

Introduction
Subcorneal pustular dermatosis (SPD), also referred to as Sneddon-Wilkinson disease, is a chronic, rare condition of unknown origin characterized by the recurrent formation of sterile pustules in the superficial layers of the skin. These pustules typically appear in annular or serpiginous patterns and are commonly found on flexural surfaces and intertriginous areas. In this case report, we present a patient with SPD successfully treated with apremilast.
Case Presentation
A 61-year-old man with a medical history of prostatic adenocarcinoma underwent radical prostatectomy two years prior, presented an 11-year history of SPD. During the physical examination, the patient exhibited the presence of vesicles, pustules, as well as superficial erosion, which resulted in the formation of fine scale and crusted lesions in the axillary regions (Figure 1A). The histopathological examination revealed the presence of subcorneal vesicles or pustules primarily composed of neutrophils, occasionally accompanied by eosinophils. Additionally, focal acantholysis was evident, along with vascular ectasia and congestion in the papillary dermis (Figure 2, A–C). Direct immunofluorescence and fungal stain were negative. No psoriasiform pattern of hyperplasia were observed as well. He had undergone several treatments, including dapsone 100 mg/daily, acitretin 25 mg/daily and colchicine 1 mg/daily with mild and transient improvement.
Figure 1.
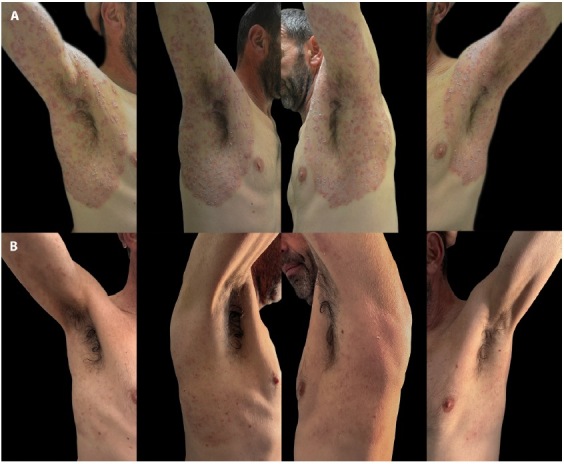
Sneddon-Wilkinson disease. (A) Vesicles, pustules, fine scale and crusted lesions in the axillary regions. (B) Resolution of the lesions after 8 weeks therapy with apremilast.
Figure 2.
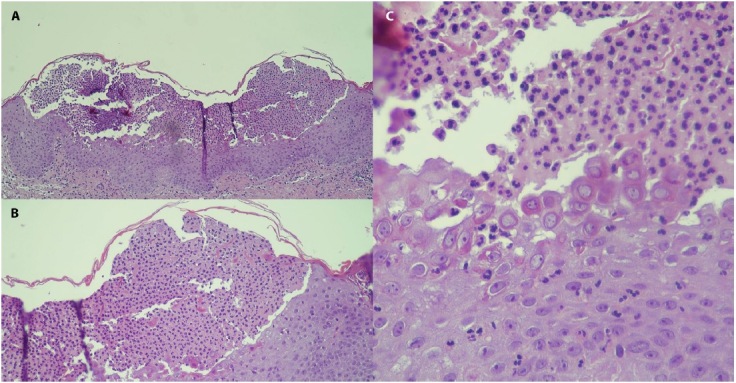
(A,B) Histopathology displaying a subcorneal pustule with thin roof leaning on the malpighian layer slightly sunken and an absent granular layer (H&E, 4x and H&E, 10x, respectively). (C) The superficial epidermis shows an acantholytic appearance below the pustule together with a granulocytic exocytosis (H&E, 40x).
Considering the contraindication of immunosuppressants due to unfavorable prognostic factors related to the primary tumor, we decided to initiate oral apremilast treatment at a dosage of 30 mg twice a day. Remarkably, complete remission of the disease was achieved within two months (Figure 1B). No side effects or relapses occurred during six-month follow-up.
In the management of SPD, oral dapsone is commonly considered as the initial treatment of choice. Several therapeutic alternatives are available, including sulphapyridines, nicotinamide, oral corticosteroids, retinoids, and phototherapy [1]. In some cases, off-label use of tumor necrosis factor-alfa blocking agents, interleukin-23 inhibitor (guselkumab) has also been reported as a potential treatment option [2]. Furthermore, a case demonstrating improvement of recalcitrant SPD with the use of apremilast has been documented [3].
Apremilast is an oral, small molecule inhibitor of phosphodiesterase 4 (PDE4) that has gained approval for treating psoriatic arthritis, Behcet disease and moderate-to-severe plaque psoriasis. It is also utilized off-label for the treatment of various dermatological conditions, including atopic dermatitis, hidradenitis suppurativa, alopecia areata and linear IgA bullous disease [4].
The exact pathogenesis of SPD is still unknown. The subcorneal pustules are a result of neutrophil aggregation within the stratum corneum. Importantly, higher levels of multiple neutrophilic chemotactic factors including IL-8 and TNF-α have been observed within the uppermost epidermis and in the blister fluid, but also in the bloodstream [1]. Apremilast not only inhibits the production of IL-8, a crucial chemotactic factor for neutrophils but also reduces the levels of other proinflammatory cytokines such as TNF-α [5]. These cytokines play a significant role in neutrophil recruitment and infiltration, contributing to the disease pathogenesis. Furthermore, apremilast represents a drug with a highly favorable safety profile and can be used in patients with specific comorbidities, such as a personal history of cancer.
Conclusions
In conclusion, this case report highlights the remarkable therapeutic efficacy of apremilast in the management of SPD, particularly in cases where conventional and off-label treatments have shown limited response or are contraindicated.
Footnotes
Funding: None.
Competing Interests: None.
Authorship: All authors have contributed significantly to this publication.
References
- 1.Cheng S, Edmonds E, Ben-Gashir M, Yu RC. Subcorneal pustular dermatosis: 50 years on. Clin Exp Dermatol. 2008;33(3):229–233. doi: 10.1111/j.1365-2230.2008.02706.x. [DOI] [PubMed] [Google Scholar]
- 2.Teraki Y, Sugai S. Treatment of recalcitrant subcorneal pustular dermatosis with guselkumab. Int J Dermatol. 2021;60(4):e153–e154. doi: 10.1111/ijd.15311. [DOI] [PubMed] [Google Scholar]
- 3.Magdaleno-Tapial J, Valenzuela-Oñate C, Alonso-Carpio M, et al. Improvement of recalcitrant Sneddon-Wilkinson disease with apremilast. Australas J Dermatol. 2020;61(2):185–186. doi: 10.1111/ajd.13253. [DOI] [PubMed] [Google Scholar]
- 4.Maione V, Bettolini L, Venturuzzo A, Tonon F, Battocchio S, Calzavara-Pinton P. Efficacy of apremilast in a case of resistant linear IgA bullous disease. Int J Dermatol. 2023;62(5):e300–e302. doi: 10.1111/ijd.16548. [DOI] [PubMed] [Google Scholar]
- 5.Schett G, Sloan VS, Stevens RM, Schafer P. Apremilast: a novel PDE4 inhibitor in the treatment of autoimmune and inflammatory diseases. Ther Adv Musculoskelet Dis. 2010;2(5):271–278. doi: 10.1177/1759720X10381432. [DOI] [PMC free article] [PubMed] [Google Scholar]