

Abstract
Objective: Infertility is a complex condition that depends on numerous mechanisms regarding its occurrence and evolution. It does not appear as a single pathology, and therefore the diagnosis and management involve both the identification of etiological causes and other possible systemic interactions.
Infertility is defined as a succession of unsuccessful attempts of unprotected intercourse within a couple for 12 months, during the reproductive life. Among the many causes related to infertility, uterine pathology has an important place and hysteroscopy is outstanding in diagnosing and treating various pathologies in this category.
Material and methods: This descriptive study was conducted on a retrospective analysis of a group of patients from Bucur Clinical Hospital, Bucharest, Romania. The main data were obtained from medical electronic records and included the type of infertility, associated diagnoses and symptoms, previous investigations, hysteroscopic procedure and follow-up. In order to obtain the database, the above parameters were evaluated and processed in the IBM SPSS Statistics version 28, including other few graphs processed in Microsoft Office Excel 2007.
Results:The present study included 51 patients aged between 20 and 40 years, with a mean of 32.02 ± 3.7. Out of the total number of patients, 76.47% of participants to the present study were diagnosed with secondary infertility and 58.82% described menometrorrhagias as the most common symptom. Endometrial polyps were more frequently associated with menometrorrhagias (70% of patients), while synechiae and secondary amenorrhea were found together in 75% of cases. Previous ultrasound evaluation identified uterine cavity abnormalities as nonhomogeneous echo-pattern in 58.82% of cases, with some of them being suggestive of endometrial polyps (37.25%), intrauterine synechiae (3.92%) and uterine fibromas (9.8%). We noticed that 12% of cases required laparoscopy and 4% laparotomy. The outcomes of hysteroscopic management resulted in a conception rate of 39%. We found that 20% of pregnancies achieved were complicated with placenta praevia, 5% with gestational hypertension and 15% with imminence of abortion.
Conclusions:Secondary infertility was more frequently encountered than primary infertility and the most common associated manifestations included menometrorrhagia, followed by secondary amenorrhea and pelvic-abdominal pain. Transvaginal ultrasound was correlated with hysteroscopic diagnosed pathology; posthysteroscopic results were favourable, regardless of the size and location of changes in the uterine cavity, thus highlighting the importance of hysteroscopic therapeutic techniques in increasing the chances of conception.
Keywords:infertility, hysteroscopy, pathology, symptoms, young women.
INTRODUCTION
Infertility is a complex condition that depends on numerous mechanisms regarding its occurrence and evolution. It does not appear as a single pathology, and therefore the diagnosis and management involve both the identification of the etiological causes and other possible systemic interactions (1). It is a health problem characterized by failure to achieve pregnancy after 12 months of regular unprotected intercourse (2).
Globally, infertility affects between 8 and 12% of couples of reproductive age and it is increasingly caused by women related factors, particularly in developed countries, where the tendency to delay pregnancy beyond 35 years significantly reduces the chances of fertility (3). Fertility decline with increasing age is linked to a gradual decrease in the number of primordial follicles (4). Understanding the mechanisms underlying the decline in fertility and ovarian function, associated conditions including primary ovarian failure and menopause, it is essential to manage premature oestradiol deficiency (5). Men are also found to contribute to 50% of all infertility cases (6).
All emotional and psychological implications associated with the diagnosis of infertility, including feelings of isolation, powerlessness and loss of control, are felt more intensely by women. There is an overwhelming stigma attached in both family and cultural contexts (7, 8).
The secondary infertility refers to a woman's inability to get pregnant after previously conceiving or having a baby (9). Causes of secondary infertility in women include age, endometriosis, tubal pathology related or not to high genital infections, polycystic ovary syndrome, excessive weight gain, emotional factors and many other causes. Another factor is uterine pathology, which is involved in about 10-15% of cases (10).
Diagnostic or operative hysteroscopy plays a major role in the evaluation of the uterine cavity and it is a very important method of assessing causes of uterine origin (11). The first hysteroscopic investigation was performed in 1869 for a 60-year-old patient with metrorrhagia. The first cauterization of an intrauterine polyp with silver nitrate was also performed during the same operation. This was the starting point of the technique that today has become indispensable. The main indications include the investigation of infertility, abnormal bleeding in pre- or post-menopausal periods, secondary amenorrhea, hormonal treatments and intracavitary polyps or fibromas (12). Infertility is a feasible indication for this investigation because hysteroscopy can provide accurate information and can treat many pathologies at the same time (13).
The aim of the study was to identify the particularities of hysteroscopy performed for infertility. The objectives of the study were the observation of the most common clinical manifestations and pathologies associated with infertility and the evaluation of the results obtained after hysteroscopy.
MATERIAL AND METHODS
This descriptive study was conducted on a retrospective analysis of a group of patients from Bucur Clinical Hospital, Bucharest, Romania. The data was randomized from the hospital record by searching for patients with infertility who underwent hysteroscopy. The following parameters were collected: personal data (age, parity, history), duration of hospitalization, main and secondary diagnosis, associated symptoms, ultrasound images or other imaging data, hysteroscopy and surgical technique, other investigations and procedures, complications and results of hysteroscopy.
The inclusion criteria were formulated using infertility as the primary diagnosis and hysteroscopy as the diagnostic or operative procedure.
The exclusion criteria consisted of partial or total lack of data to complete the parameters.
All parameters were evaluated and processed in IBM SPSS Statistics software, version 28. Quantitative variables were expressed by mean ± standard deviation (SD). Statistical results were generated using histograms, pie charts, bar or line graphs and tables, adding to the processing graphs obtained with Microsoft Office Excel 2007.
RESULTS
The study included 51 patients diagnosed with primary or secondary infertility after having been examined at Bucur Clinical Hospital, Bucharest, Romania, who met the inclusion and exclusion criteria and underwent hysteroscopy.
The main diagnosis was formulated as primary infertility or secondary infertility. The number of patients with primary infertility was significantly lower than that of subjects with secondary infertility (23.53% versus 76.47%, respectively) (Figure 1).
Many of patients did not attend our clinic for infertility but for symptoms such as amenorrhea, pelvic pain, menorrhagia or metrorrhagia. The symptoms were not present in all participants to the current study; some of them came to hospital without any symptoms, their only problem being the impossibility to achieve a spontaneous pregnancy. Out of the total of 30 patients with menometrorrhagia (58.8% of all study subjects), 25 (83.3%) had secondary infertility, five (16,6%) other women associated pelvic pain and other two (6,6%) amenorrhea. In contrast, primary infertility was more common in asymptomatic women (Figure 2).
Gynaecological ultrasound offers the opportunity to examine patients and correlate clinical findings. Proximity of pelvic anatomy through the vaginal approach provides an improved image resolution. The pelvic ultrasonography was performed in all cases, and 41 of them did not associate other investigations besides hysteroscopy (80.4%). Hysterosalpingography was performed in four cases (7.8%), MRI in three other ones (5.9%) and chromosalpingography also in three patients (Table 1).
The total number of cases were evaluated sonographically with non-homogeneous intracavitary endometrial formation, 37.25% were images suggestive of endometrial polyps; 17.65% of patients were diagnosed with polyps only hysteroscopically without ultrasound diagnosis. Intrauterine synechia was also identified ultrasonographically in 3.92% of cases, showing a homogeneous endometrial structure in 9.80% of cases (Table 2).
Tubal pathologies such as hydrosalpinx, pelvic inflammatory disease, endometriosis, history of tubal ectopic pregnancy or previous tubal surgery were described only in patients with secondary infertility; one case of infertility caused by intrauterine foreign body was also described. Ovarian dysfunction was associated with the diagnosis of primary infertility; 24 out or 28 patients (85.71%) with endometrial polyps had secondary infertility, while five out of seven subjects (71.42%) with intrauterine synechiae had primary infertility (Table 3).
Once the cause of infertility was treated, the outcome was expected. The pregnancy outcome could not be identified in 14 of the 51 patients (27.45%) included in the study group; according to data analysed by us, 20 patients (39%) achieved at least one pregnancy, while the other 17 women (33%) did not (Figure 3).
In the cases with polyp sizes < 10 mm, almost 40% of patients did not have a favorable response in terms of pregnancy outcome, while almost 20% of subjects succeeded. For the next interval, 10-15 mm, more than 60% of patients become pregnant and 23% of study participants not. The number of women with uterine polyps >15 mm who did not get pregnant was double that of those with pregnancy obtained after hysteroscopy (Figure 4).
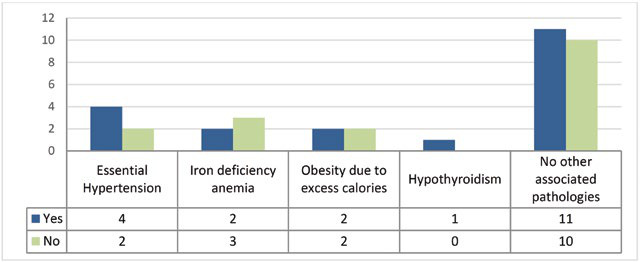
Among women who achieved at least one pregnancy, there were 11 cases (55%) with no underlying condition, four patients (20%) with essential hypertension, two subjects with iron deficiency anemia (10%) and two women (10%) with obesity due to excess calories (Table 4).
During pregnancy follow-up, four cases (20%) were complicated by placenta praevia, while three cases (15%) had an episode of imminent abortion and 5% of subjects developed gestational hypertension (Figure 5).
DISCUSSION
An important role in fertility is played by psychoemotional and nutritional factors. A study found in the literature refers to the Holocaust and shows that the Nazis sought methods of sterilizing Jewish women. Immediately after arriving in the concentration camps, more than 98% of women stopped menstruating. There is minimal information on the causes of amenorrhea other than malnutrition and trauma (14, 15). Ninety-three testimonies were collected from female Holocaust survivors or their descendants, which revealed that 98% of all interviewed women failed to conceive or carry a pregnancy to term. Amenorrhea among Jewish women in concentration camps was linked to trauma and/or malnutrition, but the role of exogenous hormones administered without the women's knowledge was not excluded (16, 17).
Tuberculosis, an infectious disease caused by Mycobacterium tuberculosis, is a major health problem in underdeveloped countries (18) but also a cause of infertility. Female genital tuberculosis is known as a disease of young women (20-40 years) (19, 20), usually diagnosed during infertility evaluations (21, 22). Infertility is the most common condition, occurring due to irreversible damage, and the organs commonly affected by genital tuberculosis are the fallopian tubes (90%) (23), ovaries (10-30%), endometrium (50%), cervix and vagina (24).
The type of infertility depends on the age intervals of women at reproductive age. In our study, age limits varied between 20 and 40 years, with a mean of 32.02 ± 3.7. Of these, 76.47% were diagnosed with secondary infertility, compared to 23.53% with primary infertility. Analysis of data from the Global Burden of Disease Study showed that women aged 20 to 24 years were comprised in the group with the lowest infertility rates (3%). But the group of women aged 35-39 had the highest infertility rates (5.5%) (25). The prevalence of infertility increases with age (26).
Regarding the most frequent clinical associations attributed to infertility in all study participants, 58.82% described menometrorrhagia as a significant change in reproductive life, followed by secondary amenorrhea and pelvic-abdominal pain. The most relevant associations were found between uterine synechiae and secondary amenorrhea (75%) as well as endometrial polyps that presented with menometrorrhagia (70%). Data from the literature support the increased prevalence of synechiae ranging from 0.3% to 21.5%, with a reduced diagnostic rate given that in most cases they do not show clinical manifestations (27). Menometrorrhagia is often determined separately from the diagnosis of infertility (28), and it is associated with other pathologies; some studies show that about 16% are associated with infertility, bleeding and intrauterine pathology (29). In our study, menometrorrhagia occurred in 58.82% of subjects.
Infertility associated medical conditions include essential hypertension, obesity, hypothyroidism, anemia and hyperprolactinemia. In most cases, patients do not show any associated pathologies. In the absence of patient data on BMI and lifestyle, associations of these conditions and infertility are difficult to identify. Iron deficiency anemia can be explained by excessive blood loss caused by menometrorrhagia or in the context of chronic inflammation (30). This chronic inflammation may explain hypertension if it is associated with tubal pathology and implicitly with sexually transmitted diseases (31). Hypothyroidism is also involved in embryo implantation and development, especially in the presence of antibodies; it is also a cause of anovulation, as is hyperprolactinemia (32).
Polyps and their influence on infertility have been a topic of research for which many findings support the hypothesis that the rate of infertility increases as uterine deformity occurs (33). In our study group, the analysis regarding the size of the uterine polyps found 21 polyps <1.5 cm and seven polyps > 1.5 cm. During hysteroscopy, polypectomy and biopsy were performed for 20 of them, with the remaining semen being relevant for diagnostic hysteroscopy and endometrial biopsy. Also, there was one hysteroscopy procedure that ended with the inability of dilating the cervical canal. Data from various studies support the importance of polyps when their size increases by more than 1.5 cm, being relevant both for infertility and for the risk of malignancy (34). Polypectomy can increase fertility rates in women with endometrial polyps of various sizes. This was supported in a study that included women diagnosed with infertility and endometrial polyps who underwent hysteroscopic polypectomy prior to intrauterine insemination. It was found that polypectomy significantly improved the rate of achieving pregnancy from 28% to 63% (35, 36).
Ultrasound measurements did not lead to a favorable diagnosis rate. The aspects suggestive for uterine pathologies were identified by ultrasound as non-homogeneous endometrial pattern in a rate of 58.82%. In a study that followed the same parameters, ultrasound identified only 12.9% of the existent uterine pathology, of which the highest rate was attributed to synechiae (5.6%), followed by fibroids (3.3%) and polyps (only 2.2%). The major difference was that the study from the literature analysed a population of 870 patients (37).
The complication rate of hysteroscopy was 16% of all cases, 12% associated with laparoscopy and 4% with laparotomy. Three of these patients had a history of surgical intervention, other three women had gynaecological infections and two women associated malformations or uterine stenosis in their medical history. In literature, the most common causes leading to abdominal surgical procedures are hysteroscopic perforations, massive hemorrhages, obstacles that prevent the introduction of the vaginal hysteroscope, infections or absorption of administered fluids. A study that looked up for these complications in a larger group of patients found a rate of 0.76% perforations, 0.12% hemorrhagic events, 0.6% systemic infections and 0.9% urinary tract infections (38).
The outcome of obtaining a pregnancy was analysed in the study group, considering the significant complete data on 14 patients out of the 51 (27.45%). A conception rate of 39% was obtained following hysteroscopy procedures. Statistics have shown that the chances of becoming pregnant were higher in patients undergoing hysteroscopy than those who did not benefit from this procedure, even if only for diagnostic purposes (39).
In a study on 125 patients of which 65 had uterine polyps >2.5 cm, we were interested in subjects’ evolution after hysteroscopic polypectomy and noticed that 80% of all patients achieved a spontaneous pregnancy, with 70% of them having successful pregnancies (40, 35). There were no correlations between the sizes of the polyps and post-resection outcome. Similar results could be observed in our study too. It is important to note that in the case of polyps >1.5 cm, a double percentage of patients did not become pregnant after hysteroscopy. In women with endometrial polyps and irregular menstrual cycles, without any other diagnosed cause, studies show that fertility rates are significantly improved after polypectomy (41, 42).
The analysis of patients who obtained the pregnancy showed no complications in 60% of cases. Complications included placenta praevia in 20% of pregnancies, followed by imminent abortions in 15% of cases and gestational hypertension in 5% of pregnant subjects, with the resulting 40% of evolving complications being also relevant compared to the literature. Another study conducted for this purpose described a 42.6% rate of complications such as gestational diabetes or pre-eclampsia (43).
CONCLUSIONS
Secondary infertility was more frequent than primary infertility and the most commonly associated manifestations included menometrorrhagia, followed by secondary amenorrhea and pelvic-abdominal pain.
The most common uterine pathology associated with infertility was the endometrial polyp; uterine polyps and fibroids have been most frequently associated with secondary infertility. Endovaginal ultrasound was correlated with hysteroscopic diagnosed pathology; post-hysteroscopic results were favourable regardless of the size and location of changes in the uterine cavity, thus highlighting the importance of hysteroscopic therapeutic techniques in increasing the chances of conception.
Hysteroscopy is the main investigation of the uterine cavity. Its importance has been highlighted by its diagnostic and treatment techniques, including polypectomy, synecholysis, foreign body extraction, and biopsy. This approach has a favorable impact on future pregnancies because positive results are seen in most cases where diagnosis and treatment of the existing pathologies was done accurately.
Conflicts of interest: none declared.
Financial support: none declared.
FIGURE 1.
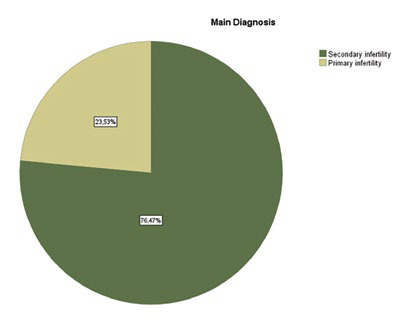
Types of infertility
FIGURE 2.
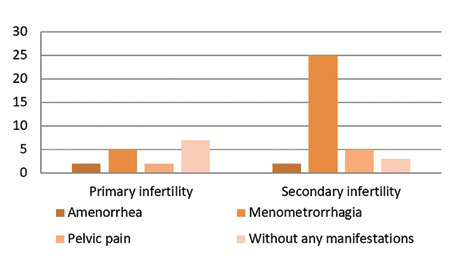
Symptoms in women with infertility
TABLE 1.
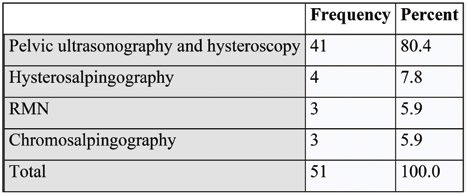
Investigations performed in the current study
TABLE 2.
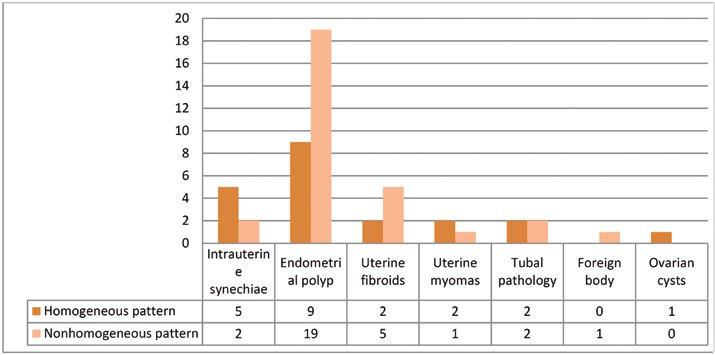
Correlation between ultrasonography and hysteroscopy findings
TABLE 3.
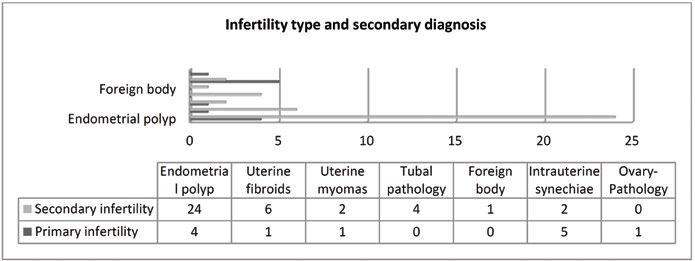
Associated pathologies according to the type of infertility
TABLE 4.
Representative images after binarization of the macular area at the choriocapillaris plexus indicating the perfused area of a female in preterm (a) and full-term (b) pregnancy
FIGURE 3.
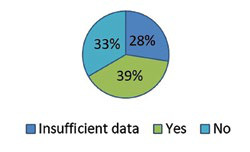
Pregnancy outcome
FIGURE 4.
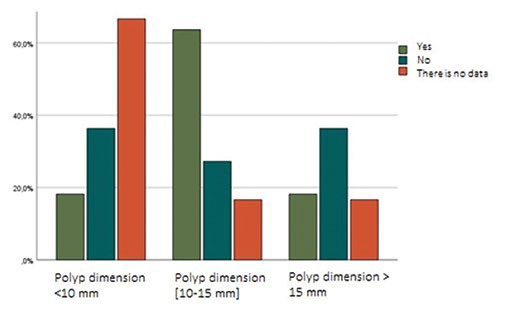
Pregnancy outcome related to the size of endometrial polyps
FIGURE 4.
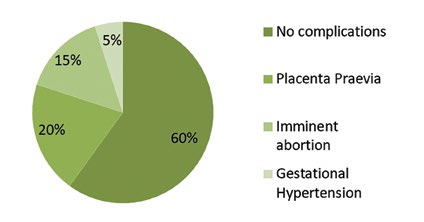
Complications during pregnancy
Contributor Information
Cristina Diana POPESCU, IOSUD/PhD Department, ”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania; Department of Obstetrics and Gynaecology, “St John” Hospital, “Bucur” Maternity, Bucharest, Romania; ”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania.
Romina-Marina SIMA, Department of Obstetrics and Gynaecology, “St John” Hospital, “Bucur” Maternity, Bucharest, Romania; ”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania.
Mihaela AMZA, IOSUD/PhD Department, ”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania; Department of Obstetrics and Gynaecology, “St John” Hospital, “Bucur” Maternity, Bucharest, Romania; ”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania.
Tina Ioana BOBEI, IOSUD/PhD Department, ”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania; Department of Obstetrics and Gynaecology, “St John” Hospital, “Bucur” Maternity, Bucharest, Romania; ”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania.
Silvia CIRSTOIU, ”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania.
Liana PLES, Department of Obstetrics and Gynaecology, “St John” Hospital, “Bucur” Maternity, Bucharest, Romania; ”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania.
References
- 1.Matzuk MM, Lamb DJ. The biology of infertility: research advances and clinical challenges. Nat Med. 2008;14:1197–213. doi: 10.1038/nm.f.1895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vander Borght M, Wyns C. Fertility and infertility: Definition and epidemiology. Clin Biochem. 2018;62:2–10. doi: 10.1016/j.clinbiochem.2018.03.012. [DOI] [PubMed] [Google Scholar]
- 3.Vander Borght M, Wyns C. Fertility and Infertility: Definition and Epidemiology. Clin Biochem. 2018;62:2–10. doi: 10.1016/j.clinbiochem.2018.03.012. [DOI] [PubMed] [Google Scholar]
- 4.Eshre Guideline. Management of Women with Premature Ovarian Insufficiency. Hum Reprod. 2016;31:926–937. doi: 10.1093/humrep/dew027. [DOI] [PubMed] [Google Scholar]
- 5.Marongiu M, Crisponi L, Uda M, Pelosi E. Editorial: Female Infertility: Genetics of Reproductive Ageing, Menopause and Primary Ovarian Insufficiency. Front Genet. 20229;13:839758. doi: 10.3389/fgene.2022.839758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Foran D, Chen R, Jayasena CN, et al. The use of hormone stimulation in male infertility. Curr Opin Pharmacol. 2023;68:1471–4892. doi: 10.1016/j.coph.2022.102333. [DOI] [PubMed] [Google Scholar]
- 7.Bhamani SS, Zahid N, Zahid W, et al. Association of depression and resilience with fertility quality of life among patients presenting to the infertility centre for treatment in Karachi, Pakistan. BMC Public Health. 2020;20:1–11. doi: 10.1186/s12889-020-09706-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Vander Borght M, Wyns C. Fertility and infertility: Definition and epidemiology. Clin Biochem. 2018;62:2–10. doi: 10.1016/j.clinbiochem.2018.03.012. [DOI] [PubMed] [Google Scholar]
- 9.Ghaffari F, Arabipoor A. The role of conception type in the definition of primary and secondary infertility. Int J Reprod Biomed. 2018;16:355–356. [PMC free article] [PubMed] [Google Scholar]
- 10.Brosens I, Gordts S, Valkenburg M, et al. Investigation of the infertile couple: when is the appropriate time to explore female infertility? Hum Reprod. 2004;19:1689–1692. doi: 10.1093/humrep/deh314. [DOI] [PubMed] [Google Scholar]
- 11.Bettocchi S, Nappi L, Ceci O, Selvaggi L. What does ‘diagnostic hysteroscopy’ mean today ? The role of the new techniques. Curr Opin Obstet Gynecol. 2003;15:303–308. doi: 10.1097/01.gco.0000084241.09900.c8. [DOI] [PubMed] [Google Scholar]
- 12.Cholkeri-Singh A, Jill K. Hysteroscopy safety. Curr Opin Obstet Gynecol. 2016;28:250–254. doi: 10.1097/GCO.0000000000000289. [DOI] [PubMed] [Google Scholar]
- 13.Bettocchi S, Achilarre MT, Ceci O, Luigi S. Fertility-Enhancing Hysteroscopi Surgery 2011. [DOI] [PubMed]
- 14.Alfred Pasternak, Philip G. Brooks, The long-term effects of the Holocaust on the reproductive function of female survivors. Journal of Minimally Invasive Gynecology. 2007;2:211–217. doi: 10.1016/j.jmig.2006.10.026. [DOI] [PubMed] [Google Scholar]
- 15.Sjoerd GE, van Noord PAH, Peeters PHM, et al. Grobbee,Menstruation during and after caloric restriction: The 1944–1945 Dutch famine. Fertil Steril 2007. [DOI] [PubMed]
- 16.Kleinplatz PJ, Weindling P. Women's experiences of infertility after the Holocaust. Soc Sci Med. 2022;309:115250. doi: 10.1016/j.socscimed.2022.115250. [DOI] [PubMed] [Google Scholar]
- 17.Pasternak A, Brooks PG. The long-term effects of the Holocaust on the reproductive function of female survivors. J Minim Invasive Gynecol. 2007;14:211–217. doi: 10.1016/j.jmig.2006.10.026. [DOI] [PubMed] [Google Scholar]
- 19.Shrivastava G, Patel K. Genital tuberculosis: Evaluating microscopy, culture, histopathology and PCR for diagnosis all play their role. Int J Curr Microbiol App Sci. 2014;3:439–445. [Google Scholar]
- 20.Mohakul SK, Beela VRK, Tiru P. Hysteroscopy findings and its correlation with latent endometrial tuberculosis in infertility. Gynecological Surgery. 2015;12:31–39. [Google Scholar]
- 21.Fatima T, Hasan R, Malik FR, et al. Female genital tuberculosis in Pakistan – A retrospective review of 10-year laboratory data and analysis of 32 cases. Int J Mycobacteriol. 2021;10:66–70. doi: 10.4103/ijmy.ijmy_6_21. [DOI] [PubMed] [Google Scholar]
- 22.Grace GA, Devaleenal DB, Natrajan M. Genital tuberculosis in females. Indian J Med Res. 2017;145:425–436. doi: 10.4103/ijmr.IJMR_1550_15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Namavar Jahromi B, Parsanezhad ME, Ghane-Shirazi R. Female genital tuberculosis and infertility. Int J Gynaecol Obstet. 2001;75:269–272. doi: 10.1016/s0020-7292(01)00494-5. [DOI] [PubMed] [Google Scholar]
- 24.Abebe M, Lakew M, Kidane D, et al. Female genital tuberculosis in Ethiopia. Int J Gynaecol Obstet. 2004;84:241–246. doi: 10.1016/j.ijgo.2003.11.002. [DOI] [PubMed] [Google Scholar]
- 25.Sun H, Gong TT, Jiang YT, et al. Global, regional, and national prevalence and disability-adjusted life-years for infertility in 195 countries and territories, 1990-2017: results from a global burden of disease study, 2017. Aging (Albany NY) 2019. [DOI] [PMC free article] [PubMed]
- 26.Snow M, Vranich TM, Perin J, Trent M. Estimates of infertility in the United States: 1995-2019. Fertil Steril. 2022;118:560. doi: 10.1016/j.fertnstert.2022.05.018. [DOI] [PubMed] [Google Scholar]
- 27.Khan Z, Goldberg JM. Hysteroscopic Management of Asherman’s Syndrome. J Minim Invasive Gynecol [Internet] 2018. [DOI] [PubMed]
- 28.Tariq R, Al-Fareed Z, Mehvish I, et al. PREVALENCE OF DYSFUNCTIONAL UTERINE BLEEDING IN PATIENTS WITH SUB FERTILITY. Pakistan Postgraduate Medical Journal 2021.
- 29.Sacha CR, Souter I. Abnormal Uterine Bleeding in Women with Infertility. Current Obstetrics and Gynecology reports. 2017;6:42–50. [Google Scholar]
- 30.Dishuck CF, Perchik JD, Porter KK, Gunn DD. Advanced Imaging in Female Infertility. Curr Urol Rep. 2019;20:0. doi: 10.1007/s11934-019-0942-0. [DOI] [PubMed] [Google Scholar]
- 31.Farland L V, Sc M, Grodstein F, et al. Of hypertension. Fertil Steril [Internet] 2011.
- 32.Hart RJ. Physiological aspects of female fertility: Role of the environment, modern lifestyle, and genetics. Physiol Rev. 2016;96:873–909. doi: 10.1152/physrev.00023.2015. [DOI] [PubMed] [Google Scholar]
- 33.Pritts EA, Parker WH, Olive DL. Fibroids and infertility: an updated systematic review of the evidence. Fertil Steril [Internet] 2009. [DOI] [PubMed]
- 34.Nijkang NP, Anderson L, Markham R, Manconi F. Endometrial polyps: Pathogenesis, sequelae and treatment. SAGE Open Med. 2019;7:2050312119848247. doi: 10.1177/2050312119848247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Pérez-Medina T, Bajo-Arenas J, Salazar F, et al. Endometrial polyps and their implication in the pregnancy rates of patients undergoing intrauterine insemination: a prospective, randomized study. Hum Reprod. 2005;20:1632. doi: 10.1093/humrep/deh822. [DOI] [PubMed] [Google Scholar]
- 36.Coutifaris C, Myers ER, Guzick DS, et al. Histological dating of timed endometrial biopsy tissue is not related to fertility status. Fertil Steril. 2004;82:1264. doi: 10.1016/j.fertnstert.2004.03.069. [DOI] [PubMed] [Google Scholar]
- 37.Varlas V, Rhazi Y, Cloțea E, et al. Hysterolaparoscopy: A Gold Standard for Diagnosing and Treating Infertility and Benign Uterine Pathology. J Clin Med. 2021;10:3749. doi: 10.3390/jcm10163749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Stephen EH, Chandra A. Use of infertility services in the United States: 1995. Fam Plann Perspect. 2000;32:132–137. [PubMed] [Google Scholar]
- 39.Al-Quran F, Al-Fayez N, Qudah S. Spontaneous Pregnancy Rate after Hysteroscopic Removal of Endometrial Polyps in Infertility Patients: Experience at King Hussein Medical Center. J R Med Serv. 2018;25:27–31. [Google Scholar]
- 40.Stamatellos I, Apostolides A, stamatopoulos P, Bontis J. Pregnancy rates after hysteroscopic polypectomy depending on the size or number of the polyps. Arch Gynecol Obstet. 2008;277:395–399. doi: 10.1007/s00404-007-0460-z. [DOI] [PubMed] [Google Scholar]
- 41.Silberstein T, Saphier O, VanVoorhis BJ, Plosker SM. Endometrial polyps in reproductive-age fertile and infertile women. Isr Med Assoc J. 2006;8:192–195. [PubMed] [Google Scholar]
- 42.Lieng M, Istre O, Sandvik L, et al. Clinical effectiveness of transcervical polyp resection in women with endometrial polyps: a randomised controlled trial. J Minim Invasive Gynecol. 2010;17:351–357. doi: 10.1016/j.jmig.2010.01.019. [DOI] [PubMed] [Google Scholar]
- 43.Zhu X, Huang C, Wu L, et al. Perinatal Outcomes and Related Risk Factors of Single vs Twin Pregnancy Complicated by Gestational Diabetes Mellitus: Meta-Analysis. Comput Math Methods Med 2022. [DOI] [PMC free article] [PubMed]