with physical performance and cognitive function in older adults: a systematic review and meta‐analysis. Ageing Res Rev 2021;70:101395. [DOI] [PubMed] [Google Scholar]
- 41. Pana A, Sourtzi P, Kalokairinou A, Pastroudis A, Chatzopoulos ST, Velonaki VS. Association between muscle strength and sleep quality and duration among middle‐aged and older adults: a systematic review. Eur Geriatr Med 2021;12:27–44. [DOI] [PubMed] [Google Scholar]
- 42. Izzo A, Massimino E, Riccardi G, Della PG. A narrative review on sarcopenia in type 2 diabetes mellitus: prevalence and associated factors. Nutrients 2021;13:183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. von Haehling S, Morley JE, Coats AJS, Anker SD. Ethical guidelines for publishing in the Journal of Cachexia, Sarcopenia and Muscle: update 2021. J Cachexia Sarcopenia Muscle 2021;12:2259–2261. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Pearson's and Spearman's correlation coefficients of the relationship between age and lower‐extremity muscle power.
Table S2. Pearson's correlation coefficients of the relationship between age and lower‐extremity muscle power adjusted by body mass index.
Table S3. Normative values for estimated relative muscle power in men, stratified by age groups.
Table S4. Normative values for estimated allometric muscle power in men, stratified by age groups.
Table S5. Normative values for estimated specific muscle power in men, stratified by age groups.
Table S6. Normative values for estimated relative muscle power in women, stratified by age groups.
Table S7. Normative values for estimated allometric muscle power in women, stratified by age groups.
Table S8. Normative values for estimated specific muscle power in women, stratified by age groups.