

ABSTRACT
Herbal products in dentistry have grown significantly. In the current scenario, herbal products are believed to be an effective adjunct to other medications. The present study aims to evaluate Eucalyptus oil and miswak (Salvadora persica) toothpaste for its efficacy in observable reduction in plaque and gingival bleeding. Sixty participants with gingivitis were enrolled in the present study. The study included an interim period (washout) comparing miswak and Eucalyptus toothpaste. Plaque scores were measured at designated time intervals. Both herbal toothpastes significantly decreased plaque index. Nevertheless, with relation to miswak (P = 0.002), Eucalyptus oil-based toothpaste exhibited reduction in bleeding scores. When participants were asked to return to their routine toothpaste, no changes were observed. Results from the study showed that the toothpaste containing Eucalyptus showed a significant decrease in gingival bleeding. More investigations should be looked on the medicinal applications of Eucalyptus toothpaste on commonly seen periodontal parameters.
Keywords: Dental related plaque, Eucalyptus, gingivitis, herbal toothpaste, miswak, Salvadora persica
INTRODUCTION
Dental plaque accumulation results in gingival inflammation and other oral diseases.[1,2] Chronic gingivitis is the most prevalent form. Redness, soreness, swelling, a glossy surface, and bleeding distinguish gingivitis clinically.[3] Due to its major advantages, the use of herbal medicine has increased significantly over the years. Herbal toothpaste such as miswak is popular when compared to conventional nonherbal kinds of toothpaste owing to their various characteristics, namely the presence of natural ingredients, alcohol-zero formulations, no artificial preservatives, and taste. They are proven to be efficient in decreasing plaque, gingival bleeding, and mouth odor.[4,5,6] Miswak is used for brushing in the form of a stick in most parts of the world and many studies have reported its bactericidal efficacy against anaerobic bacteria.[7,8]
Eucalyptus oil, procured from Australian Eucalyptus tree, produces an essential oil which is used to treat various diseases. Phytopharmacological process that includes drying, crushing, and distillation is used for extraction of essential components from Eucalyptus leaves.[9] Against Haemophilus influenzae and Staphylococcus pyogenes, Eucalyptus oil has high cytotoxic and antibacterial action.[10] Our study aims to investigate the efficacy of the selected herbal toothpastes regarding treatment of plaque and gingival bleeding.
MATERIALS AND METHODS
The study was approved by the University ethical committee (D-H-S-2021-NOV-24-19). The research was conducted from September 1, 2021, to January 10, 2022. It is registered on clinicaltrials.gov (NCT05363956). The two herbal toothpastes which were used in this randomized crossover clinical study: miswak toothpaste (Dabur, India) contains primarily miswak, with traces of essential oils; Eucalyptus toothpaste (Eucalyptus-Bio [Argiletz, France]) contains green illite clay, essential oils, and primarily Eucalyptus. The study was done in accordance with the Helsinki Declaration and further revised in 2013.
Patient selection
The sample size was determined using the PS program online version 3.16 (power and sample size calculations). A sample size of 30 was allotted for each group, putting the total number of participants at 60.[11] Participants medically fit, aged 20–60 years, with gingival inflammation (score of 1) were part of the inclusion criteria. Medically compromised patients taking medications for associated medical conditions, participants with periodontitis, participants who have received periodontal treatment in the past 6 months, and participants using herbal dentifrices were part of the exclusion criteria.
Study design
This study was conducted over 3 weeks. The study was a crossover randomized single-blind design. The participants were briefed, and consent was taken. Randomization for the study was done by drawing lots. To achieve blinding, lots were given and a code was incorporated to assign participants to their respective groups. An oral examination was done on all participants at the beginning of the trial (baseline). The baseline score and the scores at different time points in the 20 days duration were recorded and follow-up was maintained.
A dentifrice labeled with a number was given to the participants. The modified bass technique was taught to the patients and they were instructed to brush for 2 min with a 1 cm streak of paste and asked to perform brushing twice daily. A video of the technique was given and the technique further demonstrated. At the first visit during morning hours, the Oral Hygiene Index was calculated using, Simplified Oral Hygiene Index,[12] and the gingival index of all teeth[11] was recorded. Those patients who demonstrated bleeding scores of 2 and 3 in the initial examinations were excluded. All examinations were performed in the morning at all recall visits and done by the same examiner, as this helps in quantifying the results and reducing the risk of bias. The toothpaste was labeled as (1 Toothpaste) for miswak and (2 Toothpaste) for Eucalyptus oil.
Participants were instructed to use toothpaste one morning and night for 72 h. Three days later, evaluation was done for gingival bleeding and plaque. The 3 days study design was developed based on the 72 h plaque accumulation model by Marchetti et al.[13] Furthermore, to determine efficacy of the dentifrices, at the start of the study (baseline), oral prophylaxis was not performed and this was further validated by a landmark study by Page and Schroeder where gingivitis was observed on the 7th day.[14]
Following a 2-week washout period and to further prevent any bias in the outcome of our study, the participants were advised to use their routine toothpaste during the washout period and do not use any other herbal paste. To mitigate the possibility of bias, it was observed from previous studies that the interim (washout) period is at least five times more than the treatment’s half-life.[15] At the baseline of toothpaste 2, the gingival and plaque scores of the participants were assessed.
Both herbal toothpastes (Eucalyptus-Bio, Argiletz, France) were given and instructed to be used for the next 3 days, twice a day. Plaque as well as gingival bleeding was evaluated 72 h after brushing in the morning [Figure 1].
Figure 1.
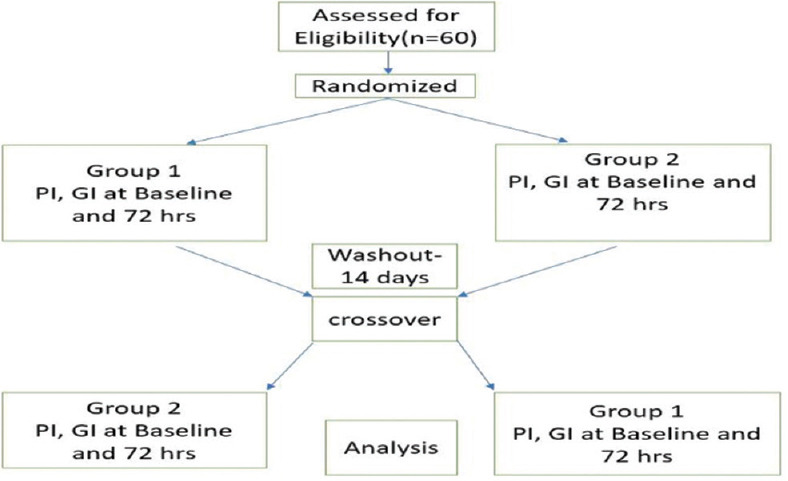
Flowchart
RESULTS
Analysis was done using SPSS software (version 28, Armonk, IBM Corp., New York, USA). Mann–Whitney U-test was used for intragroup comparison. Wilcoxon signed-rank test was performed for evaluation among the visit in each group to evaluate plaque and gingival index scores. P ≤ 0.05 was considered statistically significant.
Significant efficacy in plaque reduction was shown by both miswak and Eucalyptus paste [Tables 1 and 2], there was no statistical difference among the two. During the third visit [Table 2], participants were asked to use their routine toothpaste, scores of P = 0.083 and P = 0.636 were seen for miswak and Eucalyptus toothpaste, respectively.
Table 1.
Comparison of plaque index between the toothpastes at each time point
| Group 1 | Group 2 | P | |||
|---|---|---|---|---|---|
|
|
|
||||
| Median | IQR | Median | IOR | ||
| Baseline | 0.41 | 0.25–0.67 | 2 | 1.67–2.67 | <0.001* |
| After miswak (72 h) | 0.33 | 0.25–0.5 | 1.67 | 1.45–2 | <0.001* |
| Oral hygiene (washout period-14 days) | 0.42 | 0.25–0.42 | 1.67 | 1.5–1.83 | <0.001* |
| After Eucalyptus oil (72 h) | 0.31 | 0–0.5 | 1.3 | 1.2–1.67 | <0.001* |
*P<0.05 significance. IQR: Interquartile range
Table 2.
Comparison of plaque index at different time points in each group
| Miswak | Eucalyptus oil | |
|---|---|---|
| First-second | 0.002* | <0.001* |
| Second-third | 0.083 | 0.636 |
| Third-fourth | <0.001* | <0.001* |
| Second-fourth | <0.001* | <0.001* |
*P<0.05 significance
When Plaque scores (PS) were compared between each visit, comparable difference was observed among both toothpaste, P < 0.05. Both groups exhibited significant changes in PS, comparing the second from the fourth visit. There was no statistically significant observation made in PS when seen overall between the pastes, as both exhibited equal efficacy [Tables 1 and 2].
A significant finding was seen when evaluated among visits between the group along with observable change in gingival bleeding (GB) among the groups (P < 0.001) [Table 3]. There was a further observable difference in gingival bleeding values among the groups when observed from baseline to the fourth visit. Comparing Eucalyptus (0.001) in reducing gingival bleeding, miswak was less (0.008) when evaluating the time points – second and fourth visit [Table 4].
Table 3.
Comparison of a gingival index among the toothpastes at each time points
| Group 1 | Group 2 | P | |||
|---|---|---|---|---|---|
|
|
|
||||
| Median | IQR | Median | IQR | ||
| Baseline | 0 | 0–1 | 2.5 | 2–3 | <0.001* |
| After miswak (72 h) | 0 | 0–1 | 2 | 1–2 | <0.001* |
| Oral hygiene (washout period-14 days) | 0 | 0–1 | 1 | 1.75–2 | <0.001* |
| After Eucalyptus oil (72 h) | 0 | 0–1 | 1 | 1–2 | <0.001* |
*P<0.05 significance. IQR: Interquartile range
Table 4.
Comparison of gingival index at different time points in each group
| Miswak | Eucalyptus | |
|---|---|---|
| First-second | 0.025* | <0.001* |
| Second-third | 0.564 | 0.157 |
| Third-fourth | 0.014* | <0.001* |
| Second-fourth | 0.008* | <0.001* |
*P<0.05 significance
DISCUSSION
A study to evaluate miswak toothpaste when compared with another herbal paste (Paradontax) and a control routine chemical formulated paste (Colgate) was done.[16] There were no significant variations in approximal plaque index when compared to the Sulcus Bleeding Index (SBI) between any of the three groups. Compared to routine control, the herbal pastes reduced the SBI significantly. This was in agreement with the present study, where Eucalyptus oil-based toothpaste significantly reduced gingival bleeding when compared to miswak, but nevertheless did not show reduction in PS. In the current experimental study when patients were placed in the washout period and instructed to use their routine toothpaste, no significant effect on plaque or gingival indices was observed.
The values obtained in our current study are consistent with an earlier study where utilizing miswak chewing gum along with scaling or without prophylaxis resulted in a significant gingival bleeding reduction.[17]
No oral health benefits were reported in another study which involved miswak toothpaste. A likely reason is miswak paste’s active ingredients being lost during manufacturing.[18] A similar study using a randomized clinical crossover design to evaluate Moringa oleifera paste with miswak toothpaste, showed observable reduction in gingival bleeding and PS with relation to Moringa toothpaste, the values obtained in our study correlated to this, although the active ingredient was Eucalyptus oil-based paste.[6]
Retarding biofilm formation, bacterial adherence, and gingival inflammation were reported in studies related to Eucalyptus camaldulensis and Mentha spicata essential oils. This further strengthened the finding that essential oils can influence the development in biofilm and further help in the development of anticaries treatments.[19] In cancer patients with necrotic ulcers, when given Eucalyptus oil rinse and was instructed to rinse twice a day, it resulted in elimination of foul smell and complete reepithelialization where in some individuals the ulcers began to heal.[20,21] No evidence of extrinsic tooth stain with both herbal dentifrices was reported along with no adverse reactions seen throughout the duration of the study.
The duration of the study and the number of participants were some of the possible limitations in the current study. Maximal therapeutic benefit may not have achieved as the herbal dentifrices were given for 3 days only. Participants that were given miswak toothpaste reported a bland taste, whereas participants reported pleasant taste when given Eucalyptus toothpaste and they were willing to continue using it. Moreover, less significant gingival and PS shown by miswak when compared to Eucalyptus toothpaste could be due to the unpleasant taste of miswak, thereby possibly reducing the use of miswak paste by the participants. Furthermore, to understand the clinical performance of these herbal toothpastes, studies can be performed using larger sample size and longer time points.
CONCLUSION
An active role was demonstrated by both herbal toothpaste in terms of gingival bleeding and plaque. In contrast to the high quantity of research done with relation to miswak, sparingly few have been published on the effects of Eucalyptus in the oral cavity. Further research on the efficacy of Eucalyptus oil is needed.
Institutional ethical review
D-H-S-2021-NOV-24-19.
Data availability
The current study is registered on clinicaltrials.gov (NCT05363956).
Financial support and sponsorship
The study is self-funded.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Haque MM, Alsareii SA. A review of the therapeutic effects of using miswak (Salvadora persica) on oral health. Saudi Med J. 2015;36:530–43. doi: 10.15537/smj.2015.5.10785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Marsh PD. Plaque as a biofilm: Pharmacological principles of drug delivery and action in the sub- and supragingival environment. Oral Dis. 2003;9(Suppl 1):16–22. doi: 10.1034/j.1601-0825.9.s1.4.x. [DOI] [PubMed] [Google Scholar]
- 3.Trombelli L, Farina R, Silva CO, Tatakis DN. Plaque-induced gingivitis: Case definition and diagnostic considerations. J Periodontol. 2018;89(Suppl 1):S46–73. doi: 10.1002/JPER.17-0576. [DOI] [PubMed] [Google Scholar]
- 4.Muntean A, Sava S, Delean AG, Mihailescu AM, Dumitrescu LS, Moldovan M, et al. Toothpaste composition effect on enamel chromatic and morphological characteristics: In vitro analysis. Materials (Basel) 2019;12:2610. doi: 10.3390/ma12162610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kumar G, Jalaluddin M, Rout P, Mohanty R, Dileep CL. Emerging trends of herbal care in dentistry. J Clin Diagn Res. 2013;7:1827–9. doi: 10.7860/JCDR/2013/6339.3282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Duarte K, Thomas B, Varma SR, Kamath V, Shetty B, Kuduruthullah S, et al. Antiplaque efficacy of a novel Moringa oleifera dentifrice: A randomized clinical crossover study. Eur J Dent. 2022;16:768–74. doi: 10.1055/s-0041-1736418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nordin A, Bin Saim A, Ramli R, Abdul Hamid A, Mohd Nasri NW, Bt Hj Idrus R. Miswak and oral health: An evidence-based review. Saudi J Biol Sci. 2020;27:1801–10. doi: 10.1016/j.sjbs.2020.05.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Al-Otaibi M. The miswak (chewing stick) and oral health. Studies on oral hygiene practices of urban Saudi Arabians. Swed Dent J Suppl. 2004;(167):2–75. [PubMed] [Google Scholar]
- 9.Dhakad AK, Pandey VV, Beg S, Rawat JM, Singh A. Biological, medicinal and toxicological significance of Eucalyptus leaf essential oil: A review. J Sci Food Agric. 2018;98:833–48. doi: 10.1002/jsfa.8600. [DOI] [PubMed] [Google Scholar]
- 10.Sharifi-Rad J, Sureda A, Tenore GC, Daglia M, Sharifi-Rad M, Valussi M, et al. Biological activities of essential oils: From plant chemoecology to traditional healing systems. Molecules. 2017;22:70. doi: 10.3390/molecules22010070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Löe H. The gingival index, the plaque index and the retention index systems. J Periodontol. 1967;38:l610–6. doi: 10.1902/jop.1967.38.6.610. [DOI] [PubMed] [Google Scholar]
- 12.Greene JC, Vermillion JR. The simplified oral hygiene index. J Am Dent Assoc. 1964;68:7–13. doi: 10.14219/jada.archive.1964.0034. [DOI] [PubMed] [Google Scholar]
- 13.Marchetti E, Mummolo S, Di Mattia J, Casalena F, Di Martino S, Mattei A, et al. Efficacy of essential oil mouthwash with and without alcohol: A 3-day plaque accumulation model. Trials. 2011;12:262. doi: 10.1186/1745-6215-12-262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Page RC, Schroeder HE. Pathogenesis of inflammatory periodontal disease. A summary of current work. Lab Invest. 1976;34:235–49. [PubMed] [Google Scholar]
- 15.Evans SR. Clinical trial structures. J Exp Stroke Transl Med. 2010;3:8–18. doi: 10.6030/1939-067x-3.1.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Azaripour A, Mahmoodi B, Habibi E, Willershausen I, Schmidtmann I, Willershausen B. Effectiveness of a miswak extract-containing toothpaste on gingival inflammation: A randomized clinical trial. Int J Dent Hyg. 2017;15:195–202. doi: 10.1111/idh.12195. [DOI] [PubMed] [Google Scholar]
- 17.Amoian B, Moghadamnia AA, Barzi S, Sheykholeslami S, Rangiani A. Salvadora persica extract chewing gum and gingival health: Improvement of gingival and probe-bleeding index. Complement Ther Clin Pract. 2010;16:121–3. doi: 10.1016/j.ctcp.2009.11.002. [DOI] [PubMed] [Google Scholar]
- 18.Quinlan R, Robson G, Pack AR. A study comparing the efficacy of a toothpaste containing extract of Salvadora persica with a standard fluoride toothpaste. J N Z Soc Periodontol. 1994;(77):7–14. [PubMed] [Google Scholar]
- 19.Rasooli I, Shayegh S, Astaneh S. The effect of Mentha spicata and Eucalyptus camaldulensis essential oils on dental biofilm. Int J Dent Hyg. 2009;7:196–203. doi: 10.1111/j.1601-5037.2009.00389.x. [DOI] [PubMed] [Google Scholar]
- 20.Warnke PH, Sherry E, Russo PA, Açil Y, Wiltfang J, Sivananthan S, et al. Antibacterial essential oils in malodorous cancer patients: Clinical observations in 30 patients. Phytomedicine. 2006;13:463–7. doi: 10.1016/j.phymed.2005.09.012. [DOI] [PubMed] [Google Scholar]
- 21.Nagata H, Inagaki Y, Tanaka M, Ojima M, Kataoka K, Kuboniwa M, et al. Effect of eucalyptus extract chewing gum on periodontal health: A double-masked, randomized trial. J Periodontol. 2008;79:1378–85. doi: 10.1902/jop.2008.070622. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The current study is registered on clinicaltrials.gov (NCT05363956).