

Abstract
BACKGROUND:
Coronary artery disease is the most common cause of cardiovascular disease. Smoking is one of the triggering factors for CAD, which increases mortality and morbidity rates. The aim of this study was to assess the impact of the SMART heart package on high-risk adults' knowledge and practice of coronary artery disease prevention.
MATERIAL AND METHOD:
A quasi-experimental research study was conducted in India from March 25 to April 23, 2022, through a house-to-house survey. This survey was conducted among 200 adults out of 159 high-risk adults who were identified by a screening tool, using a systematic random sampling technique to select 60 subjects for the study. A SMART heart package intervention was administered for selected high-risk adults. The pre-test and the post-test were conducted using self-administered structured questionnaires for knowledge and a non-observation checklist for practice. The data had been analyzed by the Statistical Package for Social Science (SPSS) version 20.0.
RESULTS:
The findings show that at the baseline level of knowledge and practice, the majority of the subjects had inadequate knowledge 43 (71.7%) and 51 (85.0%) had poor practice, whereas after administration of the SMART heart package, 29 (48.3%) of subjects had moderately adequate knowledge and 29 (48.3%) had average practice. At baseline, the mean score was 41.5%, which increased to 79.1% on knowledge and 37.2% to 72.5% on practice after the implementation of the intervention, which was statistically significant (P < 0.001).
CONCLUSION:
Hence, the SMART heart package was effective in increasing the level of knowledge and practice of CAD prevention among high-risk adults.
Keywords: Demonstration, education, high risk, prevention, remonstration, SMART heart package
Introduction
The circulatory system that circulates the blood transports oxygen, carbon dioxide, nutrients, hormones, and immune cells to and from the tissues and end organs.[1] Coronary artery disease (CAD) surges cardiovascular mortality worldwide, with >4.5 million deaths in the developing world.[2] Coronary artery disease (CAD), the most fatal heart disease due to its high incidence and high mortality rate, leads to sudden cardiac arrest and threats to human health.[3,4]
CAD is caused by the thickening and hardening of the arterial walls as well as plaque depositions such as fat, cholesterol, fibers, and calcium in the arteries. The plaque that is built inside the artery causes narrowing, restricting the blood flow, and depriving oxygen to the heart. It reduces blood flow and oxygen supply to the heart muscles, which can cause shortness of breath, angina, heart attacks, heart failure, and dysrhythmias.[5]
India is one among the countries with the highest burden of cardiovascular disease (CVD) worldwide. CAD prevalence rate is ranging from 1% to 13.2% in urban populations over the past several decades. The annual deaths from CVD in India have risen from 2.26 million in 1990 to 4.77 million in 2020. A likelihood of high burden of CVD in the future is because of high incident rates of obesity, hypertension, and diabetes in urban Indian cohorts.[6]
According to report in 2019, 32% of all global deaths were due to cardiovascular diseases (CVDs) with an estimated 17.9 million people and 85% among those were due to heart attack and stroke, causing cardiovascular diseases (CVDs) a number one cause of death globally.[7,8]
Smoking, physical inactivity, dangerous alcohol consumption, and a low intake of fruits and vegetables have all been linked to the development of coronary heart disease (CHD). The majority of the risk factors that aids development of heart attacks and strokes are preventable with early detection of CAD, appropriate intervention, and lifestyle modification, which reduces the mortality rate by 35–60%.[9,10]
Rapid socioeconomic development in developing countries has increased exposure to CAD risk factors such as diabetes, genetic factors, hypercholesterolemia, and hypertension. These risk factors are decreased by the relative lack of prevention and control measures for CAD in developing countries.[11,12]
Along with the biomarkers of CAD, the focus must be shifted toward the traditional risk factors of CAD such as cigarette smoking, hypertension, obesity, hyperlipidemia, diabetes mellitus, and insulin resistance by the most developing countries.[13]
Cardiovascular diseases, a major cause of mortality and morbidity in Indians, leads to more than 25% of deaths. It has been predicted that within the next 15 years, this country will host more than half the cases of heart disease in the world. Both the urban and rural communities of India have recorded the increased incidences of coronary heart disease and stroke. Coronary heart disease is estimated to become the most common cause of death in India within 15 years.[14,15]
A study was conducted on knowledge regarding preventive measures of coronary artery disease among patients attending out patients department. Study found that only 15.33% had a good level of knowledge and rest of the subjects 84.67% had a poor knowledge. The study suggests that an awareness-raising campaign about CAD preventive measures can be implemented periodically in the community to reduce the burden of such a devastating disease of CVD.[16]
The above studies mentioned that there is an alarming rise in CAD and its risk factors among adults in both urban and rural areas. A majority of adults did not practice routine and essential activities which help in maintaining health like healthy lifestyle activities like a balanced diet, exercise, adequate rest, sleep, psychological balance, and recreational activities due to urbanization and work-related burden. The researcher felt that public should be aware about the importance of these routine healthy activities as essential parts of life in the prevention of CAD, which rapidly increases the incidence of CVD and can be controlled. Other components also need to be considered such as poor management of diabetes and hypertension ends with cardiovascular disease, and it needs to be given more concern. Despite widespread efforts to raise awareness, many people are still unaware of the consequences and prevention of CAD-related risk factors. Hence, the researcher identified that in Indian context, none of the studies were conducted among high-risk adults to prevent CAD and combination of multiple strategies studies also not has been undertaken as trails for this population only single intervention studies were conducted in India and western countries, it shows that there is an urgent need to take up measures to raise awareness levels to the public, which is the key component to enhancing compliance on prevention of CAD. So investigators felt that it is important to screen the adults for high risk in the future getting CAD and to impart preventive aspects at the earliest.
Materials and Methods
Study design and setting
Quantitative research was conducted to assess the effectiveness of the SMART heart package on knowledge and practice regarding the prevention of coronary artery disease among high-risk adults. Using a one-group, quasi-experimental pretest and post-test, the design was implemented. The pre-test level of knowledge and practice was assessed on the same day after screening the subjects, followed by the SMART heart package intervention administered to selected subjects, and the post-test was conducted after 20 days, the duration of data collection being 4 weeks.
Study participants and sampling
From March 25 to April 23, 2022, the study was conducted in Upnagar, an urban community in Bangalore. The research investigator performed a house-to-house survey to identify the high-risk adults above the age of 21. Totally 200 adults screened out of 159 high-risk adults were identified, and 60 subjects were selected for the study using a simple random sampling technique and a lottery method. Samples were allocated to six groups, and each group had ten high-risk adults [Figure 1].
Figure 1.
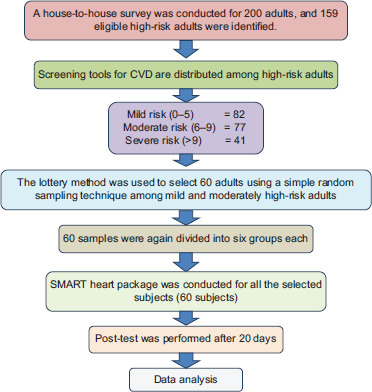
Schematic representation of sampling selection process and sampling technique
The sample size of the study was calculated considering knowledge as a primary outcome variable. Similar study was conducted by Gayathri “Effectiveness of Heart Smart Package on Knowledge and skill regarding prevention of Coronary Artery Disease among at risk Clients attending chronic outpatient Clinics at selected setting, Andhra Pradesh. (2016),” and the sample size was estimated using power analysis (α =5% and power
((1-β) =80%) and effect size 0.63. A total of 50 subjects were needed to achieve a significance of 0.05.
Sample size—estimated
Study required = 50 subjects
20% added for attrition
Total samples required 60
Ethical consideration
The study was approved by the research ethical committee at the Padmashree Institute of Nursing, and formal permission was obtained from the concerned authority of Kengeri Upnagar PHC with the registration number 05_N316_119594 on March 30, 2022, and informed consent was obtained from the subjects.
SMART heart package
The study was conducted for a total duration of about 4 weeks. The researcher obtained official permission from the Kengeri Upnagar PHC urban community and informed consent from the sample. The eligible samples were selected based on a simple random sampling technique, and the baseline level of knowledge and practice was assessed using structured questionnaires and a non-observational checklist.
Followed by an Stress Management and Recreational Techniques (SMART) heart package, which included the components of education, demonstration, and re-demonstration sessions on prevention of CAD. An education intervention was conducted by the research investigator use of lecturer and interactive session on focusing the aim of encouraging the behavioral changes among the participants topic focusing on healthy diet, regular exercises, cessation of smoking and alcohol, monitoring optimum health, recreational techniques, and stress reduction techniques with the use of PowerPoint and charts for a duration of 30 to 40 minutes. A demonstration session was conducted aimed at improving healthy physical activities and exercise; the session was organized by the researcher on warm-up, twist crunches, squats, static lunges, deep breathing exercises, and cool-down exercises for 15 minutes. A re-demonstration session goal to practice the strategies or activities was demonstrated by investigators and here by the participants who were asked to perform the demonstrated exercise under the supervision of a researcher every day for 15 minutes for 20 days continuously. The total selected subjects were divided into six groups, and each consisted of ten members to implement the intervention according to group.
A post-test was performed after 20 days of study using the same knowledge and practice tools. After the completion of the study, the remaining eligible high-risk adults who had not been selected through the sampling technique received a similar intervention.
Measurement of outcomes
The tool consists of four parts. Section A cardiovascular screening tool consists of 11 items like blood pressure, blood glucose level, BMI, smoking, alcohol, and diet. Section B consists of demographic data, which gives baseline information on CVD such as age, gender, religion, marital status, types of family, educational status, occupational status, family income per month, comorbidities, weight, height, and BMI. Section C knowledge questionnaire had 26 items in two domains, such as general information regarding CAD (ten items) and regarding preventive measures for CAD (16 items) scoring interpretation of the tool <50% = inadequate, 50–75% = moderately adequate, and >75% = adequate knowledge. Section D practice checklist had 16 items, interpreting the tool <50% = poor, 50–75% = average, and >75% = good practice.
The tool reliability obtained by using the split-half method was 0.85 for knowledge and 0.92 for practice. The study's tools were reliable to conduct the research.
Statistical analysis
The data were analyzed by using version 20.0, that is, SPSS package. Paired t-test was used to compare the mean scores before and after the administration SMART package, Chi-square test used to associate the outcome variables with demographic variables and Karl Pearson coefficient of correlation used to correlate the knowledge and practice.
Results
A total of 60 subjects were enrolled, with the majority (53.3%) being between the ages of 41 and 50. There were more males (37, 61.7% of the total) than females. Forty-one (68.3%) of adults belonged to the Hindu religion. According to the demographic characteristics, 28 (46.7%) of the adults had a graduate or higher education and 24 (40.0%) were private employees. Other characteristics have been given in Table 1.
Table 1.
Demographic characteristics of high-risk adults
| Demographic variables | Categories | Frequency | Percentage (n=60) |
|---|---|---|---|
| Age in years | 21–30 years | 5 | 8.3 |
| 31–40 years | 13 | 21.7 | |
| 41–50 years | 32 | 53.3 | |
| 51–60 years | 10 | 16.6 | |
| Gender | Male | 37 | 61.7 |
| Female | 23 | 38.3 | |
| Religion | Hindu | 41 | 68.3 |
| Muslim | 14 | 23.3 | |
| Christian | 5 | 8.3 | |
| Others | - | - | |
| Marital status | Unmarried | 2 | 3.3 |
| Married | 51 | 85 | |
| Divorced | 5 | 8.3 | |
| Widow/widower | 2 | 3.3 | |
| Type of family | Nuclear family | 22 | 36.7 |
| Joint family | 19 | 31.7 | |
| Extended family | 19 | 31.7 | |
| Educational status | Primary education | 5 | 8.3 |
| Secondary education | 6 | 10.0 | |
| PUC | 21 | 35.0 | |
| Graduate and above | 28 | 46.7 | |
| Occupational status | Unemployed | 12 | 20.0 |
| Daily wages | 5 | 8.3 | |
| Govt. employee | 19 | 31.7 | |
| Private employee | 24 | 40.0 | |
| Family Income per month | ≤10,000 | 10 | 16.7 |
| 10,001–15,000 | 5 | 8.3 | |
| 15,001–20,000 | 31 | 51.7 | |
| >20,000 | 14 | 23.3 | |
| Comorbidities | Hypertension | 17 | 28.3 |
| Diabetes mellitus | 22 | 36.7 | |
| Others | 21 | 35.0 | |
| Weight (kg) | 51–60 | 33 | 55.0 |
| 61–70 | 16 | 26.7 | |
| 71–80 | 9 | 15.0 | |
| 80 and above | 2 | 3.3 | |
| Height (feet) | 4.6–5.5 | 38 | 63.3 |
| 5.6–6.6 | 20 | 33.3 | |
| 6.6–7.5 | 2 | 3.3 | |
| BMI (Kg/m2) | Underweight (<18.5) | 1 | 1.7 |
| Normal (18.5–24.5) | 2 | 3.3 | |
| Overweight (25.0–29.9) | 38 | 63.3 | |
| Obesity (>30.0) | 19 | 31.7 |
Figure 2 shows that the majority of subjects, at baseline, 43 (71.6%), had inadequate knowledge, while 16 (26.7%) adults had moderate adequate knowledge, whereas after administration of the SMART heart package, 29 (48.4%) adults had moderately adequate knowledge and 26 (43.3%) adults had adequate knowledge. Above findings are evident that the invention was beneficial for selected subjects to improve knowledge on prevention of CAD which helps the subjects decrease chance of developing the CAD.
Figure 2.
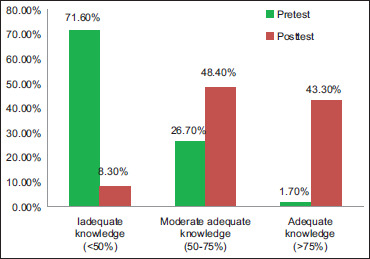
Level on knowledge in the pre-test and post-test
Figure 3 shows that the majority of subjects in the baseline sample, 51 (85%), had poor practice, nine (15%) adults had average practice, and the study shows that none of the adults have good practice, whereas, after administration of the SMART heart package, 29 (48.4%) adults had average practice and 17 (28.3%) had good practice. Above findings manifest that the invention was helpful for selected subjects to improve practice on prevention of CAD which helps the subjects decrease chance of developing the CAD.
Figure 3.
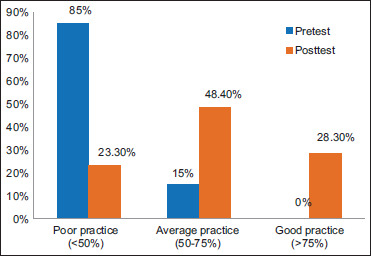
Level on practice in the pre-test and post-test
The baseline knowledge mean score of 10.80 increased by 20.57 in the post-test, and the difference in mean score was 9.77, whereas in practice the mean score of 23.80 increased by 46.42 in the post-test, and 22.62 is the difference in mean score. After administering the SMART heart package to high-risk adults, they were able to gain knowledge and practice on the prevention of CAD [Table 2]. The SMART heart package has an effect on increasing knowledge and practice levels, which affects high-risk adults' ability to prevent CAD.
Table 2.
Range, mean, standard deviation, and mean percentage level of knowledge and practice in the pre-test and post-test
| Aspect of knowledge regarding CAD | Max Score | |
(n=60) |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-test |
Post-test |
||||||||
| Range | Mean | SD | Mean % | Range | Mean | SD | Mean % | ||
| General information of CAD | 10 | 2–6 | 3.95 | 0.98 | 39.5 | 3-10 | 7.52 | 1.96 | 75.2 |
| Prevention of CAD | 16 | 3–14 | 6.85 | 1.94 | 42.8 | 8-16 | 13.05 | 2.44 | 81.6 |
| Overall | 26 | 6–20 | 10.80 | 2.27 | 41.5 | 11-26 | 20.57 | 4.07 | 79.1 |
| Level of practice | 64 | 13–35 | 23.80 | 5.29 | 37.2 | 28-62 | 46.42 | 10.93 | 72.5 |
Tables presented the overall gain in the mean score for knowledge 9.76 ± 4.86 and practice 22.61 ± 11.26, and there was a high statistical significance at P < 0.001 [Table 3]. The maximum gain in the mean percentage was found in aspects on prevention of CAD after the administration of intervention; it shows that the participants were able to understand and follow interventions on preventive aspects and strategies regarding CAD. Participants had low mean scores in the baseline, which shows they were not aware of preventive aspects of CAD, and participants had received adequate information from the research investigator during the interactive session which is evident improvement in the mean score in the post-test. The study results are evident that interventions are more beneficial to impart the knowledge and improve good practice among high-risk adults. This intervention can be continued for all the participants for a longer duration to maintaining good health to prevent cardiovascular disease.
Table 3.
Comparison of pre-test and post-test level on knowledge and practice
| Aspect of knowledge regarding CAD | Max. Score | Paired t-difference (Enhancement) |
Paired “t” test | P (n=60) | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean % | ||||
| General information | 10 | 3.56 | 2.04 | 35.6 | 13.510* | P<0.001 |
| Prevention of CAD | 16 | 6.20 | 3.42 | 38.7 | 14.007* | P<0.001 |
| Over all knowledge | 26 | 9.76 | 4.89 | 37.5 | 15.460* | P<0.001 |
| Level of practice | 64 | 22.61 | 11.26 | 35.3 | 15.557* | P<0.001 |
*-denotes significant
Correlation between level on knowledge and practice
It shows that the correlation is 0.405; it was found to be positive and statistically significant at P < 0.05 level. This is evident that as knowledge increases, the practice also increases.
Discussion
The study was initiated to identify the impact of the SMART heart package on urban community. Recent data show that over the past ten years, the prevalence of CAD in India has grown up. The study revealed that the SMART heart package had improved the level on knowledge and practice regarding prevention of CAD. There was a significant improvement in the mean score on knowledge from 41.5 to 79.1, the mean difference percentage was 37.5, on practice from 37.2 to 72.5, and the mean difference percentage was 35.3 after the administration of the intervention. The SMART heart package was statistically highly significant for knowledge and practice at P < 0.001 level.
A similar study was conducted to assess knowledge on coronary artery diseases (CAD) among patients attending medical OPD, and the results show that 44% of patients had average knowledge, 34% had good knowledge, and 22% had below average knowledge about CAD among patients attending medical OPD.[17] Another study identified the quasi-experimental pre- and post-test design with implementation of intervention, which consist of education and demonstration. The study showed that paired t value 9.40, which is highly statistically significant at P < 0.001.[18]
The majority of adults and family members in the urban community may not be aware of the preventive aspects of CAD. Day by day, the prevalence of CAD and its mortality rate increase, even in young adults. Hence, healthcare professionals have a vital role in controlling and preventing the disease, so providing a SMART heart package regarding prevention of CAD can contribute to better knowledge and practice among family members and the high-risk population. Furthermore, emphasizing or reinforcing the knowledge and practice among high-risk adults helps in the prevention of cardiovascular disease and maintaining optimum health in society. In the hospital OPD, rural community, and industries, SMART heart package intervention can be implemented by involving family members, individual, friends, and peer groups to enhance their knowledge and practice on prevention of cardiovascular disease.
Prevention is better than cure; nurses working in the community and non-profit organizations can plan multiple component interventions for the high-risk adults in the community level. Nurses can utilize and implement SMART heart package for their community area to maintain optimum health to the public. Nurses were easy accessible healthcare professional so then can conduct long-term follow-up studies in the future. Public health nurse can do survey in the community to identify the high-risk family for cardiovascular disease, and family-based intervention can be administered.
Limitations and recommendation
The study's findings contain some limitations. Adults' levels on knowledge and practice may be different depending on their educational circumstances, locality, and age. The study only includes high-risk adults. Researcher had difficulty in involving planned research activity as per schedule due to sample work pattern.
Conclusion
The proposed SMART heart package significantly increased high-risk subject's level on knowledge and practice toward CAD prevention. However, there is a need to conduct a CAD awareness program or the SMART heart package in the hospital, home care setting, and community or healthcare settings to improve or increase knowledge and practice regarding CAD prevention. Adults at high risk for CAD will benefit, and this helps in upholding their respectable health status.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
Our heartfelt gratitude goes to the Padmashree Institute of Nursing, the medical surgical department and HOD, as well as the study participants.
References
- 1.Chantler PD, Frisbee JC.Circulatory system alterations under stress. In Cardiovascular Implications of Stress and Depression. Academic Press; 2020. p. 111–39 [Google Scholar]
- 2.Okrainec K, Banerjee DK, Eisenberg MJ.Coronary artery disease in the developing world Am Heart J 20041487–15 [DOI] [PubMed] [Google Scholar]
- 3.Wah TY, Gopal Raj R, Iqbal U.Automated diagnosis of coronary artery disease: A review and workflow Cardiol Res Pract 201820182016282. doi: 10.1155/2018/2016282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zhou W, Wang Y.A network-based analysis of the types of coronary artery disease from traditional Chinese medicine perspective: Potential for therapeutics and drug discovery J Ethnopharmacol 201415166–77 [DOI] [PubMed] [Google Scholar]
- 5.Bruning RS, Sturek M.Benefits of exercise training on coronary blood flow in coronary artery disease patients Prog Cardiovasc Dis 201557443–53 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Purohit V, Mehta K.Study of congestive cardiac failure cases at tertiary care hospital: Observational study Indian Journal of Basic and Applied Medical Research 2021:10257–260. DOI: 10.36848/IJBAMR/2020/26215.55705 [Google Scholar]
- 7.Mc Namara K, Alzubaidi H, Jackson JK.Cardiovascular disease as a leading cause of death: How are pharmacists getting involved? Integr Pharm Res Pract 201981–11. doi: 10.2147/IPRP.S133088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sharma H, Saini VK, Sarawag M, Ahuja J.Study on the association of dietary habits with cardiovascular disease in south-eastern Rajasthan Int J Pharm Clin Res 2022141–8 [Google Scholar]
- 9.Dale LP, Whittaker R, Jiang Y, Stewart R, Rolleston A, Maddison R.Improving coronary heart disease self-management using mobile technologies (Text4Heart): A randomised controlled trial protocol Trials 2014151–9. doi: 10.1186/1745-6215-15-71 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kavi A, Walvekar PR, Patil RS.Biological risk factors for coronary artery disease among adults residing in rural area of North Karnataka, India J Family Med Prim Care 20198148–53 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Okrainec K, Banerjee DK, Eisenberg MJ.Coronary artery disease in the developing world Am Heart J 20041487–15 [DOI] [PubMed] [Google Scholar]
- 12.Gaziano TA, Bitton A, Anand S, Abrahams-Gessel S, Murphy A.Growing epidemic of coronary heart disease in low-and middle-income countries Curr Probl Cardiol 20103572–115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aje TO, Miller M.Cardiovascular disease: A global problem extending into the developing world World J Cardiol 200913–10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gupta R, Joshi P, Mohan V, Reddy KS, Yusuf S.Epidemiology and causation of coronary heart disease and stroke in India Heart 20089416–26 [DOI] [PubMed] [Google Scholar]
- 15.Stein CE, Fall CH, Kumaran K, Osmond C, Barker DJ, Cox V.Fetal growth and coronary heart disease in south India Lancet 19963481269–73 [DOI] [PubMed] [Google Scholar]
- 16.Choudhary M, Sharma K, Sodhi JK.Knowledge regarding preventive measures of coronary artery disease among patient attending out patient departments of selected hospital of Ludhiana city Int J Healthc Sci 2014260–3 [Google Scholar]
- 17.Chouhan P, Williams V. To assess knowledge regarding coronary artery diseases (cad) among patients attending medical OPD with a view to develop guidelines on life style modifications at selected hospitals. Int J Dev Res. 2017;7:10195. [Google Scholar]
- 18. Gayathri K. Effectiveness of Heart Smart Package on Knowledge and skill regarding prevention of Coronary Artery Disease among at risk Clients attending chronic outpatient Clinics at selected setting, Andhra Pradesh (Doctoral dissertation, Omayal Achi College of Nursing, Chennai) [Google Scholar]