

Abstract
Objective:
Cancer, particularly during young adulthood, can evoke difficult emotions, interfere with normative developmental activities, and challenge coping responses. Emotion-regulating coping efforts aimed at active emotional processing (EP) and emotional expression (EE) can be beneficial to cancer adjustment and perceptions of positive growth. However, it may be that EP and EE work differently to influence well-being. This study examines relationships of EP and EE with psychological distress, posttraumatic growth (PTG), and resilience. We expect that EP will be positively associated with PTG and resilience, whereas EE will be negatively associated with psychological distress.
Methods:
Young adults with cancer (Mage=34.68, N=57) completed measures of emotional approach coping (EP and EE), psychological distress (depressive symptoms, fear of cancer recurrence; FCR) and indicators of positive adjustment and growth (resilience and PTG).
Results:
Greater use of EP was associated with higher resilience (β=0.48, p=.003) and PTG (β=0.27, p=.05), whereas greater use of EE was associated with lower resilience (β= −0.33, p=.04). The EE x EP interaction was significant for FCR (β=0.29, p=.04) such that low EE was associated with lower FCR in those with high EP. Interaction effects were not significant for depressive symptoms, resilience, or PTG.
Conclusions:
Findings highlight differing relationships between EP and EE among young adults with cancer. Interventions aimed at increasing emotion-regulating coping strategies may prove useful in facilitating positive adjustment and growth, strengthening young adults’ ability to cope with the diverse effects of disease, treatment, and survivorship.
Keywords: emotional processing, emotional expression, depressive symptoms, fear of cancer recurrence, posttraumatic growth, resilience, young adult cancer, oncology
Background
Young adults with cancer (aged 18–39) face many challenges resulting from cancer diagnosis and treatment. Disruptions to relational activities (e.g., marriage, family planning) and developmental milestones (e.g., educational/vocational attainment), alternations in social relationships, fear of cancer recurrence (FCR), and physical changes from cancer treatment contribute to the psychological burden of a cancer diagnosis during young adulthood and make this a distinct group requiring specialized care.1 Successful coping with the challenges and interruptions to daily life can foster positive changes and adjustment, including posttraumatic growth (PTG) and enhanced resilience.2,3 Coping efforts aimed at emotion regulation (e.g., processing and expressing emotions) have potential to impact indicators of both positive and negative adjustment to cancer. The aim of this study was to examine the relationship between specific emotional-regulating coping strategies of processing and expressing emotions and psychological distress (i.e., depressive symptoms and FCR), PTG, and resilience among young adults with cancer.
Emotional approach coping
Emotional approach coping (EAC), which involves processing and expressing one’s emotions in response to stressful experiences, has been proposed to play a critical role in adjustment to cancer.4 EAC calls upon functionalist theories of emotion5, which suggest that processing and expressing emotions (e.g., fear, happiness) facilitates adjustment and underlies successful self-regulation4,6,7. EAC further extends early emotion-focused coping research8 which was often confounded with negative emotions, distress, and avoidance.4
EAC involves two distinct yet related strategies: emotional processing (EP) and emotional expression (EE). EP involves an active attempt to acknowledge, explore, and understand one’s emotions whereas4 whereas EE involves active verbal and/or nonverbal efforts to communicate or symbolize one’s emotional experience. Commonly examined as a unitary construct averaging across EP and EE, these constructs are often only modestly, positively correlated. As such, research exists supporting differences in psychological distress and adjustment among chronic illness populations when EP and EE are examined separately4,6,9,10.
Emotional processing and expression: Adjustment to cancer
Emotional expression may influence adjustment by actively directing attention towards present concerns.4 Repeated EE may also serve to decrease attendance to negative emotions.4,11 Indeed, higher EE has been consistently associated with lower depressive symptoms and cancer-related intrusive thoughts among cancer survivors12,13 (e.g., fear of cancer recurrence). While, to our knowledge, there are no studies of relationships between EE and FCR, emotional expression in general is thought to influence adjustment by putting feelings to words (i.e., affect labeling) 14,15 Further, expressing emotions to supportive others may release feelings about the possibility of death.16 This is an important relationship to more deeply understand as 65–90% of young adult cancer survivors endorse FCR.15
Whereas the preponderance of research on emotional-regulatory coping predictors of cancer adjustment focuses on distress; investigations of emotional-regulatory coping predictors of positive adaptation and growth are needed to inform research targeted to helping young adults with cancer to thrive and bounce back (i.e., resilience) from cancer and gain increased appreciation for life (i.e., PTG). Emotional processing, which is often associated with items that pertain to a reflection on feelings15,18 may facilitate meaning making by directing one’s attention towards actively processing, acknowledging, and understanding emotions. This process may provide opportunities for young adults with cancer to return and exceed to prior levels of functioning, which is likely to elicit resilience and enhance PTG.17
The Current Study
While a sizeable body of literature characterizes coping strategies among young adults with cancer19,20, few have focused on emotion-regulating coping strategies aimed at actively processing and expressing emotions.4 The need to understand EAC in young adults is paramount as young adults with cancer report greater psychological distress as well as greater positive growth than older survivors.21 Younger age is also the most consistent predictor of increased FCR.22 Moreover, painful negative emotions among young adults tend to persist across the cancer continuum.21
Taken together, depressive symptoms, FCR, PTG, and resilience among young adults with cancer constitute the favorable and adverse psychological sequelae of a cancer diagnosis. Given that young adults with cancer often experience a long period of survivorship after diagnosis and treatment, EP and EE coping strategies that help foster positive psychological adjustment might be integral to facilitating long-term psychological well-being.
The purpose of this study was to examine the potential of coping through EP and EE on psychological distress (i.e., depressive symptoms and FCR) and positive aspects of well-being (i.e., PTG and resilience) among young adults with cancer. We hypothesized:
H1: EP will be positively associated with PTG and resilience
H2: EE will be negatively associated with depressive symptoms and FCR
Further, given differences in distress and adjustment across EP and EE in prior literature4,6,9,10, we examined the moderating role of EP and EE on psychological distress and positive aspects of well-being. The specific hypotheses are as follows:
H3: EP will moderate the relationship between EE and PTG and resilience, such that higher use of EP will be positively associated with PTG and resilience among those with relatively low EE.
H4: EE will moderate the relationship between EP and depressive symptoms and FCR, such that higher use of EE will be negatively associated with depressive symptoms and FCR among those with relatively low EP.
Method
Participants and procedures
Young adults with cancer who were diagnosed with cancer between the ages of 18–39 within the prior five years were recruited to take part in a broader study of cancer-related support communication.23 Participants were recruited through social media posts (Facebook/Twitter) via cancer-related social media organizations (Army of Women, GRYT Health, Lacuna Loft, and Young Survival Coalition) and directed to a link to complete the questionnaire. Participants were additionally recruited through the Pennsylvania State Cancer Registry where eligible participants were mailed a study information sheet and opted into receiving a survey link to the questionnaire. All participants completed the questionnaire online between December 2017 and March 2019, and were entered into a drawing to receive a gift card. Informed consent was obtained from all participants and procedures were approved by the appropriate Institutional Review Board (approval number: 2017–0807).
Demographic and medical characteristics are displayed in Table 1. Five participants were excluded from analyses due to incomplete data resulting in a final sample size of 57 young adults who ranged in age from 24–42 (Mage=34.68, SD=4.89), were predominantly female (94.7%), White (93.0%), and diagnosed with breast cancer (71.9%), with average time since diagnosis at 2.5 years (M=28.29 months, SD=31.44).
Table 1.
Study Sample (N=57)
| Variable | N (%) | Range |
|---|---|---|
|
| ||
| Age [M(SD)] | 34.68 (4.89) | 24–42 |
| Female | 54 (94.7%) | |
| Race/ethnicity | ||
| White | 53 (93.0%) | |
| Asian | 2 (3.5%) | |
| Black/African American | 1 (1.8%) | |
| Hispanic/Latino | 1 (1.8%) | |
| Education | ||
| High school degree | 2 (3.5%) | |
| Some college/Trade/Business school | 8 (14.0%) | |
| 4-year college degree | 23 (40.3%) | |
| Graduate degree | 24 (42.1%) | |
| Employment status | ||
| Employed | 39 (68.4%) | |
| Student | 3 (5.3%) | |
| Medical leave/disability/unemployed | 15 (25.5%) | |
| Relationship status | ||
| Single | 11 (19.3%) | |
| Married/Partnered | 42 (73.7%) | |
| Divorced/Widowed | 4 (7.0%) | |
| Cancer type | ||
| Breast | 41 (71.9%) | |
| Othera | 16 (28.1%) | |
| Cancer stage | ||
| Early Stage (0-III) | 49 (86.0%) | |
| Stage IV | 1 (1.8%) | |
| Not staged (e.g., brain cancer) | 7 (12.2%) | |
| Treatmentb | ||
| Surgery | 53 (93.0%) | |
| Chemotherapy | 41 (71.9%) | |
| Hormone | 37 (64.9%) | |
| Radiation | 25 (43.9%) | |
| Treatment status | ||
| Completed main treatmentc | 52 (91.2%) | |
| Months since diagnosis [M(SD)] | 28.29 (31.44) | |
Brain/Hodgkin’s/Cervical/Leukemia/Colon/Ovarian/Thyroid/Salivary gland/Testicular;
>1 treatment could be selected;
includes active hormonal therapy
Measures
Emotional Approach Coping.
EAC was measured using the Emotional Approach Coping scales4 which consist of the 4-item EP (“I realize that my feelings are valid and important”) and the 4-item EE (“I feel free to express my emotions”) scales. Participants rated their agreement on a 4-point scale ranging from, (1) I don’t do this at all to (4) I do this a lot. Cronbach’s alpha was 0.87 for EP and 0.94 for EE.
Depressive Symptoms.
Depressive symptoms during the past week were measured by the 10- item version of the Center for Epidemiological Studies Depression Scale (CESD-10).24 Participants rated their agreement with items on a 4-point scale, ranging from (0) rarely or none of the time to (3) all of the time. Sample items included, “I felt lonely” and “I felt happy”. A total score of 10 is typically used as a cut off for identifying individuals at risk for clinical depression.24 Scores were summed to a total score where higher scores reflected more depressive symptoms. Cronbach’s alpha was 0.80.
Fear of Recurrence.
FCR was measured using the 4-item adapted scale (for all cancer types) of the Concerns about Recurrence Scale.25 Participants rated their agreement with items on a 5-point scale, ranging from (0) not at all to (4) extremely. A sample item included, “How often does the possibility that your cancer could recur upset you”. A total score was calculated as the average of all items with higher scores indicating more resilience. Cronbach’s alpha was 0.96.
Resilience.
Resilience was measured using the Brief Resilience Scale.26 Participants rated their agreement with items on a 5-point scale, ranging from (1) strongly disagree to (5) strongly agree. A sample item included, “I tend to bounce back quickly after hard times”. A total score was calculated as the average of all items with higher scores indicating more resilience. Cronbach’s alpha was 0.85.
Posttraumatic Growth.
PTG was measured using the 10-item Posttraumatic Growth Inventory (PTGI-SF).27 Participants rated their agreement with items as a result of their cancer diagnosis on a 6-point scale ranging from, (0) I did not experience this change to (5) I experienced this change to a very great degree. A sample item included, “I changed my priorities about what is important in my life”. A total score was calculated as the sum of all items with higher scores indicating more perceived PTG. Cronbach’s alpha was 0.88.
Data Analytic Plan
Descriptive statistics and zero-order correlations were conducted for key study variables. Associations between demographic [age, education, income, employment status (employed vs. not employed), ethnicity], cancer-related variables [time since diagnosis, cancer type (breast vs. not), cancer stage, treatment status], and history of a depressive or anxiety disorder with dependent variables were examined as possible covariates. Significant associations were controlled for in relevant models.
Multiple linear regression was used to test study hypotheses. In each model, relevant covariates were entered in the first block, EP and EE were entered in the second block, and the interaction term (EP x EE/EE X EP) was included in the third block. To avoid multicollinearity, variables were centered around the mean, and interaction terms were analyzed in accordance with methods outlined by Aiken & West.28 To interpret significant interaction terms, simple slopes analyses were conducted with values at one standard deviation above and below the mean of EP/EE using the PROCESS macro29 in SPSS. Adjustments for multiple comparisons were not made.
Power Analysis.
Power analyses were conducted using G*Power 3.1. An a priori power analysis, with n=52 as the smallest possible sample size at 80% power to detect moderate to large effects given an alpha of 0.05, suggested that we were adequately powered given our sample size. Further, a post-hoc power analysis was conducted to determine whether the final sample size (N=57) obtained in this study was sufficient to detect an effect. With an effect size of 0.15, a sample size of 57 and a significance criterion of 0.5, the statistical power was adequate (>80%).
Results
Descriptive statistics and identification of covariates
Descriptive statistics and correlations are presented in Table 2. On average young adults reported moderately engaging in EP (M=2.70, SD=0.75) and EE (M=2.47, SD=0.87). They reported thinking about FCR a moderate amount (M=3.73, SD=1.53), and experienced high levels of PTG (M=27.51, SD=10.18) and resilience (M=3.43, SD=0.71). Over half of the sample (n=32; 56.3%) met the CESD-10 cutoff of ≥ 10 (M=11.16, SD=5.44) indicative of clinical depression.
Table 2.
Descriptive statistics and correlations
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| 1. EP | 2.70 | 0.75 | - | .56*** | −.13 | −.13 | .29* | .42** |
| 2. EE | 2.47 | 0.87 | - | −.21 | .05 | −.02 | .38** | |
| 3. Depressive sx | 11.16 | 5.44 | - | .26 | −.44** | .04 | ||
| 4. FCR | 3.73 | 1.53 | - | −.34* | .02 | |||
| 5. Resilience | 3.43 | 0.71 | - | .06 | ||||
| 6. PTG | 27.51 | 10.18 | - | |||||
p<.05,
p<.01,
p<.001
Hypothesis testing
H1: Emotional Processing.
Supporting the study hypothesis, greater levels of EP were significantly associated with higher levels of resilience (β=0.48, p=.003) and PTG (β=0.27, p=.05). See Table 3.
Table 3.
EP/EE and psychological distress and adjustment
| Variable | ΔR2 | B | SE | β |
|---|---|---|---|---|
|
| ||||
| Depressive symptoms | ||||
| Block 1 | 0.18 | |||
| Income | −3.90 | 1.60 | −0.30* | |
| Hx depression | −0.55 | 1.34 | −0.33* | |
| Block 2 | 0.05 | |||
| EP | −0.31 | 1.12 | −0.04 | |
| EE | −1.19 | 0.97 | −0.19 | |
| Block 3 | 0.00 | |||
| EE X EP | 0.37 | 1.11 | 0.04 | |
| F(5,56)=3.10*, Adjusted R2=0.16 | ||||
| Fear of cancer recurrence | ||||
| Block 1 | 0.04 | |||
| Time since diagnosis | −0.01 | 0.01 | 0.25† | |
| Block 2 | 0.04 | |||
| EP | −0.63 | 0.32 | −0.31† | |
| EE | 0.54 | 0.28 | 0.31† | |
| Block 3 | 0.08 | |||
| EE X EP | 0.70 | 0.32 | 0.29* | |
| F(4,56)=2.46*, Adjusted R2=0.16 | ||||
| Resilience | ||||
| Block 1 | 0.13 | |||
| Employment | −0.37 | 0.20 | −0.25 | |
| Hx depression | 0.29 | 0.18 | 0.21† | |
| Block 2 | 0.13 | |||
| EP | 0.45 | 0.14 | 0.48* | |
| EE | −0.27 | 0.13 | −0.33* | |
| Block 3 | 0.01 | |||
| EP X EE | −0.10 | 0.14 | −0.09 | |
| F(5,56)=3.74**, Adjusted R2=0.20 | ||||
| Posttraumatic growth | ||||
| Block 1 | 0.30 | |||
| Time since diagnosis | 0.06 | 0.04 | 0.20† | |
| Age | −0.38 | 0.24 | −0.18 | |
| Ethnicity | −5.27 | 3.03 | −0.20† | |
| Hx anxiety | −5.50 | 2.32 | −0.27* | |
| Block 2 | 0.13 | |||
| EP | 3.69 | 1.82 | 0.27* | |
| EE | 1.77 | 1.67 | 0.15 | |
| Block 3 | 0.01 | |||
| EP X EE | 1.47 | 1.86 | 0.09 | |
| F(7,56)=5.35***, Adjusted R2=0.35 | ||||
p<.05,
p<.01,
p<.001,
p<0.10
H2: Emotional Expression.
Contrary to what was hypothesized, greater levels of EE were only marginally associated with higher levels of FCR (β= 0.31, p=.06) and were not significantly associated with depressive symptoms. See Table 3.
H3: Emotional Processing Moderation.
Contrary to hypotheses, there were no significant EP x EE interactions for PTG and resilience.
H4: Emotional Expression Moderation.
There was a significant EE x EP interaction for FCR (β= 0.29, p=.04), which explained an additional 8% of the variance beyond the main effects (see Figure 1), however, in the opposite direction than hypothesized. Simple slope analyses revealed lower, and not higher, use of EE was associated with lower FCR among those engaging in high, and not low, EP (β= −1.24, p<.05). The slope was marginally significant for average levels (β= −0.63, p=.06) of EP and not significant at low levels of EP. There was no significant EE x EP interaction for depressive symptoms. See Table 3.
Fig 1.
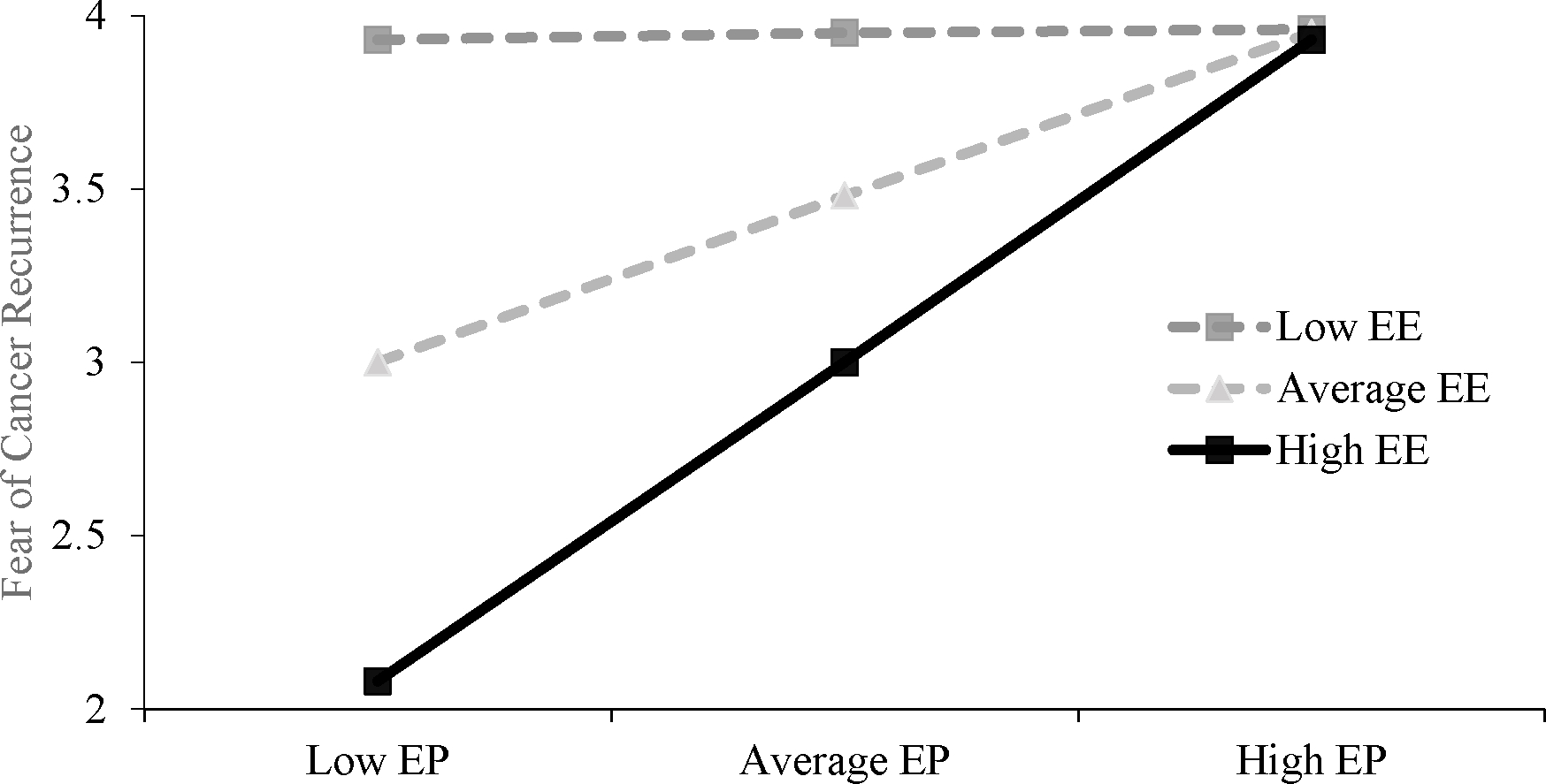
Interaction of EE and EP. Figure displays the interaction effect for fear of cancer recurrence. Analyses controlled for time since diagnosis. Dashed lines denote non-significant simple slopes.
Discussion
This study examined the relationship of EP and EE on psychological adjustment and positive outcomes among young adults with cancer. Coping through emotional-regulatory efforts may be an important tool for young adults with cancer; however, study findings suggest that EP and EE exert differential effects on psychological adjustment.
Contrary to hypotheses, EE was not associated with lower depressive symptoms and was marginally associated with higher, and not lower, FCR, potentially suggesting that the ability to express one’s emotions might not uniformly aid in buffering negative emotions in the cancer context. Further, use of EE was significantly associated with lower resilience. Given these patterns of findings, it is important to consider that the benefits of EE often do not occur in a vacuum and the social context surrounding EE plays an important role in facilitating adjustment.
Young adults with cancer often experience altered social relationships, feeling like their social networks lack understanding towards their cancer experience and find dealing with their cancer experience to be too difficult to handle.30,31 Further, young adults with cancer report receiving insufficient or constrained social support (e.g., pity, changing the subject).30,31 It may be that a socially constraining environment is preventing young adults from successfully disclosing thoughts and feelings related to cancer. Future studies would benefit from extending current findings to examine the influence of relevant social factors in the context of emotional expression.
Consistent with hypotheses, coping through EP was positively associated with resilience. This finding aligns with emotion regulation research suggesting that individuals faced with stressors can benefit from utilizing emotion regulation strategies aimed at processing and understanding one’s emotions to maintain positive well-being and foster resilience.32 Given our finding of coping through EE being associated with lower resilience it may be that fostering resilience involves understanding emotions more deeply, rather than explicitly expressing emotions.
EP was also significantly positively associated with PTG, consistent with hypotheses. Indeed, PTG often involves a series of cognitive and emotional engagement.14 EP that involves deliberate emotional processing (e.g., reflection) is essential in the development of PTG14, especially when individuals try to make sense of a stressful event. Therefore, coping through EP may foster a deliberate focus on the meaning making after cancer33 translating to increased feelings of PTG.
Our findings for EP being positively associated with resilience and PTG might also reflect a focus on the cancer experience as a transformative experience, a tangible change in relation to some sort of catalyst (e.g., changes experienced in post-illness life)34, that is fostered by an active attempt to acknowledge, explore, and understand one’s emotions. Previous research among young adults with cancer has suggested that some young adults experience cancer as a positive transformative experience while others do not, often taking a fatalistic view of their cancer experience.35 Drawing on current study findings fostering and encouraging EP may be one avenue to further understand how young adults restructure their cancer experience and themselves in positive ways.
The EE x EP interaction was only significant for FCR. We had hypothesized that greater use of EE, in the context of low EP, would be associated with lower FCR; however, it was greater use of EP, in the context of low EE, that was associated with lower FCR. Several theorists36,37 have suggested that FCR comprises cognitions, beliefs, and emotions. It is plausible that young adults are more likely to actively process and try to understand thoughts related to FCR rather than communicate one’s emotional experience surrounding FCR. This line of thinking aligns with previous research38, which suggests that young adults do not want to burden their social networks with their cancer experience. Future studies would benefit from considering the role that the social environment has in facilitating or hindering emotional expression in the context of FCR.
It is also important to consider that young adults living increasingly in the digital age and future research would benefit from examining the role that online cancer support groups, cancer-related posts on social media, and blogging about one’s cancer experience might play in facilitating emotional expression and processing. Indeed, previous research has suggested that young adults frequently exchange support (i.e., emotional, informational), utilize coping strategies (i.e., humor, emotional expression/venting), and often use metaphoric and euphemistic (i.e., lump, growth) language to describe their cancer and cancer experiences.39,40 These types of online talk, sharing personal feelings and experiences as well as journaling/blogging, can help shape emotional expression and deepen emotional processing which, given current study findings, may have implications for psychological distress and well-being.
Study Limitations
The present study is not without limitations. First, the data were cross-sectional in nature. Future studies should explore the potential for a dynamic relationship of coping through EP and EE on psychological adjustment, adaptation, and growth as it unfolds over time. All demographic and clinical data (including diagnosis) were self-reported. Moreover, the majority of participants were White, female and breast cancer sample, thus limiting generalizability. However, breast cancer is the leading site of new cancers diagnosed in older young adults (aged 30–39), which represents our sample mean, thus accurately capturing this cohort. Further, emotional regulation in the form of emotional processing and emotional expression are understudied in young adults with cancer, compared to the adult literature, which shows the benefit of emotional approach coping for psychological well-being, therefore laying the groundwork for future research to replicate these findings across a more heterogeneous young adult cancer population.
It should be noted that EP and EE were measured in regard to how young adults with cancer generally respond to emotions when experiencing a stressful situation. Future studies should explore the relationships of EP and EE when assessed using situational, cancer-specific stressors. It also may be true that some of our study findings may be explained by characteristics often generally present in young adulthood: optimism and a tendency to perceive that negative effects are rare. Last, majority of young adults were recruited through social media outlets which requires one to “like” or “follow” that specific cancer-related organization. It may be that those who are more inclined to follow these cancer-related organizations and access their supports experience benefits from emotional processing and expression that may impact psychological distress and well-being. More work is needed to disentangle the role that social media might play in facilitating or impeding adjustment to disease among young adults with cancer.
Clinical Implications
Reinforcing the benefit of actively expressing and processing emotion by disclosing thoughts and feelings and dedicating time to understand what one is feeling is vital to positive adjustment to cancer. Providing psychoeducation to young adults with cancer about the benefit of expressing and processing emotions as well as education surrounding which coping strategy may be responsive to situational demands may promote greater psychological adjustment, positive adaptation, and growth after being diagnosed with cancer and throughout the cancer continuum.
An important implication of these findings for clinicians working with young adults with cancer is that EP and EE work differently to affect adjustment to disease in ways that imply that different emotional coping strategies may be differentially helpful and should be considered when evaluating and intervening on young adults coping. Specifically, tailoring coping interventions should capitalize on both EP and EE coping strategies to positively impact adjustment to disease. This might include a focus on expressing emotions, by putting feeling to words, and engaging in emotional processing through affect labeling and cognitive reappraisal which serves to better acknowledge, explore and understand one’s emotions.
Conclusions
Actively processing and/or expressing one’s emotional experiences can be considered a form of adaptive emotional regulation. Indeed, seminal conceptualizations of emotion regulation define this process as “the processes by which individuals influence which emotions they have, when they have them, and how they experience and express these emotions”.32 In the context of coping, emotion regulation may serve a protective function in reducing psychological distress and facilitating positive adaptation and growth. However, emotion regulation strategies that promote active engagement with emotional processing and expression may be underutilized among young adult cancer patients. Fostering EP and EE throughout the cancer trajectory has the potential to reduce stress and other negative psychological outcomes to promote adaptation and growth, subsequently improving the quality of life and well-being of young adults with cancer.
Acknowledgements:
Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Number F99CA222727 (PI: Darabos; Hunter College, City University of New York). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This research was additionally supported by funds from the American Psychological Foundation (PI: Darabos) and the Graduate Center Doctoral Student Research Grant (PI: Darabos). KD is supported by a NCI Training Grant (K00CA222727; PI: Darabos); MR is supported by a NRSA Training Grant (T32CA229114–01; PI: Shields). Part of these data were supplied by the Bureau of Health Statistics & Registries, Pennsylvania Department of Health, Harrisburg, Pennsylvania. The Pennsylvania Department of Health specifically disclaims responsibility for any analyses, interpretations or conclusions. The authors would like to thank the Army of Women, GRYT Health, Lacuna Loft, and the Young Survival Coalition for their assistance in recruitment.
Footnotes
Conflict of Interest: The authors declare that they have no conflicts of interest.
Data Availability Statement:
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- 1.Zebrack B (2011) Psychological, social, and behavioral issues for young adults with cancer. Cancer 117 (S10):2289–2294. doi: 10.1002/cncr.26056 [DOI] [PubMed] [Google Scholar]
- 2.Wang AW-T, Hoyt MA (2020) Cancer-related masculinity threat in young adults with testicular cancer: the moderating role of benefit finding. Anxiety, Stress, & Coping:1–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Greup SR, Kaal SE, Jansen R, Manten-Horst E, Thong MS, van der Graaf WT, Prins JB, Husson O (2018) Post-traumatic growth and resilience in adolescent and young adult cancer patients: an overview. Journal of adolescent and young adult oncology 7 (1):1–14 [DOI] [PubMed] [Google Scholar]
- 4.Stanton AL, Danoff-Burg S, Cameron CL, Bishop M, Collins CA, Kirk SB, Sworowski LA, Twillman R (2000) Emotionally expressive coping predicts psychological and physical adjustment to breast cancer. Journal of consulting and clinical psychology 68 (5):875. [PubMed] [Google Scholar]
- 5.Campos JJ, Mumme D, Kermoian R, Campos RG (1994) A functionalist perspective on the nature of emotion. Japanese Journal of Research on Emotions 2 (1):1–20 [PubMed] [Google Scholar]
- 6.Jasinski MJ, Lumley MA, Latsch DV, Schuster E, Kinner E, Burns JW (2016) Assessing anger expression: construct validity of three emotion expression-related measures. Journal of personality assessment 98 (6):640–648 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ekman P (1992) Are there basic emotions? [DOI] [PubMed] [Google Scholar]
- 8.Lazarus RS, Folkman S (1984) Stress, appraisal, and coping. Springer publishing company, [Google Scholar]
- 9.Hoyt MA, Wang AW-T, Boggero IA, Eisenlohr-Moul TA, Stanton AL, Segerstrom SC (2020) Emotional approach coping in older adults as predictor of physical and mental health. Psychology and Aging 35 (4):591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hoyt MA, Stanton AL, Irwin MR, Thomas KS (2013) Cancer-related masculine threat, emotional approach coping, and physical functioning following treatment for prostate cancer. Health Psychology 32 (1):66. [DOI] [PubMed] [Google Scholar]
- 11.Foa EB, Kozak MJ (1986) Emotional processing of fear: exposure to corrective information. Psychological bulletin 99 (1):20. [PubMed] [Google Scholar]
- 12.Austenfeld JL, Stanton AL (2004) Coping through emotional approach: a new look at emotion, coping, and health-related outcomes. Journal of personality 72 (6):1335–1364 [DOI] [PubMed] [Google Scholar]
- 13.Cho D, Park CL, Blank TO (2013) Emotional approach coping: Gender differences on psychological adjustment in young to middle-aged cancer survivors. Psychology & Health 28 (8):874–894. doi: 10.1080/08870446.2012.762979 [DOI] [PubMed] [Google Scholar]
- 14.Tedeschi RG, Calhoun LG (2004) Posttraumatic growth: Conceptual foundations and empirical evidence. Psychological Inquiry 15 (1):1–18. doi: 10.1207/s15327965pli1501_01 [DOI] [Google Scholar]
- 15.Rude SS, Little Maestas K, Neff K (2007) Paying attention to distress: What’s wrong with rumination? Cognition and Emotion 21 (4):843–864 [Google Scholar]
- 16.Hoyt MA (2009) Gender role conflict and emotional approach coping in men with cancer. Psychology and Health 24 (8):981–996 [DOI] [PubMed] [Google Scholar]
- 17.Yeung NCY, Lu Q, Wong CCY, Huynh HC (2016) The roles of needs satisfaction, cognitive appraisals, and coping strategies in promoting posttraumatic growth: A stress and coping perspective. Psychological Trauma: Theory, Research, Practice, and Policy 8 (3):284–292. doi: 10.1037/tra0000091 [DOI] [PubMed] [Google Scholar]
- 18.Stanton AL (2011) Regulating emotions during stressful experiences: The adaptive utility of coping through emotional approach. [Google Scholar]
- 19.Kyngäs H, Mikkonen R, Nousiainen EM, Rytilahti M, Seppänen P, Vaattovaara R, Jämsä T (2001) Coping with the onset of cancer: coping strategies and resources of young people with cancer. European journal of cancer care 10 (1):6–11 [DOI] [PubMed] [Google Scholar]
- 20.Miedema B, Hamilton R, Easley J (2007) From “invincibility” to “normalcy”: Coping strategies of young adults during the cancer journey. Palliative & Supportive Care 5 (1):41–49 [DOI] [PubMed] [Google Scholar]
- 21.Lang MJ, Giese-Davis J, Patton SB, Campbell DJ (2018) Does age matter? Comparing post-treatment psychosocial outcomes in young adult and older adult cancer survivors with their cancer-free peers. Psycho-oncology 27 (5):1404–1411 [DOI] [PubMed] [Google Scholar]
- 22.Shay LA, Carpentier MY, Vernon SW (2016) Prevalence and correlates of fear of recurrence among adolescent and young adult versus older adult post-treatment cancer survivors. Supportive Care in Cancer 24 (11):4689–4696 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Darabos K, Hoyt MA, Ford JS (2019) Relational processes and psychological adjustment among young adults with cancer: The role of technology-related communication. Psycho-Oncology 28 (12):2406–2414 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Andresen EM, Malmgren JA, Carter WB, Patrick DL (1994) Screening for depression in well older adults: Evaluation of a short form of the CES-D. American journal of preventive medicine 10 (2):77–84 [PubMed] [Google Scholar]
- 25.Vickberg SMJ (2003) The Concerns About Recurrence Scale (CARS): a systematic measure of women’s fears about the possibility of breast cancer recurrence. Annals of Behavioral Medicine 25 (1):16–24 [DOI] [PubMed] [Google Scholar]
- 26.Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J (2008) The brief resilience scale: assessing the ability to bounce back. International journal of behavioral medicine 15 (3):194–200 [DOI] [PubMed] [Google Scholar]
- 27.Cann A, Calhoun LG, Tedeschi RG, Taku K, Vishnevsky T, Triplett KN, Danhauer SC (2010) A short form of the Posttraumatic Growth Inventory. Anxiety, Stress, & Coping 23 (2):127–137 [DOI] [PubMed] [Google Scholar]
- 28.Aiken LS, West SG (1991) Multiple regression: Testing and interpreting interactions. Multiple regression: Testing and interpreting interactions. Sage Publications, Inc, Thousand Oaks, CA, US [Google Scholar]
- 29.Hayes AF (2017) Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Guilford publications, [Google Scholar]
- 30.Iannarino NT, Scott AM, Shaunfield SL (2017) Normative Social Support in Young Adult Cancer Survivors. Qual Health Res 27 (2):271–284. doi: 10.1177/1049732315627645 [DOI] [PubMed] [Google Scholar]
- 31.Breuer N, Sender A, Daneck L, Mentschke L, Leuteritz K, Friedrich M, Nowe E, Stöbel-Richter Y, Geue K (2017) How do young adults with cancer perceive social support? A qualitative study. Journal of psychosocial oncology 35 (3):292–308 [DOI] [PubMed] [Google Scholar]
- 32.Gross JJ (1998) The emerging field of emotion regulation: An integrative review. Review of general psychology 2 (3):271–299 [Google Scholar]
- 33.Taku K, Tedeschi RG, Cann A, Calhoun LG (2009) The culture of disclosure: Effects of perceived reactions to disclosure on posttraumatic growth and distress in Japan. Journal of Social and Clinical Psychology 28 (10):1226–1243 [Google Scholar]
- 34.Paterson B, Thorne S, Crawford J, Tarko M (1999) Living with Diabetes as a Transformational Experience. Qualitative Health Research 9 (6):786–802. doi: 10.1177/104973299129122289 [DOI] [PubMed] [Google Scholar]
- 35.Head KJ, Iannarino NT (2019) “It Changed Our Outlook on How We Want to Live”: Cancer as a Transformative Health Experience for Young Adult Survivors and Their Family Members. Qual Health Res 29 (3):404–417. doi: 10.1177/1049732318800674 [DOI] [PubMed] [Google Scholar]
- 36.Lee-Jones C, Humphris G, Dixon R, Bebbington Hatcher M (1997) Fear of cancer recurrence—a literature review and proposed cognitive formulation to explain exacerbation of recurrence fears. Psycho-Oncology: Journal of the Psychological, Social and Behavioral Dimensions of Cancer 6 (2):95–105 [DOI] [PubMed] [Google Scholar]
- 37.Leventhal H, Diefenbach M, Leventhal EA (1992) Illness cognition: using common sense to understand treatment adherence and affect cognition interactions. Cognitive therapy and research 16 (2):143–163 [Google Scholar]
- 38.Barnett ME, Shuk EM, Conway FP, Ford JS (2014) Cancer-related disclosure among adolescent and young adult cancer survivors: a qualitative study. Journal of adolescent and young adult oncology 3 (3):123–129 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Myrick JG, Holton AE, Himelboim I, Love B (2016) #Stupidcancer: Exploring a Typology of Social Support and the Role of Emotional Expression in a Social Media Community. Health Communication 31 (5):596–605. doi: 10.1080/10410236.2014.981664 [DOI] [PubMed] [Google Scholar]
- 40.Love B, Crook B, Thompson CM, Zaitchik S, Knapp J, LeFebvre L, Jones B, Donovan-Kicken E, Eargle E, Rechis R (2012) Exploring Psychosocial Support Online: A Content Analysis of Messages in an Adolescent and Young Adult Cancer Community. Cyberpsychology, Behavior, and Social Networking 15 (10):555–559. doi: 10.1089/cyber.2012.0138 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.