

Abstract
Post‐intensive care syndrome comprises physical, cognitive, and mental impairments in patients treated in an intensive care unit (ICU). It occurs either during the ICU stay or following ICU discharge and is related to the patients' long‐term prognosis. The same concept also applies to pediatric patients, and it can greatly affect the mental status of family members. In the 10 years since post‐intensive care syndrome was first proposed, research has greatly expanded. Here, we summarize the recent evidence on post‐intensive care syndrome regarding its pathophysiology, epidemiology, assessment, risk factors, prevention, and treatments. We highlight new topics, future directions, and strategies to overcome post‐intensive care syndrome among people treated in an ICU. Clinical and basic research are still needed to elucidate the mechanistic insights and to discover therapeutic targets and new interventions for post‐intensive care syndrome.
Keywords: cognitive impairment, mental impairment, physical impairment, post‐intensive care syndrome
Post‐intensive care syndrome (PICS) includes physical, cognitive, and mental impairments that occur during ICU stay or following ICU discharge as well as the long‐term prognosis of ICU patients. This review summarizes the outline of PICS, including chronic pain, risk factors, and assessment, as well as recent evidence of the prevention and treatment of PICS. Furthermore, looking ahead to the next decade, this review highlights the potential of ICU telemedicine, support for the return to work, and community health care toward the social reintegration of patients with PICS.

BACKGROUND
Advances in acute medicine and critical care have dramatically improved short‐term mortality in critically ill patients. Innovations in intensive care units (ICUs), in therapeutic guidelines, and in education for medical staff, have contributed to saving patients who were critically ill in ICUs. 1 , 2 Short‐term outcomes have improved in the last two decades, particularly in cases of sepsis, 3 , 4 , 5 but the road to reintegration for people treated in an ICU is long, and after discharge the patients often carry a variety of burdens throughout their lives. 6 Moreover, as the world population ages in both economically advanced and developing countries, dramatic increases in such burdens are predicted in the coming decades; in some countries, the number of older adults already outweighs the number of children. 7 , 8 , 9 , 10 This worldwide expansion of the aging population is predicted to greatly increase the demand to assist critically ill patients and ICUs.
Post‐intensive care syndrome (PICS) consists of physical, cognitive, and mental impairments that occur during the ICU stay or following ICU or hospital discharge. It impacts upon the long‐term prognosis of patients in the ICU, and it can affect their families. Recently, research on this subject has steadily increased (Figure 1). Meanwhile, the coronavirus disease 2019 (COVID‐19) pandemic has caused several long‐term sequelae, so‐called “long‐COVID” or “post‐acute COVID‐19”, 11 and symptoms associated with PICS. 12 In this review article, we therefore summarize these recent advances and update information on chronic pain, PICS‐related disorders, and on recent advances regarding PICS prevention and treatments.
FIGURE 1.
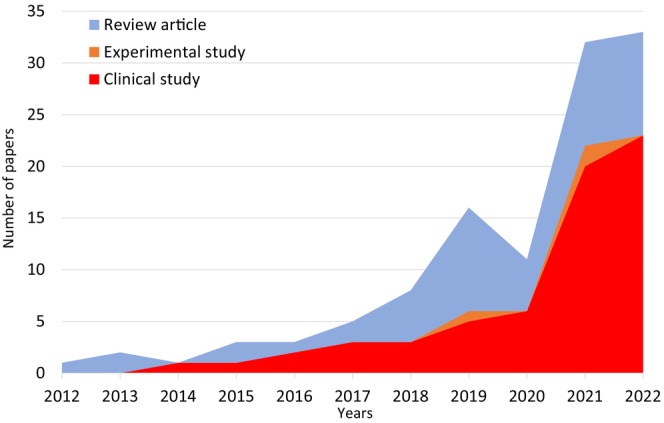
Number of published PICS‐related papers per year. (Post‐intensive care syndrome [Title]) OR (Post intensive care syndrome [Title]) was searched in PubMed (https://pubmed.ncbi.nlm.nih.gov/) on June 29th 6:00 am. Articles were divided into three groups: clinical study, experimental study, and review articles.
PICS DOMAINS
Physical impairment
Among the three domains of PICS (physical impairment, cognitive impairment, and affects upon mental health), physical impairment is the most common and can be severe, greatly affecting the quality of life (QOL) of critically ill patients. Within the domain of physical impairment, ICU‐acquired weakness (ICU‐AW) is a concept that encompasses critical illness‐related myopathy, polyneuropathy, polyneuromyopathy, and muscle deconditioning due to disuse atrophy. ICU‐AW impacts upon long‐term morbidity and mortality, 13 , 14 and ICU‐AW symptoms can persist for up to 10 years and frequently impair QOL. 15 Physical impairments and ICU‐AW were recently found to be closely related to muscle atrophy. 16 This muscle atrophy is caused by inflammation‐induced abnormal immunoreactions to human organs as a systemic inflammatory response syndrome. 17 Among the immune cells, macrophages and neutrophils are closely related to muscle atrophy; macrophages release pro‐inflammatory cytokines and destroy the muscle tissue. 18 Similarly, neutrophil infiltration in muscle tissue has been confirmed to cause muscle atrophy in sepsis, 19 so it is important to note the relationship between the immune reaction and muscle atrophy for future intervention.
Cognitive impairment
Cognitive impairments include impaired memory, executive function, language, attention, and visual–spatial abilities, and these are associated with poor functioning and reduced QOL. Possible risk factors for long‐term cognitive impairments have been reported as race, educational level, hospital type, delirium duration, in‐hospital acute stress symptoms, and acute respiratory distress syndrome (ARDS). 20 , 21 , 22 ARDS was associated with a highly observed decline of cognitive function of 87% at discharge, 36% at 6 months, and 30% (range 25%–45%) at 1 year. 22 Furthermore, a 2020 observational study using an unsupervised machine learning methodology reported three different types of cognitive phenotypes in patients with PICS. 23 First, patients with type 1 phenotype had fewer days of opioid administration than those with type 2 or 3 phenotypes, and lower accumulated doses of opioids than those with type 3 phenotypes. Second, patients with type 2 phenotype were mainly women, were older, and had more comorbidities and lower accumulated doses of sedative drugs than those with type 3 phenotype. The patients with type 3 phenotype showed the highest levels of cognitive impairment. It is unclear whether the phenotype of cognitive impairment is related to the outcome, treatment, or prevention, but this novel approach successfully classified the patterns of cognitive impairment in PICS. The phenotyping approach may aid in detection of the type of cognitive decline and could facilitate efficient and personalized treatment strategies.
Mental health problems in PICS
Recent data on mental health in PICS show that depression and anxiety primarily negatively affect food intake. 24 , 25 , 26 Even 12 months after intensive care, 25% of patients still have significant appetite loss, with severity of depression an independent factor contributing to this. 26 Fatigue is another topic relevant to mental health in PICS. 27 , 28 In the ALTOS study, 27 70% of ARDS survivors reported clinically significant fatigue at 6 months, and 27% reported co‐occurring anxiety, depression, and fatigue. Increased anxiety and depressive symptoms were associated with greater fatigue. Patients reporting appetite loss or fatigue after ICU discharge should therefore be screened for physical and psychological disturbances. A systematic review reported that post‐ICU follow‐up was associated with improved depressive symptoms, mental health‐related QOL, and PTSD symptoms. 29 However, post‐ICU follow‐up has no fixed structure and is difficult to evaluate. ICU diaries, in which ICU staff record the events of a patient's stay in an ICU, have been shown to reduce the incidence of mental health problems. 30 However, early rehabilitation did not significantly improve mental health‐related outcomes. 31
Chronic pain
Chronic pain is a major healthcare issue for people who have been treated in an ICU. 32 6 months following ICU discharge, pain and pain requiring treatment were reported in 44% and 32% of patients, respectively, 33 with the shoulders being most frequently affected. Elsewhere, pain and moderate‐to‐severe pain were reported in 77% and 31% of patients, respectively, 3 months after discharge from an ICU. 34 Disturbance in daily life because of pain was reported in 59% of the patients, and similar results were observed 12 months after discharge. Chronic pain unrelated to the ICU stay may develop in people who have been treated in an ICU. To address this issue, the concept of chronic intensive care‐related pain was proposed to distinguish between chronic ICU‐related and non‐ICU‐related pain, 35 and it was observed to exist in 33.2% of people treated in an ICU. ICU‐related pain was diagnosed if the patient considered that their pain originated from the ICU stay. The characteristics of chronic pain in people treated in an ICU were comprehensively summarized in a recent narrative review. 36 Chronic pain is also common among the patients with COVID‐19 that were treated in an ICU. 37 Approximately 50% of critical COVID‐19 patients reported pain, and 38.5% reported clinically relevant pain. Pain is common during an ICU stay, 38 and there is a substantial risk of ICU‐acquired pain becoming chronic (ICU‐acquired chronic pain). Chronic pain exacerbates physical, mental, and cognitive impairments and vice versa, 39 and PICS becomes more complicated and serious in the presence of chronic pain. Chronic pain has been considered to be an independent entity in people who have been treated in an ICU (Figure 2A); however, it is closely associated with inflammatory response 40 and may have a similar pathophysiology to the physical dysfunction of PICS. Considering chronic pain as one of the features of PICS may therefore be both reasonable and beneficial (Figure 2B).
FIGURE 2.
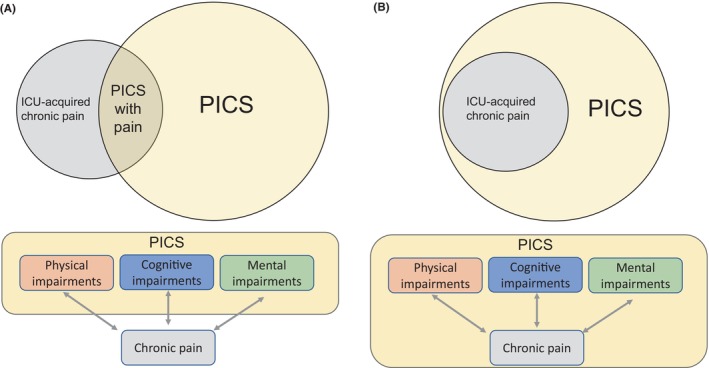
Relationship between PICS and ICU‐acquired chronic pain. (A) Current concept: ICU‐acquired chronic pain is independent of PICS although partly overlapping. (B) Authors' hypothesis: ICU‐acquired chronic pain is included in PICS and related to each PICS domain.
Post‐intensive care syndrome‐family
Family members of people treated in an ICU can have physical and psychological symptoms, including anxiety, depression, PTSD, and complicated grief. These symptoms have been termed “post‐intensive care syndrome‐family” (PICS‐F), and there is a prevalence rate of 20%–40%. 41 Family members with scores of ≥8 in the anxiety and depression components of the hospital anxiety and depression scale (HADS) have been considered to have anxiety and depression. 42 An average score of ≥1.6 in the impact of event scale‐revised (IES‐R) was said to indicate PTSD. 43 Risk factors for PICS‐F are lower educational level, poor communication between staff, being required to take crucial decisions, and having a loved one who either died or was critically ill. 44 , 45 To reduce the PICS‐F, clinicians should consider preventive measures, including liberalized family presence, 46 structured communication strategy, 47 family support, and communication by a trained nurse. 48 Impairments within families usually develop beyond the psychological, such as physical and socioeconomical impairments, thus affecting quality of life. 49 , 50 The concept of PICS‐F should be extended beyond psychological impairments of the families to also include consideration of physical and socioeconomical impairments.
Pediatric PICS (PICS‐p)
Although studies on pediatric PICS (PICS‐p) are limited, recent data has suggested that children who survive critical illness are at similar risk to adult patients. 51 A systematic review investigating the outcomes of children treated in a pediatric intensive care unit (PICU) reported that they can have physical, cognitive, and psychological dysfunctions following discharge from it. 52 In another report, PICU admission‐associated physical dysfunction was present at PICU discharge in 10%–36% of patients and persisted for over 2 years post‐discharge in 10%–13% of children treated in a PICU. 53 Elsewhere, among pediatric patients with severe sepsis, 50.5% reportedly had acquired new disability in overall function and 28% in cognitive function at PICU discharge. 54 In another report, both children and their parents had high rates of acute stress and post‐traumatic stress following PICU admission. 55 In 2018, the concept of PICS‐p was first categorized into four domains: physical, cognitive, emotional, and social health. 56 The aspects that are particularly relevant to the pediatric population include the presence of significant variations in their baseline health status and developmental stage, so there are therefore various recovery trajectories. Furthermore, recognizing the impact of critical illness on the social functioning of children and their families, social health was added as the fourth domain in PICS‐p, because pediatric patients and their families tend to be closely interrelated. Recent advances, including the development of clinical practice guidelines on the prevention and management of pain, agitation, neuromuscular blockade, and delirium in critically ill pediatric patients with consideration of the ICU environment and early mobility (PANDEM), are expected to contribute to the prevention of PICS‐p. 57
PICS‐RELATED DISORDERS
Persistent inflammation, immunosuppression, and catabolism syndrome
Sequelae of immune deficiency frequently occur after critical care, wherein several infectious complications easily occur as second hits; such an immune aspect of PICS is called persistent inflammation, immunosuppression, and catabolism syndrome (PIICS) (Figure 3). 58 , 59 Once PIICS occurs, the long‐term prognosis of mortality and physical impairment is likely to be poor. 59 , 60 The originally proposed clinical criteria for PIICS included C‐reactive protein (CRP) level, lymphocyte count, and serum albumin concentration. 12 Optimal cutoff values for the PIICS criteria were reported as CRP level of >2 mg/dL, albumin level of <3.0 g/dL, and lymphocyte count of <800/mm3 on Day 14 following critical care. 61 Based on these criteria, PIICS is expected to be recognized in clinical practice. Patients with PIICS have PICS‐related symptoms including impaired activities of daily living with a prolonged ICU stay. 62 , 63 When patients were evaluated in a PICS follow‐up clinic, physical PICS was confirmed more frequently in the patients with PIICS during the admission period. 64 The association between PIICS and PICS requires further clarification.
FIGURE 3.
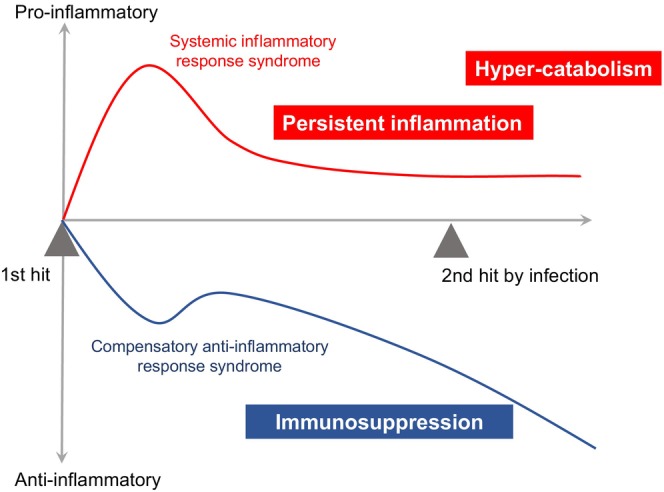
Concept of persistent inflammation, immunosuppression, and catabolism syndrome (PIICS). In ICU patients, the first hit (e.g., sepsis, trauma, and burn) causes persistent inflammation, immunosuppression, and hyper‐catabolism, thereby leading to the likelihood of a second hit caused by the infection.
Prevalence of PICS
The incidence rate of PICS has been reported to be 50%–70% at 6 months following ICU discharge. 12 , 65 Based on the combined data of our study and an integrated analysis of diagnostic procedure 5 , 66 in Japan, the annual number of patients with PICS following sepsis is thought to be approximately 420,000. Furthermore, PICS at 3 months was related to the significant increase in 2‐year mortality in patients with sepsis, addressing the profound impact of PICS on the long‐term mortality of patients in the ICU. 66
Risk factors for PICS
Risk factors for PICS are classified into patient backgrounds, severity of illness, medical care, and stress from the environment (Figure 4). A meta‐analysis reported that significant risk factors of PICS were female sex, comorbid psychiatric disorders, and negative ICU experiences. 67 Delirium was associated with mental impairment; older age, female sex, and higher severity were each significantly associated with physical impairment. To reduce the incidence of PICS, the actual content of medical care is important because immobilization, prolonged ventilator management, and prolonged stay in an ICU are the possible risk factors for PICS. 61 As for patient background, frailty is a recently proposed risk factor of PICS. 68 Oral frailty, insufficient oral intake, is also possible risk factor. 69 As environmental stress factors, extraordinary stimuli to the sensory organs, such as alarm sounds and light in the ICU, should be adjusted where possible to minimize the patients' stress.
FIGURE 4.
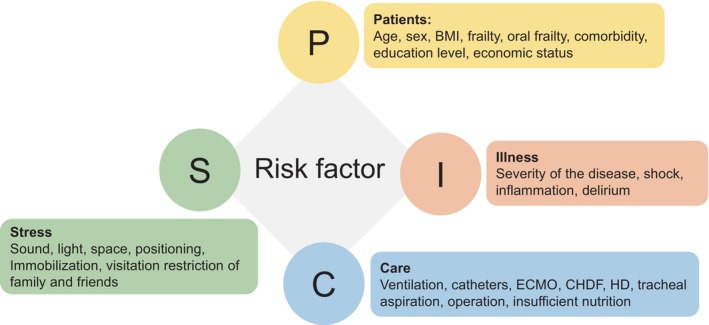
Risk factors for PICS. Letters (P, I, C, and S) include each component shown in the figure.
PICS assessment
In 2020, the Society of Critical Care Medicine summarized the PICS assessment tools. 43 A strong recommendation was Montreal cognitive assessment (MoCA) for cognition and HADS for anxiety and depression. A weak recommendation was IES‐R or IES‐6 for PTSD and a 6‐min walk test or physical components of EuroQol EQ‐5D‐5L for physical impairments. In 2023, the Japanese Society of Intensive Care Medicine recommended 6‐min walk test, medical research council (MRC) score, and grip strength for physical functions, MoCA, Mini‐Mental State Examination (MMSE), and short memory questionnaire (SMQ) for cognitive function, HADS, IES‐R, and patient health questionnaire‐9 (PHQ‐9) for mental health, Barthel Index, Instrumental Activities of Daily Living (IADL), and Functional Independence Measure (FIM) for the activities of daily living, and Short Form‐36 (SF‐36), SF‐12, EQ‐5D‐5L, 3L, and VAS for quality of life. 70 The PICS assessment tools are summarized in Table 1.
TABLE 1.
PICS assessment instruments.
| Category | Methods | Features |
|---|---|---|
| Physical | ||
| Muscle strength | MRC score | Manual muscle testing at 12 points |
| Handgrip strength | Objective evaluation by handgrip dynamometry | |
| Function | 6‐min walk test | Limited to ambulatory patients |
| ADL | Barthel index | ADL independence <85 |
| IADL | 8 items, 0–8 range | |
| FIM | 13 physical and 5 cognitive items | |
| Cognition | ||
| Cognition | MoCA | Mild 18–25, moderate 10–17, severe <10 |
| MMSE | Mild <24, moderate <20, severe <10 | |
| SMQ | Cutoff <40 in 4–46 range | |
| Mental health | ||
| Anxiety and depression | HADS | Cutoff ≥8 in 0–14 range |
| Depression | PHQ‐9 | Cutoff ≥10 in 0–27 range |
| PTSD | IES‐R | Cutoff > average 1.6 in 0–4 range |
| IES‐6 | Short version, cutoff > average 1.75 in 0–4 range | |
| QOL | ||
| QOL | EQ‐5D‐5L, 3L, VAS | 5 levels, 3 levels, or VAS, 0–1 range |
| SF‐36 | Cut off ≥10 score changes in 0–100 range | |
Abbreviations: ADL, activities of daily living; EQ‐5D‐5L, Euroqol‐5dimention‐5 level; FIM, functional independence measure; HADS, hospital anxiety and depression scale; IADL, instrumental ADL; IES‐R, impact of event scale‐revised; MMSE, mini‐mental state examination; MoCA, Montreal cognitive assessment; MRC score, medical research council score; PCL, PTSD check list for DSM‐5; PHQ, patient health questionnaire; SF‐36, short form‐36 items; SMQ, short memory questionnaire; VAS, visual analog scale.
PREVENTION AND TREATMENT
LIBERATION bundle (ABCDEF bundle)
The ABCDEF bundle is composed of six different elements of ICU care (Figure 5). This bundle is not just a collection of the six aspects of ICU care, but a bundled care plan that can show the maximum synergic effects when performed together. 71 The outcomes (e.g., weaning from mechanical ventilation, pain scale, delirium, physical restraint in place, etc.) reportedly improved as the adherence of the bundle increased. 72 Therefore, it is strongly recommended that all six elements should be incorporated into daily ICU care. However, there are several obstacles or barriers to simultaneously performing the bundle. 73 The implementation of the bundle, either as an entire bundle or an individual element, was extremely low, despite the current recommendations on the guidelines. 74 The best approach to introduce the bundle into the ICU should be determined according to the situation, system, and policy at the ICU. The key is thought to be not to introduce the six elements simultaneously, but to introduce them in a staged manner. A long‐term cohort study with a robust design of introducing the bundle care step by step showed the staged effects of the bundle care. Performance of the full bundle was associated with better outcomes and the partial introduction of the bundle were associated with better quality of ICU care. 75 As an example, element E (early mobility and exercise) may be a suitable starter for the bundle implementation. 76 In a recent study, the bundle compliance rate was not associated with PICS prevalence, although the 6‐month mortality was lower with a higher bundle compliance rate. 65 Studies with robust study design and statistical methods are warranted to investigate the effect of bundle care on the long‐term outcomes, such as prognosis, functional disabilities, and quality of care.
FIGURE 5.
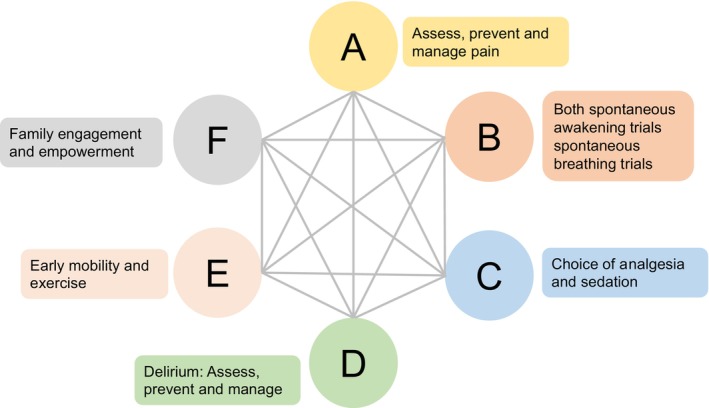
ABCDEF bundle for PICS prevention. The ABCDEF bundle includes A–F components shown in the figure.
Delirium management
Delirium is associated with increased mortality, length of ICU stay, and medical costs. 77 Delirium measurement is therefore a current and substantial issue in the ICU setting. The most prevalent assessment tools for screening for delirium in the ICU are the confusion assessment method for the ICU (CAM‐ICU) and the intensive care delirium screening checklist (ICDSC). 78 , 79 Both can assess delirium with a high accuracy in critically ill patients, but the CAM‐ICU tool may be superior in ruling out patients without delirium. 80 Regarding the prevention and/or treatment of delirium, several interventions are possible. As pharmacological agents, dexmedetomidine and non‐benzodiazepine sedative may be used to prevent delirium. As non‐pharmacological interventions, maintaining good sleep hygiene, early mobility, and family support may help improve delirium. 81 Adopting an unrestricted visiting policy for patients under ICU care may safely reduce the incidence rate of delirium without increasing the risks of infection from visitors. 82 Recently, real‐time monitoring of neuropsychologic condition by electroencephalography was newly tested for detecting early dementia. The real‐time monitoring technique can immediately provide information of waveforms or neuronal patterns associated with delirium. In the future, delirium may be dramatically reduced by the use of these new techniques as immediate interventions.
Early rehabilitation
Initiating rehabilitation for critically ill patients within 72 h may improve physical and cognitive function to prevent PICS, 83 but the optimal rehabilitation program in the ICU has not reached consensus. A recent randomized control trial clarified that an increase in active rehabilitation did not significantly increase the number of days the patients were alive and out of the hospital compared with the usual daily level of rehabilitation in the ICU among adults undergoing mechanical ventilation. 84 Rehabilitation was more effective in trials where the control group received a low‐dose physical rehabilitation (<5 days per week), 85 so there may be no add‐on benefit to active rehabilitation interventions above the usual daily rehabilitation. In patients with difficulty in usual early rehabilitation, neuromuscular electrical muscle stimulation (NMES) is a possible option to safely rehabilitate their limbs using weak electrical current. Although critically ill patients have 10%–20% of muscle atrophy in their limbs, 16 NMES can prevent muscle atrophy. 86 Furthermore, a recent meta‐analysis revealed that the use of NMES results in a decreased occurrence of ICU‐AW in patients with critical illness. 87 Only one study has investigated its effect on patient QOL; it was not different at hospital discharge. 88
Rehabilitation following discharge from ICU
Rehabilitation following ICU discharge has received much attention. 89 An expert consensus statement on physical rehabilitation after hospital discharge included an understanding of PICS and recovery. 90 However, the efficacy of home‐based rehabilitation on PICS remains unclear because there are fewer cases than those of early rehabilitation in the ICU. A recent pilot study clarified that home‐based rehabilitation for patients with PICS‐related symptoms was feasible and positively perceived by both patients and professionals. 91
Nutrition supports
Nutrition directly contributes to muscle volume maintenance and recovery, 92 which is linked to attenuating physical impairment. As “overfeeding” in the early period of the acute phase would be possibly harmful to the immune system 93 and muscles, 94 the “permissive underfeeding” strategy is occasionally chosen. Although the number of clinical studies investigating the effect of nutrition therapy on the improvement of physical function is increasing, 95 an appropriate nutrition intervention, wherein more energy or protein was provided, was not identified to decrease the PICS occurrence. 96 , 97 Theoretically, nutrition alone cannot directly contribute to physical functions and would instead have merely synergistic effects with exercise. Combining early mobilization and nutrition therapy has been reported to prevent muscle volume loss in patients at ICU. 98 At this time, adequate nutritional delivery as recommended by the current international guidelines for critical care nutrition should be considered as a reasonable strategy to minimize PICS. This includes energy equivalent to the 30 kcal/kg/day or full energy expenditure evaluated by indirect calorimetry, and protein of 1.3 g/kg/day or >1.2 g/kg/day, to be achieved from Days 3 to 7 of ICU admission, or at least after Day 7. 99 , 100
Nursing care
Nurses can play a central role in the long‐term outcomes of patients and their families. Relaxing of visiting restrictions is recommended because it is expected to reduce the incidence of patient delirium and to improve family satisfaction without increasing the risks of ICU‐acquired infections. 2 , 82 Nurses may improve the psychological outcomes for families by providing information during visits and by encouraging family participation in patient care. 101 Moreover, it is recommended that nurses discuss shared decision‐making with patients and their families regarding goals of care and treatment plans and offer educational advice. 1 To ensure patient safety, physical restraint is commonly practiced in the ICUs, but several adverse events have been reported. 102 Physical restraints should be minimized through the use of alternative methods, including adequate observation and communication, appropriate sedation management, non‐pharmacologic delirium care, and adjustments to the care environment. 103 , 104 Follow‐up and transitions of care are important to ensure the continuity of patient and family‐centered care. Recent studies suggest that nurses' interviews with patients' families and follow‐up after discharge from the ICU may improve the quality of life of patients and their families. 105 , 106 Critical care transition programs, in which ICU clinicians (including nurses) follow‐up patients on the wards after discharge from the ICU for a few days or until clinically stable, reduce the risk of in‐hospital mortality and could potentially reduce the risk of ICU readmission. 1 Establishing a system to continue the nursing care provided in the ICU after discharge from the ICU is important, although verification of its effectiveness is required.
ICU diaries
ICU diaries are typically written by medical staff or family members to document a patient's experiences during their stay in the ICU, and they may sometimes include photos. Reading an ICU diary after intensive care allows patients and their families to fill in memory gaps and to correct distorted memories and delusions. Using ICU diaries resulted in 26.3% lower PTSD scores in families of critically ill patients (95% confidence interval: 4.8% to 52.2%). 107 A recent systematic review of ICU diaries showed that ICU diaries reduce the risk of developing anxiety, depression, and PTSD in critically ill patients. 30 Rehabilitation guidelines for PICS prevention recommend the use of ICU diaries to reduce the risk of psychiatric symptoms in critically ill patients. 108
PICS round and follow‐up
The concept of PICS follow‐up is to provide a continuum of care from the ICU to the ward and discharge through multidisciplinary ward rounds and outpatient services. Critical care transition programs, including rapid response, medical emergency, and critical care outreach teams, and ICU nurse liaison programs, reduce the ICU re‐admissions and improve medication safety through medical reconciliation. 109 , 110 Outpatient clinics provide early detection and treatment of PICS; they aim to improve quality of life by providing information, understanding the context of life events, and providing appropriate social services, with the ICU serving as a safety net for patients. They also play a role in improving quality, educating, and motivating ICU staff, understanding the patient experience, improving morale, and preventing burnout. 111 , 112 In the United Kingdom, to provide appropriate rehabilitation or other specialist services, the national rehabilitation guidelines published in 2009 recommended a face‐to‐face review 2–3 months following ICU discharge. 113 The Society of Critical Care Medicine recommends an outpatient evaluation 2–4 weeks following discharge. 43 In the 2021 UK survey, inpatient recovery and follow‐up services were performed in 72.2% of facilities with nurse‐led multidisciplinary members, often with duration of ICU stay and duration of mechanical ventilation as eligibility criteria. Outpatient services were provided in 73.9% of facilities, mostly consisting of nurses, ICU physicians, and physical therapists. 114 A practical study of a well‐conducted, nurse‐led ICU follow‐up program failed to show an improvement in the patient QOL. 115 To date, there is insufficient evidence of ICU follow‐up services improving the PICS‐related outcomes. 116 However, the physical therapy‐focused models may improve the depressive symptoms and mental health‐related QOL in the short term, whereas psychological or medical management intervention‐focused models may improve the PTSD symptoms in the medium term. 29 The InS:PIRE project is an integrated health and social care intervention program of 5 weeks of rehabilitation and peer support, and improvements in anxiety and insomnia were demonstrated. 117 Tailored interventions will be needed in PICS outpatient clinics according to the pathophysiology. Another problem is that high‐risk patients with PICS do not visit the outpatient clinic as often as high‐risk patients with PICS, and the cancelation rate is as high as half of the patients. 118 It is a future challenge to accumulate evidence and make recommendations on who should be targeted, by whom, when, and what interventions should be performed.
FUTURE DIRECTIONS AND STRATEGIES OF PICS
ICU telemedicine
Telemedicine in ICU (tele‐ICU) could be used in institutions that have critical patients and insufficient intensivists. It enables patient care from off‐site locations 24 h a day and 7 days a week. 119 A component of tele‐ICU is the educational aspect for healthcare providers and standardization of care of critically ill patients, especially outside of office hours. These components enhance patient outcomes and provide education opportunities. 120 Future tele‐ICU systems with large data analysis and artificial intelligence algorithms could improve routine practice including PICS bundle and support the care of patients and their family members anywhere in the same ICU environment, thereby preventing PICS in critically ill patients.
Support for a return‐to‐work
Returning to work following ICU discharge is a serious issue. Two systematic reviews and meta‐analyses on returns‐to‐work among critically ill patients indicated that delayed return to work and unemployment were common and there were sustained problems following intensive care treatment. 121 , 122 A recent meta‐analysis reported that 36% of the patients who were employed became unemployed within 1 year following the ICU discharge. 121 Factors that may be associated with returning to work may include cognitive and physical dysfunction. 123 Furthermore, the return‐to‐work rates are related not only to the patient's physical performance but also to the national employment and disability policies. 124 A systematic review of studies on patients with musculoskeletal and pain‐related conditions and psychiatric disorders reported that workplace support was related to the return‐to‐work duration. 125 Workplace support includes health‐related support, return‐to‐work planning, case management, and job adjustments, including changes in working hours or duties. A multifaceted rather than one‐dimensional support is thought to be effective. 125 The government and employers must work to return people treated in an ICU to the workplace and to provide multifaceted support.
The strategy of PICS in older adults
In recent years, there has been an increase in the number of older patients managed in ICUs. Older adults are more susceptible to severe illness because of reduced physiological reserves and decreased immune function, 126 which are the risk factors for poor outcomes in the ICU. Older patients are at particularly high risk of developing ICU‐AW 127 and can benefit from the identification and optimization of modifiable factors related to their disability, such as optimizing nutritional status, early mobilization, and incorporating care bundles to reduce this risk. In the PICS bundle, early rehabilitation and nutrition support can prevent PICS, especially in older adults. The use of TPN during hospitalization is associated with increased mortality in elderly people compared with in younger patients, 128 so early oral or enteral nutrition is recommended for elderly patients treated in an ICU. The incidence of cognitive impairment is 1.6 times higher than normal. 128 Sleep plays an important role in recovery, as sleep disturbances have been shown to be associated with cognitive decline in older patients treated in an ICU. 129 Facilitating quality sleep is important for older patients treated in an ICU to prevent cognitive decline and delirium. The recovery of physical function in older adults takes a comparatively long time or is limited, 129 so it is essential to target improvement in residual and compensatory functions. 130 Additionally, early support for families or caregivers from the admission of the patient to the ICU is required when independence in daily living is expected to be challenging, and careful observation should continue after discharge.
Cooperation with the local medical community
Cooperation with local medical care providers, including primary care, 131 is important for patients in PICS and their families as they seek to reintegrate into society. We believe that PICS is one of the best places to follow‐up on PICS because it is the first point of contact for local residents and can provide patient‐centered and family‐oriented medical care. 132 In addition, medical support, such as PICS awareness‐raising activities, 133 are essential for collaboration with local medical services. Furthermore, the provision of livelihood and social support from the local government, such as the development of a service system required 134 after a PICS diagnosis, is also necessary. These types of support should be organically linked, and the use of a community‐based integrated care system 135 that provides comprehensive support to local residents should be specifically considered. This effort will require cooperation with the entire community, including local governments, local healthcare providers, businesses, non‐profit organizations, and residents. The Future Directions and Strategies for PICS section of this paper contains insights not discussed in the previous reviews of PICS care. While there is still much to be discussed about how to effectively collaborate with the local medical community, it is important to establish the community‐based integrated care system that includes PICS.
Future research focus
The number of studies on PICS has increased over the years, with 64 clinical studies published in 2022 alone (Figure 1). However, most are observational studies, and there is a lack of intervention studies. We summarized future research focus we mentioned in clinical section in Table 2, required to conduct intervention studies. As well as clinical intervention studies, basic molecular studies are essential to elucidate the pathophysiology and mechanisms of PICS. However, only a few basic studies have been conducted in laboratory animals. 19 , 136 , 137 , 138 In experimental models, mice that survived after sepsis presented with physical and mental impairments 138 and 1600 kDa‐hyaluronan improved grip strength after sepsis. 136 Sepsis has been demonstrated to cause neutrophil infiltration in the muscles leading to muscle atrophy and weakness in mice. 19 Additionally, infiltrated regulatory T and Th2 cells contribute to attenuate sepsis‐associated encephalopathy and alleviate the mental disorder by resolving the neuroinflammation in the chronic phase of sepsis. 137 Further clinical and basic research is needed to elucidate mechanistic insights and to discover therapeutic targets and new interventions for PICS.
TABLE 2.
Future research focus in PICS.
| Category | Future research focus |
|---|---|
| Physical impairments | Relationship between the immune reaction and muscle atrophy |
| PIICS | Association between PIICS and PICS requires further clarification |
| Bundle care | Effectiveness of bundle care on the long‐term outcomes |
| Delirium | Impact of real‐time monitoring of neuropsychologic condition by electroencephalography to detect delirium |
| Nursing care | Effectiveness of nursing care system after ICU discharge |
| Tele‐ICU | Effectiveness of tele‐ICU to provide PICS bundle and support the care of patients |
| Cooperation with local medical care | Impact of the community‐based integrated care system to prevent PICS |
Abbreviation: PIICS, persistent inflammation, immunosuppression, and catabolism syndrome.
CONCLUSIONS
PICS includes physical, cognitive, and mental impairments that occur during the ICU stay or following ICU discharge, affecting the long‐term prognosis of patients at ICU. This review summarized the recent evidence and potential strategies to overcome PICS among people treated in an ICU. It has been 10 years since PICS was first proposed, 139 and further clinical and basic research are needed to elucidate mechanistic insights and discover therapeutic targets and new interventions for PICS.
CONFLICT OF INTEREST STATEMENT
Dr. Yutaka Kondo is an Editorial Board member of AMS Journal and a co‐author of this article. To minimize bias, they were excluded from all editorial decision‐making related to the acceptance of this article for publication. The other authors declare no conflicts of interest in relation to this review article.
ACKNOWLEDGMENTS
We acknowledge proofreading and editing by Benjamin Phillis at the Clinical Study Support Center at Wakayama Medical University.
Inoue S, Nakanishi N, Amaya F, Fujinami Y, Hatakeyama J, Hifumi T, et al. Post‐intensive care syndrome: Recent advances and future directions. Acute Med Surg. 2024;11:e929. 10.1002/ams2.929
DATA AVAILABILITY STATEMENT
Data sharing not applicable—No new data generated.
REFERENCES
- 1. Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Egi M, Ogura H, Yatabe T, Atagi K, Inoue S, Iba T, et al. The Japanese clinical practice guidelines for management of sepsis and septic shock 2020 (J‐SSCG 2020). Acute Med Surg. 2021;8(1):e659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Kadri SS, Rhee C, Strich JR, Morales MK, Hohmann S, Menchaca J, et al. Estimating ten‐year trends in septic shock incidence and mortality in United States academic medical centers using clinical data. Chest. 2017;151(2):278–285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Rhee C, Dantes R, Epstein L, Murphy DJ, Seymour CW, Iwashyna TJ, et al. Incidence and trends of sepsis in US hospitals using clinical vs claims data, 2009–2014. JAMA. 2017;318(13):1241–1249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Imaeda T, Nakada TA, Takahashi N, Yamao Y, Nakagawa S, Ogura H, et al. Trends in the incidence and outcome of sepsis using data from a Japanese nationwide medical claims database‐the Japan Sepsis Alliance (JaSA) study group. Crit Care. 2021;25(1):338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Yende S, Austin S, Rhodes A, Finfer S, Opal S, Thompson T, et al. Long‐term quality of life among survivors of severe sepsis: analyses of two international trials. Crit Care Med. 2016;44(8):1461–1467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Lutz W, Sanderson W, Scherbov S. The coming acceleration of global population ageing. Nature. 2008;451(7179):716–719. [DOI] [PubMed] [Google Scholar]
- 8. Fuster V. Changing demographics: a new approach to global health care due to the aging population. J Am Coll Cardiol. 2017;69(24):3002–3005. [DOI] [PubMed] [Google Scholar]
- 9. Steeper M, Plebanski M, Flanagan KL. The global challenge and future strategies for keeping the world's aging population healthy by vaccination. Trans R Soc Trop Med Hyg. 2016;110(8):427–431. [DOI] [PubMed] [Google Scholar]
- 10. The Lancet . Ageing in China: a ticking bomb. Lancet. 2016;388(10056):2058. [DOI] [PubMed] [Google Scholar]
- 11. Yomogida K, Zhu S, Rubino F, Figueroa W, Balanji N, Holman E. Post‐acute sequelae of SARS‐CoV‐2 infection among adults aged ≥18 years—Long Beach, California, April 1–December 10, 2020. MMWR Morb Mortal Wkly Rep. 2021;70(37):1274–1277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Hatakeyama J, Inoue S, Liu K, Yamakawa K, Nishida T, Ohshimo S, et al. Prevalence and risk factor analysis of post‐intensive care syndrome in patients with COVID‐19 requiring mechanical ventilation: a multicenter prospective observational study. J Clin Med. 2022;11(19):5758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Van Aerde N, Meersseman P, Debaveye Y, Wilmer A, Gunst J, Casaer MP, et al. Five‐year impact of ICU‐acquired neuromuscular complications: a prospective, observational study. Intensive Care Med. 2020;46(6):1184–1193. [DOI] [PubMed] [Google Scholar]
- 14. Saccheri C, Morawiec E, Delemazure J, Mayaux J, Dubé BP, Similowski T, et al. ICU‐acquired weakness, diaphragm dysfunction and long‐term outcomes of critically ill patients. Ann Intensive Care. 2020;10(1):1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Meyer‐Frießem CH, Malewicz NM, Rath S, Ebel M, Kaisler M, Tegenthoff M, et al. Incidence, time course and influence on quality of life of intensive care unit‐acquired weakness symptoms in long‐term intensive care survivors. J Intensive Care Med. 2021;36(11):1313–1322. [DOI] [PubMed] [Google Scholar]
- 16. Nakanishi N, Oto J, Tsutsumi R, Akimoto Y, Nakano Y, Nishimura M. Upper limb muscle atrophy associated with in‐hospital mortality and physical function impairments in mechanically ventilated critically ill adults: a two‐center prospective observational study. J Intensive Care. 2020;8(1):87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Yao YM, Osuchowski MF, Wang JH, Pan ZK. Editorial: immune dysfunction: an update of new immune cell subsets and cytokines in sepsis. Front Immunol. 2021;12:822068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. VanderVeen BN, Murphy EA, Carson JA. The impact of immune cells on the skeletal muscle microenvironment during cancer cachexia. Front Physiol. 2020;11:1037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Nakanishi N, Ono Y, Miyazaki Y, Moriyama N, Fujioka K, Yamashita K, et al. Sepsis causes neutrophil infiltration in muscle leading to muscle atrophy and weakness in mice. Front Immunol. 2022;13:950646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Pandharipande PP, Girard TD, Jackson JC, Morandi A, Thompson JL, Pun BT, et al. Long‐term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306–1316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Haddad DN, Mart MF, Wang L, Lindsell CJ, Raman R, Nordness MF, et al. Socioeconomic factors and intensive care unit‐related cognitive impairment. Ann Surg. 2020;272(4):596–602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Huang M, Gedansky A, Hassett CE, Price C, Fan TH, Stephens RS, et al. Pathophysiology of brain injury and neurological outcome in acute respiratory distress syndrome: a scoping review of preclinical to clinical studies. Neurocrit Care. 2021;35(2):518–527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Fernández‐Gonzalo S, Navarra‐Ventura G, Bacardit N, Gomà Fernández G, de Haro C, Subirà C, et al. Cognitive phenotypes 1 month after ICU discharge in mechanically ventilated patients: a prospective observational cohort study. Crit Care. 2020;24(1):618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Merriweather JL, Salisbury LG, Walsh TS, Smith P. Nutritional care after critical illness: a qualitative study of patients' experiences. J Hum Nutr Diet. 2016;29(2):127–136. [DOI] [PubMed] [Google Scholar]
- 25. Moisey LL, Merriweather JL, Drover JW. The role of nutrition rehabilitation in the recovery of survivors of critical illness: underrecognized and underappreciated. Crit Care. 2022;26(1):270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Kitayama M, Unoki T, Sasaki A, Sakuramoto H, Uemura S, Tsujimoto T, et al. Appetite loss and associated factors at 1 year after intensive care unit elder survivors in a secondary analysis of the SMAP‐HoPe study. Sci Rep. 2023;13(1):1079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Neufeld KJ, Leoutsakos JS, Yan H, Lin S, Zabinski JS, Dinglas VD, et al. Fatigue symptoms during the first year following ARDS. Chest. 2020;158(3):999–1007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Geense WW, Zegers M, Peters MAA, Ewalds E, Simons KS, Vermeulen H, et al. New physical, mental, and cognitive problems 1 year after ICU admission: a prospective multicenter study. Am J Respir Crit Care Med. 2021;203(12):1512–1521. [DOI] [PubMed] [Google Scholar]
- 29. Rosa RG, Ferreira GE, Viola TW, Robinson CC, Kochhann R, Berto PP, et al. Effects of post‐ICU follow‐up on subject outcomes: a systematic review and meta‐analysis. J Crit Care. 2019;52:115–125. [DOI] [PubMed] [Google Scholar]
- 30. Sun X, Huang D, Zeng F, Ye Q, Xiao H, Lv D, et al. Effect of intensive care unit diary on incidence of posttraumatic stress disorder, anxiety, and depression of adult intensive care unit survivors: a systematic review and meta‐analysis. J Adv Nurs. 2021;77(7):2929–2941. [DOI] [PubMed] [Google Scholar]
- 31. Fuke R, Hifumi T, Kondo Y, Hatakeyama J, Takei T, Yamakawa K, et al. Early rehabilitation to prevent postintensive care syndrome in patients with critical illness: a systematic review and meta‐analysis. BMJ Open. 2018;8(5):e019998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Kaarlola A, Pettila V, Kekki P. Quality of life six years after intensive care. Intensive Care Med. 2003;29(8):1294–1299. [DOI] [PubMed] [Google Scholar]
- 33. Battle CE, Lovett S, Hutchings H. Chronic pain in survivors of critical illness: a retrospective analysis of incidence and risk factors. Crit Care. 2013;17(3):R101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Hayhurst CJ, Jackson JC, Archer KR, Thompson JL, Chandrasekhar R, Hughes CG. Pain and its long‐term interference of daily life after critical illness. Anesth Analg. 2018;127(3):690–697. [DOI] [PubMed] [Google Scholar]
- 35. Baumbach P, Götz T, Günther A, Weiss T, Meissner W. Prevalence and characteristics of chronic intensive care‐related pain: the role of severe sepsis and septic shock. Crit Care Med. 2016;44(6):1129–1137. [DOI] [PubMed] [Google Scholar]
- 36. Kemp HI, Laycock H, Costello A, Brett SJ. Chronic pain in critical care survivors: a narrative review. Br J Anaesth. 2019;123(2):e372–e384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Ojeda A, Calvo A, Cuñat T, Mellado‐Artigas R, Comino‐Trinidad O, Aliaga J, et al. Characteristics and influence on quality of life of new‐onset pain in critical COVID‐19 survivors. Eur J Pain. 2022;26(3):680–694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Chanques G, Sebbane M, Barbotte E, Viel E, Eledjam JJ, Jaber S. A prospective study of pain at rest: incidence and characteristics of an unrecognized symptom in surgical and trauma versus medical intensive care unit patients. Anesthesiology. 2007;107(5):858–860. [DOI] [PubMed] [Google Scholar]
- 39. Dansie EJ, Turk DC. Assessment of patients with chronic pain. Br J Anaesth. 2013;111(1):19–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Matsuda M, Huh Y, Ji RR. Roles of inflammation, neurogenic inflammation, and neuroinflammation in pain. J Anesth. 2019;33(1):131–139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Jones C, Skirrow P, Griffiths RD, Humphris G, Ingleby S, Eddleston J, et al. Post‐traumatic stress disorder‐related symptoms in relatives of patients following intensive care. Intensive Care Med. 2004;30(3):456–460. [DOI] [PubMed] [Google Scholar]
- 42. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. [DOI] [PubMed] [Google Scholar]
- 43. Mikkelsen ME, Still M, Anderson BJ, Bienvenu OJ, Brodsky MB, Brummel N, et al. Society of Critical Care Medicine's international consensus conference on prediction and identification of long‐term impairments after critical illness. Crit Care Med. 2020;48(11):1670–1679. [DOI] [PubMed] [Google Scholar]
- 44. Gries CJ, Engelberg RA, Kross EK, Zatzick D, Nielsen EL, Downey L, et al. Predictors of symptoms of posttraumatic stress and depression in family members after patient death in the ICU. Chest. 2010;137(2):280–287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Azoulay E, Pochard F, Kentish‐Barnes N, Chevret S, Aboab J, Adrie C, et al. Risk of post‐traumatic stress symptoms in family members of intensive care unit patients. Am J Respir Crit Care Med. 2005;171(9):987–994. [DOI] [PubMed] [Google Scholar]
- 46. Rosa RG, Falavigna M, da Silva DB, Sganzerla D, Santos MMS, Kochhann R, et al. Effect of flexible family visitation on delirium among patients in the intensive care unit: the ICU visits randomized clinical trial. JAMA. 2019;322(3):216–228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Lautrette A, Darmon M, Megarbane B, Joly LM, Chevret S, Adrie C, et al. A communication strategy and brochure for relatives of patients dying in the ICU. N Engl J Med. 2007;356(5):469–478. [DOI] [PubMed] [Google Scholar]
- 48. White DB, Angus DC, Shields AM, Buddadhumaruk P, Pidro C, Paner C, et al. A randomized trial of a family‐support intervention in intensive care units. N Engl J Med. 2018;378(25):2365–2375. [DOI] [PubMed] [Google Scholar]
- 49. McPeake J, Auriemma CL, Harhay MO. Understanding the impact of critical illness on families: a call for standardization of outcomes and longitudinal research. Ann Am Thorac Soc. 2021;18(11):1783–1785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Cameron JI, Chu LM, Matte A, Tomlinson G, Chan L, Thomas C, et al. One‐year outcomes in caregivers of critically ill patients. N Engl J Med. 2016;374(19):1831–1841. [DOI] [PubMed] [Google Scholar]
- 51. Pinto NP, Rhinesmith EW, Kim TY, Ladner PH, Pollack MM. Long‐term function after pediatric critical illness: results from the survivor outcomes study. Pediatr Crit Care Med. 2017;18(3):e122–e130. [DOI] [PubMed] [Google Scholar]
- 52. Herrup EA, Wieczorek B, Kudchadkar SR. Characteristics of postintensive care syndrome in survivors of pediatric critical illness: a systematic review. World J Crit Care Med. 2017;6(2):124–134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Ong C, Lee JH, Leow MK, Puthucheary ZA. Functional outcomes and physical impairments in pediatric critical care survivors: a scoping review. Pediatr Crit Care Med. 2016;17(5):e247–e259. [DOI] [PubMed] [Google Scholar]
- 54. Sankar J, Moodu S, Kumar K, Sankar MJ, Kabra SK, Lodha R. Functional outcomes at 1 year after PICU discharge in critically ill children with severe sepsis. Pediatr Crit Care Med. 2021;22(1):40–49. [DOI] [PubMed] [Google Scholar]
- 55. Nelson LP, Lachman SE, Li SW, Gold JI. The effects of family functioning on the development of posttraumatic stress in children and their parents following admission to the PICU. Pediatr Crit Care Med. 2019;20(4):e208–e215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Manning JC, Pinto NP, Rennick JE, Colville G, Curley MAQ. Conceptualizing post intensive care syndrome in children—the PICS‐p framework. Pediatr Crit Care Med. 2018;19(4):298–300. [DOI] [PubMed] [Google Scholar]
- 57. Smith HAB, Besunder JB, Betters KA, Johnson PN, Srinivasan V, Stormorken A, et al. 2022 Society of Critical Care Medicine clinical practice guidelines on prevention and management of pain, agitation, neuromuscular blockade, and delirium in critically ill pediatric patients with consideration of the ICU environment and early mobility. Pediatr Crit Care Med. 2022;23(2):e74–e110. [DOI] [PubMed] [Google Scholar]
- 58. Gentile LF, Cuenca AG, Efron PA, Ang D, Bihorac A, McKinley BA, et al. Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care. J Trauma Acute Care Surg. 2012;72(6):1491–1501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Mira JC, Gentile LF, Mathias BJ, Efron PA, Brakenridge SC, Mohr AM, et al. Sepsis pathophysiology, chronic critical illness, and persistent inflammation‐immunosuppression and catabolism syndrome. Crit Care Med. 2017;45(2):253–262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Nakamura K, Ogura K, Nakano H, Naraba H, Takahashi Y, Sonoo T, et al. Disseminated intravascular coagulopathy is associated with the outcome of persistent inflammation, immunosuppression and catabolism syndrome. J Clin Med. 2020;9(8):2662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Pandharipande P, Banerjee A, McGrane S, Ely EW. Liberation and animation for ventilated ICU patients: the ABCDE bundle for the back‐end of critical care. Crit Care. 2010;14(3):157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Nakamura K, Ogura K, Nakano H, Naraba H, Takahashi Y, Sonoo T, et al. C‐reactive protein clustering to clarify persistent inflammation, immunosuppression and catabolism syndrome. Intensive Care Med. 2020;46(3):437–443. [DOI] [PubMed] [Google Scholar]
- 63. Yang N, Li B, Ye B, Ke L, Chen F, Lu G, et al. The long‐term quality of life in patients with persistent inflammation‐immunosuppression and catabolism syndrome after severe acute pancreatitis: a retrospective cohort study. J Crit Care. 2017;42:101–106. [DOI] [PubMed] [Google Scholar]
- 64. Suganuma S, Idei M, Nakano H, Koyama Y, Hashimoto H, Yokoyama N, et al. Impact of persistent inflammation, immunosuppression, and catabolism syndrome during intensive care admission on each post‐intensive care syndrome component in a PICS clinic. J Clin Med. 2023;12(16):5427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Kawakami D, Fujitani S, Morimoto T, Dote H, Takita M, Takaba A, et al. Prevalence of post‐intensive care syndrome among Japanese intensive care unit patients: a prospective, multicenter, observational J‐PICS study. Crit Care. 2021;25(1):69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Inoue S, Nakanishi N, Sugiyama J, Moriyama N, Miyazaki Y, Sugimoto T, et al. Prevalence and long‐term prognosis of post‐intensive care syndrome after sepsis: a single‐center prospective observational study. J Clin Med. 2022;11(18):5257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Lee M, Kang J, Jeong YJ. Risk factors for post‐intensive care syndrome: a systematic review and meta‐analysis. Aust Crit Care. 2020;33(3):287–294. [DOI] [PubMed] [Google Scholar]
- 68. Muscedere J, Waters B, Varambally A, Bagshaw SM, Boyd JG, Maslove D, et al. The impact of frailty on intensive care unit outcomes: a systematic review and meta‐analysis. Intensive Care Med. 2017;43(8):1105–1122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Tanaka T, Takahashi K, Hirano H, Kikutani T, Watanabe Y, Ohara Y, et al. Oral frailty as a risk factor for physical frailty and mortality in community‐dwelling elderly. J Gerontol A Biol Sci Med Sci. 2018;73(12):1661–1667. [DOI] [PubMed] [Google Scholar]
- 70. Nakanishi N. Instruments to assess post‐intensive care syndrome assessment: a scoping review and modified Delphi method study. Crit Care. 2023;27:430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Ely EW. The ABCDEF bundle: science and philosophy of how ICU liberation serves patients and families. Crit Care Med. 2017;45(2):321–330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Pun BT, Balas MC, Barnes‐Daly MA, Thompson JL, Aldrich JM, Barr J, et al. Caring for critically ill patients with the ABCDEF bundle: results of the ICU liberation collaborative in over 15,000 adults. Crit Care Med. 2019;47(1):3–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Moraes FDS, Marengo LL, Moura MDG, Bergamaschi CC, de Sá Del Fiol F, Lopes LC, et al. ABCDE and ABCDEF care bundles: a systematic review of the implementation process in intensive care units. Medicine. 2022;101(25):e29499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Liu K, Nakamura K, Katsukawa H, Nydahl P, Ely EW, Kudchadkar SR, et al. Implementation of the ABCDEF bundle for critically ill ICU patients during the COVID‐19 pandemic: a multi‐national 1‐day point prevalence study. Front Med. 2021;8:735860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Hsieh SJ, Otusanya O, Gershengorn HB, Hope AA, Dayton C, Levi D, et al. Staged implementation of awakening and breathing, coordination, delirium monitoring and management, and early mobilization bundle improves patient outcomes and reduces hospital costs. Crit Care Med. 2019;47(7):885–893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. Liu K, Ogura T, Takahashi K, Nakamura M, Ohtake H, Fujiduka K, et al. A progressive early mobilization program is significantly associated with clinical and economic improvement: a single‐center quality comparison study. Crit Care Med. 2019;47(9):e744–e752. [DOI] [PubMed] [Google Scholar]
- 77. Stollings JL, Kotfis K, Chanques G, Pun BT, Pandharipande PP, Ely EW. Delirium in critical illness: clinical manifestations, outcomes, and management. Intensive Care Med. 2021;47(10):1089–1103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Ely EW, Inouye SK, Bernard GR, Gordon S, Francis J, May L, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM‐ICU). JAMA. 2001;286(21):2703–2710. [DOI] [PubMed] [Google Scholar]
- 79. Bergeron N, Dubois MJ, Dumont M, Dial S, Skrobik Y. Intensive care delirium screening checklist: evaluation of a new screening tool. Intensive Care Med. 2001;27(5):859–864. [DOI] [PubMed] [Google Scholar]
- 80. Chen TJ, Chung YW, Chang HR, Chen PY, Wu CR, Hsieh SH, et al. Diagnostic accuracy of the CAM‐ICU and ICDSC in detecting intensive care unit delirium: a bivariate meta‐analysis. Int J Nurs Stud. 2021;113:103782. [DOI] [PubMed] [Google Scholar]
- 81. Hayhurst CJ, Pandharipande PP, Hughes CG. Intensive care unit delirium: a review of diagnosis, prevention, and treatment. Anesthesiology. 2016;125(6):1229–1241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Wu Y, Wang G, Zhang Z, Fan L, Ma F, Yue W, et al. Efficacy and safety of unrestricted visiting policy for critically ill patients: a meta‐analysis. Crit Care. 2022;26(1):267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Matsuoka A, Yoshihiro S, Shida H, Aikawa G, Fujinami Y, Kawamura Y, et al. Effects of mobilization within 72 h of ICU admission in critically ill patients: an updated systematic review and meta‐analysis of randomized controlled trials. J Clin Med. 2023;12(18):5888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Hodgson CL, Bailey M, Bellomo R, Brickell K, Broadley T, Buhr H, et al. Early active mobilization during mechanical ventilation in the ICU. N Engl J Med. 2022;387(19):1747–1758. [DOI] [PubMed] [Google Scholar]
- 85. Wang YT, Lang JK, Haines KJ, Skinner EH, Haines TP. Physical rehabilitation in the ICU: a systematic review and meta‐analysis. Crit Care Med. 2022;50(3):375–388. [DOI] [PubMed] [Google Scholar]
- 86. Nakanishi N, Oto J, Tsutsumi R, Yamamoto T, Ueno Y, Nakataki E, et al. Effect of electrical muscle stimulation on upper and lower limb muscles in critically ill patients: a two‐center randomized controlled trial. Crit Care Med. 2020;48(11):e997–e1003. [DOI] [PubMed] [Google Scholar]
- 87. Nakanishi N, Yoshihiro S, Kawamura Y, Aikawa G, Shida H, Shimizu M, et al. Effect of neuromuscular electrical stimulation in patients with critical illness: an updated systematic review and meta‐analysis of randomized controlled trials. Crit Care Med. 2023;51:1386–1396. [DOI] [PubMed] [Google Scholar]
- 88. Campos DR, Bueno TBC, Anjos J, Zoppi D, Dantas BG, Gosselink R, et al. Early neuromuscular electrical stimulation in addition to early mobilization improves functional status and decreases hospitalization days of critically ill patients. Crit Care Med. 2022;50(7):1116–1126. [DOI] [PubMed] [Google Scholar]
- 89. Taito S, Yamauchi K, Tsujimoto Y, Banno M, Tsujimoto H, Kataoka Y. Does enhanced physical rehabilitation following intensive care unit discharge improve outcomes in patients who received mechanical ventilation? A systematic review and meta‐analysis. BMJ Open. 2019;9(6):e026075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Major ME, Kwakman R, Kho ME, Connolly B, McWilliams D, Denehy L, et al. Surviving critical illness: what is next? An expert consensus statement on physical rehabilitation after hospital discharge. Crit Care. 2016;20(1):354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Major ME, Dettling‐Ihnenfeldt D, Ramaekers SPJ, Engelbert RHH, van der Schaaf M. Feasibility of a home‐based interdisciplinary rehabilitation program for patients with post‐intensive care syndrome: the REACH study. Crit Care. 2021;25(1):279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92. Landi F, Camprubi‐Robles M, Bear DE, Cederholm T, Malafarina V, Welch AA, et al. Muscle loss: The new malnutrition challenge in clinical practice. Clinical nutrition. Clin Nutr. 2019;38(5):2113–2120. [DOI] [PubMed] [Google Scholar]
- 93. Ziegler TR. Parenteral nutrition in the critically ill patient. N Engl J Med. 2009;361(11):1088–1097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94. Casaer MP, Wilmer A, Hermans G, Wouters PJ, Mesotten D, Van den Berghe G. Role of disease and macronutrient dose in the randomized controlled EPaNIC trial: a post hoc analysis. Am J Respir Crit Care Med. 2013;187(3):247–255. [DOI] [PubMed] [Google Scholar]
- 95. Chapple LS, Ridley EJ, Chapman MJ. Trial design in critical care nutrition: the past, present and future. Nutrients. 2020;12(12):3694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96. Allingstrup MJ, Kondrup J, Wiis J, Claudius C, Pedersen UG, Hein‐Rasmussen R, et al. Early goal‐directed nutrition versus standard of care in adult intensive care patients: the single‐centre, randomised, outcome assessor‐blinded EAT‐ICU trial. Intensive Care Med. 2017;43(11):1637–1647. [DOI] [PubMed] [Google Scholar]
- 97. Doig GS, Simpson F, Bellomo R, Heighes PT, Sweetman EA, Chesher D, et al. Intravenous amino acid therapy for kidney function in critically ill patients: a randomized controlled trial. Intensive Care Med. 2015;41(7):1197–1208. [DOI] [PubMed] [Google Scholar]
- 98. Nakano H, Naraba H, Hashimoto H, Mochizuki M, Takahashi Y, Sonoo T, et al. Novel protocol combining physical and nutrition therapies, intensive goal‐directed REhabilitation with electrical muscle stimulation and nutrition (IGREEN) care bundle. Crit Care. 2021;25(1):415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. Singer P, Blaser AR, Berger MM, Calder PC, Casaer M, Hiesmayr M, et al. ESPEN practical and partially revised guideline: clinical nutrition in the intensive care unit. Clin Nutr. 2023;42(9):1671–1689. [DOI] [PubMed] [Google Scholar]
- 100. Compher C, Bingham AL, McCall M, Patel J, Rice TW, Braunschweig C, et al. Guidelines for the provision of nutrition support therapy in the adult critically ill patient: the American Society for Parenteral and Enteral Nutrition. JPEN J Parenter Enteral Nutr. 2022;46(1):12–41. [DOI] [PubMed] [Google Scholar]
- 101. Amass TH, Villa G, OMahony S, Badger JM, McFadden R, Walsh T, et al. Family care rituals in the ICU to reduce symptoms of post‐traumatic stress disorder in family members—a multicenter, multinational, before‐and‐after intervention trial. Crit Care Med. 2020;48(2):176–184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102. Kawai Y, Hamamoto M, Miura A, Yamaguchi M, Masuda Y, Iwata M, et al. Prevalence of and factors associated with physical restraint use in the intensive care unit: a multicenter prospective observational study in Japan. Intern Emerg Med. 2022;17(1):37–42. [DOI] [PubMed] [Google Scholar]
- 103. Freeman S, Hallett C, McHugh G. Physical restraint: experiences, attitudes and opinions of adult intensive care unit nurses. Nurs Crit Care. 2016;21(2):78–87. [DOI] [PubMed] [Google Scholar]
- 104. Happ MB. Preventing treatment interference: the nurse's role in maintaining technologic devices. Heart Lung. 2000;29(1):60–69. [DOI] [PubMed] [Google Scholar]
- 105. Ågren S, Eriksson A, Fredrikson M, Hollman‐Frisman G, Orwelius L. The health promoting conversations intervention for families with a critically ill relative: a pilot study. Intensive Crit Care Nurs. 2019;50:103–110. [DOI] [PubMed] [Google Scholar]
- 106. Lester EG, Mace RA, Bannon SM, Popok PJ, Gates MV, Meyers E, et al. Can a dyadic resiliency program improve quality of life in cognitively intact dyads of neuro‐ICU survivors and informal caregivers? Results from a pilot RCT. Neurocrit Care. 2021;35(3):756–766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107. Nielsen AH, Angel S, Egerod I, Lund TH, Renberg M, Hansen TB. The effect of family‐authored diaries on posttraumatic stress disorder in intensive care unit patients and their relatives: a randomised controlled trial (DRIP‐study). Aust Crit Care. 2020;33(2):123–129. [DOI] [PubMed] [Google Scholar]
- 108. Renner C, Jeitziner MM, Albert M, Brinkmann S, Diserens K, Dzialowski I, et al. Guideline on multimodal rehabilitation for patients with post‐intensive care syndrome. Crit Care. 2023;27(1):301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109. Niven DJ, Bastos JF, Stelfox HT. Critical care transition programs and the risk of readmission or death after discharge from an ICU: a systematic review and meta‐analysis. Crit Care Med. 2014;42(1):179–187. [DOI] [PubMed] [Google Scholar]
- 110. Bourne RS, Jennings JK, Panagioti M, Hodkinson A, Sutton A, Ashcroft DM. Medication‐related interventions to improve medication safety and patient outcomes on transition from adult intensive care settings: a systematic review and meta‐analysis. BMJ Qual Saf. 2022;31(8):609–622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Haines KJ, Sevin CM, Hibbert E, Boehm LM, Aparanji K, Bakhru RN, et al. Key mechanisms by which post‐ICU activities can improve in‐ICU care: results of the international THRIVE collaboratives. Intensive Care Med. 2019;45(7):939–947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112. Meyer J, Brett SJ, Waldmann C. Should ICU clinicians follow patients after ICU discharge? Yes. Intensive Care Med. 2018;44(9):1539–1541. [DOI] [PubMed] [Google Scholar]
- 113. NICE . Rehabilitation after critical illness. NICE clinical guideline 83. London: National Institute for Health and Care Excellence; 2009. [PubMed] [Google Scholar]
- 114. Connolly B, Milton‐Cole R, Adams C, Battle C, McPeake J, Quasim T, et al. Recovery, rehabilitation and follow‐up services following critical illness: an updated UK national cross‐sectional survey and progress report. BMJ Open. 2021;11(10):e052214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115. Cuthbertson BH, Rattray J, Campbell MK, Gager M, Roughton S, Smith A, et al. The PRaCTICaL study of nurse led, intensive care follow‐up programmes for improving long term outcomes from critical illness: a pragmatic randomised controlled trial. BMJ. 2009;339:b3723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116. Schofield‐Robinson OJ, Lewis SR, Smith AF, McPeake J, Alderson P. Follow‐up services for improving long‐term outcomes in intensive care unit (ICU) survivors. Cochrane Database Syst Rev. 2018;11(11):Cd012701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117. McPeake J, Henderson P, MacTavish P, Devine H, Daniel M, Lucie P, et al. A multicentre evaluation exploring the impact of an integrated health and social care intervention for the caregivers of ICU survivors. Crit Care. 2022;26(1):152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118. Bakhru RN, Davidson JF, Bookstaver RE, Kenes MT, Peters SP, Welborn KG, et al. Implementation of an ICU recovery clinic at a tertiary care academic center. Crit Care Explor. 2019;1(8):e0034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119. Udeh C, Udeh B, Rahman N, Canfield C, Campbell J, Hata JS. Telemedicine/virtual ICU: where are we and where are we going? Methodist Debakey Cardiovasc J. 2018;14(2):126–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120. Becker CD, Fusaro MV, Scurlock C. Telemedicine in the ICU: clinical outcomes, economic aspects, and trainee education. Curr Opin Anaesthesiol. 2019;32(2):129–135. [DOI] [PubMed] [Google Scholar]
- 121. Kamdar BB, Suri R, Suchyta MR, Digrande KF, Sherwood KD, Colantuoni E, et al. Return to work after critical illness: a systematic review and meta‐analysis. Thorax. 2020;75(1):17–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122. McPeake J, Mikkelsen ME, Quasim T, Hibbert E, Cannon P, Shaw M, et al. Return to employment after critical illness and its association with psychosocial outcomes. A systematic review and meta‐analysis. Ann Am Thorac Soc. 2019;16(10):1304–1311. [DOI] [PubMed] [Google Scholar]
- 123. Norman BC, Jackson JC, Graves JA, Girard TD, Pandharipande PP, Brummel NE, et al. Employment outcomes after critical illness: an analysis of the bringing to light the risk factors and incidence of neuropsychological dysfunction in ICU survivors cohort. Crit Care Med. 2016;44(11):2003–2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124. Su H, Dreesmann NJ, Hough CL, Bridges E, Thompson HJ. Factors associated with employment outcome after critical illness: systematic review, meta‐analysis, and meta‐regression. J Adv Nurs. 2021;77(2):653–663. [DOI] [PubMed] [Google Scholar]
- 125. Cullen KL, Irvin E, Collie A, Clay F, Gensby U, Jennings PA, et al. Effectiveness of workplace interventions in return‐to‐work for musculoskeletal, pain‐related and mental health conditions: an update of the evidence and messages for practitioners. J Occup Rehabil. 2018;28(1):1–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126. Mankowski RT, Anton SD, Ghita GL, Brumback B, Cox MC, Mohr AM, et al. Older sepsis survivors suffer persistent disability burden and poor long‐term survival. J Am Geriatr Soc. 2020;68(9):1962–1969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127. Hermans G, Casaer MP, Clerckx B, Guiza F, Vanhullebusch T, Derde S, et al. Effect of tolerating macronutrient deficit on the development of intensive‐care unit acquired weakness: a subanalysis of the EPaNIC trial. Lancet Respir Med. 2013;1(8):621–629. [DOI] [PubMed] [Google Scholar]
- 128. Guerra C, Hua M, Wunsch H. Risk of a diagnosis of dementia for elderly Medicare beneficiaries after intensive care. Anesthesiology. 2015;123(5):1105–1112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129. Khan SS, Singer BD, Vaughan DE. Molecular and physiological manifestations and measurement of aging in humans. Aging Cell. 2017;16(4):624–633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130. Boston working group on improving health care outcomes through geriatric rehabilitation. Med Care. 1997;35(Suppl 6):Js4–Js20. [DOI] [PubMed] [Google Scholar]
- 131. Scheffler RM, Weisfeld N, Ruby G, Estes EH. A manpower policy for primary health care. N Engl J Med. 1978;298(19):1058–1062. [DOI] [PubMed] [Google Scholar]
- 132. Campbell TL, McDaniel SH, Cole‐Kelly K, Hepworth J, Lorenz A. Family interviewing: a review of the literature in primary care. Fam Med. 2002;34(5):312–318. [PubMed] [Google Scholar]
- 133. Sevin CM, Jackson JC. Post‐ICU clinics should be staffed by ICU clinicians. Crit Care Med. 2019;47(2):268–272. [DOI] [PubMed] [Google Scholar]
- 134. Maki Y, Yamaguchi H. Early detection of dementia in the community under a community‐based integrated care system. Geriatr Gerontol Int. 2014;14(Suppl 2):2–10. [DOI] [PubMed] [Google Scholar]
- 135. Plochg T, Klazinga NS. Community‐based integrated care: myth or must? Int J Qual Health Care. 2002;14(2):91–101. [DOI] [PubMed] [Google Scholar]
- 136. Li L, Jiang Y, Zhu Q, Liu D, Chang M, Wang Y, et al. Hyaluronan with different molecular weights can affect the gut microbiota and pathogenetic progression of post‐intensive care syndrome mice in different ways. Int J Mol Sci. 2023;24(11):9757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137. Saito M, Fujinami Y, Ono Y, Ohyama S, Fujioka K, Yamashita K, et al. Infiltrated regulatory T cells and Th2 cells in the brain contribute to attenuation of sepsis‐associated encephalopathy and alleviation of mental impairments in mice with polymicrobial sepsis. Brain Behav Immun. 2021;92:25–38. [DOI] [PubMed] [Google Scholar]
- 138. Fujinami Y, Inoue S, Ono Y, Miyazaki Y, Fujioka K, Yamashita K, et al. Sepsis induces physical and mental impairments in a mouse model of post‐intensive care syndrome. J Clin Med. 2021;10(8):1593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139. Needham DM, Davidson J, Cohen H, Hopkins RO, Weinert C, Wunsch H, et al. Improving long‐term outcomes after discharge from intensive care unit: report from a stakeholders' conference. Crit Care Med. 2012;40(2):502–509. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing not applicable—No new data generated.