

Abstract
Background:
Climate change is causing an increase in extreme heat. Individuals with cardiovascular disease are at a high risk of heat-related adverse health effects. How the burden of extreme heat associated cardiovascular deaths in the United States (US) will change with the projected rise in extreme heat is unknown.
Methods:
We obtained data on cardiovascular deaths among adults and the number of extreme heat days (maximum heat index ≥90°F (32.2°C)) in each county in the contiguous US from 2008 to 2019. Based on Representative Concentration Pathway trajectories that model greenhouse gas emissions and Shared Socioeconomic Pathways (SSP) that model future socioeconomic scenarios and demographic projections, we obtained county-level projected number of extreme heat days and populations under two scenarios – SSP2–4.5 (representing demographic projections from a “middle of the road” socioeconomic scenario and an intermediate increase in emissions) and SSP5–8.5 (demographic projections in a “fossil-fueled development” based economy and a large increase in emissions) – for the mid-century period (2036–2065). The association of cardiovascular mortality with extreme heat was estimated with a Poisson fixed effects model. Using estimates from this model, the projected number of excess cardiovascular deaths associated with extreme heat were calculated.
Results:
Extreme heat was associated with 1651 (95% CI 921 to 2381) excess cardiovascular deaths per year in 2008–2019. By mid-century, extreme heat is projected to be associated with 4320 (95% CI 2369 to 6272) (162% (95% CI 142 to 182) increase) and 5491 (95% CI 3011 to 7972) (233% (95% CI 206 to 259) increase) excess deaths annually under SSP2–4.5 and SSP5–8.5 respectively. Elderly adults are projected to have a 3.5 (95% CI 3.2 to 3.8) times greater increase in deaths in the SSP2–4.5 scenario compared to non-elderly adults. Non-Hispanic Black adults are projected to have a 4.6 (95% CI 2.8 to 6.4) times greater increase compared to non-Hispanic White adults. The projected change in deaths was not statistically significantly different for other race and ethnicity groups or between men and women.
Conclusions:
By mid-century, extreme heat is projected to be associated with a significantly greater burden of excess cardiovascular deaths in the contiguous US.
Keywords: Climate Change, Extreme Heat, Population Health, Health Status Disparities
Introduction:
Global climate change due to greenhouse gas emissions has produced an increase in extreme weather events compared to pre-industrial levels. The frequency and intensity of extreme heat events in the United States (US) are projected to continue to increase over the next several decades.1, 2 Due in part to the central role of the cardiovascular system in thermoregulation, individuals with cardiovascular disease and risk factors are at high risk of adverse health effects related to extreme heat.3 How the burden of cardiovascular deaths related to extreme heat might be affected by the projected increase in extreme heat, along with simultaneous changes in population demographics, is unclear.
Previous studies have demonstrated that extreme heat is associated with cardiovascular mortality.4, 5 One recent analysis estimated that extreme heat may be responsible for 0.2% of all cardiovascular deaths.6 Under most plausible greenhouse gas emissions scenarios, global mean temperatures are projected to continue increase, at least until the middle of the century.7 This continued increase is projected to also increase the number of extreme heat events. These changes will occur along with several demographic changes in the US such as the increase in migration of the US population to areas which typically experience higher temperatures, a projected increase in the proportion of the US population who are elderly, as well as an increasing share of the population composed of individuals other than non-Hispanic Whites.8–10 Older individuals are at a higher risk of adverse health events related to extreme heat, related in part to a higher burden of comorbidities.11 Additionally, in the US, extreme heat is associated with a significantly greater increase in cardiovascular mortality among non-Hispanic Black compared to non-Hispanic White adults.12 Analyzing how these demographic and environmental trends interact is necessary for accurate forecasts of how extreme heat events will impact the cardiovascular health of US adults in the coming decades.
The Representative Concentration Pathways (RCP) and the Shared Socioeconomic Pathways (SSP) are potential trajectories of changes in atmospheric greenhouse gas concentrations and socioeconomic conditions that have been used in climate change modeling.13 A combination of RCP and SSP can thus provide a range of potential scenarios incorporating economic, demographic, social, and environmental changes that may occur globally through the rest of the century. To evaluate how such changes may impact extreme temperature associated cardiovascular mortality in the contiguous US, we compared the estimated number of excess cardiovascular deaths among adults in the contiguous US from 2008 to 2019 with the projected number of deaths in the mid-century period (2036–2065) based on two SSP-RCP scenarios: SSP2–4.5 which represents a plausible scenario based on economic and environmental policies that are currently being enacted to tackle greenhouse gas emissions leading to an intermediate increase in emissions and SSP5–8.5 which tracks with emissions in the previous two decades and assumes minimal emissions reduction efforts in the future, leading to a large increase in emissions.14, 15
Methods
All data used are publicly available from sources listed in this manuscript and are aggregated at the US county level. This analysis was considered exempt from review based on guidelines from the University of Pennsylvania Institutional Review Board guidelines, and informed consent was waived.
Extreme Heat
Extreme heat, which refers to temperatures significantly higher than usual for a particular area, was the primary exposure of interest. Although there is no universal definition of extreme heat, in this analysis we defined any day where the maximum heat index (HI) was ≥90 °F (32.2 °C), which is the definition used for the projections of the mean annual number of extreme heat days in each US county by mid-century obtained from data made available by the Union of Concerned Scientists.16 Heat index combines air temperature and relative humidity to provide a measure of the temperature perceived by the human body.17 A threshold of ≥90 °F was used for the primary analysis as this has been used by government agencies in the US when describing extreme heat to the general public and in previous analyses a higher burden of heat associated mortality was also noted when using lower thresholds.4, 18, 19 However, we also use alternative definitions in sensitivity analyses as noted below. The methodology used to obtained the projection is provided in detail by Dahl et al.20 Briefly, daily temperature and relative humidity from 18 Global Climate Models included in the Coupled Model Intercomparison Project Phase 5 were statistically downscaled using the Multivariate Adaptive Constructed Analogs method to cover the contiguous US to a spatial resolution of 4 kilometers.21 Modeled data from a historical period (1950–2005) was trained to a spatially and temporally granular observed meteorological dataset (gridMet). The downscaled models were then used to project the mean annual number of days in each US county with a HI above different threshold levels for different 30-year periods, including the mid-century (2036–2065) period were calculated for intermediate (RCP 4.5) and large increases (RCP 8.5) in greenhouse gas concentration trajectories. Extreme heat projections for the mid-century 30-year period were used in the Union of Concerned Scientists dataset. Additional details on RCP trajectories and this methodology are provided in Supplemental Methods S1 and S2. In addition to the number of days with HI ≥90 °F, we tested different definitions for extreme heat – HI ≥100 °F (37.8 °C) and HI ≥105 °F (40.6 °C) in secondary analyses.
Population projections
We obtained county-level, age, sex, race, and ethnicity specific population projections that account for different SSP scenarios for the mid-century period based on an analysis by Hauer.22. SSPs describe possible, and plausible, trajectories of future socioeconomic developments in the coming decades.23 Different SSP scenarios, or narratives, envision different levels of acceptance or barriers to mitigation and adaptations to climate change. These scenarios have then been used to model demographic and economic changes that could occur in human societies. For this analysis we used projections based on the SSP2 and SSP5 scenarios. SSP2 is labeled a “middle of the road” scenario and envisions a medium level of challenges to mitigation and adaptation. SSP5 describes a global economy based on “fossil-fueled development” with a high degree of barriers to mitigation but low challenges to adaptation due to the availability of economic resources. Using the National Vital Statistics System US Census Populations with Bridged Race Categories data set, Hauer first used a baseline period of 1969 to 2000 to project county-level, sub-group specific population for the projection period 2000–2015. After validating this projection with the actual county-level populations from the 2000 to 2015 period, annual, county-level, sub-group specific populations were projected for the years 2020 to 2100. These projections were then adjusted for the five SSP scenarios, using previously produced total population projections for the US under the different scenarios.24 Additional details regarding SSP scenarios and the methodology used for the projected populations are available in Supplemental Methods S1 and S3. For this analysis, we used the sub-group specific, county-level, mean annual projected population for the years 2036 to 2065.
We combined the demographic projections based on the SSPs with the number of extreme heat days based on the RCP trajectories for each county based on two combinations that were used for the Sixth Assessment Report of the Intergovernmental Panel on Climate Change: SSP2–4.5 and SSP5–8.5.7 SSP2–4.5 can be considered a plausible scenario for the state of greenhouse gas emissions if some of the ongoing and planned emissions mitigation measures are put in place resulting in an intermediate increase. SSP5–8.5 is a scenario based on continued heavy use of fossil-fuels and a subsequent large increase in emissions.
Mortality Rates
To estimate the association between the number of extreme heat days, and monthly cardiovascular rates in the current period (2008–2019), we calculated county-level, age-adjusted (standardized to the 2000 US census) monthly cardiovascular mortality rates for all adult residents (20 years of age and older) for summer months (May to September) from 2008 to 2019 using data from the National Center for Health Statistics (NCHS). Cardiovascular mortality was defined as a death with the primary cause as any disease of the circulatory system (International Statistical Classification of Diseases and Related Health Problems, 10th Revision codes I00–I99).
Death certificate data was used to identify the age, sex, race, and ethnicity of each deceased individual. Data regarding race and ethnicity in death certificates in the US has been shown to have excellent agreement with self-reported Black and White race and Hispanic ethnicity.25 As small area mortality rates can be statistically unstable, we used spatial empirical Bayes smoothed mortality rates (Supplemental Methods S4).26
Outcomes
The primary outcome of interest is the mean, annual, estimated excess cardiovascular mortality rate in the contiguous US in the mid-century period in the SSP2–4.5 and SSP5–8.5 scenarios. Secondary outcomes include excess cardiovascular mortality rates among subgroups of age, sex, race, and ethnicity.
Data sources and missing data
Additional data sources not stated above and data missingness are listed in Supplemental Methods S5.
Statistical Analysis
We first calculated the proportion of total cardiovascular deaths during summer months (May to September) from 2008 to 2019 among different sub-groups of gender, race, and ethnicity. We then calculated summary measures of county-level demographic, clinical, and health care–related variables in the current period. We also calculated the median number of extreme heat days in the current period and mid-century projections for RCP 4.5 and RCP 8.5 trajectories and the median county population of the different sub-groups of interest in the current period, and the projected population under the SSP2 and SSP5 scenarios.
We then estimated the association between the number of extreme heat days per month and monthly cardiovascular mortality rate in the current period (2008–2019) using a Poisson fixed-effects regression model. The model includes year and month fixed effects as well as additional time varying environmental (e.g. precipitation, days with elevated fine particulate matter), economic (e.g., unemployment and poverty rates), land development (proportion of land with forest cover, proportion developed), demographic (e.g., proportion of county residents other than non-Hispanic White), healthcare related variables (e.g., number of primary care providers) as listed in the in Supplemental Methods S6. As diabetes may be associated with impaired thermoregulation and is also an important cardiovascular risk factor, the proportion of county residents with diabetes was also included as a covariate.27 Additional details about the fixed effects model are provided in Supplemental Methods S6. We compared alternative specifications of covariates in the primary model using the Bayesian Information Criterion. Additional goodness of fit statistics were also calculated. As previous studies have shown that the association between extreme heat and health outcomes differs by age, we estimated fixed effects models for non-elderly (20 to 64 year old) and elderly (65 years of age and older) adults separately in a simultaneous estimation framework that allowed us to combine the estimates for each age sub-group and then estimate the number of excess deaths associated with extreme heat across all counties in the contiguous US.28 The estimated excess number of deaths associated with extreme heat in the current period was the difference in the predicted number of cardiovascular deaths based on the observed value of the model covariates, including number of extreme heat days, in each county and the predicted number if there were no extreme heat days, but other covariates were unchanged.
Using the regression coefficients from the Poisson model described above, the estimated number of excess deaths in the mid-century period (2036–2065) associated with extreme heat were then calculated as the difference in the predicted number of cardiovascular deaths based on the projected number of extreme heat days (based on RCP 4.5 and RCP 8.5) in each county and the predicted number of deaths without any extreme heat day occurring. The projected population (based on SSP2 and SSP5) (for elderly and non-elderly adults separately) for each county was also used to calculate the total number of estimated deaths in each county. We then calculated the percent change in annual excess mortality compared to the current period under the different population and emissions scenarios for each county. To understand how changes in extreme heat days, along with demographic changes, impact change in the number of deaths associated with extreme heat, we also calculated summary measures for the percent change in the number of extreme heat days, adult population, and proportion of the population 65 years of age and older by quartiles of US counties based on the percent change in the estimated number of excess of deaths associated with extreme heat.
In secondary analyses we estimated the number of excess deaths in different subgroups – men, women, non-Hispanic Black, non-Hispanic White, non-Hispanic other races, Hispanic (any race), elderly, non-elderly adults, metropolitan counties, and non-metropolitan counties. As with the primary model, we estimated the number of deaths for the current and mid-century period as well as the precent change between the two time periods. We also compared the percent change for the different sub-groups with each other by calculating the ratio of the change (i.e., the percent change of a sub-group divided by the percent change of the reference group). We also estimated the primary model using different extreme heat thresholds and using an alternative definition of cardiovascular disease (Supplemental Table S1).
Results are presented as means with SD or 95% CI or median with interquartile range (IQR). All p-values were 2 sided, and values ≤0.05 were considered statistically significant. Empirical Bayes smoothing was performed with Geoda. Other statistical analyses were conducted with Stata 18 (StataCorp, College Station, TX). The Stata module ppmlhdfe was used to fit the Poisson fixed-effects models.29
Results
All 3,108 counties in the contiguous United States were included in the analysis. From 2008 to 2019, there were a total of 3,818,017 deaths attributed to cardiovascular disease in these counties among adults in summer months. Of these deaths, 49.6% were among women, 12.3% among non-Hispanic Black adults, 84.9% among non-Hispanic White adults, 2.5% among non-Hispanic adults of other races, 5.8% among Hispanic adults of any race, and 0.3% among adults with unknown race or ethnicity. The median Bayesian smoothed monthly cardiovascular mortality rate over the study period was 26.1 (IQR 22.2 to 30.7) deaths per 100,000 adults. Other environmental, economic, and healthcare related summary measures for the 2008 to 2019 period included in the fixed effects model are listed in Table 1. The county median annual number of days with maximum HI ≥90 °F in summer months in 2008–2019 was 54 (IQR 23 to 93) (Table 2).
Table 1 –
County economic, environmental, and demographic characteristics - 2008–2019*
| Median (interquartile range) | |
|---|---|
| Monthly values | |
| Mean monthly precipitation (inches) | 2.8 (1.5, 4.3) |
| Percentage of county population living in areas affected by drought† | 0 (0, 7.0) |
| Number of days with ozone concentration above Environmental Protection Agency standard ‡ | 0 (0, 0) |
| Number of days with fine particulate matter (PM2.5) concentration above Environmental Protection Agency standard § | 0 (0, 0) |
| Number of days with Federal Emergency Management Agency disaster declaration | 0 (0, 0) |
| Unemployment rate (percentage) | 5.7 (4, 8.1) |
| Annual values | |
| Percentage of land area with forest cover | 26.2 (6.0, 52.2) |
| Percentage of land area developed ǁ | 6.0 (4.0, 9.2) |
| Number of primary care providers per 100,000 adult residents | 64.6 (39.6, 94.3) |
| Number of hospital beds per 100,000 adult residents | 270.7 (105.5, 513.7) |
| Percentage of adult residents with diabetes | 8.0 (7.2, 9.3) |
| Percentage of 18 to 64 year old residents without health insurance | 17.3 (12.2, 23.0) |
| Percentage of residents living in poverty | 15.2 (11.6, 19.6) |
| Median household income (US dollars) # | 41556 (35918, 48304) |
| Percentage of adult residents other than non-Hispanic White | 12.7 (5.4, 30.2) |
| Percentage of residents 65 years of age and older | 22.9 (20.0, 26.4) |
All values represent the mean value for the 2008 to 2019 period
Moderate drought or more based on the data from the US Drought Monitor
Based on Environmental Protection Agency National Ambient Air Quality Standard thresholds of 35 μg/m3
Based on Environmental Protection Agency National Ambient Air Quality Standard thresholds of 0.07 ppm
Low, medium, or high intensity development
Inflation adjusted to 2008 dollars
Table 2:
Current (2008–2019) and projected mid-century (2036–2065) number of extreme heat days and population in counties in the contiguous United States
| Number of days per year with daily maximum heat index: | Current* Median (interquartile range) |
RCP 4.5 Trajectory† Median (interquartile range) |
RCP 8.5 Trajectory† Median (interquartile range) |
|---|---|---|---|
| ≥90 °F (32.2 °C) | 54 (23, 93) | 71 (38, 104) | 80 (47, 112) |
| ≥100 °F (37.8 °C) | 12 (2, 32) | 24 (8, 49) | 35 (14, 63) |
| ≥105 °F (40.6 °C) | 3 (0, 11) | 10 (2, 25) | 18 (5, 38) |
| Population: | Current‡ | SSP2 Scenario§ | SSP5 Scenario§ |
| All adults (20 years and older) | 19524 (8337, 50287) | 18252 (7324, 54304) | 20747 (8351, 62266) |
| Non-elderly adults (20 to 64 years old) | 14999 (6220, 39233) | 12791 (5183, 38128) | 14509 (5877, 43317) |
| Elderly adults (65 years and older) | 4404 (2033, 11083) | 5514 (2126, 16440\) | 6267 (2409, 18951) |
| Women | 9749 (4153, 25744) | 8988 (3597, 27413) | 10189 (4058, 31195) |
| Men | 9615 (4191, 24611) | 9366 (3830, 27426) | 10703 (4342, 31393) |
| Hispanic adults (any race) | 602 (189, 2751) | 1896 (762, 7967) | 2430 (992, 10162) |
| Non-Hispanic Black adults | 562 (63, 3972) | 1225 (360, 5191) | 1505 (453, 6287) |
| Non-Hispanic White adults | 15748 (6473, 41802) | 11756 (4290, 35246) | 13671 (5003, 42414) |
| Non-Hispanic adults of other race ǁ | 413 (153, 1643) | 676 (243, 2644) | 846 (304, 3351) |
| Adults living in metropolitan counties # | 71449 (23651, 163867) | 82109 (24078, 229104) | 93589 (27371, 262199) |
| Adults living in non-metropolitan counties # | 12554 (6012, 24428) | 11158 (5089, 23081) | 12601 (5768, 26288) |
Based on the mean annual number of extreme heat days in each county during summer months (May to September)
RCP - Representative Concentration Pathway. RCP 4.5 refers to radiative forcing value in the year 2100 of 4.5 W/m2 and represents an intermediate increase of greenhouse gas emissions trajectory. RCP 8.5 refers to radiative forcing value in the year 2100 of 8.5 W/m2 and represents a large increase of greenhouse gas emissions trajectory.
Mean annual population from 2008 to 2019
SSP - Shared Socioeconomic Pathways. SSP2 is a “Middle of the road” scenario and SSP5 is a “Fossil-Fueled Development” scenario for socio-economic changes. Projected population reflects mean annual values from 2036 to 2065
Adults of non-White, non-White race, and non-Hispanic ethnicity
County metropolitan status based on the 2013 National Center for Health Statistics Urban-Rural Classification Scheme
The median annual number of extreme heat days is projected to increase to 71 (IQR 38 to 104) and 80 (IQR 47 to 112) under the RCP 4.5 and RCP 8.5 trajectories respectively (Table 2). The mean total number of adults living in the contiguous US is projected to change from 233,008,985 in the 2008–2019 period to 309,413,281 and 354,597,998 in the mid-century period under the SSP2 and SSP5 scenarios respectively. The median adult population across counties in the contiguous US is projected to change from 19,524 (IQR 8,337 to 50,287) in the current period to 18,252 (IQR 7,324 to 54,304) and 20,747 (IQR 8,351 to 62,266) under the SSP2 and SSP5 scenarios respectively (Table 2). The median projected percent change in the adult population between the current and mid-century periods is −4.6% (IQR −19.1% to 18.4%) and 8.5% (IQR −8.3% to 35.8%) under the SSP2 and SSP5 scenarios respectively. The median proportion of county residents who are 65 years and older is projected to increase from 23.0% (IQR 19.9% to 26.1%) in the current period to 30.6% (IQR 27.0% to 33.8%) and 30.7% (IQR 27.1% to 34.1%) under the SSP2 and SSP5 scenarios respectively. Projected populations for different sub-groups and for metropolitan and non-metropolitan counties are listed in Table 2.
Between 2008 and 2019, there were a total of 12,243,859 (mean: 1,020,322 (SD=59,221) per year) cardiovascular deaths among adults living in the contiguous US during summer months. In the Poisson fixed effect model, in the current period, 1 additional extreme heat day was associated with a 0.05% (95% CI 0.02% to 0.07%) increase in cardiovascular mortality among elderly adults and 0.05% (95% CI 0.01% to 0.09%) increase among non-elderly adults. Goodness of fit statistics for the model and alternative specification of covariates are listed in Supplemental Table S2. The mean annual estimated excess cardiovascular deaths associated with extreme heat in 2008–2019 were 1,651.4 (95% CI 921.4 to 2,381.3) (Table 3, Figure). In the SSP2–4.5 scenario, the mean annual estimated excess cardiovascular deaths associated with extreme heat in the mid-century periods is 4,320.2 (95% CI 2,368.5 to 6,272.0) representing a 161.6% (95% CI 141.5% to 181.7%) increase from the current period. In the SSP5–8.5 scenario, the mean number of estimated deaths is 5,491.3 (95% CI 3,010.6 to 7972.0) representing a 232.5% (95% CI 206.3% to 258.8%) increase.
Table 3:
Estimated excess cardiovascular deaths associated with extreme heat days in the current (2008–2019) and mid-century (2036–2065) periods in the contiguous United States*†
| Current | SSP2–4.5‡ | SSP5–8.5‡ | |||
|---|---|---|---|---|---|
| Population | Estimated excess deaths number of deaths, (95% CI) | Estimated excess deaths number of deaths, (95% CI) | Percent change compared to current period %, (95% CI) | Estimated excess deaths number of deaths, (95% CI) | Percent change compared to current period %, (95% CI) |
| All adults (20 years and older) | 1651.4 (921.4, 2381.3) | 4320.2 (2368.5, 6272.0) | 161.6 (141.5, 181.7) | 5491.3 (3010.6, 7972.0) | 232.5 (206.3, 258.8) |
| Elderly adults (65 years and older) | 1339.5 (684.8, 1994.3) | 3842.2 (1972.8, 5711.7) | 186.8 (178.2, 195.5) | 4894.2 (2515.3, 7273.1) | 265.4 (253.7, 277.0) |
| Non-elderly adults (20 to 64 years old) | 311.8 (51.3, 572.3) | 478.0 (74.7, 881.3) | 53.3 (49.1, 57.5) | 597.1 (92.8, 1101.5) | 91.5 (85.7, 97.3) |
| Women | 649.2 (235.4, 1063.0) | 1887.66 (774.4, 3001.0) | 190.8 (158.5, 223.0) | 2390.5 (983.3, 3797.7) | 268.2 (226.5, 309.9) |
| Men | 1117.4 (619.7, 1615.2) | 2900.9 (1595.4, 4206.5) | 159.6 (135.5, 183.7) | 3711.8 (2040.4, 5383.3) | 232.2 (200.3, 264.0) |
| Hispanic adults (any race) | 36.2 (−163.8, 236.2) | 604.8 (−1082.2, 2291.9) | 1570.6 (−3446.4, 6587.6) | 830.6 (−1480.6, 3141.9) | 2194.3 (−4711.9, 9100.5) |
| Non-Hispanic Black adults | 325.3 (−25.1, 675.6) | 1511.8 (40.2, 2983.3) | 364.8 (230.0, 499.5) | 2062.6 (56.2, 4069.1) | 534.1 (348.3, 719.9) |
| Non-Hispanic White adults | 1004.7 (449.3, 1560.0) | 1806.3 (713.0, 2899.6) | 79.8(63.1, 96.5) | 2428.8 (956.4, 3901.2) | 141.8 (118.9, 164.6) |
| Non-Hispanic adults of other race § | 6.4 (−63.7, 76.5) | 241.1 (−336.1, 818.3) | 3646.0 (−28912.7, 36204.7) | 348.0 (−479.6, 1175.5) | 5307.3 (−41789.2, 52403.9) |
| Adults living in metropolitan counties ǁ | 1267.2 (564.9, 1969.4) | 3620.9 (1531.5, 5710.3) | 185.7 (158.0, 213.5) | 4602.2 (1945.8, 7258.5) | 263.2 (227.2, 299.2) |
| Adults living in non-metropolitan counties ǁ | 425.9 (241.0, 610.9) | 627.2 (353.9, 900.6) | 47.3 (40.4, 54.1) | 796.6 (449.2, 1144.0) | 87.0 (77.9, 96.2) |
Extreme heat defined as maximum daily heat index ≥90 °F (32.2 °C)
Estimated excess deaths based on Poisson fixed effects model with monthly and annual covariates from the 2008–2019 period (Supplemental Methods S6). Excess deaths were then estimated by calculating the difference between the number of predicted deaths in each county with all covariates at their observed value and the number of predicted deaths if there were no extreme heat days. For the projected number of excess deaths in the mid-century period, the number of extreme heat days and county population were replaced with projected values when calculating the difference while keeping the regression coefficients the same.
SSP - Shared Socioeconomic Pathways. SSP2–4.5 refers to a “Middle of the road” scenario for socio-economic changes and an intermediate increase in greenhouse gas emissions trajectory. SSP5–8.5 refers to a “Fossil-Fueled Development” scenario for socio-economic changes and a large increase in greenhouse gas emissions trajectory.
Adults of non-White, non-White race, and non-Hispanic ethnicity
County metropolitan status based on the 2013 National Center for Health Statistics Urban-Rural Classification Scheme
Figure – Estimated number of excess cardiovascular deaths associated with extreme heat per 1 million adult residents in the current (2008–2019) and mid-century (2036–2065) periods in the contiguous United States*†‡.
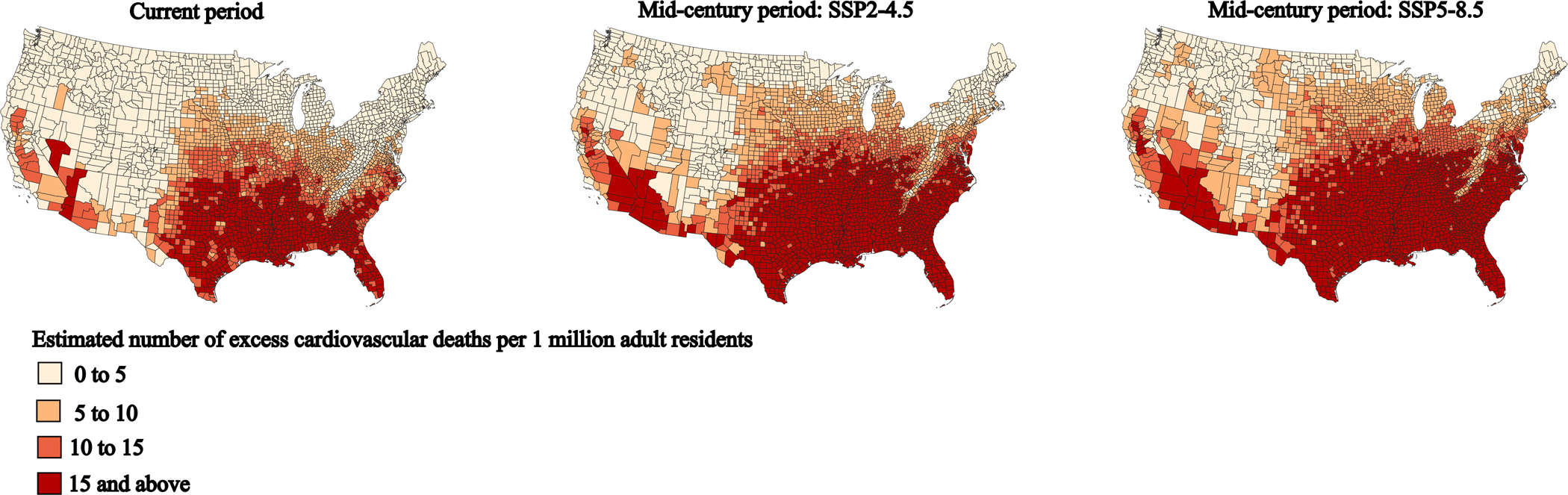
* Extreme heat defined as maximum daily heat index ≥90 °F (32.2 °C)
† Estimated excess deaths based on Poisson fixed effects model with monthly and annual covariates from the 2008–2019 period (Supplemental Methods S6). Excess deaths were then estimated by calculating the difference between the number of predicted deaths in each county with all covariates at their observed value and the number of predicted deaths if there were no extreme heat days. For the projected number of excess deaths in the mid-century period, the number of extreme heat days and county population were replaced with projected values when calculating the difference while keeping the regression coefficients the same.
‡ SSP - Shared Socioeconomic Pathways. SSP2–4.5 refers to a “Middle of the road” scenario for socio-economic changes and an intermediate increase in greenhouse gas emissions trajectory. SSP5–8.5 refers to a “Fossil-Fueled Development” scenario for socioeconomic changes and a large increase in greenhouse gas emissions trajectory.
The median projected percent change in extreme heat associated cardiovascular deaths across counties was 64.1% (IQR 17.9% to 155.5%) and 116.8% (IQR 48.1% to 255.4%) under the under the SSP2–4.5 and SSP5–8.5 scenarios respectively. For the SSP2–4.5 scenario, among counties in the quartile with the lowest percent change in the number of deaths, there was a mean −0.5% (95% CI −3.1% to −2.2%) change in the number of extreme heat associated deaths, a median change of 445.8% (IQR 279.2% to 476.0%) in the annual number of extreme heat days, and a −10.2% change in the adult population between the current and mid-century periods. In the second quartile, there was a 41.6% (95% CI 35.0% to 48.2%) increase in the number of excess deaths, a 478.8% (IQR 429.7% to 544.6%) increase in the number of extreme heat days, and a 1.0% change in the adult population. In the third quartile, there was a 110.7% (95% CI 97.8% to 123.6%) increase in deaths, a 562.8% (IQR 464.4% to 672.9%) increase in the number of extreme heat days, and a 14.8% increase in the adult population. Among counties in the highest quartile for percent change in the number of deaths, there was a 271.0% (95% CI 238.7% to 303.2%) increase in deaths associated with extreme heat, a 604.7% (IQR 482.4% to 845.7%) increase in the number of extreme heat days, and a 52.5% increase in the adult population. The change in the number of extreme heat associated deaths, extreme heat days, and adult population in the SSP5–8.5 scenario are listed in table 3.
Using alternative definitions of extreme heat, in 2008–2019, the mean number of annual estimated excess cardiovascular deaths associated with extreme heat were 1043.2 (95% CI 761.6 to 1,324.9) and 461.7 (95% CI 297.9 to 625.6) for maximum daily HI ≥100 °F (37.8 °C) and ≥105 °F (40.6 °C) respectively (Supplemental Table S3). For maximum daily HI ≥100 °F, the mean annual estimated excess cardiovascular deaths associated with extreme heat in the mid-century period is 3,915.5 (95% CI 2,903.5 to 4,927.5) in the SSP2–4.5 scenario (275.3% (95% CI 252.4% to 298.2%) increase) and 5,771.5 (95% CI 4,284.0 to 7,259.1) in the SSP5–8.5 scenario (453.2% (95% CI 418.4% to 488.1%) increase). For maximum daily HI ≥105 °F, the mean annual estimated excess cardiovascular deaths associated with extreme heat in the mid-century period is 2,420.0 (95% CI 1,601.8 to 3,238.2) in the SSP2–4.5 scenario (424.1% (95% CI 388.1% to 460.0%) increase) and 4,169.4 (95% CI 2,759.3 to 5,579.5) in the SSP5–8.5 scenario (803.0% (95% CI 738.5% to 867.4%) increase).
In secondary analyses, the projected percentage change in estimated excess deaths associated with extreme heat for elderly adults was 186.8% (95% CI 178.2% to 195.5%) and 265.4% (95% CI 253.7% to 277.0%) and for non-elderly adults was 53.3% (95% CI 49.1% to 57.5%) and 91.5% (95% CI 85.7% to 97.3%) under the SSP2–4.5 and SSP5–8.5 scenarios respectively. The percentage change in estimated excess deaths was 3.5 (95% CI 3.2 to 3.8) and 2.9 (95% CI 2.7 to 3.1) times higher among elderly adults compared to non-elderly adults under the SSP2–4.5 and SSP5–8.5 scenarios respectively. The percentage change in excess deaths was similar for men and women. Among non-Hispanic Black adults, the percentage change in excess deaths was 364.8% (95% CI 230.0% to 499.5%) and 534.1% (95% CI 348.3% to 719.9%) and among non-Hispanic White adults it was 79.8% (95% CI 63.1% to 96.5%) and 141.8% (95% CI 118.9% to 164.6%) under the SSP2–4.5 and SSP5–8.5 scenarios respectively. The percent change was 4.6 (95% CI 2.8 to 6.4) and 3.8 (95% CI 2.4 to 5.1) times higher among non-Hispanic Black adults compared to non-Hispanic White adults under the SSP2–4.5 and SSP5–8.5 scenarios respectively. Although the mean estimated number of excess deaths increased for both non-Hispanic adults of other races and Hispanic adults, the change was not statistically significantly different from zero. The percent change in excess deaths increased to a greater degree in metropolitan compared to non-metropolitan counties (3.9 (95% CI 3.1 to 4.7) and 3.0 (95% CI 2.5 to 3.5) under the SSP2–4.5 and SSP5–8.5 scenarios respectively). When using an alternative, narrower, definition of cardiovascular mortality, the overall results of the analysis were similar (Supplemental Table S4).
Discussion:
The projected number of excess cardiovascular deaths across the contiguous US due to extreme heat is estimated to increase 161.6% (95% CI 141.5% to 181.7%) under an intermediate increase in greenhouse gas emissions scenario (resulting from current emissions reduction policies that are likely to be implemented) and 232.5% (95% CI 206.3% to 258.8%) under a large increase in emissions scenario (following emissions trends based on the previous two decades with minimal emissions reduction efforts). In secondary analyses, there was a significantly greater increase in estimated excess deaths among older compared to younger adults, among non-Hispanic Black compared to non-Hispanic White adults, and in metropolitan vs. non-metropolitan counties.
Extreme heat can affect cardiovascular health through several possible biological mechanisms. As the cardiovascular system plays a key role in thermoregulation, in response to prolonged heat exposure, there can be an increase in cardiac strain resulting from higher heart rate and contractility.30 Additionally, heat can increase cytokine release and thrombosis leading to an increased risk of myocardial infarction and stroke.31 Medications commonly used by patients with cardiovascular conditions, including beta-blockers and diuretics, also alter thermoregulation and may make individuals more vulnerable to the adverse health effects of heat exposure.32, 33 Previous studies have therefore noted an increase in cardiovascular morbidity and mortality associated with extreme temperatures.4, 11, 34 Heat exposure has also been associated with deaths from ischemic heart disease, stroke, and heart failure specifically.6
Given the vulnerability of individuals with cardiovascular disease and risk factors to heat exposure, it is crucial to understand how environmental changes due to climate change, coupled with socioeconomic and demographic changes, will affect the future burden of cardiovascular mortality. For the purposes of this analysis, we adopted a modeling framework used in previous Intergovernmental Panel on Climate Change reports. This framework provides a range of potential scenarios for how societies may develop as well as the trajectory of emissions increases. Under both a scenario representing a plausible trajectory of greenhouse gas emissions increase based on emissions reduction policies that are likely to be implemented (SSP2–4.5) and a scenario representing a worst-case scenario where emissions trends are similar to those observed in the previous two decades (SSP5–8.5), the number of estimated excess deaths associated with extreme heat in the contiguous US will increase dramatically. This is in part related to the increase in extreme heat days, which are projected to increase 30% to 50%, based on a threshold of HI ≥90 °F. Additionally, demographic changes such as the aging of the population, continued migration of Americans to warmer areas, and a more racially and ethnically diverse population in the US is likely to impact the overall burden of extreme heat related mortality.8 While the number of excess deaths is projected to increase under both scenarios, the magnitude of the increase is on average lower in the lower emissions increase trajectory. This suggests that more aggressive policies aimed at reducing greenhouse gas emissions may pay health dividends. With the growing realization of the health impacts of extreme heat, investigation of potential thermoprotective agents may be needed. One recent study suggest that statins may be one potential class of medications with such an effect.35
Previous studies have demonstrated that burden of extreme heat is experienced disproportionately by different populations, including older adults, as well as non-Hispanic Black adults in the US.4, 12 This may be due to the higher burden of cardiovascular disease and risk factors. However, other factors include the lower access to air conditioning and a greater degree of the urban health island effect in neighborhoods with a higher proportion of residents other than non-Hispanic White.36, 37 Lack of infrastructure investment in communities and neighborhoods that have historically faced discrimination places the individuals living there at some of the highest risk for the growing health impacts of climate change. This analysis therefore suggests that by identifying such high-risk communities, potential targeting of mitigation strategies at these communities may have a potentially large public health impact. Such strategies may include increasing tree canopy cover, use of novel surfaces that may lower the urban heat island effect, and heat action plans that accommodate the needs of different communities.38–40
As with any projection, there is uncertainty regarding how the association between extreme heat and cardiovascular mortality may change over the coming decades. Our analysis assumes that the association between extreme heat and cardiovascular mortality in the mid-century period is the same as in the current period. There is some evidence that the association between temperature and mortality has attenuated over time, possibly due to greater adaptation such as more widespread use of air conditioning.41 Additionally, advances in therapies for cardiovascular disease and risk factors will affect mortality rates. Conversely, although our model accounts for population-level prevalence of diabetes, the prevalence of diabetes and obesity is increasing, and individuals may become increasingly vulnerable to the health effects of extreme temperatures.42
This study has some limitations. Due to the observational nature of the study, causality cannot be assumed. As a county-level ecological analysis, inferences at the individual level cannot be made. The fixed-effects model used to estimate the association between heat and cardiovascular mortality controlled for both measured and unmeasured time-invariant confounding, but residual time varying confounding may be possible. The primary model was estimated using monthly, rather than daily mortality rates, as the mortality data made available by the NCHS does not provide more temporally granular information. Therefore, it is not possible to specifically link a particular death to the occurrence of an extreme heat day in a given month. However, this approach allows for more statistically stable mortality estimates from areas with smaller populations. Additionally, due to privacy concerns, most localities in the US do not make detailed daily mortality data available. The county-level population and extreme heat projections for the mid-century periods are available only as point estimates, therefore, our approach does not account for uncertainty within these projections. However, we used different population and extreme heat projections to understand a potential range of the increase in estimated extreme heat days. We used an absolute, rather than relative or area-specific, threshold to define extreme heat. This was done as these thresholds were used to define extreme heat in the mid-century by the projections used for this analysis. It is possible that using an absolute, rather than a relative, threshold may underestimate the impact of extreme heat as in certain areas of the US where temperatures tend to be elevated (e.g., in South and Southwestern parts of the country), due to behavioral, cultural, and infrastructure differences, individuals and communities may be better adapted to high heat levels and elevated mortality may only be noted when temperatures (or heat index) rises above historic norms for that particular area. Our analysis is limited to extreme heat days during summer months only and is unable to account for deaths occurring outside of these months, as the source of our 2008–2019 data on extreme heat days – the Centers for Disease Control and Prevention’s Environmental Public Health Tracking Program – tracks extreme heat days only in summer months (May to September). As this analysis is limited to extreme heat, it does not account for potential changes in cardiovascular mortality associated with other changes that may occur due to climate change, including changes in extreme cold temperatures. Although the number of extreme cold days has declined on average in the past few decades, there is evidence that the frequency of extreme cold events in certain parts of the US may have risen due to climate change.43 Therefore, predicting how deaths due to extreme cold may change in the coming decades will require a greater understanding of how climate change will impact various extreme weather phenomena.
The estimated number of cardiovascular deaths associated with extreme heat in the contiguous US is projected to increase dramatically in the coming decades. Certain groups may experience a disproportionate increase in excess mortality including older adults, non-Hispanic Black adults, and people living in metropolitan areas. Clinical and community-based mitigation strategies, along with global efforts to confront climate change, are needed to address this growing public health issue.
Supplementary Material
Table 4:
Percent change in estimated deaths, extreme heat days, and population between current and mid-century periods by quartile of counties based on the percent change in extreme heat associated deaths*
| Quartile of US counties based on percent change in extreme heat associated estimated cardiovascular deaths between current and mid-century periods | Mean percent change in estimated cardiovascular deaths associated with extreme heat † (95% CI) |
Population-weighted median percent change in the number of extreme heat days ‡ (IQR) |
Percent change in total adult population § | Percent change in the proportion of adult population 65 years of age and older ǁ |
|---|---|---|---|---|
| SSP2–4.5 #** | ||||
| First quartile | −0.5% (−3.1%, −2.2%) | 445.8% (279.2%, 476.0%) | −10.2% | 20.4% |
| Second quartile | 41.6% (35.0%, 48.2%) | 478.8% (429.7%, 544.6%) | 1.0% | 32.9% |
| Third quartile | 110.7% (97.8% to 123.6%) | 562.8% (464.4%, 672.9%) | 14.8% | 44.6% |
| Fourth quartile | 271.0% (238.7%, 303.2%) | 604.7% (482.4%, 845.7%) | 52.5% | 67.3% |
| SSP5–8.5 #¶ | ||||
| First quartile | 24.0% (20.5%, 27.5%) | 489.3% (461.3%, 520.3%) | −2.9% | 19.0% |
| Second quartile | 83.1% (73.7%, 92.4%) | 521.5% (475.0%, 608.4%) | 13.8% | 34.5% |
| Third quartile | 188.3% (169.6%, 207.0%) | 634.7% (504.8%, 795.7%) | 38.1% | 47.3% |
| Fourth quartile | 395.6% (351.0%, 440.1%) | 736.8% (528.7%, 1188.6%) | 73.1% | 69.3% |
Excludes 116 out of 3108 counties in the contiguous US with no extreme heat days in 2008 to 2019
Estimated excess deaths based on Poisson fixed effects model with monthly and annual covariates from the 2008–2019 period (Supplemental Methods S6). Excess deaths were then estimated by calculating the difference between the number of predicted deaths in each county with all covariates at their observed value and the number of predicted deaths if there were no extreme heat days. Percent change in the estimated excess calculated is the percent change in estimated excess deaths in the current period and the mid-century period with values representing the mean percent change across all counties in the quartile.
Percent change in the annual number of extreme heat days (defined as maximum daily heat index ≥90 °F (32.2 °C). Values represent the median percent change between the current and mid-century periods for each quartile of counties weighted by the projected mid-century adult population
Percent change in the total number of adults (20 years of age and older) between the current and mid-century periods residing in each quartile of counties
Percent change in the proportion of all adults who are 65 years and older between the current and mid-century periods in each quartile of counties
SSP - Shared Socioeconomic Pathways. SSP2–4.5 refers to a “Middle of the road” scenario for socio-economic changes and an intermediate increase in greenhouse gas emissions trajectory. SSP5–8.5 refers to a “Fossil-Fueled Development” scenario for socio-economic changes and a large increase in greenhouse gas emissions trajectory
Percent change in estimated excess deaths between current and mid-century periods under the SSP2–4.5 scenario – First quartile: −57.1% to 17.9%, second quartile: 17.9% to 64.1%, third quartile: 64.1% to 155.4%, fourth quartile: 155.5% to 80,848.3%
Percent change in estimated excess deaths between current and mid-century periods under the SSP4–8.5 scenario – First quartile: −47.9% to 48.0%, second quartile: 48.2% to 116.7%, third quartile: 117.0% to 255.4%, fourth quartile: 244.4% to 121.090.9%
Table 5:
Ratio of the percent changes in projected estimated excess cardiovascular deaths associated with extreme heat compared to current period (2008–2019) between sub-groups of age, gender, race, and ethnicity*†
| SSP2–4.5‡ (95% CI) |
SSP5–8.5‡ (95% CI) |
|
|---|---|---|
| Elderly (65 years and older) compared to non-elderly (20 to 64 years old) adults | 3.5 (3.2, 3.8) | 2.9 (2.7, 3.1) |
| Women compared to men | 1.2 (0.9, 1.5) | 1.2 (0.9, 1.4) |
| Hispanic (any race) compared to non-Hispanic White adults | 19.7 (−43.2, 82.6) | 15.5 (−33.2, 64.2) |
| Non-Hispanic Black compared to non-Hispanic White adults | 4.6 (2.8, 6.4) | 3.8 (2.4, 5.1) |
| Non-Hispanic other race compared to non-Hispanic White adults § | 45.7 (−362.8, 454.2) | 37.5 (−295.1, 370.0) |
| Adults living in metropolitan compared to non-metropolitan counties ǁ | 3.9 (3.1, 4.7) | 3.0 (2.5, 3.5) |
Extreme heat defined as maximum daily heat index ≥90 °F (32.2 °C)
Percent change in estimated excess deaths is based on the difference between estimated excess cardiovascular deaths associated with extreme heat in the current period and the mid-century (2036–2065) period.
SSP - Shared Socioeconomic Pathways. SSP2–4.5 refers to a “Middle of the road” scenario for socio-economic changes and an intermediate increase in greenhouse gas emissions trajectory. SSP5–8.5 refers to a “Fossil-Fueled Development” scenario for socio-economic changes and a large increase in greenhouse gas emissions trajectory.
Other race refers to adults of non-White, non-White race, and non-Hispanic ethnicity
County metropolitan status based on the 2013 National Center for Health Statistics Urban-Rural Classification Scheme
Clinical Perspective.
What Is New?
The number of cardiovascular deaths associated with extreme heat among adults living in the contiguous United States is projected to have a statistically significant increase from the current period (2008–2019) to the mid-century period (2036–2065).
The mean number of extreme heat associated cardiovascular deaths per year is projected to increase 162% (95% CI 142% to 182%) in a scenario representing greenhouse gas emissions increase resulting from current climate policies or 233% (95% CI 206% to 259%) in a scenario representing large greenhouse gas emissions increases.
The projected increase in extreme heat associated cardiovascular deaths is estimated to be significantly greater among older adults compared to younger adults and among non-Hispanic Black adults compared to non-Hispanic white adults.
What Are the Clinical Implications?
Due to a combination of continued increase in extreme heat days, aging of the US population, and continued migration to warmer areas, the number of cardiovascular deaths associated with extreme heat are projected to continue to increase in the coming decades.
This increase has the potential to exacerbate pre-existing disparities in cardiovascular health between communities notably for non-Hispanic Black compared to non-Hispanic White adults.
Urgent public health and infrastructure interventions are needed to help communities adapt to the projected increases in extreme heat and to mitigate its adverse health effects.
Acknowledgements:
Funding/Support:
Sameed Ahmed M. Khatana receives grant funding from the National Heart, Lung, and Blood Institute (K23 HL153772) and the American Heart Association (20CDA35320251).
Non-standard Abbreviations and Acronyms:
- US
United States
- SSP
Shared Socioeconomic Pathways
- CI
Confidence Interval
- RCP
Representative Concentration Pathways
- HI
Heat Index
- NCHS
National Center for Health Statistics
- ICD
International Statistical Classification of Diseases and Related Health Problems
- IQR
Interquartile Range
- SD
Standard Deviation
Footnotes
Disclosures:
Sameed Ahmed M. Khatana has received personal fees from AcademyHealth
Ashwin S. Nathan has received institutional research funding from Abiomed and Biosense
Webster and has received speaker fees from Abiomed.
References
- 1.Meehl GA and Tebaldi C. More intense, more frequent, and longer lasting heat waves in the 21st century. Science. 2004;305:994–7. [DOI] [PubMed] [Google Scholar]
- 2.Vose R, Easterling D, Kunkel K, LeGrande A and Wehner M. Temperature changes in the United States. Climate Science Special Report: Fourth National Climate Assessment, Volume I US Global Change Research Program. Climate Science Special Report: Fourth National Climate Assessment, Volume I. 2017:185–206. [Google Scholar]
- 3.Ebi KL, Capon A, Berry P, Broderick C, de Dear R, Havenith G, Honda Y, Kovats RS, Ma W, Malik A, et al. Hot weather and heat extremes: health risks. Lancet. 2021;398:698–708. [DOI] [PubMed] [Google Scholar]
- 4.Khatana SAM, Werner RM and Groeneveld PW. Association of Extreme Heat and Cardiovascular Mortality in the United States: A County-Level Longitudinal Analysis From 2008 to 2017. Circulation. 2022;146:249–261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Barnett AG, Hajat S, Gasparrini A and Rocklov J. Cold and heat waves in the United States. Environ Res. 2012;112:218–24. [DOI] [PubMed] [Google Scholar]
- 6.Alahmad B, Khraishah H, Roye D, Vicedo-Cabrera AM, Guo Y, Papatheodorou SI, Achilleos S, Acquaotta F, Armstrong B, Bell ML, et al. Associations Between Extreme Temperatures and Cardiovascular Cause-Specific Mortality: Results From 27 Countries. Circulation. 2023;147:35–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lee JY, Marotzk J, Bala G, Cao L, Corti S, Dunne JP, Engelbrecht F, Fischer E, Fyfe JC, Jones C, et al. The Physical Science Basis. Contribution of Working Group I to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change 2021:553–67217. [Google Scholar]
- 8.Vespa J, Armstrong DM and Medina L. Demographic turning points for the United States: Population projections for 2020 to 2060. Report P25–1144. US Department of Commerce, Economics and Statistics Administration, US Census Bureau. 2018. [Google Scholar]
- 9.Kerns K and Locklear LS. Three new census bureau products show domestic migration at regional, state, and county levels. US Census Bureau. https://www.census.gov/library/stories/2019/04/moves-from-south-west-dominate-recent-migration-flows.html. Published 2019. Updated October 28, 2021. Accessed July 26, 2023, 2023. [Google Scholar]
- 10.Mackun P. About 14.6 million people live in 40 counties in five states. US Census Bureau. https://www.census.gov/library/stories/2019/02/fast-growth-in-desert-southwest-continues.html. Published 2019. Updated October 8, 2021. Accessed July 26, 2023, 2023. [Google Scholar]
- 11.Lin S, Luo M, Walker RJ, Liu X, Hwang SA and Chinery R. Extreme high temperatures and hospital admissions for respiratory and cardiovascular diseases. Epidemiology. 2009;20:738–46. [DOI] [PubMed] [Google Scholar]
- 12.Gronlund CJ, Berrocal VJ, White-Newsome JL, Conlon KC and O’Neill MS. Vulnerability to extreme heat by socio-demographic characteristics and area green space among the elderly in Michigan, 1990–2007. Environ Res. 2015;136:449–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.O’Neill BC, Carter TR, Ebi K, Harrison PA, Kemp-Benedict E, Kok K, Kriegler E, Preston BL, Riahi K, Sillmann J, et al. Achievements and needs for the climate change scenario framework. Nat Clim Chang. 2020;10:1074–1084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hausfather Z and Peters GP. Emissions – the ‘business as usual’ story is misleading. Nature. 2020;577:618–620. [DOI] [PubMed] [Google Scholar]
- 15.Schwalm CR, Glendon S and Duffy PB. RCP8.5 tracks cumulative CO2 emissions. Proceedings of the National Academy of Sciences. 2020;117:19656–19657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Dahl K, Spanger-Siegfried E, Licker R, Caldas A, Abatzoglou J, Mailloux N, Cleetus R, Udvardy S, Declet-Barreto J and Worth P. Killer heat in the United States: climate choices and the future of dangerously hot days. 2019. [Google Scholar]
- 17.The Heat Index Equation. National Weather Service. https://www.wpc.ncep.noaa.gov/html/heatindex_equation.shtml. Updated May 12, 2022. Accessed June 3, 2023. [Google Scholar]
- 18.Extreme Heat | What. Federal Emergency Management Agency. https://community.fema.gov/ProtectiveActions/s/article/Extreme-Heat-What. Accessed July 27, 2023, 2023. [Google Scholar]
- 19.Khatana SAM, Werner RM and Groeneveld PW. Association of Extreme Heat With All-Cause Mortality in the Contiguous US, 2008–2017. JAMA Netw Open. 2022;5:e2212957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dahl K, Licker R, Abatzoglou JT and Declet-Barreto J. Increased frequency of and population exposure to extreme heat index days in the United States during the 21st century. Environmental Research Communications. 2019;1:075002. [Google Scholar]
- 21.Abatzoglou JT. Development of gridded surface meteorological data for ecological applications and modelling. International Journal of Climatology. 2013;33:121–131. [Google Scholar]
- 22.Hauer ME. Population projections for U.S. counties by age, sex, and race controlled to shared socioeconomic pathway. Scientific Data. 2019;6:190005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Riahi K, van Vuuren DP, Kriegler E, Edmonds J, O’Neill BC, Fujimori S, Bauer N, Calvin K, Dellink R, Fricko O, et al. The Shared Socioeconomic Pathways and their energy, land use, and greenhouse gas emissions implications: An overview. Global Environ Chang. 2017;42:153–168. [Google Scholar]
- 24.Jones B and O’Neill BC. Spatially explicit global population scenarios consistent with the Shared Socioeconomic Pathways. Environmental Research Letters. 2016;11:084003. [Google Scholar]
- 25.Arias E, Heron M, National Center for Health S, Hakes J and Bureau USC. The Validity of Race and Hispanic-origin Reporting on Death Certificates in the United States: An Update. Vital Health Stat 2. 2016:1–21. [PubMed] [Google Scholar]
- 26.Mollié A Bayesian mapping of disease. Markov chain Monte Carlo in practice. 1996;1:359–379. [Google Scholar]
- 27.Vallianou NG, Geladari EV, Kounatidis D, Geladari CV, Stratigou T, Dourakis SP, Andreadis EA and Dalamaga M. Diabetes mellitus in the era of climate change. Diabetes Metab. 2021;47:101205. [DOI] [PubMed] [Google Scholar]
- 28.Mize TD, Doan L and Long JS. A general framework for comparing predictions and marginal effects across models. Sociological Methodology. 2019;49:152–189. [Google Scholar]
- 29.Correia S, Guimarães P and Zylkin T. Fast Poisson estimation with high-dimensional fixed effects. The Stata Journal. 2019;20:115 – 95. [Google Scholar]
- 30.Chaseling GK, Iglesies-Grau J, Juneau M, Nigam A, Kaiser D and Gagnon D. Extreme Heat and Cardiovascular Health: What a Cardiovascular Health Professional Should Know. Can J Cardiol. 2021;37:1828–1836. [DOI] [PubMed] [Google Scholar]
- 31.Mora C, Counsell CWW, Bielecki CR and Louis LV. Twenty-Seven Ways a Heat Wave Can Kill You: Deadly Heat in the Era of Climate Change. Circ Cardiovasc Qual Outcomes. 2017;10. [DOI] [PubMed] [Google Scholar]
- 32.Pescatello LS, Mack GW, Leach CN, Jr. and Nadel ER. Effect of beta-adrenergic blockade on thermoregulation during exercise. J Appl Physiol (1985). 1987;62:1448–52. [DOI] [PubMed] [Google Scholar]
- 33.Balmain BN, Sabapathy S, Jay O, Adsett J, Stewart GM, Jayasinghe R and Morris NR. Heart Failure and Thermoregulatory Control: Can Patients With Heart Failure Handle the Heat? J Card Fail. 2017;23:621–627. [DOI] [PubMed] [Google Scholar]
- 34.Bobb JF, Obermeyer Z, Wang Y and Dominici F. Cause-specific risk of hospital admission related to extreme heat in older adults. JAMA. 2014;312:2659–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Nam YH, Bilker WB, Leonard CE, Bell ML, Alexander LM and Hennessy S. Effect of statins on the association between high temperature and all-cause mortality in a socioeconomically disadvantaged population: a cohort study. Sci Rep. 2019;9:4685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hsu A, Sheriff G, Chakraborty T and Manya D. Disproportionate exposure to urban heat island intensity across major US cities. Nat Commun. 2021;12:2721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.O’Neill MS, Zanobetti A and Schwartz J. Disparities by race in heat-related mortality in four US cities: the role of air conditioning prevalence. J Urban Health. 2005;82:191–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Iungman T, Cirach M, Marando F, Pereira Barboza E, Khomenko S, Masselot P, Quijal-Zamorano M, Mueller N, Gasparrini A, Urquiza J, et al. Cooling cities through urban green infrastructure: a health impact assessment of European cities. Lancet. 2023;401:577–589. [DOI] [PubMed] [Google Scholar]
- 39.Sen S and Khazanovich L. Limited application of reflective surfaces can mitigate urban heat pollution. Nat Commun. 2021;12:3491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Guardaro M, Messerschmidt M, Hondula DM, Grimm NB and Redman CL. Building community heat action plans story by story: A three neighborhood case study. Cities. 2020;107:102886. [Google Scholar]
- 41.Nordio F, Zanobetti A, Colicino E, Kloog I and Schwartz J. Changing patterns of the temperature-mortality association by time and location in the US, and implications for climate change. Environ Int. 2015;81:80–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS and Koplan JP. The continuing epidemics of obesity and diabetes in the United States. JAMA. 2001;286:1195–200. [DOI] [PubMed] [Google Scholar]
- 43.Cohen J, Agel L, Barlow M, Garfinkel CI and White I. Linking Arctic variability and change with extreme winter weather in the United States. Science. 2021;373:1116–1121. [DOI] [PubMed] [Google Scholar]
- 44.van Vuuren DP, Edmonds J, Kainuma M, Riahi K, Thomson A, Hibbard K, Hurtt GC, Kram T, Krey V, Lamarque JF, et al. The representative concentration pathways: an overview. Climatic Change. 2011;109:5–31. [Google Scholar]
- 45.Intergovernmental Panel On Climate Change. Climate change 2014: synthesis report. Contribution of Working Groups I, II and III to the fifth assessment report of the Intergovernmental Panel on Climate Change. Core Writing Team, Pachauri RK and Meyer LA (eds) IPCC, Geneva. 2014;151. [Google Scholar]
- 46.Lee J-Y, Marotzke J, Bala G, Cao L, Corti S, Dunne JP, Engelbrecht F, Fischer E, Fyfe JC, Jones C, et al. Future global climate: scenario-based projections and near-term information. In: Masson-Delmotte V, Zhai P, Pirani A, Connors SL, Pean C, Berger S, Caud N, Chen Y, Goldfarb L, Gomis MI, Huang M, Leitzell K, Lonnoy E, Matthews JBR, Maycock TK, Waterfield T, Yelekçi O, Yu R and Zhou B, eds. Climate Change 2021: The Physical Science Basis Contribution of Working Group I to the Sixth : Assessment Report of the Intergovernmental Panel on Climate Change : Chapter 4 Genf, Switzerland: IPCC; 2021: 1–195. [Google Scholar]
- 47.Hausfather Z Explainer: How ‘shared socioeconomic pathways’ explore future climate change. Carbon Brief. https://www.carbonbrief.org/explainer-how-shared-socioeconomic-pathways-explore-future-climate-change/. Published 2018. Accessed June 1, 2023. [Google Scholar]
- 48.Kc S and Lutz W. The human core of the shared socioeconomic pathways: Population scenarios by age, sex and level of education for all countries to 2100. Glob Environ Change. 2017;42:181–192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Population Projections 2004 – 2030 by State, Age and Sex: Methodology Summary https://wonder.cdc.gov/wonder/help/populations/population-projections/methodology.html. Updated November 19, 2019. Accessed June 5, 2023. [Google Scholar]
- 50.Hamilton CH and Perry J. A short method for projecting population by age from one decennial census to another. Social Forces. 1962;41:163–170. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.