

Abstract
Background:
Preeclampsia (PE) is a multisystem pregnancy disorder that increases maternal-perinatal morbidity and mortality significantly. MicroRNA-155 (miR-155) overexpression in the sera of pregnant women has been linked to preeclampsia. Researchers discovered that miR-155 acts during pregnancy by down-regulating and reducing the cysteine-rich angiogenic inducer 61 (CYR61), which causes local ischemia as well as oxidative stress.
Methods:
The level of miR-155 expression in all serum samples was quantified using real-time polymerase chain reaction (RT-PCR), and serum CYR61 was measured using enzyme-linked immunosorbent assays. Together with the Cyr-61/miR-155 ratio, they were evaluated as biomarkers for PE pathogenesis and severity prediction.
Results:
MiR-155 expression, serum CYR61 levels, and Cyr-61/miR-155 ratios were all significantly higher in PE patients compared to the control group. Serum CYR61 levels and the Cyr-61/miR-155 ratio differed significantly between mild and severe PE patients.
Conclusions
MiR-155 expression, serum CYR61 levels, and Cyr-61/miR-155 may serve as biomarkers for PE pathogenesis and severity prediction.
Key Words: Biomarker, Cysteine-Rich Protein 61, MicroRNAs, Pre-Eclampsia
Introduction
Pre-eclampsia (PE), a multi-system disorder affecting 5-8% of overall pregnancies; is common throughout the 20th gestational week and until the end of pregnancy. It is a major cause of maternal-prenatal morbidity as well as mortality (1). PE's hallmark symptoms are arterial hypertension, oedema, and proteinuria. In addition, neurological complaints like headache associated with nausea and vomiting are common with PE (2, 3). Although early-onset PE, which happens even before the 33rd week of gestation, is relatively uncommon, it is associated with agreater incidence of both maternal as well as fatal comorbidities, particularly in comparison to late-onset PE (4, 5).
Several inherited, angiogenic, developmental, and/or metabolite deregulators have been implicated in PE spiral artery remodeling, placental oxygenation, immune and redox toleration at the mother-foetal interface, as well as angiogenic and antiangiogenic disbalancing factors that precipitate chronic placental oxygen lack and ischemia (1).
A small noncoding RNA molecule known as microRNAs (miRNAs; containing 18–27 nucleotides) regulates the synthesis of more than 30% of the overall gene products, which are proteins. As a result, miRNAs play a vital mechanistic regulatory role in nearly every biological process, including proliferation, differentiation, apoptosis, angiogenesis, immune response, embryonic development, and others, and thus their dysregulation is considered one of the patho-mechanistics of many diseases, including PE (6). miRNAs are expressed by placental tissue during pregnancy, and their concentration varies based on weeks of gestation and the placental growth phase, highlighting their importance in placental regulation (7).
Definite deregulated miRNAs are confirmed to be specific to the placental pathogenesis of PE as well as the liver, brain, immune system, and kidney affections. Therefore, PE is considered a multisystem disorder because any deregulation of these miRNAs affects the normal function of target genes in the placenta as well as in those systems (8, 9). MiR-155, which has been linked to impaired cytotrophoblast differentiation and apoptosis, incomplete spiral artery invasion, and decreased blood flow to and from the placenta, was discovered in the sera of pregnant women with PE (10). Overexpression of miR-155 was proven to contribute to preeclampsia by down-regulating cysteine-rich angiogenic inducer 61 (CYR61), an early angiogenic regulating element throughout pregnancy, in addition to reducing its stability and resulting in local ischemia with subsequent oxidative stress (4).
Materials and Methods
Subjects
All participants provided written informed consent prior to participating in the study. In this case control study, from August 2019 to February 2021, 50 pregnant women with PE who were presented to Tanta University Hospitals' Gynaecology and Obstetrics Department were divided into two groups matched in age. The first one included twenty-five cases of mild PE. The other twenty-five cases were of severe PE. Another twenty-five healthy pregnant women matched for age and sex were represented in the control group (III). PE severity is determined according to the American College of Obstetricians and Gynaecologists (ACOG) criteria. Mild PE patients should have a blood pressure of 140/90 mmHg and proteinuria of more than 0.3 g/L per day. Those with severe PE, on the other hand, have a blood pressure of have a blood pressure of 160/110 mmHg and proteinuria of more than 5.0 g/L per day (11).
Blood collection
A full, detailed history had been obtained for all cases aligned within the study, including age, gravidity, positive family history, gestational age, and the onset of PE, as well as clinical examinations including blood pressure, oedema, weight, height, and BMI. 24-hour urine sample was collected and centrifuged for protein estimation using a turbidimetric method (using TCA at 3%, by Biosystem reagent kit on a semi- automated analyser, the BTS-350 (Biosystem S.A., Barcelona, Spain). Blood samples: 6 mL of venous blood was gathered under complete aseptic conditions and subdivided into three compartments. The first was one mL of blood treated with EDTA for CBC analysis on an electronic automatic analyser (ERMA Inc. Poland, 3459.9020). The second was 1.6 ml of blood added to a Na citrated tube for a coagulation profile (PT, INR, and PTT) using an automated coagulometer (Stago STA compact using kits from DIAGNOSTICA STAGO. Neoptimal 10, 01164, PTT, 00595 and CaCl2 0.025 M, 00367). The remainder of the blood was drawn into a plain tube, and the separated serum was aliquoted and stored at -80 °C for further analysis.
Biochemical assays
Liver enzymes and renal functions were measured by KONELAB PRIME 60i apparatus using kits obtained from Thermo Fisher Scientific Oy-Finland (981769, 981771, 981820, and 981811, respectively for ALT, AST, serum urea, and serum creatinine).
Measurement of serum level of CYR61 Using Enzyme-linked Immunosorbent Assay Kit for CYR61, from R &D systems (DCYR10): The quantitative sandwich enzyme immunoassay technique was used in this assay with a microplate that had been pre-coated with a human Cyr61 specific monoclonal antibody. Upon pipetting each of standards and / or samples into the wells, the immobilized antibody bound to any Cyr61 present. An enzyme linked human Cyr61 specific polyclonal antibody was added to the wells just after the precise removal of any unbound substances, followed by another wash, addition of substrate solution with subsequent colour propagation that proportionate to the amount of well bounded Cyr61in the initial step, and finally, colour propagation was halted, and its intensity was analysed.
MiR-515 expression level by RT-PCR
The miRNeasy Mini Kit had been used for total RNA extraction with miRNA from specimens (217004, Qiagen, Germany). Purity of RNA was ascertained using a Nanodrop 2000 spectrophotometer (USA) by dividing the maximum absorption ratio at 260 nm on that at 280 nm to calculate a ratio of 2.0 to 2.2. cDNA was generated using the miScriptII RT Kit (217004 QIAGEN, Germany) for RT qPCR reverse transcription (1st step). miR-155 detection by miScript SYBR Green PCR kit (Qiagen NV, 217004) was carried out in a 25 μl final volume containing 2.5 μl of each of the following: cDNA, miScript universal primer, miScript primer assay (RNU6B or miR-155) with 5 μl of RNAse free water, and 12.5 μl of SYBR Green PCR Master mix. Forward and reverse miR primers were provided by (Qiagen, Germany) with sequences of 5′-GCTTCGGCAGCACATATACTAAAAT-3′; and 5′-CGCTTCACGAATTTGCGTGTCAT3′. for RNU6B and 5′-CTGTTAATGCTAATCGTGATAG-3′ and 5′-GCAGGGTCCGAGGT-3′ for miR-155. Real-time PCR was carried out on an Applied Biosystems (USA) Real-time PCR cycler under the following conditions: Initial activation at 95 °C for 15 minutes was followed by 40 cycles of denaturation at 94 °C for 30 seconds, annealing at 55 °C for 1 minute, and extension at 70 °C for 1 minute, during which fluorescence was acquired. Because there is no control for miR in serum, we used the U6B small nuclear RNA gene (RNU6B) as an endogenous control. RNU6B was easily detectable in serum, and there was no significant difference in RNU6B cycle threshold (Ct) values between controls and other samples. We chose RNU6B as the normalization control because its expression levels were more stable and variable. Relative expression of miR-155 was calculated using 2 - Δ Ct formula Where CT = (CT miR – CT control) and Ct is the fractional cycle number at which the fluorescence passes the fixed threshold.
Statistical Analysis
SPSS V.16 was used for statistical presentation and analysis of the current study, which included the mean, standard deviation, unpaired student "t" test, and Fisher's exact test.
Results
Demographic and clinical features of the studied groups
This study included 50 pregnant women with PE divided into two groups: group (I): included 25 cases with mild PE, group (II): included 25 cases of severe PE and 25 healthy pregnant women matched for age and sex representing the control group.
The general characteristics of the study population were summarized in Table 1. It shows no significant difference between patients with PE and control groups regarding their gestational age, and body mass index. However, maternal age, systolic and diastolic arterial blood pressure were significantly increased in PE patients than controls. Gestational age, systolic and diastolic arterial blood pressure were significantly higher in severe PE compared to patients with mild PE (Table 1).
Table 1.
General characteristics and routine investigations.
| Factor | Controls | PE cases | P-value | Mild PE | Severe PE | P-value |
|---|---|---|---|---|---|---|
| (n = 25) | (n = 50) | (n = 25) | (n = 25) | |||
| Maternal age (years) | 27.0 ± 2.4 | 28.5 ± 2.3 | 0.01* | 28.0 ± 2.5 | 29.0 ± 1.96 | 0.120 |
| Gestational age (weeks) | 32 ± 2 | 31 ± 3 | 0.088 | 32 ± 2 | 30 ± 3 | 0.004* |
| BMI | 32.7 ± 3.6 | 33.7 ± 2.5 | 0.221 | 33.5 ± 2.5 | 33.8 ± 2.5 | 0.667 |
| SBP (mmHg) | 115 ± 7 | 156 ± 10 | < 0.001* | 148 ± 5 | 165 ± 7 | < 0.001* |
| DBP (mmHg) | 70 ± 7 | 115 ± 11 | < 0.001* | 105 ± 4 | 125 ± 4 | < 0.001* |
| Hb (g/dl) | 10.0 ± 0.7 | 9.9 ± 0.7 | 0.633 | 10.0 ± 0.7 | 9.8 ± 0.8 | 0.435 |
| PT (sec) | 12.2 ± 0.7 | 12.4 ± 0.6 | 0.320 | 12.3 ± 0.7 | 12.5 ± 0.6 | 0.265 |
| PTT (sec) | 29.1 ± 1.1 | 30.0 ± 1.3 | 0.003* | 30.0 ± 1.3 | 30.0 ± 1.4 | 0.983 |
| Urea (mg/dl) | 28.0 ± 4.0 | 32.7 ± 6.3 | < 0.001* | 32.3 ± 5.7 | 33.0 ± 6.9 | 0.706 |
| Creatinine (mg/dl) | 0.9 ± 0.2 | 0.7 ± 0.2 | < 0.001* | 0.7 ± 0.3 | 0.7 ± 0.21 | 1.000 |
| ALT (IU/L) | 30 (21) | 46.5 (58) | 0.001* | 42 (65) | 50 (57) | 0.727 |
| AST (IU/l) | 24 (18) | 40.5 (52) | 0.001* | 33 (62) | 45 (53) | 0.554 |
| Proteinuria | 75 (29) | 1640 (1128) | < 0.001* | 1480 (1145) | 1950 (3200) | 0.001* |
The routine investigations were summarized in Table 1, it shows no significant difference between patients with PE and control groups regarding Hb and PT, but PTT, urea, creatinine, AST, ALT, and Proteinuria were highly significant increase in patients with PE than controls. However, creatinine was statistically significantly lower in patients compared to controls, but it was within the normal range.
There are no statistically significant differences between mild and severe PE patients regarding HB, PT, PTT, urea, creatinine, AST, and ALT. But proteinuria was significantly increased in severe PE.
CYR61 / miR-155 Ratio as biomarker for PE Diagnosis
As shown in Fig. 1 there was correlation between CYR61 and miR-155, Significant differences were observed in serum level of CYR61 / miR-155 between patients and control group (Figs. 2A & B) diagnostic accuracy of miR-155, CYR-61, or CYR-61/miR-155 ratio as biomarkers for PE, a ROC curve was calculated. The value of the area under the ROC curve (AUC) between 0.5 and 1 is considered having diagnostic significance. (Table 2 & Fig. 3A).
Fig. 1.

Correlation between cyr61 and miR-155 expression.
Fig. 2.
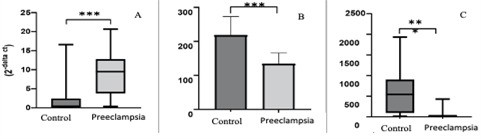
A: miR-155 expression between PE pregnancies and healthy pregnancies; 2.B: Serum level of CYR-61 between PE pregnancies and healthy pregnancies, and 2.C: CYR-61/ miR-155 ratio between PE pregnancies and healthy pregnancies.
Table 2.
miR-155 expression, serum level of CYR61 and CYR61 /miR-155 ratio between patients and controls.
| AUC | 95% CI | P-value | Cutoff value | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|
| miR-155 (2 - Δ Ct) | 0.845 | 0.743-0.918 | < 0.001 | > 2.820 | 78.0 | 84.0 |
| Cyr-61 | 0.892 | 0.799-0.952 | < 0.001 | ≤ 186 | 100.0 | 80.0 |
| Cyr-61/miR-155 | 0.8930 | 0.800-0.952 | < 0.001 | ≤ 36.79 | 78.0 | 88.0 |
| Mild PE vs. severe PE | ||||||
| miR-155(2 - Δ Ct) | 0.621 | 0.473-0.754 | 0.135 | > 6.69 | 76.0 | 48.0 |
| Cyr-61 | 0.983 | 0.831-0.986 | < 0.001 | ≤ 120 | 88.0 | 100.0 |
Fig. 3.

A: ROC curve analysis for miRNA 155, CYR-61 and CYR-61 ratio between the cases of PE pregnancies and healthy pregnancies; 3.B: ROC curve analysis for miRNA 155, CYR-61 and CYR-61 ratio between mild and severe PE pregnancies.
CYR61 / miR-155 as marker for severity of PE
Diagnostic accuracy of miR-155, CYR-61, or CYR-61/miR-155 ratio, ROC curve was calculated. (Fig. 3 & Table 2).
There were significant differences between mild and severe patients with PE in serum level of Cyr-61 and Cyr-61/miR-155 ratio. However, there were no significant differences between mild and severe patients with PE in miR-155 expression (p= 0.135) as shown in Fig. 4A.
Fig. 4.

A: miR-155 expression between mild and severe PE pregnancies; 4.B: Serum level of CYR-61 between mild and severe PE pregnancies, and 4.C: CYR-61/ miR-155 ratio between mild and severe PE pregnancies. PE: Preeclampsia.
Discussion
The present study was carried out to determine the CYR61/ miR-155 expression ratio in both mild and severe PE in comparison to the control group, and to find the possible association with the PE severity. According to the general laboratory data of the groups, there was no statistically significant difference in Hb and PT between patients and controls, but PTT, urea, AST, ALT, and proteinuria were significantly higher in PE patients than controls. These findings agree with those of other studies by Han et al. (2014) and Jahromi & Rafiee (2009), which found that PTT levels are higher in patients with severe PE than in controls. (12,13). Feldstein et al. 2019 discovered that patients with severe PE had an abnormal coagulation profile (14). It was explained by a degree of coagulative dysfunction in the endogenous coagulative pathways of severe PE, whereas the exogenous coagulative pathways remained unchanged (15). Dong et al., 2017 and Chung & To 2018 agree with our findings regarding proteinuria which is caused by reversible renal disease (16,17).
Along with miR-155, a higher expression level in PE patients was found when compared to controls. These findings supported the findings of Gan et al. (2017), who found that miR-155 levels were significantly higher in PE compared to healthy pregnant females (18). Jairajpuri et al. (2017) discovered that miR-155 was up-regulated in women with PE when compared to controls women because it interferes with trophoblastic migration,thereby inhibiting the placental angiogenesis which triggers PE (19). There were no significant differences in miR-155 expression between mild and severe PE patients throughout this study. Also, Youssef and Marei 2019 reported that miR-155 could not be used to predict the severity of PE (20). Furthermore, Kolkova et al. 2021 discovered a 1.62-fold increase in miR-155 expression in the plasma of severe PE patients versus controls, but not between mild PE patients and controls. In addition, they discovered a statistically significant difference between unselected PE patients and normal pregnancies, as well as a slight upregulation of miR-155 in both severe and late-onset PE when compared to physiological pregnancies. They found no significant differences in its expression level when comparing PE patients based on the onset and/or severity of PE (11).
These findings contradicted the findings of Zhang et al. (2010), who identified miR-155 as a PE marker and determinant of severity. There were statistically significant differences in CYR61 concentrations between mild and severe preeclampsia patients and healthy controls (P= >0.000). Furthermore, when compared to normotensive gestational-matched controls, Gellhaus et al. (2006) discovered a significant decrease in early-onset PE placental CYR61 (21, 22). In 2010, Zhang et al discovered for the first time that miR-155 contributed to PE by downregulating CYR61, an early angiogenic regulating factor during pregnancy, expression and decreasing its stability, which was involved in the initiation of local hypoxia as well as oxidative stress (4).
We discovered that miR-155, CYR-61, and the ratio of CYR-61/miR-155 expression had the potential to be diagnostic biomarkers in our study using the ROC analysis which is a widely accepted method in analysis and comparing the diagnostic accuracy of body fluid tests. We found that miR-155, CYR-61, and the CYR-61/miR-155 expression ratio had diagnostic power, with AUCs of 0.845, 0.892, and 0.8930, respectively, using ROC analysis. According to these findings, miR-155 expression and serum CYR-61 levels can be used as specific and sensitive tests for the diagnosis of PE.
Our findings confirmed an increase in miR-155 in PE pregnancies in comparison to healthy pregnancies, as well as an increase in the CYR-61/miR-155 ratio in healthy and mild PE pregnancies compared to severe PE pregnancies.
Consent to Participate
All participants provided written informed consent prior to participating in the study.
Ethical approval
The present study was approved by the Scientific Research Ethics Committee of Tanta University (approval code 35795/9/22).
Funding
The authors declare that no funds, grants, or other support were received during preparation of this manuscript.
Conflict of Interests
The authors have no relevant financial or non-financial interests to disclose.
Acknowledgements
The authors have many thanks to our colleagues in Clinical Pathology & Biochemistry departments for their help.
References
- 1.Phipps EA, Thadhani R, Benzing T, Karumanchi SA. Pre-eclampsia: pathogenesis, novel diagnostics and therapies. Nat Rev Nephrol. 2019;15(5):275–289. doi: 10.1038/s41581-019-0119-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gathiram P, Moodley J. Pre-eclampsia: its pathogenesis and pathophysiolgy. Cardiovasc J Afr. 2016;27(2):71–8. doi: 10.5830/CVJA-2016-009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Koushki M, Amiri Dash Atan N, Omidi-Ardali H, Rezaei Tavirani M. Assessment of Correlation Between miR-210 Expression and Pre-Eclampsia Risk: A Meta-Analysis. Rep Biochem Mol Biol. 2018;7(1):94–101. [PMC free article] [PubMed] [Google Scholar]
- 4.Zhang Y, Diao Z, Su L, Sun H, Li R, Cui H, Hu Y. MicroRNA-155 contributes to preeclampsia by down-regulating CYR61. Am J Obstet Gynecol. 2010;202(5):466. doi: 10.1016/j.ajog.2010.01.057. [DOI] [PubMed] [Google Scholar]
- 5.Al-Kawaz HS, Yasser OM, Mousa MJ. A New Method to Estimate Inhibition Percentage of Endogenous Digitalis in Patients with Pre-eclampsia. Rep Biochem Mol Biol. 2022;11(1):138–145. doi: 10.52547/rbmb.11.1.138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Luo R, Wang Y, Xu P, Cao G, Zhao Y, Shao X, Li YX, Chang C, Peng C, Wang YL. Hypoxia-inducible miR-210 contributes to preeclampsia via targeting thrombospondin type I domain containing 7A. Sci Rep. 2016;6:19588. doi: 10.1038/srep19588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Addo KA, Palakodety N, Hartwell HJ, Tingare A, Fry RC. Placental microRNAs: Responders to environmental chemicals and mediators of pathophysiology of the human placenta. Toxicol Rep. 2020;7:1046–1056. doi: 10.1016/j.toxrep.2020.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Xu P, Ma Y, Wu H, Wang YL. Placenta-Derived MicroRNAs in the Pathophysiology of Human Pregnancy. Front Cell Dev Biol. 2021;9:646326. doi: 10.3389/fcell.2021.646326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Vashukova ES, Glotov AS, Baranov VS. MicroRNAs Associated with Preeclampsia. Russ J Genet. 2020;56(1):1–16. [Google Scholar]
- 10.Zhang M, Muralimanoharan S, Wortman AC, Mendelson CR. Primate-specific miR-515 family members inhibit key genes in human trophoblast differentiation and are upregulated in preeclampsia. Proc Natl Acad Sci U S A. 2016;113(45):E7069–E7076. doi: 10.1073/pnas.1607849113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kolkova Z, Holubekova V, Grendar M, Nachajova M, Zubor P, Pribulova T, Loderer D, et al. Association of Circulating miRNA Expression with Preeclampsia, Its Onset, and Severity. Diagnostics (Basel). 2021;11(3):476. doi: 10.3390/diagnostics11030476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Han L, Liu X, Li H, Zou J, Yang Z, Han J, et al. Blood coagulation parameters and platelet indices: changes in normal and preeclamptic pregnancies and predictive values for preeclampsia. PLoS One. 2014;9(12):e114488. doi: 10.1371/journal.pone.0114488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Namvar Jahromi B, Rafiee SH. Coagulation factors in severe preeclampsia. Iran Red Crescent Med J. 2009;11(3):321–324. [Google Scholar]
- 14.Feldstein O, Kovo M, Tal O, Braunstein M, Grinstein E, Schreiber L, Bar J, Weiner E. The association between abnormal coagulation testing in preeclampsia, adverse pregnancy outcomes, and placental histopathology. Hypertens Pregnancy. 2019;38(3):176–183. doi: 10.1080/10641955.2019.1638396. [DOI] [PubMed] [Google Scholar]
- 15.Szabo G, Bala S. MicroRNAs in liver disease. Nat Rev Gastroenterol Hepatol. 2013;10(9):542–52. doi: 10.1038/nrgastro.2013.87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Dong X, Gou W, Li C, Wu M, Han Z, Li X, Chen Q. Proteinuria in preeclampsia: Not essential to diagnosis but related to disease severity and fetal outcomes. Pregnancy Hypertens. 2017;8:60–64. doi: 10.1016/j.preghy.2017.03.005. [DOI] [PubMed] [Google Scholar]
- 17.Chung WH, To WWK. Outcome of pregnancy with new onset proteinuria and progression to pre-eclampsia: A retrospective analysis. Pregnancy Hypertens. 2018;12:174–177. doi: 10.1016/j.preghy.2017.11.007. [DOI] [PubMed] [Google Scholar]
- 18.Gan L, Liu Z, Wei M, Chen Y, Yang X, Chen L, Xiao X. MiR-210 and miR-155 as potential diagnostic markers for pre-eclampsia pregnancies. Medicine (Baltimore). 2017;96(28):e7515. doi: 10.1097/MD.0000000000007515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jairajpuri DS, Malalla ZH, Mahmood N, Almawi WY. Circulating microRNA expression as predictor of preeclampsia and its severity. Gene. 2017;627:543–548. doi: 10.1016/j.gene.2017.07.010. [DOI] [PubMed] [Google Scholar]
- 20.Youssef HMG, Marei ES. Association of MicroRNA-210 and MicroRNA-155 with severity of preeclampsia. Pregnancy Hypertens. 2019;17:49–53. doi: 10.1016/j.preghy.2019.05.010. [DOI] [PubMed] [Google Scholar]
- 21.Gellhaus A, Schmidt M, Dunk C, Lye SJ, Kimmig R, Winterhager E. Decreased expression of the angiogenic regulators CYR61 (CCN1) and NOV (CCN3) in human placenta is associated with pre-eclampsia. Mol Hum Reprod. 2006;12(6):389–99. doi: 10.1093/molehr/gal044. [DOI] [PubMed] [Google Scholar]
- 22.Wang Z, Shan Y, Yang Y, Wang T, Guo Z. MicroRNA-155 is upregulated in the placentas of patients with preeclampsia and affects trophoblast apoptosis by targeting SHH/GLi1/BCL2. Hum Exp Toxicol. 2021;40(3):439–451. doi: 10.1177/0960327120954252. [DOI] [PubMed] [Google Scholar]