

Abstract
Introduction:
Health centers provide primary and behavioral health care to the nation’s safety net population. Many health centers served on the frontlines of the COVID-19 pandemic, which brought major changes to health center care delivery.
Objective:
To elucidate primary care and behavioral health service delivery patterns in health centers before and during the COVID-19 public health emergency (PHE).
Methods:
We compared annual and monthly patients from 2019 to 2022 for new and established patients by visit type (primary care, behavioral health) and encounter visits by modality (in-person, telehealth) across 218 health centers in 13 states.
Results:
There were 1581,744 unique patients in the sample, most from health disparate populations. Review of primary care data over 4 years show that health centers served fewer pediatric patients over time, while retaining the capacity to provide to patients 651. Monthly data on encounters highlights that the initial shift in March/April 2020 to telehealth was not sustained and that in-person visits rose steadily after November/December 2020 to return as the predominant care delivery mode. With regards to behavioral health, health centers continued to provide care to established patients throughout the PHE, while serving fewer new patients over time. In contrast to primary care, after initial uptake of telehealth in March/April 2020, telehealth encounters remained the predominant care delivery mode through 2022.
Conclusion:
Four years of data demonstrate how COVID-19 impacted delivery of primary care and behavioral health care for patients, highlighting gaps in pediatric care delivery and trends in telehealth over time.
Keywords: COVID-19, Electronic Medical Records, Healthcare Disparities, Health Services Accessibility, Longitudinal Studies, Pandemics, Primary Health Care
Introduction
Health centers (federally qualified health centers (FQHCs), FQHC look-alikes and rural health centers) are the frontline providers of primary health care to 30 million people that are disproportionately poorer, sicker and are more socioeconomically disadvantaged than the general population.1 More than 97% of health centers also provide behavioral health care services onsite to address unmet mental health and substance abuse needs in the communities they serve.2 During the COVID-19 pandemic, health centers rapidly mobilized to serve as frontline centers for testing and vaccinations within their communities.3 They were also quick adopters of telehealth, quickly transitioning patients to telemedicine.4,5 However, there is limited understanding of how such shifts and disruptions in care affected the ongoing ability of health centers, who faced unprecedented workforce challenges, to deliver primary and behavioral health care services over time.6 Using a large network of 218 health centers that share a common electronic health record, we evaluated the number of patients and encounters for primary care, behavioral health, and COVID tests and/or vaccines before and during the COVID-19 public health emergency over 4 years (2019 to 2022). We also evaluated the immediate and sustained shift to telehealth.
Methods
We used electronic health record (EHR) data from the OCHIN (not an acronym) multistate network of community-based clinics. OCHIN is a nonprofit health care innovation center that offers a fully hosted, highly customized instance of Epic practice management and EHR solutions to more than 1300 care delivery sites across the US. Our study sample included all FQHCs, health center look-alikes, and rural health centers within the OCHIN network that were active in the OCHIN EHR as of January 1, 2019, and provide primary care as evidenced by having at least 1 primary care provider and conducting ≥2000 evaluation and management (E&M) encounter visits for at least 500 unique primary care patients in 2019. We identified primary care providers using the primary and secondary taxonomy classifications using their National Provider Identifier (NPI) (Supplemental Material). Our definition of primary care provider loosely follows the ACA guidelines,7 which includes physicians with a primary specialty designation of family medicine, internal medicine, geriatric medicine, or pediatric medicine; and nurse practitioners, clinical nurse specialists, and physician assistants. After further investigation by the study team, it was determined that medical residents, naturopaths, and midwives also conducted encounters with an E&M billing code, and thus, these taxonomies were also included in our definition of a primary care provider. Primary care patients were identified if they had at least 1 E&M visit with a primary care provider. Behavioral health providers included all providers within an NPI grouping of “Behavioral Health and Social Service Providers,” or providers with NPI classifications and specializations indicating behavioral health, including psychiatrists, psychologists, counselors, licensed clinical social workers, marriage and family therapists, and behavioral analysts; and occupational therapists, nurse practitioners, clinical nurse specialists, or registered nurses with a specialization in psychiatry/mental health/addiction.
All in-person and telehealth primary care and behavioral health encounters that occurred at the eligible health centers were included. In addition, COVID tests and vaccines that occurred outside of a primary care or behavioral health encounter at the eligible health centers were included. Encounters were grouped into 3 mutually exclusive categories based on the service type: primary care, behavioral health, or COVID test/vaccine. Primary care was defined as all visits with an E&M billing code completed by a primary care provider. Behavioral health was defined as all visits with a behavioral health billing code or completed by a behavioral health provider. COVID tests were identified from LOINC codes, and COVID vaccines were identified from immunization names (Supplemental material). COVID tests and vaccines encompass those encounters where only a COVID test or vaccine was provided, and no other services were delivered. Patients who received a COVID vaccine or test as part of a primary care visit were counted as primary care patients and the encounter was considered a primary care visit. The number of visits by service type (primary care, behavioral health, COVID test/vaccine) were computed monthly from January 2019 to December 2022.
The number of patients with an encounter in each service type was computed monthly by service type. A patient could be included as a patient of multiple service types if they had an encounter for different services in a given month. New patients each month were determined for primary care and behavioral health. Patients were considered new to the service type at the time of a visit if they had no visit history within the service type at any delivery site in the OCHIN network within 36 months of their visit. For example, a patient who came into a health center for the first time in April 2020 for a behavioral health visit would be counted as a new behavioral health patient in April 2020. If the patient continued to receive behavioral health care within 36 months, they would be considered an established behavioral health patient at those later encounters. However, the patient would be considered a new primary care patient if they came for the first time for a primary care visit in March 2021, and they would be considered an established primary care patient if they came for a subsequent primary care visit in January 2022. We also stratified data monthly by age-group at the time of the visit (≤17, 18–44, 45–64, and ≥65). We additionally computed the number of visits that were delivered in-person and via telehealth. Data were also computed by quarter (see Appendix).
Results
Between January 2019 and December 2022, 218 health centers saw a total of 1,581,744 unique patients for primary care, behavioral health, or COVID-19 vaccines/tests. The 218 clinics were in 13 states of which 123 were in West, 57 were in Midwest, 22 were in New England, 13 in South and 3 were in Southwest regions. Demographic characteristics of all patients seen in the 218 clinics are presented in Table 1. Patients are largely from populations who experience health disparities. In 2022, the population included 19.5% black, 35.7% Hispanic, 66.2% public insurance, 16.7% uninsured and 78.3% under 138% of the federal poverty level.
Table 1.
Demographic Characteristics of 1,581,744 Patients Receiving Care in 218 Health Centers from 2019–2022
| 2019 | 2020 | 2021 | 2022 | |||||
|---|---|---|---|---|---|---|---|---|
| N | (%) | N | (%) | N | (%) | N | (%) | |
| Patients, All services | 838,075 | 825,112 | 905,923 | 819,043 | ||||
| Encounters, All services | 3,868,353 | 3,817,819 | 3,906,244 | 3,825,283 | ||||
| Sex | ||||||||
| Female | 470,744 | (56.2) | 462,181 | (56.0) | 502,504 | (55.5) | 459,767 | (56.1) |
| Male | 366,953 | (43.8) | 362,419 | (43.9) | 402,733 | (44.5) | 358,557 | (43.8) |
| Unknown/Other | 378 | (0.0) | 512 | (0.1) | 686 | (0.1) | 719 | (0.1) |
| Age | ||||||||
| 0 to 17 | 209,721 | (25.0) | 174,868 | (21.2) | 193,222 | (21.3) | 187,144 | (22.8) |
| 18 to 44 | 313,399 | (37.4) | 323,704 | (39.2) | 350,800 | (38.7) | 304,141 | (37.1) |
| 45 to 64 | 226,144 | (27.0) | 231,363 | (28.0) | 249,048 | (27.5) | 222,779 | (27.2) |
| 65+ | 88,805 | (10.6) | 95,170 | (11.5) | 112,846 | (12.5) | 104,967 | (12.8) |
| Race | ||||||||
| White | 523,755 | (62.5) | 507,530 | (61.5) | 554,015 | (61.2) | 493,700 | (60.3) |
| Black | 168,786 | (20.1) | 166,937 | (20.2) | 177,684 | (19.6) | 159,314 | (19.5) |
| Unknown | 82,946 | (9.9) | 89,557 | (10.9) | 105,751 | (11.7) | 100,402 | (12.3) |
| Asian | 38,868 | (4.6) | 37,652 | (4.6) | 43,045 | (4.8) | 41,546 | (5.1) |
| Multiple | 10,033 | (1.2) | 9996 | (1.2) | 11,077 | (1.2) | 10,560 | (1.3) |
| American Indian/Alaska Native | 8316 | (1.0) | 8051 | (1.0) | 8616 | (1.0) | 8158 | (1.0) |
| Native Hawaiian/Other Pacific Islander | 5371 | (0.6) | 5389 | (0.7) | 5735 | (0.6) | 5363 | (0.7) |
| Ethnicity | ||||||||
| Hispanic | 302,186 | (36.1) | 284,298 | (34.5) | 318,220 | (35.1) | 292,440 | (35.7) |
| Not Hispanic | 498,404 | (59.5) | 496,488 | (60.2) | 533,602 | (58.9) | 474,865 | (58.0) |
| Unknown | 37,485 | (4.5) | 44,326 | (5.4) | 54,101 | (6.0) | 51,738 | (6.3) |
| Insurance | ||||||||
| Medicaid | 438,356 | (52.3) | 414,425 | (50.2) | 456,591 | (50.4) | 435,187 | (53.1) |
| Medicare | 108,239 | (12.9) | 110,308 | (13.4) | 113,707 | (12.6) | 97,148 | (11.9) |
| Other Public | 13,402 | (1.6) | 10,611 | (1.3) | 10,798 | (1.2) | 9751 | (1.2) |
| Private | 137,744 | (16.4) | 152,020 | (18.4) | 172,343 | (19.0) | 140,099 | (17.1) |
| Uninsured | 140,328 | (16.7) | 137,627 | (16.7) | 151,736 | (16.7) | 136,714 | (16.7) |
| No Information | 6 | (0.0) | 121 | (0.0) | 748 | (0.1) | 144 | (0.0) |
| Hypertension | 198,400 | (23.7) | 193,740 | (23.5) | 198,303 | (21.9) | 181,611 | (22.2) |
| Diabetes | 104,376 | (12.5) | 102,716 | (12.4) | 104,928 | (11.6) | 97,155 | (11.9) |
| Primary Non-English Speaker | 261,570 | (31.2) | 243,192 | (29.5) | 278,347 | (30.7) | 265,786 | (32.5) |
| Federal Poverty Level | ||||||||
| >138% | 172,915 | (20.6) | 170,329 | (20.6) | 195,329 | (21.6) | 177,855 | (21.7) |
| <138% | 665,160 | (79.4) | 654,783 | (79.4) | 710,594 | (78.4) | 641,188 | (78.3) |
Abbreviation: PI, Pacific Islander.
The total number of patients receiving care across study health centers decreased between 2019 (n = 838,075) to 2020 (n = 825,112) and then increased in 2021 (n = 905,923) largely due to an increase in COVID tests and vaccines, before decreasing to the lowest level in 4 years in 2022 (n = 819,043). During the same period, encounters (for all services) followed similar trends (Table 2). The monthly number of patients who received primary care, behavioral health and COVID tests/vaccines is shown in Figure 1 When stratified by service type, the number of patients who received behavioral health care services remained largely stable, but there were obvious decreases in primary care and peaks in COVID tests/vaccines beginning at the start of the pandemic and stay at home orders in March 2020 (Figure 1). From 2020– 2022 changes in primary care and COVID-19 tests/vaccines continued with noticeable impacts on trends due to wider availability of COVID-19 tests in the community (approximately May-July 2020, with wide variation across states), community vaccination programs ramping up from February-April 2021, and subsequent jumps and lulls in testing and vaccines as the pandemic progressed throughout 2021 and 2022 (Figure 1).
Table 2.
Annual New and Established Patients and In-Person and Telehealth Encounters for Primary Care and Behavioral Health Care Provided by 218 Health Centers from 2019 to 2022
| 2019 | 2020 | 2021 | 2022 | % Change 2019 to 2022 | |
|---|---|---|---|---|---|
| Primary Care | |||||
| Patients | |||||
| Established patients1 | 228,533 | 197,415 | 185,702 | 176,057 | −23.0% |
| New patients1 | 689,640 | 647,950 | 663,862 | 653,475 | −5.2% |
| Age 0 to 17 | 211,698 | 172,379 | 179,962 | 180,462 | −14.8% |
| Age 18 to 44 | 303,479 | 295,219 | 292,094 | 277,146 | −8.7% |
| Age 45 to 64 | 222,636 | 218,821 | 215,613 | 208,901 | −6.2% |
| Age 65+ | 84,344 | 87,340 | 91,330 | 94,226 | 11.7% |
| Encounters | |||||
| In-person | 2,402,282 | 1,384,127 | 1,585,112 | 1,714,330 | −28.6% |
| Telehealth | 7991 | 921,254 | 707,214 | 473,513 | 5825.6% |
| Total encounters | 2,410,273 | 2,305,381 | 2,292,326 | 2,187,843 | −9.2% |
| Behavioral Health | |||||
| Patients | |||||
| Established patients1 | 78,740 | 81,598 | 82,618 | 78,272 | −0.6% |
| New patients1 | 60,783 | 53,568 | 52,133 | 48,762 | −19.8% |
| Age 0 to 17 | 18,206 | 14,976 | 15,320 | 15,026 | −17.5% |
| Age 18 to 44 | 50,821 | 51,103 | 52,837 | 49,661 | −2.3% |
| Age 45 to 64 | 33,799 | 33,133 | 31,549 | 29,461 | −12.8% |
| Age 65+ | 7069 | 7346 | 7692 | 7750 | 9.6% |
| Encounters | |||||
| In-person | 520,374 | 303,769 | 262,085 | 254,508 | −51.1% |
| Telehealth | 1883 | 307,738 | 360,483 | 336,769 | 17,784.7% |
| Total encounters | 522,257 | 611,507 | 622,568 | 591,277 | 13.2% |
Notes:
In a given year, a patient may be both a new and an established patient; in a given month, patients are unduplicated and are counted only as a new or existing patient. If a patient had multiple visits in a month in which they were a new patient, they would be considered a new patient at each visit.
Figure 1.
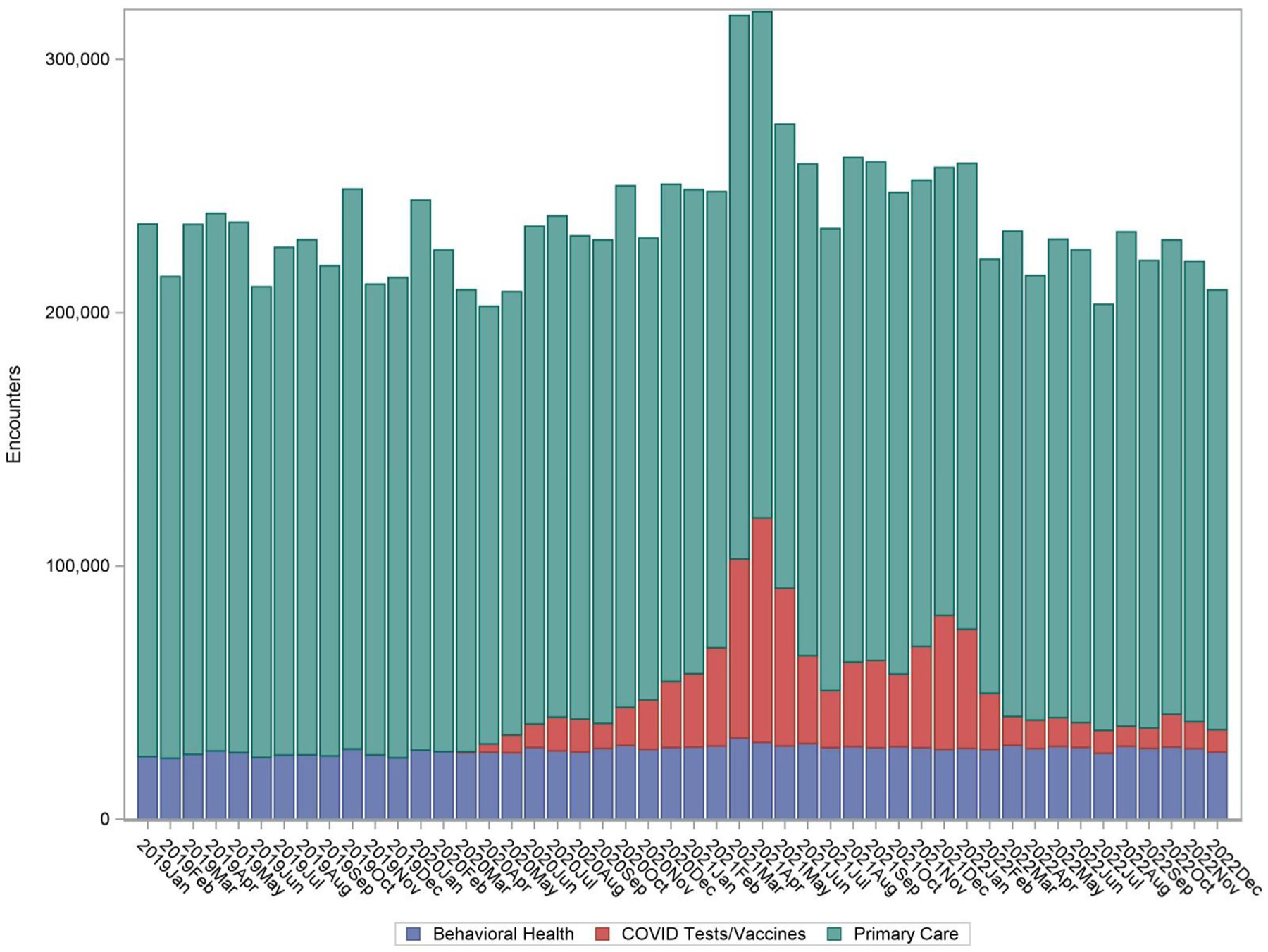
Monthly encounters for primary care, behavioral health care, and COVID tests/vaccines at 218 health centers from 2019 to 2022.
Primary Care
From 2019 to 2022, the number of established patients receiving primary care declined 23%, suggesting that some health center patients may not have received ongoing care. New patients, a measure of health center growth, declined 5.1% from 2019 to 2022. Primary care encounters declined overall 9.2% (Table 2). Monthly data shows that declines were not consistent throughout the 4 years (Figure 2). Further analysis by age-group suggests that 0 to 17, 18 to 44 and 45 to 64 age groups all experienced some declines over the 4 years (Figure 3). Age groups 18 to 44 and 45 to 64 had peaks in patients seen in Jan to April 2021, and then continued declining through 2022. By age-group, pediatric patients (new and established) experienced the greatest decrease over the 4 years, whereas patients 65+ increased. Despite some peaks in June to September 2021 and 2022, pediatric patients (0 to 17) remained lower than prepandemic levels. Conversely, the number of older primary care patients (65+) remained generally stable, with some slight increases over the 4 years. The largest decrease corresponded to stay-at-home orders in March 2020. In examining visits by care delivery modality (Figure 4), telehealth encounters increased rapidly in March/April 2020 – a finding that is consistent with stay-at-home orders. Telehealth encounters had additional peaks in December 2020/January 2021 and a slight peak in December 2022, but consistently declined over time as in-person visits rose back to the predominant care delivery mode in November/December 2020.
Figure 2.
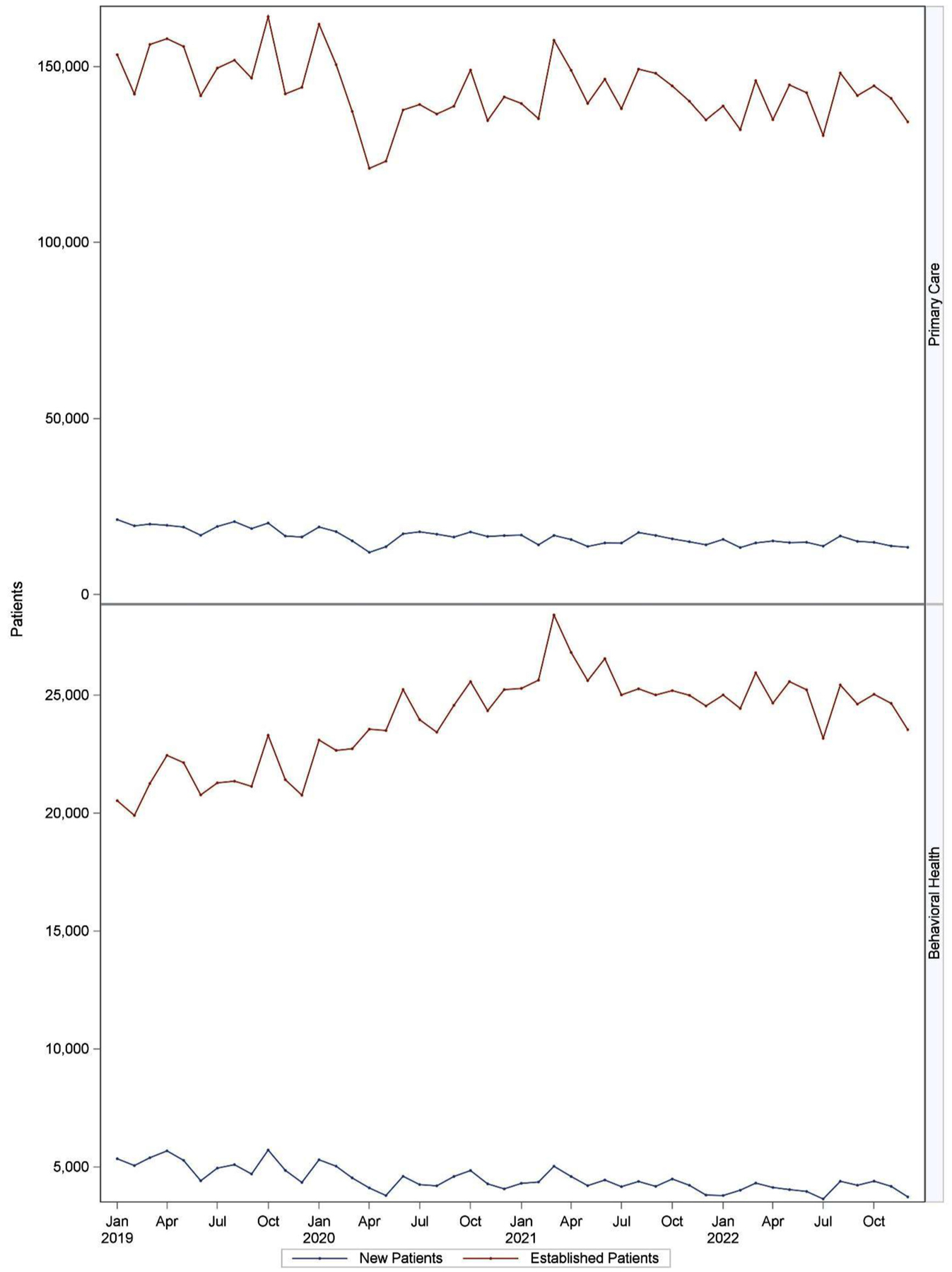
Monthly number of new and established patients with a visit for primary care and behavioral health.
Figure 3.
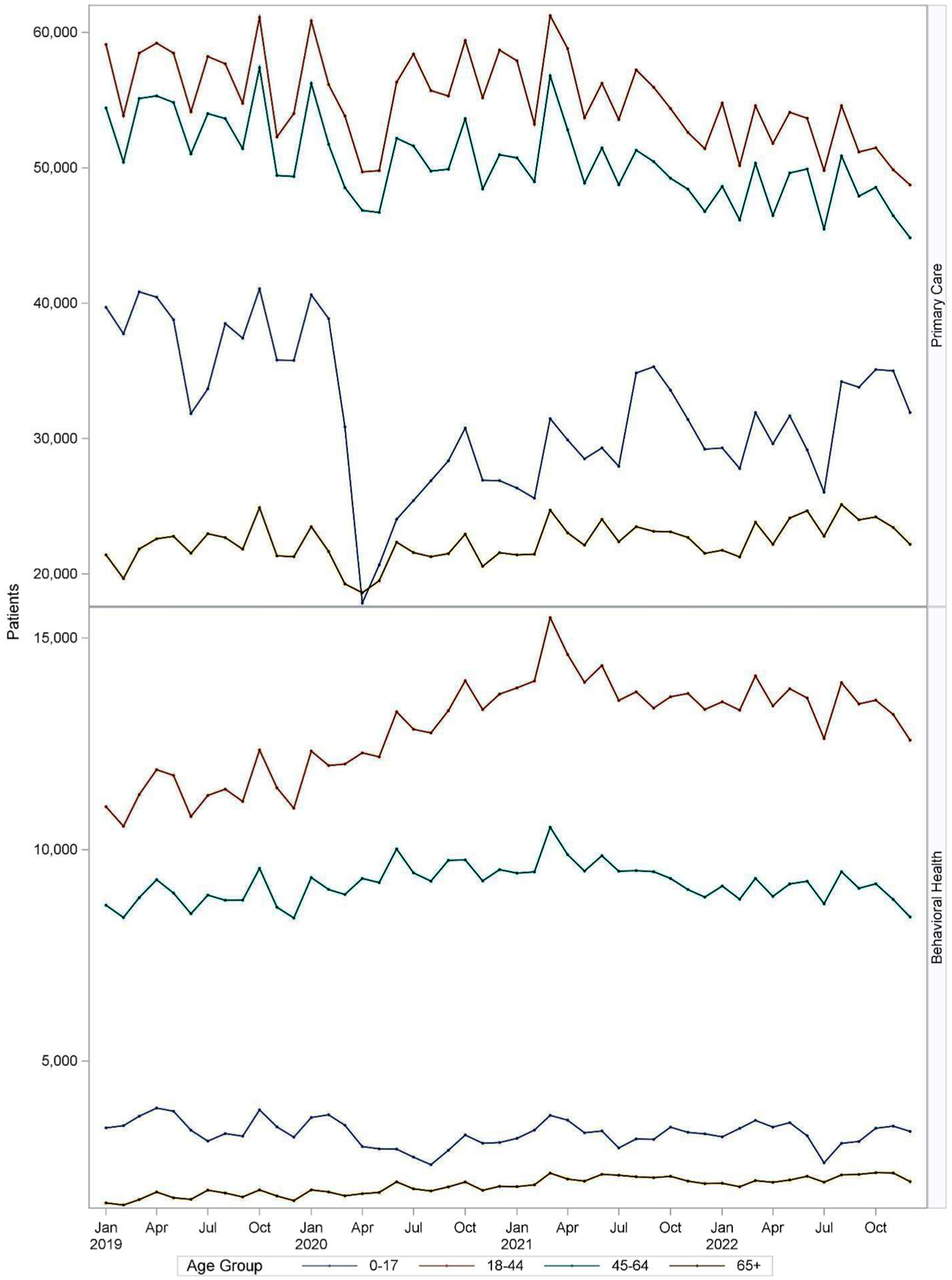
Monthly number of patients with a visit for primary care or behavioral health by age group at 218 health centers from 2019 to 2022.
Figure 4.
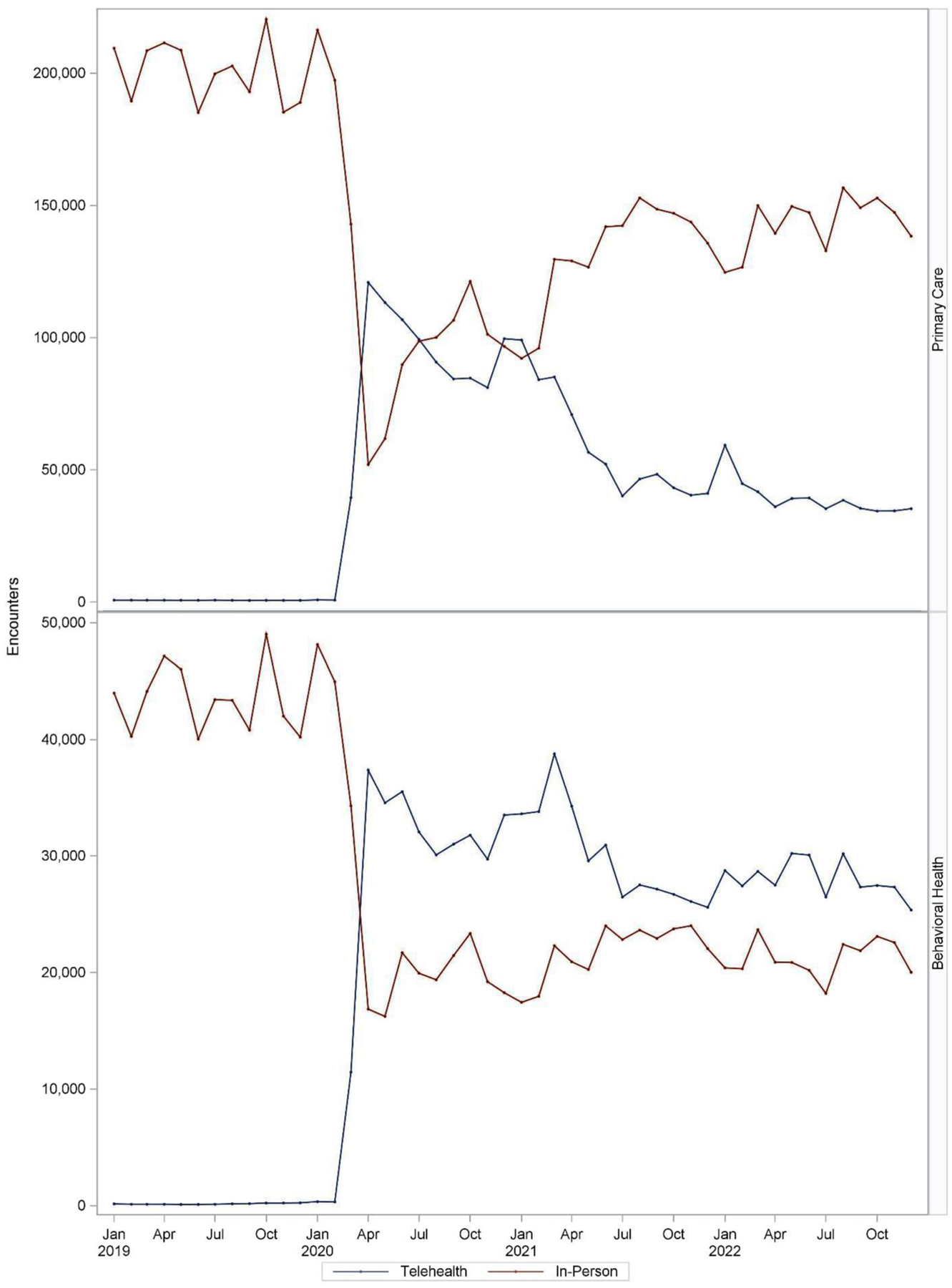
Monthly number of in-person and telehealth encounters for primary care and behavioral health (2019 to 2022).
Behavioral Health
From 2019 to 2022, there was little change in the number of established patients receiving behavioral health care, declining 0.6%. During this same period, there was a 19.8% decline in new patients (Table 2). Monthly data elucidates that the number of new patients for behavioral health began to decrease around March 2020 and remained lower than the number of prepandemic new patients through 2022, whereas established patients seen for behavioral health changed over the months, with a high number of patients seen January – March 2021 (Figure 2). Behavioral health patients by age-group changed less over the 4 years than primary care and the number of adult patients 18 to 44 and 65+ that received care at the health centers increased over the 4 years, with a peak for all age groups in February/March 2021 (Figure 3). Similar to primary care, telehealth encounters increased quickly in March/April 2020. In contrast to primary care, telehealth encounters remained the predominant care delivery mode throughout 2022 (Figure 4).
Discussion
This study provides a comprehensive picture of how COVID-19 impacted primary care and behavioral health care delivery before and throughout the COVID-19 public health emergency among health disparate populations seen in 218 health centers. Primary care providers are the foundation of the US Health care system and health centers are a main source of care in medically vulnerable communities. In 2021, health centers provided care to 1 in 3 people living in poverty.8 Though historically under-resourced, health centers across the nation were at the frontlines of the pandemic response as early testing and vaccine sites, while continuing to provide comprehensive care to the minoritized communities they serve.1 Studies suggest that although health centers were agile in their pandemic response, gaps in cancer screening9 and other preventive care services emerged.10
Health centers responded to the pandemic by allocating resources toward testing and vaccines1 and shifting patient care to telehealth, both audio and video, to meet the needs of their patients.3 Our findings suggest that this rapid shift also responded to growing needs in behavioral health care for established patients, and for primary care for established patients 65 and older, demonstrating that health centers may have allocated increasingly scarce resources toward addressing emerging mental health needs,11 and providing continuity of care for older patients, who tend to be sicker and have multiple chronic diseases.12
Our finding that pediatric primary care patients declined from 2019 to 2022 is disturbing, yet consistent with studies assessing the impact of the pandemic on the continuity of pediatric care through 2020.13–16 This is particularly concerning as our study includes safety-net populations who were already experiencing a disproportionate burden of health inequities before the pandemic. Though our report did not stratify pediatric care trends by demographic subgroups of interest (eg, race, ethnicity, insurance, state) or by in-person versus telehealth, other studies suggest that minority and low-income children were less likely to receive telehealth care and less likely to resume care after COVID-19 disruptions.13,17,18 Ongoing research is needed to evaluate if disparities in access and receipt of pediatric primary care continue to be exacerbated longer-term and which strategies are effective in supporting continuity of care.
The decrease in new primary care patients suggest that health centers may have reduced capacity to see new patients, a well-documented challenge among health centers and in primary care overall that was exacerbated by the pandemic.6,19 This could partly be due to organizational shifting of services (eg, testing and vaccines) or organizational constraints (eg, staffing and resources).6 This is especially concerning given that the health disparity gap widened during the pandemic and poverty remains high.20
The uptake in telehealth reflects well-documented trends.21,22 Of note, the continued high volume of behavioral health telehealth visits represents what will likely remain a sustainable shift in care, particularly in states that adopt telehealth parity policies, and one that is largely acceptable to patients.23,24
The OCHIN network provides a unique electronic medical record window into care by health centers in multiple states but may not be representative of all health centers. Only health centers that provided primary care were included in the study; health centers that focus exclusively on behavioral health or nonprimary care services were not captured. COVID-related care by health centers that did not generate an encounter code were also not included. In addition, it is likely that care delivery experiences throughout the pandemic (eg, transition to telehealth) may be more homogenous among clinics sharing a single instance of a hosted EHR.25 This study includes 218 health center clinic sites across 13 states; nationally health centers serve 30 million people in more than 14,000 sites.8 Overall, the demographic population in this study is reflective of all health centers in terms of race/ethnicity and low-income. Compared with all health centers, clinics in this study had a higher percent of patients who were publicly insured (eg, Medicaid) and a slightly lower precent who are uninsured.2 This is due to OCHIN having a larger presence in Medicaid expansion states.26 Although state policies have a significant impact on health care delivery for safety-net populations, health centers in all regions shared commonalities throughout the pandemic.
To our knowledge, this study represents the most recent snapshot of health center care delivery trends through 2022. It is still too early to fully understand how health centers shifting to respond to emerging needs throughout the pandemic, including the transition to virtual care, may have impacted access to primary care, patient health/outcomes among safety-net populations and the nature of clinical care delivery in our nation’s health centers.27,28 This work is part of 2 mixed-methods National Institute of Health-awarded studies to understand how care delivery changes in health centers impact clinical care delivery and patient outcomes over 6 years.
This work underscores how the COVID-19 pandemic impacted care delivery in health centers for new and established patients, by age-group and by care delivery. It also identifies gaps for some patient groups that can be addressed through recent national investment to strengthen health centers29 striving to meet the evolving needs of traditionally underserved patients and communities.
Supplementary Material
Funding:
This work is supported by a grant from the National Institute on Aging: 1R01 AG074946-01.
Footnotes
Conflict of interest: The authors have no conflicts of interest to declare.
References
- 1.Community Health Center Chartbook. 2021; Available at: https://www.nachc.org/research-and-data/research-fact-sheets-and-infographics/2021-community-health-center-chartbook/. Accessed January 12, 2022.
- 2.Community Health Center Chartbook. 2022; Available at: https://www.nachc.org/wp-content/uploads/2022/03/Chartbook-Final-2022-Version-2.pdf. Accessed September 18. 2022.
- 3.Telehealth During COVID-19 Ensured patients were not left behind. Available at: https://www.nachc.org/wp-content/uploads/2021/07/Audio-Only-Report-Final.pdf. Accessed August 24, 2022.
- 4.Larson AE, Zahnd WE, Davis MM, et al. Before and during pandemic telemedicine use: an analysis of rural and urban safety-net clinics. Am J Prev Med 2022;63:1031–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Payán DD, Frehn JL, Garcia L, Tierney AA, Rodriguez HP. Telemedicine implementation and use in community health centers during COVID-19: Clinic personnel and patient perspectives. SSM Qual Res Health 2022;2:100054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Current State of the Health Center Workforce: Pandemic challenges and policy solutions to strengthen the workforce of the future. 2022; Available at: https://www.nachc.org/current-state-of-the-health-center-workforce/. Accessed August 24, 2022.
- 7.CMS Manual System: Pub 100–04 Medicare Claims Processing, February 25, 2011. In: Department of Health and Human Services CfMMS, ed. Change Request 7060. Vol Transmittal 2161. [Google Scholar]
- 8.Health Center Program: Impact and Growth. 2022; Available at: https://bphc.hrsa.gov/about-health-centers/health-center-program-impact-growth#:;:text=Advancing%20Health%20Equity%20for%20Millions&text=In%202021%2C%20health%20centers%20achieved,one%20in%20five%20rural%20residents. Accessed June 20, 2023.
- 9.Fisher-Borne M, Isher-Witt J, Comstock S, Perkins RB. Understanding COVID-19 impact on cervical, breast, and colorectal cancer screening among federally qualified healthcare centers participating in “Back on track with screening” quality improvement projects. Prev Med 2021;151:106681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Simon J, Mohanty N, Masinter L, Hamilton A, Jain A. COVID-19: exploring the repercussions on federally qualified health center service delivery and quality. J Health Care Poor Underserved 2021;32:137–44. [DOI] [PubMed] [Google Scholar]
- 11.Coley RL, Baum CF. Retracted: Trends in mental health symptoms, service use, and unmet need for services among U.S. adults through the first 9 months of the COVID-19 pandemic. Transl Behav Med 2021;11:1947–56. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 12.Boersma P, Black LI, Ward BW. Prevalence of multiple chronic conditions among US adults, 2018. Prev Chronic Dis 2020;17:E106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Schweiberger K, Patel SY, Mehrotra A, Ray KN. Trends in pediatric primary care visits during the coronavirus disease of 2019 pandemic. Acad Pediatr 2021;21:1426–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Brown CL, Montez K, Amati JB, et al. Impact of COVID-19 on pediatric primary care visits at four academic institutions in the Carolinas. Int J Environ Res Public Health 2021;18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Phan TT, Enlow PT, Lewis AM, et al. Persistent disparities in pediatric health care engagement during the COVID-19 pandemic. Public Health Rep 2023;138:633–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lebrun-Harris LA, Sappenfield OR, Warren MD. Missed and delayed preventive health care visits among US children due to the COVID-19 pandemic. Public Health Rep 2022;137:336–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wallis KE, Nekrasova E, Bennett AE, et al. Autism spectrum disorder screening during the COVID-19 pandemic in a large primary care network. Acad Pediatr 2022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Batioja K, Elenwo C, Hartwell M. Disparities in pediatric medical and childcare disruption due to COVID-19. JAMA Pediatr 2023;177:432–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Series 35 Fielded, February 25-March 1, 2022. Quick Covid-19 primary care survey 2022; Available at: https://www.green-center.org/covid-survey. Accessed August 24, 2022.
- 20.Monthly Poverty in 2022 Remains Elevated in February. Center on Poverty & Social Policy at Columbia University; 2022. Available at: https://static1.squarespace.com/static/610831a16c95260dbd68934a/t/623b3453e0ed764d39b715b4/1648047188230/Monthly-poverty-February-2022-CPSP.pdf. Accessed August 24, 2022. [Google Scholar]
- 21.Xu P, Hudnall M, Zhao S, Raja U, Parton J, Lewis D. Pandemic-triggered adoption of telehealth in underserved communities: descriptive study of pre-and postshutdown trends. J Med Internet Res 2022; 24:e38602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Shaver J The state of telehealth before and after the COVID-19 pandemic. Prim Care 2022;49: 517–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Steidtmann D, McBride S, Mishkind M. Patient experiences with telemental health during the COVID-19 pandemic. Journal of patient experience 2022;9:23743735221145077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Erikson C, Herring J, Park YH, Luo Q, Burke G. Association between state payment parity policies and telehealth usage at community health centers during COVID-19. J Am Med Inform Assoc 2022;29:1715–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Whaley CM, Ito Y, Kolstad JT, Cowling DW, Handel B. The health plan environment in California contributed to differential use of telehealth during the COVID-19 pandemic. Health Aff (Millwood) 2022;41:1812–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.OCHIN: About Members. Available at: https://ochin.org/members. Accessed September 20, 2022.
- 27.Corallo B, Tj Shin P, Rosenbaum S. Changes in community health center patients and services during the COVID-19 pandemic. Available at: https://www.kff.org/medicaid/issue-brief/changes-in-community-health-center-patients-and-services-during-the-covid-19-pandemic/. Accessed June 20, 2023.
- 28.Philipps RB, Baum A. The COVID-19 Tsunami: the tide goes out before it comes in. In: Health Affairs Blog. Available at: https://www.healthaffairs.org/content/forefront/covid-19-tsunami-tide-goes-out-before-comes. [Google Scholar]
- 29.HHS awards nearly $90 million to community health centers to advance health equity through better Data. Available at: https://www.hhs.gov/about/news/2022/08/08/hhs-awards-nearly-90-million-dollars-to-community-health-centers-to-advance-health-equity-through-better-data.html. Accessed August 24, 2022.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.