

Sir,
Pleuropericardial cysts (PPCs) are rare benign anomalies of the anterior and middle mediastinum. It accounts for 5%–10% of all mediastinal tumors with an incidence of 1:100,000 population.[1] Although all ages can be affected, they have been commonly reported in middle-aged adults and rarely in children.[2] It is usually congenital and most patients are asymptomatic (75%). However, two-thirds of children are symptomatic[3] due to compression or invasion of adjacent organs dominated by respiratory signs.
A 3-year-old girl was admitted with complaints of cough, fever, and coryza for 7 days. The child had a history of recurrent lower respiratory tract infections in the past year. At admission, she was febrile, tachycardic, and tachypneic, with normal blood pressure and saturation at room air. On examination, there was bilateral wheeze and crepitations, and heart sounds were muffled. Hematologic investigation revealed leukocytosis with high C-reactive protein which was suggestive of infection, but the blood culture was negative, and biochemical profiles were within the normal limits. Chest X-ray showed mediastinal widening with no cardiomegaly [Figure 1]. The child was started on antibiotics with nebulization and other supportive management. Transthoracic echocardiography was suggestive of pyopericardium with adequate biventricular function and no signs of cardiac tamponade. Contrast-enhanced computed tomography (CT) of the chest revealed a hypodense lesion of 20–40 Hounsfield unit with a well-defined margin in the left paracardiac region closely adherent to the pericardium [Figure 2a and b] which was likely a pericardial cyst. The child was operated on for cyst removal and intraoperative findings were suggestive of an 8 cm × 8 cm cyst [Figure 3] containing greenish color fluid from the aortic arch up to the apex of the heart. Pericardial fluid was exudative and the histopathology report showed a cyst lined by flattened, attenuated denuded epithelium with no features suggestive of infection. The wall of the cyst also showed dilated lymphatic spaces lined by thinned to attenuated endothelial cells along with altered fibromuscular stroma which was suggestive of a benign cystic lesion. The child was discharged after an uneventful postoperative period and is doing well after 6 months of follow-up.
Figure 1.

Chest X-ray showing mediastinal widening
Figure 2.
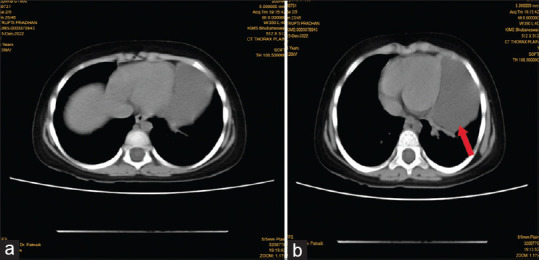
(a and b) Computed tomography scan appearance of the cyst well-defined hypodense lesion in left paracardiac region closely adherent to pericardium with extensions (marked as arrow)
Figure 3.
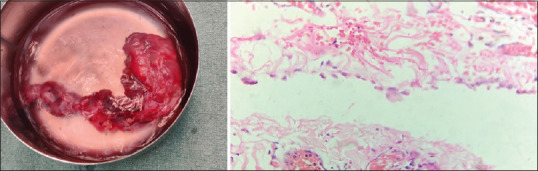
Histopathology image showing cyst lined by flattened, attenuated to cuboidal denuded epithelium focally showing microvilli. The wall of the cyst was fibrous with also showed congested capillaries, dilated lymphatics, and patchy lymphoid aggregates. Magnification value: 20–40
Reports of pericardial cysts in children have been scarce with <20 cases reported worldwide in children <18 years.[4] The most frequent location of PPC is the right cardiophrenic angle (51%–75%), followed by the left but in this case, the cyst was located in the left paracardiac region. Most of cysts are diagnosed by transthoracic echocardiography; however, a CT scan is considered the best modality for the diagnosis.
The therapeutic approach depends on the symptomatology and size, shape, and compressive nature of the cyst. In asymptomatic patients, management is conservative but symptomatic patients with large cysts need surgical resection, percutaneous aspiration of cyst, or video-assisted thoracoscopic surgery. The recurrence rate of pericardial cysts after aspiration is about 33%. The prognosis is excellent, even spontaneous resolution of lesions has been reported.[5] This case was a diagnostic dilemma because of its unusual presentation. Clinicians should be aware of this rare entity and its unusual presentation so that the diagnosis is not missed.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Patel J, Park C, Michaels J, Rosen S, Kort S. Pericardial cyst:Case reports and a literature review. Echocardiography. 2004;21:269–72. doi: 10.1111/j.0742-2822.2004.03097.x. [DOI] [PubMed] [Google Scholar]
- 2.Nina VJ, Manzano NC, Mendes VG, Salgado Filho N. Giant pericardial cyst:Case report. Rev Bras Cir Cardiovasc. 2007;22:349–51. doi: 10.1590/s0102-76382007000300013. [DOI] [PubMed] [Google Scholar]
- 3.Hekmat M, Ghaderi H, Tatari H, Arjmand Shabestari A, Mirjafari SA. Giant Pericardial cyst:A case report and review of literature. Iran J Radiol. 2016;13:e21921. doi: 10.5812/iranjradiol.21921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Noyes BE, Weber T, Vogler C. Pericardial cysts in children:Surgical or conservative approach? J Pediatr Surg. 2003;38:1263–5. doi: 10.1016/s0022-3468(03)00285-9. [DOI] [PubMed] [Google Scholar]
- 5.Moffa AP, Stoppino LP, Loizzi D, Milillo P. Spontaneous disappearance of a pericardial cyst:Case report and literature review. Korean J Thorac Cardiovasc Surg. 2018;51:72–5. doi: 10.5090/kjtcs.2018.51.1.72. [DOI] [PMC free article] [PubMed] [Google Scholar]