

Abstract
Context:
The antimicrobial potential of conventional medicaments is reduced due to their limited permeability. The use of calcium hydroxide (CH) is known to reduce the root strength. Nano intracanal medicaments have the following advantages over conventional such as higher surface area and chemical reactivity, and due to its nanosize, have better penetrability, supporting its possible use as an intracanal medicament. Nano versions of CH, chitosan (CS), CS + CH, curcumin (T), and its conventional forms are used in our study.
Aim:
The aim of this study was to evaluate and compare the depth of penetration of nanosized intracanal medicaments and their effect on fracture resistance of root dentin.
Materials and Methods:
Eighty extracted single-rooted teeth were used after decoronation. Canals were enlarged up to size 30 (0.04° taper) using Neoendo instruments (Orikam, India). Teeth were randomly assigned to two broad groups based on the type of intracanal medicament used; Group A: control (conventional) (n = 40) and Group B: nanosized intracanal medicaments (n = 40). Each group was subdivided into four experimental groups (n = 10), Group A1: CH, Group A2: CS, Group A3: curcumin (T), Group A4: CS + CH, Group B1: nano calcium hydroxide (NCH), Group B2: nano CS (NCS), Group B3: nano curcumin (NT), and Group B4: NCS + nano calcium hydroxide (NCS + NCH). All the specimens were stored in a humidor at 37°C for 4 weeks. Out of 10 specimens from each group, five specimens were used for evaluating the depth of penetration using a confocal laser scanning electron microscope, and the remaining five specimens were used for evaluating fracture resistance in a universal testing machine at the end of 4 weeks. Data were analyzed using one-way ANOVA and intergroup comparison using Tukey’s post hoc multiple comparison test.
Results:
The highest fracture resistance was seen with NCS and the maximum depth of penetration with nano calcium hydroxide (NCH).
Conclusion:
The fracture resistance and depth of penetration at a 4-week interval were higher in nano forms compared to their micro-sized counterparts with all groups. The coronal section presented the highest depth of penetration of intracanal medicaments followed by the middle and least in the apical section of root dentin with all groups.
Keywords: Depth of penetration, fracture resistance, intracanal medicament, nano chitosan, nano calcium hydroxide, nanoparticle
INTRODUCTION
The chief aim of root canal therapy is the complete eradication of microorganisms from the root canal system, preventing reinfection thereby achieving complete periradicular healing.[1] The root canal has complex anatomy, due to which instruments, irrigants, and medicaments do not reach to eliminate the microorganisms that have invaded the dentinal tubules to varying depths of 200–1500 μm, hindering the effects of host defense cells and systemically administered antibiotics. Due to the polymicrobial nature of endodontic infection, intracanal medication is required.[2] The most commonly used intracanal medicament is calcium hydroxide (CH). Its beneficial properties include antimicrobial activity and the potential to induce hard tissue formation. To bring about a favorable effect, intracanal medicament used should penetrate into the dentinal tubules to come in direct contact with microorganisms.[1,3] However, the limited permeability of conventional medicaments into the dentinal tubules negates their antimicrobial potential. Furthermore, previous studies have shown that the long-term use of CH intracanal dressing in teeth with persistent infection, resorptive defects, and open apices has a negative impact on the fracture resistance of teeth.[3] CH is also ineffective in the elimination of Enterococcus faecalis, the most important bacterium in the treatment of resistant infections.[4] Several medicaments have been proposed or used as an alternative to CH.
Curcumin (T) [(E, E)-1,7-bis (4-hydroxy-3-methoxy-phenyl)-1,6-heptadiene-3,5-ione]-(diferuloyl methane) is yellow-colored phenolic pigment extracted from turmeric, which is responsible for its biological activities . Extensive research over the last five decades indicates that curcumin possesses potent antioxidant, anti-inflammatory, antitumor, anti-HIV, and antimicrobial properties.[5,6]
Insoluble chitosan (CS) when used as a drug carrier has the added advantage of slow and controlled release of the medicament. This combination increases intracanal medicament stability. Previous studies have shown an additive effect when Ca(OH)2 was combined with CS against Candida albicans and E. faecalis.[7,8]
Nanoparticles are microscopic particles measuring <100 nm, increasing surface area/mass ratio, chemical reactivity, and bioavailability. In their nano form, intracanal medicaments can reach the complex anatomy of the root canal system. A medicament that penetrates deeper into the dentinal tubules may not only serve as a blocking agent, preventing microbial repopulation, but also inactivates them in the tubules.[1,3]
CS nanoparticles (CNP) due to higher surface area and charge density react with the negative charge surface of bacterial cell resulting in bacterial cell death. CNP have a tendency to reduce biofilm-forming bacteria and disrupt biofilm structure. The higher antibacterial activity of nano CS (NCS) could be attributed to its higher surface area, leading to better interaction with bacterial cell membrane.[3,7]
Although previous studies have evaluated the depth of penetration and fracture resistance of root dentin for CH, NCH, CS, and NCS, for curcumin (T, nano curcumin [NT]), the combination of CH and CS both in conventional and nano form (CS + CH, NCS + NCH) studies has not yet been reported in the literature. Hence, the aim of this in vitro study was to comparatively evaluate CH, nano calcium hydroxide (NCH), CS, NCS, curcumin (T), NT, CS + CH, and NCS + nano calcium hydroxide (NCS + NCH) as intracanal medicaments on the depth of penetration and fracture resistance of root dentin.
Null hypothesis: the null hypothesis considered in this study is that nano versions of CH, CS, CS + CH, and curcumin (T) have no significant difference on the depth of penetration and fracture resistance compared to its micro-sized (conventional) intracanal medicaments.
MATERIALS AND METHODS
The study obtained ethical clearance from the Institutional Research Committee (number IRBREF/IRB/CODE KLE/OCT2019/28), Bengaluru, India.
Sample preparation
Eighty freshly extracted single-rooted human teeth with single canal and fully formed apices extracted for orthodontic and periodontal reasons were selected. The teeth were decoronated at the cementoenamel junction to obtain a standardized length of 14 mm in all the groups; a 10-K file (MANI, Inc., Japan) inserted along the canal until the tip was visible at the apical foramen confirmed its working length, and then, 0.5 mm was subtracted from this length. In the crown-down technique, cleaning and shaping of the root canal were performed with rotary nickel–titanium instruments (Neoendo Orikam, India) until a master apical rotary size of 30 (0.04° taper). In between each instrument change, the canals were irrigated with 2 ml of 3% sodium hypochlorite and 15% EDTA (RC-Prep Premier Dental, India). At the end of instrumentation, canals were irrigated with 17% EDTA (Dent Wash-Prime Dental, India) for 3 min, followed by 5 ml of saline solution, and later, canals were dried using sterile paper points. After root canal preparation, the apical end of the canal was sealed with resin to create a closed-end system. Later, teeth were randomly assigned into two experimental groups (n = 40). Each group was further subdivided into four experimental groups (n = 10) based on intracanal medicaments used.
Group distribution
Group A: control (conventional intracanal medicaments)
Group A1: CH
Group A2: CS
Group A3: curcumin (T)
Group A4: CS + CH
Group B: nano form (nano intracanal medicaments)
Group B1: nano calcium hydroxide (NCH)
Group B2: NCS
Group B3: NT
Group B4: NCS + nano calcium hydroxide (NCS + NCH).
Particle size determination
DLS technique (ZetaPALS particle sizing software version 5.23, Brookhaven Instruments Corp) was used to measure the particle size distribution and zeta potential of the synthesized nanoparticles. Into 10 ml of deionized distilled water, 1 mg of the sample was dispersed and ultra-sonicated for 10 min. Later, 1 ml of the supernatant was removed and used for DLS measurement. The size of the individual particles was measured using ImageJ software and ensured they were of nanosize. The particle size of NCH, NCS, and NT particles was found to be in the size range of 308.3–315.7 nm with a mean value of 311.8 nm as the effective diameter of NCS nanoparticles; The size of nano calcium hydroxide ranged between 226.5 and 256.7 nm with mean value of 240.8 nm as effective diameter.
Placement of intracanal medicament
Group A: control (conventional intracanal medicaments)
For all the groups included in conventional intracanal medicaments for Group A1 (n = 10): CH, Group A2 (n = 10): CS, and Group A4 (n = 10): CS + CH, the powder was mixed with saline in 1:1 ratio on a glass slab with stainless steel spatula in paste consistency and inserted into the canal using Lentulo Spiral except for Group A3 (n = 10): curcumin (T), in which the powder was mixed with DMSO solution in 1:1 ratio on a glass slab with stainless steel spatula in paste consistency and inserted into the canal using Lentulo Spiral (Mani Inc., Japan).
Group B: nano form (nano intracanal medicaments)
For all the groups included in the nano group, Group B1 (n = 10): nano calcium hydroxide (NCH), Group B2 (n = 10): NCS, Group B4 (n = 10): NCS + nano calcium hydroxide (NCS + NCAOH), and Group B3 (n = 10): NT, intracanal medicaments in viscous form was injected into the canal using 27-gauge syringe except for Group B1 (n = 10): nano calcium hydroxide (NCH), in which the powder was mixed with saline in 1:1 ratio on a glass slab with stainless steel spatula to paste consistency and was inserted into the canal using Lentulo Spiral (Mani Inc., Japan).
Later, flowable composite (Restofill N Flo, Anabond Stedman Pharma Research (P) Ltd., Chennai, India) was used to seal root canals apically, and temporary filling material Cavit (MD-Temp Plus Meta Biomed Co. Ltd, Korea) was used to seal orifices with minimum 3 mm thickness. For 4 weeks, specimens were stored in a humidor at 37°C. At the end of 4 weeks, out of the 10 specimens from each group, five specimens were used to evaluate the fracture resistance in a universal testing machine, and the remaining five specimens were used for evaluating the depth of penetration using a confocal laser scanning electron microscope (CLSEM).
Evaluation of fracture resistance (universal testing machine)
The temporary material was removed, and using a round carbide bur, the root canal access was shaped to receive the loading fixture. Self-cure acrylic was used to make customized rectangular molds into which samples were embedded leaving coronal 3 mm of root structure unimpeded. A spherical tip fixture of 2 mm diameter was loaded vertically on the center of the root canal of each specimen exerting a compressive force at a crosshead speed of 0.5 mm/min. The fracture resistance of teeth was measured in Newton and subjected to statistical analysis.
Evaluation of the depth of penetration (confocal laser scanning electron microscope)
To evaluate the depth of penetration of medicaments through CLSEM, intracanal medicaments of each group were mixed with 0.1 ml of rhodamine B dye. After 4 weeks, all the samples (n = 5) from each group were sectioned at the coronal, middle, and apical thirds using a double-sided diamond disk under continuous water cooling and obtained with thickness of 1 mm at 3 mm, 5 mm, and 8 mm distance from the apex, respectively. The slices were photographed, and images were analyzed in the CLSM Image Browser (Carl Zeiss LSM 510; Jena, Germany) to measure the longest penetration depth of intracanal medicaments. Measurements were recorded using the digital measuring ruler. To obtain a single value for each section, data were averaged. All analyses were recorded and evaluated by a single operator to rule out any discrepancies and repeated two times for intra-rater reliability.
Statistical analysis
The mean and standard deviation of the fracture resistance of teeth and depth of penetration were calculated for each group, and using the one-way ANOVA and Tukey’s post hoc test, the data were statistically analyzed. Intergroup variations were analyzed by one-way ANOVA. Intragroup variations were analyzed by Tukey’s post hoc test. The level of significance β was 0.05 (i.e., P < 0.05).
RESULTS
Fracture resistance of teeth
As depicted in Table 1, the mean fracture resistance of root dentin value in nano intracanal medicaments was the highest with Group B2: NCS group – 1260.46N, followed by Group B4: 1160.23N NCS + nano calcium hydroxide (NCS + NCH) and Group B3: 1120.24N NT, and the least with Group B1: 1060.24N nano CH, which was statistically significant.
Table 1.
The mean value of fracture resistance of root dentin
| n | Mean | Std. Deviation | Std. Error | |
|---|---|---|---|---|
| GROUP A1(CH) | 5 | 374.2600 | 248.52374 | 111.14319 |
| GROUP B1 (NCH) | 5 | 1060.2460 | 89.44607 | 40.00150 |
| GROUP A2 (CS) | 5 | 993.9400 | 5.76741 | 2.57926 |
| GROUP B2(NCS) | 5 | 1260.4600 | 54.91856 | 24.56033 |
| GROUP A3 (T) | 5 | 404.04 | 159.93814 | 71.52651 |
| GROUP B3(NT) | 5 | 1120.2400 | 83.67198 | 37.41925 |
| GROUP A4 (CS + CH) | 5 | 434.5800 | 362.83085 | 162.26289 |
| Group B4 (NCS + NCH) | 5 | 1160.2360 | 54.76861 | 24.49327 |
| Total | 40 | 851.0003 | 391.00183 | 61.82282 |
ANOVA Level of Significance at P≤0.0
The mean fracture resistance of root dentin value in conventional intracanal medicaments was the highest with Group A2: 993.94N CS, followed by Group A4: 434.58N CS + CH, and the lowest with Group A3: 404.04N curcumin (T). Group A1: 374.26N CH recorded the least fracture resistance, which was statistically significant.
Depth of penetration of intracanal medicament
The mean values of the depth of penetration among the medicament groups in the coronal, middle, and apical sections, respectively, are depicted in Table 2.
Table 2.
Comparison of the mean value of depth of penetration among groups in coronal, middle and apical section (P<0.05)
| Coronal | Middle | Apical | ||||
|---|---|---|---|---|---|---|
|
|
|
|
||||
| Mean | Std.Dev. | Mean | Std.Dev. | Mean | Std.Dev. | |
| Group A1(CH) | 1086.98 | 48.4446 | 1018.0212 | 66.99758 | 388.1870 | 36.76935 |
| Group B1(NCH) | 1526.5200 | 2.84968 | 1178.6658 | 57.332730 | 1214.0276 | 8.49523 |
| Group A2(CS) | 1056.4760 | 88.05923 | 579.3370 | 1.94347 | 343.3278 | 47.02511 |
| Group B2 (NCS) | 1373.4128 | 2.849675 | 1064.8148 | 1.871503 | 840.4664 | 1.87337 |
| Group A3 (T) | 413.3030 | 31.21773 | 351.8440 | 16.71654 | 246.0944 | 18.85149 |
| Group B3 (NT) | 1041.41360 | 2.764702 | 861.4952 | 2.074442 | 469.9446 | 2.60887 |
| Group A4 (CS+CH) | 559.05400 | 2.213172 | 424.4834 | 4.39160 | 336.8986 | 2.608875 |
| Group B4 (NCS + NCH) | 1140.19440 | 4.724946 | 1048.9272 | 1.943475 | 664.7754 | 2.40616 |
The highest mean depth of penetration in the coronal, middle, and apical sections was with nano calcium hydroxide (NCH) – 1526.52 μm, 1178.66 μm, and 1214. 027 μm, and among it, the least was with NT – 1041.41 μm, 861.49 μm, and 469.9446 μm, and in conventional, the highest with CH – 1086.98 μm, 1018.02 μm, and 388.1870 μm, and the least with curcumin (T) – 413.30 μm, 351.84 μm, and 246.09 μm, respectively.
The highest depth of penetration of intracanal medicaments was seen with nano form compared to conventional form, in the coronal section compared to the middle and apical, which was statistically significant.
DISCUSSION
Nanoparticles are a class of newer medicaments that are hypothesized to have antibacterial effects. The nanosize provides an increased surface area which can absorb other medicaments and exert an antimicrobial effect. Nano intracanal medicaments, due to its smaller size, can penetrate into the deeper layers of dentin and effectively kill endodontic bacteria in the dentinal tubules by causing disruption of the biofilm.[9] CH placed in the root canal had a significantly negative effect on the strength of the root.[10,11,12] To bring about a favorable effect, any intracanal medicaments used should penetrate into dentinal tubules to come in direct contact with the microorganisms.
In the present study, the DLS technique was used to measure the size of nanoparticles. The particle size distribution and zeta potential of synthesized NCH, NCS, and NT were assessed and ensured they were of nanosize [Figure 1].
Figure 1.
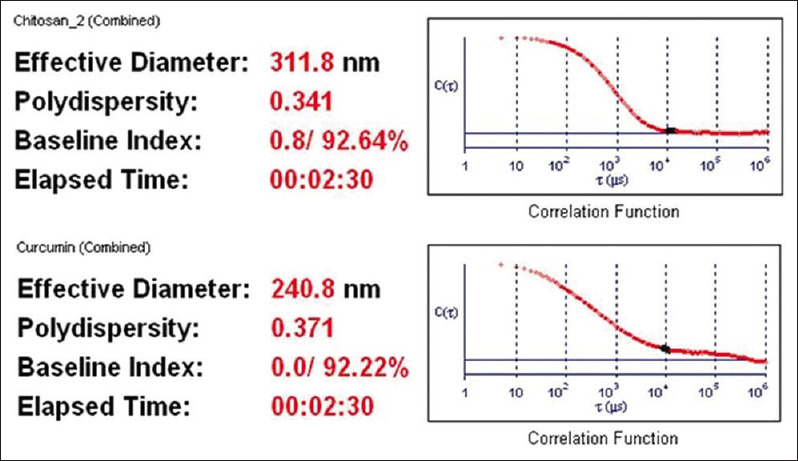
The size of nano calcium hydroxide ranged between 226.5 and 256.7 nm with mean value of 240.8 nm as effective diameter
Nano versions of CH, CS, CS + CH, and curcumin (T) had significant difference and gave better depth of penetration and fracture resistance compared to its micro-sized (conventional) intracanal medicaments.
According to the results, the null hypothesis was rejected; in the present study, NCS showed the highest fracture resistance compared to conventional and other nano intracanal medicaments [Table 1].
The previous study has concluded that NCS showed improved fracture resistance and toughness, and particles exhibit affinity to collagenase enzyme, thereby improving dentin stability in the long term which could have led to increased fracture resistance with the NCS group compared to other groups.[3]
Although curcumin has been described as a promising antibacterial drug with therapeutic potential, one of the major drawbacks of using curcumin alone is its low bioavailability, which appears to be mostly owing to poor absorption, quick metabolism, and rapid elimination.[13] NT is also proposed as a means of increasing curcumin bioavailability.[14] Curcumin nanoparticles (2–40 nm) have significant antibacterial action against Staphylococcus aureus, Escherichia coli, and Pseudomonas aeruginosa.[13] Results of the present study showed a statistically significant reduction in fracture resistance with curcumin followed by CH. The results of the present study are not in agreement with a previous study conducted where curcumin showed no effect on microhardness.[13] The possible cause for the decrease in fracture toughness still needs to be researched, and the exact reason could not be explained. Mere literature exists studying the effect of curcumin on the microhardness of root dentin. Hence, still further research in this study warrants the use of curcumin for antimicrobial treatment of root canal infection in the long term keeping in mind the negative effect of curcumin on fracture resistance of root dentin. CH resulted in a maximum reduction in fracture resistance. Most probable reason could be because of strong alkalinity of CH that leads to neutralization, dissolution or denaturation of the acid proteins and proteoglycans serving as bonding agents between collagen network and hydroxyapatite crystals in dentine. Similar to our findings, many authors have reported a decrease in the fracture resistance of teeth filled with CH.[12,15,16,17]
In a study by Naseri et al. the nano calcium hydroxide reduced the microhardness of root dentin to a lesser extent in comparison with CH, and the difference between the two medications was statistically significant, and the results of which are in agreement with our present study.[18]
Complete elimination of microbes from the root canal system is difficult to achieve, owing to its anatomical complexities and limited access to the instruments and irrigants used. However, the limited permeability of conventional medicaments into the dentinal tubules negates their antimicrobial potential. Studies have reported that smaller-sized particles show higher antibacterial activity than macro-sized ones.[1,3] Results of previous in vitro studies concluded that the antimicrobial activity of nano calcium hydroxide (NCH) was superior to conventional CH in a culture medium.[1] Thus, minimizing the particle size and production of nano form of CH enhances the penetration of the material into the dentinal tubules and also may enhance the antimicrobial efficacy due to the longer time of the drug’s presence in dentinal tubules. Nanoparticles by virtue of their size can be effectively delivered into the complex anatomies of the root canal system.[3]
The results of the present study showed that nano calcium hydroxide particles had more depth of peetration than CH [Figure 2A], which is consistent with the findings of Sireesha et al.[3,19]
Figure 2.

CLSM images of the depth of penetration of nano calcium hydroxide(2A) and nanocurcumin(2B) at the coronal (a), middle (b), and apical (c) levels
The results are in agreemennt with previous studies which proved that NCH can penetrate into deeper layers of dentin compared to CH. Numerous factors influence the penetration of material into tubules such as smear layer removal, root canal dimension, and physical and chemical properties of the material. The smaller size and large surface area/mass ratio of nanoparticles confers them with distinctive physical properties and increased chemical reactivity.[1] The above-mentioned factors could have favored the highest tubular penetration achieved by NCH.
CS showed less penetration depth compared to CH; the possible explanation could be due to its gelling-out nature which hinders its penetration into dentinal tubules.[3] NCS showed better penetration depth than CS. In spite of their smaller particle size, limited depth of penetration was evident with NCS compared to NCH, which could be again due to their tendency to agglomerate. The gelling-out nature and lack of uniform distribution of nanoparticles were observed in NCS in a previous study conducted.[3]
The least depth of penetration was with curcumin among intracanal medicaments [Figure 2B]. This is the first study to measure the depth of penetration of the curcumin and lacks evidence in the literature. Hence, further studies are required to validate the results of the present groups.
CH when combined with different vehicles has shown long-term release of calcium ions.[7,8,19] Hence, in our study, NCH was combined with NCH to study its effects on root dentin. Results showed that the combination (NCS + NCH) had better fracture resistance and depth of penetration in comparison to curcumin and its nano form. This effect of combined ICM on root dentin microstructure was evaluated here. As CS has mucoadhesive properties, whether it has a similar adhesive property to root canal dentin needs to be investigated because this property might help in the prolonged action of medicament within the root canal system.[8] This was the preliminary study determining the fracture resistance of this group; hence, there is no evidence in the literature. To validate these results, further in vitro studies need to be done.
The coronal third showed the highest mean depth of penetration for all medicaments, followed by the middle third, and the least in the apical third (P ≤ 0.05). Numerous anatomical factors such as less tubule density, the presence of sclerotic dentin, and occluded tubules could have led to the poor penetrability of medicaments in the apical third. The effectiveness of smear layer removal also reduces in the apical third of the root.[1]
Limitation
As it is in vitro study, the above findings can be checked with in vivo study. The strength of the study is the efficacy of all three nano intracanal medicaments, and its combination to know synergistic action was studied with the latest scientific approach. Here, nanotechnology was used, which is the future of dentistry.
Future scope
Studies focusing on antimicrobial activity using different nano intracanal medicaments, their dosage required and duration of action, and possible interactions with endodontic materials can be carried out.
CONCLUSION
The fracture resistance and depth of penetration at a 4-week interval were higher in nano forms compared to their micro-sized counterparts with all groups. The coronal section presented the highest depth of penetration of intracanal medicaments, followed by the middle, and the least in the apical section of root dentin with all groups. Although NT has shown good antibacterial activity, it negatively influences the strength of root dentin.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
Dr. Arun Babu : Center for Nano Science and Engineering, IISC Bangalore, Karnataka, India. Dr. Sai Prathyusha Yadama. Dr. Shishuma DS: CMTI, Bangalore, Karnataka, India.
REFERENCES
- 1.Zand V, Mokhtari H, Hasani A, Jabbari G. Comparison of the penetration depth of conventional and nano-particle calcium hydroxide into dentinal tubules. Iran Endod J. 2017;12:366–70. doi: 10.22037/iej.v12i3.16421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dalavai P, Nasreen F, Srinivasan R, Pramod J, Bhandary S, Penmatsa C. To evaluate and compare the compressive strength of root dentin exposed to calcium hydroxide, mixed with various vehicles for a period of 30 days –An in vitro study. J Conserv Dent. 2021;24:563–7. doi: 10.4103/jcd.jcd_316_21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sireesha A, Jayasree R, Vidhya S, Mahalaxmi S, Sujatha V, Kumar TS. Comparative evaluation of micron- and nano-sized intracanal medicaments on penetration and fracture resistance of root dentin –An in vitro study. Int J Biol Macromol. 2017;104:1866–73. doi: 10.1016/j.ijbiomac.2017.05.126. [DOI] [PubMed] [Google Scholar]
- 4.Basrani B, Tjäderhane L, Santos JM, Pascon E, Grad H, Lawrence HP, et al. Efficacy of chlorhexidine- and calcium hydroxide-containing medicaments against Enterococcus faecalis in vitro. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:618–24. doi: 10.1016/s1079-2104(03)00166-5. [DOI] [PubMed] [Google Scholar]
- 5.Bhawana, Basniwal RK, Buttar HS, Jain VK, Jain N. Curcumin nanoparticles:preparation, characterization, and antimicrobial study. Journal of agricultural and food chemistry. 2011;59:2056–61. doi: 10.1021/jf104402t. [DOI] [PubMed] [Google Scholar]
- 6.Neelakantan P, Subbarao C, Sharma S, Subbarao CV, Garcia-Godoy F, Gutmann JL. Effectiveness of curcumin against Enterococcus faecalis biofilm. Acta Odontol Scand. 2013;71:1453–7. doi: 10.3109/00016357.2013.769627. [DOI] [PubMed] [Google Scholar]
- 7.Shaik J, Garlapati R, Nagesh B, Sujana V, Jayaprakash T, Naidu S. Comparative evaluation of antimicrobial efficacy of triple antibiotic paste and calcium hydroxide using chitosan as carrier against Candida albicans and Enterococcus faecalis: An in vitro study. J Conserv Dent. 2014;17:335–9. doi: 10.4103/0972-0707.136444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Harshitha VS, Ranjini MA, Nadig RR. Antibacterial efficacy of nisin, calcium hydroxide, and triple antibiotic paste in combination with chitosan as an intracanal medicament against Enterococcus faecalis – An in vitro study. J Conserv Dent. 2022;25:504–9. doi: 10.4103/jcd.jcd_125_22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jhamb S, Singla R, Kaur A, Sharma J, Bhushan J. An in vitro determination of antibacterial effect of silver nanoparticles gel as an intracanal medicament in combination with other medicaments against Enterococcus fecalis. J Conserv Dent. 2019;22:479–82. doi: 10.4103/JCD.JCD_113_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Andreasen JO, Farik B, Munksgaard EC. Long-term calcium hydroxide as a root canal dressing may increase risk of root fracture. Dent Traumatol. 2002;18:134–7. doi: 10.1034/j.1600-9657.2002.00097.x. [DOI] [PubMed] [Google Scholar]
- 11.Doyon GE, Dumsha T, von Fraunhofer JA. Fracture resistance of human root dentin exposed to intracanal calcium hydroxide. J Endod. 2005;31:895–7. doi: 10.1097/01.don.0000194542.02521.af. [DOI] [PubMed] [Google Scholar]
- 12.Rosenberg B, Murray PE, Namerow K. The effect of calcium hydroxide root filling on dentin fracture strength. Dent Traumatol. 2007;23:26–9. doi: 10.1111/j.1600-9657.2006.00453.x. [DOI] [PubMed] [Google Scholar]
- 13.Prabhakar A, Taur S, Hadakar S, Sugandhan S. Comparison of antibacterial efficacy of calcium hydroxide paste, 2% chlorhexidine gel and turmeric extract as an intracanal medicament and their effect on microhardness of root dentin: An in vitro study. Int J Clin Pediatr Dent. 2013;6:171–7. doi: 10.5005/jp-journals-10005-1213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Panwar D, Sidhu K, Bhushan J, Kakkar V, Mehta M, Sharma J. Evaluation of antimicrobial efficacy of nanocurcumin-coated gutta-percha against Enterococcus faecalis: An in vitro study. J Conserv Dent. 2023;26:160–4. doi: 10.4103/jcd.jcd_512_22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Dudeja C, Taneja S, Kumari M, Singh N. An in vitro comparison of effect on fracture strength, pH and calcium ion diffusion from various biomimetic materials when used for repair of simulated root resorption defects. J Conserv Dent. 2015;18:279–83. doi: 10.4103/0972-0707.159720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Yassen GH, Vail MM, Chu TG, Platt JA. The effect of medicaments used in endodontic regeneration on root fracture and microhardness of radicular dentine. Int Endod J. 2013;46:688–95. doi: 10.1111/iej.12046. [DOI] [PubMed] [Google Scholar]
- 17.Yassen GH, Platt JA. The effect of nonsetting calcium hydroxide on root fracture and mechanical properties of radicular dentine: A systematic review. Int Endod J. 2013;46:112–8. doi: 10.1111/j.1365-2591.2012.02121.x. [DOI] [PubMed] [Google Scholar]
- 18.Naseri M, Eftekhar L, Gholami F, Atai M, Dianat O. The effect of calcium hydroxide and nano-calcium hydroxide on microhardness and superficial chemical structure of root canal dentin: An ex vivo study. J Endod. 2019;45:1148–54. doi: 10.1016/j.joen.2019.06.002. [DOI] [PubMed] [Google Scholar]
- 19.Nadar A, Muliya VS, Pai S, Pentapati KC. A comparative evaluation of calcium ion release and pH change using calcium hydroxide nanoparticles as intracanal medicament with different vehicles –An in vitro study. J Conserv Dent. 2023;26:47–51. doi: 10.4103/jcd.jcd_387_22. [DOI] [PMC free article] [PubMed] [Google Scholar]