

Abstract
Background
Nurses’ and physicians’ collaboration is a precedent for patient care. This study examined attitude change and interprofessional collaboration competencies among medical and nursing students of Iran University of Medical Sciences.
Methods
This study was quantitative cross-sectional. The study tools were two questionnaires, Attitudes Toward Interprofessional Education and IPEC Interprofessional Collaborative Competencies, which were completed by 211 medical and nursing students in online or in-person forms. The collected quantitative data were analyzed by SPSS 19 software.
Results
The results showed that nurses and physicians constituted 35.5% and 64.5% of the sample. The results of the independent T-test displayed no statistically significant difference in the mean age of both groups (P = 0.054). There was a statistically significant difference in the participants’ attitudes toward interprofessional learning, and the medical group (46.68) obtained a higher mean score than the nurse group (34.92) (P = 0.001). The two groups with varying mean scores (179.34 for medical students and 131.72 for nursing students) were significantly different in their interpersonal collaboration competencies (P = 0.001). Considering Mauchly’s test, there were statistically significant differences among medical students of varying academic years in their attitudes toward interprofessional education (P < 0.001). Nursing students were also different in their attitudes toward interprofessional education based on their academic years.
Conclusion
The results of this study showed that the attitude of nursing students towards interprofessional education and interpersonal collaboration competencies should be increased in line with medical students in order to improve the quality of medical and health services.
Keywords: Interprofessional Collaboration, Interprofessional Education, Attitude Change, Interprofessional Practice, Iran University of Medical Sciences
↑What is “already known” in this topic:
As health education programs try to incorporate more interprofessional activities into their respective programs, it is important to review methods and practices that fit their individual program.
→What this article adds:
In the first years of study, students do not feel the need for training and obtaining interprofessional qualifications. But with increasing years of education and reaching the clinical course, they understand this need and consider it necessary. Because they know that providing health services is done as a team and obtaining interprofessional qualifications leads to improving the quality of service to patients. The results of this study can help promote interprofessional education at appropriate times.
Introduction
Physicians, nurses, and other caregivers have been taught separately in conventional educational systems, and many clinical units operate as independent professions despite the significance of teamwork in this domain (1-4). In its report in 1973, the World Health Organization (WHO) disclosed medical students’ lack of preparedness for working in health teams and emphasized their holistic training by underlining the further integration of healthcare employees (5). Interprofessional education promotes participatory performance and care quality (6) and guarantees the realization of the general goals of secure, desirable, society-based treatment in the healthcare system by preparing students for participatory work (7). This education has engrossed general attention as an efficient and modern approach to promoting service quality commensurate with global transformations (8). Interprofessional education develops communication skills, enhances trust among individuals, prompts discussions on patient problems, clarifies individuals’ roles, and raises the likelihood of extra and better patient care (9).
Medical students are implicitly expected to cooperate effectively as members of the healthcare team. That is why interprofessional education has been widely accepted. The attitudes of medical and nursing students influenced by various factors are pivotal predictors of successful interprofessional education aiming to develop joint actions (10). Interprofessional learning and working are inevitable in the medical domain, with various professions that pursue a common goal. Medical students’ readiness for contributing to interprofessional activities and attention to these activities in the curricula of medical and nursing courses promote interprofessional education (11). Today, the changes in the orientations of healthcare systems due to the shifts in population patterns, disease burdens, and the increasing trend of chronic diseases, along with the necessity for complex and multilateral service provision, call for transformations in the approaches to teaching health-domain learners as well (1). Yet, an international mindset about interprofessional learning and education has developed since multilateral service provision to patients needs teamwork and the participation of various health professions (12). Various studies show that interprofessional learning and education in nursing and general medicine courses alters learners’ knowledge of their roles and responsibilities for other professions and enhances teamwork and other professions’ contribution (13-15). To promote participatory approaches in healthcare systems, interprofessional education should start from the initial years of students’ training. Although this modern educational training is over 30 years old in the world, and some countries, such as New Zealand, Ireland, and English, have embarked on extensive studies on learners’ attitudes, it has not been well-recognized in the health system of Iran (16). Since learners’ attitudes are reckoned as a fundamental factor in accepting, implementing, and succeeding in a program, the present research examined medical and nursing students’ attitude change and preparedness for interprofessional practices at the Iran University of Medical Sciences.
Methods
Research Design and Setting
The present quantitative cross-sectional study was applied in terms of its purpose and descriptive survey given its methodology.
Study population
The statistical population consisted of 1382 medical (66%) and nursing (34%) students in the 2021-2022 academic year. Based on Cochran’s formula, 286 students were selected as samples, among whom 211 students filled out the questionnaires.
Ethical considerations
All ethical considerations, such as receiving the ethics code, acquiring samples’ informed consent, and participants’ data confidentiality, were observed.
After the approval of the ethics committee of the university and the acquisition of the participants’ informed consent, the researchers distributed two questionnaires, including Attitudes Toward Interprofessional Education and IPEC Interprofessional Collaborative Competencies among medical and nursing students, in online or in-person forms.
Statistical analysis
The collected quantitative data were analyzed by SPSS 19 software. Dow, Diaz-Granados, Mazmanian, and Retchin designed the IPEC interprofessional collaboration competencies questionnaire at Virginia University to measure collaborative competencies in healthcare programs through students’ self-assessment and confirmed its validity and reliability using 481 students of various medical disciplines. Four components of IPEC interprofessional collaboration competencies include 1) values and ethics, 2) roles and responsibilities, 3) interprofessional communication, and 4) teamwork and team-based care. This scale consists of 42 items scored based on a five-point Likert scale, ranging from strongly disagree (1) to strongly agree (17). Every component encompasses eight to twelve questions, and the Cronbach alpha of all four domains has been reported at >0.90. The researchers of the present study analyzed the psychometrics of this questionnaire based on several indices and reported its acceptable validity and reliability. This instrument evaluates interprofessional collaboration competencies among nursing and medical students in four domains. Its reliability calculated by Cronbach alpha equaled 0.84, the intraclass correlation coefficient was equal to 0.82, and CVR was estimated at 0.76. Likewise, no items were omitted. The CVI evaluation led to no item removal, and only four cases needed modification. The final CVI of the questionnaire equaled 0.87.
Curran, Sharpe, and Forristall designed and examined the validity and reliability of the Attitudes Toward Interprofessional Education tool based on a five-point Likert scale (from strongly disagree (1) to strongly agree (5), ) in the faculty of medicine, nursing, pharmacology, and social work at Memorial University of Newfoundland in Canada. Besides its total rate, this instrument is also scored in three subscales of collaboration and teamwork, professional identity, and roles and responsibilities), with Cronbach alpha values of 0.88, 0.92, and 0.81 (18). Sohrabi et al. (2018) probed the validity and reliability of this scale in Iran and estimated its content validity and validity ratio at >0.62 and >0.70 for 12 items, all of which were maintained based on confirmatory factor analysis. Yet, five items were revised concerning the tool’s face validity, and two factors were named interaction-oriented interprofessional education and interprofessional education (professional adaptation). In healthcare, the test-retest reliability estimated by the Spearman Correlation coefficient and internal consistency computed by Cronbach alpha equaled 0.92 and 0.86 for the total questionnaire, and the Cronbach alpha coefficient was equal to 0.84 and 0.75 for the first and second factors (19).
Confounding variables & Random Error: No study is exempt from regular error (bias), and there is a possibility of this type of error occurring at different stages of the research project.
Ways to reduce random errors
-Increasing the sample size in both groups of medical and nursing students
-Using tools with high reliability and validity
-Determination of p-value
-Randomization
-Matching (In this method, an attempt was made to select subjects for the study in such a way that their distribution in terms of the intervening variables such as awareness of interprofessional competence, moderating variables such as age, sex, marital status, and residence; mediating variables such as academic years be the same in different exposure groups in the studying different exposure groups is the same in the study).
Results
Out of 286 distributed questionnaires, 211 (75 for nursing and 136 for medical students) were filled out, i.e., the return rate of the responses was 0.74.
Table 1 shows the gender distribution of the samples, 35.5% and 64.5% of whom are nursing and medical students. Likewise, males and females constitute 32% and 68% of the nurse group and 48% and 52% of the medical group (Table 1). Table 1 displays the residence status of the samples in both nursing and medical groups. As shown, 73% of the nursing and 50% of the medical students reside in dormitories, 20 of the nursing and 27% of the medical students live in private properties, and 7% of the nursing and 29% of the medical students stay in rentals. The results of the chi-squared test reveal that both examined groups are not significantly different in their residence status (P = 0.586). Table 1 represents the marital status of the samples and shows that 93% of the nursing and 89% of the medical group are single, and 7% of the nursing and 11% of the medical group are married. Table 1 displays a statistically significant difference between the two groups in their attitudes toward interprofessional learning (P = 0.001) (Table 1).
Table 1. Gender distribution among 211 samples; Distribution of samples’ place and marital of residence.
| Group Gender |
Nursing | Medical | ||||
|---|---|---|---|---|---|---|
| Frequency (%) | Frequency (%) | |||||
| Male | 24 (0.32) | 65 (0.48) | ||||
| Female | 51 (0.68) | 71 (0.52) | ||||
| Sum | 75 (35.5) | 136 (64.5) | ||||
| P-value = 0.001 | ||||||
| Group Residence |
Nursing | Medical | ||||
| Frequency | % | Frequency | % | |||
| Dormitory | 55 | 0.73 | 68 | 0.50 | ||
| Private | 15 | 0.20 | 39 | 0.27 | ||
| Rental | 5 | 0.7 | 29 | 0.23 | ||
| Sum | 75 | 0.100 | 136 | 0.100 | ||
| Chi-squared results | χ2 = 0.0251; df = 209; P = 0.586 | |||||
| Group Marital status |
Nursing | Medical | ||||
| Frequency (%) | Frequency (%) | |||||
| Single | 70 (0.93) | 121 (0.89) | ||||
| Married | 5 (0.7) | 15 (0.11) | ||||
| Sum | 75 (35.5) | 136 (64.5) | ||||
| Chi-squared results | χ2 = 0.0181; df = 207 P = 0.001 | |||||
Table 2 shows that According to the age-related data in Table 1, the majority of the samples are almost twenty-two years old. The results of the independent T-test display that both groups are not significantly different in their mean age (P = 0.054). The mean scores of the medical and nursing groups equal 46.68 and 34.92, respectively, and the medical group enjoys a better mean score than the nursing group (Table 2 ).
Table 2. Age mean and SD; and Mean attitudes of nursing and medical students toward interprofessional learning.
| Group | Nursing | Medical | ||||
|---|---|---|---|---|---|---|
| Mean & SD | Mean & SD | |||||
| Age | 21.74 ± 3.52 | 22.98 ± 2.73 | ||||
| Independent T-test results | t = 1.816; df = 209; P = 0.054 | |||||
| Variable | Mean | SD | Mean difference | P-value | ||
| Attitudes toward interprofessional learning | Medical | 46.68 | 4.28 | 11.76 | 0.001 | |
| Nursing | 34.92 | 5.62 | ||||
Table 3 shows that There is a statistically significant difference between the two groups(Comparing two groups’ attitudes toward components of interprofessional learning( (Table 3).
Table 3. Comparing two groups’ attitudes toward components of interprofessional learning.
| Component | Major | Mean & SD | P-value |
|---|---|---|---|
| Collaboration and teamwork | Medical | 16.09 ± 4.39 | 0.027 |
| Nursing | 12.19 ± 5.09 | ||
| Professional identity | Medical | 15.21 ± 3.28 | 0.116 |
| Nursing | 12.62 ± 3.74 | ||
| Roles and responsibilities | Medical | 15.77 ± 2.83 | 0.324 |
| Nursing | 11.93 ± 2.50 |
Table 4 shows that the two groups, with varying means, are significantly different in their interprofessional collaboration competencies ( P = 0.001). The mean score of the medical group is 179.34, and the mean score of the nursing group is 131.72. In addition, there are statistically significant differences between the groups concerning the components of interprofessional collaboration competencies (P = 0.000).
Table 4. Determining and comparing medical and nursing students’ attitudes toward interprofessional competencies and interprofessional education.
| Variable | Mean | SD | Mean difference | T | P-value | |
|---|---|---|---|---|---|---|
| Interprofessional collaboration competencies | Medical | 179.34 | 6.82 | 47.62 | 8.37 | 0.001 |
| Nursing | 131.72 | 7.63 | ||||
| Values and ethics | Medical | 34.12 | 3.16 | 5.61 | 9.15 | 0.000 |
| Nursing | 28.51 | 3.22 | ||||
| 12 roles and responsibilities | Medical | 51.14 | 3.08 | 11.88 | 10.06 | 0.001 |
| Nursing | 39.26 | 3.20 | ||||
| 12 interprofessional communication | Medical | 52.29 | 2.96 | 11.91 | 9.36 | 0.000 |
| Nursing | 40.38 | 3.28 | ||||
| 10 teamwork and team-based care | Medical | 43.71 | 2.22 | 6.61 | 9.18 | 0.000 |
| Nursing | 37.10 | 2.58 | ||||
The repeated measures ANOVA was used for the one-way intragroup analysis of variance (four measured times). Box’s M test shows that the assumption associated with the homogeneity of covariance matrices is not accepted (P < 0.0000). Also, Wilk’s Lambda test displays that time is an influential factor in the dependent variable (F = 7.114; P = 0.009). Mauchly’s test of sphericity shows that the covariance of the residuals of the dependent variable is not equal, and the assumption of the homogeneity of variances is not confirmed. For this reason, the Greenhouse-Geisser test is used to interpret the results. The repeated measures ANOVA results based on the Greenhouse-Geisser test for the dependent variables, i.e., interprofessional collaboration competencies and attitudes toward interprofessional training, at four measured times reveal significant over-time variations (Mauchly’s W = 0.0624; P = 0.001) (Table 4 ).
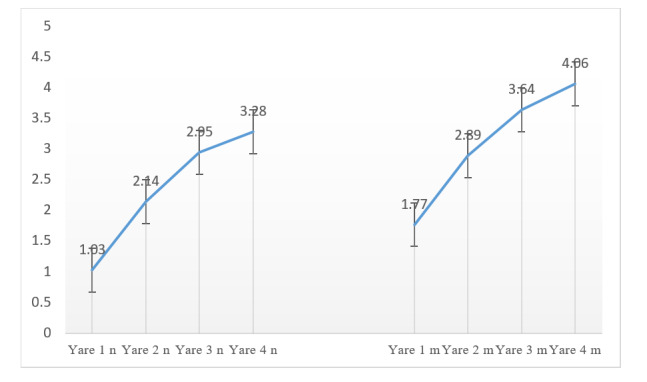
According to the repeated measures of ANOVA and Mauchly’s tests, the medical students of different academic years were significantly different in their attitudes toward interprofessional education (P < 0.001). Nursing students were also different in their attitudes toward interprofessional education based on their academic years (P < 0.003). Considering the medical students’ attitudes toward interprofessional education, we can assert that 72.4% of the variance associated with the dependent variable (attitudes toward interprofessional education) results from the impact of the academic year (η2 = 0.724). This value also equals 0.541 for the nursing students. In other words, 54.1% of the variance in the nursing students’ attitudes toward interprofessional education is tied to the academic year (η2 = 0.541). That is to say, both groups’ attitudes toward interprofessional education extensively change as they proceed in their academic years (Table 5).
Table 5. Repeated ANOVA test comparing variations in interprofessional education between two groups .
| Variable | Sum of squares | Mean of squares | F statistic | df | p-value | Eta-squared (η2) | |
|---|---|---|---|---|---|---|---|
| Variations in attitudes toward interprofessional education | Medical | 3415.240 | 2833.174 | 254.196 | 1 | 0.000 | 0.724 |
| Nursing | 0.329 | 0.181 | 0.408 | 1 | 0.003 | 0.541 | |
Figure 1 shows the changes in the attitude of medical and nursing students towards interprofessional education(Figure 1).
Figure 1.
Variations in medical and nursing students’ attitudes toward interprofessional education
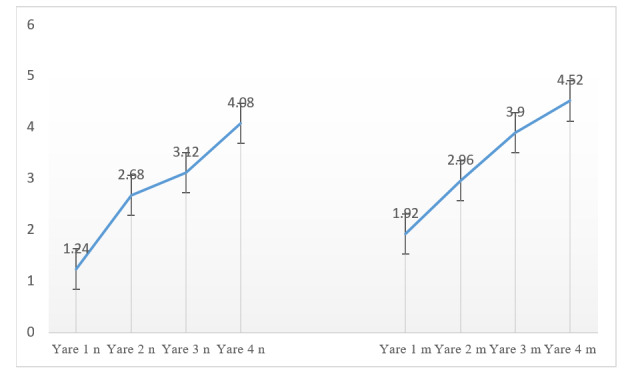
According to the repeated measures of ANOVA and Mauchly’s tests, the medical students of different academic years were significantly different in their interprofessional collaboration competencies (P < 0.001). Nursing students were also different in their interprofessional collaboration competencies based on their academic years (P < 0.003). Considering the medical students’ interprofessional collaboration competencies, we can assert that 81.2 of the variance associated with the dependent variable (interprofessional collaboration competencies) results from the impact of the academic year (η2 = 0.812). This value also equals 65.5% for nursing students. In other words, 65.5% of the variance in the nursing students’ interprofessional collaboration competencies is tied to the academic year (η2 = 0.655). That is to say, both groups’ interprofessional collaboration competencies enhance as they proceed in their academic years (Table 6).
Table 6. Repeated measures ANOVA test comparing variations in interprofessional collaboration competencies between two groups.
| Variable | Sum of squares | Mean of squares | F statistic | df | p-value | Eta-squared | |
|---|---|---|---|---|---|---|---|
| Variations in interprofessional collaboration competencies | Medical | 2760.553 | 3219.537 | 322.168 | 134 | 0.001 | 0.812 |
| Nursing | 0.415 | 0.246 | 0.386 | 74 | 0.001 | 0.655 | |
Figure 2 shows the changes in the Variations in medical and nursing students’ interprofessional collaboration competencies (Figure 2).
Figure 2.
Variations in medical and Nursing Students’ interprofessional collaboration competencies
Discussion
Many studies have referred to the significance of interprofessional competencies. Fox et al. (2018), in a scoping review, examined texts associated with interprofessional collaboration and education and found that to train healthcare professionals ready to undertake pivotal roles, practitioners should teach teamwork to students of various medical professions from the beginning years. This systematic review aimed to discover interprofessional education studies designed for teaching or evaluating teamwork skills of students of two or more health professions and find and describe influential strategies in education and assessment. It seemed that many learning activities through which interprofessional teams interact positively altered students’ perceptions and attitudes toward interprofessional education and interprofessional competency implementation. Since health training programs attempt to incorporate more interprofessional activities into their curricula, they must revisit approaches and steps that fit their individual plans. This quest highlighted the standardization of method and result reporting for those tending to employ the examined methods in their curricula (20). Interprofessional education is an educational approach emphasized in various texts and presumably can enhance interprofessional collaboration and improve care quality. Healthcare professions, including doctors, nurses, paramedics, and other positions, conventionally operate as separate professions and units despite the significance of teamwork in healthcare. Indeed, the members of these teams are rarely trained together. Besides, they study various disciplines with different educational programs and can hardly be involved in teamwork. One of the drawbacks of teamwork can lie in members’ poor perceptions of other professions. However, it has been found that teamwork is crucial for patient safety, especially when team members are well aware of their responsibilities and, consequently, make fewer mistakes. We can claim that patient care is inherently teamwork and increasingly calls for enhanced relationships among the members of the healthcare team. On the other hand, interprofessional collaboration has been introduced as an effective educational principle, such that numerous researchers have foregrounded the significance of group work and interprofessional collaboration among care providers. Hence, there must be an educational strategy to enhance team performance among healthcare personnel.
Al-Maleki et al. (2021) evaluated the attitudes and professional readiness of students and faculties at Taef University using the Readiness for Interprofessional Learning Scale (RIPLS) and believed that this parameter could improve medical education at universities. They also found no statistically significant difference between the examined groups in their interprofessional readiness (21).
In a qualitative study, Castel et al. (2018) investigated attitudes toward an interprofessional simulation experience among nursing, physical therapy, nutrition, and social work students. In this respect, they followed an exploratory case study and used open-interview questions to collect data on users’ perceptions of this experience. Based on the content analysis of the open interviews with 100 students of various professions, they extracted three themes, including higher perceptions of others’ roles, raised trust and ability to improve care consequences, and increased appreciation of the interprofessional simulation as a valuable learning experience. The participants felt comfortable working in teams, and this fostered their trust in their roles, which was a significant finding. Trusting in one’s role in strengthening teamwork tendencies is a robust force for changing the interactional approaches of professions. Interprofessional simulation is an educational strategy that promises teamwork among healthcare professionals (22).
Conclusion
The results of this study showed statistically significant differences in nursing and medical students’ attitudes toward interprofessional learning, and the medical group enjoyed a higher mean score than the nursing group. Likewise, the two groups, with varying means, were significantly different in their interprofessional collaboration competencies and attitudes toward interprofessional education. Statistically significant differences were also observed among the medical and nursing students, considering their attitudes toward interprofessional education and interprofessional collaboration based on the academic year ( P < 0.001). That is to say, both groups radically changed their attitudes toward interprofessional education and boosted their interprofessional collaboration competencies as they proceeded in their academic years. However, medical students enjoyed higher mean scores in interprofessional collaboration competencies and attitudes toward interprofessional education than their nursing peers.
The results illuminated that students do not feel the need to learn interprofessional competencies in their initial academic years. However, as they proceed in their academic years and study clinical courses, they perceive its significance, knowing that healthcare provision is a teamwork, and interprofessional competencies promote service quality. This study collected data by distributing questionnaires among medical and nursing students. By investigating students’ attitude change, the researchers concluded that interprofessional education should be a component of the education system of the healthcare team during their internships in hospitals, just as students were positively oriented to interprofessional competencies and education.
Interprofessional education is one of the educational approaches emphasized in various texts and presumably can enhance interprofessional collaboration and improve care quality. Healthcare professions, including doctors, nurses, paramedics, and other positions, conventionally operate as a set of separate professions and units despite the significance of teamwork in healthcare.
The results of this study can raise nursing and medical departments’ and faculties’ awareness of students’ attitudes toward interprofessional education and their interprofessional collaboration competencies and help promote interprofessional education at appropriate times.
Conflict of Interests
The authors declare that they have no competing interests.
Funding
This study was supported by Iran University of Medical Sciences and Center of Educational Research in Medical Science (CERMS), research fund (2022) and 21101 ID code.
Acknowledgment
The authors would like to express their deep gratitude to all the participants in this research project.
Authors Contributions
Study concept and design, D.R & G.R; Analysis and interpretation of data, A. N & G.R; Drafting of the manuscript, A.H; & L.N.S, Critical revision of the manuscript for important intellectual content, D.R and G.R.
Ethical approval
The present paper is the outcome of a research project in the Medical Science Education Research Center at the Iran University of Medical Sciences with the 21101 ID code and IR.IUMS.REC.1400.1055 ethics code.
Cite this article as : Rasouli D, Norouzi A, Ramezani G, Hashemi A, Neisani Samani L. Attitude Change and Interprofessional Collaboration Competencies among Medical and Nursing Students of Iran University of Medical Sciences. Med J Islam Repub Iran. 2023 (19 Nov);37:124. https://doi.org/10.47176/mjiri.37.124
References
- 1.Bondevik GT, Holst L, Haugland M, Baerheim A, Raaheim A. Interprofessional workplace learning in primary care: Students from different health professions work in teams in real-life settings. Int J Teach Learn High Educ. 2015;27(2):175–182. [Google Scholar]
- 2.Allen M, Macleod T, Zwicker B, Chiarot M, Critchley C. Interprofessional education in chronic non-cancer pain. J Interprof Care. 2011;25(3):221. doi: 10.3109/13561820.2011.552134. [DOI] [PubMed] [Google Scholar]
- 3.Garrusi B, Amirkafi A, Garousi S. Assessing the Viewpoint of the Faculty Members and Graduates of Kerman University of Medical Sciences Toward Interprofessional Education and Interprofessional Teamwork. Stride Dev Med Educ. 2020;17(1) [Google Scholar]
- 4.Amini B, Bigdeli S, Shirazi M, Mirshahvalad SM. Validity and reliability of the “Readiness for Interprofessional Learning Scale (RIPLS)” in Iranian context. Payavard Salamat. 2016;10(1):51. [Google Scholar]
- 5. World Health Organization. Continuing education for physicians: report of a WHO expert committee [meeting held in Geneva from 28 June to 4 July 1973 ]: World Health Organ Tech Rep Ser. 1973: 534: 1 32 [PubMed] [Google Scholar]
- 6.Reeves S. Why we need interprofessional education to improve the delivery of safe and effective care. Interface-Comunicação Saúde Educação. 2016;20:185. [Google Scholar]
- 7.Amini S, Keshmiri F, Soltani Arabshahi, Shirazi M. Development and validation of the inter-professional collaborator communication skill core competencies. Razi J Med Sci. 2014;20(115):8–16. [Google Scholar]
- 8.Lie DA, Fung CC, Trial J, Lohenry K. A comparison of two scales for assessing health professional students’ attitude toward interprofessional learning. Med Educ Online. 2013;18(1):21885. doi: 10.3402/meo.v18i0.21885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Braithwaite J, Westbrook M, Nugus P, Greenfield D, Travaglia J, Runciman W. et al. A four-year, systems-wide intervention promoting interprofessional collaboration. BMC Health Serv Res. 2012;12(1):1–8. doi: 10.1186/1472-6963-12-99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Milutinović D, Lovrić R, Simin D. Interprofessional education and collaborative practice: Psychometric analysis of the Readiness for Interprofessional Learning Scale in undergraduate Serbian healthcare student context. Nurse Educ Today. 2018;65:74–80. doi: 10.1016/j.nedt.2018.03.002. [DOI] [PubMed] [Google Scholar]
- 11.Roberts, C. , Kumar, K. Student learning in interprofessional practice-based environments: what does theory say. 2015;15(211) doi: 10.1186/s12909-015-0492-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Krueger L, Ernstmeyer K, Kirking E. Impact of interprofessional simulation on nursing students' attitudes toward teamwork and collaboration. J Nurs Educ. 2017;56(6):321. doi: 10.3928/01484834-20170518-02. [DOI] [PubMed] [Google Scholar]
- 13.Irajpour A. Inter-Professional Education: A Reflection on Education of Health Disciplines. Iran J Med Educ. 2011;10(4) [Google Scholar]
- 14.Garousi S, Garrusi B. Viewpoints of medical and nursing students regarding Medical and nursing professions: The first step in assessment of possibility of interdisciplinary training. Stride Dev Med. 2012;9(1):25–33. [Google Scholar]
- 15.Tamura Y, Seki K, Usami M, Taku S, Bontje P, Ando H. et al. Cultural adaptation and validating a Japanese version of the readiness for interprofessional learning scale (RIPLS) J Interprof Care. 2012;26(1):56–63. doi: 10.3109/13561820.2011.595848. [DOI] [PubMed] [Google Scholar]
- 16.Jafaei DR, Karimi MH, Yamani N, Irajpoor A, Saadatyar F. Interprofessional education: the strategy to improve health care print. Res Med Educ. 2015;7(1):54–62. [Google Scholar]
- 17.Lockeman KS, Dow AW, Randell AL. Validity evidence and use of the IPEC Competency Self-Assessment, Version 3. J Interprof Care. 2021;35(1):107. doi: 10.1080/13561820.2019.1699037. [DOI] [PubMed] [Google Scholar]
- 18.Curran VR, Sharpe D, Forristall J, Flynn K. Attitudes of health sciences students towards interprofessional teamwork and education. Learn.Health Soc Care. 2008;7(3):146. [Google Scholar]
- 19.Sohrabi Z, Saeed A, Salehi L. Investigation of the Validity and Reliability of Attitude Towards Inter-Professional Education (IPE) in Health Care. Iran J Health Educ Health Promot. 2018;6(1):12–19. [Google Scholar]
- 20.Fox L, Onders R, Hermansen-Kobulnicky CJ, Nguyen TN, Myran L, Linn B. et al. Teaching interprofessional teamwork skills to health professional students: A scoping review. J Interprof Care. 2018;32(2):127. doi: 10.1080/13561820.2017.1399868. [DOI] [PubMed] [Google Scholar]
- 21.Almalki A, Park YS, Tekian A, editors. Needs assessment for interprofessional education: implications for integration and readiness for practice. Healthcare (Basel) . 2021 Apr 2;9(4):411. doi: 10.3390/healthcare9040411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Costello M, Prelack K, Faller J, Huddleston J, Adly S, Doolin J. Student experiences of interprofessional simulation: Findings from a qualitative study. J Interprof Care. 2018;32(1):95. doi: 10.1080/13561820.2017.1356810. [DOI] [PubMed] [Google Scholar]