

Abstract
Background:
Assessment of dental anxiety in children is difficult because of their immature cognitive and emotional development. Drawings are well well-established emotion assessment tool. These can be used as nonverbal methods of communication for expressing the children's anxiety and emotions. Art therapy utilizes creative therapy interventions to deal with children suffering from emotional problems.
Aims and Objectives:
The aim of the study is (1) To assess the drawings of children for the presence of dental anxiety. (2) To study the effectiveness of art therapy on dental anxiety in children.
Materials and Methods:
One hundred and twenty children within the age group of 6–12 years were part of this study. The pretest assessment of dental anxiety was done using Frankl and Five facial anxiety scales. All the participants received local anesthesia during their first treatment session. At the end of the treatment session, all the participants were asked to draw a picture of their experience. The drawn figures were assessed by a psychologist. The children were allotted randomly into the study group (n = 60) and control group (n = 60). Art therapy was given to 60 children in the study group for three consecutive appointments. The posttest assessment of dental anxiety was done using Frankl and Five facial anxiety scales after completion of the entire dental treatment.
Results:
The pretest scores revealed very high level of dental anxiety in 33 (55%) children in study group and 34 (56.67%) children in control group. The posttest scores of study group, who received the art therapy, revealed that 24 (40%) children had little anxiety and 32 (53.33%) children had some anxiety. Whereas in the control group, the posttest scores showed 20 (33.33%) children had high anxiety and 39 (65%) children had very high anxiety scores. There was a significant correlation between the objective score of dental anxiety and the subjective scores of CD: H.
Conclusion:
Drawings can be used as an assessment tool for the detection of dental anxiety and art therapy effectively reduces the anxiety in pediatric patients undergoing dental treatment.
Keywords: Art therapy, dental anxiety, dental treatment, drawing, human figure drawings
Introduction
Dental anxiety is defined as a state of apprehension that something dreadful is going to happen in relation to the dental treatment and it is coupled with a sense of losing control.[1] Children are afraid of dental treatment because of needles, drilling machine. Due to various reasons, it is difficult to measure the dental anxiety in children. These include the inability to rate the extent of emotional response, improper discrimination between emotions and difficulty in understanding the situation due to immature emotional as well as cognitive development.[2] The evaluation of children's subjective response toward the dental anxiety is difficult, especially at a very young age. Tools to assess the dental anxiety include observation of child's behavior in the clinic, a questionnaire completed by parents, use of dental anxiety scales as well as self-report by the child. Self-report methods are reported to be the most reliable and valid tools for measuring dental anxiety.[3] Children's Fear Survey Schedule–Dental Subscale are mostly used questionnaire. However, it has various drawbacks such as the inability to read and comprehend the questionnaire by young children as well as inadequate response rating by children because of developmental immaturity.[4]
Art therapy believes that every individual has the ability of creative expression and the outcome of the process has minor significance than the involved therapeutic process. The British Association of Art Therapists has defined art therapy as a form of psychotherapy that uses art media as its primary mode of expression and communication. Art therapy can be achieved via drawings, coloring, figure molding, or creation of a story with the help of collages or stickers. Various studies have reported a reduction in anxiety with the help of art therapy.[5] Drawings are well-established tool for the evaluation of psychological and emotional status of children. Drawings reveal the child's emotions such as his wishes, dreams, and fears. Self-report tests based on drawings are inexpensive, easily applicable, and delightful experiences for children. Children's drawings as well as their choice of colors have been used in the assessment of their emotional status in many studies.[6] Hence, this study was designed with the following aims and objectives:
To evaluate the pretest dental anxiety in children during dental treatment
To evaluate the child's drawing as a measurement of dental anxiety
To evaluate the posttest dental anxiety in children at the end of dental treatment
To evaluate the effectiveness of art therapy on dental anxiety in the children of the study group.
Materials and Methods
The study was approved (CTRI/2023/03/050551) and conducted in the Department of Pediatric Dentistry according to the ethical standards established by the Institutional Ethical Board of Government Dental College and Hospital, Aurangabad, Maharashtra (Registration number of ethical committee relating to clinical trial of bioavailability and bioequivalence study – ECR/684/Inst/MH/2014/RR-21 dated June 30, 2021). The sample size was calculated using the Cochran formula – n = n0/1+ [(n0 − 1)/N].
Where, n0 is Cochran's sample size recommendation and calculated using the formula n0 = Z2pq/e2.
p is the estimated proportion of the population that has the attribute in question, q is 1 − p, and e is the desired level of precision (margin of error). N is the population size and n is the new adjusted sample size. After the review of the comprehensive treatment plan for 445 children, 120 children were selected who satisfied the inclusion and exclusion criteria. The children between the age group of 6 and 12 years needing dental treatment under local anesthesia, not having any medical history or dental experience were included in the study. Children with medical conditions or previous dental treatment experience were excluded from the study. Children who refused to draw were also not included in the study. Before the study the written informed consent and assent were taken from all the participants (parents and children). They were informed about the purposes of the study and their queries were resolved before the start of the study. They were assured regarding the confidentiality of the information. The participation was voluntary and no incentives were offered to them.
Study design
One hundred and twenty children satisfying the inclusion and exclusion criteria participated in the study [Figure 1]. Dental treatment was performed for all the participants under local anesthesia (Lidocaine 2% with 1: 100,000 epinephrine). The pretest assessment of dental anxiety was done using Frankl and Five facial anxiety scales. Each child was asked to draw a picture of his experience at the end of the first dental treatment session. They were provided a blank sheet of A 4 size paper, pencil, and eraser. The queries of the child related to the drawings were resolved without influencing them. Each drawing was labeled with the participant number, date of birth, gender, and date of the drawing. All the drawings were assessed using Child Drawing: Hospital (CD: H) rating scale by a psychologist who was blind to the pretest dental anxiety scores. The participants were randomly divided into study and control groups (60 each) using the lottery method. The children in the study group received art therapy (in the form of coloring pages and connecting the numbers) for their three consecutive appointments. The children in the control group continued their dental treatment routinely. At the end of their entire dental treatment, the posttest assessment of dental anxiety was done using Frankl and Five facial anxiety scales.
Figure 1.
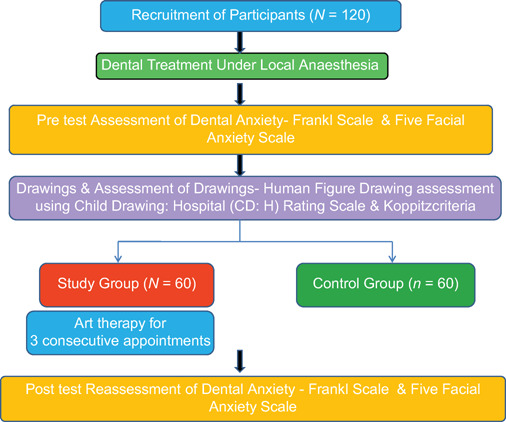
Study design
Assessment of drawings
A psychologist assessed the drawings made by the children using Child Drawing: Hospital (CD: H) drawing test given by Clatworthy.[7] The manual with scoring guide, scoring sheet, and rating scale [Figure 2] as well as the instructions for scoring the drawings was used.[7] The details of the scoring are mentioned in Figure 3. The lowest score demonstrates minimum anxiety level whereas the highest score represents the highest level of anxiety.
Figure 2.

Child drawing: hospital (CD: H) rating scale
Figure 3.
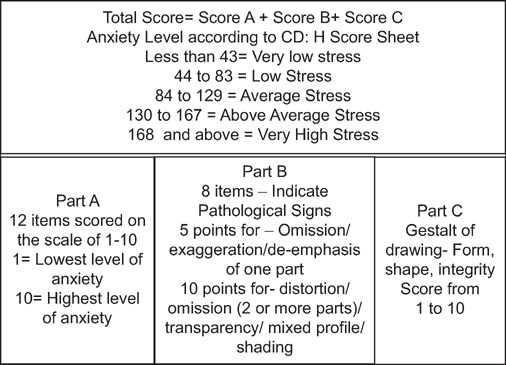
Scoring of the drawings
Statistical analysis
The descriptive statistical analysis (mean and standard deviation) was used to compare the level of dental anxiety in scores of pre- and posttest. The investigator's intra-rater reliability for Frankl and five facial anxiety scale scores was measured with Cohen's kappa. The reliability of the obtained data for Frankl and five facial anxiety scales was 0.96 and 0.94, respectively. The effectiveness of art therapy was analyzed using paired t-test.
Results
One hundred and twenty children (56 males and 64 females) within the age group of 6–12 years (Mean age of 7.16 ± 1.36) participated in this study. The distribution of demographic variables of the children is shown in Table 1. In the study group, 34 (56.67%) children were Muslims, 28 (46.67%) stayed with joint family, 23 (38.33%) parents had secondary education, and 29 (48.33%) fathers worked in private organizations with monthly income between 10000 and 15000. In the control group, 33 (55%) children were Muslims, 30 (50%) stayed with joint family, 24 (36.67%) parents had secondary education, and 28 (46.67%) fathers worked in private organizations with monthly income between 10000 and 15000. In the study group, 17 (28.33%) children showed a high level of anxiety and 33 (55%) children exhibited a very high level of anxiety in the beginning [Table 2], whereas 20 (33.33%) children showed high level of anxiety and 34 (56.77%) children exhibited very high level of anxiety in the control group [Table 3]. After receiving the art therapy only 3 (5%) children of the study group exhibited high anxiety in comparison to 39 (65%) children of the control group, who showed very high level of anxiety.
Table 1.
Description of demographic variables of children in the study and control groups
| Demographic variables | Study group, n (%) | Control group, n (%) |
|---|---|---|
| Age (years) | ||
| 6–8 | 36 (60) | 32 (53.33) |
| 10–12 | 24 (40) | 28 (46.67) |
| Gender | ||
| Male | 32 (53.33) | 24 (40) |
| Female | 28 (46.67) | 36 (60) |
| Religion | ||
| Hindu | 25 (41.67) | 27 (45) |
| Islam | 34 (56.67) | 33 (55) |
| Christian | 1 (1.66) | 0 |
| Others | 0 | 0 |
| Education of the child | ||
| 1st–3rd standard | 32 (53.33) | 29 (48.33) |
| 4th–6th standard | 28 (46.67) | 31 (51.67) |
| Type of family | ||
| Nuclear family | 26 (43.33) | 25 (41.67) |
| Joint family | 28 (46.67) | 30 (50) |
| Single parent family | 6 (10) | 5 (8.33) |
| Parent education | ||
| Illiterate | 0 | 0 |
| Primary education | 17 (28.33) | 14 (23.33) |
| Secondary education | 23 (38.33) | 24 (40) |
| Undergraduate | 20 (33.33) | 22 (36.67) |
| Postgraduate and above | 0 | 0 |
| Parent's occupation | ||
| Government employee | 12 (20) | 15 (25) |
| Private employee | 29 (48.33) | 28 (46.67) |
| Self-employed | 19 (31.67) | 17 (28.33) |
| Unemployed | 0 | 0 |
| Family income (months) | ||
| Rs. 5000–10,000 | 24 (40) | 22 (36.67) |
| Rs. 10,000–15,000 | 32 (53.33) | 36 (60) |
| Above 15,000 | 4 (6.67) | 2 (3.33) |
Table 2.
Assessment of pre- and post-test anxiety level among children in the study group
| Anxiety | No anxiety (0), n (%) | Little anxiety (1), n (%) | Some anxiety (2), n (%) | High anxiety (3), n (%) | Very high anxiety (4), n (%) |
|---|---|---|---|---|---|
| Pretest | 0 | 3 (5) | 7 (11.67) | 17 (28.33) | 33 (55) |
| Posttest | 1 (1.67) | 24 (40) | 32 (53.33) | 3 (5) | 0 |
Table 3.
Assessment of pre- and post-test anxiety level among children in the control group
| Anxiety | No anxiety (0), n (%) | Little anxiety (1), n (%) | Some anxiety (2), n (%) | High anxiety (3), n (%) | Very high anxiety (4), n (%) |
|---|---|---|---|---|---|
| Pretest | 0 | 2 (3.33) | 8 (13.33) | 16 (26.67) | 34 (56.67) |
| Posttest | 0 | 0 | 1 (1.67) | 20 (33.33) | 39 (65) |
Figure 4 shows sample of the drawings made by the children. They took 5–10 min for drawing. The average CD: H scores of the participants were 93.05 ± 25.15. Table 4 shows the gender-wise distribution of scores of CD: H, Frankl and five facial anxiety scale. Table 5 shows the effectiveness of art therapy analyzed using paired t-test. There was a significant decrease in the anxiety level in the study group. A statistically significant correlation was found between CD: H and Frankl (correlation coefficient = −0.232, P = 0.0001) as well as five facial anxieties (correlation coefficient r = +0.213 P = 0.0002) scales.
Figure 4.
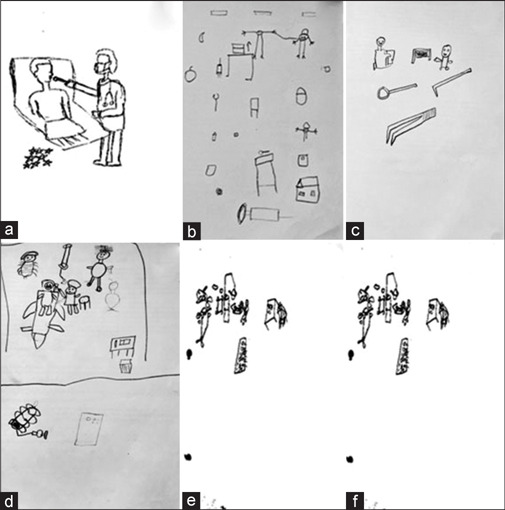
Assessment of some of the drawings. (a) This is drawn by 12-year-old girl. The child has drawn a lively picture of a dentist and a patient. She has drawn the body of the patient with incomplete hands and legs. The dental chair is floating with no base. The eyes are not properly visible and the nose is proportional to the face. Overall CD: H Score = 62 (low stress), Frankl Rating Score = 3 (positive), Five Facial Anxiety Scale = 1 (Mild Distress). (b) This is drawn by a 10-year-old boy. He has drawn a sick figure with arms and legs attached to the head. The number of fingers and toes is three. There is a lack of coordination in the drawing. Injection is drawn larger than the other figures. Overall drawing is not following Piaget's cognitive developmental stage. Emotional Indicators = Omission of nose, body, neck and feet indicating possible emotional difficulty. Overall CD: H Score = 134 (Above average stress), Frankl Rating Score = 2 (negative), Five Facial Anxiety Scale Score = 3 (severe distress). (c) This picture is drawn by a 12-year-old boy. He has two figures with ambiguous body shapes. There is absence of neck, arms, legs, nose, and feet. Overall body is disproportionate. He has done shading which indicate high level of anxiety. He has drawn dental instruments which are larger than the figures and sharp. Overall CD: H Score = 168 (very high stress), Frankl Rating Score = 2 (negative), Five Facial Anxiety Scale Score = 2 (moderate stress) (d) This is drawn by a 9-year-old boy. He has shown a dentist working on him. Large-size injection is drawn. Overall CD: H Score = 114 (average stress), Frankl Rating Score = 3(positive), Five Facial Anxiety Scale Score = 2 (moderate distress) (e) This is drawn by 7-year-old girl. She has drawn tiny figures of dentists doing the dental treatment. The figures drawn are very small in proportion to the environment. Overall CD: H Score = 165 (very high stress), Frankl Rating Score = 2 (negative), Five Facial Anxiety Scale Score = 2 (moderate stress) (f) This drawing is made by an 11-year-old boy. He has drawn a tiny stick figure of himself and larger threatening dental instruments. The drawing is not follow Piaget's cognitive developmental stage Overall CD: H Score = 174 (very high stress), Frankl Rating Score = 2 (negative), Five Facial Anxiety Scale Score = 3 (severe distress)
Table 4.
Child drawing: Hospital, Frankl and five facial anxiety scores
| Variable | Mean±SD |
P | |
|---|---|---|---|
| Girls (n=64) | Boys (n=56) | ||
| CD: H score | 148.28±23.16 | 146.35±22.42 | 0.312 |
| Frankl score | 3.12±0.52 | 3.32±0.42 | 0.514 |
| Five facial anxiety score | 4.25±2.6 | 5.15±2.8 | 0.342 |
*P<0.05 statistically significant. CD: H: Child drawing: hospital; SD: Standard deviation
Table 5.
Posttest anxiety scores comparison between the study and control groups
| Anxiety | Mean±SD | Paired t value |
|---|---|---|
| Experimental group | 0.85±0.36 | t=22.608 |
| Control group | 3.13±0.40 | P=0.000* |
*Statistically significant. SD: Standard deviation
Discussion
Dental treatment in children is challenging due to their age, emotional and psychological development. The administration of local anesthesia, extraction and pulpal treatment is usually perceived as a painful experience. Neglecting this experience could result in the development of dental anxiety thereby hampering the receipt of any dental treatment in future by the child.[7] Assessment of pain and distress in children is complex due to their limited capacity for verbal expression of emotions. Drawings of children evolve with their motor and cognitive development. A 4-year-old child can draw an identifiable human figure which becomes a proper representation of things by the age of 13 years. Children more than 6 years are likely to add major body parts such as eyes, mouth, limbs, and head to the drawings rather than drawing a stick figure.[8] Hence, we have taken the age group between 6 and 12 years for our study. Drawings made by children are useful nonverbal assessment tool reflecting their inner mental thoughts. Various studies have used drawings for the evaluation of dental anxiety. Results of these studies have shown that drawings are natural projective tool for expressing distress, fear and anxiety of children.[9,10,11] Children can draw their feelings without undergoing any special training. The materials required for drawing are inexpensive and easily available. Children in our study enjoyed drawing the person in the dental clinic. They spent 6 min on an average for drawing. In our study we used CD: H scoring guide, score sheet and rating scale for the assessment of the drawings. Clatworthy et al. have proven the internal validity of this tool in their study on hospitalized children.[7] The evaluation of our children's drawings showed that 14 children (6 boys and 8 girls, mean CD: H score was 90.42 ± 14.26) had average stress, 87 children (43 boys and 44girls, mean CD: H score was 140.42 ± 24.17) had above average stress and 19 (10 boys and 9 girls, mean CD: H score was 170.27 ± 14.32) had very high stress. We have used a combination of objective (Frankl Rating Scale) and subjective methods (Five Facial Anxiety Scale and CD: H) for the assessment of dental anxiety. CD: H scales used for measuring the dental anxiety in previous studies have shown a significant correlation with Frankl and Sound, Eye, and Motor scores. In this study, we have used Five Facial Anxiety Scale along with Frankl Rating Scale. We found a significant correlation between the CD: H score, Frankl, and Five Facial anxiety scores. Studies analyzing the children's perception regarding dental treatment with the help of their drawings have reported that children were comfortable to use drawings as self-projective tool for expressing their emotions.[12,13,14,15,16] These studies have also reported the drawings as the perfect method for portraying the distress, anxiety, and fear related to dental treatment. The assessment of drawings of children in our study also showed that the children were more comfortable expressing their feelings through drawings. Drawings are significant natural nonverbal tool for reporting their distress. This tool provides a significant amount of clinically relevant information which would help in understanding the inner mental world of the child.[17] We also found that this activity had a positive effect on the interpersonal relationship between the dentist and the child. In our study, we found no significant difference between the CD: H, Frankl and Five Facial Anxiety scores of girls and boys. These results were not in accordance with some studies in which the boys had higher scores than girls.[3,18,19,20]
Various studies have reported that art is a powerful method of communication of emotions that are difficult and painful to express verbally. There are various modalities of expressing the painful experience such as painting, drawing, sculpture, or collage. Art therapy provides a nonthreatening channel for expression of emotions. The expressed feelings are analyzed by the art therapists by transforming the art into tangible and concrete images thereby providing a fresh view of the person's conflicts and problems.[21] In our study, the children in the study group were provided with art therapy in the form of coloring pages and connecting the dots/numbers. Seventeen (28.33%) children in the study group had high anxiety and 33 (55%) had very high anxiety before administration of art therapy. Whereas in the control group, 20 (33.33%) children showed high level of anxiety, and 34 (56.67%) children exhibited very high level of anxiety. After receiving the art therapy only 3 (5%) children of the study group exhibited high anxiety in comparison to 39 (65%) children of the control group, who showed very high level of anxiety. These results clearly indicate that after administration of the art therapy to the study group, there was a significant reduction in the anxiety level as compared to the children in the control group. We did not find any significant association between the demographic variables and anxiety levels of the participants. This was in accordance with the results of previous studies.[22,23]
Limitations
In our study, the children made single drawing after the first treatment under local anesthesia. These drawings may be the reflection of the child's distress felt at the time of the dental treatment rather than his previous anxiety. Further studies are required to assess the anxiety of the children using drawings before the beginning of the dental treatment as well as after each treatment session.
Conclusion
Dental anxiety has an adverse effect in building a positive dental attitude in children. Children's drawings can be used to evaluate dental anxiety in a dental setting. Art therapy decreases dental anxiety in children and can be used effectively to improve their compliance.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to acknowledge clinical psychologist, Dr. Krishna Shinde, for evaluating the children's drawings.
References
- 1.Yadav A, Garg S, Shrivastava A, Gupta A, Dogra S, Joshi S. Child drawing: A projective tool for dental anxiety assessment. Int Healthc Res J. 2020;4:19–25. [Google Scholar]
- 2.Mathur J, Diwanji A, Sarvaiya B, Sharma D. Identifying dental anxiety in children's drawings and correlating it with Frankl's behavior rating scale. Int J Clin Pediatr Dent. 2017;10:24–8. doi: 10.5005/jp-journals-10005-1401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Clatworthy S, Simon K, Tiedeman ME. Child drawing: Hospital – An instrument designed to measure the emotional status of hospitalized school-aged children. J Pediatr Nurs. 1999;14:2–9. doi: 10.1016/S0882-5963(99)80054-2. [DOI] [PubMed] [Google Scholar]
- 4.Khokhar V, Gupta B, Kaur J. Evaluation of anxiety level of children aged 6 – 9 years during sequential dental visits using objective and subjective measures. EC Dent Sci. 2017;15:93–103. [Google Scholar]
- 5.Hagood MM. A correlational study of art-based measures of cognitive development: Clinical and research implications for art therapists working with children. Art therapy. J Am Art Ther Assoc. 2002;19:63–8. [Google Scholar]
- 6.Kaplan FF. Drawing assessment and artistic skill. Arts Psychother. 1991;18:347–52. [Google Scholar]
- 7.Clatworthy S, Simon K, Tiedeman M. Child drawing: Hospital manual. J Pediatr Nurs. 1999;14:10–8. doi: 10.1016/S0882-5963(99)80055-4. [DOI] [PubMed] [Google Scholar]
- 8.Porritt J, Buchanan H, Hall M, Gilchrist F, Marshman Z. Assessing children's dental anxiety: A systematic review of current measures. Community Dent Oral Epidemiol. 2013;41:130–42. doi: 10.1111/j.1600-0528.2012.00740.x. [DOI] [PubMed] [Google Scholar]
- 9.Al-Namankany A, Ashley P, Petrie A. The development of a dental anxiety scale with a cognitive component for children and adolescents. Pediatr Dent. 2012;34:e219–24. [PubMed] [Google Scholar]
- 10.Fawson S. Drawing development: Historical perspectives, developmental stages, current approaches. Psychol Educ Rev. 2009;33:1–9. [Google Scholar]
- 11.Aminabadi NA, Ghoreishizadeh A, Ghoreishizadeh M, Oskouei SG. Can drawing be considered a projective measure for children's distress in paediatric dentistry? Int J Paediatr Dent. 2011;21:1–12. doi: 10.1111/j.1365-263X.2010.01072.x. [DOI] [PubMed] [Google Scholar]
- 12.Guner Onur S, Tonguc Altin K, Demetgul Yurtseven B, Haznedaroglu E, Sandalli N. Children's drawing as a measurement of dental anxiety in paediatric dentistry. Int J Paediatr Dent. 2020;30:666–75. doi: 10.1111/ipd.12657. [DOI] [PubMed] [Google Scholar]
- 13.Wechsler SM, Schelini PW. Validity of human figure drawing for children's cognitive assessment. Aval Psicol. 2002;1:29–38. [Google Scholar]
- 14.Sheskin RB, Klein H, Lowental U. Assessment of children's anxiety throughout dental treatment by their drawings. ASDC J Dent Child. 1982;49:99–106. [PubMed] [Google Scholar]
- 15.Madden JR, Mowry P, Gao D, Cullen PM, Foreman NK. Creative arts therapy improves quality of life for pediatric brain tumor patients receiving outpatient chemotherapy. J Pediatr Oncol Nurs. 2010;27:133–45. doi: 10.1177/1043454209355452. [DOI] [PubMed] [Google Scholar]
- 16.Skybo T, Ryan-Wenger N, Su YH. Human figure drawings as a measure of children's emotional status: Critical review for practice. J Pediatr Nurs. 2007;22:15–28. doi: 10.1016/j.pedn.2006.05.006. [DOI] [PubMed] [Google Scholar]
- 17.Hamama L, Ronen T. Children's drawings as a self-report measurement. Child Fam Soc Work. 2009;14:90–102. [Google Scholar]
- 18.Krishnappa S, Srinath S, Vishwanath SK, Bhardwaj P, Singh R. Evaluation of facial image scale and Venham picture test used to assess dental anxiety in children. J Indian Assoc Public Health Dent. 2013;11:31–5. [Google Scholar]
- 19.Olivera CA, Gama TS, Cabral EL, Figueiredo CH, Guênes GM, Penha ES, et al. Anxiety presented by children facing dental treatment. RGO Rev Gaúch Odontol. 2018;66:212–8. [Google Scholar]
- 20.Assuncão CM, Losso EM, Andreatini R, de Menezes JV. The relationship between dental anxiety in children, adolescents and their parents at dental environment. J Indian Soc Pedod Prev Dent. 2013;31:175–9. doi: 10.4103/0970-4388.117977. [DOI] [PubMed] [Google Scholar]
- 21.Habahbeh N, Al-Saddi R, Al-Far M. The relationship between dental anxiety and reported dental treatment experience in children aged 11 to 14 years. JRMS. 2012;19:44–50. [Google Scholar]
- 22.Raja GH, Malik FS, Bashir U, Attaullah M. Dental anxiety among children of age between 5 to 10 years visiting a teaching dental hospital in Islamabad, Pakistan. J Ayub Med Coll Abbottabad. 2015;27:587–90. [PubMed] [Google Scholar]
- 23.Paryab M, Hosseinbor M. Dental anxiety and behavioral problems: A study of prevalence and related factors among a group of Iranian children aged 6-12. J Indian Soc Pedod Prev Dent. 2013;31:82–6. doi: 10.4103/0970-4388.115699. [DOI] [PubMed] [Google Scholar]