

Abstract
Single coronary artery is a rare congenital anomaly in which a single coronary artery arises from the aortic root that supplies the entire heart. It has variable clinical presentations ranging from a completely benign course to sudden cardiac death. Identifying and categorizing to high-risk type based on clinical presentation and anatomical features can present adverse cardiac events and provides better prognosis.
INTRODUCTION
Coronary artery anomalies are infrequent occurrences, with a prevalence of 1.33% in the general population [1]. Among these anomalies, the presence of a single coronary artery (SCA) is an exceptionally rare phenomenon where a solitary vessel originates from the aortic trunk to supply the entire heart. The prevalence of SCA ranges from 0.024% [2] to 0.066% [3] in individuals who have undergone coronary angiography. Complications associated with these anomalies can range in severity, from being asymptomatic to sudden death. Particularly, the course of the vessel between the aorta and pulmonary artery may result in compression during or after physical exertion [4]. Hence, awareness of such situations is crucial. In this report, we present an unusual case involving the absence of the right coronary artery and the left main coronary artery with separate left anterior descending artery and left circumflex artery ostia, detected through left heart catheterization.
CASE PRESENTATION
A 51-year-old Asian male was referred to our hospital outpatient cardiology clinic with a history of hyperlipidemia and hyperuricemia complained of gradually worsening retrosternal chest discomfort that did not radiate, occurring over a period of three months. The symptoms lasted approximately 10 min on average and subsided on their own after rest. Physical examination and vital signs were within normal limits. Resting electrocardiogram (ECG) showed a normal sinus rhythm with non-specific ST-T changes. Transthoracic echocardiogram indicated normal left ventricular function, valve function, and no regional wall motion abnormalities. An exercise stress test revealed horizontal ST depression exceeding 1 mm in the inferolateral leads, without concurrent chest pain, at 87% of the predicted maximal heart rate (Fig. 1).
Figure 1.

Exercise stress ECG showing horizontal 2 mm ST depression in multiple leads on early recovery.
Given suspected coronary artery disease, the patient underwent coronary angiography. The angiogram revealed separate origins for the left anterior descending artery (LAD) (Fig. 2) and the left circumflex artery (LCx). Mild, non-obstructive atherosclerosis was observed in the dominant LCx, which continued along the anatomical course of the right coronary artery (RCA) (Fig. 3). Injection into the right sinus of Valsalva unveiled the absence of a separate right coronary ostium from the aorta (Fig. 4). While arriving at a diagnosis for this case report, considerations of differential diagnoses, such as right coronary artery occlusion, were taken into account. The identification of an anomalous vessel in the anatomical course and the absence of regional wall motion abnormalities in the right coronary artery territory were crucial in reaching this conclusion. We didn’t offer other imaging tests like CT scanning or cardiac MRI given the fact that course of the vessel was clear on angiography alone. The patient was prescribed a beta-blocker, high-intensity statin, and a nitrate. As follow-up visits are pending, the patient has yet to return to the clinic. Initial steps will involve maximally tolerated medical therapy, and if significant symptoms persist, further interventions will be considered.
Figure 2.

The separate origin of left anterior descending artery with a normal course.
Figure 3.
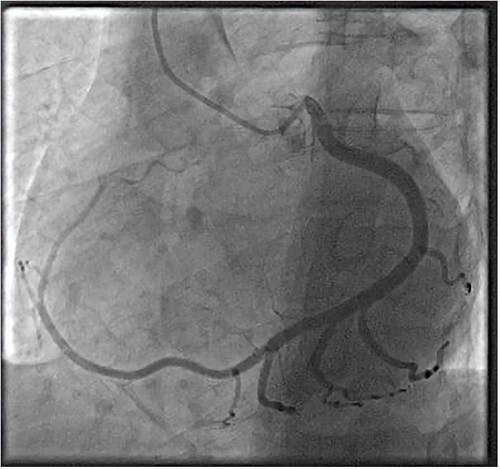
Left circumflex artery originating from left coronary sinus that terminates in the posterior atrioventricular groove to occupy RCA territory. Absence of right coronary artery with tiny branches originating from right coronary sinus.
Figure 4.

Absence of right coronary artery with tiny branches originating from right coronary sinus.
DISCUSSION
The occurrence of distinct origins for the right coronary artery and its conal branch is noted in 50% [5] of the population, while the left circumflex and left anterior descending artery exhibit separate origins in only 1% [5]. Notably, anomalies can involve the origin of the left main or left anterior descending artery from the right sinus of Valsalva or the right coronary artery, termed anomalous aortic origin of a coronary artery (AAOCA) [6]. The subsequent course of the vessel between the aorta and pulmonary artery can lead to vessel compression, myocardial ischemia, and even sudden death, particularly among young adults and teenagers [7]. Alternatively, an intramural course and acute angle of takeoff may predispose the vessel to flow obstruction. While complications are rare, they can occur during or immediately after exercise. Although sudden death might happen without warning symptoms, mechanism of cardiac events includes exercise-induced expansion of the aortic root and pulmonary trunk inducing flow reduction, potentially resulting in fatal ventricular arrhythmias and sudden death. Furthermore, compression can accentuate pre-existing coronary take-off angulation, reducing the luminal area proximally [8]. In cases where a single coronary artery originates from the right sinus of Valsalva, compression of the left anterior descending artery or its branches can occur through the same mechanism. Similarly, an origin of the right coronary artery from the left sinus of Valsalva or the left anterior descending artery can lead to myocardial ischemia and sudden death. In contrast, the origin of the left circumflex artery from the right sinus of Valsalva or the right coronary artery is generally considered clinically insignificant due to the posterior course of the vessel.
The reported incidence of abnormal aortic origin of coronary arteries is relatively low, with an approximate occurrence of 0.64% of births [9]. The most prevalent anomaly involves the left circumflex artery originating from the right sinus of Valsalva, followed by a single right coronary artery originating from the left sinus of Valsalva, both coronary arteries originating from the right sinus of Valsalva, and the left anterior descending artery originating from the right sinus of Valsalva [1]. In the present case, the right coronary artery is observed as a continuation of the distal left circumflex artery, a rather unusual scenario.
The exact underlying cause remains uncertain, yet prevailing hypotheses suggest that a deficiency in the development of a specific artery or the occurrence of artery occlusion during embryonic stages might account for the singular ostium and artery anomaly [10]. With advancing age, this anomaly can lead to clinical implications. Normally, the SA (sinoatrial) and AV (atrioventricular) nodes receive blood supply from the right coronary artery (RCA). However, when a single left coronary artery supplies these nodes, it can lead to premature degeneration due to inadequate blood flow, potentially resulting in bradyarrhythmia. Additionally, an overburdened single left coronary artery could enlarge, form fistulas, exert pressure on adjacent structures, induce early endothelial damage, and promote the onset of early atherosclerosis. In 2000, Basso and colleagues documented 27 instances of sudden death in young competitive athletes through post-mortem examinations, revealing origins of coronary arteries from incorrect sinuses (left main coronary artery from the right sinus in 23 cases, and right coronary artery from the left sinus in 4 cases) [11]. Most of these cases exhibited no clinical symptoms or diagnostic testing during their lifetime. Therefore, early detection of this critical anomaly is imperative, necessitating vigilant monitoring and maintaining a low threshold for invasive interventions.
Typically discovered incidentally, symptomatic single coronary artery (SCA) cases manifest a diverse array of symptoms, including palpitations, syncope, heart failure, and chest discomfort. While younger patients typically show no symptoms, older patients may experience symptoms as a result of concurrent atherosclerotic disease development.
Diagnosing this condition can pose challenges, particularly when patients remain asymptomatic, which is frequently the case in younger patients [12]. Employing multimodal imaging techniques such as coronary computed tomography angiography and cardiac magnetic resonance can provide valuable insights before resorting to invasive left heart catheterization. In our case, coronary angiography was conducted as part of an ischemic assessment prompted by a positive stress electrocardiogram (ECG) test. Multimodality imaging was not done in our case owing to the fact that it will not add any diagnostic value as vessel course was clear. Recognizing the interarterial pathway of an anomalous vessel is of paramount importance, necessitating a comprehensive evaluation of the entire vessel course. In our patient’s situation, the right coronary artery (RCA) was situated in the atrioventricular (AV) groove, making the likelihood of compression exceedingly rare.
Upon diagnosis, there is no established universal treatment criterion. Many anomalies are discovered incidentally and may not require specific treatment in the absence of related symptoms. Treatment decisions are often guided by the management of associated risk factors. Non-invasive approaches encompass strategies such as lipid-lowering interventions, blood pressure control, and anti-platelet therapy.
For cases requiring more invasive measures, treatment options are determined based on clinical necessity. These options encompass percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), or the implantation of a pacemaker [13]. Optimal management for each specific case must strike a balance between potential benefits and risks. In instances where high-risk characteristics are identified—such as an interarterial course, acute vessel take-off, valve-like ridge, or intramural path—in younger patients, surgical correction may be considered. In cases with significant atherosclerotic disease, PCI can be pursued [13].
However, it’s important to acknowledge that a percutaneous approach may pose certain challenges, including difficulties in cannulation and guide support, as well as the potential need for shorter guide or longer balloon and stent delivery catheters to access target lesions. It’s worth noting that the presented case encountered no difficulties in the cannulation process.
CONCLUSION
Congenital coronary artery anomalies, although infrequent, demand a heightened clinical suspicion. A single coronary artery supply, especially the absence of the right coronary artery, represents an exceedingly rare occurrence. Prompt identification and management aligned with the presenting clinical signs are of paramount importance. While left heart catheterization serves as a diagnostic tool to assess abnormal origins, a comprehensive approach involving multi-modality imaging may offer deeper insights into the vessel’s course.
Treatment, which isn’t always necessary for the incidental findings, frequently involves non-invasive medical therapy. However, cases might also necessitate revascularization procedures (PCI, CABG), or the insertion of pacemakers. Developing an understanding of high-risk attributes will aid in formulating a comprehensive treatment strategy.
Contributor Information
Murari Prasad Barakoti, Department of Cardiology, ADK Hospital, Male, Republic of Maldives.
Mohamed Shafiu, Department of Cardiothoracic and vascular surgery, ADK Hospital, Male, Republic of Maldives.
Kaushal Kishore Tiwari, Department of Cardiothoracic and vascular surgery, ADK Hospital, Male, Republic of Maldives.
Sadip Pant, PrimaCare PC, St Anne's Hospital, 289 Pleasant St, Fall River, MA, USA.
REFERENCES
- 1. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Catheter Cardiovasc Diagn 1990;21:28–40 PMID: 2208265. [DOI] [PubMed] [Google Scholar]
- 2. Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology 1979;130:39–47 PMID: 758666. [DOI] [PubMed] [Google Scholar]
- 3. Desmet W, Vanhaecke J, Vrolix M, Van de Werf F, Piessens J, Willems J. et al. Isolated single coronary artery: a review of 50,000 consecutive coronary angiographies. Eur Heart J 1992;13:1637–40 PMID: 1289093. [DOI] [PubMed] [Google Scholar]
- 4. Said SA, de Voogt WG, Bulut S, Han J, Polak P, Nijhuis RL. et al. Coronary artery disease in congenital single coronary artery in adults: a Dutch case series. World J Cardiol 2014;6:196–204 PMID: 24772259; PMCID: PMC3999339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.https://www.uptodate.com/contents/congenital-and-pediatric-coronary-artery-abnormalities
- 6. Cheezum MK, Liberthson RR, Shah NR, Villines TC, O'Gara PT, Landzberg MJ. et al. Anomalous aortic origin of a coronary artery from the inappropriate sinus of Valsalva. J Am Coll Cardiol 2017;69:1592–608 PMID: 28335843. [DOI] [PubMed] [Google Scholar]
- 7. Barth CW 3rd, Roberts WC. Left main coronary artery originating from the right sinus of Valsalva and coursing between the aorta and pulmonary trunk. J Am Coll Cardiol 1986;7:366–73 PMID: 3944356. [DOI] [PubMed] [Google Scholar]
- 8. Cheitlin MD, De Castro CM, McAllister HA. Sudden death as a complication of anomalous left coronary origin from the anterior sinus of Valsalva, a not-so-minor congenital anomaly. Circulation 1974;50:780–7 PMID: 4419670. [DOI] [PubMed] [Google Scholar]
- 9. Kimbiris D, Iskandrian AS, Segal BL, Bemis CE. Anomalous aortic origin of coronary arteries. Circulation 1978;58:606–15 PMID: 567544. [DOI] [PubMed] [Google Scholar]
- 10. Silva-Juior G d O, Miranda SW d S, Mandarim de Lacerda CA. Origin and development of the coronary arteries. Int J Morphol 2009;27:891–8 ISSN 0717-9502. [Google Scholar]
- 11. Basso C, Maron BJ, Corrado D, Thiene G. Clinical profile of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes. J Am Coll Cardiol 2000;35:1493–501 PMID: 10807452. [DOI] [PubMed] [Google Scholar]
- 12. Ahmed A, Assaf A, Mantha Y, Small D, Zughaib M. A rare anatomical variant: congenital absence of the right coronary artery with left circumflex artery supplying the right coronary artery (RCA) territory. Am J Case Rep 2021;22:e932248 PMID: 34437516; PMCID: PMC8406439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Angelini P. Coronary artery anomalies—current clinical issues: definitions, classification, incidence, clinical relevance, and treatment guidelines. Tex Heart Inst J 2002;29:271–8 PMID: 12484611; PMCID: PMC140289. [PMC free article] [PubMed] [Google Scholar]