

Abstract
Socioeconomic status (SES) is associated with white matter hyperintensities (WMH) and contributes to racial/ethnic health disparities. However, traditional measures of SES may not accurately represent individual financial circumstances among non-Latinx Black and Latinx older adults due to longstanding structural inequities. This study examined associations between multiple SES indicators (education, income, subjective financial worry) and WMH across non-Latinx Black, Latinx, and non-Latinx White older adults in the Washington Heights-Inwood Columbia Aging Project (N = 662). Latinx participants reported the lowest SES and greatest financial worry, while Black participants evidenced the most WMH. Greater financial worry was associated with higher WMH volume above and beyond education and income, which were not associated with WMH. However, this association was only evident among Latinx older adults. These results provide evidence for the minority poverty hypothesis and highlight the need for systemic socioeconomic interventions to alleviate brain health disparities in older adulthood.
Keywords: White Matter Hyperintensities, Socioeconomic Status, Racial/Ethnic Disparities, Aging
1. Introduction
Socioeconomic status (SES) has long been studied as a predictor of overall and brain health outcomes because it indicates the extent to which individuals may be able to access resources that are helpful in preventing, delaying, or combatting pathology (Beydoun et al., 2014; Marden et al., 2017; Zahodne et al., 2015). Prior research examining the effect of SES on brain outcomes indicates that lower SES is associated with lower global, gray matter, and white matter brain volumes (McEwen and Gianaros, 2010; Waldstein et al., 2017), as well as lower hippocampus and amygdala volumes (Shaked et al., 2019a; Shaked et al., 2019b). In addition to lower brain volumes, lower SES is associated with indicators of cerebrovascular disease, including white matter hyperintensities (WMH) and stroke. Links between SES and brain health may involve inflammatory (Gianaros et al., 2013), stress (Adler & Newman, 2002; McEwen & Gianaros, 2010), and metabolic (Gianaros et al., 2017) pathways.
Importantly, all of these brain health indicators are associated with increased risk of Alzheimer’s disease and related dementias (ADRD; Brickman et al., 2015). White matter hyperintensities in particular are important to consider in the context of ADRD because they may represent cardiovascular contributions to ADRD pathogenesis (Erten-Lyons et al., 2013; Launer, 2004). White matter hyperintensities are strongly associated with cognition and incident dementia (Brickman et al., 2015, 2012, 2009; Zahodne et al., 2015) and may be a key mechanism underlying racial/ethnic disparities in ADRD prevalence in non-Latinx Black and Latinx older adults.
WMH are thought to result from chronic hypoprofusion and chronic ischemic small vessel disease (Launer, 2004; Luchsinger and Mayeux, 2004), both of which can be caused by increased cardiovascular disease risk factors, such as hypertension and atherosclerosis, as well as heart disease. These risk factors have important social and structural determinants (e.g., SES, access to healthy food and medical care) that lead to stark racial/ethnic disparities in cardiovascular disease (Lopez-Neyman et al., 2022; Javed et al., 2022). Because cardiovascular disease risk is strongly influenced by social and structural determinants of health that disadvantage many non-Latinx Black and Latinx individuals, further studying the associations between such social determinants (i.e., SES) and clinical-pathological intermediates of ADRD (i.e., WMH) is important for alleviating health inequity. Disadvantaged socioeconomic circumstances, such as stress related to finances, may be uniquely important to study when considering disparities in risk factors for ADRD (e.g., in WMH) among non-Latinx Black and Latinx older adults.
While existing research documents associations between lower SES and worse brain health outcomes (McEwen and Gianaros, 2010; Waldstein et al., 2017), a limitation of this research is the use of limited indicators to estimate SES, such as years of education or total income. While education and income are important aspects of SES, they may not capture the full picture of an individual’s socioeconomic position because they do not entirely account for available material resources (e.g., assets) or the extent to which socioeconomic resources are sufficient given other individual-level factors, such as family size, amount of debt, medical expenses, and other financial strains. Given the multitude of factors relevant to SES, asking individuals about all possible factors is impractical (Adler et al., 2012). In this case, subjective and/or aggregate indicators of SES may better capture the day-to-day reality of finances and better reflect individuals’ specific circumstances. Indeed, measures of subjective social status predict health outcomes above and beyond traditional socioeconomic indicators such as education and income (Adler et al., 2000; Goodman et al., 2003; Hu et al., 2005; Singh-Manoux et al., 2003). For example, Zahodne and colleagues (2018) found that subjective social status, as estimated by how participants viewed their social position in society, was associated with episodic memory independent of educational attainment, occupation, income, and wealth. However, it is unknown whether subjective social status predicts brain health outcomes above and beyond traditional SES measures.
Financial worry, a subjective measure of SES that indicates how much individuals worry that their expenses will exceed their income, may more accurately reflect individuals’ day-to-day financial circumstances and their potential health impact than traditional indicators (Figure 1). While traditional indicators such as income and education measure specific resources available to an individual, financial worry assesses whether all of an individual’s available resources are sufficient in meeting their unique financial obligations. Although measures of financial worry do not explicitly query individual-level factors that can influence financial obligations such as family size or debt, individuals likely take these considerations into account when answering the holistic question of how much they worry about their finances. Furthermore, the subjective nature of financial worry may better capture the stress and/or strain individuals experience in relation to their socioeconomic status. Given that socioeconomic status is theorized to influence brain health, in part, through stress and/or inflammatory pathways (Adler and Newman, 2002; Gianaros et al., 2013; McEwen and Gianaros, 2010), financial worry may be a more proximal predictor of physiological dysregulation and poor health, as illustrated in Figure 1.
Figure 1.
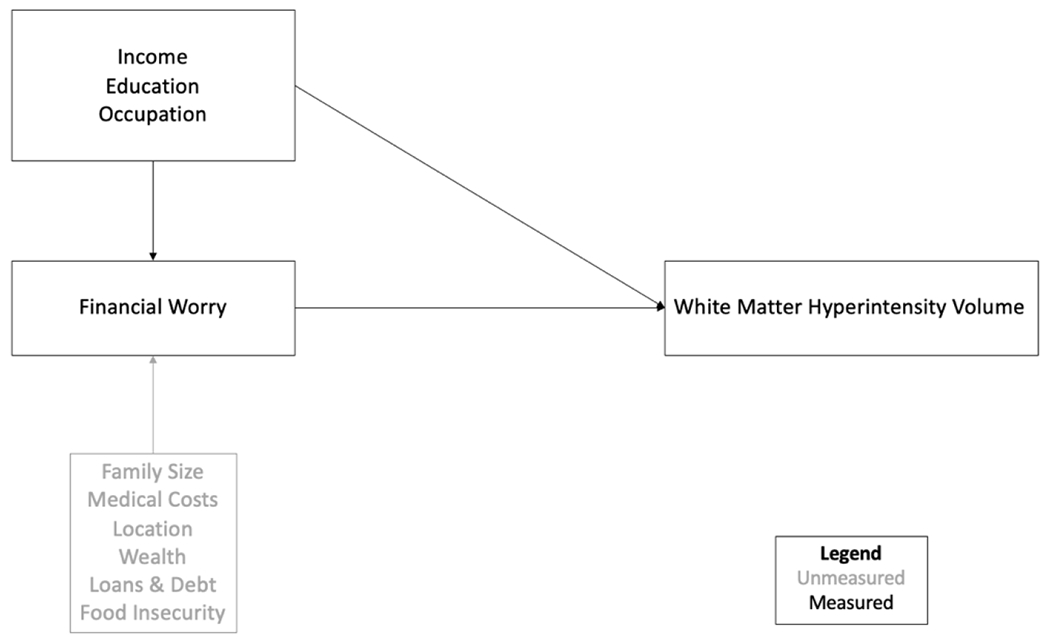
Conceptual model of factors contributing to financial worry and proposed model of associations between financial worry, traditional indicators of socioeconomic status, and white matter hyperintensity volume.
Financial worry may be particularly predictive of brain health among non-Latinx Black and Latinx individuals, for whom traditional socioeconomic indicators (e.g., income, education) are not entirely representative of financial reality. According to the diminishing returns hypothesis, non-Latinx Black Americans in particular do not reap the same health benefits of high SES (as typically indicated by education, income, and employment) as non-Latinx White Americans (Farmer and Ferraro, 2005; Shuey and Willson, 2008) as a result of racial discrimination that increases barriers to or prevents important health behaviors, such as access to health care. With regard to brain health, Waldstein and colleagues (2017) found that the association between higher SES (i.e., income and whether the participant was above the poverty line) and greater brain volumes was stronger among non-Latinx White participants than among non-Latinx Black participants. Consistent with the diminishing returns hypothesis, this finding was driven by smaller brain health benefits for non-Latinx Black individuals in the high SES group compared with non-Latinx White participants (Farmer and Ferraro, 2005; Shuey and Willson, 2008). This study also found that the association between lower SES and more white matter lesions was stronger among non-Latinx Black participants than among non-Latinx Whites (Waldstein et al., 2017). This latter finding is in line with the minority poverty hypothesis, which states that racial disparities in health are greatest at the lowest levels of SES (Farmer and Ferraro, 2005). Together, these results suggest that SES-brain health associations may differ across non-Latinx Black and non-Latinx White adults. While the diminishing returns and minority poverty hypotheses are well documented in terms of Black-White health disparities, less is known about whether these patterns extend to Latinx individuals in the US (Aponte, 1991; Assari and Bazargan, 2020).
Traditional indicators of SES may also be less predictive of health in historically marginalized groups due to unique financial circumstances resulting from structural racism and cultural norms (Shavers, 2007). For example, Latinx and non-Latinx Black adults in the US are disproportionately affected by racist policies in lending and housing, such as redlining, which lead to more limited opportunities for accumulating wealth and accessing high quality, affordable health care. Latinx adults also tend to have larger families (Cohn and Passel, 2018; Landale et al., 2006), and due to financial need and/or cultural preferences, both Latinx and non-Latinx Black adults are more likely to live in multi-generational households (Cohn and Passel, 2018), which can lead to greater household expenses. Latinx immigrants in particular may also be supporting family members in their country of origin (Calzada et al., 2012; López-Anuarbe et al., 2015). As a result, these groups may experience greater financial worry more so than non-Latinx Whites even at the same income level. Therefore, subjective, aggregate indicators of SES may be particularly useful to better approximate financial conditions and estimate how financial strain influences health outcomes across race/ethnicity.
This study examined whether: 1) financial worry was associated with WMH above and beyond markers of SES that are more commonly considered in epidemiological research (i.e., education and income); and 2) associations between SES (financial worry, education, income) and WMH differed across racial and ethnic groups. Based on prior research examining links between SES and brain health as well as subjective SES and cognition, we predicted that greater financial worry would be related to more WMH above and beyond traditional SES indicators. Based on the diminishing returns and minority poverty hypotheses, we also predicted that education and income would be less strongly associated with WMH, while financial worry would be more strongly associated with WMH, among Latinx and non-Latinx Black participants than non-Latinx White participants.
2. Methods
2.1. Participants
Participants were drawn from the Washington Heights-Inwood Columbia Aging Project (WHICAP; Manly et al., 2005; Tang et al., 2001), which is a prospective, community-based, longitudinal study of cognitive and brain aging in northern Manhattan. All WHICAP participants were identified from residents in northern Manhattan using Medicare lists and/or commercial marketing companies in recruitment efforts beginning 1992, 1999, and 2009 (ongoing). Enrolled participants are evaluated every 18-24 months. Beginning in 2011, a random sample WHICAP participants without dementia were invited to undergo 3T MRI. In 2017, WHICAP participants received an expanded psychosocial evaluation, which included a measure of financial worry. As of late 2020, 824 WHICAP participants had received both a baseline MRI scan and psychosocial questionnaires. A median of 2.29 years (SD = 2.20) passed between the date of MRI and the date at which psychosocial questionnaires were administered. Inclusion criteria for the present study were: (1) without a diagnosis of dementia at the time psychosocial questionnaires were completed, (2) self-reported race/ethnicity as non-Latinx White, non-Latinx Black, or Latinx (any race), and (3) had complete data on all covariates (i.e., age, sex/gender, education, income, depressive symptoms). Of the 824 participants, 25 participants were excluded because they identified as belonging to a racial/ethnic group other than non-Latinx White, non-Latinx Black, or Latinx, one participant was excluded due to missing race/ethnicity, 62 participants were excluded due to diagnosis of dementia or inability to be tested for dementia, and 74 were excluded due to missing covariates. The final sample comprised 662 participants.
2.2. Procedures
2.2.1. Exposure Variables
Financial worry was measured with the question, “How much do you worry that your total income will not be enough to meet your expenses and bills?” which was originally used in the 2005 Gallup Public Opinion Poll to estimate racial and ethnic differences in financial comfort (Arora, 2005). Participants were given the option to respond on a Likert-type scale to indicate their financial worry, as follows: (1) a great deal, (2) a lot, (3) a little, (4) not a lot. Responses were then reverse coded, such that higher scores indicated greater financial worry. Education was self-reported and operationalized as years (0-20). Joint (i.e., income of participant and their spouse, if applicable) monthly income was self-reported and coded into 12 ordinal categories ranging from $450 or less per month (1) to $4,000 or more per month (12), which was treated as a continuous variable in all analyses.
2.2.2. White Matter Hyperintensities
Structural MRI was conducted on a 3.0T Philips Achieva scanner at Columbia University Medical Center. T2-weighted fluid attenuated inversion recovery (FLAIR) images were acquired in the axial orientation (repetition time = 8000 ms, echo time = 332.0 ms, inversion time = 2400 ms, field of view = 240 mm x 240 mm x 180 mm matrix with 1mm x 1mm x 1mm resolution). Whole-brain WMH volumes were quantified from T2-weighted FLAIR images with in-house developed software (Brickman et al., 2012, 2011, 2009; Igwe et al., 2022). Briefly, images were brain extracted (Smith, 2002), and the intensity histogram was fit with a Gaussian curve. Voxels with intensities greater than 2.1 standard deviations above the image mean were labeled as WMH. WMH were visually inspected and manually corrected if needed; labeled voxels were summed and multiplied by voxel dimensions to yield volumes in cm3.
2.2.3. Covariates
Sex/gender was self-reported as male (0) or female (1). Participants were not asked to distinguish between sex and gender, so their response may indicate either or both. Race and ethnicity were self-reported separately using the format of the 2000 census. Race/ethnicity was dummy coded to reflect three non-overlapping categories (non-Latinx Black, Latinx [any race], or non-Latinx White). Non-Latinx White was the reference group. Depressive symptoms were quantified using the Centers for Epidemiological Study of Depression (CES-D; Radloff, 1977) scale. Cardiovascular disease burden was not included as a covariate, as it was hypothesized to lie in the causal pathway between financial worry and WMH volume.
2.3. Statistical Analysis
Sample characteristics and group differences were examined in SPSS 28. Analyses of variance (i.e., ANOVAs) were conducted to identify group differences in the variables of interest. Bivariate correlations among the SES variables (i.e., financial worry, joint monthly income, education) were examined separately in the entire sample and in each racial/ethnic group.
Primary models were conducted in Mplus version 8. To examine Aim 1 (does financial worry predict WMH above and beyond education and income?), a multiple regression examined the association between financial worry and total WMH controlling for age, sex/gender, depressive symptoms, race/ethnicity, education, and income. Of note, this model may have underestimated associations involving education and income because financial worry may reflect a mediator of associations between these traditional SES indicators and WMH. To explore this possibility, a path analysis estimated effects of education and income on WMH through financial worry. For Aim 2 (do associations between SES and WMH differ across race/ethnicity?), models analyzed for Aim 1 were stratified by race/ethnicity to further examine the relationship between SES and total WMH within each group based on prior research indicating that race/ethnicity stratified models may be an epidemiologically more accurate way to estimate racial/ethnic health disparities (Ward et al., 2019). Nonetheless, to statistically examine whether there was a different effect of financial worry on WMH across race and ethnicity, we also conducted multiple group models, constraining all variables of interest (i.e., education, income, financial worry), and then freeing one parameter at a time. These multiple group models examined differences between Latinx and non-Latinx Black participants, Latinx and non-Latinx White participants, and non-Latinx Black and White participants. Separate sensitivity analyses were conducted to examine whether 1) cardiovascular disease burden, 2) intracranial volume, or 3) time between MRI exam and psychosocial assessment influenced associations between financial worry and WMH.
3. Results
Table 1 summarizes the sample characteristics and unadjusted group differences, and specific pairwise comparisons and effect sizes are summarized in Supplementary Table 1. Latinx participants reported greater financial worry than non-Latinx Black and non-Latinx White participants; non-Latinx Black and non-Latinx White participants did not differ in financial worry. Levels of financial worry were somewhat low across all three groups. Of note, there was variance in financial worry across groups (i.e., the range was 1-4 in all three groups). Latinx participants had the fewest years of education, followed by non-Latinx Black and non-Latinx White participants. Latinx participants had the lowest monthly income, followed by non-Latinx Black and non-Latinx White participants. Non-Latinx Black participants had greater WMH volume than Latinx participants; however, neither non-Latinx Black nor Latinx participants had different WMH volume from non-Latinx White participants.
Table 1.
Sample characteristics.
| Entire Sample (N=662) |
Black (N=223) |
Latinx (N=271) |
White (N=168) |
Effect Size a | |
|---|---|---|---|---|---|
|
| |||||
|
M(SD) or % |
|||||
| Age at Scan | 74.25 (5.85) | 73.97 (6.01) | 75.11 (6.16) | 73.24 (4.89) | .017* |
| Education | 12.41 (4.61) | 13.80 (2.79) | 8.97 (4.23) | 16.12 (3.04) | .424* |
| Joint Monthly Income (1-12)b |
8.15 (3.00) | 8.78 (2.49) | 6.27 (2.46) | 10.35 (2.52) | .313* |
| % Female | 62.10% | 65.0% | 64.58% | 54.17% | .095 e |
| CESD total (1-8)c | 1.30 (1.70) | 1.25 (1.72) | 1.39 (1.74) | 1.23 (1.62) | .002 |
| Total WMH (in cm3)d | 4.47 (5.32) | 5.14 (5.42) | 3.94 (5.10) | 4.46 (5.46) | .009 |
| Financial Worry (1-4) | 1.62 (.82) | 1.57 (.76) | 1.79 (.86) | 1.41 (.78) | .035* |
| Vascular disease burden (0-3)f | 1.11 (.847) | 1.19 (.827) | 1.23 (.865) | .807 (.770) | .044 |
Note.
Effect size is partial eta2, except for % Female (see Note “e”).
indicates group difference at p < .05 using Bonferroni post-hoc correction. See Supplementary Tables 1 and 2 for specific pairwise comparisons and effect sizes.
Joint monthly income was self-reported and coded into ordinal categories ranging from 1-12. An “8” represents a joint monthly income of $1,501-$1,750; a “6” represents a joint monthly income of $1,001-$1250; and a “10” represents a joint monthly income of $2000-$3000.
CESD = Centers for Epidemiologic Studies of Depression Scale (Radloff, 1977)
WMH = white matter hyperintensities
Effect size is Cramer’s v
Vascular disease burden = count of hypertension, diabetes, and/or heart disease.
Table 2 summarizes bivariate correlations among the socioeconomic variables in the entire sample, as well as within each racial/ethnic group. There were small to moderate correlations between financial worry and the other SES constructs (i.e., education and income). In the entire sample, financial worry was moderately correlated with income (r = −.346, p < .001) but minimally with education (r = −.121, p = .002). Significant in all groups, correlations between financial worry and income were largest in non-Latinx White participants, followed by non-Latinx Black and Latinx participants. The largest correlation identified in the entire sample was between education and income in non-Latinx Black participants, followed by Latinx and non-Latinx White participants. Supplementary Tables 2 and 3 summarize Fisher’s r-to-z transformations, which show that associations between financial worry and WMH were reliably stronger in the Latinx group compared to the other groups. The association between financial worry and income was significantly weaker in the Latinx group compared to the non-Latinx White group. All other correlations did not differ reliably across groups.
Table 2.
Bivariate correlations among socioeconomic variables in the entire sample and in each racial/ethnic group.
| Entire Sample (N=662) |
Non-Latinx Black (N=223) |
Latinx (N=271) |
Non-Latinx White (N=168) |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | |
| 1. Financial Worry | - | −.346* | −.121* | .060 | - | −.305* | .039 | −.030 | - | −.224* | −.011 | .199* | - | −.418* | −.028 | .046 |
| 2. Joint Monthly Income | −.346* | - | .519* | −.011 | −.305* | - | .326* | −.065 | −.224* | - | .241* | −.014 | −.418* | - | .185* | −.103 |
| 3. Education | −.121* | .519* | - | .035 | .039 | .326* | - | −.041 | −.011 | .241* | - | −.037 | −.028 | .185* | - | .087 |
| 4. WMHa | .060 | −.011 | .035 | - | −.030 | −.065 | −.041 | - | .199* | −.014 | −.037 | - | .046 | −.103 | .087 | - |
Note.
p < .05. Values reflect two-tailed Pearson correlation coefficients.
WMH = White Matter Hyperintensities in cm3
3.1. Aim 1: Associations between Financial Worry and WMH
The multiple regression model summarized in Table 3 revealed that greater financial worry was associated with more WMH, even after accounting for education and income levels. Neither education nor income was a unique predictor of WMH in this model. A subsequent analysis explored whether associations involving education and income were masked by the inclusion of financial worry, which could represent a potential mediator of the effects of education and income. Results indicated no indirect effects of income (ß= −.023, SE = .014, p = .109) nor education (ß = .007, SE = .006, p = .221) on WMH volume through financial worry. These analyses, while cross-sectional and therefore limited in ability to evaluate mediation, confirm findings from the initial regression model and bivariate correlations indicating that financial worry is a related but separate construct from income and education, which are not strongly associated with WMH volume in this sample.
Table 3.
Regression models of adjusted associations between predictors and white matter hyperintensities.
| Entire Sample (N=662) |
Non-Latinx Black (N=223) |
Latinx (N=271) |
Non-Latinx White (N=168) |
|
|---|---|---|---|---|
|
| ||||
| Predictor | β [95% CI]a | |||
|
|
||||
| Age | .184* [.108, .259] | .192* [.061, .324] | .145* [.026, .264] | .235* [.091, .379] |
| Education | .035 [−.069, .139] | −.016 [−.156, .124] | −.019 [−.142, .104] | .136 [−.013, .286] |
| Joint Monthly Income | −.039 [−.139, .062] | −.059 [−.209, .091] | .056 [−.072, .183] | −.117 [−.283, .048] |
| Sex/Gender | −.054 [−.130, .022] | −.063 [−.196, .070] | −.024 [−.143, .094] | −.082 [−.231, .066] |
| Depressive Symptoms | −.040 [−.121, .042] | −.013 [−.167, .141] | −.062 [−.182, .057] | .003 [−.161, .179] |
| Financial Worry | .090* [.000, .180] | −.033 [−.188, .123] | .260* [.121, .399] | .008 [−.162, .179] |
| Black Race | .048 [−.050, .146] | - | - | - |
| Latinx Ethnicity | −.088 [−.216, .039] | - | - | - |
Note.
p < .05
CI = confidence interval
B = Standardized estimates
While depressive symptoms were included as a covariate in the primary model because of the potential for depressive symptoms to bias subjective reporting of financial worry, depressive symptoms could also represent a mediator of the association between financial worry and WMH. Therefore, a sensitivity analysis excluded depressive symptoms from the Aim 1 model. Without depressive symptoms as a covariate, the association between financial worry and WMH was no longer significant (ß = .082, SE = .044, p = .065, 95% CI [−.005, .169]). These results suggest that in this sample, depressive symptoms are not likely to mediate the association between financial worry and WMH because the effect size of financial worry on WMH decreased rather than increased when excluding depressive symptoms. These results also support the initial decision to covary for depressive symptoms to isolate financial worry from mood-related response bias.
3.2. Aim 2: Racial/Ethnic Differences in the Association between SES and WMH
As shown in Table 3, stratified models revealed that greater financial worry was associated with more WMH among Latinx participants but not among non-Latinx Black or non-Latinx White participants. These results are also illustrated in Figure 2. Among Latinx participants, greater financial worry was associated with increased WMH. In contrast, non-Latinx White participants evidenced relatively low WMH volume regardless of financial worry, while non-Latinx Black participants evidenced relatively high WMH volume even at the lowest level of financial worry, although these associations were not reliably different. Education and income were not associated with WMH. Results from multiple group models testing demonstrated that this association was not reliably different in the three groups.
Figure 2. Racial and ethnic group differences in the association between financial worry and white matter hyperintensities.
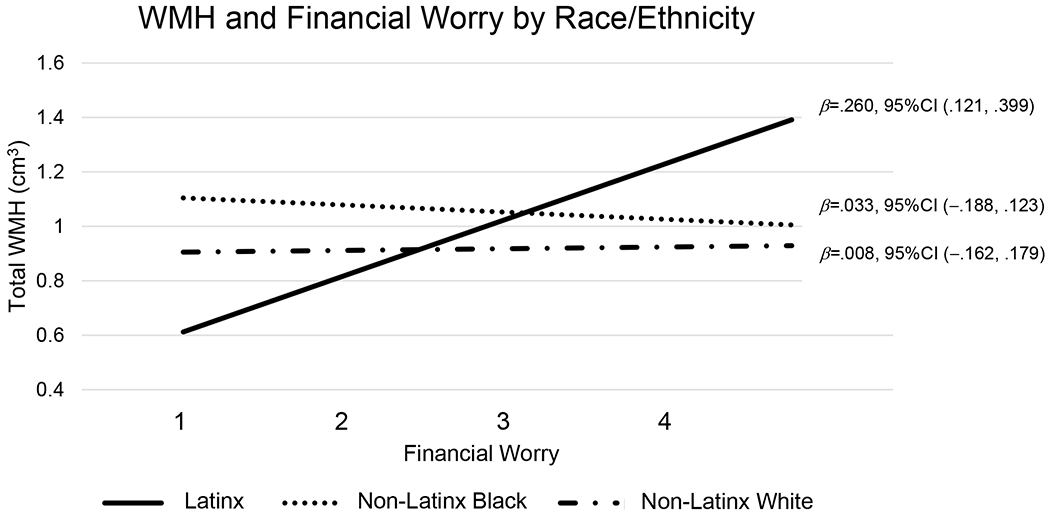
Note. WMH = white matter hyperintensities. Estimates controlled for covariates (i.e., age, sex/gender, education, income, depressive symptoms.
3.3. Sensitivity Analyses
Supplementary Table 1 demonstrates group differences in cardiovascular disease burden (i.e., total count of hypertension, diabetes, and/or heart disease), and Supplementary Table 4 demonstrates results from the primary model regressing WMH on financial worry with cardiovascular disease burden added as a covariate. Results revealed that Latinx and non-Latinx Black participants had a higher cardiovascular disease burden than non-Latinx Whites, but that cardiovascular disease burden was only significantly associated with WMH among Latinx participants. In the whole sample, the effect of financial worry on WMH remained the same as in the original results after adding cardiovascular disease burden as a covariate. In the Latinx group, the association between financial worry and WMH was attenuated by only 3% and remained significant after adding cardiovascular disease burden as a covariate (Supplementary Table 4).
A separate sensitivity analysis examined whether total intracranial volume altered associations between financial worry and WMH. Results from this sensitivity analysis were the same as the primary model, with the magnitude of associations between financial worry and WMH remaining the same across all groups and in the entire sample. Another separate sensitivity analysis was conducted examining whether time between MRI exam and psychosocial questionnaire administration changed associations between financial worry and WMH. Results from this sensitivity analysis were the same as the primary model, with the magnitude and significance of associations between financial worry and WMH remaining the same in the entire sample and in each racial/ethnic group.
4. Discussion
This cross-sectional study in a sample of racially and ethnically diverse older adults provides evidence that greater financial worry is not only associated with greater WMH volume above and beyond education and income, but also a stronger correlate of WMH than traditional measures of SES. These findings extend prior research on subjective SES and cognition (Kim et al., 2021; Zahodne et al., 2018) and suggest that subjective SES may also be relevant to brain health (i.e., WMH volume). However, these findings were qualified by preliminary evidence of racial/ethnic differences in the link between financial worry and WMH. Specifically, this association was unique to Latinx participants, who also reported more financial worry than non-Latinx White and Black older participants. These results underscore the potential utility of measuring subjective SES for health disparities research. While inferential tests revealed no statistically reliable differences in the association between financial worry and WMH across racial/ethnic groups, recent epidemiological frameworks suggest that stratified models may be the most appropriate method of assessing racial/ethnic disparities, especially when there is a disparity in the exposure (i.e., financial worry; Ward et al., 2019).
The finding that financial worry was associated with WMH above and beyond objective indicators of SES is consistent with previous research on other health outcomes and suggests that financial worry may capture additional, unmeasured components of socioeconomic disadvantage (e.g., food deserts, medical debt, intergenerational poverty) that are important for health. These factors, which often go unmeasured in ADRD cohort studies, may influence health via multiple pathways, such as stress and resource access/acquisition. While prior research has established that typically measured indicators of SES, such as income and education, are associated with brain health (Waldstein et al., 2017), the role of more subjective measures of SES in contributing to brain health and aging is poorly understood. The results of the present study suggest that subjective measures of SES such as financial worry may add to our understanding of the magnitude of the impact of SES on brain health.
Financial worry may be particularly important to consider when studying the influence of SES on health in Latinx and non-Latinx Black older adults due to historical and current structural racism in various aspects of objective SES, such as homeownership, educational opportunities, and income inequality (Shavers, 2007). As a result, these groups may report more financial worry than non-Latinx Whites at the same educational and/or income levels. Furthermore, based on the diminishing returns and minority poverty hypotheses, SES may be differently associated with health outcomes across different races/ethnicities (Farmer and Ferraro, 2005; Shuey and Willson, 2008), which is particularly important to consider when examining documented brain health disparities in older adulthood (Brickman et al., 2008).
Thus, we tested whether associations between financial worry and WMH volume differed across race/ethnicity. The finding that greater financial worry was associated with disproportionately greater WMH volume among Latinx older adults is consistent with the minority poverty hypothesis, which states that health disparities are greatest at the lowest levels of SES because socioeconomic disadvantage can compound on other racially/ethnically-patterned experiences of marginalization to produce worse health outcomes among racial and ethnic minority groups with low SES (Farmer and Ferraro, 2005). Financial worry may reflect circumstances faced disproportionately by Latinx older adults even at the same level of education and income, such as food insecurity, which is associated with increased self-report of worry (McAuliffe et al., 2021). Further, chronic worry is associated with dysregulation of the biological stress response (i.e., cortisol reactivity) in response to other stressors (Lewis et al., 2017). Additional studies are needed to delineate the extent to which specific stressors disproportionally faced by to Latinx older adults (e.g., acculturative stress, documentation and/or immigration status; Muñoz et al., 2021; Valentín-Cortés et al., 2020) could interact with financial worry to predict brain health.
Latinx older adults reported more financial worry than non-Latinx White and Black older adults, which may reflect contextual factors unique to Latinx older adults. For example, Latinx individuals in the US are more likely to have larger families than non-Latinx White and Black individuals (Cohn and Passel, 2018; Landale et al., 2006), and Latinx immigrants frequently provide financial support to family members living in their home countries (López-Anuarbe et al., 2015), which has been linked to the cultural value of familismo (Calzada et al., 2012). Moreover, Latinx older adults who immigrated to the US may not experience the same benefits as individuals who were born in the US, such as reliance on large family networks, generational wealth and resources, and governmental support (Thompson and Suarez, 2019). These cultural differences may help to explain why associations were detected among Latinx participants, but not among non-Latinx Black participants, who showed the highest levels of WMH. Greater WMH burden among non-Latinx Black older adults is in line with prior findings from the same cohort (Brickman et al., 2012, 2008) and may be due other social determinants of health, such as discriminatory stress (Clark et al., 1999).
We also documented racial/ethnic disparities in cardiovascular disease burden and found that including this covariate only slightly reduced the association between financial worry and WMH in Latinx participants, pointing to other potential mediators. Indeed, the magnitude of the association of financial worry with WMH was approximately twice that of cardiovascular disease burden with WMH in this group. These results suggest that financial worry is a salient, meaningful construct that is associated with worse brain health, above and beyond racial/ethnic disparities in cardiovascular disease.
Strengths of this study include a well-characterized, diverse, community-based sample and examination of both objective and subjective measures of SES. This study extends extant research on subjective measures of SES in relation to health by examining brain health and including three racial/ethnic groups. While the community-based nature of the study is a strength, this also limits the generalizability of the group-specific findings to primarily Caribbean Latinx older adults residing in northern Manhattan, which may not accurately represent Latinx older adults with other origins (Garcia et al., 2020; González et al., 2019). An additional limitation of this study is the cross-sectional nature of the analyses. The time period between brain MRI and administration of the psychosocial questionnaires (and subsequent measure of financial worry) is also a limitation, as prior research suggests that financial strain may decline with time (Francoeur, 2002). Little is known whether the chronicity or timing of financial worry moderates its effects on brain health; thus, results cannot necessarily be generalized to financial worry occurring at a specific time as a predictor of WMH. Additionally, the causes of financial worry may be important to consider when conducting future research examining SES-WMH associations. Future research should examine longitudinal associations between financial worry and WMH volume, as well as associations between financial worry and cognition, and examine how financial worry may be associated with generalized anxiety and chronic stress.
In conclusion, results from this cross-sectional study point to the importance of examining more subjective, aggregate indicators of SES that may better capture the impact of SES on brain health than typical, single indicators such as income and education. Intervening on financial worry via programs such as universal basic income, as well as providing need-based support to families who meet specific SES criteria, may be one way to address health inequities in ADRD; however, more research is needed regarding potential interventions. Measuring more than just education and income may be particularly important racially/ethnically marginalized individuals in the US, who face additional financial and psychosocial barriers and whose unique contexts may influence and interact with SES. Better understanding the association between various aspects of SES and brain health over time may help inform targeted, systemic interventions for groups that are particularly at risk for both financial strain and age-related cognitive morbidity, which may help alleviate racial and ethnic disparities in older age.
Supplementary Material
Highlights.
Financial worry is a separate construct from education and income
More financial worry was associated with greater white matter hyperintensity burden
This was only true for Latinx participants, not Black or White participants
Findings support inclusion of subjective socioeconomic measures in aging research
Societal interventions aimed at financial support may alleviate disparities in aging
Acknowledgements
Data collection and sharing for this project was supported by the Washington Heights-Inwood Columbia Aging Project (WHICAP, P01AG07232, R01AG037212, and RF1AG054023) funded by the National Institute on Aging (NIA) and through NIA grant numbers R00AG047963, R01AG054520, and R01AG034189. The corresponding author was supported by NIA F31AG077758. This manuscript has been reviewed by WHICAP investigators for scientific content and consistency of data interpretation with previous WHICAP study publications. We acknowledge the WHICAP study participants and the WHICAP research and support staff for their contributions to this study. This work was also supported by the National Institute on Aging (R01AG082307, P30AG059300, K01AG073588); National Center for Advancing Translational Sciences (KL2TR002241, UL1TR002240); and the Antonia Lemstra Fund at the Michigan Alzheimer’s Disease Center. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Michigan Alzheimer’s Disease Center. The authors report no conflicts of interest.
References
- Adler NE, Bush NR, Pantell MS, 2012. Rigor, vigor, and the study of health disparities. Proc. Natl. Acad. Sci 109, 17154–17159. 10.1073/pnas.1121399109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adler NE, Epel ES, Castellazzo G, Ickovics JR, 2000. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy white women. Heal. Psychol 10.1037/0278-6133.19.6.586 [DOI] [PubMed] [Google Scholar]
- Adler NE, Newman K, 2002. Socioeconomic disparities in health: Pathways and policies. Health Aff. 10.1377/hlthaff.21.2.60 [DOI] [PubMed] [Google Scholar]
- Aponte R, 1991. Urban Hispanic poverty: Disaggregations and explanations. Soc. Probl 38, 516–528. [Google Scholar]
- Arora R, 2005. Minorities Still Struggle to Meet Basic Needs [WWW Document]. Gallup. URL https://news.gallup.com/poll/17497/minorities-still-struggle-meet-basic-needs.aspx (accessed 2.9.21). [Google Scholar]
- Assari S, Bazargan M, 2020. Educational Attainment and Tobacco Harm Knowledge Among American Adults: Diminished Returns of African Americans and Hispanics. Int. J. Epidemiol. Res 7, 6–11. 10.34172/ijer.2020.02 [DOI] [PubMed] [Google Scholar]
- Beydoun MA, Beydoun HA, Gamaldo AA, Teel A, Zonderman AB, Wang Y, 2014. Epidemiologic studies of modifiable factors associated with cognition and dementia: Systematic review and meta-analysis. BMC Public Health. 10.1186/1471-2458-14-643 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brickman AM, Muraskin J, Zimmerman ME, 2009. Structural neuroimaging in Altheimer’s disease: do white matter hyperintensities matter? Dialogues Clin. Neurosci 11, 181–190. 10.31887/DCNS.2009.11.2/ambrickman [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brickman AM, Provenzano FA, Muraskin J, Manly JJ, Blum S, Apa Z, Stern Y, Brown TR, Luchsinger JA, Mayeux R, 2012. Regional White Matter Hyperintensity Volume, Not Hippocampal Atrophy, Predicts Incident Alzheimer Disease in the Community. Arch. Neurol 69, 1621. 10.1001/archneurol.2012.1527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brickman AM, Schupf N, Manly JJ, Luchsinger JA, Andrews H, Tang MX, Reitz C, Small SA, Mayeux R, Decarli C, Brown TR, 2008. Brain morphology in older African Americans, caribbean hispanics, and whites from northern Manhattan. Arch. Neurol 65, 1053–1061. 10.1001/archneur.65.8.1053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brickman AM, Sneed JR, Provenzano FA, Garcon E, Johnert L, Muraskin J, Yeung L-K, Zimmerman ME, Roose SP, 2011. Quantitative approaches for assessment of white matter hyperintensities in elderly populations. Psychiatry Res. Neuroimaging 193, 101–106. 10.1016/j.pscychresns.2011.03.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brickman AM, Zahodne LB, Guzman VA, Narkhede A, Meier IB, Griffith EY, Provenzano FA, Schupf N, Manly JJ, Stern Y, Luchsinger JA, Mayeux R, 2015. Reconsidering harbingers of dementia: progression of parietal lobe white matter hyperintensities predicts Alzheimer’s disease incidence. Neurobiol. Aging 36, 27–32. 10.1016/j.neurobiolaging.2014.07.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calzada EJ, Tamis-LeMonda CS, Yoshikawa H, 2012. Familismo in Mexican and Dominican Families From Low-Income,Urban Communities: 10.1177/0192513X12460218 34, 1696–1724. 10.1177/0192513X12460218 [DOI] [Google Scholar]
- Clark R, Anderson NB, Clark VR, Williams DR, 1999. Racism as a Stressor for African Americans: A Biopsychosocial Model. Am. Psychol 10.1037/0003-066X.54.10.805 [DOI] [PubMed] [Google Scholar]
- Cohn D, Passel JS, 2018. Record 64 million Americans live in multigenerational households | Pew Research Center; [WWW Document]. Pew Res. Cent. URL https://www.pewresearch.org/fact-tank/2018/04/05/a-record-64-million-americans-live-in-multigenerational-households/ (accessed 2.24.21). [Google Scholar]
- Erten-Lyons D, Woltjer R, Kaye J, Mattek N, Dodge HH, Green S, Tran H, Howieson DB, Wild K, Silbert LC, 2013. Neuropathologic basis of white matter hyperintensity accumulation with advanced age. Neurology 81, 977–983. 10.1212/WNL.0b013e3182a43e45 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farmer MM, Ferraro KF, 2005. Are racial disparities in health conditional on socioeconomic status? Soc. Sci. Med 60, 191–204. 10.1016/j.socscimed.2004.04.026 [DOI] [PubMed] [Google Scholar]
- Francoeur RB, 2002. Use of an Income-Equivalence Scale to Understand Age-Related Changes in Financial Strain. Res. Aging 24, 445–472. 10.1177/01627502024004003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garcia MA, Reyes AM, García C, Chiu CT, Macias G, 2020. Nativity and Country of Origin Variations in Life Expectancy With Functional Limitations Among Older Hispanics in the United States. Res. Aging 42, 199–207. 10.1177/0164027520914512 [DOI] [PubMed] [Google Scholar]
- Gianaros PJ, Marsland AL, Sheu LK, Erickson KI, Verstynen TD, 2013. Inflammatory Pathways Link Socioeconomic Inequalities to White Matter Architecture. Cereb. Cortex 23, 2058–2071. 10.1093/cercor/bhs191 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gianaros PJ, Kuan DCH, Marsland AL, Sheu LK, Hackman DA, Miller KG, & Manuck SB (2017). Community socioeconomic disadvantage in midlife relates to cortical morphology via neuroendocrine and cardiometabolic pathways. Cerebral cortex, 27(1), 460–473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- González HM, Tarraf W, Fornage M, González KA, Chai A, Youngblood M, Abreu M. de los A., Zeng D, Thomas S, Talavera GA, Gallo LC, Kaplan R, Daviglus ML, Schneiderman N, 2019. A research framework for cognitive aging and Alzheimer’s disease among diverse US Latinos: Design and implementation of the Hispanic Community Health Study/Study of Latinos—Investigation of Neurocognitive Aging (SOL-INCA). Alzheimer’s Dement. 10.1016/j.jalz.2019.08.192 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goodman E, Adler NE, Daniels SR, Morrison JA, Slap GB, Dolan LM, 2003. Impact of Objective and Subjective Social Status on Obesity in a Biracial Cohort of Adolescents. Obes. Res 11, 1018–1026. 10.1038/oby.2003.140 [DOI] [PubMed] [Google Scholar]
- Hu P, Adler NE, Goldman N, Weinstein M, Seeman TE, 2005. Relationship Between Subjective Social Status and Measures of Health in Older Taiwanese Persons. J. Am. Geriatr. Soc 53, 483–488. 10.1111/j.1532-5415.2005.53169.x [DOI] [PubMed] [Google Scholar]
- Igwe KC, Lao PJ, Vorburger RS, Banerjee A, Rivera A, Chesebro A, Laing K, Manly JJ, Brickman AM, 2022. Automatic quantification of white matter hyperintensities on T2-weighted fluid attenuated inversion recovery magnetic resonance imaging. Magn Reson Imaging. 85, 71–79. 10.1016/j.mri.2021.10.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Javed Z, Haisum Maqsood M, Yahya T, Amin Z, Acquah I, Valero-Elizondo J, Andrieni J, Dubey P, Jackson RK, Daffin MA, Cainzos-Achirica M, Hyder AA, Nasir K, 2022. Race, Racism, and Cardiovascular Health: Applying a Social Determinants of Health Framework to Racial/Ethnic Disparities in Cardiovascular Disease. Circ. Cardiovasc. Qual. Outcomes 15, e007917. 10.1161/CIRCOUTCOMES.121.007917 [DOI] [PubMed] [Google Scholar]
- Kim JH, Sumerlin TS, Goggins WB, Kwong EMS, Leung J, Yu B, Kwok TCY, 2021. Does Low Subjective Social Status Predict Cognitive Decline in Chinese Older Adults? A 4-Year Longitudinal Study From Hong Kong. Am. J. Geriatr. Psychiatry 10.1016/j.jagp.2021.01.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landale NS, Oropesa RS, Bradatan C, 2006. Hispanics and the Future of America, Hispanics and the Future of America. National Academies Press, Washington, D.C. 10.17226/11539 [DOI] [Google Scholar]
- Launer LJ, 2004. Epidemiology of White Matter Lesions. Top. Magn. Reson. Imaging 15, 365–367. 10.1097/01.rmr.0000168216.98338.8d [DOI] [PubMed] [Google Scholar]
- Lewis EJ, Yoon KL, Joormann J, 2017. Emotion regulation and biological stress responding: associations with worry, rumination, and reappraisal. 10.1080/02699931.2017.1310088 32, 1487–1498. 10.1080/02699931.2017.1310088 [DOI] [PubMed] [Google Scholar]
- López-Anuarbe M, Cruz-Saco M, Park Y, 2015. More than Altruism: Cultural Norms and Remittances among Hispanics in the U.S. J. Int. Migr. Integr 17. [Google Scholar]
- Lopez-Neyman SM, Davis K, Zohoori N, Broughton KS, Moore CE, Miketinas D, 2022. Racial disparities and prevalence of cardiovascular disease risk factors, cardiometabolic risk factors, and cardiovascular health metrics among US adults: NHANES 2011–2018. Sci. Rep 12, 1–10. 10.1038/s41598-022-21878-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luchsinger JA, Mayeux R, 2004. Cardiovascular risk factors and Alzheimer’s disease. Curr. Atheroscler. Rep 6, 261–266. 10.1007/s11883-004-0056-z [DOI] [PubMed] [Google Scholar]
- Macleod J, Davey Smith G, Metcalfe C, Hart C, 2005. Is subjective social status a more important determinant of health than objective social status? Evidence from a prospective observational study of Scottish men. Soc. Sci. Med 61, 1916–1929. 10.1016/j.socscimed.2005.04.009 [DOI] [PubMed] [Google Scholar]
- Manly JJ, Bell-McGinty S, Tang M-X, Schupf N, Stern Y, Mayeux R, 2005. Implementing Diagnostic Criteria and Estimating Frequency of Mild Cognitive Impairment in an Urban Community. Arch. Neurol 62, 1739. 10.1001/archneur.62.11.1739 [DOI] [PubMed] [Google Scholar]
- Marden JR, Tchetgen Tchetgen EJ, Kawachi I, Glymour MM, 2017. Contribution of Socioeconomic Status at 3 Life-Course Periods to Late-Life Memory Function and Decline: Early and Late Predictors of Dementia Risk, in: American Journal of Epidemiology. 10.1093/aje/kwx155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McAuliffe C, Daly Z, Black J, Pumarino J, Gadermann A, Slemon A, Thomson KC, Richardson C, Jenkins EK, 2021. Examining the associations between food worry and mental health during the early months of the COVID-19 pandemic in Canada. Can. J. Public Heal 2021 1125 112, 843–852. 10.17269/S41997-021-00557-W [DOI] [PMC free article] [PubMed] [Google Scholar]
- McEwen BS, Gianaros PJ, 2010. Central role of the brain in stress and adaptation: Links to socioeconomic status, health, and disease. Ann. N. Y. Acad. Sci 1186, 190–222. 10.1111/j.1749-6632.2009.05331.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muñoz E, Gallo LC, Hua S, Sliwinski MJ, Kaplan R, Lipton RB, González HM, Penedo FJ, Tarraf W, Daviglus ML, Llabre MM, Isasi CR, 2021. Stress Is Associated with Neurocognitive Function in Hispanic/Latino Adults: Results from HCHS/SOL Socio-Cultural Ancillary Study. Journals Gerontol. - Ser. B Psychol. Sci. Soc. Sci 76, E122–E128. 10.1093/GERONB/GBZ144 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radloff LS, 1977. The CES-D Scale. Appl. Psychol. Meas 1, 385–401. 10.1177/014662167700100306 [DOI] [Google Scholar]
- Shaked D, Leibel DK, Katzel LI, Davatzikos C, Gullapalli RP, Seliger SL, Erus G, Evans MK, Zonderman AB, Waldstein SR, 2019a. Disparities in diffuse cortical white matter integrity between socioeconomic groups. Front. Hum. Neurosci 13, 198. 10.3389/fnhum.2019.00198 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaked D, Millman ZB, Beatty Moody DL, Rosenberger WF, Shao H, Katzel LI, Davatzikos C, Gullapalli RP, Seliger SL, Erus G, Evans MK, Zonderman AB, Waldstein SR, 2019b. Sociodemographic disparities in corticolimbic structures. PLoS One 14. 10.1371/journal.pone.0216338 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shavers VL, 2007. Measurement of Socioeconomic Status in Health Disparities Research. [PMC free article] [PubMed]
- Shuey KM, Willson AE, 2008. Cumulative Disadvantage and Black-White Disparities in Life-Course Health Trajectories. Res. Aging 30, 200–225. 10.1177/0164027507311151 [DOI] [Google Scholar]
- Singh-Manoux A, Adler NE, Marmot MG, 2003. Subjective social status: its determinants and its association with measures of ill-health in the Whitehall II study. Soc. Sci. Med 56, 1321–1333. 10.1016/S0277-9536(02)00131-4 [DOI] [PubMed] [Google Scholar]
- Smith SM, 2002. Fast robust automated brain extraction. Hum Brain Mapp. 17(3):143–155. doi: 10.1002/hbm.10062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tang M-X, Cross P, Andrews H, Jacobs DM, Small S, Bell K, Merchant C, Lantigua R, Costa R, Stern Y, Mayeux R, 2001. Incidence of AD in African-Americans, Caribbean Hispanics, and Caucasians in northern Manhattan. Neurology 56, 49–56. 10.1212/WNL.56.1.49 [DOI] [PubMed] [Google Scholar]
- Thompson JP, Suarez GA, 2019. Accounting for racial wealth disparities in the United States. Working Papers. [Google Scholar]
- Valentín-Cortés M, Benavides Q, Bryce R, Rabinowitz E, Rion R, Lopez WD, Fleming PJ, 2020. Application of the Minority Stress Theory: Understanding the Mental Health of Undocumented Latinx Immigrants. Am. J. Community Psychol 66, 325–336. 10.1002/AJCP.12455 [DOI] [PubMed] [Google Scholar]
- Waldstein SR, Dore GA, Davatzikos C, Katzel LI, Gullapalli R, Seliger SL, Kouo T, Rosenberger WF, Erus G, Evans MK, Zonderman AB, 2017. Differential associations of socioeconomic status with global brain volumes and white matter lesions in African American and white adults: The HANDLS SCAN study. Psychosom. Med 79, 327–335. 10.1097/PSY.0000000000000408 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ward JB, Gartner DR, Keyes KM, Fliss MD, McClure ES, Robinson WR, 2019. How do we assess a racial disparity in health? Distribution, interaction, and interpretation in epidemiological studies. Ann. Epidemiol 29, 1–7. 10.1016/j.annepidem.2018.09.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willie CV, 1989. The Caste and Class Controversy on Race and Poverty: Round Two of The Willie/Wilson Debate. General Hall, Inc., Dix Hills, NY. [Google Scholar]
- Zahodne L, Manly J, Narkhede A, Griffith E, DeCarli C, Schupf N, Mayeux R, Brickman A, 2015. Structural MRI Predictors of Late-Life Cognition Differ Across African Americans, Hispanics, and Whites. Curr. Alzheimer Res 12, 632–639. 10.2174/1567205012666150530203214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zahodne LB, Kraal AZ, Zaheed A, Sol K, 2018. Subjective Social Status Predicts Late-Life Memory Trajectories through Both Mental and Physical Health Pathways. Gerontology 64, 466–474. 10.1159/000487304 [DOI] [PubMed] [Google Scholar]
- Zahodne LB, Stern Y, Manly JJ, 2015. Differing effects of education on cognitive decline in diverse elders with low versus high educational attainment. Neuropsychology 29, 649–657. 10.1037/neu0000141 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.