

Abstract
Purpose:
To (a) evaluate cross-sectional and longitudinal associations between controlling parental feeding practices in adolescence (i.e., restrictive feeding and pressure-to-eat) and intuitive eating (IE) in adolescence and emerging adulthood; and (b) explore child gender and parental concern about child weight as moderators.
Methods:
The sample included participants (N=1,383) from the population-based EAT 20102018 study who provided data in adolescence (14.4±2.0 years) and emerging adulthood (22.0 ± 2.0 years) and had at least one caregiver complete surveys in adolescence. Generalized estimating equations evaluated cross-sectional and longitudinal associations between restrictive feeding and pressure-to-eat in adolescence and IE in adolescence and emerging adulthood. Interactions with gender and parental concern over child weight in adolescence were explored.
Results:
Restrictive feeding was cross-sectionally associated with lower IE in adolescence (b=0.04), though evidence of moderation by parental weight concern indicated this association was only observed in the context of low parental weight concern. Greater pressure-to-eat was associated with lower adolescent IE among boys but higher IE among girls. Longitudinally, the association between pressure-to-eat in adolescence and IE in emerging adulthood differed by parental weight concern; greater pressure-to-eat predicted higher emerging adult IE at high parental weight concern, but lower IE at low parental weight concern.
Conclusions:
Controlling feeding practices in adolescence displayed differential associations with child IE in adolescence and emerging adulthood based on child gender and parental concern over child weight. Notably, pressure-to-eat was associated with greater IE among adolescent girls but lower IE among boys. Results suggest parental feeding is a valuable intervention target.
Impacts and Contribution Statement:
Although parents’ use of restrictive and pressure-to-eat feeding practices appear to impact their adolescent’s intuitive eating in the short- and long-term, these impacts differ depending on their child’s gender and how concerned parents are about their child’s weight. Results can be used to refine interventions that promote intuitive eating.
Keywords: controlling feeding, adolescence, emerging adulthood, intuitive eating, family factors
Intuitive eating (IE) is an approach best known for its emphasis on eating according to hunger and satiety cues [1]. Research on the positive correlates and outcomes of IE continues to proliferate. Data show people who eat intuitively have greater self-esteem, body appreciation, and psychological functioning, lower weight-bias internalization, and engage in less disordered eating [2–4]. Some evidence also suggests IE may benefit health biomarkers (e.g., Hb1AC) [5,6]. However, comparatively little research exists on factors that shape the development of IE, which will be crucial to assist in the identification of novel intervention targets.
Parents use a variety of feeding practices, which play a powerful role in shaping child eating behaviors [7,8]. Controlling feeding practices (i.e., restrictive feeding and pressure-to-eat), in particular, are well-studied and appear to have long-term implications for the development of maladaptive eating behaviors in young people. [9]. For instance, data consistently show that restrictive feeding by the parent predicts eating in the absence of hunger, emotional eating, and disordered eating by the child [9–11]. Research on the impact of parental pressure-to-eat on child eating behaviors is less consistent and appears to vary across child gender; however, some studies suggest maternal pressure-to-eat also may contribute to children eating in the absence of hunger [10,12,13] (though one study found the inverse result among young boys [14]). These outcomes are concerning, given that eating in the absence of hunger is longitudinally associated with binge and loss-of-control eating [15], and disordered eating is linked to physical and mental health morbidity and elevated eating disorder risk [16].
Data on the associations between parental feeding practices and IE specifically, however, are limited. Two cross-sectional studies examined the associations between feeding practices and parents’ own IE in infancy and early childhood [17,18]. One found that parental IE was positively associated with a responsive infant feeding style [17]. The other found that parental IE moderated the association between concern over the child’s weight and restrictive feeding, such that mothers with high weight concern and low-to-average IE were more likely to use restrictive feeding with their 2–5 year-old children [18]. Only two known studies, both retrospective, have investigated the association between parental feeding practices and the child’s IE [19,20]. One found no association between either pressure-to-eat or restrictive feeding and IE [20], whereas another found that recollection of parental restrictive feeding in childhood was associated with lower IE among college women [19]. However, retrospective reports are prone to recall bias [21] and in Ellis et al., parent and child recollection of parental feeding practices did not significantly correlate with each other. Thus, although preliminary data suggest controlling feeding practices might hinder IE development, longitudinal data are needed to confirm and extend findings. Further, most extant research examined parental feeding practices in childhood, making it unclear whether parental feeding strategies in adolescence continue to play a role in shaping IE. Because adolescence is a developmental stage during which young people transition to independence and establish lifelong health behaviors, it is a particularly important potential intervention point [22].
Thus, the purpose of this study was to evaluate the cross-sectional and longitudinal associations among controlling parental feeding practices (i.e., restrictive feeding, pressure-to-eat) in adolescence and the child’s IE in adolescence and eight years later in emerging adulthood. Data show parental concerns over the child’s weight are associated with the feeding practices they use. For instance, parents are more likely to use pressure-to-eat among children whose actual or perceived weight is lower, but restrictive feeding practices with children whose actual or perceived weight is higher [23,24]. Although parental weight concerns likely directly influence the feeding strategies parents choose, these concerns may also intensify the effects of such practices. For instance, a parent concerned about their child’s weight and engaging in restrictive feeding practices may make weight-related comments during mealtimes or while clothes shopping. This weightrelated pressure in tandem with restrictive feeding could make a child especially vulnerable to ignoring their hunger/satiety cues. For instance, the child may perceive they need rules to guide their eating (vs. hunger) and may themselves develop restrictive eating patterns. Therefore, we included parental concern about child weight as a moderator as we perceived that weight concerns will likely be conveyed to the child in explicit and implicit ways that may be particularly detrimental to a child’s IE. Additionally, we considered both child and parent gender as moderators, given findings that the association between parental feeding strategies and child eating behaviors differs across child gender [14], and most research has focused specifically on maternal feeding practices, leaving the role of parent gender in the family food environment unclear. We expected that exposure to both restrictive feeding and pressure-to-eat by parents in adolescence would be concurrently associated with lower IE in adolescence and would predict lower IE in emerging adulthood. Further, we hypothesized that parental weight concerns in adolescence would strengthen the association between controlling feeding practices and IE, with high controlling feeding and high weight concerns being associated with the lowest IE scores. Results will enhance understanding of factors affecting IE development, which can be used to inform interventions that promote this adaptive eating style among youth and families.
Method
Study Design and Participants
EAT 2010–2018 (Eating and Activity over Time) and the coordinated Project F-EAT (Families and Eating and Activity among Teens) are population-based longitudinal studies of eating, activity, and weight-related attitudes and behaviors among young people (EAT 2010–2018) [25] and their families (F-EAT) [26]. Adolescents from public schools in Minneapolis/St. Paul, Minnesota completed baseline surveys during the 2009–2010 academic year (EAT 2010; N=2,793, Mage=14.4±2.0 years) and were asked to identify up to two parents/caregivers to complete surveys by mail or phone. At least one parent/caregiver (hereafter referred to as “parents”) participated for 85.3% of the sample.
Of the original sample, 65.8% completed follow-up surveys in 2017–2018 (EAT 2018; N=1,568, Mage = 22.0 ± 2.0 years). Attrition did not occur at random, with responders more likely to be White, female, and at higher socioeconomic status (SES). Therefore, we used inverse probability weighting (IPW) to minimize response bias and facilitate extrapolation of findings back to the original EAT 2010 sample [27]. Weights were calculated with the aim to create estimates representative of the 2010 baseline, population-based sample, and were derived based on several EAT 2010 variables, including sociodemographic information, past year dieting frequency, and observed weight status. Study procedures were approved by the University of Minnesota’s Institutional Review Board Human Subjects Committee.
The analytic sample included participants (N=1,383; 52.7% female, 47.3% male in adolescence) who provided IE data at both EAT 2010 and 2018 and had at least one parent participate in F-EAT 2010. The sample identified as 52.0% female, 46.4% male, and 0.7% another gender identity (0.9% did not report gender in adulthood) and was diverse across race/ethnicity (19.7% Asian, 28.9% Black, 16.7% Latinx, 14.5% Multiracial/Other, 19.8% White) and SES (37.1% low, 20.8% lower middle, 17.4% middle, 13.3% upper middle, 7.8% high).
Most female caregivers (N=1,294; Mage=41.6 ± 7.8) identified as the participant’s mother (96.8%); 2.1% identified as another female caregiver and 1.1% as a stepmother. Of the 842 male caregivers (Mage = 44.8 ± 8.4), 87.9% identified as the participant’s father, 9.1% as the stepfather, and 3.0% as another male caregiver.
Survey Development
Development of the EAT-2010 survey was guided by Social Cognitive Theory with an ecological perspective, a review of previous Project EAT surveys, multidisciplinary expert review, and pilot testing with adolescents. Details of the EAT 2010 and F-EAT survey development process and survey psychometrics have been previously published [28]. Key items from the EAT 2010 survey were retained at EAT 2018 to facilitate longitudinal analyses and modified, when appropriate, to reflect secular trends and the developmental transition. Focus groups were held with 29 young people to evaluate the 2018 survey; once finalized, a subgroup of EAT 2018 participants (n=112) completed the survey twice within three weeks to assess test-retest reliability.
Measures
Parental Feeding
Parents reported their controlling feeding practices through items from the Birch’s Child Feeding Questionnaire (CFQ) [29]. Six items from the restriction subscale measured restrictive feeding (e.g., “I intentionally keep some foods out of my child’s reach”); specifically, we excluded the items on using food as a reward given these items demonstrated poor fit on the restraint factor in a confirmatory factor analysis of the CFQ among adolescents [30]. We used the pressure subscale from the CFQ to measure PE (e.g., “My child should always eat all of the food on his/her plate”). Items were rated on a 4-point scale from 1=Disagree to 4=Agree and averaged, with higher scores reflecting greater controlling feeding [test-reliability r=0.72 (restrictive feeding), r=0.73 (PE); McDonald’s ω=0.71 (restrictive feeding); McDonald’s ω=0.87 (PE)].
Parental Weight Concern
Parents indicated their degree of concern about their child’s weight through the item, “How concerned are you about your child’s weight?,” which was originally developed for the Nepean Kids Growing Up Parent Questionnaire [31]. Response options included: 1=Not at all concerned, 2=A little concerned, 3=Quite concerned, and 4=Very concerned. Test-retest reliability was 0.68.
Intuitive Eating
Three items adapted from the Intuitive Eating Scale (IES) assessed IE [32,33]. These items included: “I stop eating when I feel full” (Eating for Physical Rather than Emotional Reasons subscale), “I eat everything that is on my plate, even if I’m not that hungry” (part of the item pool on the Eating for Physical Rather than Emotional Reasons subscale), and “I trust my body to tell me how much to eat” (Reliance on Hunger/Satiety Cues subscale). Items were rated on a 4-point scale, from 1=Hardly ever to 4=Almost always. The second item was reverse-scored, and items were averaged to derive an overall IE score, with higher scores reflecting greater IE (test-retest r=0.57; adolescence: McDonald’s ω=0.50; emerging adulthood: McDonald’s ω=0.56,).
Demographics
Participants self-reported their gender identity, age, and race/ethnicity. Household SES was determined via a classification and regression tree-based algorithm based on parent educational attainment, employment status, and public assistance receipt during the youth’s adolescence (testretest r=0.90) [34]. Parents also reported their role (i.e., mother, father, stepmother, stepfather, other female guardian, other male guardian) and age.
Data Analysis
Data preparation and analyses were conducted in R Studio v1.4. All analyses incorporated IPW [27], with statistical significance set at p<.05. We conducted paired-samples t-tests to evaluate whether IE differed between adolescence and emerging adulthood and whether parental restrictive eating, pressure-to-eat, or weight concern differed by parent gender. Independent samples t-tests evaluated whether mother and father restrictive eating, pressure-to-eat, or weight concern differed by child gender.
Because some children (n=752) had two parents included in analyses, we accounted for the within-family correlation using generalized estimating equations (GEE) with an independent correlation structure. GEE models were conducted using the gee and geepack packages in R. Crosssectional models in adolescence and longitudinal models of parental feeding in adolescence predicting IE in emerging adulthood were conducted. We also explored parental weight concern as a moderator of the associations between parental feeding and child IE.
Restrictive feeding and pressure-to-eat were modeled separately as independent variables (IVs). IE was entered as the DV. The moderating effect of parental weight concern was investigated by adding an interaction term to the model (restrictive feeding or pressure-to-eat x weight concern). Models adjusted for child age, race/ethnicity, child and parent gender, and SES. Longitudinal models adjusted for IE in adolescence. We explored whether the associations between parental feeding and IE differed by parent and child gender by adding interaction terms (parent or child gender x parental feeding). Because our IVs (parental feeding and weight concerns) were measured in adolescence, we included adolescent-reported gender identity in analyses. We used the sjPlot and ggplot2 packages to plot significant interactions and evaluate the nature of differences.
Results
Average IE decreased from adolescence (2.94±.59) to adulthood (2.87±.59) overall, t(1376)=3.25, p=.001 (Table 1). In both adolescence and emerging adulthood, male participants reported significantly lower IE than female participants [adolescence: t(1376)=−2.21, p=.03; emerging adulthood: t(1373.1)=−2.75, p=.01].
Table 1.
Descriptive Statistics and Gender Differences in Parental Feeding and Weight Concern
| Intuitive Eating Across Time Points | ||
|---|---|---|
| Adolescence (14.3±2.0) |
Adulthood (22.1±2.0) |
|
| Intuitive eating | ||
| Female | 2.97 (.58) | 2.90 (.61) |
| Male | 2.89 (.60) | 2.82 (.57) |
| Overall | 2.94 (.59) | 2.87 (.59) |
| Parental Factors During Adolescence | ||
| Mother | Father | |
| Restrictive feeding | ||
| Female child | 2.49 (.92) | 2.46 (.89) |
| Male child | 2.49 (.89) | 2.54 (.81) |
| Overall | 2.49 (.91) | 2.49 (.86) |
| Pressure-to-eat | ||
| Female child | 2.16 (.84) | 2.21 (.81) |
| Male child | 2.14 (.84) | 2.27 (.83) |
| Overall | 2.15 (.84) | 2.23 (.82) |
| Weight concern | ||
| Female child | 1.60 (.87) | 1.64 (.88) |
| Male child | 1.59 (.86) | 1.61 (.90) |
| Overall | 1.60 (.87) | 1.63 (.89) |
Parental feeding practices and weight concern did not significantly differ by child gender. Restrictive feeding was comparable between mothers and fathers [M=2.49±.91 (mothers); M=2.49±.86 (fathers), t(1586.8) = −0.03, p = .97]. Fathers reported significantly greater pressureto-eat (M=2.23±.82) than mothers (M=2.15±.84), t(1590.0) = −2.78, p = .005. Mothers (M=1.60±.87) and fathers (M=1.63±.89) reported similar concern about their child’s weight, t(1576.0) = −1.08, p = .28.
Adolescent and emerging adult IE were positively associated (Table 2). Both feeding strategies were negatively associated with IE at both time-points. Parental weight concerns were associated with higher restrictive feeding and pressure-to-eat.
Table 2.
Correlations between Study Variables
| 1. | 2. | 3. | 4. | 5. | ||
|---|---|---|---|---|---|---|
| 1. | IE (adolescence) | -- | ||||
| 2. | IE (adulthood) | .21*** | -- | |||
| 3. | Restrictive feeding (adolescence) | −.07** | −.04* | -- | ||
| 4. | Pressure-to-eat (adolescence) | −.06** | −.07** | .35*** | -- | |
| 5. | Parental concern about child’s weight | −.02 | −.09*** | .29*** | .11*** | -- |
Note. IE=Intuitive eating
p<.05
p<.01
p<.001
Restrictive Feeding
Restrictive feeding was cross-sectionally associated with lower IE in adolescence (b=0.04, p=.03; Table 2). This association did not significantly differ by parent (p=.09) or child gender (p=.53). However, the interaction between restrictive feeding and parental weight concern was significant (p=.02); when accompanied by low parental weight concern, restrictive feeding was negatively associated with IE, whereas restrictive feeding was not associated with IE when accompanied by high parental weight concern (Figure 1). Simple slopes for restrictive feeding by level of parental weight concern are presented in the Supplemental Material, as are results of stratified analyses by parental perception of the adolescent’s weight (“underweight,” about right, “overweight”), which indicate the interaction remained significant only for parents who perceived their adolescent’s weight as “overweight.”
Figure 1.
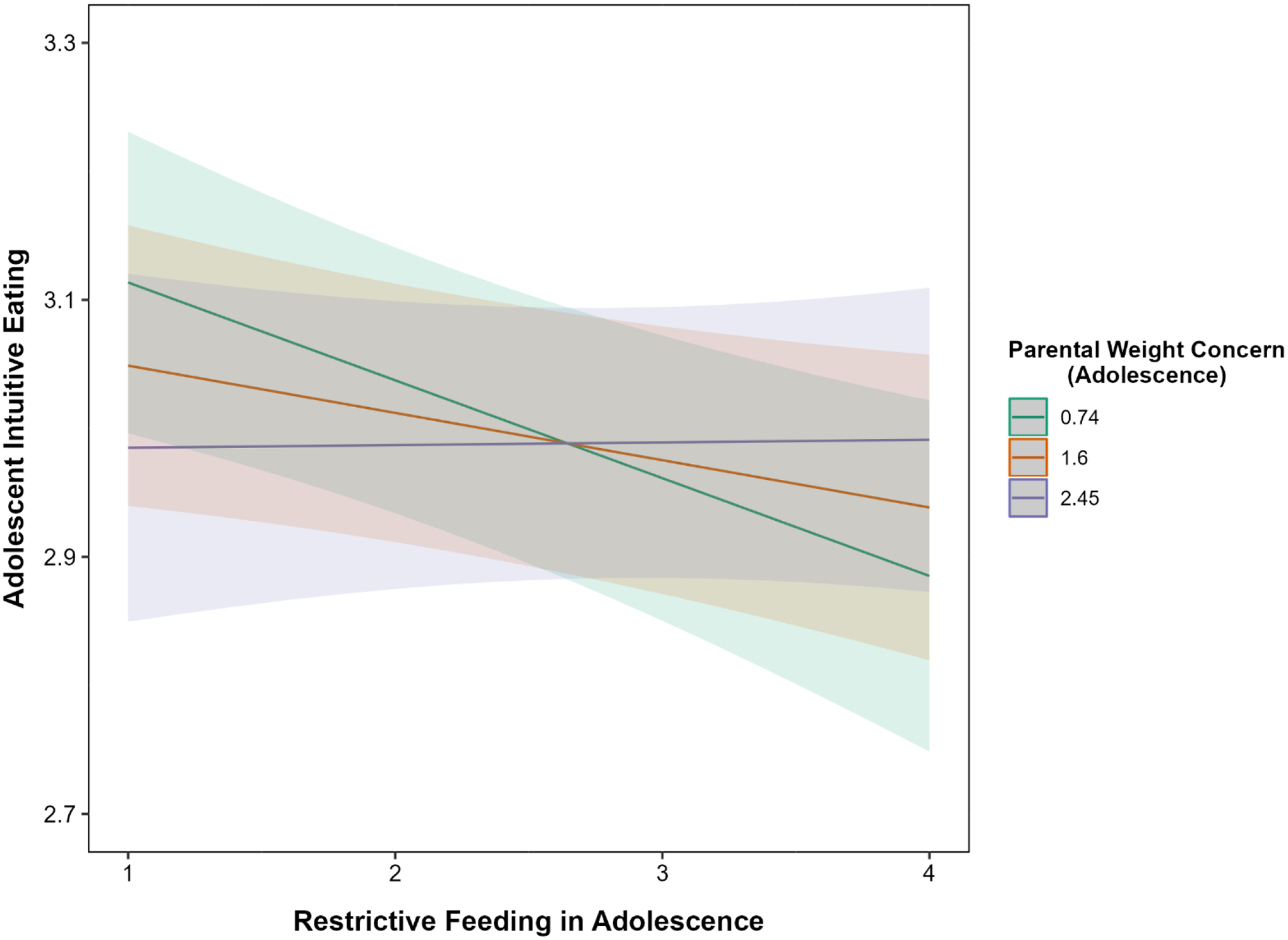
Cross-Sectional Association between Parental Restrictive Feeding and Child Intuitive Eating in Adolescence by Parental Weight Concern
Note. Parental weight concern is shown at < −1 SD below the mean, within 1 SD of the mean, and > +1 SD above the mean.
Restrictive feeding in adolescence did not significantly predict IE in emerging adulthood (b=−0.01, p=.50). This association did not differ by parent (p=.59) or child gender (p=.85) or by parental weight concern (p=.11).
Pressure-to-Eat
The association between pressure-to-eat and IE in adolescence was not significant (b=0.02, p=.45), nor did it differ by parent gender (p=.49). However, the interaction between pressure-to-eat and child gender was significant (p=.01); greater pressure-to-eat corresponded to lower IE among boys but higher IE among girls (Figure 2). The interaction between pressure-toeat and parental weight concern was not significant (p=.96).
Figure 2.
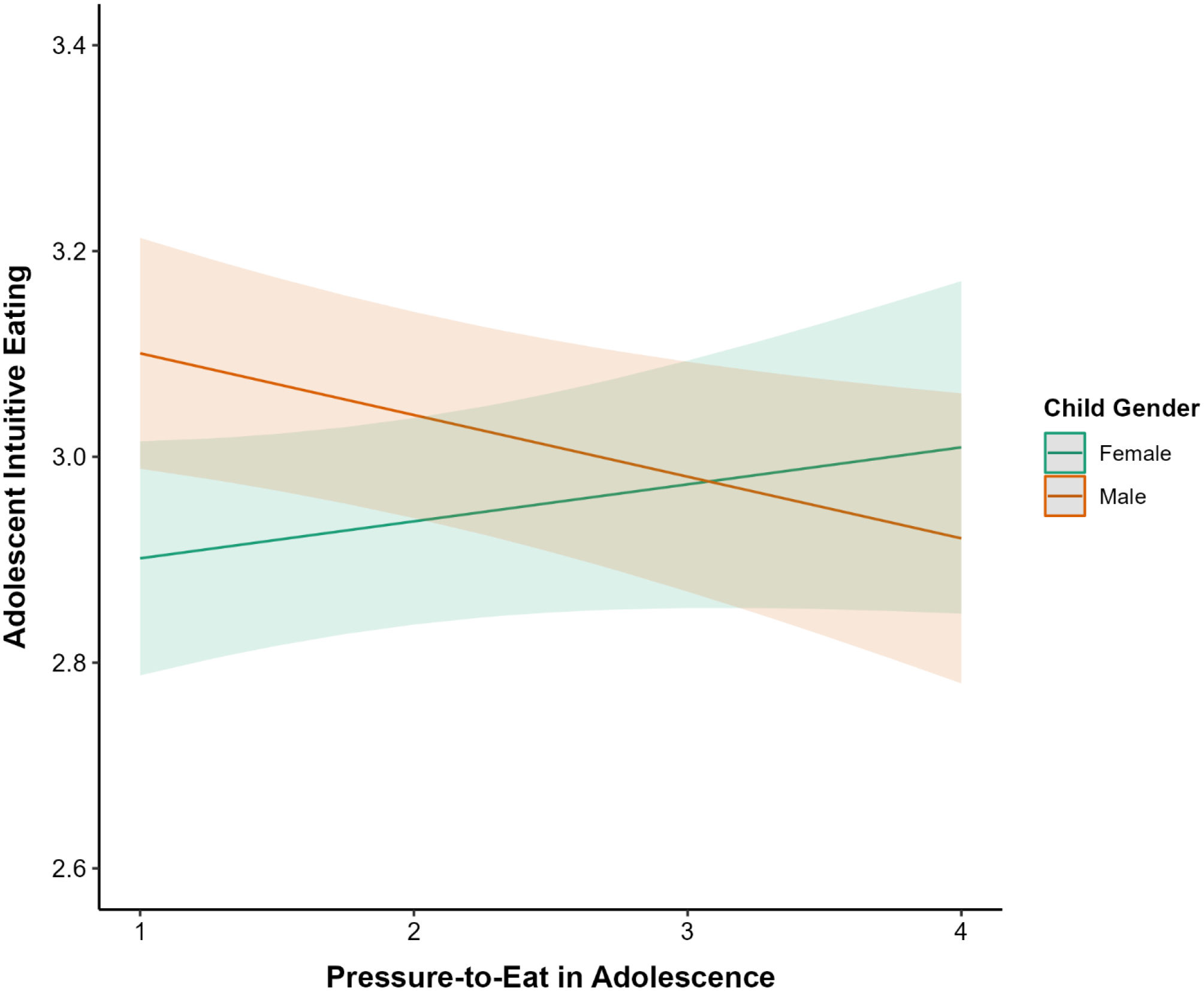
Cross-Sectional Association between Parental Pressure-to-Eat and Intuitive Eating in Adolescence by Child Gender
The association between pressure-to-eat in adolescence and child IE in emerging adulthood was not significant (b=−0.001, p=.75), and did not differ by parent (p=.44) or child gender (p=.14). However, there was a significant interaction between pressure-to-eat and parental weight concern (p=.01). At low parental weight concern, greater pressure-to-eat was associated with lower IE. However, at high parental weight concern, greater pressure-to-eat was associated with greater IE (Figure 3). Adding parental perception of the adolescent’s weight “underweight,” about right, “overweight”) as a covariate to the model did not change the pattern of results. Simple slopes and stratified analyses by parental perception of the adolescent’s weight are available in Supplemental Material.
Figure 3.
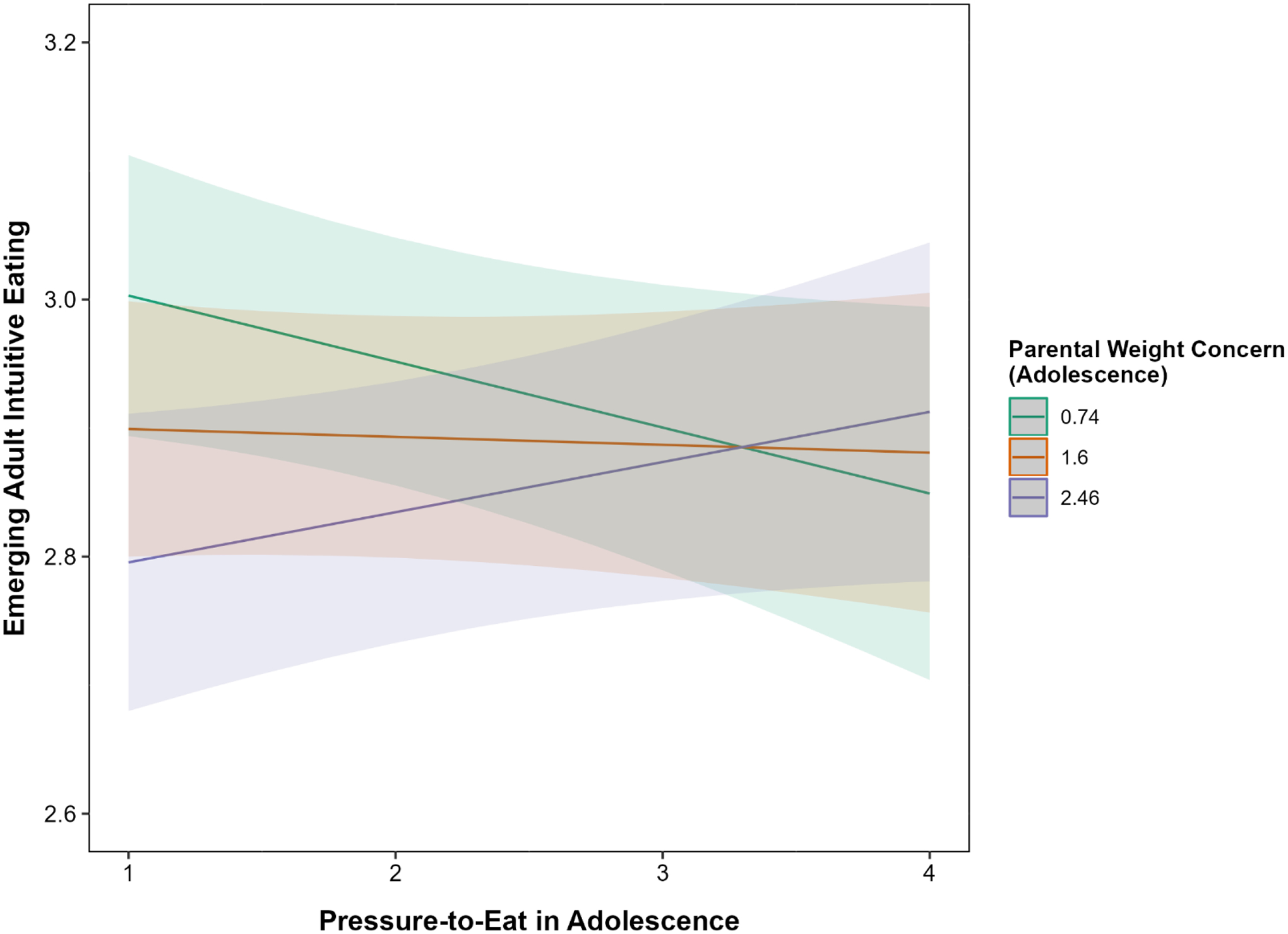
Longitudinal Association between Parental Pressure-to-Eat in Adolescence on Child Intuitive Eating in Emerging Adulthood by Parental Weight Concern in Adolescence
Note. Parental weight concern is shown at < −1 SD below the mean, within 1 SD of the mean, and > +1 SD above the mean.
Discussion
In a diverse, population-based sample of young people, this study examined associations among controlling parental feeding practices during adolescence with their children’s IE in adolescence and emerging adulthood. We also assessed moderation of these associations by child gender, parent gender, and parental concerns about their child’s weight during adolescence. In cross-sectional analyses, greater parental engagement in restrictive feeding practices was associated with lower adolescent IE in the full sample; however, this association was strongest when parents expressed low levels of concern about their child’s weight. Additionally, greater parental engagement in pressure-to-eat feeding practices was cross-sectionally associated with lower IE in boys but higher IE in girls during adolescence. Parent gender did not moderate any observed associations.
Although IE decreased from adolescence to emerging adulthood, parental feeding practices during adolescence generally did not emerge as important predictors of these changes in child IE, with one caveat. Longitudinally, the only significant finding was that the association between pressure-to-eat during adolescence and child IE in emerging adulthood differed by the level of parental concern about their child’s weight in adolescence. Specifically, greater pressureto-eat predicted decreased child IE during emerging adulthood when accompanied by low levels of parental concern about their child’s weight but predicted increased child IE during emerging adulthood when accompanied by high levels of parental concern about their child’s weight. Conversely, restrictive feeding in adolescence did not predict emerging adult IE. When considered alongside the observed cross-sectional associations, this evidence suggests that parental feeding practices likely play a larger role in shaping the development of IE in young people during childhood itself, rather than leading to changes in IE beyond childhood. In adulthood, myriad other factors likely affect IE, including (but not limited to) SES, food security, work and school schedules, and social media [35,36]. Taken together, findings from this study build upon prior literature to help elucidate the role parental controlling feeding practices may play in IE development in young people.
The observed cross-sectional association between greater restrictive feeding and lower child IE in adolescence aligns with results of a prior retrospective study in which recollection of restrictive feeding during childhood was associated with lower IE among college women [19], and also coheres with prior studies demonstrating associations between restrictive feeding and child disordered eating [9–11,37]. Based on the evidence that parental restrictive feeding practices are linked with more maladaptive and less adaptive eating in children and adolescents, restrictive parental feeding practices stand out as a target for intervention.
Our finding that the association between pressure-to-eat and child IE differed by child gender also maps onto prior research [10,14]. For example, similar to our finding that pressureto-eat was associated with lower IE in boys, prior work in this sample demonstrated that pressure-to-eat was associated with more dieting and greater use of disordered-weight control behaviors in adolescent boys but not girls [38]. It is possible these findings could, at least in part, reflect that parents may be more likely to use pressure-to-eat practices with children they are concerned are not eating enough. Societal appearance ideals are gendered, such that thinness— and, correspondingly, eating less—is promoted more for girls and women, whereas muscularity—and, correspondingly, eating enough—is promoted more for boys and men [39]. These gendered appearance ideals likely do influence differences in parents’ feeding approaches with sons versus daughters. Although pressure-to-eat did not differ by adolescent gender in this study, it is likely that boys and girls experienced such pressure differently. For instance, our finding that greater pressure-to-eat was associated with higher IE in adolescent girls could relate back to gendered appearance ideals. In a society where thinness ideals are thrust upon girls, receiving encouragement to eat from their parents may help counteract those societal ideals and promote a healthier relationship with food for them. Conversely, pressure-to-eat may promote less IE in adolescent boys by way of encouraging them to override their internal hunger and satiety cues. It is unclear why the cross-sectional interaction between pressure-to-eat and child gender was not observed longitudinally. As noted previously, it is certainly plausible that myriad other factors are salient predictors of eating during emerging adulthood, including work/school schedules, social media, and peer/relationship influences.
Examination of parental concerns about their child’s weight during adolescence shed light on nuanced relationships between parental feeding practices and child IE. As parents are more likely to use pressure-to-eat practices among children whose weight is lower and more likely to use restrictive practices with children whose weight is higher [23,24], we expected higher parental concerns about their child’s weight to exacerbate associations between controlling feeding practices and IE, such that the combination of high controlling parental feeding practices and high parental weight concerns would result in the lowest IE scores for children. Instead, we found that for both restrictive feeding and pressure-to-eat, associations between more controlling feeding practices and lower IE were actually strongest in the context of lower parental concern about their child’s weight. These somewhat unexpected findings suggest reasons other than parental weight concerns could be driving controlling parental feeding practices. For example, a prior study found that food insecurity was associated with greater use of both restrictive feeding and pressure-to-eat practices [40]. Perhaps use of controlled feeding practices in a food-insecure environment could exacerbate the tension between ensuring that, on one hand, the child eats enough food, but on the other hand ensuring that an excess is not consumed (reflecting concerns about limited availability) [41]). There is evidence food insecurity is related to lower levels of IE in young people [35] and may therefore be an important factor to consider when interpreting the somewhat unexpected moderation results in this study. It is important to note, however, that for both restrictive feeding and pressure-to-eat, the highest IE scores observed in this study corresponded to low parental controlling feeding practices and low parental concern over child weight, consistent with our study hypotheses.
The present study has both strengths and limitations. Important strengths of the study include its large, diverse, and population-based sample, its longitudinal design, and the incorporation of parents’ own report of feeding practices and concern over child weight. Limitations of the study include the self-report nature of the data and the use of an abbreviated IE measure. Including IE alongside many variables of interest to eating-related health necessitated a brief measure, but meant we were unable to assess nuanced associations between parental feeding and IE’s domains. Additionally, internal consistency of our IE measure was low, which is expected with few items. The inclusion of one reverse-coded item may have further contributed to lower-than-expected internal consistency. Nevertheless, measures with lower reliability still provide valuable information and are more likely to underestimate than overestimate associations [42]. Additionally, it is not clear to what extent findings may generalize beyond the Minneapolis-St. Paul metropolitan area of Minnesota from which participants in this study were recruited. Although the longitudinal design is a strength both parental, we are still limited in the temporality we can establish. It is likely parental feeding is also shaped by child characteristics (e.g., picky eating, allergies, gastrointestinal concerns), and it is also possible that shared factors (e.g., genetics) may contribute to feeding and child eating styles. Finally, feeding practices vary across SES, culture, and ethnicity; for instance, data show both pressure-to-eat and restrictive feeding are more common among marginalized racial and ethnic groups, which is likely related to cultural norms, acculturation, and economic resources [43]. Therefore, such sociodemographic factors likely contribute meaningfully to the association between feeding strategies and IE and merit further investigation in future work.
In conclusion, we examined cross-sectional and longitudinal associations between controlling parental feeding practices and IE in adolescence and emerging adulthood. Parental concerns about child weight and gender were tested as potential moderating variables. We found cross-sectional evidence that restrictive feeding practices were correlated with lower IE in adolescence, which was exacerbated among parents with low weight concerns. In contrast, gender moderated the association between pressure-to-eat and IE, such that a negative association was observed among boys while the reverse was true for girls. Few significant longitudinal relations emerged, except that a negative and positive association between pressureto-eat and IE emerged at low and high parental weight concerns, respectively. Results revealed several important future research directions. Specifically, it is important to investigate mechanisms underlying the observed differences in pressure-to-eat on IE by adolescent gender, including potentially sociocultural appearance pressures. Second, it will be important to examine whether food insecurity and disadvantage more broadly help explain the unexpected moderation results between controlling feeding and parental weight concerns on IE. Finally, given the effect of controlling feeding practices on IE appeared to weaken in adulthood, it will be important to examine the most salient predictors of IE during the key developmental period of early adulthood.
Supplementary Material
Table 3.
Cross-Sectional and Longitudinal Associations between Parental Controlling Feeding Strategies in Adolescence and Intuitive Eating
| Cross-sectional (Adolescence) | Longitudinal (Adolescence – Emerging Adulthood) | |||||
|---|---|---|---|---|---|---|
| Restrictive feeding (RF) | b (SE) | 95% CI | p | b (SE) | 95% CI | p |
| RF | −0.04 (.02) | [−0.07, −0.01] | .03 | −0.01 (.02) | [−0.05, 0.02] | .50 |
| RF x Parent Gender | −0.04 (.02) | [−0.09, 0.01] | .09 | −0.01 (.02) | [−0.06, 0.04] | .59 |
| RF x Child Gender | −0.02 (.04) | [−0.09, 0.05] | .53 | −0.01 (.03) | [−0.07, 0.06] | .85 |
| RF x WC | 0.05 (.02) | [0.01, 0.08] | .02 | 0.03 (.02) | [−0.01, 0.07] | .11 |
| Pressure-to-eat (PE) | ||||||
| PE | −0.02 (.02) | [−0.06, 0.03] | .45 | −0.001 (.02) | [−0.05, 0.03] | .75 |
| PE x Parent Gender | −0.02 (.03) | [−0.07, 0.03] | .49 | −0.02 (.03) | [−0.07, 0.03] | .44 |
| PE x Child Gender | −0.10 (.04) | [−0.17, −0.02] | .01 | 0.05 (.04) | [−0.02, 0.12] | .14 |
| PE x WC | −0.001 (.02) | [−0.04, 0.04] | .96 | 0.05 (.02) | [0.02, 0.09] | .01 |
Note. WC=weight concern. Scores on the RF and PE scales ranged from 1–4, with higher scores representing greater controlling feeding. Unstandardized beta values are presented, which reflect the average difference in IE for every 1-unit increase in continuous variables. For gender, it represents the average IE difference between male and female-identifying participants, with women as the reference group. Interaction coefficients reflect the difference in one variable for every one-unit increase in the other; for instance, for every 1 unit increase in gender, maternal pressure-to-eat changes by .10, reflecting that boys experience greater pressure-to-eat than girls.
Acknowledgements:
Data collection for the study was supported by Grant Number R01HL127077 from the National Heart, Lung, and Blood Institute (PI: Dianne Neumark-Sztainer). The authors’ time to conduct and describe the analysis reported within this manuscript was supported by Grant Numbers R35HL139853 and T32HL150452 from the National Heart, Lung, and Blood Institute (PI: Dianne Neumark-Sztainer). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Heart, Lung, and Blood Institute, the National Institute of Mental Health, or the National Institutes of Health.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of interest: None
CRediT author statement: CBB: Conceptualization, Data Analysis, Writing – Original Draft.
VMH: Conceptualization, Data Analysis, Writing – Original Draft, Review & Editing. JL: Writing – Original Draft, Review & Editing. RFR: Writing – Review & Editing. KAL: Supervision, Writing – Review & Editing. DNS: Conceptualization, Supervision, Writing – Review & Editing.
Ethical standards: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the University of Minnesota Institutional Review Board Human Subjects Committee (IRB ID: 1101S94792). This IRB holds a Federal Wide Assurance, number FWA00000312, from the Office for Human Research Protection in the Department of Health and Human Services in the United States. Written informed consent was obtained from all participants.
References
- [1].Tribole E, Resch E. Intuitive eating: A revolutionary program that works. New York, NY: St. Martin’s Press; 2020. [Google Scholar]
- [2].Linardon J, Tylka TL, Fuller-Tyszkiewicz M. Intuitive eating and its psychological correlates: A meta-analysis. International Journal of Eating Disorders 2021;54:1073–98. [DOI] [PubMed] [Google Scholar]
- [3].Hazzard VM, Telke SE, Simone M, et al. Intuitive eating longitudinally predicts better psychological health and lower use of disordered eating behaviors: Findings from EAT 2010–2018. Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity 2021;26:287–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Burnette CB, Mazzeo SE. An uncontrolled pilot feasibility trial of an intuitive eating intervention for college women with disordered eating delivered through group and guided self‐help modalities. International Journal of Eating Disorders 2020;53:1405–17. [DOI] [PubMed] [Google Scholar]
- [5].Van Dyke N, Drinkwater EJ. Relationships between intuitive eating and health indicators: Literature review. Public Health Nutrition 2014;17:1757–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Quansah DY, Gilbert L, Gross J, et al. Intuitive eating is associated with improved health indicators at 1-year postpartum in women with gestational diabetes mellitus. Journal of Health Psychology 2019:135910531986981. [DOI] [PubMed] [Google Scholar]
- [7].Birch LL, Fisher JO. Mothers’ child-feeding practices influence daughters’ eating and weight. The American Journal of Clinical Nutrition 2000;71:1054–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Berge JM, Miller J, Veblen-Mortenson S, et al. A bidirectional analysis of feeding practices and eating behaviors in parent/child dyads from low-income and minority households. The Journal of Pediatrics 2020;221:93–98.e20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Grammer AC, Balantekin KN, Barch DM, et al. Parent-Child influences on child eating self-regulation and weight in early childhood: A systematic review. Appetite 2022;168:105733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Harris H, Mallan KM, Nambiar S, et al. The relationship between controlling feeding practices and boys’ and girls’ eating in the absence of hunger. Eating Behaviors 2014;15:519–22. [DOI] [PubMed] [Google Scholar]
- [11].Farrow CV, Haycraft E, Blissett JM. Teaching our children when to eat: how parental feeding practices inform the development of emotional eating—a longitudinal experimental design. The American Journal of Clinical Nutrition 2015;101:908–13. [DOI] [PubMed] [Google Scholar]
- [12].Derks IPM, Bolhuis K, Sijbrands EJG, et al. Predictors and patterns of eating behaviors across childhood: Results from The Generation R study. Appetite 2019;141:104295. [DOI] [PubMed] [Google Scholar]
- [13].Galindo L, Power TG, Beck AD, et al. Predicting preschool children’s eating in the absence of hunger from maternal pressure to eat: A longitudinal study of low-income, Latina mothers. Appetite 2018;120:281–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Boots SB, Tiggemann M, Corsini N. Eating in the absence of hunger in young children: The role of maternal feeding strategies. Appetite 2018;130:45–9. [DOI] [PubMed] [Google Scholar]
- [15].Balantekin KN, Birch LL, Savage JS. Eating in the absence of hunger during childhood predicts self-reported binge eating in adolescence. Eating Behaviors 2017;24:7–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Kärkkäinen U, Mustelin L, Raevuori A, et al. Do disordered eating behaviours have longterm health-related consequences? European Eating Disorders Review 2018;26:22–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Khalsa AS, Woo JG, Kharofa RY, et al. Parental intuitive eating behaviors and their association with infant feeding styles among low-income families. Eating Behaviors 2019;32:78–84. [DOI] [PubMed] [Google Scholar]
- [18].Tylka TL, Lumeng JC, Eneli IU. Maternal intuitive eating as a moderator of the association between concern about child weight and restrictive child feeding. Appetite 2015;95:158–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Ellis JM, Galloway AT, Webb RM, et al. Recollections of pressure to eat during childhood, but not picky eating, predict young adult eating behavior. Appetite 2016;97:58–63. [DOI] [PubMed] [Google Scholar]
- [20].Liu Y, Cui T, Barnhart WR, et al. Associations among retrospective parenting styles, retrospective food parenting, and current eating behaviors in Chinese adults. Appetite 2023;184:106512. [DOI] [PubMed] [Google Scholar]
- [21].Coughlin SS. Recall bias in epidemiologic studies. Journal of Clinical Epidemiology 1990;43:87–91. [DOI] [PubMed] [Google Scholar]
- [22].Sawyer SM, Afifi RA, Bearinger LH, et al. Adolescence: a foundation for future health. The Lancet 2012;379:1630–40. [DOI] [PubMed] [Google Scholar]
- [23].Loth KA, MacLehose RF, Fulkerson JA, et al. Food-related parenting practices and adolescent weight status: A population-based study. Pediatrics 2013;131:e1443–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].May AL, Donohue M, Scanlon KS, et al. Child-feeding strategies are associated with maternal concern about children becoming overweight, but not children’s weight status. Journal of the American Dietetic Association 2007;107:1167–74. [DOI] [PubMed] [Google Scholar]
- [25].Neumark-Sztainer DR, Wall M, Fulkerson JA, et al. Changes in the frequency of family meals from 1999 to 2010 in the homes of adolescents: Trends by sociodemographic characteristics. Journal of Adolescent Health 2013;52:201–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Neumark-Sztainer DR, MacLehose R, Loth K, et al. What’s for dinner? Types of food served at family dinner differ across parent and family characteristics. Public Health Nutrition 2014;17:145–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Seaman SR, White IR. Review of inverse probability weighting for dealing with missing data: Statistical Methods in Medical Research 2011;22:278–95. [DOI] [PubMed] [Google Scholar]
- [28].Larson N, Neumark-Sztainer DR, Story M, et al. Identifying correlates of young adults’ weight behavior: Survey development. American Journal of Health Behavior 2011;35:712–25. [PMC free article] [PubMed] [Google Scholar]
- [29].Birch LL, Fisher JO, Grimm-Thomas K, et al. Confirmatory factor analysis of the Child Feeding Questionnaire: a measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 2001;36:201–10. [DOI] [PubMed] [Google Scholar]
- [30].Kaur H, Li C, Nazir N, et al. Confirmatory factor analysis of the Child-Feeding Questionnaire among parents of adolescents. Appetite 2006;47:36–45. [DOI] [PubMed] [Google Scholar]
- [31].Campbell KJ, Crawford DA, Salmon J, et al. Associations between the home food environment and obesity-promoting eating behaviors in adolescence. Obesity 2007;15:719–30. [DOI] [PubMed] [Google Scholar]
- [32].Tylka TL. Development and psychometric evaluation of a measure of intuitive eating. Journal of Counseling Psychology 2006;53:226–40. [Google Scholar]
- [33].Tylka TL, Kroon Van Diest AM. The Intuitive Eating Scale–2: Item refinement and psychometric evaluation with college women and men. Journal of Counseling Psychology 2013;60:137–53. [DOI] [PubMed] [Google Scholar]
- [34].Neumark-Sztainer DR, Hannan PJ, Story M, et al. Family meal patterns: Associations with sociodemographic characteristics and improved dietary intake among adolescents. Journal of the American Dietetic Association 2003;103:317–22. [DOI] [PubMed] [Google Scholar]
- [35].Burnette CB, Hazzard VM, Larson N, et al. Is intuitive eating a privileged approach? Cross-sectional and longitudinal associations between food insecurity and intuitive eating. Public Health Nutrition 2023:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Burnette CB, Hazzard VM, Hahn SL, et al. Like parent, like child? Intuitive eating among emerging adults and their parents. Appetite 2022;176:106132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Birch LL, Fisher JO, Davison KK. Learning to overeat: maternal use of restrictive feeding practices promotes girls’ eating in the absence of hunger. The American Journal of Clinical Nutrition 2003;78:215–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Loth KA, MacLehose RF, Fulkerson JA, et al. Are food restriction and pressure-to-eat parenting practices associated with adolescent disordered eating behaviors? International Journal of Eating Disorders 2014;47:310–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Boyd H, Murnen SK. Thin and sexy vs. muscular and dominant: Prevalence of gendered body ideals in popular dolls and action figures. Body Image 2017;21:90–6. [DOI] [PubMed] [Google Scholar]
- [40].Darling KE, Fahrenkamp AJ, Ruzicka EB, et al. Controlling feeding practices mediate the association between food insecurity and parent-reported child BMI percentile. Children’s Health Care 2018;47:275–88. [Google Scholar]
- [41].Trofholz AC, Tate A, Keithahn H, et al. Family meal characteristics in racially/ethnically diverse and immigrant/refugee households by household food security status: A mixed methods study. Appetite 2021;157:105000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Schmitt N. Uses and abuses of coefficient alpha. Psychological Assessment 1996;8:350. [Google Scholar]
- [43].Loth KA, MacLehose RF, Fulkerson JA, et al. Eat this, not that! Parental demographic correlates of food-related parenting practices. Appetite 2013;60:140–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.