

Abstract
Objective
Embolic protection devices are useful for preventing distal embolism during carotid artery stenting (CAS); however, complications have been reported. The successful removal of a filter fragment trapped at the distal edge of a carotid stent during the retrieval procedure is described.
Case Presentation
CAS was performed for internal carotid artery stenosis in a patient in his 70s, and the carotid stent was successfully placed. During the retrieval procedure, the tip of the filter was trapped at the distal edge of the stent and detached from the filter. Using a snare kit, the filter tip was successfully retrieved, and no postoperative neurological symptoms occurred.
Conclusion
The edge of a carotid stent can potentially trap devices. When trapping or fragmentation of a device is suspected, it is necessary to evaluate the situation and cause, and the device should be appropriately retrieved without using force.
Keywords: carotid artery stenting, embolic protection device, distal protection filter, closed-cell stent, complication
Introduction
Carotid artery stenting (CAS) is a widely recognized method for preventing ischemic stroke in patients with carotid artery stenosis.1–3) An important concern in CAS is the risk of perioperative complications; the reported rate of ischemic complications is slightly higher in CAS than in carotid endarterectomy.2,3) Various embolic protection devices (EPDs) have been used to prevent intraoperative distal embolism; these include filter protection devices, which are commonly used in routine clinical practice and effectively capture emboli.4,5) However, complications associated with EPDs have been reported,6–8) including carotid vasospasm, thrombosis, flow impairment, arterial dissection, and although rare, device entrapment.5–7,9–12) We report the successful retrieval of a protection filter fragment that was trapped at the distal end of a carotid stent.
Case Presentation
A patient in his 70s presented to our hospital with asymptomatic left internal carotid artery (ICA) stenosis that had progressed over the past 5 years. He had a history of diabetes mellitus, dyslipidemia, and chronic renal dysfunction. Carotid angiography showed 74% stenosis of the left ICA based on the criteria used in the North American Symptomatic Carotid Endarterectomy Trial (Fig. 1A–1C). Ultrasonography revealed a hypoechoic plaque in the left ICA with a peak systolic velocity of 91.8 cm/s (Fig. 1D and 1E).
Fig. 1. (A–C) Preoperative left common carotid angiography on anteroposterior (A) and lateral (B) views and 3D rotational DSA (C) show 74% stenosis based on the criteria used by the North American Symptomatic Carotid Endarterectomy Trial at the origin of the left ICA. (D and E) Preoperative ultrasonography reveals a hypoechoic plaque with no acoustic shadow in the left ICA. ICA: internal carotid artery.

Dual antiplatelet therapy (DAPT) with 100 mg acetylsalicylic acid and 75 mg clopidogrel was administered 2 weeks before CAS. CAS was performed under general anesthesia. An 8-Fr sheath introducer was inserted via the right femoral artery, and heparin was administered to prolong the activated clotting time to >275 s. An 8-Fr guiding catheter (Launcher; Medtronic, Minneapolis, MN, USA) was inserted into the left common carotid artery, and a filter (FilterWire EZ; Boston Scientific, Natick, MA, USA) was passed through the stenotic lesion and deployed in the distal ICA. Predilatation was performed using a 4.0 × 30 mm balloon catheter (Sterling; Boston Scientific), and a 10 × 31 mm stent (Carotid Wallstent; Boston Scientific) was placed to cover the stenotic lesion sufficiently. Postdilatation was performed using a 4.5 × 20 mm balloon catheter (Sterling; Boston Scientific). Following postdilatation, we navigated a retrieval catheter and inserted the filter into the catheter; to prevent squeezing out the debris in the filter, the filter was only partially inserted. We retrieved the filter while feeling some resistance at the distal end of the stent.
Subsequent carotid angiography and 3D rotational DSA revealed an enhancement defect at the distal end of the stent (Fig. 2A–2D). The filter had fragmented and differed from its original form (Fig. 3A and 3B). The filter tip appeared to be trapped at the distal end of the stent. Considering the risk of thrombus formation and distal migration, we decided that it must be retrieved.
Fig. 2. (A and B) Left common carotid angiography after carotid stent deployment on anteroposterior (A) and right oblique (B) views shows a partial imaging defect at the distal end of the carotid stent in the ICA (black arrows). (C and D) 3D rotational DSA on coronal (C) and axial (D) views identifies an imaging defect (white arrows) at the same site as in panels (A) and (B). ICA: internal carotid artery.
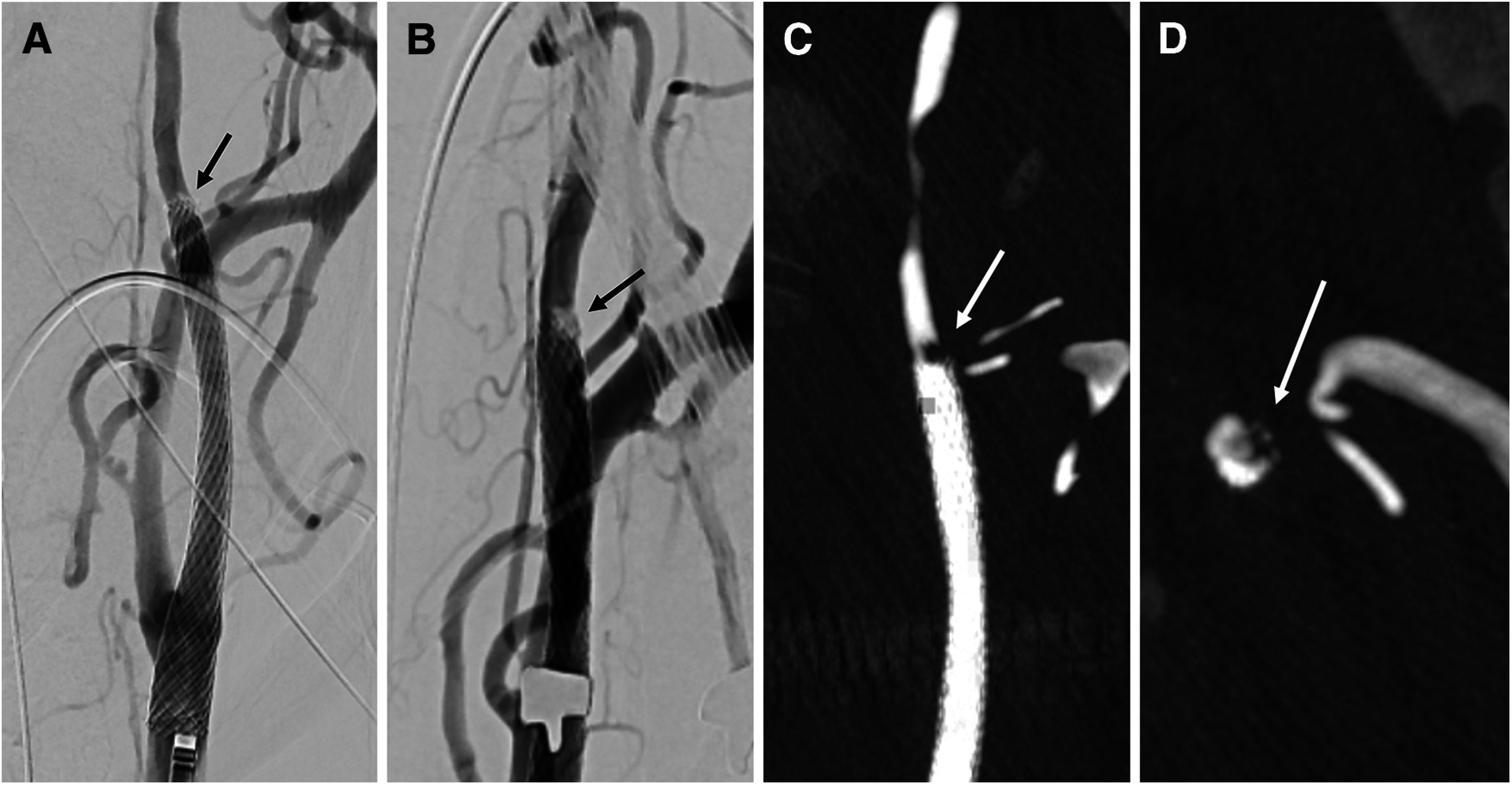
Fig. 3. (A) The fragmented filter (black arrow) and missing part of the original filter (dotted structure) are shown. (B) An unused FilterWire EZ is shown. (C) A goose neck snare (black arrow) is guided and opened at the distal end of the carotid stent to capture the filter fragment. (D) The filter fragment has been retrieved, and the imaging defect has disappeared (black arrow).
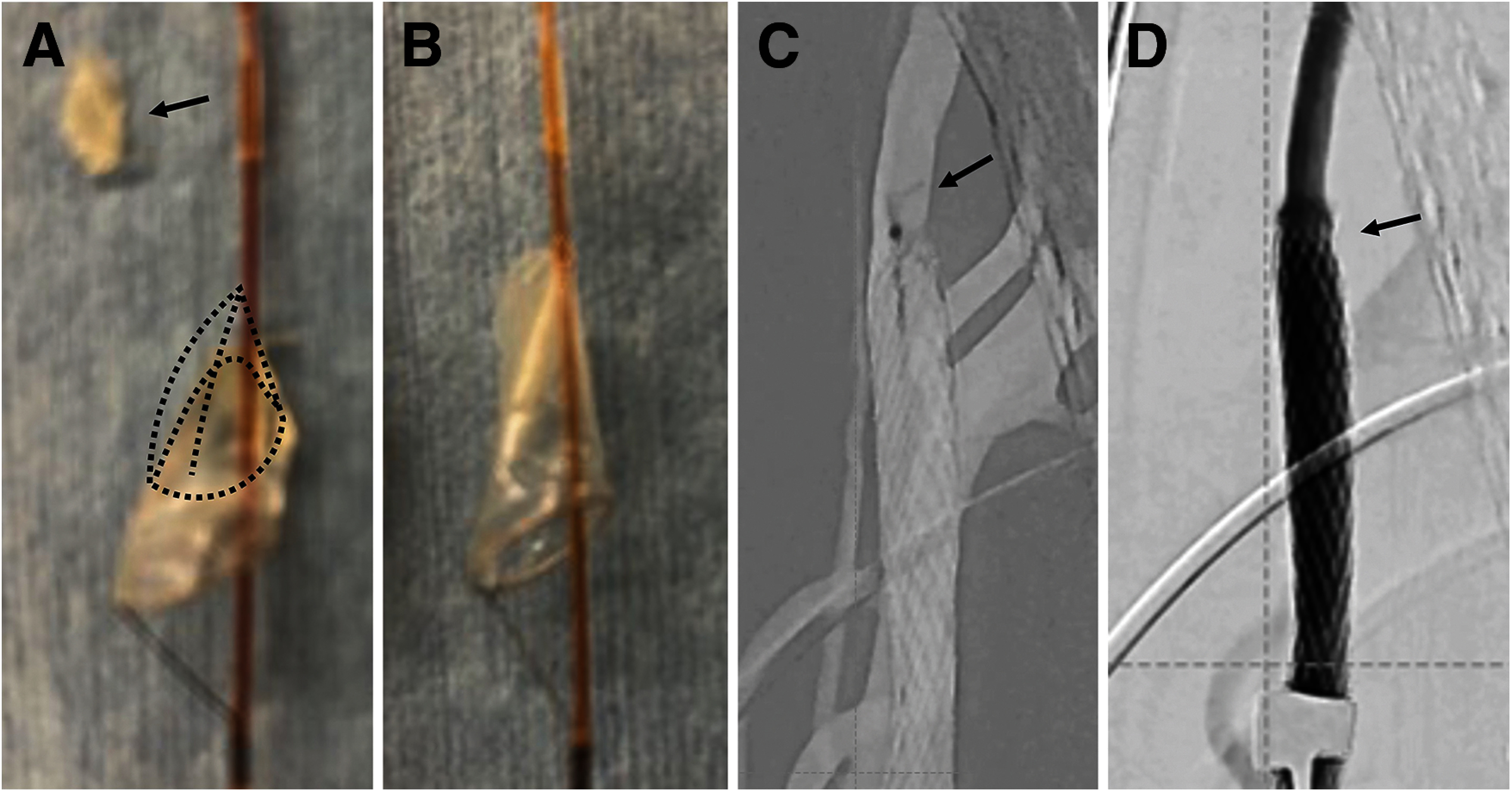
We exchanged the guiding catheter to the balloon-guiding catheter (8-Fr Optimo; Tokai Medical Products, Aichi, Japan) to prevent the filter tip from migrating distally. A microcatheter (Excelsior 1018; Stryker, Kalamazoo, MI, USA) and a 4-mm Amplatz Goose Neck Snare (Medtronic) were navigated, and the trapped filter tip was successfully captured and retrieved (Fig. 3C). Carotid angiography confirmed the disappearance of the contrast defect (Fig. 3D). After the procedure, the patient had no neurological deficits, and diffusion-weighted brain MRI on postoperative day 1 revealed no ischemic lesions. The patient was discharged home on postoperative day 5.
Discussion
In the present case, the tip of filter not fully contained within the retrieval catheter was captured and fragmented at the distal end of the carotid stent. This particular complication has not been previously reported in either closed-cell– or open-cell–type stents. We successfully retrieved the filter tip using an Amplatz Goose Neck Snare kit to avoid the risk of thrombus formation and distal migration of the tip.
Various EPDs have been used to prevent distal embolism during CAS; however, EPDs cause complications at a reported rate of 0.9%.6) Such complications include carotid vasospasm, thrombosis, flow impairment, vascular injury including dissection, and rarely, device entrapment.5,6)
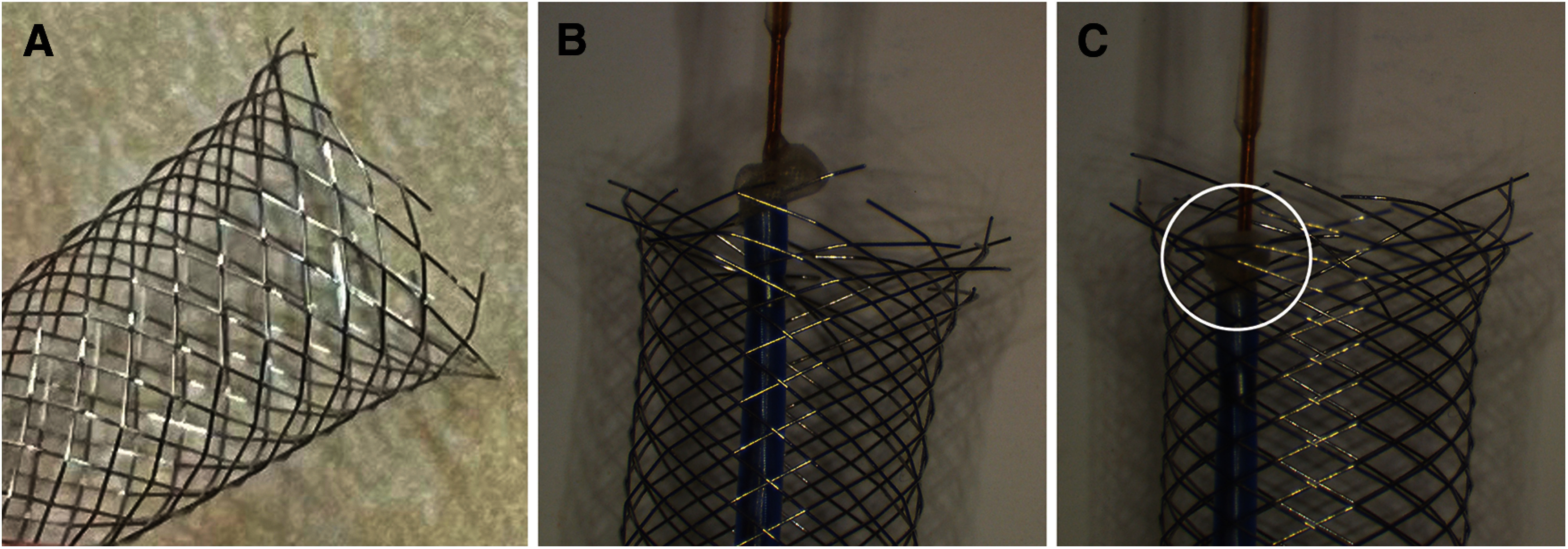
Since the Carotid Wallstent is a closed-cell–type stent, other devices are less likely to get caught in the middle portion of the stent and cause trouble. Previously, there have been reports of failures in which the tip of catheter caught on the proximal end of the stent when advancing to retrieve the EPD.9,13) Although the Carotid Wallstent is a closed-cell–type stent, metal wires protrude sharply at both ends (Fig. 4A), and this structure may be related to trapping the device. In addition, filters have a reticulate structure that becomes slightly dangled when inserted in the retrieval catheter, and thus may be easily ensnared by the sharp edge of the stent (Fig. 4B and 4C). In our case, the entrapment of the filter tip at the end of the stent may have resulted from the partial insertion of the filter into the retrieval catheter, which was done to prevent the debris in the filter from being squeezed out into the bloodstream. The use of excessive force to retrieve trapped filters is considered the main cause of filter fragmentation, and is usually ineffective and often dangerous and thus should be avoided.12) Advancing another catheter is an effective option when device trapping occurs.9) When a device is trapped at the distal end of a stent, another catheter with a larger diameter than the traditional 4-Fr retrieval catheter is included or a guiding catheter should be advanced and attempted to retrieve without pulling back the device. However, we must be aware of the risk of these catheters becoming trapped in the proximal end of the stent.
Fig. 4. (A) Although the Carotid Wallstent is a closed-cell–type stent, its end is slightly jagged. (B and C) Laboratory experiments. As the filter partially inserted into the retrieval catheter is pulled back, a barb on the distal end of the stent is caught and deflected inward (circle).
A device remaining in an artery poses a risk of ischemic complications due to thrombus formation and distal migration of the device. There have been several reports on device trapping and the treatment of complications. Endovascular techniques were used in some cases,9) whereas surgery was required in others.10–12) In the present case, we retrieved the filter tip using a snare kit. To avoid potential migration of the trapped filter tip during the retrieval procedure, we navigated a balloon guiding catheter and performed the procedure under proximal flow control. This salvage method was effective and feasible. Cone-beam CT provides useful information on the relationship between the captured device and the stent. If our retrieval attempt had failed, we may have considered placing an additional stent to immobilize the trapped filter tip to the arterial wall.11) However, although immobilization is an effective option,14) thrombus formation after immobilization has been reported despite administration of DAPT.11) On the other hand, device retrieval by a direct surgery has been reported that it can be performed safely despite the risk of DAPT and systemic heparinization.12) Thus, if the retrieval of the device by a snare kit is not possible, we consider that device retrieval by a direct surgery is preferable.
The filter tip in our case was composed of a highly radiolucent material and was first recognized as a contrast defect on imaging. However, we did not realize that the filter tip had come off until confirmatory angiography was performed. After stent deployment, carefully performing the procedure before the final imaging examination is important.
Conclusion
We report a case in which a filter fragment trapped at the distal end of a carotid stent was successfully retrieved during CAS. The sharp edge of the carotid stent can trap devices. When unusual behavior or resistance is noticed during the retrieval of a filter device, the cause should be determined and the use of excessive force avoided.
Disclosure Statement
Kazutaka Sumita received lecture fees from Stryker. The other authors declare that they have no conflicts of interest.
References
- 1).Massop D, Dave R, Metzger C, et al. Stenting and angioplasty with protection in patients at high-risk for endarterectomy: SAPPHIRE worldwide registry first 2,001 patients. Catheter Cardiovasc Interv 2009; 73: 129–136. [DOI] [PubMed] [Google Scholar]
- 2).Brott TG, Hobson RW II, Howard G, et al. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363: 11–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3).Rosenfield K, Matsumura JS, Chaturvedi S, et al. Randomized trial of stent versus surgery for asymptomatic carotid stenosis. N Engl J Med 2016; 374: 1011–1020. [DOI] [PubMed] [Google Scholar]
- 4).Angelini A, Reimers B, Della Barbera M, et al. Cerebral protection during carotid artery stenting: collection and histopathologic analysis of embolized debris. Stroke 2002; 33: 456–461. [DOI] [PubMed] [Google Scholar]
- 5).Vijayvergiya R, Otaal PS, Bagga S, et al. Symptomatic carotid vasospasm caused by a distal-protection device during stent angioplasty of the right internal carotid artery. Tex Heart Inst J 2010; 37: 226–229. [PMC free article] [PubMed] [Google Scholar]
- 6).Cremonesi A, Manetti R, Setacci F, et al. Protected carotid stenting: clinical advantages and complications of embolic protection devices in 442 consecutive patients. Stroke 2003; 34: 1936–1941. [DOI] [PubMed] [Google Scholar]
- 7).Hayashi K, Horie N, Morikawa M, et al. Pathophysiology of flow impairment during carotid artery stenting with an embolus protection filter. Acta Neurochir (Wien) 2014; 156: 1721–1728. [DOI] [PubMed] [Google Scholar]
- 8).Khalid N, Javed H, Rogers T, et al. Adverse events and modes of failure related to the FilterWire EZ Embolic Protection System: lessons learned from an analytic review of the FDA MAUDE database. Catheter Cardiovasc Interv 2019; 94: 157–164. [DOI] [PubMed] [Google Scholar]
- 9).Daugherty WP, White JB, Cloft HJ, et al. Rescue retrieval of AngioGuard embolic capture system after failure of capture sheath retrieval in carotid angioplasty and stenting. AJNR Am J Neuroradiol 2008; 29: 1594–1595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10).Shilling K, Uretsky BF, Hunter GC. Entrapment of a cerebral embolic protection device: a case report. Vasc Endovascular Surg 2006; 40: 229–233. [DOI] [PubMed] [Google Scholar]
- 11).Li T, Zha Y, Bo L, et al. Surgical management for retained distal embolic protection device and fractured guidewire after carotid artery stenting. J Surg Case Rep 2016; 2016: rjw105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12).Page P, Niemann D, Son C, et al. Retained distal protection device during carotid artery stenting necessitating carotid endarterectomy: a complication and management considerations. Surg Neurol Int 2018; 9: 123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13).Kuhn AL, Puri AS, de Macedo Rodrigues K, et al. Trapped embolic protection device: a salvage technique. Cureus 2020; 12: e9228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14).Schütz A, Solymosi L, Vince GH, et al. Proximal stent fixation of fractured coils: technical note. Neuroradiology 2005; 47: 874–878. [DOI] [PubMed] [Google Scholar]