

Abstract
Innovations in projectile design present unique challenges for trauma surgeons when treating gunshot victims. The G2 Radically Invasive Projectile (G2 Research, Winder, Georgia, USA) (G2RIP) is a frangible, rapidly expanding bullet resulting in a distinct pattern of injury consisting of diffuse hemorrhage with multicavity trauma as well as unique radiographic features of the projectile. To efficiently manage patients injured by the G2RIP, trauma surgeons must be aware of these distinct characteristics, and of previous patterns in effective management such as liberal damage control and extensive use of CT. Understanding previous presentation and management of patients injured by the G2RIP can aid in improving patient care in the trauma center.
Keywords: Wounds, Gunshot; Firearms; Multiple Trauma
Introduction and background
Firearm ballistics, including projectile design and velocity, convey unique injury patterns and lethality.1 2 Trauma providers will benefit from a familiarity with novel ballistics that may affect clinical management. In this report, we discuss the case of a patient injured by a single gunshot wound using a G2 Radically Invasive Projectile (G2RIP) (figure 1) and review the current literature in its regard to fragmenting firearm bullets.
Figure 1.

G2 Radically Invasive Projectile ammunition.
Case report
A patient in their mid-30s presented hypotensive, tachycardic, and with altered mental status to an American College of Surgeons-verified level one trauma center with a single gunshot wound to the left anterior thoracoabdomen. Chest and abdominal plain radiography indicated multiple small projectiles in the midline at the diaphragm and in the mid-abdomen (figure 2). The patient underwent immediate laparotomy and was found to have multiple left phrenotomies with left hemothorax, massive hemoperitoneum with lacerated spleen and pancreatic tail, hilar laceration to the left kidney with large perinephric hematoma, and lacerated stomach and colon. Left nephrectomy, splenectomy, colectomy, gastrorrhaphy, and phrenorrhaphy were performed.
Figure 2.
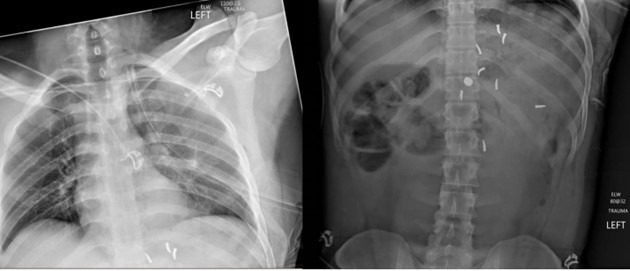
Chest and abdominal plain radiograph.
Multiple small pointed metallic objects were found in the peritoneal cavity (figure 3).
Figure 3.

Foreign body from peritoneal cavity.
Though it appeared the life-threatening injuries had been addressed, the patient continued to have ongoing bleeding from the left thoracostomy. The midline laparotomy was extended across the costal margin into a left anterolateral thoracotomy. There was no hemopericardium, but numerous lacerations were evident along the parietal pleura along the spine, and there were multiple intercostal vessel lacerations. Hemorrhage control was achieved with suture ligation. No aortic or esophageal laceration was encountered. After surgical hemorrhage control was achieved, a temporary closure was performed, and the patient underwent CT imaging. CT showed foreign bodies scattered throughout the torso, including in proximity to the esophagus (figure 4). No new injuries were identified on CT. The following day, the patient returned to the operating room where they underwent esophagogastroduodenoscopy revealing foreign bodies but no esophagotomy or new gastrotomy. The patient’s chest and abdomen were partially closed. At a third and final laparotomy, distal pancreatectomy was performed for a saponified, injured distal pancreas, as well as colon anastomosis and diverting ileostomy. The patient’s postoperative course was complicated by the development of an abdominal abscess requiring percutaneous drainage. The patient was discharged home on hospital day 31.
Figure 4.
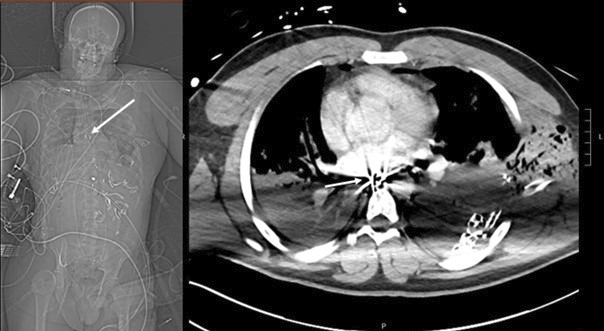
Torso CT. Arrows indicate radiopaque foreign body in proximity to the esophagus.
Discussion
Ballistics of the G2RIP round made this case unique. Though there was one external ballistic injury on physical examination, radiography and operation revealed numerous projectiles. The dispersion of projectiles was wide and non-uniform. The non-uniform dispersion may be related to the non-uniform composition of the solid and hollow viscera.3 4 As in this case, the non-uniform trajectory of the individual trocars can lead to diffuse bleeding in regions distant from the entry wound or final position of the trocars themselves. Further, due to their sharpened edges and small size, trocars are prone to migration within the body cavities, possibly leading to inconsistencies among interval films and between radiography and surgery. Although traditional bullets will generally enter and exit the gastrointestinal tract, the G2RIP trocar appears more likely to come to rest in the lumen of the gastrointestinal tract. Though the RIP round presents multiple unique challenges, the characteristic appearance of the trocars on film will alert the astute clinician to their presence.
Literature reports regarding the G2RIP round are limited to single cases or small case series; however, all previous reports reflect a unique pattern of injury associated with this ammunition. Understanding this pattern of injury will prepare trauma providers to manage the likely numerous distinct injuries more quickly and efficiently. Table 1 summarizes previously reported cases and their associated patterns of injury (table 1).
Table 1.
Reported cases on G2RIP round
| Reference | Age | Sex | Report emphasis | Multisystem trauma | Diffuse hemorrhage | Proximal dispersion | Distal base progression | Irregular trajectory | Trocar exit | Non separated trocars | Trocars in GI lumen | Common exit wound | Trocar migration |
| 3 | 34 | Female | Radiologic evaluation | X | X | X | |||||||
| 3 | 27 | Male | Radiologic evaluation | X | X | X | |||||||
| 3 | 19 | Male | Radiologic evaluation | X | X | ||||||||
| 3 | 23 | Female | Radiologic evaluation | X | |||||||||
| 7 | 24 | Male | Radiologic evaluation | X | X | ||||||||
| 7 | 24 | Male | Radiologic evaluation | X | X | ||||||||
| 7 | 35 | Male | Radiologic evaluation | X | X | ||||||||
| 6 | 15 | Male | Surgical management | X | X | X | |||||||
| 5 | 22 | Male | Surgical management | X | X | ||||||||
| 4 | 25 | Female | Radiologic evaluation | X | X | X | X | ||||||
| Current report | 30s | Surgical management | X | X | X | X | X |
GI, gastrointestinal; G2RIP, G2 Radically Invasive Projectile.
Two reports of the G2RIP round have focused on relevance to the trauma surgeon. In both prior reports, as in this report, damage control surgery was required because of the complexity of the injuries and severe physiologic derangement of the victims. Additionally, torso CT was performed after the first trauma operation to fully understand the extent of the injury and prepare for the next operation. A third common characteristic of the G2RIP round is the involvement of multiple body regions. Our patient had thoracic and abdominal involvement, as was reported by Hakki et al.5 Iverson et al reported abdominal and proximal lower extremity involvement.6 Although cavity penetration of the trocars depends on impact location, tissue composition, and ballistic variables, it is worth noting that the trocars do have the potential to cause massive organ damage in multiple cavities. Finally, the use of gastrointestinal endoscopy, as in the case reported here, has been previously described. Though the use of gastrointestinal endoscopy is not unusual in trauma surgery, the fact that two of three reported cases used gastrointestinal endoscopy to identify portions of the projectile suggests the propensity of the trocars to reside in the gastrointestinal lumen.
Conclusion
The G2RIP round is a novel projectile that presents unique challenges for the trauma surgeon. Its radiographic features are characteristic, making preoperative scout X-ray of the entire torso particularly high yield for surgical planning. By recognizing its appearance, the trauma surgeon can prepare for its complex and extensive injury pattern. We recommend the surgeon be prepared to explore multiple cavities or body regions at the first operation, liberally use damage control and CT, and be prepared to use endoscopy to locate all of the projectiles and injuries.
Footnotes
Contributors: MB conducted the literature search and drafted the article. CMD provided critical review. AMK provided critical review. AB conducted the literature search and drafted the article.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Ethics statements
Patient consent for publication
Obtained.
Ethics approval
This research was exempted from full review by the Institutional Review Board at the University of Kentucky because it was judged to present minimal risks to research subjects.
References
- 1.Rhee PM, Moore EE, Joseph B, Tang A, Pandit V, Vercruysse G. Gunshot wounds: A review of ballistics, bullets, weapons, and myths. J Trauma Acute Care Surg 2016;80:853–67. 10.1097/TA.0000000000001037 [DOI] [PubMed] [Google Scholar]
- 2.Padrta JC, Barone JE, Reed DM, Wheeler G. Expanding handgun bullets. J Trauma 1997;43:516–20. 10.1097/00005373-199709000-00022 [DOI] [PubMed] [Google Scholar]
- 3.Ditkofsky N, Maresky HS, Steenburg S. Radically invasive projectiles-first reports and imaging features of this new and dangerous bullet. Emerg Radiol 2020;27:393–7. 10.1007/s10140-020-01766-5 [DOI] [PubMed] [Google Scholar]
- 4.Zhang X, Cain MD, Williams CD, Spears TA, Poulos CK. G2 research radically invasive projectile: the importance of recognizing its imaging and autopsy patterns. Am J Forensic Med Pathol 2021;42:248–51. 10.1097/PAF.0000000000000669 [DOI] [PubMed] [Google Scholar]
- 5.Hakki L, Smith A, Babin J, Hunt J, Duchesne J, Greiffenstein P. Effects of a Fragmenting handgun bullet: considerations for trauma care providers. Injury 2019;50:1143–6. 10.1016/j.injury.2019.01.033 [DOI] [PubMed] [Google Scholar]
- 6.Iverson KR, Curtis E, Brown IE, Salcedo ES, Anderson JT. New Fragmenting bullet leads to unexpected injury pattern: A case report involving the radically invasive projectile. Trauma 2019;21:73–6. 10.1177/1460408618759365 10.1177/1460408618759365 [DOI] [Google Scholar]
- 7.Stacy GS, Thomas S. The G2 research R.I.P. Fragmenting bullet-radiographic features of a recently encountered projectile. Skeletal Radiol 2020;49:1663–8. 10.1007/s00256-020-03486-w [DOI] [PubMed] [Google Scholar]