

Abstract
Polyneuropathy, organomegaly, endocrinopathy, M protein elevation, and skin changes (POEMS) syndrome is one of the rare paraneoplastic disorders of the multiorgan association whose initialism describes the principal clinical features as polyneuropathy, organomegaly, endocrinopathy, M-protein elevation, and skin changes caused by an underlying plasma cell disorder, one of the major diagnostic criteria for which is the presence of an osseous lesion. We present a case of POEMS syndrome with nearly all signs and symptoms on clinical and hematological examinations, which was further investigated with MRI of the whole spine and 18F-fluorodeoxyglucose positron emission tomography/computed tomography scan, as the latter is a very useful imaging modality for evaluation of any paraneoplastic syndromes, including myeloproliferative disorders such as plasmacytoma or multiple myeloma, and lymphoproliferative or other malignancies.
Keywords: 18F-fluorodeoxyglucose, chronic inflammatory demyelinating polyradiculoneuropathy, fluorodeoxyglucose positron emission tomography/computed tomography scan, multiple myeloma, plasmacytoma, POEMS syndrome
Introduction
The paraneoplastic POEMS syndrome with multiorgan involvement is primarily due to an underlying plasma cell neoplasm[1,2] characterized by Dispenzieri diagnostic criteria which are further categorized into major and minor.[3] The major criteria for the syndrome are polyneuropathy, clonal plasma cell disorder, osteosclerotic lesion, elevated vascular endothelial growth factor, and the presence of Castleman disease. Minor criteria include organomegaly, endocrinopathy, characteristic skin changes, papilledema, extravascular volume overload, and thrombocytosis. Diagnoses are often delayed because the syndrome is rare and can be mistaken for other neurologic disorders, most commonly chronic inflammatory demyelinating polyradiculoneuropathy (CIDP). POEMS syndrome should also be distinguished from one of its variants, known as Castleman disease, which has no clonal plasma cell proliferation and little to no peripheral neuropathy but shows the presence of lymphadenopathy.[4]
Background and Procedure
A 55-year-old male presented with complaints of polyneuropathy in the form of paresthesias, numbness, and weakness in bilateral lower and upper limbs and was found to have absent deep tendon reflexes in heels as well as flexion of the proximal interphalangeal joints of bilateral upper fifth digits with their contractures [Figure 1a] since 3 years associated with weight loss of over 20 kg in the last 3 years, which was being treated as CIDP with no clinical improvement. The clinical examination also found diffuse hyperpigmentation of the skin, mild splenomegaly, and mild diffuse subcutaneous edema. The complete blood count (CBC) shows mild anemia with 9.8 mg/dl hemoglobin and thrombocytosis with platelet counts of about 620,000/uL. The endocrinological examination revealed hypothyroidism with a TSH of 12.5 mU/L, Free T3 of 0.11 ng/dl, and Free T4 of 0.4 ng/dl. The patient also complained of fatigue and sexual problems. Selective serum protein electrophoresis reveals the presence of the M band and M (monoclonal) protein, which is an essential marker in the diagnosis of POEMS syndrome. Monoclonal protein is often associated with unusual bone hardening or thickening. The serum immunofixation also revealed an immunoglobulin G lambda monoclonal protein. The electromyography showed a demyelinating sensorimotor neuropathy. Whole-body plain X-ray screening found a heterogeneous lesion involving the entire D10 vertebra [Figure 1b].
Figure 1.
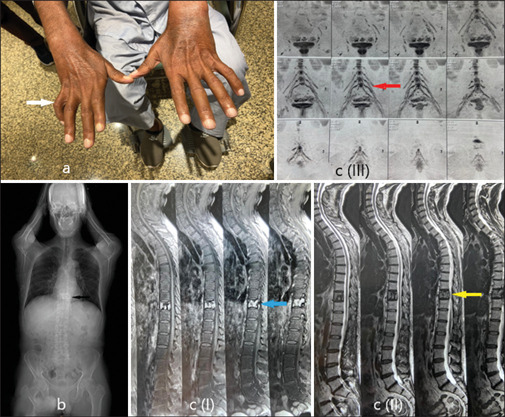
(a) Flexion of the proximal interphalangeal joints of the bilateral upper 5th digits with their contractures and hyperpigmentation of the skin (black arrow). (b) Whole-body plain X-ray screening found a mixed lytic sclerotic lesion involving the entire D10 vertebra (white arrow). (c) MRI findings in sagittal T1 and T2, and MRI neurography. Sagittal sequences in T1 reveal a contrast-enhancing lesion (c) (I), blue arrow] with T2 hyperintense signal intensity (c) (II), yellow arrow] and an expansile lesion in the D10 vertebral body with cortical erosions and a solid periosteal reaction. The rest of the spine was unremarkable. The MRI neurography of the lumbosacral plexus (c) (III), red arrow] reveals thickening and an increase in nerve calibre and signal intensity with perineural edoema
The MRI lumbosacral spine with whole-spine screening was done, which revealed a T1 contrast-enhancing lesion [Figure 1c (I)] with a T2 hyperintense signal [Figure 1c (II)] in the D10 vertebral body with cortical erosions and a solid periosteal reaction. The rest of the spine was unremarkable. The MRI neurography of the lumbosacral plexus [Figure 1c (III)] reveals thickening and an increase in nerve caliber and signal intensity with perineural edema.
The patient was then referred for whole-body 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) imaging to further characterize the lesion as well as for the presence of disease elsewhere in the body. The FDG PET/CT scan reveals a metabolically active expansile-enhancing soft-tissue osteolytic lesion with dense interspersed sclerosis that was seen in the body of the D10 vertebra contiguously involving its posterior elements with cortical erosions and SUVmax 11.2 [Figure 2a and b]. Mild erosions in the adjoining right 10th rib with a solid periosteal reaction were also noted. Atrophy and fatty replacement of the bilateral leg muscles are incidentally seen, which is attributed to a known polyneuropathy. In addition, mild splenomegaly is noted with a span of about 15 cm with no obvious focal lesion, as well as diffuse subcutaneous edema secondary to fluid overload. A CT-guided biopsy of the D10 vertebral lesion was performed and found monoclonal plasma cell proliferation, further confirming the diagnosis of POEMS syndrome secondary to solitary plasmacytoma.
Figure 2.
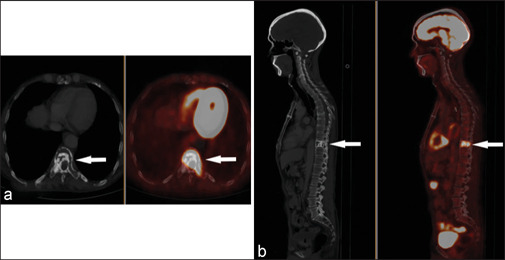
(a) Axial images and (b) sagittal images in the CT bone window and fused PET/CT in white arrows. The whole-body 18F-FDG PET/CT scan reveals a metabolically active (SUVmax 11.2) expansile-enhancing soft tissue osteolytic lesion with dense interspersed sclerosis in the body of the D10 vertebra contiguously involving its posterior elements with cortical erosions and solid periosteal reactions. Mild erosions of the adjoining right 10th rib were also noted
Conclusion
POEMS syndrome, also known as osteosclerotic myeloma, is a rare but treatable cause of polyneuropathy resulting from an underlying plasma cell disorder. The diagnosis of POEMS syndrome is made based on a composite of clinical, laboratory, and imaging features, which suggests a multisystemic involvement. Among the diagnostic criteria, sclerotic osseous lesions, organomegaly, and extravascular volume overload may be detected by imaging modalities. As a whole-body scan modality, 18F-FDG PET/CT has great advantages for evaluating many systemic diseases, especially hematologic diseases such as lymphoma and multiple myeloma that also involve multiple systems.[5] Our study showed that an 18F-FDG PET/CT scan could visualize many important features of POEMS syndrome, especially the diagnostic osseous lesion, splenomegaly, and changes in fluid overload.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Albertí MA, Martinez-Yélamos S, Fernandez A, Vidaller A, Narváez JA, Cano LM, et al. 18F-FDG PET/CT in the evaluation of POEMS syndrome. Eur J Radiol. 2010;76:180–2. doi: 10.1016/j.ejrad.2009.06.004. [DOI] [PubMed] [Google Scholar]
- 2.Montoriol PF, Cachin F, Michel JL, Soubrier M. Two more cases of evaluation of POEMS syndrome using 18-FDG PET/CT. Eur J Radiol. 2011;80:861–4. doi: 10.1016/j.ejrad.2010.04.030. [DOI] [PubMed] [Google Scholar]
- 3.Brown R, Ginsberg L. POEMS syndrome: Clinical update. J Neurol. 2019;266:268–77. doi: 10.1007/s00415-018-9110-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dispenzieri A. POEMS syndrome: 2017 update on diagnosis, risk stratification, and management. Am J Hematol. 2017;92:814–29. doi: 10.1002/ajh.24802. [DOI] [PubMed] [Google Scholar]
- 5.Pan Q, Li J, Li F, Zhou D, Zhu Z. Characterizing POEMS syndrome with 18F-FDG PET/CT. J Nucl Med. 2015;56:1334–7. doi: 10.2967/jnumed.115.160507. [DOI] [PubMed] [Google Scholar]