

Abstract
Background
Perforated peptic ulcer is a common abdominal disease that is treated by surgery. The development of laparoscopic surgery has changed the way to treat such abdominal surgical emergencies. The results of some clinical trials suggest that laparoscopic surgery could be a better strategy than open surgery in the correction of perforated peptic ulcer but the evidence is not strongly in favour for or against this intervention.
Objectives
To measure the effect of laparoscopic surgical treatment versus open surgical treatment in patients with a diagnosis of perforated peptic ulcer in relation to abdominal septic complications, surgical wound infection, extra‐abdominal complications, hospital length of stay and direct costs.
Search methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) on The Cochrane Library (2004, Issue 2), PubMed/MEDLINE (1966 to July 2004), EMBASE (1985 to November 2004) and LILACS (1988 to November 2004) as well as the reference lists of relevant articles. Searches in all databases were updated in December 2009 and January 2012. We did not confine our search to English language publications.
Selection criteria
Randomized clinical trials comparing laparoscopic surgery versus open surgery for the repair of perforated peptic ulcer using any mechanical method of closure (suture, omental patch or fibrin sealant).
Data collection and analysis
Primary outcome measures included proportion of septic and other abdominal complications (surgical site infection, suture leakage, intra‐abdominal abscess, postoperative ileus) and extra‐abdominal complications (pulmonary). Secondary outcomes included mortality, time to return to normal diet, time of nasogastric aspiration, hospital length‐of‐stay and costs. Outcomes were summarized by reporting odds ratios (ORs) and 95% confidence intervals (CIs), using the fixed‐effect model.
Main results
We included three randomized clinical trials of acceptable quality. We found no statistically significant differences between laparoscopic and open surgery in the proportion of abdominal septic complications (OR 0.66; 95% CI 0.30 to 1.47), pulmonary complications (OR 0.52; 95% CI 0.08 to 3.55) or number of septic abdominal complications (OR 0.60; 95% CI 0.32 to 1.15). Heterogeneity was significant for pulmonary complications and operating time.
Authors' conclusions
This review suggests that a decrease in septic abdominal complications may exist when laparoscopic surgery is used to correct perforated peptic ulcer. However, it is necessary to perform more randomized controlled trials with a greater number of patients to confirm such an assumption, guaranteeing a long learning curve for participating surgeons. With the information provided it could be said that laparoscopic surgery results are not clinically different from those of open surgery.
Keywords: Humans, Laparoscopy, Peptic Ulcer Perforation, Peptic Ulcer Perforation/surgery, Randomized Controlled Trials as Topic
Plain language summary
Laparoscopic (minimally invasive) repair for perforated peptic ulcer disease
A perforated peptic ulcer can be repaired using either open surgery or laparoscopy, a minimally invasive surgical technique sometimes known as 'keyhole' surgery. Three randomized controlled trials were identified that compared the two methods. These trials included patients with clinical suspicion of perforated peptic ulcer that was confirmed at surgery. Both laparoscopic and open repairs were made with an omentum patch or fibrin sealant. The primary outcomes assessed were septic abdominal and extra‐abdominal complications. Secondary outcomes assessed were mortality, operation time and hospital length of stay. The quality of the trials was acceptable. There were no statistically significant differences in septic abdominal complications between laparoscopic and open repair of perforated peptic ulcer. More randomized controlled trials with a greater number of patients are needed to confirm such an assumption, guaranteeing a long learning curve for participating surgeons.
Summary of findings
Summary of findings for the main comparison. Laparoscopic surgery versus open surgery for perforated peptic ulcer disease.
| Laparoscopic surgery versus open surgery for perforated peptic ulcer disease | ||||||
| Patient or population: patients with perforated peptic ulcer disease Settings: hospitalized patients from developed countries and availability of laparoscopy equipment Intervention: laparoscopic surgery versus open surgery | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Laparoscopic surgery versus open surgery | |||||
| Septic abdominal complications (presence or absence) Clinical definition Follow‐up: 30 to 60 days | 155 per 1000 | 108 per 1000 (52 to 213) | OR 0.66 (0.3 to 1.47) | 214 (2 studies) | ⊕⊕⊝⊝ low1,2 | |
| Pulmonary complications (presence or absence) Follow‐up: 30 to 60 days | 86 per 1000 | 46 per 1000 (7 to 249) | OR 0.52 (0.08 to 3.55) | 315 (3 studies) | ⊕⊕⊝⊝ low | |
| Surgical site infection Follow‐up: 30 to 60 days | 72 per 1000 | 21 per 1000 (6 to 72) | OR 0.28 (0.08 to 1) | 315 (3 studies) | ⊕⊕⊕⊝ moderate3 | |
| Suture dehiscence Follow‐up: 30 to 60 days | 13 per 1000 | 20 per 1000 (4 to 96) | OR 1.52 (0.29 to 7.98) | 315 (3 studies) | ⊕⊕⊝⊝ low3 | |
| Postoperative ileus Follow‐up: 30 to 60 days | Study population | OR 0.54 (0.16 to 1.8) | 315 (3 studies) | ⊕⊕⊝⊝ low4,5 | ||
| 46 per 1000 | 25 per 1000 (8 to 80) | |||||
| Moderate | ||||||
| 35 per 1000 | 19 per 1000 (6 to 61) | |||||
| Intra‐abdominal abscess Follow‐up: 30 to 60 days | 20 per 1000 | 23 per 1000 (7 to 75) | OR 1.15 (0.33 to 4.03) | 315 (3 studies) | ⊕⊝⊝⊝ very low5,6,7 | |
| Operative time Follow‐up: 30 to 60 days | The mean operative time in the control groups was minutes | The mean operative time in the intervention groups was 14.62 higher (35.25 lower to 64.49 higher) | 214 (2 studies) | ⊕⊝⊝⊝ very low7,8 | ||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; OR: Odds ratio; | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Imprecision is probably because the small sample size of the studies and the lack of reporting form the largest one. 2 There are only three RCTs, all with positive results. Two were from the same city in China. There are no reports from other developed or undeveloped countries where other types of laparoscopic procedures are currently undertaken. 3 For suture dehiscence there are too few events to consider the results precise. 4 The measurement of postoperative ileus is subjective and heterogeneous between groups. 5 The multicenter trial showed no intra‐abdominal abscesses. This can be explained because it is the last one published, where the training curve could be already reached. 6 Former trials showed an increase in intra‐abdominal abscesses in comparison with the last one. Data are very different between trials. 7 There are only three RCT, all with positive results. Two were from the same city in China. There is no report from other developed or undeveloped countries where other types of laparoscopic procedures are currently undertaken. 8 The operative time has a very large confidence interval that could be explained by the lack of completion of the training curve in the former trials.
Background
Description of the condition
The appearance of laparoscopy in the late 1980s marked a milestone in surgery. Its advantages of diminished pain, surgical wound complications, hospital stay and global costs in uncomplicated cases of gallbladder disease (Gadacz 2000) led to the expansion of its use to other intra‐abdominal organs such as the distal oesophagus, the proximal stomach (Chekan 1999; Consensus 1997; Horgan 1997; Klingler 1999) and the colon (Rickard 2001; Tisminezky 2000).
Most of the early laparoscopic approaches were confined to elective surgery. However, with the improvement of technology and the gaining of experience the laparoscopic approach for acute intra‐abdominal pathologies can be applied more widely (Bergamaschi 2000; Pamoukian 2001; Sauerland 2004).
Peptic ulcer perforation is the second most frequent abdominal perforation that requires surgery, following perforated appendicitis. Peptic ulcer is a common disease in the general population. It is estimated that almost 10% of American men will suffer from duodenal ulcer in their lifetime, although its incidence varies within a country (Paimela 1991) as it is more frequent in men and the incidence increases with age. Peptic ulcer disease has been associated with many etiological factors such as Helicobacter pylori infection, non‐steroidal anti‐inflammatory drug (NSAID) use, stress, cigarette smoking, diet and genetics but multifactorial hypotheses are widely accepted. Complications of peptic ulcer include bleeding, obstruction and perforation and they are still treated by general surgeons.
Elective surgery for peptic ulcer disease has decreased significantly over the years due to the introduction of effective medical therapies, first with histamine type 2 (H2)‐receptor antagonists and more recently with proton pump inhibitors. However, the principal complications of perforation and hemorrhage remain indications for surgery. (Paimela 1991; Svanes 1995).
Description of the intervention
Since the first description of surgery for acute perforated peptic ulcer many techniques have been recommended. Ulcers can be repaired by hand suturing the edges of the wound or using surgical stapling devices, covering the defect using an omental patch, or closing it with a fibrin sealant or a gelatin plug product (Darzi 1993; Matsuda 1995; Tate 1993; Walsh 1993).
Since the early 1990s, some authors have suggested that in cases of perforated peptic ulcer the laparoscopic approach may offer theoretical advantages over the open approach. Such advantages include reduced size of the surgical wound and diminished postoperative pain; fewer postoperative complications; less intestinal manipulation, which should diminish postoperative ileus and the long‐term risk of future adhesive obstructive complications; and the global cost savings derived from a shorter hospital stay and an earlier return to daily activities (Benoit 1993; Michelet 2000; Mouret 1990; Naesgaard 1999; Sunderland 1992). Furthermore, it has been suggested that laparoscopic repair could be the best choice for patients with adverse prognostic factors such as advanced age and coexisting cardiopulmonary diseases, or a clinical evaluation delayed beyond 12 hours from the onset of symptoms (Chou 2000; Hermansson 1999). However, some authors have also found that laparoscopic repair presents a somewhat higher incidence of leaks and is a more time‐consuming procedure (Lau 1995; Lee 2001).
Why it is important to do this review
Controlled trials have been carried out trying to evaluate this approach. However, the results are inconclusive because of methodological weaknesses in the trials and the small numbers of participants (Druart 1997; Gomez‐Ferrer 1996; Katkhouda 1999; Kum 1993; Lau 1995; Lau 1996; Lau 1998; Michelet 2000; Ozmen 1995; Robertson 2000; Siu 2002). A systematic review is, therefore, appropriate as meta‐analysis may prove informative as to the comparative efficacy and complication rates for the two surgical approaches.
Thus, the present systematic review was developed to answer the following question: is laparoscopic treatment of perforated peptic ulcer associated with reduced wound complications, postoperative intra‐abdominal sepsis, duration of hospitalization and overall cost compared to the conventional (open) approach?
Objectives
To assess laparoscopic surgical treatment versus open surgical treatment in patients with perforated peptic ulcer diagnosis in terms of abdominal septic complications, surgical wound infection, extra‐abdominal complications, hospital stay and direct costs.
Methods
Criteria for considering studies for this review
Types of studies
The review included randomized controlled trials that were performed after 1988, the date of the first surgical procedure using laparoscopy (Mouret 1990). Restrictions regarding language were not applied.
Studies including patients managed with an open abdomen from the beginning of surgery or that did not have information about relevant clinical outcomes (surgical wound infection, intra‐abdominal infection and hospital length of stay) were excluded.
Types of participants
Adult patients, older than 18 years, with a preoperative clinical diagnosis and intraoperative confirmation of a perforated ulcer (gastric or duodenal) that was corrected by any mechanical method (primary suture, omentum patch, synthetic material patch) by a surgeon.
Types of interventions
Laparoscopic versus open surgery correction of the ulcer with any mechanical method (primary suture, omentum patch, synthetic material patch or resection), with or without insufflation.
Types of outcome measures
Primary outcomes
Septic and other abdominal and extra‐abdominal complications, defined according to the Centers for Disease Control (CDC) classification (Garner 1996) and recorded as 'number of complications' and 'at least one abdominal complication'.
We considered the following abdominal complications: intra‐abdominal abscess; anastomosis leakage; secondary peritonitis; surgical‐site infection; prolonged ileus for more than 72 hours without recovery of bowel movement, clinically‐determined; and incisional hernia.
Secondary outcomes
Mortality
Number of interventions
Conversion rate for the laparoscopic group
Nasogastric tube duration
Total analgesic dose
Time to return to normal diet
Overall duration of hospitalisation
Operation time
Outcome measures were measured within the period 30 days after surgery.
Search methods for identification of studies
Electronic searches
A search was conducted to identify all published and unpublished randomized controlled trials.
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) on The Cochrane Library (4th quarter, 2011), PubMed/MEDLINE (1946 to December 2011), EMBASE (1980 to December 2011) and LILACS (1988 to December 2011) as well as reference lists of relevant articles. Searches in all databases were updated in January 2012. We did not confine our search to English language publications. The Cochrane highly sensitive search strategy for identifying randomized trials in MEDLINE, sensitivity maximising version, Ovid format (Higgins 2008) was combined with the search terms in Appendix 1 to identify randomized controlled trials in MEDLINE. The MEDLINE search strategy was adapted for use in the other databases searched.
Searching other resources
Reference lists from trials selected by electronic searching were screened to identify further relevant trials. Abstracts from the conference proceedings of the American Digestive Disease Week (DDW), published in Gastroenterology and the United European Gastroenterology Week (UEGW) and appearing in Gut, were handsearched.
In addition, members of the Cochrane Upper Gastric and Pancreatic Diseases Group, experts in the field and pharmaceutical companies were contacted and asked to provide details of any outstanding clinical trials or relevant unpublished studies. The websites from ClinicalTrials.gov from the US National Institutes of Health, Current Controlled Trials, International Clinical Trials Registry Platform from the World Health Organization, Clinical Trials Registry‐India (CTRI) and Pan African Clinical Trial Register were reviewed to identify completed or ongoing trials.
Data collection and analysis
Selection of studies
AS, CM and MV reviewed the abstracts of the identified articles independently and selected the studies to be included.
Data extraction and management
CM and MV extracted the data using a previously designed format. They were trained at the beginning of the study on data extraction methods, especially on the non‐imputation of results from the reports. Disagreement between review authors were solved by consensus. The concordance between the extractors was evaluated using an intraclass correlation coefficient and kappa coefficient; the value was 0.99. The studies were centrally blinded by the review authors for the title of the article, authors and publication source. For missing data from the published trials, AS communicated directly with the authors by e‐mail.
A comparison was made between the type of treatment and septic and other complications: abdominal including surgical site infection, intra‐abdominal abscess, leakage from the suture site and prolonged ileus; and extra‐abdominal, specifically pulmonary complications. The number of re‐operations, mortality and hospital length of stay were also compared. Statistical analysis was performed using the Cochrane RevMan 5.0 software.
Assessment of risk of bias in included studies
Assessment of risk of bias was performed by CM and MV. The assessment focused on sequence generation, allocation concealment, blinding, incomplete outcome data, follow‐up losses, intention‐to‐treat method of analysis and selective reporting as recommended by Cochrane Handbook for Systematic Reviews of Interventions Version 5.0 (Higgins 2008).
Measures of treatment effect
The results for each outcome were measured using the crude odds ratio (OR) for categorical variables not related by time; log hazard ratio for time‐to‐event variables; and means differences for continuous variables. The 95% confidence interval (CI) was also estimated.
Dealing with missing data
For missing data, trial authors were contacted via e‐mail. For cases in which the data in an article were in measurement units that differed from the review format, the extractor registered the original data and the review authors performed the necessary conversion.
Assessment of heterogeneity
Heterogeneity analysis was performed using the Q test, with heterogeneity considered significant when P value < 0.1. The I² statistic was used to quantify the presence of heterogeneity in the pooled results.
Assessment of reporting biases
The identification of publication bias with the funnel plot, planned in the protocol, could not be performed because of the small number of articles included in the review.
Data synthesis
The fixed‐effect model and the Mantel‐Haenszel method for the measurement of the global effects outcome were used.
Subgroup analysis and investigation of heterogeneity
If there was significant heterogeneity, a re‐analysis with the random‐effects method was done as well as a sensitivity analysis to try to consider the potential source of the heterogeneity. The origin of the heterogeneity was explained qualitatively. Although a stratified analysis by disease severity was planned in the protocol, as a way to explain any heterogeneity, it was impossible to do because of the lack of information about the severity of the disease in the included studies.
Sensitivity analysis
This was not carried out due to the small number of included studies and insufficient data on items such as surgeon experience or volume of cases, which may be important factors.
Results
Description of studies
Results of the search
Thirteen studies were identified by the primary search. Nine of these were excluded because they were comparative studies and did not use randomization (Bergamaschi 2000; Bhogal 2008; Katkhouda 1999; Lemaitre 2005; Mehendale 2002; Minutolo 2009; Nicolau 2008; Robertson 2000; Vettoretto 2005); another was excluded because of missing and duplicate data (Lau 1998). We tried to contact the authors but received no response.
All studies were identified in MEDLINE and all were in the English language. The one article that was in a language other than English stated clearly in the abstract that it was not a randomized controlled trial, so it was not translated.
Requests to authors and other sources of information did not provide further studies.
Included studies
Three studies were included (Bertleff 2009; Lau 1996; Siu 2002). The updated literature search of January 2012 did not identify any new studies eligible for inclusion. Please see 'Characteristics of included studies'. Inclusion criteria were similar for the three included studies: adult patients with a clinical diagnosis of perforated peptic ulcer (as shown by peritoneal irritation, pneumoperitoneum on chest x‐ray) made by the attending surgeon.
Exclusion criteria were also similar for the included studies:
previous abdominal surgery;
concomitant bleeding of the ulcer, or gastric outlet obstruction;
intraoperative diagnosis of hollow viscus perforation different from peptic ulcer;
perforated peptic ulcer that required definitive surgery, criteria not reported;
cardiopulmonary severe disease that impeded a long‐duration surgical procedure;
clinically sealed ulcer by the omentum at the time of surgery (Lau 1996; Siu 2002);
pregnancy.
Design
Bertleff 2009 was a multicenter, parallel design randomized controlled trial (RCT) over 77 months; Lau 1996 was a parallel group RCT, which took place over 28 months; as was Siu 2002 which took place over 41 months.
Sample sizes
The three studies included 315 patients in total (Bertleff 2009; Lau 1996; Siu 2002), 163 in the laparoscopy group (52 in Bertleff 2009, 48 in Lau 1996 and 63 in Siu 2002) and 152 in the open‐surgery group (49 in Bertleff 2009, 45 in Lau 1996 and 58 in Siu 2002).
Setting
The three included studies were carried out in a hospital setting. Bertleff 2009 was a multicenter, parallel design RCT conducted in nine medical centers in the Netherlands over 77 months. Lau 1996 was a parallel group RCT that took place over 28 months in the Prince of Wales Hospital, Shatin, New Territories, Hong Kong. Siu 2002 was also a parallel group RCT from the Pamela Youde Nethersole Eastern Hospital, Chai Wan, Hong Kong, Special Administrative Region, China and took place over 41 months.
Participants
The studies did not report on baseline differences in participant age, sex, disease severity (measured with APACHE II score and American Society of Anesthesiologists (ASA) classification), shock, concomitant diseases, ulcer localization or perforation size. Only Bertleff 2009 mentioned the grade of peritonitis, which was similar for both groups.
Interventions
Interventions were as follows. Open surgery was by a midline laparotomy with closure of the ulcer with omentum using the technique of Cellan‐Jones. In the Lau (Lau 1996) study, two more groups were created within the open and laparoscopic surgery groups: one with the Cellan‐Jones technique and the other using sponge and fibrin sealant and peritoneal toilet. Laparoscopic surgery included the creation of a pneumoperitoneum with carbon dioxide at 15 mm Hg using a 10 mm trocar and the insertion of a further two or three 5 mm trocars with closure of the perforation with omentum sutured by the same technique as with open surgery or using a sponge and fibrin sealant.
All patients received antibiotics: one study for a day (Lau 1996), in Siu 2002 five days, and Bertleff 2009 did not specify the type of antibiotic or the time of administration. Postoperative analgesia was maintained with pethidine (1 mg/kg every 4 hours) in Lau 1996 and Siu 2002. Bertleff 2009 used opiates but did not specify the type and doses used.
The included studies mentioned that the surgical procedures were performed by trained surgeons, or by residents accompanied by trained surgeons with experience in open and laparoscopic surgery. However, none of the studies described the number of procedures that the surgeons had previously carried out.
Outcomes
All three included studies reported complications, time of nasogastric aspiration, pain assessed with a Visual Analogue Scale (VAS), operation time, analgesic use, conversion rate for the laparoscopic group and length of hospital stay. Lau 1996 and Siu 2002 also reported duration of intravenous fluid maintenance and time to resume oral diet.
Excluded studies
Ten studies did not meet the inclusion criteria for the review. Please see 'Characteristics of excluded studies'.
Risk of bias in included studies
Participants in the included studies were randomized using computer‐generated random numbers and the concealment of assignment was done using sealed envelopes. Assessment of outcomes was not blinded in either of the studies. In Siu 2002 an independent surgeon made the evaluations for return to normal activities and work.
Follow up was at day 30 but in one study there were no assessments for 27% of the laparoscopy group and 31% of the open surgery group at this date (Lau 1996). However, authors clearly stated that all patients were evaluated at week 8 (Table 2). An intention‐to‐treat analysis for primary outcomes was carried out in all studies.
CM and MV differed in their assessment of outcomes related to suture dehiscence and morbidity in the Siu article (Siu 2002) and with blind outcome assessment, operative time and nasogastric aspiration time in the Lau article (Lau 1996). AS reviewed the articles and resolved the differences. Figure 1 and Figure 2 provide summaries of the risk of bias, please also see the Characteristics of included studies table for risk of bias assessments for each included study.
1.
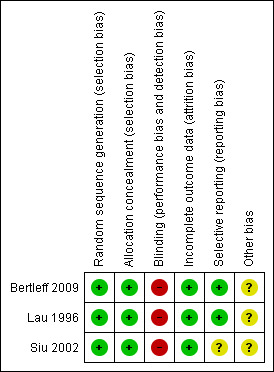
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
2.
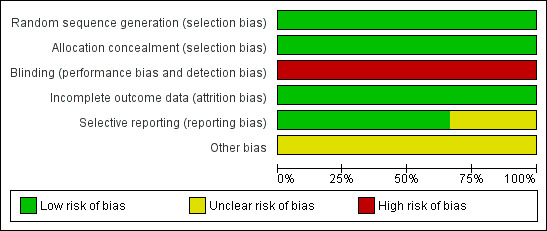
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
Sequence generation was adequate in all three included studies, being computer generated. Allocation concealment was also adequate in all three included studies, being achieved by sealed envelopes.
Blinding
Blinding was not possible as the studies compared open surgery with laparoscopy. Blinding probably did not affect the assessment of hard outcomes such as surgical complications, but it was possible that length of stay and pain assessment could have been biased by non‐blind evaluation of outcomes.
Incomplete outcome data
There were no missing outcome data in any of the three included trials.
Selective reporting
Two trials (Bertleff 2009; Lau 1996) adequately reported all outcome data and were judged to be free of selective outcome reporting. There was insufficient information in Siu 2002 to judge this, but analysis of the trial data from this study suggests that any bias due to selective outcome reporting in this study should not greatly bias the results of the analyses.
Other potential sources of bias
In surgical trials, there is always a bias related to the learning curve for the new surgical methods. However, we believe this bias was not present in the included studies because the experience of the surgeons was similar.
In multicenter trials, a bias related to high volume and low volume centers is possible. There was no information about the number of patients by center to investigate this further.
Effects of interventions
See: Table 1
Laparoscopic surgery versus open surgery
Primary outcomes
Septic and other abdominal and extra‐abdominal complications
Twelve of 111 patients (10.8%) in the laparoscopy group had an abdominal complication against 16 of 103 (15.5%) in the open‐surgery group (OR 0.66; 95% CI 0.30 to 1.47; Analysis 1.1). The Bertleff 2009 study did record reliable data for this outcome and, when contacted, the authors did not offer any additional data about this outcome. No statistically significant differences or significant heterogeneity were observed.
1.1. Analysis.
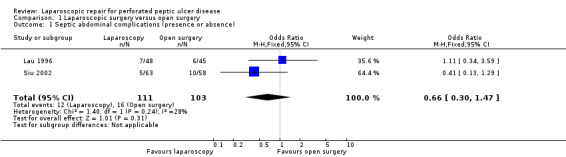
Comparison 1 Laparoscopic surgery versus open surgery, Outcome 1 Septic abdominal complications (presence or absence).
Septic extra‐abdominal complications, specifically pulmonary complications, occurred in eight patients in Bertleff 2009 (three in the laparoscopic group), in four patients in Lau 1996 (three in the laparoscopic group) and seven patients in Siu 2002 (none in the laparoscopic group) (OR 0.43; 95% CI 0.17 to 1.12; analysis not shown), which was not statistically significant. The heterogeneity test had a P value of 0.09 and the I² was 58%. As stated in the protocol, we performed an analysis using the random‐effects method but without any change in the results (OR 0.52; 95% CI 0.08 to 3.55; Analysis 1.2).
1.2. Analysis.
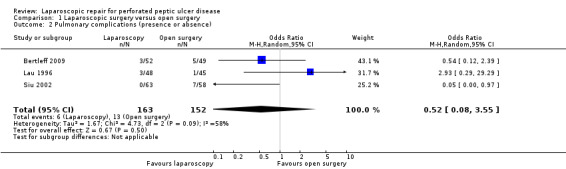
Comparison 1 Laparoscopic surgery versus open surgery, Outcome 2 Pulmonary complications (presence or absence).
The absolute number of septic abdominal complications was 18 (12.3%) in the laparoscopy group and 26 (17.1%) in the open‐surgery group. The OR was 0.60 (95% CI 0.32 to 1.15; Analysis 1.3) but the difference was not statistically significant. One patient in the laparoscopic group, from the Siu 2002 study, had two concurrent complications (suture leakage and intra‐abdominal abscess). In the Bertleff 2009 study there were patients with more than one complication but it was impossible to get reliable information about the number.
1.3. Analysis.
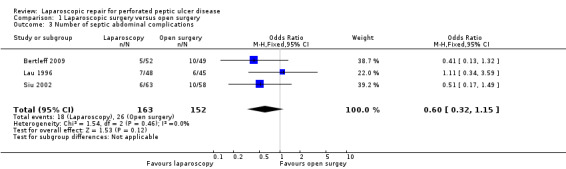
Comparison 1 Laparoscopic surgery versus open surgery, Outcome 3 Number of septic abdominal complications.
Three patients in the laparoscopic group (1.8%) and 11 (7.2%) in the open‐surgery group had a surgical site infection (OR 0.26; 95% CI 0.08 to 0.9). The analysis made with a random‐effects model showed an OR of 0.28 (95% CI 0.08 to 1.0; Analysis 1.4).
1.4. Analysis.
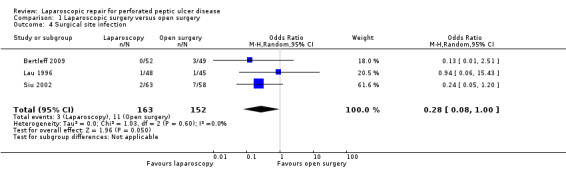
Comparison 1 Laparoscopic surgery versus open surgery, Outcome 4 Surgical site infection.
Suture dehiscence was reported in four patients in the laparoscopy group (2.4%) versus two patients in the open group (1.3%) with an OR of 1.70 (95% CI 0.36 to 8.07). As stated in the protocol, we performed an analysis using the random‐effects method (Analysis 1.5) but without any change in the results.
1.5. Analysis.

Comparison 1 Laparoscopic surgery versus open surgery, Outcome 5 Suture dehiscence.
Postoperative ileus occurred in four patients from the laparoscopy group (2.5%) and in seven in the open‐surgery group with an OR of 0.54 (95% CI 0.16 to 1.80; Analysis 1.6). As stated in the protocol, we performed an analysis using the random‐effects method but without any change in the results.
1.6. Analysis.
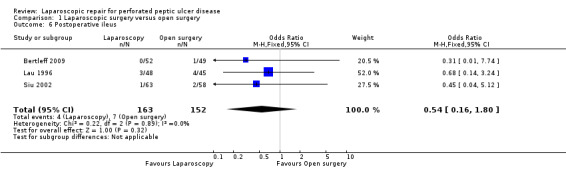
Comparison 1 Laparoscopic surgery versus open surgery, Outcome 6 Postoperative ileus.
Four patients had intra‐abdominal abscesses in the laparoscopic group and three patients in the open‐surgery group (OR 1.15; 95% CI 0.33 to 4.03; Analysis 1.7) but this difference was not statistically significant.
1.7. Analysis.
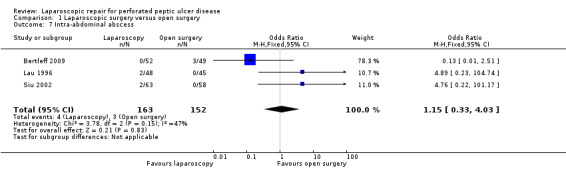
Comparison 1 Laparoscopic surgery versus open surgery, Outcome 7 Intra‐abdominal abscess.
Incisional hernia incidence was similar between groups, two patients for laparoscopic repair and one for the open‐surgery group (OR 0.93; 95% CI 0.21 to 4.15; Analysis 1.8). None of these comparisons showed a statistically significant difference or heterogeneity.
1.8. Analysis.
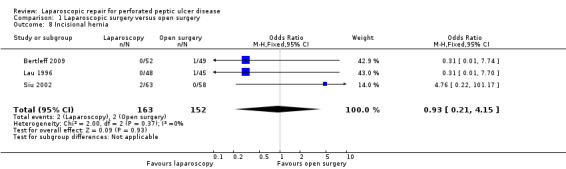
Comparison 1 Laparoscopic surgery versus open surgery, Outcome 8 Incisional hernia.
Secondary outcomes
Mortality
For the secondary outcomes, five patients died in the laparoscopic group (3.0%) and eight patients in the open‐surgery group (5.3%) with an OR of 0.57 (95% CI 0.18 to 1.78; Analysis 1.9). This was not statistically significant.
1.9. Analysis.
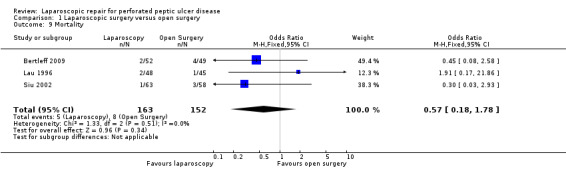
Comparison 1 Laparoscopic surgery versus open surgery, Outcome 9 Mortality.
Number of interventions
Six patients were re‐operated on in the laparoscopic group (5.4%), almost twice as many as in the open‐surgery group (three patients (2.9%)) but this difference was not statistically significant (OR 1.89; 95% CI 0.46 to 7.71; Analysis 1.10). The Bertleff 2009 study did not contain any information about this outcome and in the other trials (Lau 1996; Siu 2002) the investigators did not offer additional data.
1.10. Analysis.
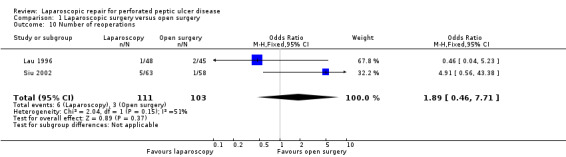
Comparison 1 Laparoscopic surgery versus open surgery, Outcome 10 Number of reoperations.
Analgesic doses
Bertleff 2009 reported opiate requirements but not the doses used. Data reported in a non‐parametric form are reported in Table 2. The Included trials reported lower analgesic dose or time requirements for the patients in the laparoscopic group.
1. Measures reported in non‐parametric form.
| Variable | Study | Laparoscopic group | Open surgery group | P value |
| Nasogastric aspiration time (median and range) | Bertleff 2009 | 2 (3.0) IQR | 3 (1.3) IQR | 0.33 |
| Siu 2002 | 3 (2‐33) | 3(1‐8) | 0.28 | |
| Lau 1996 | 2 (1‐4)/ 3 (2‐1) | 2 (1‐13)/ 3(1‐17) | No significant (P value not reported) | |
| Time to return to oral diet | Siu 2002 | 4 (3‐35) | 5 (3‐24) | 0.06 |
| Lau 1996 | 4 (3‐7)/ 4 (2‐11) | 4 (3‐16)/ 4 (3‐19) | No significant (P value not reported) | |
| Length of stay | Bertleff 2009 | 6.5 (9.3) IQR | 8 (7.3) IQR | 0.23 |
| Siu 2002 | 6 (4‐35) | 7 (4‐39) | 0.004 | |
| Lau 1996 | 5 (3‐20)/ 6 (3‐11) | 5 (3‐19)/ 5 (2‐21) | No significant (P value not reported) | |
| Analgesic doses | Siu 2002 | 0 (0‐11) | 6 (1‐30) | <0.001 |
| Lau 1996 | 1 (0‐12)/ 2 (0‐17) | 3 (0‐10)/ 4 (1‐9) | 0.03 | |
| Bertleff 2009 | 1 (1.25) median days of analgesics | 1 (1.0) median days of analgesics | 0.007 |
Time of nasogastric aspiration
Table 2 contains the medians and ranges for the time of nasogastric aspiration. The differences between open surgery and laparoscopy were not statistically significant.
Time to return to oral diet
Bertleff 2009 did not reported time to return to oral diet; the results for Lau 1996 and Siu 2002 are in Table 2. The differences were not statistically significant.
Overall duration of hospitalization
These data were reported non‐parametrically and are reported in Table 2. In Siu 2002, hospital length‐of‐stay was statistically in favour of laparoscopic repair; but not in Lau 1996 and Bertleff 2009.
Operation time
The operation time was different between studies. Siu 2002 reported a lower time for laparoscopic repair (42 ± 25.1 min) than in the open‐surgery group (52.3 ± 24.8 min); the difference was statistically significant (P = 0.02). On the contrary, Bertleff 2009 reported a longer operation time for the laparoscopic group (median 75 min) versus the open‐surgery group (50 min), a non‐statistically significant difference, but did not report standard deviations. Lau 1996 reported a longer operation time for the laparoscopic group (94.3 ± 40.3 min) than the open‐surgery group (53.7 ± 42.6 min); this difference was statistically significant (P = 0.001). The weighted mean difference was 0.77 min (95% CI ‐7.10 to 8.64; Analysis 1.11), which was not statistically significant, but with a highly significant heterogeneity test (P < 0.00001, I² = 96%). The analysis with a random‐effects model did not change the non‐significant result. The conversion rate for the laparoscopy group was 13 patients with a global frequency of 7.9%.
1.11. Analysis.
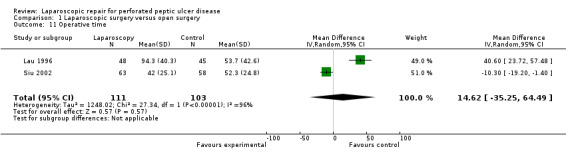
Comparison 1 Laparoscopic surgery versus open surgery, Outcome 11 Operative time.
Discussion
Summary of main results
Although there was a tendency for a decrease in septic intra‐abdominal complications, surgical site infection, postoperative ileus, pulmonary complications and mortality with laparoscopic repair compared with open surgery, none of these were statistically significant. However, there was a tendency for an increase in the number of intra‐abdominal abscesses and re‐operations, without statistical significance. This finding could be related to surgeon experience in laparoscopic surgery. It is not possible to draw any conclusions about suture dehiscence and incisional hernia with the two procedures.
Other important variables, time of nasogastric aspiration and time to return to an oral diet, were reported in a non‐parametric format and were not statistically different between groups. In Siu 2002, hospital length of stay was statistically in favour of laparoscopic repair; but not in Lau 1996 and Bertleff 2009. Included trials reported lower analgesic doses or time requirements for the patients in the laparoscopic group. With these findings it is impossible to suggest any beneficial effects in terms of direct costs and this subject should be assessed in other studies specifically designed to assess cost‐effectiveness.
Statistical heterogeneity was found in the frequency of pulmonary complications and in operation times. It is hard to explain heterogeneity for pulmonary complications with the available data. In the case of operation time, the Siu 2002 study showed a shorter operation time for the laparoscopic procedure than did the Lau 1996 and Bertleff 2009 studies. This could be explained by greater experience with minimally‐invasive surgery. The results of this systematic review must be interpreted carefully because of the small sample sizes of the included trials.
Overall completeness and applicability of evidence
Clinical heterogeneity was not identified in the relevant clinical variables of the included studies so it is probable that the patients were similar.
Another important point to discuss is the learning curve for surgeons. It is accepted that surgical procedures are highly dependent on ability and the familiarity that surgeons have with different techniques. Introduction of a new surgical technique has a better prognosis when surgeon experience with it is greater (Solomon 1998). For the included trials, there was no objective information that helped to define the point on the learning curve of the surgeons, which affects the generalizability of the results. However, a conversion rate of 7.9% shows that experience with the technique is enough to consider the laparoscopic approach in these cases. The high number of patients operated on per month and the low conversion rates suggest high experience. It is probable that new trials will provide better outcomes because of greater experience with laparoscopic techniques. In relation to the generalizability of the results, it is important to highlight that two included studies were from Hong Kong, which could be important especially in relation to age, obesity and comorbid conditions of presenting patients. However, the most recent trial from the Netherlands is a multicenter trial with better generalizability.
This systematic review suggests that a decrease in septic abdominal complications may result when laparoscopic surgery is used to correct a perforated peptic ulcer as compared with open surgery. More trials are needed to confirm such an assumption and to assess the effect of the learning curve on outcomes, thus guaranteeing a long learning curve for participating surgeons.
Quality of the evidence
In general terms the quality of the trials was acceptable. There are concerns about blind assessment of outcomes. This quality criterion is difficult to obtain in surgical trials, where it is impossible to blind evaluators to the surgical group. To improve the outcome evaluation and to be closer to ideal blind assessment, it has been proposed that evaluators who are independent from the treating team, or non‐physician evaluators, are equipped with a predesigned data form and used for the evaluations (Solomon 1998; Thomas 2004). Such strategies were applied in some included clinical trials so we consider that outcomes evaluation, although bias susceptible, was strong enough to support the results, even more so considering that outcomes assessed were hard and not dependent on subjective evaluation. Greater than 20% of participants were lost to follow up at 30 days in the study of Lau 1996. However, it is probable that these losses only affected the measures of time to return to work and to normal activities as surgical complications usually occur during the first week when patients are still in hospital.
Potential biases in the review process
None are known.
Agreements and disagreements with other studies or reviews
From the information provided by the clinical trials included in this review, outcomes from laparoscopic surgery for perforated peptic ulcers are not clinically different from those of open surgery, which is the actual gold standard. With the conversion rates reported in this systematic review, laparoscopic surgery could be the first therapeutic option in patients with perforated peptic ulcer after considering other variables such as experience, costs and availability.
Authors' conclusions
Implications for practice.
With the present data, it is not clear whether laparoscopic surgery offers advantages in terms of a decrease in septic abdominal complications when compared with open surgery. There is a trend towards a reduction in these complications but the limited number of clinical trials prevents any strong conclusion. Surgeons that decide to apply this technology must make a judicious cost‐benefit assessment, about which there is little related evidence.
Implications for research.
It is necessary to have randomized controlled trials with large sample sizes, better outcomes assessments and in different populations. Besides, variables that measure the experience of surgeons with laparoscopic repair must be introduced and assessed. Data for cost and resources consumption variables are also needed.
What's new
| Date | Event | Description |
|---|---|---|
| 6 July 2015 | Amended | Amendment to data on pulmonary complications in abstract. No change to conclusions. |
History
Protocol first published: Issue 2, 2004 Review first published: Issue 4, 2005
| Date | Event | Description |
|---|---|---|
| 3 July 2012 | New citation required but conclusions have not changed | One additional study added to excluded studies. Conclusions unchanged. |
| 3 July 2012 | New search has been performed | Updated. |
| 28 February 2010 | New search has been performed | Updated |
| 30 October 2008 | Amended | Converted to new review format. |
| 26 May 2005 | New citation required and conclusions have changed | Substantive amendment |
| 29 September 2004 | New search has been performed | Minor update |
Acknowledgements
To Iris Gordon, Gemma Sutherington, Racquel Simpson for the help they provided with the search strategy and language amendments. To Jan Lilleyman and Cathy Bennett for editing and methodological advice.
To the Centro Cochrane Iberaoamericano for their support to finish this review and Ivan Sola and Marta Roque for language amendments.
Appendices
Appendix 1. MEDLINE search strategy
randomized controlled trial [pt]
controlled clinical trial [pt]
randomized Field: Title/Abstract
placebo Field: Title/Abstract
randomly Field: Title/Abstract
trial Field: Title/Abstract
groups Field: Title/Abstract
1 OR 2 OR 3 OR 4 OR 4 OR 5 OR 6 OR 7
Limits: Humans
8 AND 9
("Peptic Ulcer"[Mesh] OR "Peptic Ulcer Perforation"[Mesh] OR "Peptic Ulcer Hemorrhage"[Mesh])
duoden* NEAR ulcer*
stomach* NEAR ulcer*
bleed* NEAR ulcer*
rebleed* NEAR ulcer*
gastrointestinal NEAR bleed*
gastrointestinal NEAR rebleed*
gastrointestinal NEAR hemorrhag*
gastrointestinal NEAR haemorrhag*
ulcer NEAR haemorrhag*
ulcer NEAR hemorrhag*
ulcer NEAR perforat*
11 OR 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
laparoscop*
"Laparoscopy"[Mesh]
24 OR 25
23 AND 26
10 AND 27
28 Limits: Publication Date from 2004 to 2009
Data and analyses
Comparison 1. Laparoscopic surgery versus open surgery.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Septic abdominal complications (presence or absence) | 2 | 214 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.30, 1.47] |
| 2 Pulmonary complications (presence or absence) | 3 | 315 | Odds Ratio (M‐H, Random, 95% CI) | 0.52 [0.08, 3.55] |
| 3 Number of septic abdominal complications | 3 | 315 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.60 [0.32, 1.15] |
| 4 Surgical site infection | 3 | 315 | Odds Ratio (M‐H, Random, 95% CI) | 0.28 [0.08, 1.00] |
| 5 Suture dehiscence | 3 | 315 | Odds Ratio (M‐H, Random, 95% CI) | 1.52 [0.29, 7.98] |
| 6 Postoperative ileus | 3 | 315 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.54 [0.16, 1.80] |
| 7 Intra‐abdominal abscess | 3 | 315 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.15 [0.33, 4.03] |
| 8 Incisional hernia | 3 | 315 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.21, 4.15] |
| 9 Mortality | 3 | 315 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.57 [0.18, 1.78] |
| 10 Number of reoperations | 2 | 214 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.89 [0.46, 7.71] |
| 11 Operative time | 2 | 214 | Mean Difference (IV, Random, 95% CI) | 14.62 [‐35.25, 64.49] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Bertleff 2009.
| Methods | 77 months, multicenter RCT parallel design, randomized using computer‐generated random numbers, concealment of allocation using sealed envelopes, outcome assessment was carried out by the treating team, losses to follow up not reported, intention‐to‐treat analysis | |
| Participants | 101 patients (52 for laparoscopic group and 49 for open‐surgery group).
Sex: 61 men/40 women
Mean age: 61 years
Site of perforation: duodenum (34), juxtapyloric (61)
Size of perforation: 10 mm
Age of inclusion not reported, but probably adults.
Inclusion criteria: clinical diagnosis of perforated peptic ulcer made by the surgeon and confirmed at the operation room.
Exclusions criteria:
Inability to read the Dutch language patient information booklet Inability to complete informed consent Prior upper abdominal surgery Current pregnancy. Severity assessed by ASA score (mean 1) and Mannheim Peritonitis Index (mean 16‐19‐5). |
|
| Interventions | Intravenous antibiotics at the diagnosis, type and time not specified. All patients were allocated for Helicobacter pylori eradication therapy. For postoperative analgesia, patients were prescribed opiates. Dose and frequency not specified. Upper midline incisions were made in patients assigned to open repair. Perforations were repaired with sutures alone or in combination with omental patch. For laparoscopic repair, pneumoperitoneum was established (pressure not stated) and three trocars were introduced and the ulcer was closed with sutures alone or in combination with omental patch. The number of participating surgeons, the number of cases previously operated by the surgeon and the number of patients operated by each surgeon or center was not reported. | |
| Outcomes | Postoperative complications Time of nasogastric aspiration Pain assessed with visual analogue scale Conversion rate for laparoscopic group Operation time Time of analgesic use Length of hospital stay | |
| Notes | Sample size was not calculated. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Surgeons contacted the study coordinator" "The envelope randomisation was based on a computer‐generated list provided by the trial statistician" |
| Allocation concealment (selection bias) | Low risk | "randomisation took place by opening a sealed envelope" |
| Blinding (performance bias and detection bias) All outcomes | High risk | "this was an unblinded trial" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing outcome data |
| Selective reporting (reporting bias) | Low risk | Protocol published on the Clinicaltrials.gov website |
| Other bias | Unclear risk | In surgical trials, there is always a bias related with learning curve for the new surgical methods. However, we believe this bias is not present in this trial because the experience of surgeons is similar. In multicenter trials, a bias related with high volume and low volume centers is possible. There is no information about the number of patients by center. |
Lau 1996.
| Methods | 28 months, RCT parallel design, randomized using computer‐generated random numbers by the block method, concealment of allocation using sealed envelopes, outcome assessment was made by two assessors (not stated if independent from the treating team and blind) for pain evaluation and by the treating team for activity, work return evaluation and complications, available to follow‐up at 4 weeks: 73% for laparoscopic group versus 69% for open surgery group but all live patients available at 8 weeks for gastroscopy, to intention‐to‐treat analysis. | |
| Participants | 93 patients (48 for laparoscopic group and 45 for open surgery group). Sex: 79 men/14 women Mean age 47.8 to 52.3 years Site of perforation: duodenum (76), juxtapyloric (11), gastric (6) Size of perforation 1‐25 mm Age of inclusion not reported, but probably adults. Inclusion criteria: Clinical diagnosis of perforated peptic ulcer made by the surgeon and confirmed at the operation room. Exclusions criteria: Complicated ulcers that required definitive surgery (criteria not stated) Bleeding ulcer Previous abdominal operations Serious associated cardiopulmonary diseases Clinically sealed perforation. Severity assessed by APACHE II score. Median 6. | |
| Interventions | Intravenous cefuroxime 750 mg and metronidazole 500 mg were given at the time of induction and for the first postoperative day. For postoperative analgesia, patients were prescribed pethidine 1 mg/kg every 4 hours as required. Upper midline incisions were made in patients assigned to open repair. Perforations were repaired with the Cellan‐Jones method or using a rolled piece of gelatin sponge placed in the perforation and secured with fibrin sealant. For laparoscopic repair, pneumoperitoneum was established at 15 mm Hg, and three trocars were introduced and the ulcer was sutured with a piece of omentum and non‐absorbable suture or using a gelatin and fibrin sealant. The number of participating surgeons, the number of cases previously operated by the surgeon and the number of patients operated by each surgeon was not reported. The study divided laparoscopic and open surgery groups in two groups: one repaired with suture and the other repaired with fibrin sealant. We did not consider this distinction to be important and we re‐aggregated the data. | |
| Outcomes | Complications Time of nasogastric aspiration Time of intravenous fluid maintenance Pain assessed with Visual Analogue Scale Conversion rate for laparoscopic group Operation time Analgesic use Time to resume oral diet Length of hospital stay | |
| Notes | Sample size was calculated using the analgesic doses using a previous study made by the same authors. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Computer‐generated blocked random numbers were used" |
| Allocation concealment (selection bias) | Low risk | "to assign the type of surgery, which was written on a card sealed in a completely opaque envelope. Envelopes were drawn randomly by the senior duty nurse in the operating department" |
| Blinding (performance bias and detection bias) All outcomes | High risk | "All patients were assessed by the treating team approximately 4 weeks postoperatively in the outpatient clinic" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "At the end of 6 to 8 weeks after surgery, gastroscopy showed that the ulcers had healed for all patients", "Similar proportions of patients with laparoscopic repair (group 1 and 2) and open repair (groups 3 and 4) were available at follow‐up (73% vs. 69%), respectively", "The data for patients who did not attend this first follow‐up visit but who were called back for a check‐up gastroscopy were not included in this analysis because there was a delay of at least 1 month in the recording of these data, which made it less reliable" We believe that lost to follow up at four weeks for measuring returning to work do no affect results of important outcomes for this systematic review. |
| Selective reporting (reporting bias) | Low risk | Authors reported a second study in 1998 that is consistent with data from this study. |
| Other bias | Unclear risk | In surgical trials, there is always a bias related with learning curve for the new surgical methods. However, we believe this bias is not present in this trial because experience of surgeons is similar. |
Siu 2002.
| Methods | 41 months, RCT parallel design, randomized using computer‐generated random numbers by the block method, concealment of allocation using sealed envelopes, outcome assessment was made by assessors independent from the treating team for pain evaluation; by independent surgeons not blinded for discharge and by the treating surgeon not blinded for activity, work return evaluation and complications, intention‐to‐treat analysis, without losses to follow up | |
| Participants | 121 patients (63 for the laparoscopic group and 58 for the open surgery group) Sex: 98 men/ 23 women Mean age: 53.8 to 56.1 years Site of perforation: duodenum (93), pyloric‐prepyloric (27), gastric (1) Size of perforation: 4.7 to 5.2 mm Age: patients older than 16 years old Inclusion criteria: Clinical diagnosis of perforated peptic ulcer made by the surgeon and confirmed at the operating room. Exclusion criteria: Gastric outlet obstruction Bleeding ulcer Previous abdominal operations Clinically sealed perforation. Severity assessed by ASA classification and Boey risk factors scale. 81% of patients classified as ASA I and II and 95% as Boey risk scale 0 and 1 (good prognosis). | |
| Interventions | Intravenous cefuroxime 750 mg was given at the time of induction and continued for 5 days. For postoperative analgesia, patients were prescribed pethidine 1 mg/kg every 4 hours as required. Upper midline incisions were made in patients assigned to open repair. Perforations were repaired with the Cellan‐Jones method. For laparoscopic repair, pneumoperitoneum was established at 15 mm Hg, and three trocars were introduced and the ulcer was sutured with a piece of omentum and non‐absorbable suture. The number of participating surgeons, the number of cases previously operated by the surgeon and the number of patients operated by each surgeon was not reported. | |
| Outcomes | Complications Analgesic use Time of nasogastric aspiration Time of intravenous fluid maintenance Pain assessed with Visual Analogue Scale Conversion rate for laparoscopic group Operation time Time to resume oral diet Length of hospital stay | |
| Notes | Sample size was calculated using the analgesic dose data in a previous study by the authors. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomization was performed after the decision was made for surgery; it took place in the operating room control room by a person not otherwise involved in the clinical setting", "computer‐generated random numbers" |
| Allocation concealment (selection bias) | Low risk | "Randomization was undertaken by consecutively numbered opaque sealed envelopes containing the treatment options" |
| Blinding (performance bias and detection bias) All outcomes | High risk | "An independent assessor visited every patient in the morning to record the clinical progress, analgesic requirements, and pain score", "Patients were assessed by independent surgeons for discharge if they could tolerate a normal diet, could fully ambulate, and required only oral analgesics. Both the independent assessor and in‐charge surgeons were not blinded with respect to study groups." Blinding probably do not affect the assessment of hard outcomes as surgical complications, but it is possible that length of stay and pain assessment could be biased by non blinding evaluation of outcomes. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There were no losses to follow up |
| Selective reporting (reporting bias) | Unclear risk | Although there is no other information in the report of the trial, analysis of the article offers enough information to assume that any bias due to selective outcome reporting should not greatly affect the results. |
| Other bias | Unclear risk | In surgical trials, there is always a bias related with learning curve for the new surgical methods. However, we believe this bias is not present in this trial because experience of surgeons is similar. |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Bergamaschi 2000 | Prospective non‐randomized clinical trial |
| Bhogal 2008 | Prospective non‐randomized clinical trial |
| Katkhouda 1999 | Prospective non‐randomized clinical trial |
| Lau 1998 | No data about septic complications |
| Lemaitre 2005 | Prospective non‐randomized clinical trial |
| Mehendale 2002 | Prospective non‐randomized clinical trial |
| Minutolo 2009 | Prospective non‐randomized clinical trial |
| Nicolau 2008 | Prospective non‐randomized clinical trial |
| Robertson 2000 | Prospective non‐randomized clinical trial |
| Vettoretto 2005 | Prospective non‐randomized clinical trial |
Contributions of authors
Conceived, designed and coordinated the review: AES Collected data for the review: CHM, MIV Developed search strategy: AES, CHM, MIV Undertook searches: AES, CHM, MIV Screened search results: AES, CHM, MIV Organized retrieval of papers: CHM, MIV Managed papers retrieval: AES Screened retrieved papers against inclusion criteria: AES, CHM, MIV Appraised quality of papers: CHM, MIV Wrote to authors of papers for additional information: AES Provided additional data about papers: AES Managed data for the review: AES, CHM, MIV Abstracted data from papers: CHM, MIV Entered data into RevMan: AES Analysed data: AES Interpreted data: AES, CHM, MIV Provided a methodological perspective: AES, CHM, MIV Provided a clinical perspective: AES, CHM, MIV Wrote the review: AES, CHM, MIV
Sources of support
Internal sources
Universidad de La Sabana, Chia., Colombia.
Grupo de Epidemiologia Clínica. Facultad de Medicina. Universidad de Antioquia, Colombia.
External sources
Latinoamerican Clinical Epidemiology Network Scolarship, Colombia.
Centre Cochrane Iberoamericà, Spain.
Declarations of interest
None known
Edited (no change to conclusions)
References
References to studies included in this review
Bertleff 2009 {published data only}
- Bertleff MJ, Halm JA, Bemelman WA, Ham AC, Harst E, Oei HI, et al. Randomized clinical trial of laparoscopic versus open repair of the perforated peptic ulcer: the LAMA Trial. World Journal of Surgery 2009;33:1368‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lau 1996 {published data only}
- Lau WY, Leung KL, Kwong KH, Davey IC, Robertson C, Dawson JJ, et al. A randomized study comparing laparoscopic versus open repair of perforated peptic ulcer using suture or sutureless technique. Annals of Surgery 1996;224:131‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Siu 2002 {published data only}
- Siu WT, Leong HT, Law BK, Chau CH, Li AC, Fung KH, et al. Laparoscopic repair for perforated peptic ulcer: a randomized controlled trial. Annals of Surgery 2002;235:313‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Bergamaschi 2000 {published data only}
- Bergamaschi R. Laparoscopic surgery for uncomplicated diverticulitis: advantages?. Scandinavian Journal of Gastroenterology 2000;35:449‐51. [DOI] [PubMed] [Google Scholar]
Bhogal 2008 {published data only}
- Bhogal RH, Athwal R, Durkin D, Deakin M, Cheruvu CN. Comparison between open and laparoscopic repair of perforated peptic ulcer disease. World Journal of Surgery 2008;32(11):2371‐4. [DOI] [PubMed] [Google Scholar]
Katkhouda 1999 {published data only}
- Katkhouda N, Mavor E, Mason RJ, Campos GM, Soroushyari A, Berne TV. Laparoscopic repair of perforated duodenal ulcers: outcome and efficacy in 30 consecutive patients. Archives of Surgery 1999;134:845‐8. [DOI] [PubMed] [Google Scholar]
Lau 1998 {published data only}
- Lau JY, Lo SY, Ng EK, Lee DW, Lam YH, Chung SC. A randomized comparison of acute phase response and endotoxemia in patients with perforated peptic ulcers receiving laparoscopic or open patch repair. American Journal of Surgery 1998;175:325‐7. [DOI] [PubMed] [Google Scholar]
Lemaitre 2005 {published data only}
- Lemaitre J, El Founas W, Simoens C, Ngongang C, Smets D, Mendes da Costa P. Surgical management of acute perforation of peptic ulcers. A single centre experience. Acta Chirurgica Belgica 2005;105:588‐91. [DOI] [PubMed] [Google Scholar]
Mehendale 2002 {published data only}
- Mehendale VG, Shenoy SN, Joshi AM, Chaudhari NC. Laparoscopic versus open surgical closure of perforated duodenal ulcers: a comparative study. Indian Journal of Gastroenterology 2002;21:222–4. [PubMed] [Google Scholar]
Minutolo 2009 {published data only}
- Minutolo V, Gagliano G, Rinzivillo C, Minutolo O, Carnazza M, Racalbuto A, et al. Laparoscopic surgical treatment of perforated duodenal ulcer. Chirurgia Italiana 2009;61:309‐13. [PubMed] [Google Scholar]
Nicolau 2008 {published data only}
- Nicolau AE, Merlan V, Veste V, Micu B, Beuran M. Laparoscopic suture repair of perforated duodenal peptic ulcer for patients without risk factors. Chirurgia (Bucur) 2008;103:629‐33. [PubMed] [Google Scholar]
Robertson 2000 {published data only}
- Robertson GS, Wemyss‐Holden SA, Maddern GJ. Laparoscopic repair of perforated peptic ulcers. The role of laparoscopy in generalised peritonitis. Annals of the Royal College of Surgeons of England 2000;82:6‐10. [PMC free article] [PubMed] [Google Scholar]
Vettoretto 2005 {published data only}
- Vettoretto N, Poiatti R, Fisogni D, Diana DR, Balestra L, Giovanetti M. Comparison between laparoscopic and open repair for perforated peptic ulcer. Chirurgia Italiana 2005;57:317‐22. [PubMed] [Google Scholar]
Additional references
Benoit 1993
- Benoit J, Champault GG, Lebhar E, Sezeur A. Sutureless laparoscopic treatment of perforated duodenal ulcer. British Journal of Surgery 1993;80:1212. [DOI] [PubMed] [Google Scholar]
Chekan 1999
- Chekan EG, Pappas TN. The laparoscopic management of gastroesophageal reflux disease. Advances in Surgery 1999;32:305‐30. [PubMed] [Google Scholar]
Chou 2000
- Chou NH, Mok KT, Chang HT, Liu SI, Tsai CC, Wang BW, Chen IS. Risk factors of mortality in perforated peptic ulcer. European Journal of Surgery 2000;166:149‐53. [DOI] [PubMed] [Google Scholar]
Consensus 1997
- Anonymous. Laparoscopic antireflux surgery for gastroesophageal reflux disease (GERD). Results of a Consensus Development Conference. Held at the Fourth International Congress of the European Association for Endoscopic Surgery (E.A.E.S.), Trondheim, Norway. Surgical Endoscopy 1997;11:413‐26. [PubMed] [Google Scholar]
Darzi 1993
- Darzi A, Cheshire NJ, Somers SS, Super PA, Guillou PJ, Monson JR. Laparoscopic omental patch repair of perforated duodenal ulcer with an automated stapler. British Journal of Surgery 1993;80:1552. [DOI] [PubMed] [Google Scholar]
Druart 1997
- Druart ML, Hee R, Etienne J, et al. Laparoscopic repair of perforated duodenal ulcer. A prospective multicenter clinical trial. Surgical Endoscopy 1997;11:1017‐20. [DOI] [PubMed] [Google Scholar]
Gadacz 2000
- Gadacz TR. Update on laparoscopic cholecystectomy, including a clinical pathway. Surgical Clinics of North America 2000;80:1127‐49. [DOI] [PubMed] [Google Scholar]
Garner 1996
- Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. APIC Infection Control and Applied Epidemiology: Principles and practice. First Edition. St Louis: Mosby, 1996. [Google Scholar]
Gomez‐Ferrer 1996
- Gomez‐Ferrer F, Balique JG, Azagra S, et al. Laparoscopic surgery for duodenal ulcer: first results of a multicentre study applying a personal procedure. British Journal of Surgery 1996;83:547‐50. [DOI] [PubMed] [Google Scholar]
Hermansson 1999
- Hermansson M, Stael von Holstein C, Zilling T. Surgical approach and prognostic factors after peptic ulcer perforation. European Journal of Surgery 1999;165:566‐72. [DOI] [PubMed] [Google Scholar]
Higgins 2008
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1[updated September 2008]. The Cochrane Collaboration. Available from www.cochrane‐handbook.org., 2008. [Google Scholar]
Horgan 1997
- Horgan S, Pellegrini CA. Surgical treatment of gastroesophageal reflux disease. Surgical Clinics of North America 1997;77:1063‐82. [DOI] [PubMed] [Google Scholar]
Klingler 1999
- Klingler PJ, Bammer T, Wetscher GJ, et al. Minimally invasive surgical techniques for the treatment of gastroesophageal reflux disease. Digestive Diseases 1999;17:23‐36. [DOI] [PubMed] [Google Scholar]
Kum 1993
- Kum CK, Isaac JR, Tekant Y, Ngoi SS, Goh PM. Laparoscopic repair of perforated peptic ulcer. British Journal of Surgery 1993;80:535. [DOI] [PubMed] [Google Scholar]
Lau 1995
- Lau WY, Leung KL, Zhu XL, Lam YH, Chung SC, Li AK. Laparoscopic repair of perforated peptic ulcer. British Journal of Surgery 1995;82:814‐6. [DOI] [PubMed] [Google Scholar]
Lee 2001
- Lee FY, Leung KL, Lai PB, Lau JW. Selection of patients for laparoscopic repair of perforated peptic ulcer. British Journal of Surgery 2001;88:133‐6. [DOI] [PubMed] [Google Scholar]
Matsuda 1995
- Matsuda M, Nishiyama M, Hanai T, Saeki S, Watanabe T. Laparoscopic omental patch repair for perforated peptic ulcer. Annals of Surgery 1995;221:236‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
Michelet 2000
- Michelet I, Agresta F. Perforated peptic ulcer: laparoscopic approach. European Journal of Surgery 2000;66:405‐8. [DOI] [PubMed] [Google Scholar]
Mouret 1990
- Mouret P, Francois Y, Vignal J, Barth X, Lombard‐Platet R. Laparoscopic treatment of perforated peptic ulcer. British Journal of Surgery 1990;77:1006. [DOI] [PubMed] [Google Scholar]
Naesgaard 1999
- Naesgaard JM, Edwin B, Reiertsen O, Trondsen E, Faerden AE, Rosseland AR. Laparoscopic and open operation in patients with perforated peptic ulcer. European Journal of Surgery 1999;165:209‐14. [DOI] [PubMed] [Google Scholar]
Ozmen 1995
- Ozmen V, Muslumanoglu M, Igci A, Bugra D. Laparoscopic treatment of duodenal ulcer by bilateral truncal vagotomy and endoscopic balloon dilatation. Journal of Laparoendoscopic Surgery 1995;5:21‐6. [DOI] [PubMed] [Google Scholar]
Paimela 1991
- Paimela H, Tuompo PK, Perakyl T, Saario I, Hockerstedt K, Kivilaakso E. Peptic ulcer surgery during the H2‐receptor antagonist era: a population‐based epidemiological study of ulcer surgery in Helsinki from 1972 to 1987. British Journal of Surgery 1991;78:28‐31. [DOI] [PubMed] [Google Scholar]
Pamoukian 2001
- Pamoukian VN, Gagner M. Laparoscopic necrosectomy for acute necrotizing pancreatitis. Journal of Hepatobiliary and Pancreatic Surgery 2001;8:221‐3. [DOI] [PubMed] [Google Scholar]
Rickard 2001
- Rickard MJ, Bokey EL. Laparoscopy for colon cancer. Surgical Oncology Clinics of North America 2001;10:579‐97. [PubMed] [Google Scholar]
Sauerland 2004
- Sauerland S, Lefering R, Neugebauer EA. Laparoscopic versus open surgery for suspected appendicitis. Cochrane Database of Systematic Reviews 2004, Issue 4. [DOI: 10.1002/14651858.CD001546.pub3] [DOI] [PubMed] [Google Scholar]
Solomon 1998
- Solomon M, McLeod R. Surgery and the randomised controlled trial: past, present and future. Medical Journal of Australia 1998;169:380‐3. [DOI] [PubMed] [Google Scholar]
Sunderland 1992
- Sunderland GT, Chisholm EM, Lau WY, Chung SC, Li AK. Laparoscopic repair of perforated peptic ulcer. British Journal of Surgery 1992;79:785. [DOI] [PubMed] [Google Scholar]
Svanes 1995
- Svanes C, Lie RT, Kvale G, Svanes K, Soreide O. Incidence of perforated ulcer in western Norway, 1935‐1990: cohort‐ or period‐dependent time trends?. American Journal of Epidemiology 1995;141:836‐44. [DOI] [PubMed] [Google Scholar]
Tate 1993
- Tate JJ, Dawson JW, Lau WY, Li AK. Sutureless laparoscopic treatment of perforated duodenal ulcer. British Journal of Surgery 1993;80:235. [DOI] [PubMed] [Google Scholar]
Thomas 2004
- Thomas A, Farrokhyar F, Bhandari M, Tandan V. Users’ guide to the surgical literature How to assess a randomized controlled trial in surgery. Canadian Journal of Surgery 2004;47:200‐8. [PMC free article] [PubMed] [Google Scholar]
Tisminezky 2000
- Tisminezky B, Nelson H. Laparoscopic approach to colon cancer. Advances in Surgery 2000;34:67‐119. [PubMed] [Google Scholar]
Walsh 1993
- Walsh CJ, Khoo DE, Motson RW. Laparoscopic repair of perforated peptic ulcer. British Journal of Surgery 1993;80:127. [PubMed] [Google Scholar]