

Abstract
Introduction:
The U.S. Preventive Services Task Force recommends clinicians screen children aged 6 years or older for obesity and offer or refer children with obesity to intensive weight management programs. This study explores clinician awareness of weight management programs meeting the recommendation, adherence to the recommendation of screening and referral, and associations between provider and practice characteristics and weight management program referrals.
Methods:
This cross-sectional study used data from the DocStyles survey 2017, a web-based panel survey, analyzed in 2017. Among 1,023 clinicians who see pediatric patients, this study examined clinician awareness of weight management programs in their communities that met the recommendation, practice of screening for childhood obesity, and referral to weight management programs. Multivariable logistic regression estimated associations between the demographic and practice characteristics of clinicians and weight management program referrals.
Results:
Only 24.6% of surveyed clinicians were aware of a weight management program that met the U.S. Preventive Services Task Force recommendation in their community; of those aware, 88.9% referred patients to these weight management programs. Most (83.6%) clinicians screened children for obesity in ≥75% of visits. Overall, 53.5% of clinicians provided referrals to weight management programs. Referral was higher among female clinicians and clinicians serving mostly middle-income patients. Providers without teaching hospital privileges had lower odds of referral.
Conclusions:
Adherence to clinical recommendations is essential to curbing the childhood obesity epidemic. Only one in four surveyed clinicians were aware of weight management programs in their community meeting U.S. Preventive Services Task Force criteria. Half of clinicians referred pediatric patients with obesity to a weight management program. Results suggest efforts are needed to increase awareness of, and referral to, weight management programs meeting the recommendation.
INTRODUCTION
About 18.5%, or 13.7 million, children in the U.S. are living with obesity (BMI equal to or greater than the 95th percentile for age and sex).1 Childhood obesity is associated with insulin resistance, dyslipidemia, hypertension, asthma, bullying, weight stigma, and multiple other medical and psychological sequelae.2−7 In 2017, the U.S. Preventive Services Task Force (USPSTF) recommended that clinicians screen all children aged 6 years and older for obesity, upholding its 2010 statement.8,9 Furthermore, USPSTF recommended that children and adolescents with obesity be offered or referred to a comprehensive, intensive behavioral intervention to improve weight status.8
The recommendation states these weight management programs (WMPs) should be multicomponent, family-centered, lifestyle-based weight management interventions.8 There was sufficient evidence to recommend moderate- to high-intensity comprehensive programs (moderate defined as 25 or more to fewer than 75 hours; high defined as 75 hours or more of child or family contact over at least a 2- to 12-month period).8,10−12 Such interventions lead to modest improvements in weight status within 12 months; a few reports suggest that results may be sustained for longer than a year.13,14 Reductions in BMI may improve blood pressure, hyper-lipidemia, and insulin resistance,15,16 as well as have positive benefits for psychological well-being.17
A challenge to clinicians is the paucity of WMPs that meet the USPSTF recommendation available to children and families who need them.11 Prior data used to formulate the 2010 recommendation indicated that fewer than half of pediatricians and family physicians knew of pediatric WMPs where they could refer patients.18 Little is known about the extent to which clinicians are currently implementing the recommendation by USPSTF. Such information would be valuable to support efforts in targeting clinician groups to promote adherence to the recommendation. Therefore, the study objectives are to (1) explore clinician awareness of WMPs specifically meeting USPSTF criteria, (2) determine clinician adherence to the USPSTF recommendation of screening children for obesity, and (3) examine referral to WMPs and characteristics associated with referral practices, among clinicians who see pediatric patients.
METHODS
This cross-sectional study used data from DocStyles survey 2017, a web-based panel survey of U.S. healthcare providers administered by Porter Novelli Public Services. The survey was designed to provide insights to healthcare provider behaviors regarding a variety of health issues.
Study Sample
Respondents were from the SERMO Global Medical Panel—a global market research provider.19 Panelists were verified using a double opt-in signup process with telephone confirmation at their workplace. Respondents were paid an honorarium of $23−$85 for completing the survey, based on the number of questions they were asked to complete. From the SERMO panel, Porter Novelli set sample size quotas that included 1,000 primary care physicians, 250 pediatricians, and 250 nurse practitioners, as well as 250 obstetrician/gynecologists, 250 oncologists, 150 retail pharmacists, and 100 hospital pharmacists. When comparing physician respondents from DocStyles survey 2017 to physicians in the American Medical Association Physician Master File, more survey respondents were male (69.6% vs 58.0%), slightly older (48.1 vs 47.0 years), and practiced for a shorter duration (17.6 vs 19.3 years); this is similar to the previous survey year.20 DocStyles survey 2017 was open from June 8 to August 9, 2017; the updated USPSTF childhood obesity recommendation was published on June 20, 2017, which upheld the previous recommendation in its 2010 statement.8,9
Eligibility criteria for DocStyles survey 2017 included healthcare professionals seeing patients within the U.S. for >3 years in an individual, group, or hospital practice. As depicted in Figure 1, the subset of pediatric obesity questions used in this analysis were asked only of pediatricians, internists, family practitioners, and nurse practitioners (n=1,509). Through the use of skip patterns, only respondents who reported seeing pediatric patients completed the section for this analysis (n=1,023). Of these, 918 responded to the question about screening children for obesity. Finally, 891 respondents answered questions about referral to WMP for childhood obesity. Compared with these 891, clinicians who had missing data did not differ significantly by demographics. However, they differed by specialty (higher proportion of internists and nurse practitioners) and work setting (higher proportion of inpatient clinicians). The Centers for Disease Control and Prevention licensed the results of the DocStyles 2017 survey post-collection from Porter Novelli, and analysis of these data was exempt from IRB approval because personal identifiers were not included in the data files. Results were analyzed in 2017.
Figure 1.
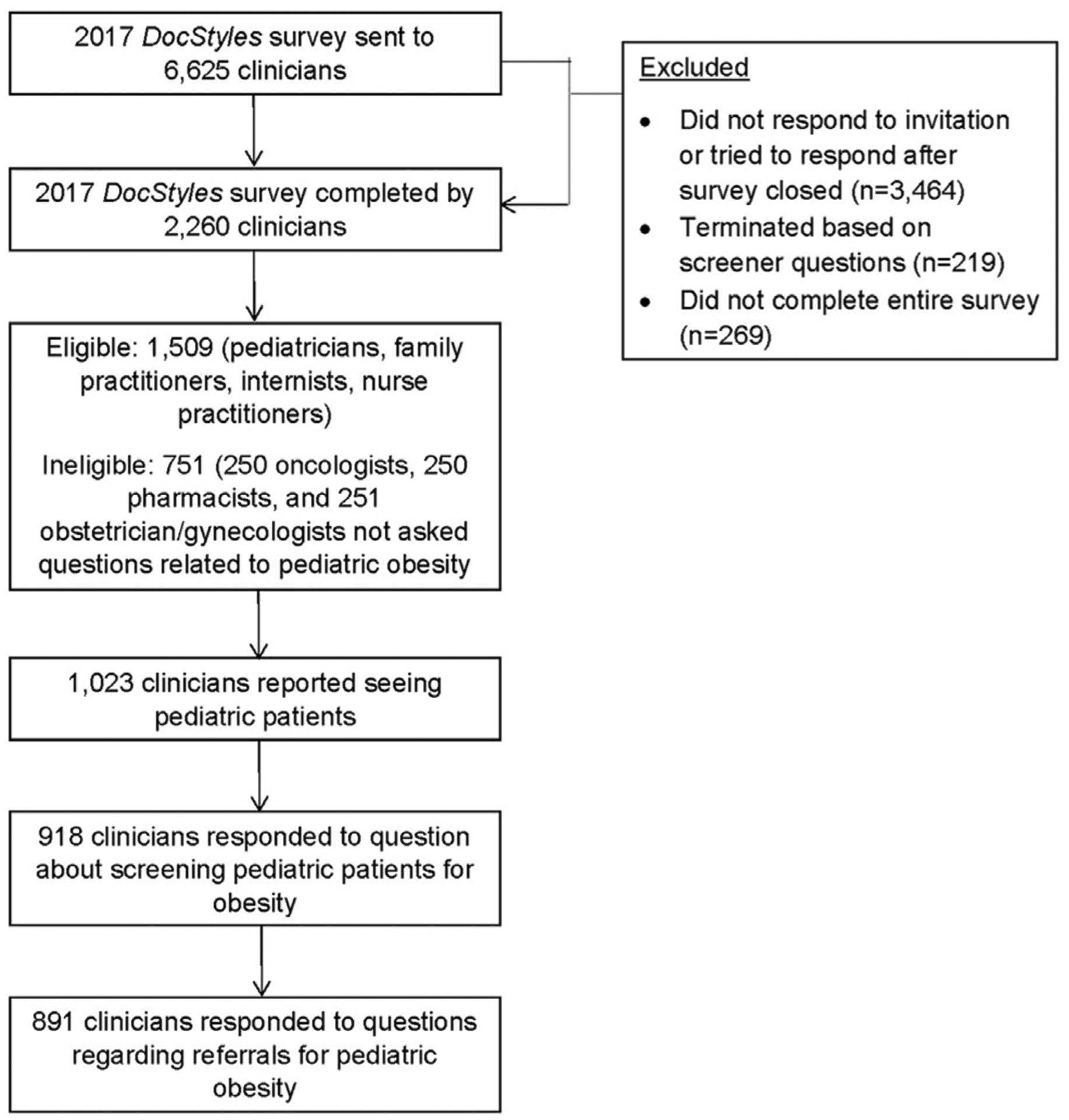
Analytic sample flow chart for DocStyles survey, 2017.
Measures
Respondents were asked about their awareness of and referral to WMPs specifically meeting USPSTF criteria. The query was phrased as: The current U.S. Preventative Services Task Force (USPSTF) Recommendations advise that children aged 6−18 years with obesity be referred to family-centered, weight management programs that provide >25 hours of nutrition and physical activity counseling and behavior change therapy over a 6-month period. Are you aware of any programs that meet the current USPSTF recommendations in the community that you serve? Possible responses included: yes, no, and don’t know. If yes was the response, the follow-up prompt was: Do you refer patients to this program(s)?, which had the same response options. Clinician screening for childhood obesity was assessed by asking: At approximately what percentage of your pediatric well-child visits do you screen for obesity using BMI-for-age and sex growth charts? Respondents were asked to provide a continuous variable (range, 0−100). The mean was calculated and also categorized data into four categories (<25%, 25% to <50%, 50% to <75%, and ≥75%).
These analyses were exploratory for the association between clinician, clinical practice, and clinician reported patient characteristics and the main outcome variable of referral to community or clinic-based WMPs. Clinicians were asked: What action(s) do you typically take for children with obesity (i.e., BMI ≥95th percentile) for the purpose of weight management? Response choices included: (1) Schedule a follow-up visit for obesity, or referral to (2) a subspecialty, such as endocrinology or gastroenterology; (3) a registered dietitian; (4) a behavioral/mental health professional; (5) a health educator/coach; (6) a community-based weight management program/organization (e.g., YMCA, Weight Watchers); and (7) to a clinic- or hospital-based weight management program/organization. Responses were categorized as yes or no. Choices 6 and 7 were combined into a single outcome variable of referral to a WMP, which is the focus of this study. An analysis of responses to Options 1−5 are explored in a separate study.
Covariates included provider, clinical practice, and reported patient characteristics. Provider characteristics included clinician age (<45 or ≥45 years), gender (male or female), and race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, non-Hispanic Asian, or non-Hispanic other/multiracial). Age categories were based on prior studies and respondent distribution. Clinical practice characteristics included census region location of the practice (Northeast, South, Midwest, West), medical specialty (family practice, internal medicine, pediatrics, nurse practitioner), primary work setting (inpatient [hospital], individual outpatient [solo clinic practice], group outpatient [clinic practice with more than one clinician]), teaching hospital privileges (yes or no), and number of well-child visits per week (less than five, five to 14, or ≥15 visits; initially reported as a continuous variable; categories were determined by distribution of responses). Patient characteristics were reported by clinicians. For patient household annual income, providers were asked to select the category that best described the approximate financial situation of the majority of their patients. Responses were grouped into three categories based on data distribution, and included low-income (<$50,000), middle-income ($50,000 to <$100,000), and high-income (≥$100,000). Clinicians also reported the percentage of their pediatric patients with obesity; based on data distribution these were categorized as <10%, 10% to <20%, 20% to <40%, and ≥40%.
Statistical Analysis
Statistical analyses were performed using SAS, version 9.4. Chi-square tests assessed the crude associations between reported referral to WMP and provider, clinical practice, and patient characteristics, with p<0.05 as the criterion for statistical significance. A multivariable logistic regression model estimated the AORs and 95% CIs for characteristics associated with WMP referral and included all covariates in one model.
RESULTS
Table 1 shows the clinician, clinical practice, and patient characteristics of the 1,023 clinicians. The majority of respondents were non-Hispanic white (73.1%) and worked in a group outpatient setting (73.3%). Clinician-reported patient characteristics included a relatively even distribution of patient income class (low-, middle-, and high-income patient panels were 34.0%, 35.5%, and 30.7%, respectively). Regarding clinician awareness of WMPs within the context of the USPSTF recommendation, 24.6% of clinicians reported being aware of WMPs in their communities that met USPSTF criteria, 58.4% were not aware of such WMPs in their communities, and 17.0% did not know (Table 1).
Table 1.
Characteristics of Clinicians Who See Children, Clinical Practice, and Patients, DocStyles Survey 2017 (n=1,023)
| Characteristics | All respondents, n (%) |
|---|---|
| Clinicians | |
| Total | 1,023 (100) |
| Age | |
| <45 years | 419 (41.0) |
| ≥45 years | 604 (59.0) |
| Gender | |
| Male | 567 (55.4) |
| Female | 456 (44.6) |
| Race/ethnicity | |
| White, non-Hispanic | 748 (73.1) |
| Black, non-Hispanic | 29 (2.8) |
| Hispanic | 42 (4.1) |
| Asian, non-Hispanic | 152 (14.9) |
| Other/multiracial, non-Hispanic | 52 (5.1) |
| Clinical practice | |
| Census region | |
| Northeast | 222 (21.7) |
| South | 368 (36.0) |
| Midwest | 213 (20.8) |
| West | 220 (21.5) |
| Specialty | |
| Family practitioner | 459 (44.9) |
| Internist | 148 (14.5) |
| Pediatrician | 250 (24.4) |
| Nurse practitioner | 166 (16.2) |
| Work setting | |
| Individual outpatient | 194 (19.0) |
| Group outpatient | 750 (73.3) |
| Inpatient | 79 (7.7) |
| Teaching hospital privileges | |
| Yes | 457 (45.7) |
| No | 566 (55.3) |
| Number of well-child visits per week | |
| <5 | 308 (30.1) |
| 5 to 14 | 335 (32.8) |
| ≥15 | 380 (37.2) |
| Clinician reported patient characteristics | |
| Patient income | |
| Low (<$50,000) | 348 (34.0) |
| Middle ($50,000 to <$100,000) | 361 (35.5) |
| High (≥$100,000) | 314 (30.7) |
| Pediatric patients with obesity among those who screen their patients (n=899) | |
| <10% | 173 (19.2) |
| 10% to <20% | 260 (28.9) |
| 20% to <40% | 333 (37.0) |
| ≥40% | 133 (14.8) |
| Clinicians aware of WMP within community meeting USPSTF recommendation | |
| Yes | 252 (24.6) |
| No | 597 (58.4) |
| Don’t know | 174 (17.0) |
Note: Due to rounding, the sum of percentages in each category may not exactly equal 100.0.
WMP, weight management program; USPSTF, U.S. Preventive Services Task Force.
Figure 2 shows the prevalence of adherence to the USPSTF recommendation for pediatric obesity screening. Of the 918 question respondents, 6.5% of clinicians reported screening children for obesity <25% of the time, 3.5% of clinicians screened for obesity 25%−50% of the time, 6.4% of clinicians screened for obesity 50% to <75% of the time, and 83.6% of clinicians screened for obesity ≥75% of the time (Figure 2). Furthermore, 19 (2.1%) clinicians reported not screening for obesity, whereas 715 (77.9%) screened ≥90% of the time, and 632 (69.0%) clinicians reported screening 100% of the time (data not shown).
Figure 2.
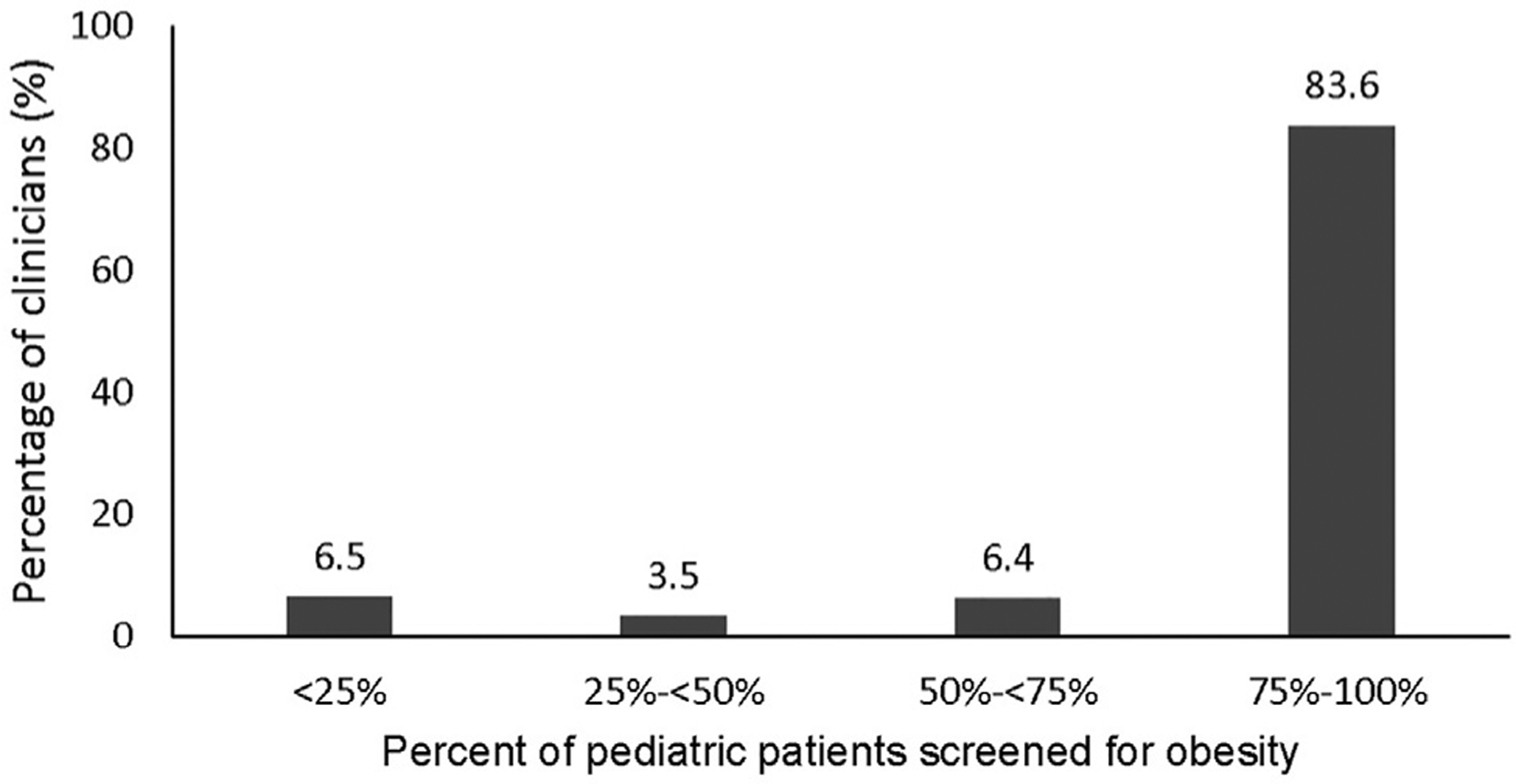
Prevalence of pediatric obesity screening among clinicians who see children, DocStyles survey 2017 (n=918).
USPSTF recommends children found to have obesity after screening be offered or referred to comprehensive behavioral interventions. Among 891 clinicians who responded to questions about referral practices, about half of clinicians (n=477, 53.5%) reported referring children with obesity to a WMP (Table 2). However, among providers aware of WMPs meeting the USPSTF recommendation in their community (n=252), the vast majority (n=224, 88.9%) referred their patients there (data not shown).
Table 2.
AORs for Clinicians Characteristics and Pediatric WMP Referrals, DocStyles 2017 (n=891)
| Provided community- or clinical-based WMP referral | |||
|---|---|---|---|
| Characteristics | All respondents, n (%) | Bivariate analysis, n (%) | Multivariate analysis,a AOR (95% CI) |
| Clinicians | |||
| Total | 891 (100) | 477 (53.5) | — |
| Age | |||
| <45 years | 357 (40.1) | 206 (57.7) | ref |
| ≥45 years | 534 (59.9) | 271 (50.8) | 0.83 (0.62, 1.11) |
| Gender | |||
| Male | 499 (56.0) | 243 (48.7) | ref |
| Female | 392 (44.0) | 234 (59.7) | 1.63 (1.20, 2.21) |
| Race/ethnicity | |||
| White, non-Hispanic | 652 (73.2) | 342 (52.5) | ref |
| Black, non-Hispanic | 21 (2.4) | 10 (47.6) | 0.79 (0.32, 1.97) |
| Hispanic | 37 (4.2) | 23 (62.2) | 1.24 (0.60, 2.55) |
| Asian, non-Hispanic | 135 (15.2) | 74 (54.8) | 1.00 (0.67, 1.49) |
| Asian, non-Hispanic | 135 (15.2) | 74 (54.8) | 1.00 (0.67, 1.49) |
| Other/multiracial, non-Hispanic | 46 (5.2) | 28 (60.9) | 1.25 (0.66, 2.39) |
| Clinical practice | |||
| Census region | |||
| Northeast | 196 (22.0) | 109 (55.6) | 1.10 (0.75, 1.60) |
| South | 319 (35.8) | 159 (49.8) | ref |
| Midwest | 188 (21.1) | 108 (57.5) | 1.39 (0.95, 2.03) |
| West | 188 (21.1) | 101 (53.7) | 1.20 (0.82, 1.75) |
| Specialty | |||
| Family practitioner | 420 (47.1) | 193 (46.0) | 0.70 (0.47, 1.04) |
| Internist | 113 (12.7) | 70 (62.0) | 1.21 (0.70, 2.09) |
| Pediatrician | 228 (25.6) | 139 (61.0) | ref |
| Nurse practitioner | 130 (14.6) | 75 (57.7) | 0.95 (0.56, 1.61) |
| Work setting | |||
| Individual outpatient | 170 (19.1) | 86 (50.6) | 1.00 (0.70, 1.44) |
| Group outpatient | 673 (75.5) | 361 (53.6) | ref |
| Inpatient | 48 (5.4) | 30 (62.5) | 1.06 (0.55, 2.01) |
| Teaching hospital privileges | |||
| Yes | 401 (45.0) | 253 (63.1) | ref |
| No | 490 (55.0) | 224 (45.7) | 0.51 (0.38, 0.68) |
| Number of well-child visits per week | |||
| <5 | 190 (21.3) | 92 (48.4) | ref |
| 5 to 14 | 324 (36.4) | 162 (50.0) | 0.97 (0.67, 1.43) |
| ≥15 | 377 (42.3) | 223 (59.2) | 1.23 (0.81, 1.88) |
| Clinician reported patient characteristics | |||
| Patient income | |||
| Low (<$50,000) | 302 (33.9) | 159 (52.7) | 1.24 (0.88, 1.75) |
| Middle ($50,000 to <$100,000) | 314 (35.2) | 183 (58.3) | 1.63 (1.16, 2.29) |
| High (≥$100,000) | 275 (30.9) | 135 (49.1) | ref |
| Pediatric patients with obesity | |||
| <10% | 165 (18.5) | 89 (53.9) | ref |
| 10% to <20% | 260 (29.2) | 132 (50.8) | 0.80 (0.53, 1.22) |
| 20% to <40% | 333 (37.4) | 183 (55.0) | 0.92 (0.62, 1.37) |
| ≥40% | 133 (14.9) | 73 (54.9) | 0.84 (0.52, 1.37) |
Note: Boldface indicates statistical significance (p<0.05).
All provider medical practice and patient characteristics were included in one model. 95% CI does not include 1.00.
WMP, weight management program.
Based on unadjusted analyses, there were differences in referrals based on clinician age, gender, specialty, teaching hospital privileges, and number of well-child visits per week. Results from adjusted analysis indicated that female clinicians had higher odds of WMP referral than male clinicians (AOR=1.63, 95% CI=1.20, 2.21). Additionally, providers without teaching hospital privileges had lower odds of referral to WMP compared with clinicians with teaching hospital privileges (AOR=0.51, 95% CI=0.38, 0.68). Finally, clinicians serving middle-income patients had higher odds of WMP referral compared with providers with upper-income patients (AOR=1.63, 95% CI=1.16, 2.29; Table 2).
DISCUSSION
In this study, only 25% of clinicians were aware of WMPs in their communities that met USPSTF criteria, 58% were not aware of any in their communities, and 17% did not know of such programs. Although a large majority of clinicians screened pediatric patients for obesity, only half referred patients to a WMP. Higher odds of referral were associated with being female or serving middle-income patients, and lower odds of WMP referral were associated with not having teaching hospital privileges. Both awareness and access are necessary for a recommendation to become actionable. Lack of knowledge or awareness among clinicians about WMPs in their community meeting USPSTF criteria was suggested by the 17% of clinicians who responded they “don’t know” whether appropriate programs were available. Increasing awareness among clinicians could facilitate appropriate referrals when resources are available.
The first component of the USPSTF recommendation addresses obesity screening.8 The majority (84%) of clinicians who responded to questions about screening reported screening for obesity at least 75% of the time, and most reported screening for obesity at every single well-child visit. By comparison, data from the National Committee for Quality Assurance in 2016 indicated that BMI assessment for children ages 3−17 years ranged from 52% to 69%.21 This discrepancy could reflect differences in data collection; the National Committee for Quality Assurance uses administrative data and DocStyles uses clinician self-report. Although providers may screen for obesity more than is documented in health records, social desirability bias could also inflate screening estimates within DocStyles data. Overall, screening and diagnosis of children with obesity may have been facilitated in the past decade by the widespread implementation of electronic health records.22,23
In addition to those who did not know whether WMPs existed in their community, almost 60% of clinicians reported they were not aware of WMPs in their community meeting the USPSTF recommendation. Answering no regarding awareness could reflect that either a program truly does not exist (lack of access) or a program exists but the clinician was not aware of it (lack of awareness). The inability to distinguish between these two scenarios is a study limitation.
Despite high rates of obesity screening, this study suggests that the uptake of the second component of the USPSTF recommendation—referral to comprehensive and intensive behavioral interventions—is substantially lower. Only half of the clinicians referred children to a WMP; more research is needed to determine why. Formally assessing whether lack of WMP awareness versus lack of WMP access or services is a gap that should be addressed, as different approaches would address these issues.24 Interestingly, even though half of the providers referred children to WMPs, only one in four clinicians were aware of WMPs in their communities meeting the USPSTF recommendation. Therefore, providers may refer children to WMPs within their communities that do not meet USPSTF recommendations, or providers may refer children to WMPs that may meet criteria but exist outside of their communities. Clinicians may select other referral options for childhood obesity other than WMPs, however, this is not necessarily consistent with the USPSTF recommendation. Experts have noted WMPs are largely limited to tertiary care centers and lack significant presence within many communities.8,10,11,25−27 Encouragingly, when providers were aware of a WMP meeting USPSTF criteria, almost 90% referred patients to this program.
Referrals to WMPs were associated with clinician teaching hospital privileges, reported patient income, and provider gender. Clinicians without teaching hospital privileges were half as likely to refer pediatric patients with obesity to WMPs. Teaching hospitals are usually located in urban centers and often have more resources compared with non-teaching hospitals.28 Intensive pediatric WMPs are often located in pediatric medical centers or tertiary care centers.29 Clinicians without teaching hospital affiliations may be outside of a referral system or geographic range of a WMP. These providers could potentially practice in a more rural area, where many children and families do not have convenient access to adequate weight management resources.25,29,30 Although inpatient providers in this study had a higher percentage of WMP referrals than outpatient providers, there was no significant association, potentially due to small sample size.
Clinicians serving majority middle-income patients had higher rates of patient referral to WMPs compared with clinicians serving majority high-income patients. Because of limitations of the survey, authors were unable to determine the characteristics of patients being referred to WMPs. However, promoting the establishment of WMPs in communities that are geographically and socioeconomically diverse may benefit more children across the U.S.
Female clinicians had 63% higher odds of referral to WMP compared with males. In a prior study, female gender affected screening and counseling services, with women more likely to engage in preventive care.31 Another study showed that female physicians were more likely to refer adult patients with obesity to weight loss programs,32 but this is the first study that has revealed this pattern for referral to pediatric WMPs.
The health and well-being of children with obesity can be improved by appropriate weight management care.25 Improved access by increasing the number of WMPs could be potentially achieved in two ways. First, more comprehensive, intensive WMPs could be implemented in communities where they currently do not exist. Introducing a WMP that is publicly available for procurement and rapid implementation may be a strategy to achieve this.33 Second, WMPs that currently exist but do not meet the USPSTF recommendation, could alter their curricula in order to ensure adherence to best practices. Some USPSTF-consistent WMPs have been successful in the community setting.34,35
Limitations
This is the first study to report clinician adherence to the 2017 USPSTF childhood obesity recommendation regarding childhood obesity screening and referral to WMPs. Although a prior study has examined this at the state level,36 this study uses data from clinicians across the nation. However, this study is subject to limitations. The updated USPSTF recommendation regarding childhood obesity was published on June 20, 2017, during the DocStyles survey 2017 sampling period of June 8 to August 9, 2017; therefore, an element of recency may have affected awareness among surveyed clinicians. However, because the 2017 update upheld the prior USPSTF recommendation without any significant changes, the timing of publication release would not likely have had a large impact on survey response outcomes. DocStyles is a panel survey, and thus not necessarily representative of the population; therefore, these results may not be generalizable to clinicians throughout the country. Another potential limitation is the obesity screening question. Other professional groups and societies, including the American Academy of Pediatrics, have recommended that healthcare providers address weight management and lifestyle issues with all pediatric patients.37,38 However, the USPSTF recommendation only applies to children aged 6 years or older. The DocStyles survey screening question asked about children aged 17 years or younger. Therefore, the frequency of childhood obesity screening overall may not reflect screening in the older age group addressed by the USPSTF. It is possible that screening rates for older children would be higher than those for all children, as prior research showed that identification of obesity may be lower among preschool-aged children and highest among adolescents.39 This survey also specifically asked about pediatric well visits, however, these comprise only 29% of pediatric clinic visits.40 Therefore, responses do not necessarily encompass referrals made during sick visits, which could potentially reflect a different population. Finally, DocStyles survey data were based on clinician self-report about their practices and patients rather than definitive measurements, such as actual referrals and patient income and, thus, may be subject to bias. Bias could also exist if clinicians who engaged in WMP referrals were more likely to respond to questions regarding this practice.
CONCLUSIONS
This study found that among surveyed participants, the majority of clinicians screen children for obesity, as recommended by USPSTF. However, only half of healthcare providers refer children with obesity to WMPs. Fewer still, only one quarter of clinicians caring for pediatric patients are aware of WMPs meeting USPSTF criteria in their community. Therefore, only a fraction of children referred to WMPs may be receiving evidence-based services. Yet, the great majority of clinicians refer children to WMPs meeting the USPSTF recommendation when they are aware of such a resource in their community. Clinical recommendation adherence is an important component to curbing the problem of childhood obesity. Effective communication of recommendations, and accessible programs for provider referral, are crucial to their implementation into clinical practice. Improvement is needed in increasing the access and referral to comprehensive, intensive pediatric WMPs that meet the USPSTF recommendation in communities across the nation.
ACKNOWLEDGMENTS
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
No financial disclosures were reported by the authors of this paper.
REFERENCES
- 1.Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity among adults and youth: United States, 2015−2016. NCHS Data Brief. 2017(288):1–8. [PubMed] [Google Scholar]
- 2.Akinbami LJ, Rossen LM, Fakhouri THI, Fryar CD. Asthma prevalence trends by weight status among U.S. children aged 2−19 years, 1988−2014. Pediatr Obes. 2018;13(6):393–396. 10.1111/ijpo.12246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bocca G, Ongering EC, Stolk RP, Sauer PJ. Insulin resistance and cardiovascular risk factors in 3- to 5-year-old overweight or obese children. Horm Res Paediatr. 2013;80(3):201–206. 10.1159/000354662. [DOI] [PubMed] [Google Scholar]
- 4.Mazor-Aronovitch K, Lotan D, Modan-Moses D, Fradkin A, Pinhas-Hamiel O. Blood pressure in obese and overweight children and adolescents. Isr Med Assoc J. 2014;16(3):157–161. [PubMed] [Google Scholar]
- 5.Pont SJ, Puhl R, Cook SR, Slusser W. Stigma experienced by children and adolescents with obesity. Pediatrics. 2017;140(6):e20173034. 10.1542/peds.2017-3034. [DOI] [PubMed] [Google Scholar]
- 6.Sikorski C, Luppa M, Luck T, Riedel-Heller SG. Weight stigma “gets under the skin”-evidence for an adapted psychological mediation framework: a systematic review. Obesity (Silver Spring). 2015;23 (2):266–276. 10.1002/oby.20952. [DOI] [PubMed] [Google Scholar]
- 7.Skinner AC, Perrin EM, Moss LA, Skelton JA. Cardiometabolic risks and severity of obesity in children and young adults. N Engl J Med. 2015;373(14):1307–1317. 10.1056/NEJMoa1502821. [DOI] [PubMed] [Google Scholar]
- 8.Grossman DC, Bibbins-Domingo K, Curry SJ, et al. Screening for obesity in children and adolescents: U.S. Preventive Services Task Force recommendation statement. JAMA. 2017;317(23):2417–2426. 10.1001/jama.2017.6803. [DOI] [PubMed] [Google Scholar]
- 9.Barton M Screening for obesity in children and adolescents: U.S. Preventive Services Task Force recommendation statement. Pediatrics. 2010;125(2):361–367. 10.1542/peds.2009-2037. [DOI] [PubMed] [Google Scholar]
- 10.Block JP, Oken E. Practical considerations for the U.S. Preventive Services Task Force recommendations on obesity in children and adolescents. JAMA Intern Med. 2017;177(8):1077–1079. 10.1001/jamainternmed.2017.1978. [DOI] [PubMed] [Google Scholar]
- 11.Wilfley DE, Staiano AE, Altman M, et al. Improving access and systems of care for evidence-based childhood obesity treatment: conference key findings and next steps. Obesity (Silver Spring). 2017;25 (1):16–29. 10.1002/oby.21712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Whitlock EP, O’Connor EA, Williams SB, Beil TL, Lutz KW. Effectiveness of weight management interventions in children: a targeted systematic review for the USPSTF. Pediatrics. 2010;125(2):e396–e418. 10.1542/peds.2009-1955. [DOI] [PubMed] [Google Scholar]
- 13.Epstein LH, Paluch RA, Roemmich JN, Beecher MD. Family-based obesity treatment, then and now: twenty-five years of pediatric obesity treatment. Health Psychol. 2007;26(4):381–391. 10.1037/0278-6133.26.4.381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Savoye M, Nowicka P, Shaw M, et al. Long-term results of an obesity program in an ethnically diverse pediatric population. Pediatrics. 2011;127(3):402–410. 10.1542/peds.2010-0697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kirk S, Zeller M, Claytor R, Santangelo M, Khoury PR, Daniels SR. The relationship of health outcomes to improvement in BMI in children and adolescents. Obes Res. 2005;13(5):876–882. 10.1038/oby.2005.101. [DOI] [PubMed] [Google Scholar]
- 16.O’Connor EA, Evans CV, Burda BU, Walsh ES, Eder M, Lozano P. Screening for obesity and intervention for weight management in children and adolescents: evidence report and systematic review for the U.S. Preventive Services Task Force. JAMA. 2017;317(23):2427–2444. 10.1001/jama.2017.0332. [DOI] [PubMed] [Google Scholar]
- 17.Lloyd-Richardson EE, Jelalian E, Sato AF, Hart CN, Mehlenbeck R, Wing RR. Two-year follow-up of an adolescent behavioral weight control intervention. Pediatrics. 2012;130(2):e281–e288. 10.1542/peds.2011-3283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Woolford SJ, Clark SJ, Gebremariam A, Davis MM, Freed GL. Physicians’ perspectives on referring obese adolescents to pediatric multi-disciplinary weight management programs. Clin Pediatr (Phila). 2010;49(9):871–875. 10.1177/0009922810368287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.SERMO. Our Research Network. www.sermo.com/business-solutions/introduction#our-research. Published 2017. Accessed February 14, 2018.
- 20.Tan CH, Hungerford DW, Denny CH, McKnight-Eily LR. Screening for alcohol misuse: practices among U.S. primary care providers, DocStyles 2016. Am J Prev Med. 2018;54(2):173–180. 10.1016/j.amepre.2017.11.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.National Committee for Quality Assurance. HEDIS measures and technical resources. www.ncqa.org/report-cards/health-plans/state-of-health-care-quality/2017-table-of-contents/weight-assessment. Accessed February 1, 2017.
- 22.Coleman KJ, Hsii AC, Koebnick C, et al. Implementation of clinical practice guidelines for pediatric weight management. J Pediatr. 2012;160(6):918–922.e1. 10.1016/j.jpeds.2011.12.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Shaikh U, Berrong J, Nettiksimmons J, Byrd RS. Impact of electronic health record clinical decision support on the management of pediatric obesity. Am J Med Qual. 2015;30(1):72–80. 10.1177/1062860613517926. [DOI] [PubMed] [Google Scholar]
- 24.Brauer P, Royall D, Dwyer J, et al. Obesity services planning framework for interprofessional primary care organizations. Prim Health Care Res Dev. 2017;18(2):135–147. 10.1017/S1463423616000372. [DOI] [PubMed] [Google Scholar]
- 25.Ambler KA, Hagedorn DW, Ball GD. Referrals for pediatric weight management: the importance of proximity. BMC Health Serv Res. 2010;10:302. 10.1186/1472-6963-10-302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Jasik CB, King EC, Rhodes E, et al. Characteristics of youth presenting for weight management: retrospective national data from the POWER Study Group. Child Obes. 2015;11(5):630–637. 10.1089/chi.2015.0053. [DOI] [PubMed] [Google Scholar]
- 27.Kirk S, Armstrong S, King E, et al. Establishment of the Pediatric Obesity Weight Evaluation Registry: a national research collaborative for identifying the optimal assessment and treatment of pediatric obesity. Child Obes. 2017;13(1):9–17. 10.1089/chi.2016.0060. [DOI] [PubMed] [Google Scholar]
- 28.Shahian DM, Nordberg P, Meyer GS, et al. Contemporary performance of U.S. teaching and nonteaching hospitals. Acad Med. 2012; 87(6):701–708. 10.1097/ACM.0b013e318253676a. [DOI] [PubMed] [Google Scholar]
- 29.Cohen GM, Irby MB, Boles K, Jordan C, Skelton JA. Telemedicine and pediatric obesity treatment: review of the literature and lessons learned. Clin Obes. 2012;2(3−4):103–111. 10.1111/j.1758-8111.2012.00050.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Davis AM, James RL, Curtis MR, Felts SM, Daley CM. Pediatric obesity attitudes, services, and information among rural parents: a qualitative study. Obesity (Silver Spring). 2008;16(9):2133–2140. 10.1038/oby.2008.312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Henderson JT. Weisman CS. Physician gender effects on preventive screening and counseling: an analysis of male and female patients’ health care experiences. Med Care. 2001;39(12):1281–1292. 10.1097/00005650-200112000-00004. [DOI] [PubMed] [Google Scholar]
- 32.Dutton GR, Herman KG, Tan F, et al. Patient and physician characteristics associated with the provision of weight loss counseling in primary care. Obes Res Clin Pract. 2014;8(2):e123–e130. 10.1016/j.orcp.2012.12.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kolotourou M, Radley D, Gammon C, Smith L, Chadwick P, Sacher PM. Long-term outcomes following the MEND 7–13 child weight management program. Child Obes. 2015;11(3):325–330. 10.1089/chi.2014.0092. [DOI] [PubMed] [Google Scholar]
- 34.Sacher PM, Kolotourou M, Chadwick PM, et al. Randomized controlled trial of the MEND program: a family-based community intervention for childhood obesity. Obesity (Silver Spring). 2010;18(suppl 1):S62–S68. 10.1038/oby.2009.433. [DOI] [PubMed] [Google Scholar]
- 35.Davis AM, Daldalian MC, Mayfield CA, et al. Outcomes from an urban pediatric obesity program targeting minority youth: the Healthy Hawks program. Child Obes. 2013;9(6):492–500. 10.1089/chi.2013.0053. [DOI] [PubMed] [Google Scholar]
- 36.Staiano A, Marker A, Liu M, Hayden E, Hsia D, Broyles S. Childhood obesity screening and treatment practices of pediatric healthcare providers. J La State Med Soc. 2017;169(1):2–10. [PMC free article] [PubMed] [Google Scholar]
- 37.Barlow SE. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics. 2007;120(suppl 4):S164–S192. 10.1542/peds.2007-2329C. [DOI] [PubMed] [Google Scholar]
- 38.Daniels L, Heath ALM, Williams SM, et al. Baby-led introduction to SolidS (BLISS) study: a randomised controlled trial of a baby-led approach to complementary feeding. BMC Pediatr. 2015;15:179. 10.1186/s12887-015-0491-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.O’Brien SH, Holubkov R, Reis EC. Identification, evaluation, and management of obesity in an academic primary care center. Pediatrics. 2004;114(2):e154–e159. 10.1542/peds.114.2.e154. [DOI] [PubMed] [Google Scholar]
- 40.American Academy of Pediatrics. Profile of pediatric office visits. www.aap.org/en-us/professional-resources/practice-transformation/managing-practice/Pages/Profile-of-Pediatric-Office-Visits.aspx. Accessed July 30, 2018.