

Abstract
We designed a parent-directed home-visiting intervention targeting socioeconomic status (SES) disparities in children’s early language environments. A randomized controlled trial was used to evaluate whether the intervention improved parents’ knowledge of child language development and increased the amount and diversity of parent talk. Twenty-three mother–child dyads (12 experimental, 11 control, aged 1;5–3;0) participated in eight weekly hour-long home-visits. In the experimental group, but not the control group, parent knowledge of language development increased significantly one week and four months after the intervention. In lab-based observations, parent word types and tokens and child word types increased significantly one week, but not four months, post-intervention. In home-based observations, adult word tokens, conversational turn counts, and child vocalization counts increased significantly during the intervention, but not post-intervention. The results demonstrate the malleability of child-directed language behaviors and knowledge of child language development among low-SES parents.
INTRODUCTION
Variations in early language environments have well-documented effects on children’s language development and educational outcomes (Connell & Prinz, 2002; Forget-Dubois, Dionne, Lemelin, Pérusse, Tremblay & Boivin, 2009; Huttenlocher, Vasilyeva, Cymerman & Levine, 2002; Walker, Greenwood, Hart & Carta, 1994). Children’s parents are the most important source of early language input to children and, as such, are also the primary source of variation in input.
Although there is a substantial body of research showing that early parent language input is critical to the pace of child language learning, much less is known about why parents vary in how they talk to their children. Rowe (2008) explored three factors that have the potential to explain why parents from low socioeconomic status (SES) households speak differently to their children than parents from high-SES households – differences in (1) beliefs about child development, (3) verbal ability, or (3) overall talkativeness. Rowe analyzed parent speech measures from video-recordings of forty-seven parent–child dyads and from recordings of the parents talking to the research assistant present at the session. She also measured parent verbal ability using the Vocabulary subtest of the Wechsler Adult Intelligence Scale-Revised (WAIS-R; Wechsler, 1997) and obtained parent scores on the Knowledge of Infant Development Inventory (MacPhee, 1981) survey. She found that parents who were low versus high in SES did not differ in the number of word tokens they used with the research assistant, and that parental verbal ability did not mediate the relation between SES and child-directed speech. However, parent knowledge of child development did emerge as a mediating factor between SES and child-directed speech. In general, parents whose beliefs were aligned with views expressed by pediatricians and textbooks exhibited behaviors known to facilitate child language development—these parents talked more, showed more word diversity, and produced longer utterances than parents whose views were less aligned with the pediatricians and textbooks. Although correlational, Rowe’s findings raise the possibility that changing parent knowledge about child development has the potential to influence how parents talk to their children.
Parent knowledge of child development has, in fact, been found to affect parenting behavior more generally. For example, knowledge of child rearing correlates with increased investments in parenting (Bornstein, Hendricks, Hahn, Haynes, Painter & Tamis-LeMonda, 2003) and leads to more accurate interpretations of child behaviors (Bugental & Happaney, 2002). Knowledge of child development affects mothers’ style of play with their children and correlates with children’s scores on the Bayley Scales of Infant Development (Dichtelmiller, Meisels, Plunkett, Bozytnski, Claflin & Mangelsdorf, 1992). Understanding developmental milestones is associated with exposing children to new activities, such as reading to them and telling stories (Ninio, 1997). In general, parents from higher-SES backgrounds have greater knowledge of child development and corresponding parenting practices, and they acquire and update that knowledge more readily, than do parents from lower-SES backgrounds (Stevens, 1984). Differences in parent knowledge about developmental milestones might then play a key role in determining differences in how parents from high- versus low-SES backgrounds talk to their children.
Previous interventions predicated on altering parental language behavior, however, have failed to demonstrate sustained adult behavior change or long-term positive child outcomes in low-SES populations. The literature questions the idea of successful linguistic behavior change, especially in low-income adult populations (Tannock & Girolametto, 1992). We hypothesize that previous interventions have failed because the transfer of knowledge approach did not systematically incorporate necessary behavior change strategies. The behavior change literature suggests that incorporating theoretically based behavior change techniques into the development of interventions is an essential component to help ensure success. While a transfer of knowledge is critical, it is ultimately behavior change techniques that allow knowledge to be transformed into action.
The goal of our study was to develop and assess the effectiveness of a new intervention designed to increase knowledge of language development in parents from low-SES backgrounds, and to support their language input to their children. We used techniques borrowed from the behavior change literature, including goal-setting and self-monitoring based on quantitative feedback, and modeling effective strategies, that have been found to be highly effective in changing a range of behaviors (Abraham & Michie, 2008; Michie, 2005; Michie, Jochelson, Markham & Bridle, 2009). Specifically, in addition to providing parents with key findings about language development, our intervention incorporated the following two components from the behavior change literature: (1) quantitative feedback, in this case providing parents with numerical data on how much they talk to their children; and (2) video-modeling, in this case providing strategies to increase the quantity and quality of talk to their children. We assessed the effectiveness of the intervention by examining changes in parent knowledge, as well as changes in parent linguistic behavior. To the extent possible, we also measured changes in child language outcomes.
Socioeconomic-status-related disparities in early language environments
Household socioeconomic status predicts children’s school readiness and their subsequent academic achievement (Halle et al., 2009; Hart & Risley, 1992; Hoff, 2003). On average, children from low-SES homes enter kindergarten with lower language and literacy skills than their higher-SES peers (Connell & Prinz, 2002; Dieterich, Assel, Swank, Smith & Landry, 2006; Stipek & Ryan, 1997). Moreover, this disparity persists throughout these students’ academic careers, and predicts lower high-school graduation rates and economic opportunities (Duncan & Murnane, 2011).
Although differences in the home environments of high- and low-SES families are multi-faceted, many studies implicate SES-related differences in the language children are exposed to in early childhood as a critical factor in children’s dissimilar language-learning trajectories. Definitions of SES vary widely in the literature. The studies reviewed here define SES as a measure based on education, a combination of education and income, or a combination of education and occupation. Importantly, regardless of how SES is measured, it has been found to be related to children’s language environment. For example, mothers from low-SES backgrounds produce significantly less speech and gesture than those from high-SES backgrounds (Hoff, 2003; Huttenlocher et al., 2002; Rowe & Goldin-Meadow, 2009; Walker et al., 1994). It is estimated that children living in poverty will hear thirty million fewer words by age four than their higher-SES peers (Hart & Risley, 1995). In addition to differences in quantity, the language provided to children by mothers of low-SES backgrounds has been reported to differ in quality from that of higher-SES mothers (but see Cartmill, Armstrong, Gleitman, Goldin-Meadow, Medina & Trueswell, 2013, for evidence that quality does not always correlate with SES) – shorter mean length of utterances, lower syntactic complexity, fewer open-ended questions, and more directives (Hoff, 2003, 2013; Huttenlocher, Vasilyeva, Waterfall, Vevea & Hedges, 2007). Importantly, these quantitative and qualitative differences in maternal language input have been shown to mediate the relation between SES and children’s language outcomes (Hoff, 2003).
Parenting intervention research
Parent-focused interventions have played a prominent role in the literature on disparities in early learning and development. Emphasis has typically been placed on generalized parental behaviors, such as nurturing and discipline, with child-directed language behavior a component of the intervention rather than the primary behavioral target (Brooks-Gunn & Markman, 2005). For example, programs have focused on teaching parents how to respond constructively and contingently to children’s behavioral cues, and have demonstrated positive changes in child behavior as a result of these interventions (e.g. Phillips, 2011). One of the best-documented and effective programs is the evidence-based Play and Learning Strategies (PALS), a responsive parenting intervention that has demonstrated positive socio-emotional, language, and cognitive effects on children (Landry, Smith, Swank & Guttentag, 2008).This intervention uses a trained parent facilitator and video of parent–child interaction to foster the parent–child bond and, ultimately, to promote positive child development outcomes.
Parent interventions aimed at developing child literacy skills have been a particular focus of research. Parent-directed literacy interventions typically encourage parents to read books with their children (Dickinson & McCabe, 2001; National Early Literacy Panel, 2008; Rowe, 2008; Snow, Griffin & Burns, 2005; Whitehurst, Epstein, Angell, Payne, Crone & Fischel, 1994). Book reading interventions have demonstrated significant improvements in child vocabulary and emergent literacy skills (National Early Literacy Panel, 2008; Whitehurst, Epstein et al., 1994). The success of programs such as Reach out and Read in increasing children’s receptive and expressive language skills (Klass, Dreyer & Mendelsohn, 2009) provides fertile ground for interventions designed to generalize to everyday language interactions outside of the book reading context.
Compared to efforts to improve literacy skills in typically developing children from low-SES backgrounds, parent-directed interventions for children with language delays or disabilities related to hearing loss, autism, and specific language impairment target a wider range of parental language behaviors and broader enrichment of a child’s early language environment (Kaiser & Hancock, 2003; Kashinath, Woods & Goldstein, 2006; Roberts & Kaiser, 2011). A meta-analysis of eighteen language intervention studies in which parents were trained to implement interventions with their language-delayed children demonstrated positive effects on receptive and expressive language (Roberts & Kaiser, 2011). Despite this success, Roberts and Kaiser note that the studies they reviewed focused exclusively on children with known disabilities and the majority of participants were from middle-class backgrounds, limiting the relevance of the findings to typically developing children from low-SES backgrounds. Nonetheless, the success of parent-directed language interventions for children with disabilities raises the possibility that it may be possible to change the language input that parents from low-SES backgrounds provide to their children.
The intervention curriculum
Building on the research literature cited above, we developed a parent-focused intervention aimed at enriching the quantitative and qualitative aspects of children’s early home language environment. This intervention consisted of eight educational computer-based modules that made use of the embedded behavior change techniques (quantitative linguistic feedback and video-modeling of strategies designed to increase the quantity and quality of child-directed talk) described below (see Table 1 for an overview of the content of each module). The eight intervention modules were implemented in eight weekly home visits by a trained coach working one-on-one with each parent. The eight modules were built to be implemented in sequence, with each new module building upon the content of all preceding modules. For example, three key strategies for parents to enrich their child’s home language environment, referred to as the ‘3TS’, were interwoven throughout the curriculum: TALK MORE, TUNE IN, and TAKE TURNS with your child. The 3Ts strategies and accompanying scientific justification for their effectiveness were introduced in Module 1, and then revisited throughout the remaining seven modules. The intention behind the use of the 3Ts was to provide parents with an easy-to-understand and easy-to-remember set of evidence-based strategies. Each of the seven remaining modules provided parents with specific activities that instantiated the 3Ts and could be easily implemented in everyday life. For example, book sharing (Module 5) was an opportunity to introduce new vocabulary (Talk More), converse about the contents of the book (Take Turns), and explore children’s interests (Tune In). Taken as a whole, the eight-module sequence built a toolbox of strategies and identified everyday contexts that parents could use to create an enriched home language environment for their children.
TABLE 1.
Overview of the intervention curriculum
| Module | Description |
|---|---|
| Day I | This foundational module introduced mothers to the overarching themes and concepts revisited throughout the intervention curriculum. The module included information about the critical period for language development, the lasting impact of language on the brain, and a description of quantitative linguistic feedback (Gilkerson & Richards, 2008; Hart & Risley, 1995; Suskind et al., 2013). |
| Narration | Discussed the importance of parental language input during the critical period. Concepts and strategies designed to increase adult word count through ‘talking more’ while incorporating responsive parenting behaviors, namely co-constructed narration and joint attention (Hanen Centre, 2011; Kaiser & Hancock, 2003). |
| Conversational Turns | Expanded on the concepts and skills covered in the Narration module, adding responsive parenting skills that encouraged longer conversations between mother and child (i.e. increasing wait time, increasing child-directed speech, and adjusting input to the child’s level during play) (Hanen Centre, 2011; Kaiser & Hancock, 2003). |
| Directives | Provided mothers with strategies to reduce directive language by increasing prompts and encouragements. It is important to note that this module did not evaluate parenting styles, but presented prompts and encouragements as methods for increasing amount of talk and conversational turn-taking. For example, an animation of a parent asking her child to put his shoes on by using a directive (“Go get your shoes”) is contrasted with an animation of the parent using prompts to achieve the same goal (“What do we have to put on before we go outside?”) (Landry, Smith & Swank, 2006). |
| Book Sharing | Introduced mothers to the differences between sharing a book with their child and READING a book TO their child. Dialogic book reading was modeled to provide mothers with an activity that supported parent–child interaction and increased parent language input (Whitehurst, Arnold, Epstein, Angell, Smith & Fischel, 1994; Zevenbergen & Whitehurst, 2003). |
| TV & Media Diet | Discussed the importance of reducing children’s television and screen time exposure. Described the negative impact of technology, such as cell phones, on parental language input (Christakis, Zimmerman, DiGiuseppe & McCarty, 2004). |
| Fun with Numbers | Discussed incorporating math and spatial language into everyday routines and conversations, further building mothers’ repertoire of descriptive language (Levine, Suriyakham, Rowe, Huttenlocher & Gunderson, 2010). |
| It Takes a Village | Reviewed the concepts and strategies in the previous modules. In order to further enrich the children’s language environments and harness social capital, mothers were encouraged to share what they learned with other important persons and caretakers in their children’s lives (Small, 2010). |
The educational curriculum built upon language development research, as well as the behavior change literature (Baxendale & Hesketh, 2003; Heath & Heath, 2007; Kaiser & Hancock, 2003; Michie et al., 2009). The intervention was designed to enhance parent–child interactions shown to positively impact children’s school readiness (e.g. conversational turns, responsive parenting, decontextualized language, etc.). An enriched early language environment involves more than a simple increase in the amount of talk in the home; it also involves the complex interplay of rich language and responsive parenting behaviors. Thus, the ultimate goal of this intervention was to affect not only the quantity of parent linguistic input, but also the quality of parent–child linguistic interactions, such as conversational turns and joint attention activities. This goal was instantiated in the 3Ts, which emphasize not only quantity (Talk More) but also quality and responsiveness (Tune In and Take Turns).
Importantly, the intervention was respectful of differences in parenting styles, as well as idiomatic speech and dialect. The curriculum was honed to encourage parental behaviors known to support language outcomes associated with school readiness and achievement, goals that are endorsed by parents of all SES groups in the US (Driessen, Smit & Sleegers, 2005; Stevenson, Chen & Uttal, 1990).
Knowledge of child language development
Building on Rowe’s (2008) finding that the relation between parent SES and child-directed speech is mediated by maternal knowledge of child development, the intervention strongly emphasized building parent knowledge of child language development. Consequently, the intervention focuses on teaching parents about the link between their own linguistic behavior and their child’s early language development and eventual school readiness (Hoff, 2003; Rowe, 2008). The intervention also includes discussions of the implications of early language development for a child’s educational outcomes and life-course trajectory, as well as parental strategies that are effective in enhancing children’s early language environment.
Belief in the malleability of intelligence
In addition to providing parents with strategies for creating more enriched linguistic home environments for their children, the intervention also addresses parents’ beliefs about the malleability of children’s language and cognitive skills. Parental empowerment and self-efficacy remain central to many parent-directed programs working with low-income populations, but these approaches are not sufficient if parents do not also believe that their child’s intelligence is malleable and can be positively influenced by parent input (Ajzen, 1996; DesJardin & Eisenberg, 2007; White & Wellington, 2009). Dweck (2006) has shown that individuals generally subscribe to one of two divergent lay theories of intelligence – an ‘entity theory’ or an ‘incremental theory’. Those holding an entity theory view intelligence as static and unchangeable, whereas those holding an incremental theory believe that intelligence is malleable and can be increased through effort. Moorman and Pomerantz (2010) showed that mothers’ beliefs about the malleability of intelligence can be changed: mothers who were prompted to hold an incremental mindset displayed more constructive involvement (such as asking guiding questions, waiting for their children to complete a task by themselves, or letting children correct their mistakes) in their children’s learning processes than mothers who were prompted to hold an entity mindset. Further, interventions that promote an incremental theory in the learner have been shown to enhance academic achievement among middle-school and college students (Aronson, Fried & Good, 2002; Blackwell, Trzesniewski & Dweck, 2007; Good, Aronson & Inzlicht, 2003). Based on these findings, we encouraged parents to adopt an incremental theory of intelligence by emphasizing that ‘children aren’t born smart; they’re made smart’ and that ‘parent talk is what grows their child’s brain’, as a way to motivate parents to change their own behavior for their child’s benefit. This is a critical strategy to help parents understand that their own actions can increase their child’s intelligence.
Objective, frequent feedback on performance
Altering adult behavior, especially a behavior as ingrained as language, presents a complex and significant challenge. The behavior change literature demonstrates the critical importance of incorporating well-defined, theory-driven strategies for supporting adult behavior change for an intervention to be effective (Michie et al., 2009). The intervention curriculum draws on two research-based techniques adapted from the behavior change literature – video-modeling and quantitative linguistic feedback (Janz, Champion & Stretcher, 2002; Mendelsohn et al., 2007).
Video-modeling
A key behavioral strategy of the intervention is video-modeling of the language behaviors targeted in each module. Video-modeling involves parents videotaping themselves performing (‘modeling’) an intended behavior with their child, and subsequently analyzing the video with the interventionist to gain greater insight into that behavior (Landry et al., 2008; Mendelsohn et al., 2007). We have adapted this technique for the current intervention by having the interventionist first videotape and review herself performing the target activity with the child (e.g. using prompts instead of directives), and then videotaping, and reviewing, the parent performing the same activity with the child. This adaptation transforms a potentially evaluative process into a collaborative process. At the end of each weekly module, a target activity related to the module topic is video-modeled in this way.
Quantitative linguistic feedback
Quantitative linguistic feedback is a behavioral strategy that harnesses the Language ENvironment Analysis (LENA) technology in a manner analogous to a ‘linguistic pedometer’ (Gilkerson & Richards, 2008; Sacks et al., 2014; Suskind et al., 2013). The LENA is a digital recording device and software package that tracks the number of words a child is exposed to, along with the number of conversational turns the child takes with an adult (or adults), for up to a sixteen-hour period. During each intervention visit, the measures of parent speech obtained from the LENA were presented to the parents to provide them with concrete feedback about the home language environment they were providing for their child. The LENA measures served as a type of ‘biofeedback’, allowing parents to establish concrete goals and to monitor their progress towards achieving those goals.
METHOD
The current study is a small randomized controlled trial (RCT) undertaken to assess the feasibility and efficacy of an intervention aimed at increasing parent knowledge of child language development and improving the quality and quantity of parent–child language interaction. Change in parent behavior was measured by comparing pre-intervention assessments to immediate and delayed post-intervention assessments, as described below in the Design section.
The feasibility study reported here is the foundation for a large-scale longitudinal trial. Only a longitudinal design will allow us to investigate the long-term effects of the intervention on parent’s language knowledge and behaviors and on children’s language outcomes and subsequent school readiness.
Study participants
Caregiver–child dyads were recruited from the south side of Chicago throughout the two-year RCT period. All of the caregivers in our sample were the mothers of the children under their care. Low socioeconomic status was determined through mothers’ eligibility for Medicaid and/or Women, Infants, and Children (WIC, Federal Supplemental Nutrition Program) (185% of the Federal Poverty Line) as a proxy for income. Of the 122 families recruited and assessed for study eligibility, 51 did not meet our inclusion criteria (exclusion was based on socioeconomic status: n = 7, developmental delay: n = 10, child age: n = 18, and maternal major depressive episode: n = 16). Another 24 declined to participate due to time constraints or were not reachable when research staff repeatedly attempted to contact them by phone. The remaining 37 families were randomly assigned to the control (n = 19) or experimental (n = 18) conditions. Ten families (4 experimental; 6 control) did not complete the baseline measures, 1 (experimental) dropped out of the study mid-intervention, and 3 (2 control, 1 experimental) dropped out during post-intervention follow-up, resulting in a total of 23 families who completed all study activities (12 experimental, 11 control). The participant flow chart (Figure 1) illustrates the advancement of experimental and control dyads through the intervention trial.
Fig. 1.
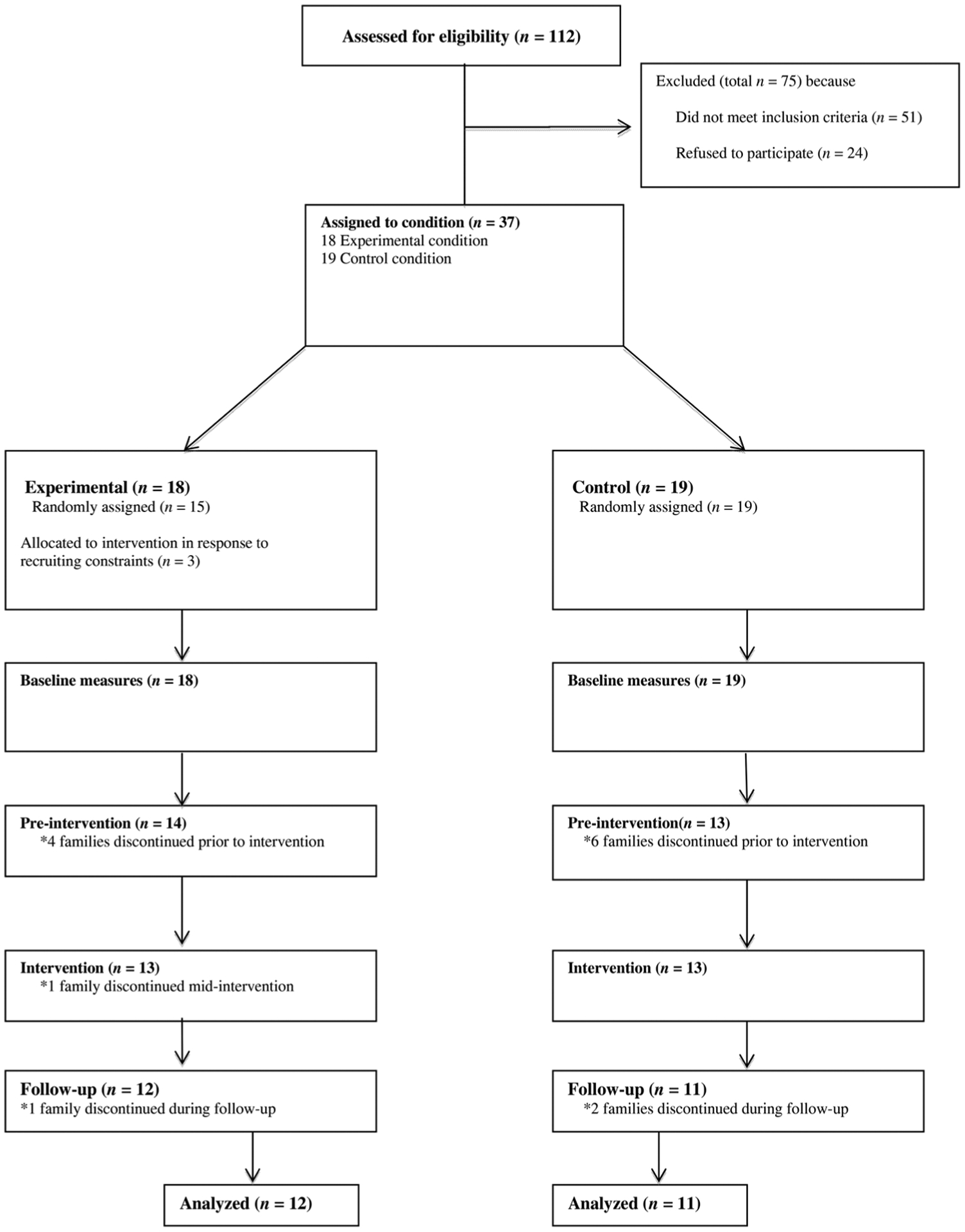
Participation from recruitment to analysis.
The sample included 9 girls (39%) and 14 boys (61%) between the ages of 1;5 and 3;0 at baseline (M = 2;2, SD = 6·0 months). Eleven children (4 girls, 7 boys; aged 2;1, SD = 5·5 months) were in the control condition and twelve children (5 girls, 7 boys; aged 2;5, SD = 4·4 months) were in the experimental condition. Birth order was distributed as follows between the two groups: in the experimental condition, children ranked M = 1·67 (SD = 0·98) and in the control condition, children ranked M = 2·18 (SD = 1·25). The children’s ages and birth orders across the two groups were not balanced (see also Table 2) due to the small sample size of this feasibility study. For analyses, parent and child outcomes were adjusted for child age. Sample size limitations precluded incorporating additional covariates (i.e. birth order, gender) into the analyses. However, there was no correlation between birth order and the number of words parents produced at baseline (r = − 0·24, n = 23, p =·29), suggesting that birth order did not impact the outcomes of this study. Mothers ranged in age from 19 to 41 years (M = 26·5 years, SD = 5·5 years). The total study period for each participating dyad was approximately six months, including baseline and follow-up assessments. All enrolled participants received compensation (Experimental: $500; Control: $200) for their involvement in the study.
TABLE 2.
Balance table
| Control | Experimental | |||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Completers | Baseline | Completers | |||||
| Variables | (n = 19) | (n = 11) | (n = 18) | (n = 12) | ||||
| Child characteristics | ||||||||
| Mean age in months (SD) | 2;0 | (6·0) | 2;1 | (6·0) | 2;4 | (6·0) | 2;5 | (4·0) |
| Gender | ||||||||
| Female (%) | 36·8 | 36·4 | 38·9 | 39·7 | ||||
| Male (%) | 63·2 | 63·6 | 61·1 | 58·3 | ||||
| Mean birth order (SD) | 2·2 | (1·3) | 1·7 | (1·0) | ||||
| Language scorea (SD) | 34·2 | (21·0) | 39·8 | (22·6) | 33·7 | (30·1) | 32·4 | (27·4) |
| Mother characteristics | ||||||||
| Mean age in years (SD) | 27·2 | (5·5) | 28·4 | (5·3) | 25·8 | (5·5) | 26·8 | (5·9) |
| Race | ||||||||
| Black (%) | 89·5 | 90·9 | 83·3 | 83·3 | ||||
| White (%) | 10·5 | 9·1 | 16·7 | 16·7 | ||||
| Household income below $15,000 (%) | 68·4 | 72·7 | 61·1 | 66·7 | ||||
| Graduated 4-year college | 10·5 | 18·1 | 11·1 | 16·7 | ||||
| Single-parent households (%) | 68·4 | 81·8 | 88·9 | 91·7 | ||||
| IQ (%)b | 92·8 | (16·1) | 92·7 | (17·4) | 94·2 | (13·5) | 95·2 | (13·5) |
| Literacyc (SD) | 10·9 | (2·9) | 11·6 | (2·2) | 10·1 | (2·8) | 10·8 | (2·3) |
| Depressiond (SD) | 5·3 | (4·2) | 5·5 | (4·2) | 5·8 | (3·0) | 6·2 | (2·8) |
| Parent stresse | 41·2 | 47·4 | 28·3 | 30·8 | ||||
| Working memoryf (SD) | 19·0 | (10·1) | 17·5 | (3·0) | 21·9 | (9·1) | 21·7 | (9·7) |
notes: The characteristics in this table that do not balance for the ‘completers’ group are the mean age of the children as well as the birth order of the children.
McArthur CDI. In the baseline sample, 14 observations in control and 16 observations in experimental group had scores for this test. In the completers sample, there were 9 observations in control and 11 in experimental group.
WASI IQ score. In the baseline sample, 13 observations in control and 17 observations in experimental group had scores for this test.
STAR-grade score. In the baseline sample, only 16 observations in control and 20 observations in experimental group had scores for this test.
CES-D-10 score.
Stress index % score.
OSPAN total score. In the baseline sample, only 17 observations in control and 18 observations in experimental group had scores for this test.
The demographics form included items probing mother and child characteristics (i.e. age, gender, ethnicity, education) and items probing the family’s home environment (i.e. number of persons in household, weekly schedule, primary caregivers). The Center for Epidemiological Studies Depression Scale (CES-D-10) was used to screen mothers for Major Depressive Disorder (MDD) because of the potential risk that MDD symptoms might confound intervention uptake (Stein et al., 2008). Appropriate referrals were offered to participants who were experiencing self-harm.
DESIGN
Experimental condition
Families in the experimental condition received eight weekly 60-minute home visits from one of two trained home visitors. Home visits included an interactive educational component (multi-media module; approximately 35 minutes), a behavior feedback component (quantitative linguistic feedback; approximately 10 minutes), an opportunity for mothers to practice new skills (video-modeling; approximately 10 minutes), and a goal-setting activity (approximately 5 minutes). The family was provided with an age-appropriate children’s book at the end of each home visit.
Educational multi-media modules
The standardized multi-media modules were presented to the parent on a laptop computer. Home visitors followed a semi-structured script that allowed for active discussion and incorporation of parent input while supporting fidelity of intervention implementation. Each of the eight multi-media modules focused on concepts and strategies that mothers could use to enrich a specific aspect of their children’s early language environment (e.g. book sharing, narration, conversations; for more detail see Table 1). Mothers were introduced to strategies for enriching children’s early language environment through easy-to-understand analogies and concrete examples. Examples of what to do, and what not to do, with a child were illustrated through animated scenarios. Books with interactive characteristics (e.g. felt letters, hidden flaps) were chosen to support child engagement and promote parent–child interaction. Books were chosen to support the goal of the module (e.g. a number book to support the Fun with Numbers module).
Quantitative linguistic feedback
In the week between modules, mothers audio-recorded a typical day (10 hours) with their child using the LENA recording system. Based on LENA’s automated analysis of the language environment (see ‘Measures‘ section, below, for a full description), mothers were given quantitative linguistic feedback in the form of easy-to-understand weekly reports. The individualized reports were designed to provide mothers with informative data about the quantity of their talk, the frequency of their communicative interactions with their child, and their progress throughout the intervention program (Suskind et al., 2013). After each recording was processed, research staff created bar graphs that outlined pertinent information from the recording and allowed for comparison to previous recording days. Each report included the daily averages of adult word counts, conversational turn counts, and television time for all recording days. For the most recent recording day, the report also included hourly averages of adult word counts and conversational turn counts. In addition to the family’s language environment, the bar graphs included information on language environment norms drawn from the LENA (v3·1·5) Natural Language Study corpus (Gilkerson & Richards, 2008). The LENA corpus is based on recordings from 329 parent–child dyads, representative of the US population with regard to parents’ education levels. It contains approximately 32,000 hours of spontaneous speech and provides normative data on adult words, child vocalizations, and adult–child conversational turns per day. According to the sample, hourly adult word counts do not change as a function of child age (M = 1,023·3, 50th percentile), whereas conversational turns and child vocalizations do (see Table 3 for percentile scores of children within the age range of this study). Parents learned to interpret their weekly LENA recording data through comparison of their word count and turn count results to the 50th, 75th, and 95th percentile values (labeled Average, Above Average, and Highest, for better understanding) from the LENA (v3·1·5) corpus. Parents were presented with these population averages in order to motivate discussion about progress, goals, and population comparisons. During these discussions, home visitors highlighted the mother’s strengths and supported her sense of self-efficacy by providing encouragement and individualized problem-solving suggestions. Conversations relating to the feedback report informed the pacing of the home visits and the mother’s weekly goal-setting.
TABLE 3.
LENA Natural Language Corpus percentiles for ages 1;5 to 3;0
| Percentile | Adult word count | Conversational turn count* | Child vocalization count* |
|---|---|---|---|
| 25th | 730·2 | 21·8–29·2 | 91·7–132·3 |
| 50th | 1,023·3 | 31·7–42·8 | 126·7–187·3 |
| 75th | 1,365·7 | 43·3–59·1 | 167·4–251·9 |
| 95th | 1,944·8 | 63·4–87·2 | 235·9–361·7 |
note:
Note that hourly adult word counts do not change as a function of child age whereas conversational turns and child vocalizations do, which is why a range is given here indicating averages for children aged 1;5 to 3;0.
Video-modeling
With the exception of the first home visit, each intervention week included a video-modeling exercise in which the home visitor modeled a desired behavior with the child. The mother then practiced the behavior with her child, and the home visitor and mother reviewed and discussed the strategies used by both the home visitor and the mother.
Goal-setting
In the final activity of each home visit, the home visitor and mother discussed the mother’s goals for the next week and scheduled the next LENA recording day, to take place prior to the next home visit. The goals reflected the intervention’s focus on increasing parent talk and conversational interaction, as well as decreasing television time. Based on the parents’ LENA feedback report and percentiles from the LENA (v3·1·5) Natural Language Study corpus, mothers and home visitors set numeric LENA recording goals for their upcoming recording. The goal-setting process happened collaboratively between mother and home visitor, driven by parents’ self-identified motivations (e.g. to maintain an ‘above average’ turn count; to build a communicative relationship with the child by tuning in; for her child to be the first family member to go to college), and directed by the home visitor to reinforce specific module content. The home visitors suggested modest, incremental goal ranges during each session to offer parents achievable goals. To reach these targets, the mother and home visitor set goals for using specific behavior strategies learned in the week’s module; e.g. the parent would target meal times to narrate and engage the child in conversational turns during food preparation, eating, and clean-up. The home visitor highlighted the mother’s strengths that might aid her in accomplishing these goals, as well as potential barriers that might impede her from incorporating the new behaviors into her daily routine. The mother then completed a goal-setting worksheet with her chosen goals, which was reviewed at the following home visit.
Control condition
The control condition consisted of a nutrition intervention that involved eight weekly home visits from a research assistant. During each home visit, the research assistant reviewed a nutrition information sheet with the mother for approximately 5–10 minutes. Although not as intensive as the 60-minute experimental condition home visits, the control and experimental conditions were equivalent in number and frequency of home visits provided. All measures (e.g. LENA, videos of parent–child interactions, knowledge of child development) that were taken with the experimental condition were also taken with the control condition. Control families did not receive books.
PROCEDURE
Study activities for both the experimental and control families included three lab observations. These observations occurred at the local university medical center before the intervention (baseline, lab-BL), one week post-intervention (lab-Post1week), and four months post-intervention (lab-Post 4mon). At these sessions, parents completed a questionnaire that assessed parents’ knowledge and beliefs about child language development, created for the purposes of this study (see ‘Measures‘ section, below, for a full description). At each of the three lab observation sessions, parent–child dyads also participated in 30-minute videotaped play sessions. These play sessions were transcribed and coded to assess parent and child language behavior.
Additional study activities included eight weekly home visits and fourteen ten-hour home observation sessions consisting of audio-recordings of the home language environment using the LENA recorders. Of the fourteen recordings, three were baseline recordings that took place just prior to the start of the intervention (home-BL), seven were weekly recordings between each of the eight weekly home visits (home-during intervention), and four were post-intervention recordings at one week post-intervention (home-Post 1week), one month post-intervention (home-Post 1mon), two months post-intervention (home-Post 2mon), and four months post-intervention (home-Post 4mon). For a week-by-week breakdown of activities in the lab and at home, see Table 4.
TABLE 4A :
Lab observations
| Timeline | Week | Control | Experimental |
|---|---|---|---|
| Lab observation: baseline (lab-BL) | 1 | Questionnaire: parent Video-recorded play session: parent & child |
Questionnaire: parent Video-recorded play session: parent & child |
| Lab observation: post-intervention 1 (lab-Post 1 week) | 12 | Questionnaire: parent Video-recorded play session: parent & child |
Questionnaire: parent Video-recorded play session: parent & child |
| Lab observation: post-intervention 2 (lab-Post 4mon) | 28 | Questionnaire: parent Video-recorded play session: parent & child |
Questionnaire: parent Video-recorded play session: parent & child |
MEASURES
Parent knowledge of child language development
A questionnaire measuring parent knowledge of child language development was developed to assess change following participation in the intervention program. Each question on the thirty-item instrument (see Table 5) was based on a specific research finding in the literature. Questions were grouped into five domains reflecting curriculum content related to language development. These domains included: language acquisition, dialogic reading practices, support for math learning, predictors of school success, and TV viewing habits. The items included statements about the potential lasting impact of parent language input (e.g. “How many words 3-year-olds know can predict how well they might do in kindergarten”), methods for maintaining child engagement in interaction (e.g. “Babies should be able to see your face when you talk to them”), and realistic expectations of child language behavior (e.g. “By the age of 3, children answer questions just as quickly as adults”). The entire instrument used a five-point Likert scale with the following response categories: (1) Strongly Disagree, (2) Disagree, (3) Neither Agree nor Disagree, (4) Agree, and (5) Strongly Agree. Each question could be scored as either (1) Correct or (0) Not Correct by collapsing the positive and negative response choices into just two categories, Agree (4 + 5), or Disagree (1 + 2). All neutral responses and unanswered questions were scored as (0) Not Correct. To calculate an overall score, each participant received a percentage of correct responses out of the total, with the highest possible score being 100% of thirty questions answered correctly.
TABLE 5.
Questionnaire items
| We would like to know what you think about young children. Circle a number to show how much you agree with the following sentences. This is what the numbers mean: | 1 = Strongly disagree with the statement |
| 2 = Somewhat disagree with the statement | |
| 3 = Unsure about the statement | |
| 4 = Somewhat agree with the statement | |
| 5 = Strongly agree with the statement | |
| Think about children aged 0–3. | |
| For these questions think about how children learn to talk. | Correct answer* |
| 1. Using baby-talk (i.e. talking in a sing-song voice) helps babies learn how to talk. | A |
| 2. Children learn fewer words when adults talk with a warm tone. | D |
| 3. Babies should be able to see your face when you talk to them. | A |
| 4. By the age of 3, children answer questions just as quickly as adults. | D |
| 5. Parents should not talk back when their toddlers use ‘baby-talk’ (like when they say “ba-ba” instead of “teddy bear”). | D |
| 6. Pointing to things is one way that babies learn how to talk. | A |
| 7. Adults cannot have conversations with babies who can’t talk yet. | D |
| 8. Children learn fewer words when they don’t pay attention to what you’re saying. | A |
| 9. Parents need to know a lot of big words to teach children how to talk. | D |
| For these questions think about reading to children. | |
| 10. You cannot teach children anything new by reading them the same book over and over. | D |
| 11. Parents who have trouble reading can help their children learn how to read books. | A |
| 12. Some books should be kept where babies can reach them. | A |
| 13. When reading with toddlers, you should always read all of the words on one page before moving on to the next page. | D |
| 14. 2-year-olds should do their best to listen quietly when you read to them. | D |
| 15. Children can learn from looking at books by themselves before they know how to read. | A |
| For these questions think about children learning math. | |
| 16. Saying numbers and counting are the only ways you can help toddlers get ready to learn math in school. | D |
| 17. Toddlers need to learn how to count before they can understand math. | D |
| 18. Talking about the difference between tall and short teaches toddlers about math. | A |
| 19. It’s best for children to wait until they are old enough for school to learn about math. | D |
| 20. Children are learning about math when they learn the names of different shapes (like triangles and squares). | A |
| For these questions think about children starting school. | |
| 21. Children who know fewer words when they start school will probably do worse in third grade than their classmates who know more words. | A |
| 22. Talking to children cannot make them smarter. | D |
| 23. How many words 3-year-olds know can predict how well they might do in kindergarten. | A |
| 24. Children should be told what to do instead of given choices. | D |
| 25. How many words 3-year-olds know cannot predict how many new words they will learn during their lifetime. | D |
| 26. Talking to 3-year-olds can help them do better in school. | A |
| 27. It’s the school’s responsibility to make sure children learn how to read and do math. | D |
| For these questions think about children watching television. | |
| 28. Watching educational TV is good for children of all ages. | D |
| 29. Having conversations with adults while watching television can help 3-year-olds learn new words. | A |
| 30. The more television children under 2 watch by themselves the more words they learn. | D |
notes:
A = Agree, D = Disagree.
The instrument was revised several times with the help of experts in the field who ensured that the content of each question appropriately reflected the current state of developmental theory. Approximately 300 participants at church fairs in low-SES neighborhoods completed the instrument in several waves. Question wording was changed in response to participant feedback about questions that were hard to understand and those that did not appropriately reflect intended question content. Reliability of the survey was assessed by analyzing test–retest stability in the control group. The control group contained thirteen participants who completed the survey at lab-BL (Time 1) and lab-Post 1week (Time 2) (this group contains two participants who were not included in the final sample). The average time elapsed between Time 1 and Time 2 was 77 days (range 50–105 days). The control participants’ overall score on the survey generated a test–retest reliability coefficient of r = 0·75 (p = ·003), suggesting that the instrument is reliable.
The instrument contained 5% passive sentences and had an overall Flesch Reading Ease score of 72·6 (SD = 16·96; on a scale of 0–100, scores close to 100 are easier to read) (Flesch, 1948; Williamson & Martin, 2010). On average, the instrument read at a 6·06 (SD = 2·24) Flesch Kincaid Grade level (a readability test of the comprehension difficulty of a standard English passage, scored as the normative reading level for US school grades). The questionnaire was self-administered. All parents were literate: on the STAR reading assessment (Algozzine, Wang & Boukhtiarov, 2011; Renaissance Learning, 2014), parents in the experimental group scored at an average grade level of M = 10·83 (SD = 2·3) and parents in the control group scored at M = 11·62 (SD = 2·18). Reading levels did not significantly differ between groups.
Lab observations (30-minute recordings)
Each parent–child dyad participated in three 30-minute play sessions over the course of the trial (lab-BL, lab-Post 1week, and lab-Post 4mon). At each play session, the parent and child were given a standardized set of toys (e.g. a puzzle, wooden blocks, and toy animals) and the book Goodnight Moon. Research staff suggested that parents read and play with their child.
A trained research assistant transcribed and coded each 30-minute video using a coding system developed to describe language in home observations of mother–child interactions from ages 1;2 to 4;10 (Goldin-Meadow, Levine, Hedges, Huttenlocher, Raudenbush & Small, 2014). At the time of transcription and coding, the research assistant was blind to participant condition and to the time-point of the video. All meaningful sounds from the mother and child were transcribed. Child and adult sounds that were used to refer to events, properties, entities, onomatopoeia, or evaluations were considered words (Sauer, Levine & Goldin-Meadow, 2010). A second coder, also blind to participant condition and to the time-point of the video, transcribed 25% of the videos. Word agreement between the two coders was 77% and utterance agreement was 80%.
Measures of how much talk mother and child produced (number of words (tokens) and number of utterances), a measure of word diversity (number of different words (types)), and a measure of sentence length (mean length of utterance in words (MLUw)) were analyzed. An utterance refers to any single speech act preceded and followed by a pause, a change in conversational turn, or a change in intonational pattern. Word tokens refer to the total number of words spoken, and word types refer to the number of unique words spoken. Morphologically inflected variants of words (e.g. run, running) were counted as a single word type. Words produced in imitation of the mother were included in the count of child word types because children typically only imitate words that they spontaneously produce themselves (Slobin & Welsh, 1967).
Home observations (10-hour recordings)
The LENA system includes audio-recording devices and specialized processing software that automates the gathering and analysis of quantitative data on child vocalizations, adult vocalizations, background noise, and parent–child interaction in the home environment (Gilkerson & Richards, 2008; Greenwood, Thiemann-Bourque, Walker, Buzhardt & Gilkerson, 2011). The LENA audio-recorder, the Digital Language Processor (DLP), records up to sixteen consecutive hours of audio data. It is worn by the child in the front pocket of a t-shirt designed specifically for use with the LENA system. The DLP remains in the t-shirt pocket for the length of the recording, allowing the LENA system to identify the target child’s vocalizations and interactions, as well as the vocalizations of interlocutors. The LENA software then processes the encrypted audio information on the DLP.
The LENA software uses previously tested and verified algorithms to categorize vocalizations (Xu, Gilkerson, Richards, Yapanel & Gray, 2009). Three major categories of LENA data were analyzed: adult word count, child vocalization count, and conversational turn count. Adult word count is an estimate of the total number of words spoken by an adult within hearing range of the target child. Conversational turn count measures adult–child linguistic interaction by estimating the number of verbal exchanges that occur between child and adult. Child vocalization count is an estimate of the total number of vocalizations from the target child. The LENA uses child age to set parameters for labeling a child’s sound as a vocalization (Gilkerson & Richards, 2008; Xu et al., 2009).
RESULTS
Intervention effects on parent knowledge and lab observation outcomes
We first examined the effects of the intervention on parent knowledge of child language development (based on the questionnaire) and on parent and child language behaviors (based on the video-coded observations of parent–child interactions in the lab). Each of these outcomes was measured at the three time points – lab-BL, lab-Post 1week, and lab-Post 4mon. Table 6 displays the means and standard deviations at the three observation points for the questionnaire and the parent and child lab observation measures.
TABLE 6.
Means and standard deviations for the knowledge questionnaire and lab observation outcomes over study period
| Lab-BL M(SD) | Lab-Post 1week M(SD) | Lab-Post 4mon M(SD) | ||||
|---|---|---|---|---|---|---|
| Experimental group (n = 12) | ||||||
| Questionnaire score | 19·00 | (3·00) | 21·31** | (5·2) | 21·33** | (3·9) |
| Parent utterances per 30mm | 565·01 | (119·10) | 615·03* | (77·89) | 582·52 | (137·20) |
| Parent MLUw per 30mm | 3·48 | (0·52) | 3·72 | (0·41) | 3·74 | (0·45) |
| Parent word tokens per 30mm | 2075·90 | (400·28) | 2404·08** | (422·89) | 2335·90 | (506·81) |
| Parent word types per 30mm | 288·14 | (30·23) | 336·25*** | (47·43) | 332·80 | (61·57) |
| Child utterances per 30mm | 255·90 | (76·56) | 334·72 | (81·87) | 350·79 | (113·58) |
| Child MLUw per 30mm | 1·81 | (0·47) | 2·10 | (0·56) | 2·33 | (0·50) |
| Child word tokens per 30min | 507·02 | (210·902) | 787·29* | (301·62) | 904·18 | (345·3) |
| Child word types per 30min | 125·03 | (36·76) | 168·91*** | (45·97) | 182·41* | (40·78) |
| Control group (n = 11) | ||||||
| Questionnaire score | 19·18 | (3·90) | 17·80 | (5·60) | 18·00 | (5·3) |
| Parent utterances per 30min | 573·79 | (156·80) | 522·25 | (132·60) | 503·61 | (109·9) |
| Parent MLUw per 30min | 3·52 | (1·22) | 3·19 | (0·50) | 3·43 | (0·7) |
| Parent word tokens per 30min | 1970·00 | (538·90) | 1828·10 | 581·20 | 1852·00 | (608·8) |
| Parent word types per 30min | 280·26 | (68·70) | 260·09 | (66·80) | 283·15 | (83·3) |
| Child utterances per 30min | 210·35 | (101·40) | 260·14 | (128·10) | 274·07 | (103·1) |
| Child MLUw per 30min | 1·69 | (0·49) | 1·77 | (0·60) | 2·02 | (0·6) |
| Child word tokens per 30min | 384·46 | (270·30) | 541·26 | (380·20) | 616·06 | (317·5) |
| Child word types per 30min | 101·22 | (44·70) | 109·88 | (52·30) | 131·12 | (48·8) |
notes:
p < ·1;
p < ·05;
p < ·01.
We examined whether the intervention had a positive effect on parent and child outcomes at lab-Post 1week and at lab-Post 4mon. For each of the outcome measures displayed in Table 6, we estimated the effects of the intervention by conducting separate ordinary least squares (OLS) regressions with a cluster-correction to account for shared variance arising from the repeated measures design. Each regression included dummy variables for GROUP (Control vs. Experimental), lab-POST 1WEEK (BL vs. Post 1week), and lab-POST 4MON (BL vs. Post 4mon). In addition, each regression included two Group × Time interaction terms. The first interaction term (Group × Post 1WEEK) reflects the impact of the intervention calculated one week after its conclusion. The second interaction term (Group × Post 4MON) reflects the impact of the intervention calculated four months after its conclusion. Each regression also included a covariate for child age (in months), as child age was not balanced across experimental groups (Table 2). While there were potential precision gains to be had from controlling for additional baseline covariates (e.g. birth order, gender), sample size limitations precluded us from incorporating additional covariates into the analyses.
The results of these regression models are presented in Table 7. First, a significant Group × Post 1WEEK interaction effect demonstrated that the intervention had a statistically significant impact at lab-Post 1week on the following parent outcomes: questionnaire score (β = 3·69, t(62) = 2·06, p < ·05, d = 0·49); number of parent word tokens (β = 561·0, t(61) = 2·30, p < ·03, d = 0·88); number of parent word types (β = 68·3, t(61) = 3·23, p < ·01, d = 0·72); and number of child word types (β = 35·2, t(61) = 3·38, p < ·01, d = 0·75). The intervention had a marginally significant effect on the number of parent utterances (β = 101·7, t(61) = 1·98, p < ·06, d = 0·52), and the number of child word tokens (β = 123·5, t(61) = 1·73, p < ·10, d = 0·57). Cohen’s effect size values (based on sample means and pooled standard deviation) suggest a moderate to high practical significance for all of these interaction effects.
TABLE 7.
Effect of group on intervention and lab observation outcomes (n = 69 observations)
| Outcome variables | Coefficients | Model | |||
|---|---|---|---|---|---|
| β | SE | F stat | dF | R-squared | |
| Questionnaire | 1·22 | 61 | 0·1003 | ||
| Group | −0·36 | 2·01 | |||
| Lab-Post 1week | −1·38* | 0·75 | |||
| Lab-Post 4mon | −1·18 | 0·79 | |||
| Group*Lab-Post 1 weeka | 3·69** | 1·79 | |||
| Group*Lab-Post 4monb | 3·52** | 1·52 | |||
| Child age | 0·04 | 0·21 | |||
| Parent utterances | 2·16 | 61 | 0·0870 | ||
| Group | −12·8 | 61·8 | |||
| Lab-Post 1week | −51·5 | 32·3 | |||
| Lab-Post 4mon | −70·1* | 34·4 | |||
| Group*Lab-Post 1 weeka | 101·7* | 51·4 | |||
| Group*Lab-Post 4monb | 87·6 | 52·1 | |||
| Child age | 0·90 | 5·1 | |||
| Parent MLUw | 8·44 | 61 | 0·1972 | ||
| Group | −0·26 | 0·36 | |||
| Lab-Post 1week | −0·34 | 0·35 | |||
| Lab-Post 4mon | −0·08 | 0·33 | |||
| Group*Lab-Post 1 weeka | 0·57 | 0·37 | |||
| Group*Lab-Post 4monb | 0·33 | 0·36 | |||
| Child age | 0·05** | 0·02 | |||
| Parent word tokens | 2·84 | 61 | 0.2593 | ||
| Group | −27·5 | 205·2 | |||
| Lab-Post 1week | −141·9 | 157·7 | |||
| Lab-Post 4mon | −115·6 | 160·6 | |||
| Group*Lab-Post 1 weeka | 561·0** | 243·6 | |||
| Group*Lab-Post 4monb | 375·6 | 244·0 | |||
| Child age | 29·7 | 20·6 | |||
| Parent word types | 8·85 | 61 | 0·4088 | ||
| Group | −20·9 | 24·3 | |||
| Lab-Post 1week | −20·2 | 15·7 | |||
| Lab-Post 4mon | 3·41 | 21·5 | |||
| Group*Lab-Post 1 weeka | 68·3*** | 21·1 | |||
| Group*Lab-Post 4monb | 41·2 | 25·7 | |||
| Child age | 6·4** | 2·4 | |||
| Child utterances | 17·14 | 61 | 0·3351 | ||
| Group | 10·2 | 37·9 | |||
| Lab-Post 1week | 49·8** | 21·9 | |||
| Lab-Post 4mon | 64·4 | 38 | |||
| Group*Lab-Post 1 weeka | 29·0 | 30·9 | |||
| Group*Lab-Post 4monb | 39·5 | 41·1 | |||
| Child age | 7·9*** | 2·7 | |||
| Child MLUw | 11·36 | 61 | 0·3662 | ||
| Group | −0·11 | 0·21 | |||
| Lab-Post 1week | 0·08 | 0·13 | |||
| Lab-Post 4mon | 0·34 | 0·14 | |||
| Group*Lab-Post 1 weeka | 0·21 | 0·17 | |||
| Group*Lab-Post 4monb | 0·18 | 0·16 | |||
| Child Age | 0·05*** | 0·01 | |||
| Child word tokens | 26·76 | 61 | 0·1433 | ||
| Group | −0·15 | 109·5 | |||
| Lab-Post 1week | 156·8*** | 45·1 | |||
| Lab-Post 4mon | 233·8*** | 103·9 | |||
| Group*Lab-Post 1weeka | 123·5* | 71·3 | |||
| Group*Lab-Post 4monb | 163·3 | 114·5 | |||
| Child age | 27·4*** | 20·6 | |||
| Child word types | 38 | 61 | 0·5990 | ||
| Group | −1·56 | 16·0 | |||
| Lab-Post 1week | 8·6 | 7·8 | |||
| Lab-Post 4mon | 30·4** | 13·8 | |||
| Group*Lab-Post 1weeka | 35·2*** | 10·4 | |||
| Group*Lab-Post 4monb | 27·0* | 15·0 | |||
| Child age | 5·7*** | 1·0 | |||
notes: This model uses an interaction variable to isolate the effect of experimental group on the outcome from the effect of the time period. The coefficient we show is the effect of experimental group on the outcome, in the given time interval.
Knowledge questionnaire outcomes are raw scores and lab observation outcomes are normalized to a 30-minute length.
Interaction between group and lab-Post 1week.
Interaction between group and lab-Post 4mon.
p < ·1,
p < ·05,
p < ·01.
Second, we examined the Group × lab-Post 4MON interaction term to determine whether the intervention had a positive effect at lab-Post 4mon, for parents or children. Intervention effects were not as strong at this time point as they were at lab-Post 1week. The Group × lab-POST 4MON interaction term only reached statistical significance for the parent questionnaire score (β = 3·52, t(62) = 2·31, p < ·03, d = 0·51) and marginal significance for the number of child word types (β = 27·0, t(61) = 1·81, p < ·08, d = 1·12). Cohen’s effect size values (based on sample means and pooled standard deviation) suggested a moderate to high practical significance for these interaction effects.
No statistically significant intervention effect was found at either lab-Post 1week or lab-Post 4mon for the remaining child lab observation measures (number of child utterances and child MLUw) or for parent MLUw.
Parent knowledge questionnaire results in detail
On average, the control group questionnaire scores did not significantly differ between lab visits. Control group participants answered 63% (SD = 27%) of questions correctly at lab-BL. At lab-Post 1week, control participants provided 59% (SD = 26%) correct answers, and at lab-Post 4mon, they answered 60% (SD = 26%) correctly. In contrast, the experimental group participants answered 60% (SD = 32%) of questions correctly at lab-BL, and increased to 71% (SD = 19%) at the lab-Post 1week visit, a significant difference that was maintained at lab-Post 4mon visit (M = 72%, SD = 22%). On average, the experimental group showed an increase of 10 percentage points in correct answers in each of the five subsections of the questionnaire at their lab-Post 1week and 4mon visits, whereas control participants’ scores remained unchanged.
Prior to the manipulation (at baseline), both the experimental and control groups answered the same questions correctly on the questionnaire and showed a high degree of overlap (⩾75% of parents answered correctly in both groups). In the How children learn to talk section, participants in both groups knew that it is not the case that children learn fewer words when adults talk in a warm tone (Q2) or that parents need to know a lot of big words in order to support a child’s language learning (Q9). Participants answered correctly that babies should see their face when they talk to them (Q3), and that they can have conversations with babies too young to talk (Q7). In the thinking about reading to children section, participants in both the control and the experimental group knew that children can learn from reading the same book over and over (Q10), that books should be kept within babies’ reach (Q12), and that children can learn from looking at books by themselves even before they can read (Q15). In the Children starting school section, participants in both groups answered correctly that talking to children helps them learn (Q22) and do better in school (Q26), and that it is not only the school’s responsibility to help children learn to read and do math (Q27). Thus, the control and experimental groups responded in roughly the same ways on the questionnaire before the intervention.
However, after the intervention, parents in the experimental group showed an increase of ⩾25 percentage points from their lab-BL visit to their lab-Post 1week and 4mon visits on ten questionnaire items (see Table 5), whereas the control group did not show this magnitude of gain on any item. In the How children learn to talk section, more parents agreed after the intervention that child-directed speech supports language learning (Q1) and that children learn more in joint attentional settings (Q8). In the Thinking about reading to children section, more parents now disagreed that reading all the words on a page is necessary (Q13), and that toddlers should sit quietly during reading sessions (Q14). In the Children learning math section, more parents now agreed that talking about tall and short (Q18) as well as learning the names of shapes (Q20) are beneficial for math learning. In the Children starting school section, more parents agreed that knowing fewer words upon school entry leads to worse outcomes in third grade (Q21) and that the number of words a child knows by age three predicts how well the child will do in kindergarten (Q23). Finally, in the Children watching television section, more parents now disagreed that educational TV is good for children of all ages (Q28), and that children under two learn words from watching TV alone (Q30). Participants in the control group did not show increases of ⩾25 percentage points on any of the thirty questionnaire items.
Intervention effects on home observation outcomes
We next examined the effects of the intervention on the LENA outcomes (adult word count, conversational turn count, and child vocalization count). We conducted separate OLS regressions for each LENA outcome. Table 8 displays the means and standard deviations of the home observation measures calculated at the following study periods: Baseline (home-BL = 3 recordings), During-Intervention (7 recordings), and Post-Intervention (home-Post 1week, 2mon, 3mon, 4mon = 4 recordings).
TABLE 8.
Means and standard deviations for the home observations measures over study period
| Home-BL M (SD) |
During intervention M (SD) |
Home-Post M (SD) |
||||
|---|---|---|---|---|---|---|
| Experimental group (n = 12) | ||||||
| Adult word count | 685·36 | (386·83) | 946·22*** | (456·78) | 819·10 | (465·76) |
| Conversational turn count | 26·24 | (16·96) | 41·95*** | (20·83) | 35·14 | (19·72) |
| Child vocalization count | 14·36 | (79·05) | 162·01** | (78·9) | 160·45 | (79·54) |
| Control group (n = 11) | ||||||
| Adult word count | 861·70 | (413·00) | 809·91 | (437·66) | 808·93 | (396·62) |
| Conversational turn count | 28·73 | (15·29) | 29·46 | (16·54) | 28·64 | (18·67) |
| Child vocalization count | 117·39 | (58·86) | 126·28 | (66·17) | 123·91 | (73·82) |
NOTES:
p < ·05,
p < ·01.
Each regression included dummy variables for Group (Control vs. Experimental), During-Intervention (home-BL vs. During-Intervention), and Post-Intervention (BL vs. home-Post 1week, 2mon, 3mon, 4mon). As noted above, there were three recordings during the Baseline period, seven during the Intervention period, and four during the Post-Intervention period (see Table 4b). Each regression also included two Group × Time interaction terms. The first interaction term (Group × During-Intervention) represents the impact of the intervention calculated during the Intervention period. The second interaction term (Group × Post-Intervention) represents the impact of the intervention measured after the intervention’s conclusion. All OLS specifications included a covariate for child age (in months). Results of these regression models are displayed in Table 9.
TABLE 4B :
Home observations
| Timeline | Week | Control | Experimental |
|---|---|---|---|
| Home observation: baseline (home-BL) | 1 | LENA baseline recording 1 | LENA baseline recording 1 |
| 2 | LENA baseline recording 2 | LENA baseline recording 2 | |
| 3 | LENA baseline recording 3 | LENA baseline recording 3 | |
| Intervention | 4 | Nutrition curriculum week 1+ LENA recording 4 | Intervention curriculum week 1 + LENA recording 4 |
| 5 | Nutrition curriculum week 2 + LENA recording 5 | Intervention curriculum week 2 + LENA recording 5 | |
| 6 | Nutrition curriculum week 3 + LENA recording 6 | Intervention curriculum week 3 + LENA recording 6 | |
| 7 | Nutrition curriculum week 4 + LENA recording 7 | Intervention curriculum week 4 + LENA recording 7 | |
| 8 | Nutrition curriculum week 5 + LENA recording 8 | Intervention curriculum week 5 + LENA recording 8 | |
| 9 | Nutrition curriculum week 6 + LENA recording 9 | Intervention curriculum week 6 + LENA recording 9 | |
| 10 | Nutrition curriculum week 7 + LENA recording 10 | Intervention curriculum week 7 + LENA recording 10 | |
| 11 | Nutrition curriculum week 8 | Intervention curriculum week 8 | |
| Home observation: post-intervention 1 (home-Post 1 week) | 12 | LENA recording 11 | LENA recording 11 |
| Home observation: post-intervention 2 (home-Post 1 mon) | 16 | LENA recording 12 | LENA recording 12 |
| Home observation: post-intervention 3 (home-Post 2mon) | 20 | LENA recording 13 | LENA recording 13 |
| Home observation: post-intervention 4 (home-Post 4mon) | 28 | LENA recording 14 | LENA recording 14 |
TABLE 9.
Effect of group on home observation outcomes (n = 364 observations)
| Adult word count | Conversational turn count | Child vocalization count | ||||
|---|---|---|---|---|---|---|
| Variables | β | SE | β | SE | β | SE |
| Coefficients | ||||||
| Experimental group | −147·05 | 163·3 | −0·83 | 6·8 | −3·8 | 28·16 |
| During-interventiona | −51·8 | 66.6 | 0·73 | 1·4 | 8·88 | 6·96 |
| Post-interventionb | −51·4 | 97.3 | −0·02 | 3·567 | 6·48 | 12·61 |
| Group*During-Interventionc | 312·7*** | 113·0 | 15·0*** | 3·3 | 38·77** | 17·31 |
| Group*Post-interventiond | 185·2 | 128 | 8·90 | 6·22 | 39·61 | 27·12 |
| Child age | −6·5 | 10.4 | −0·35 | 0·57 | 0·17 | 2·02 |
| Model statistics | ||||||
| F-statistic | 3·01 | 5·16 | 2·28 | |||
| dF | 315 | 305 | 315 | |||
| R-squared | 0·0369 | 0·1003 | 0·069 | |||
notes: This model uses an interaction variable to isolate the effect of experimental group on the outcome from the effect of the time period. The coefficient we show is the effect of experimental group on the outcome, in the given time interval.
All standard errors are cluster-corrected at the individual level.
During-intervention measures recordings during the intervention.
Post-intervention measures recordings 1 week, 1month, 2 months, and 4 months after intervention.
Interaction between experimental group and during-intervention.
Interaction between experimental group and post-intervention.
p < ·05,
p < ·01.
A significant Group × Intervention effect was found for all three home observation outcomes that occurred during the course of the intervention: adult word count (β = 312·7, t(315) = 2·77, p < ·01, d = 0·34); conversational turn count (β = 15·0, t(315) = 4·54, p < ·01, d = 0·66); and child vocalization count (β = 38·77, t(315) = 2·24, p < ·04, d = 0·43). Cohen’s effect size values (based on sample means and pooled standard deviation) suggested a moderate practical significance for these interaction effects.
Figure 2 displays the temporal pattern of intervention effects on the home observation outcomes over the course of the study period. These results suggest that the intervention began having impacts early in the intervention period, and that these impacts were sustained throughout the intervention period prior to attenuating after the intervention ended.
Fig. 2.
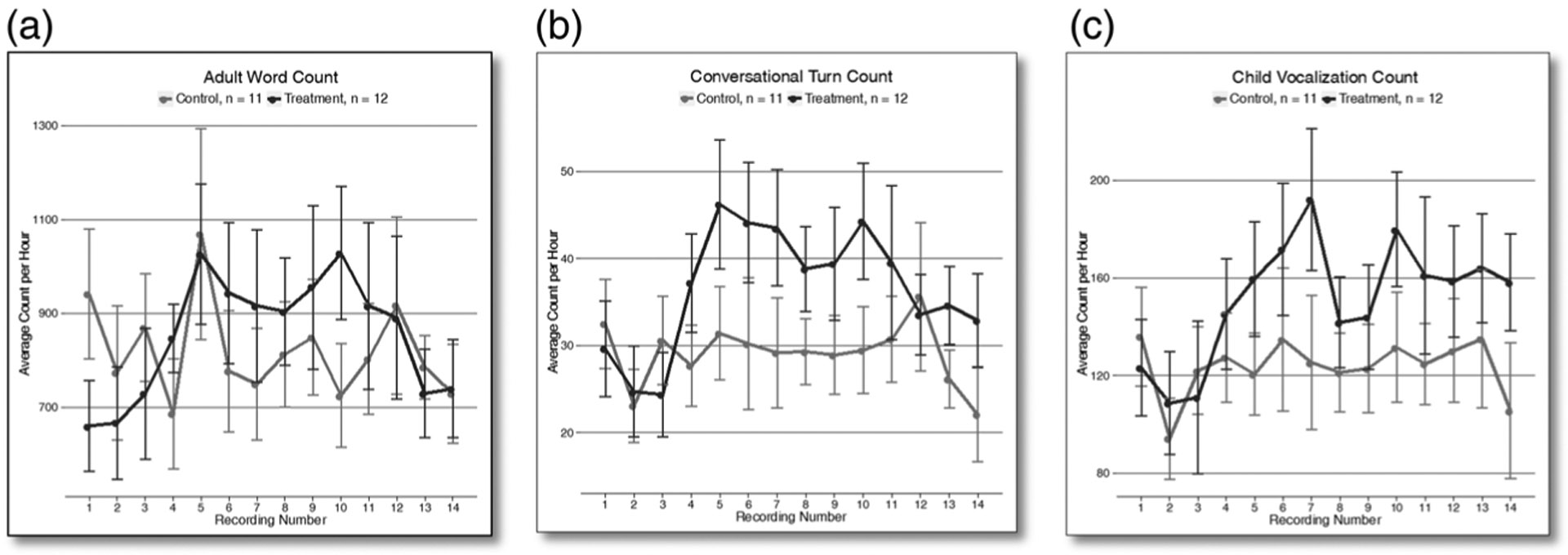
The temporal pattern of intervention effects on LENA outcomes over study period.
We next examined the impact of the intervention on the four home observations that occurred after the intervention was completed (home-Post 1week, 2mon, 3mon, 4mon). None of the Group × Post-Intervention terms were statistically significant at conventional levels of significance (p < ·05).
Determining the impact of parental knowledge on parent language outcomes
Post-hoc regressions confirm that mothers’ questionnaire score is a statistically significant mediator of the intervention’s effect on the lab-observation outcomes parent word tokens (β = 34·8, t(60) = 2·04, p < ·05), and parent word types (β = 3·63, t(60) = 2·15, p < ·05) (see Table 10), and a marginally significant mediator of the intervention’s effect on the home observation outcome LENA conversational turn count (β = 0·39, t(307) = 1·72, p < ·1) (see Table 11). Our small sample size prevented us from including this variable as a covariate in all regression models, yet these post-hoc results provide additional confirmation that the intervention modified mothers’ beliefs about the cognitive development of their children, which in turn led to positive patterns of mother–child interaction.
TABLE 10.
Lab observation outcomes with questionnaire score as a covariate
| Coefficients | Model | ||||
|---|---|---|---|---|---|
| Outcome variables | β | SE | F stat | dF | R-squared |
| Parent utterances | 2·62 | 60 | 0·1248 | ||
| Group | −10·9 | 62·2 | |||
| Lab-Post 1week | −43·9 | 29·2 | |||
| Lab-Post 4mon | −60·2* | 31·9 | |||
| Group*Lab-Post 1weeka | 81·2 | 49·0 | |||
| Group*Lab-Post 4monb | 64·8 | 52·2 | |||
| Questionnaire score | 5·54 | 5·03 | |||
| Child age | 0·7 | 4·87 | |||
| Parent word tokens | 4·85 | 60 | 0·3294 | ||
| Group | −15·7 | 208·7 | |||
| Lab-Post 1week | −94·0 | 151·8 | |||
| Lab-Post 4mon | −53·7 | 155·7 | |||
| Group*Lab-Post 1weeka | 432·6* | 244·0 | |||
| Group*Lab-Post 4monb | 232·6 | 246·8 | |||
| Questionnaire score | 34.8** | 17·0 | |||
| Child age | 28·5 | 18·0 | |||
| Parent word types | 10·04 | 60 | 0·4647 | ||
| Group | −19·6 | 23·1 | |||
| Lab-Post 1week | −15·2 | 16·2 | |||
| Lab-Post 4mon | 9·9 | 20·9 | |||
| Group*Lab-Post 1weeka | 54·9** | 23·4 | |||
| Group*Lab-Post 4monb | 26·3 | 26·8 | |||
| Questionnaire score | 3·63** | 1·69 | |||
| Child age | 6·28*** | 2·00 | |||
notes: This model uses an interaction variable to isolate the effect of experimental group on the outcome from the effect of time period. The coefficient we show is the effect of experimental group on the outcome, in the given time interval.
Knowledge questionnaire outcomes are raw scores and lab observation outcomes are normalized to a 30-minute length.
Interaction between group and lab-Post 1week.
Interaction between group and lab-Post 4mon.
p < ·1,
p < ·05,
p < ·01.
TABLE 11.
Home observation outcomes with questionnaire score as a covariate
| Adult word count | Conversational turn count | |||
|---|---|---|---|---|
| Variables | β | SE | β | SE |
| Coefficients | ||||
| Experimental group | −143·4 | 162·0 | −0·58 | 6·76 |
| During-interventiona | −42·9 | 64·8 | 1·68 | 1·47 |
| Post-interventionb | −112·0 | 76·0 | −3·50 | 2·96 |
| Group*During-interventionc | 288·8*** | 110·0 | 12·43*** | 4·11 |
| Group*Post-interventiond | 230·6** | 105·8 | 10·79* | 5·56 |
| Questionnaire score | 6·46 | 8·75 | 0·69* | 0·40 |
| Child age | −7·08 | 9·71 | −0·40 | 0·50 |
| Model statistics | ||||
| F-statistic | 2·56 | 9·26 | ||
| dF | 307 | 307 | ||
| R-squared | 0·0494 | 0·1554 | ||
notes: This model uses an interaction variable to isolate the effect of experimental group on the outcome from the effect of time period. The coefficient we show is the effect of experimental group on the outcome, in the given time interval.
All standard errors are cluster-corrected at the individual level.
During-intervention measures recordings during the intervention.
Post-intervention measures recordings 1 week, 1month, 2 months, and 4 months after intervention.
Interaction between experimental group and during-intervention.
Interaction between experimental group and post-intervention.
p < ·1,
p < ·05,
p < ·01.
Comparison of participants’ home observation averages and LENA (v3.1·5) Natural Language Corpus percentiles
During the intervention period, participants in the experimental condition were provided with feedback on their weekly LENA scores, together with a report of how their scores compared to population-level averages (Gilkerson & Richards, 2008). Participants saw line graphs representing the 50th, 75th, and 95th percentile for adult word count and conversational turn count (see Table 3 for percentile scores for the age range of this study).
To provide a closer look at individual growth trajectories, in Figures 3 and 4 we compare both groups’ adult word counts and conversational turn counts to LENA population averages, grouped into five percentile ranks: (1) below 25%, (2) 25th–49thth, (3) 50th–74th, (4) 75th–94th, (5) 95th and beyond. For completeness, in Figure 5, we compare both groups’ child vocalization counts to LENA population averages.
Fig. 3a–c.
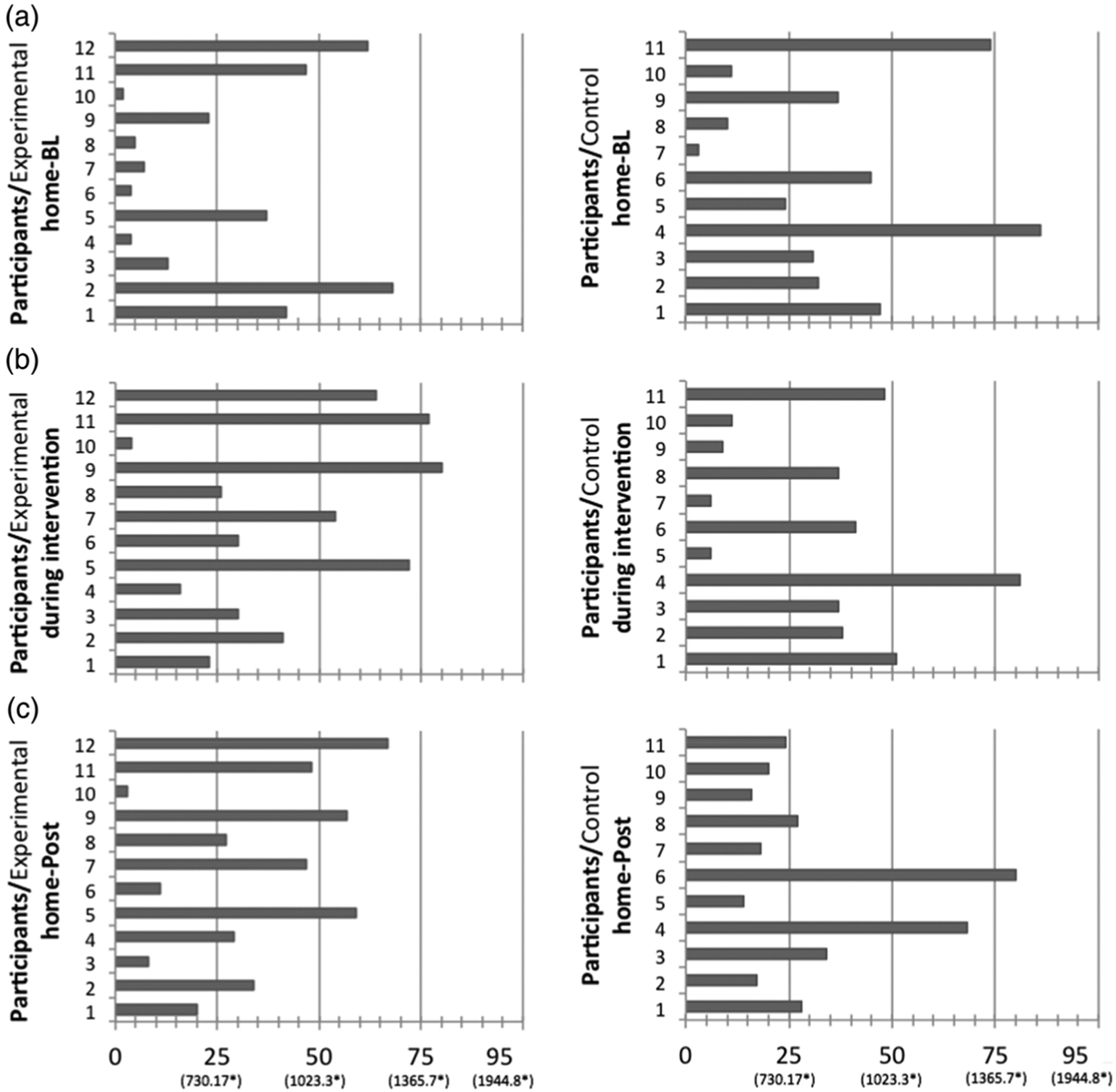
Experimental participants’ (n = 12) and control participants’ (n = 11) hourly adult word count averages and hourly LENA (v3·1·5) Natural Language Corpus percentiles.*
Fig. 4a–c.
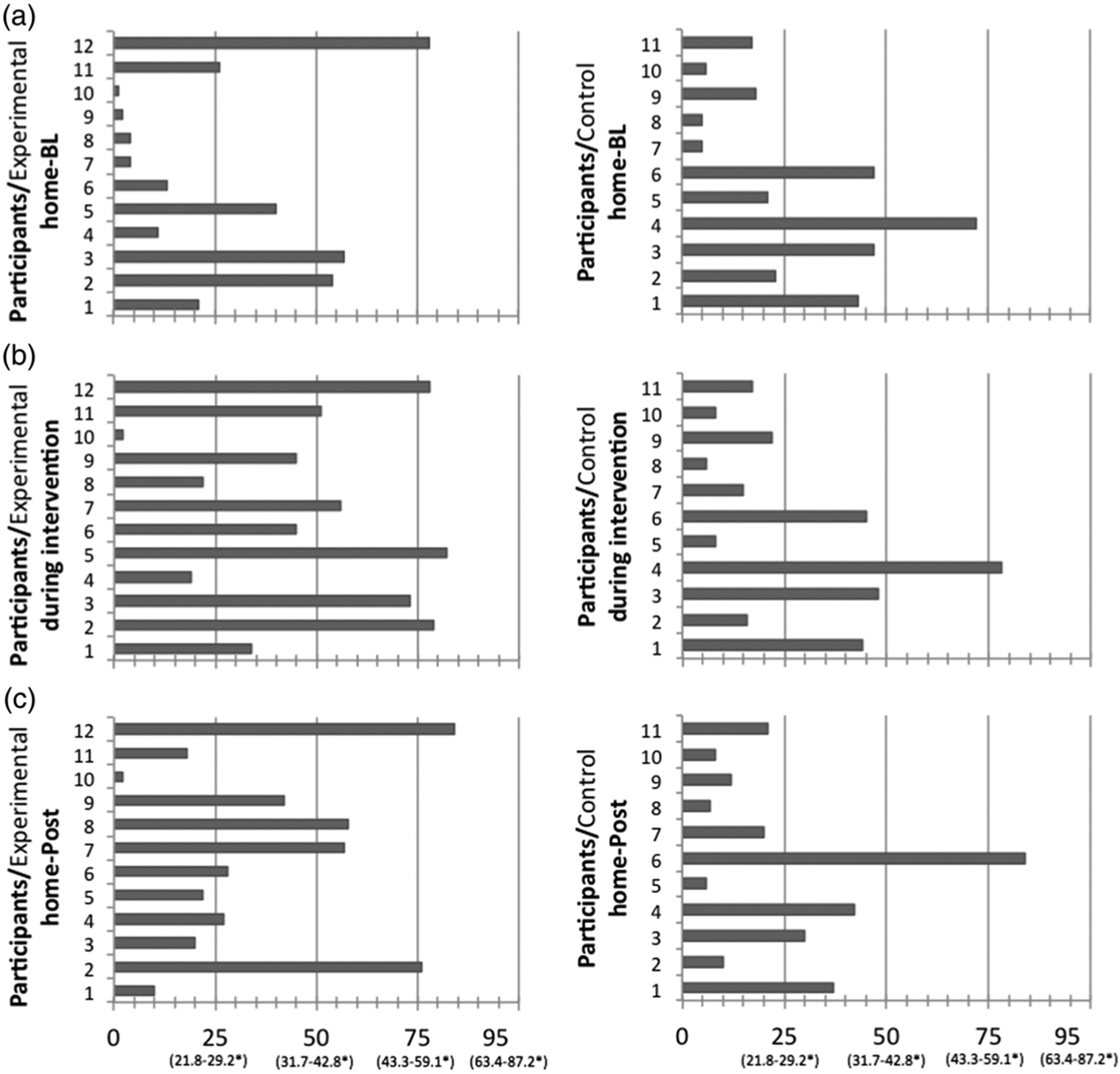
Experimental participants’ (n = 12) and control participants’ (n = 11) hourly conversational turn count averages and hourly LENA (v3·1·5) Natural Language Corpus percentiles.*
Fig. 5a–c.
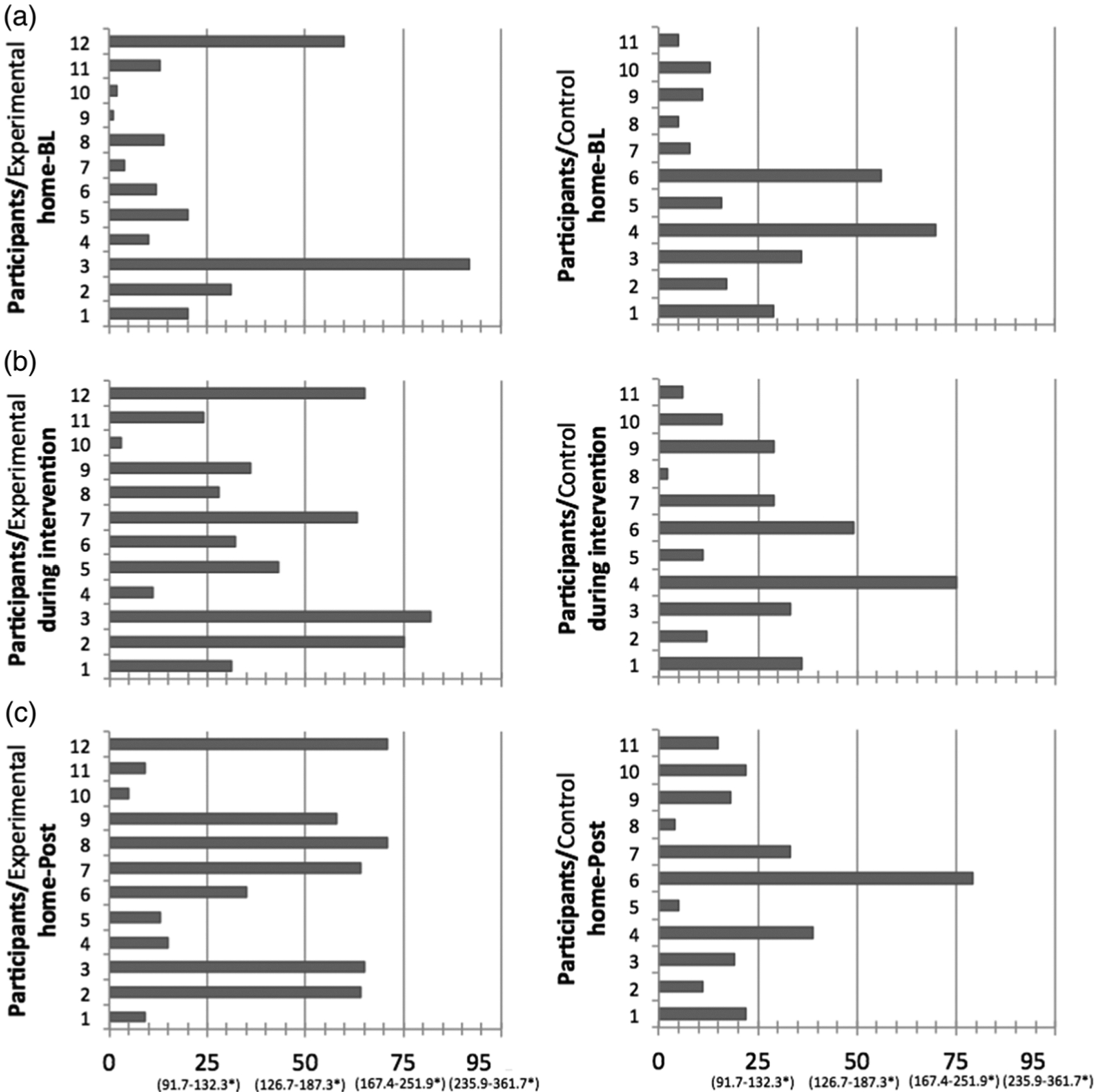
Experimental participants’ (n = 12) and control participants’ (n = 11) hourly child vocalizations count averages and hourly LENA (v3·1·5) Natural Language Corpus percentiles.*
With regard to adult word count at home-BL, Figure 3a shows that most participants scored below average and closer to the 25th percentile. During the intervention period (Figure 3b), 33% (n = 4) of experimental participants increased their baseline adult word counts by one percentile rank, 17% (n = 2) increased their scores by two percentile ranks, and 8% (n = 1) increased by three percentile ranks. At home-Post (Figure 3c), 25% (n = 3) of experimental participants maintained an increase of one percentile rank, 8% (n = 1) newly increased by one percentile rank from baseline, and 8% (n = 1) maintained an increase of two percentile ranks. With regard to the control group, Figure 3b shows that during the intervention 18% (n = 2) of participants increased their adult word counts by one percentile rank. At home-Post (Figure 3c), 9% (n = 1) maintain an increase of one percentile rank and 9% (n = 1) newly increased by two percentile ranks from baseline.
With regard to conversational turn count at home-BL, Figure 4a shows that most participants scored below average and closer to the 25th percentile. During the intervention period (Figure 4b), we see that in the experimental group, 42% (n = 5) of participants increased their scores by one percentile rank and 17% (n = 2) increased by two. At home-Post (Figure 4c), 25% (n = 3) maintained an increase of one percentile rank and 8% (n = 1) newly increased by one percentile rank from baseline; 8% (n = 1) maintained an increase of two percentile ranks and 8% (n = 1) newly increased by two ranks from baseline. In Figure 4b, we see that in the control group 9% (n = 1) of participants increased their turn count by one percentile rank during the intervention and at home-Post (Figure 4c), and 9% (n = 1) newly increased by two percentile ranks from baseline.
Concerning child vocalization counts at home-BL, Figure 5a shows that most participants scored below the 25th percentile. During the intervention period (Figure 5b), we see that in the experimental group, 50% (n = 6) of participants improved by one percentile rank and 8% (n = 1) improved by two ranks. At home-Post (Figure 5c), 25% (n = 3) maintained an increase of one percentile rank (17% (n = 2) of these increased by an additional rank at home-Post) and 8% (n = 1) newly increased by one rank from baseline. With regard to the control group, 27% (n = 3) participants increased by one percentile rank during the intervention (Figure 5d) and 9% (n = 1) maintained this increase at home-Post (Figure 5c). A further 9% (n = 1) newly increased by one percentile rank from baseline.
Taken together, the results obtained through lab and home observations suggest that the behaviors most susceptible to change – at least in the short term – are parents’ types and tokens. Additionally, parents’ overall vocabulary increases, as does the number of conversational turns they take with their children. The change in exactly these behavioral outcomes appears to be mediated by the change in parents’ knowledge of child language development as measured by the questionnaire. Participants’ behaviors least susceptible to change over the course of the intervention appear to be the number of utterances and the mean length of those utterances (MLUw).
DISCUSSION
Developing an intervention with the goals of increasing and enriching parents’ language interactions with their preschool children, improving children’s school readiness, and decreasing the SES-linked achievement gap requires a systematic, iterative approach. We focused here on changing parent language because it has been shown to have an impact on child language, which, in turn, predicts school readiness (Connell & Prinz, 2002; Huttenlocher et al., 2002). The crucial first step, presented in this paper, was to determine whether a parent-focused intervention program can change parent knowledge about language development and, most importantly, parent language input. This first step provides the foundation for parent-focused language interventions designed to impact child language and educational outcomes.
We found that the intervention significantly increased parent knowledge about the role of language input, particularly their own language input, in scaffolding their child’s language development. With regard to changes in parent knowledge as measured by the questionnaire, baseline to post-intervention scores show sizeable increases such that, after the intervention, more parents believed that child-directed speech helps babies’ language development (50% increase in the experimental group, 24% increase in control) and that children learn more words if parents and children jointly attend to what is being talked about (25% increase in experimental, 3% increase in control). With regard to reading, scores after the intervention showed that more parents understood that reading interactions with toddlers are more conducive to learning if toddlers can move around (33% increase in experimental, 24% decrease in control) and skip pages if they want to (50% increase in experimental, 22% increase in control). Post-intervention scores also showed that more parents now believed that talking about tall and short as well as learning about the names for shapes helps children learn math (33% increase on both items in experimental, 3% and 1% decrease in control, respectively), and that how many words children know before they start school predicts how well they do in kindergarten (58% increase in experimental, 26% decrease in control).
While our limited sample size prevented us from including the variable parent knowledge as a covariate in all regression models, a post-hoc analysis of parental language outcomes showed that parent knowledge of child development mediated the increase in the lab observation outcomes word tokens and word types as well as the home observation outcome conversational turn count.
The intervention significantly increased parents’ linguistic interactions with their children during the intervention as measured by three parameters: the amount parents talked to their children (home observations: adult word count; lab observations: word tokens), the amount of turn-taking between parents and children (home observations: conversational turn count), and the diversity and quantity of parents’ vocabulary (lab observations: word types and tokens).
Overall, our findings support the hypothesis that the linguistic behavior of low-SES mothers is malleable, at least over the short term. The increase in conversational turn counts is promising in that previous studies have shown this measure to be positively correlated with child receptive language (VanDam, Ambrose & Moeller, 2012) and school readiness (Huttenlocher et al., 2007; Zimmerman et al., 2009).
Because of the study’s limited time frame and small sample size, we were not certain that the intervention would have an effect on child outcomes. We did find that child vocalization counts were significantly higher during the intervention for the experimental group than for the control group. Moreover, child word types, as measured through lab observations, were significantly higher at lab-Post 1week and marginally higher at lab-Post 4mon for the experimental group than for the control group. These findings provide tentative support for our hypothesis that child language and school achievement outcomes can be positively affected by changing parent linguistic behaviors. Word types, in particular, are an index of vocabulary knowledge, and have been shown to be an important index of later literacy and school readiness (Harlaar, Hayiou-Thomas, Dale & Plomin, 2008).
Taken together, the home and lab observation results suggest that parent-directed language enrichment interventions can change home language environments of children from low-SES backgrounds, at least in the short term. Our ability to create short-term behavioral change is a prerequisite for sustained change. However, the ultimate goal is sustained parental behavior change after the intervention ends and sustained positive impacts on child outcomes. A challenge for behavioral interventions is the development of appropriate methods to assure that behavioral changes are maintained. We assessed whether parent behavior change in the experimental versus control groups was sustained over time by obtaining home observation measures post-intervention at home-post 1week, 1mon, 2mon, 4mon and lab observations of parent–child language interactions at lab-post 1week and lab-post 4mon. The post-intervention lab observation measures (parent types, tokens, and utterances) demonstrated significant changes one week after the intervention was completed. The post-intervention home observation measures were not statistically different from baseline, possibly because of the small sample size in this pilot study.
The sustainability found in the lab observation measures could be related to the parents knowing that they were being observed by the experimenters. Further, it is likely to be easier to sustain a quality interaction for half an hour than throughout the 10-hour home observations.
Importantly, while parents’ language behaviors changed only in the short term (i.e. during the intervention), parents’ knowledge of child language development showed a sustained increase that endured for four months after the intervention ended. This demonstrates the effectiveness of the intervention for increasing parents’ knowledge of child development, a critical predictor of parents’ linguistic interactions with their children (Rowe, 2008). However, it also indicates that it is easier to change parents’ knowledge than parents’ language behaviors. Although increasing parents’ knowledge of child language development may be a crucial prerequisite for changing parents’ language behavior, our findings show that even a long-term increase in parents’ knowledge is not sufficient by itself to create long-term behavior change. The lack of sustained change in parents’ language behavior highlights the need for additional methods that can produce sustained changes. One interesting idea that emerges from this comparison is to encourage parents’ focus on repeatedly improving their language interactions during smaller time frames. Many short quality interactions may add up to an improved linguistic environment for the child, and may be more sustainable than having parents focus on improving their linguistic interactions over long stretches of time.
Limitations, practical implications, and next steps
The primary limitations of this study – the small sample size and the less than optimal results at the long-term follow-up – reflect the need for incremental and rigorous iterative testing necessary for behavioral intervention development. The small sample size precluded a more nuanced evaluation of other differences between the experimental and control groups that might have influenced intervention uptake. Factors of this sort may be particularly important given the heterogeneity of families living in poverty. Further, the limited follow-up prevented a complete assessment of behavioral sustainability and the natural progression of change, as well as an assessment of longer-term child outcomes. Ultimately, a longitudinal study with more participants is required to determine whether the parent behavior changes seen during intervention are sustainable and, most critically, whether those changes translate into positive impacts on child language outcomes and later school readiness.
Building on the promise of the current study and the imperative for addressing the early home language environments of children of low-SES, the next steps in the iterative development will be to evaluate methods for sustaining the intervention’s elicited behavior change (Hoff, 2013). The positive feedback about the program received from experimental group parents not only provides cause for optimism, but also offers three potential ways to improve sustainability. The next iteration of the intervention is currently in progress and the following changes will be integrated.
First, the curriculum will be increased from eight to twelve modules in response to the needs articulated by the target population (Nation et al., 2003). Additional modules will incorporate concepts such as executive function and self-regulation, in response to parent requests for information about how they might use their ‘talk’ to shape child behavior.
Second, the curriculum will be supplemented by post-intervention home observation boosters. Allowing parents to continue to monitor their language behavior via the LENA after the initial intervention ends could help sustain the changes in talk seen during the intervention, analogous to allowing an individual in a weight-loss intervention continued access to a scale. This change might be even more effective if the parents were able to discuss the home observation results with an interventionist over the phone on a weekly basis.
Third, in addition to promoting sustainability, we need to determine which aspects of the intervention are most critical in effecting behavior change – increasing parent knowledge of child language development, convincing parents that their child’s intelligence is malleable, providing quantitative linguistic feedback, or a synergy among these factors. In light of the heterogeneity of the low-SES population, it will also be important to determine which parent moderators (e.g. education level, depression level, number of other children in the household, support network, working memory), if any, play a role in intervention uptake. The combined insights into individual-level variability and the effectiveness of various intervention components will allow for a more nuanced theoretical understanding of the effects described here and the potential for creating a response to intervention model.
Although the causes of the persistent academic achievement gap between children from low- and high-SES homes are complex and multi-faceted, the critical role of early home language environment as a root cause of the disparity is undeniable. The current study represents a first step towards developing a parent-directed intervention that has the potential to improve the language learning trajectories of low-SES children. The results indicate the potential to change both parent–child language interactions and child language learning trajectories during and immediately following the intervention. The challenge, as for most interventions, is sustainability. Overall, the results show that this intervention can provide parents with the tools to successfully enrich their child’s early home language environment, harnessing a powerful way to reduce academic disparities among children who live in poverty.
Acknowledgments
First and foremost, we would like to thank the participating families for so generously allowing us into their homes and for devoting a significant amount of their time to this study. Further, we thank Gabriel Weinberger and Robert Webber for conducting the statistical analyses, and Alison Hundertmark and Alyssa Anneken for designing figures and tables. This study was funded by a Clinical and Translational Science Award (UL1 RR 024999, KL2 RR 025000) to Dana Suskind and by the Hemera Regnant Foundation.
Contributor Information
DANA L. SUSKIND, University of Chicago Medicine, Department of Surgery, Division of Otolaryngology
KRISTIN R. LEFFEL, University of Chicago Medicine, Department of Surgery, Division of Otolaryngology
EILEEN GRAF, University of Chicago Medicine, Department of Surgery, Division of Otolaryngology.
MARC W. HERNANDEZ, University of Chicago, National Opinion Research Center
ELIZABETH A. GUNDERSON, Temple University, Department of Psychology
SHANNON G. SAPOLICH, University of Chicago, School of Social Service Administration
ELIZABETH SUSKIND, University of Chicago Medicine, Department of Surgery, Division of Otolaryngology.
LINDSEY LEININGER, School of Public Health, University of Illinois, Chicago.
SUSAN GOLDIN-MEADOW, University of Chicago, Department of Psychology.
SUSAN C. LEVINE, University of Chicago, Department of Psychology
REFERENCES
- Abraham C & Michie S (2008). A taxonomy of behavior change techniques used in interventions. Health Psychology 27(3), 379–87. [DOI] [PubMed] [Google Scholar]
- Ajzen I (1996). The directive influence of attitudes on behavior. In Gollwitzer PM & Bargh JA (eds), The psychology of action: linking cognition and motivation to behavior, 385–403. New York, NY: Guilford Press. [Google Scholar]
- Algozzine B, Wang C & Boukhtiarov A (2011). A comparison of progress monitoring scores and end-of-grade achievement. New Waves-Educational Research & Development 14(1), 3–21. [Google Scholar]
- Aronson J, Fried CB & Good C (2002). Reducing the effects of stereotype threat on African American college students by shaping theories of intelligence. Journal of Experimental Social Psychology 38(2), 113–25. [Google Scholar]
- Baxendale J & Hesketh A (2003). Comparison of the effectiveness of the Hanen ParentProgramme and traditional clinic therapy. International Journal of Language & Communication Disorders/Royal College of Speech & Language Therapists 38(4), 397–415. [DOI] [PubMed] [Google Scholar]
- Blackwell LS, Trzesniewski KH & Dweck CS (2007). Implicit theories of intelligence predict achievement across an adolescent transition: a longitudinal study and an intervention. Child Development 78(1), 246–63. [DOI] [PubMed] [Google Scholar]
- Bornstein MH, Hendricks C, Hahn C-S, Haynes OM, Painter KM & Tamis-LeMonda CS (2003). Contributors to self-perceived competence, satisfaction, investment, and role balance in maternal parenting: a multivariate ecological analysis. Parenting 3(4), 285–326. [Google Scholar]
- Brooks-Gunn J & Markman L (2005). The contribution of parenting to ethnic and racial gaps in school readiness. The Future of Children 15(1), 139–68. [DOI] [PubMed] [Google Scholar]
- Bugental DB & Happaney K (2002). Parental attributions. In Bornstein Marc H. (Ed.), Handbook of parenting: Vol. 3: Being and becoming a parent (2nd ed.), 509–35. Mahwah, NJ: Lawrence Erlbaum Associates Publishers. [Google Scholar]
- Cartmill EA, Armstrong BF, Gleitman LR, Goldin-Meadow S, Medina TN & Trueswell JC (2013). Quality of early parent input predicts child vocabulary 3 years later. Proceedings of the National Academy of Sciences, 110(28), 11278–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christakis DA, Zimmerman FJ, DiGiuseppe DL & McCarty CA (2004). Early television exposure and subsequent attentional problems in children. Pediatrics 113(4), 708–13. [DOI] [PubMed] [Google Scholar]
- Connell CM & Prinz RJ (2002). The impact of childcare and parent–child interactions on school readiness and social skills development for low-income African American children. Journal of School Psychology 40(2), 177–93. [Google Scholar]
- DesJardin JL & Eisenberg LS (2007). Maternal contributions: supporting language development in young children with cochlear implants. Ear and Hearing 28(4), 456–69. [DOI] [PubMed] [Google Scholar]
- Dichtelmiller M, Meisels SJ, Plunkett JW, Bozytnski MEA, Claflin C & Mangelsdorf SC (1992). The relationship of parental knowledge to the development of extremely low birth weight infants. Journal of Early Intervention 16(3), 210–20. [Google Scholar]
- Dickinson DK & McCabe A (2001). Bringing it all together: the multiple origins, skills, and environmental supports of early literacy. Learning Disabilities Research & Practice 16 (4), 186–202. [Google Scholar]
- Dieterich SE, Assel MA, Swank P, Smith KE & Landry SH (2006). The impact of early maternal verbal scaffolding and child language abilities on later decoding and reading comprehension skills. Journal of School Psychology 43(6), 481–94. [Google Scholar]
- Driessen G, Smit F & Sleegers P (2005). Parental involvement and educational achievement. British Educational Research Journal 31(4), 509–32. [Google Scholar]
- Duncan GJ & Murnane RJ (2011). Whither opportunity? Rising inequality, schools, and children’s life chances. New York: Russell Sage Foundation. [Google Scholar]
- Dweck CS (2006). Mindset: the new psychology of success. New York, NY: Random House. [Google Scholar]
- Flesch R (1948). A new readability yardstick. Journal of Applied Psychology 32(3), 221–33. [DOI] [PubMed] [Google Scholar]
- Forget-Dubois N, Dionne G, Lemelin J-P, Pérusse D, Tremblay RE & Boivin M (2009). Early child language mediates the relation between home environment and school readiness. Child Development 80(3), 736–49. [DOI] [PubMed] [Google Scholar]
- Gilkerson J & Richards JA (2008). The LENA foundation natural language study technical report. Online: <http://www.lenafoundation.org/TechReport.aspx/Natural_Language_Study/LTR-02-2>.
- Goldin-Meadow S, Levine SC, Hedges LV, Huttenlocher J, Raudenbush SW & Small SL (2014). New evidence about language and cognitive development based on a longitudinal study: hypotheses for intervention. American Psychologist 69(6), 588–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Good C, Aronson J & Inzlicht M (2003). Improving adolescents’ standardized test performance: an intervention to reduce the effects of stereotype threat. Journal of Applied Developmental Psychology 24(6), 645–62. [Google Scholar]
- Greenwood CR, Thiemann-Bourque K, Walker D, Buzhardt J & Gilkerson J (2011). Assessing children’s home language environments using automatic speech recognition technology. Communication Disorders Quarterly 32(2), 92–83. [Google Scholar]
- Halle T, Forry N, Hair E, Perper K, Wandner L, Wessel J & Vick J (2009). Disparities in early learning and development: lessons from the early childhood longitudinal study – Birth cohort (ECLS-B). Child Trends, online: <http://www.childtrends.org/?publications=disparities-in-early-learning-and-development-lessons-from-the-early-childhood-longitudinal-study-birth-cohort-ecls-b>, pp. 1–7. [Google Scholar]
- Hanen Centre (2011). The Hanen Centre: helping you help children communicate. Online: <http://www.hanen.org/Home.aspx>.
- Harlaar N, Hayiou-Thomas ME, Dale PS & Plomin R (2008). Why do preschool language abilities correlate with later reading? A twin study. Journal of Speech, Language, and Hearing Research 51(3), 688–705. [DOI] [PubMed] [Google Scholar]
- Hart B & Risley TR (1992). American parenting of language-learning children: persisting differences in family–child interactions observed in natural home environments. Developmental Psychology 28(6), 1096–105. [Google Scholar]
- Hart B & Risley TR (1995). Meaningful differences in the everyday experience of young American children. Baltimore, MD: P.H. Brookes. [Google Scholar]
- Heath C & Heath Dan(2007). Made to stick: why some ideas work in the world and others die. New York: Random House. [Google Scholar]
- Hoff E (2003). The specificity of environmental influence: socioeconomic status affects early vocabulary development via maternal speech. Child Development 74(5), 1368–78. [DOI] [PubMed] [Google Scholar]
- Hoff E (2013). Interpreting the early language trajectories of children from low-SES and language minority homes: implications for closing achievement gaps. Developmental Psychology 49(1), 4–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huttenlocher J, Vasilyeva M, Cymerman E & Levine S (2002). Language input and child syntax. Cognitive Psychology 45(3), 337–74. [DOI] [PubMed] [Google Scholar]
- Huttenlocher J, Vasilyeva M, Waterfall HR, Vevea JL & Hedges LV (2007). The varieties of speech to young children. Developmental Psychology 43(5), 1062–83. [DOI] [PubMed] [Google Scholar]
- Janz N, Champion VL & Stretcher VJ (2002). The health belief model. In Glanz K, Rimer BK & Viswanath K (eds), Health behavior and health education: theory, research, and practice, 44–66. San Francisco, CA: Jossey-Bass. [Google Scholar]
- Kaiser AP & Hancock TB (2003). Teaching parents new skills to support their young children’s development. Infants and Young Children 16(1), 9–21. [Google Scholar]
- Kashinath S, Woods J & Goldstein H (2006). Enhancing generalized teaching strategy use in daily routines by parents of children with autism. Journal of Speech, Language, and Hearing Research 49(3), 466–85. [DOI] [PubMed] [Google Scholar]
- Klass P, Dreyer BP & Mendelsohn AL (2009). Reach out and read: literacy promotion in pediatric primary care. Advances in Pediatrics 56, 11–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landry SH, Smith KE & Swank PR (2006). Responsive parenting: establishing early foundations for social, communication, and independent problem-solving skills. Developmental Psychology 42(4), 627–42. [DOI] [PubMed] [Google Scholar]
- Landry SH, Smith KE, Swank PR & Guttentag C (2008). A responsive parenting intervention: the optimal timing across early childhood for impacting maternal behaviors and child outcomes. Developmental Psychology 44(5), 1335–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levine SC, Suriyakham LW, Rowe ML, Huttenlocher J & Gunderson EA (2010). What counts in the development of young children’s number knowledge? Developmental Psychology 46(5), 1309–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacPhee D (1981). Knowledge of infant development inventory. Chapel Hill, NC: Educational Testing Service. [Google Scholar]
- Mendelsohn AL, Valdez PT, Flynn V, Foley GM, Berkule SB, Tomopoulos S, Dreyer BP (2007). Use of videotaped interactions during pediatric well-child care: impact at 33 months on parenting and on child development. Journal of Developmental and Behavioral Pediatrics 28(3), 206–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michie S (2005). Changing behavior: theoretical development needs protocol adherence. Health Psychology 24(4), 439. [DOI] [PubMed] [Google Scholar]
- Michie S, Jochelson K, Markham WA & Bridle C (2009). Low-income groups and behaviour change interventions: a review of intervention content, effectiveness and theoretical frameworks. Journal of Epidemiology and Community Health 63(8), 610–22. [DOI] [PubMed] [Google Scholar]
- Moorman EA & Pomerantz EM (2010). Ability mindsets influence the quality of mothers’ involvement in children’s learning: an experimental investigation. Developmental Psychology 46(5), 1354–62. [DOI] [PubMed] [Google Scholar]
- Nation M, Crusto C, Wandersman A, Kumpfer KL, Seybolt D, Morrissey-Kane E & Davino K (2003). What works in prevention: principles of effective prevention programs. American Psychologist 58(6/7), 449–56. [DOI] [PubMed] [Google Scholar]
- National Early Literacy Panel (2008). Developing early literacy: report of the National Early Literacy Panel. Washington, DC: National Institute for Literacy. [Google Scholar]
- Ninio A (1979). The naive theory of the infant and other maternal attitudes in two subgroups in Israel. Child Development 50(4), 976–80. [PubMed] [Google Scholar]
- Phillips M (2011). Parenting, time use, and disparities in academic outcomes. In Duncan GJ & Murnane RJ(eds), Whither opportunity? Rising inequality, schools, and children’s life chances, 207–228. New York, NY: Russell Sage Foundation. [Google Scholar]
- Renaissance Learning (2014). STAR reading technical manual. Online: <http://doc.renlearn.com/KMNet/R004384310GJD780.pdf>.
- Roberts MY & Kaiser AP (2011). The effectiveness of parent-implemented language interventions: a meta-analysis. American Journal of Speech-Language Pathology/American Speech-Language-Hearing Association 20(3), 180–99. [DOI] [PubMed] [Google Scholar]
- Rowe ML (2008). Child-directed speech: relation to socioeconomic status, knowledge of child development and child vocabulary skill. Journal of Child Language 35(1), 185–205. [DOI] [PubMed] [Google Scholar]
- Rowe ML & Goldin-Meadow S (2009). Differences in early gesture explain SES disparities in child vocabulary size at school entry. Science 323(5916), 951–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sacks C, Shay S, Repplinger L, Leffel KR, Sapolich SG, Suskind E, Tannenbaum S, & Suskind D (2014). Pilot testing of a parent-directed intervention (Project ASPIRE) for underserved children who are deaf or hard of hearing. Child Language Teaching and Therapy 30(1), 91–102. [Google Scholar]
- Sauer E, Levine SC & Goldin-Meadow S (2010). Early gesture predicts language delay in children with pre- or perinatal brain lesions. Child Development 81(2), 528–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slobin DI & Welsh CA (1967). Elicited cinitation as a research tool in developmental psycholinguistics. Berkeley, CA: Language-Behavior Research Laboratory. [Google Scholar]
- Small ML (2010). Unanticipated gains: origins of network inequality in everyday life. New York, NY: Oxford University Press. [Google Scholar]
- Snow C, Griffin P & Burns MS (2005). Knowledge to support the teaching of reading: preparing teachers for a changing world (1st ed.). San Francisco: Jossey-Bass. [Google Scholar]
- Stein A, Malmberg LE, Sylva K, Barnes J, Leach P & FCCC team (2008). The influence of maternal depression, caregiving, and socioeconomic status in the post-natal year on children’s language development. Child: Care, Health and Development 34(5), 603–12. [DOI] [PubMed] [Google Scholar]
- Stevens JH Jr. (1984). Child development knowledge and parenting skills. Family Relations 33(2), 237–44. [Google Scholar]
- Stevenson HW, Chen C & Uttal DH (1990). Beliefs and achievement: a study of Black, White, and Hispanic children. Child Development 61(2), 508–23. [DOI] [PubMed] [Google Scholar]
- Stipek DJ & Ryan RH (1997). Economically disadvantaged preschoolers: ready to learn but further to go. Developmental Psychology 33(4), 711–23. [DOI] [PubMed] [Google Scholar]
- Suskind D, Leffel KR, Hernandez MW, Sapolich SG, Suskind E, Kirkham E & Meehan P (2013). An exploratory study of ‘quantitative linguistic feedback’: effect of LENA feedback on adult language production. Communication Disorders Quarterly 34(4), 199–209 [Google Scholar]
- Tannock R & Girolametto L (1992). Reassessing parent-focused language intervention programs (E. R. J & Warren S, Eds.) (Vol. 1). Baltimore, MD: Paul H. Brookes Publishing. [Google Scholar]
- VanDam M, Ambrose SE & Moeller MP (2012). Quantity of parental language in the home environments of hard-of-hearing 2-year-olds. Journal of Deaf Studies and Deaf Education 17(4), 402–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walker D, Greenwood C, Hart B & Carta J (1994). Prediction of school outcomes based on early language production and socioeconomic factors. Child Development 65(2 Spec No), 606–21. [PubMed] [Google Scholar]
- Wechsler D (1997). Wechsler Adult Intelligence Scale—3rd Edition (WAIS-3®). San Antonio, TX: Harcourt Assessment. [Google Scholar]
- White KM & Wellington L (2009). Predicting participation in group parenting education in an Australian sample: the role of attitudes, norms, and control factors. Journal of Primary Prevention 30(2), 173–89. [DOI] [PubMed] [Google Scholar]
- Whitehurst GJ, Arnold DS, Epstein JN, Angell AL, Smith M & Fischel JE (1994). A picture book reading intervention in day care and home for children from low-income families. Developmental Psychology 30(5), 679–689. [Google Scholar]
- Whitehurst GJ, Epstein JN, Angell AL, Payne AC, Crone DA & Fischel JE (1994). Outcomes of an emergent literacy intervention in Head Start. Journal of Educational Psychology 86(4), 524–55. [Google Scholar]
- Williamson JML & Martin AG (2010). Analysis of patient information leaflets provided by a district general hospital by the Flesch and Flesch–Kincaid method. International Journal of Clinical Practice 64(13), 1824–31. [DOI] [PubMed] [Google Scholar]
- Xu D, Gilkerson J, Richards JA, Yapanel U & Gray S (2009). Child vocalization composition as discriminant information for automatic autism detection. Conference Proceedings: 31st Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society. Conference, 2009, 2518–2522. Online: <doi: 10.1109/IEMBS.2009.5334846>. [DOI] [PubMed] [Google Scholar]
- Zevenbergen AA & Whitehurst GJ (2003). Dialogic reading: a shared picture book reading intervention for preschoolers. In Van Kleeck A , Bauer EB & Stahl SA (eds), On reading books to children: parents and teachers (pp. 170–192). Mahwah, NJ & London: LEA. [Google Scholar]
- Zimmerman FJ, Gilkerson J, Richards JA, Christakis DA, Xu D, Gray S & Yapanel U (2009). Teaching by listening: the importance of adult–child conversations to language development. Pediatrics 124(1), 342–9. [DOI] [PubMed] [Google Scholar]