

Abstract
Background and Aims
Pressure ulcer is a considerable health problem and is associated with an increased hospital length of stay (LOS), nursing effort, costs, and reduced quality of life. The aim of this analysis is to compare the economic, clinical, and nursing benefit after the implementation of the powered hybrid mattress Dyna‐Form Mercury Advance SMARTcare® in 2019 with the situation in 2017 (rental systems Arjo BariAir® and Arjo TheraKair Visio®, and purchased foam mattresses Arjo Simuflex®) using a single center.
Methods
In the framework of a budget impact analysis, a difference‐in‐difference approach was used to compare pre‐implementation longitudinal data (2017) with post‐implementation data (2019). The longitudinal data comprise the mattress resource use, patient characteristics, and LOS. The care effort was gathered based on a full survey of all 75 members of the nursing staff using the online tool “LimeSurvey.” In this survey, the resource use of the different mattress systems was identified in terms of time (minutes or days). This analysis was performed from the hospital perspective and included direct costs of mattress systems, Austrian diagnostic‐related group costs for the hospital stay and nursing staff costs for 2019.
Results
Based on 1253 patients “at‐risk,” the total yearly costs implementing the powered hybrid mattress amounts to 654,248€ compared with 901,469€ when using Arjo products. The budget impact shows a cost advantage of 247,221€. Furthermore, the powered hybrid mattress system leads to fewer nursing‐staff time in minutes per year (−1,031,097 min [1,993,204 vs. 3,024,302]); 242€ are saved per patient. Compared with the Arjo products, fewer inpatient cases of pressure ulcers (−44 cases [0 vs. 44]) were documented.
Conclusion
Despite the higher total outlay of costs associated with the powered hybrid mattress, the long‐term savings potential showed a significant cost advantage per annum for the single center. Therefore, the use of the hybrid mattress leads to considerable economic, clinical, and nursing benefits.
Keywords: Austria, economic evaluation, hospital stay, mattresses, pressure ulcer
Key points
The implementation of mattress systems supports pressure ulcer prevention and leads to a decrease in hospital length of stay, nursing effort, costs, and improved quality of life in inpatient settings.
The budget impact shows a considerable cost advantage when using the powered hybrid mattress.
1. INTRODUCTION
Pressure ulcers, also synonymous with decubitus ulcers, are defined as localized pressure injuries that are caused by damage of the skin and/or subcutaneous layers due to unrelieved shear, pressure, or friction. 1 , 2 In addition, the skin microclimate (airflow, skin moisture, as well as skin temperature between patient's skin and support surface) affects the skin structure and increases the risk associated with friction and shear. 3 , 4 Pressure injuries are classified by the European Pressure Ulcer Advisory Panel (EPUAP), National Pressure Injury Advisory Panel (NPIAP), and the Pan Pacific Pressure Injury Alliance (PPPIA). Their classification system of 2019 is based on six various stages (Table 1). 5 The pressure ulcer definition described in the International Classification of Diseases for Mortality and Morbidity Statistics of the World Health Organization 2019 is consistent with the pressure ulcer definition of the EPUAP/NPIAP/PPPIA listed in Table 1. 2
Table 1.
Six‐staged classification system of the EPUAP/NPIAP/PPPIA (2019).
| Stages | Definition |
|---|---|
| Stage 1 | Intact skin with a local appearance of nonblanchable erythema |
| Stage 2 | Partial‐thickness skin loss with exposed dermis |
| Stage 3 | Full‐thickness skin loss |
| Stage 4 | Full‐thickness skin and tissue loss with visible fascia, muscle, tendon, ligament, cartilage, or bone |
| Unstageable pressure injury | Full‐thickness skin and tissue loss that is obscured by slough or eschar so that the severity of injury cannot be confirmed until slough or eschar is removed |
| A deep tissue pressure injury | Local injury of persistent, non‐blanchable deep red, maroon, purple discoloration, or epidermal separation revealing a dark wound bed or blood‐filled blister |
In general, skin damage caused by pressure ulcer is a considerable health problem and is associated with an increased hospital length of stay (LOS), nursing effort, costs, and reduced quality of life. The occurrence of new cases of pressure ulcer is considered a significant quality indicator in the care of hospital patients or nursing home residents. In hospitals, patients in intensive care units have a higher risk of developing pressure ulcers than patients in other hospital wards. 6
Due to these purposes, various support surfaces are currently in use to minimize the risk of developing decubitus ulcers in inpatient settings. Therefore, the aim of this analysis is to compare the economic, clinical, and nursing benefit of the post‐implementation data regarding the powered hybrid mattress, referred to as hybrid mattress, Dyna‐Form Mercury Advance SMARTcare® purchased for the total bed capacity (116 beds) in 2019, with the pre‐implementation data of 2017 (rental systems Arjo BariAir® and Arjo TheraKair Visio®, and purchased foam mattresses Arjo Simuflex®) in a single center (LKH Südsteiermark; Bad Radkersburg; a hospital in the Austrian region of Styria).
This evaluation will help to inform whether the decision to move from a typical model of foam and dynamic air system rentals, to a hybrid system would have the desired outcomes of reducing total lifetime cost and budget impact to the facility, and have the additional benefit of comparatively reducing pressure ulcer cases.
2. MATERIALS AND METHODS
The model was constructed and analyzed by using Microsoft Excel 365 (Figure 1). The analysis was designed based on the consolidated health economic reporting standards. 7 Furthermore, this present evaluation was performed in consideration of the Budget Impact Analysis Good Research Practices published by the ISPOR Task Force, 8 as well as the Austrian health economic guidelines. 9 In the framework of this budget impact analysis, a difference‐in‐difference approach was used to compare the world with (2019) and the world without (2017) the hybrid mattress system. A difference‐in‐difference method is a quasi‐experimental modeling technique for juxtaposing various public health parameters like nonpharmacological medicinal treatments at two or more different time periods, 10 which is why this approach was used for comparing the various mattress systems in this budget impact analysis. Regarding the longitudinal‐data of 2017, the information comprises mattress resource use, patient characteristics, and LOS. In the present model, the time horizon for comparing the world with and without the hybrid mattress is 1 year (year 2019). The analysis was performed from the hospital perspective using a single center and the following direct cost components: costs of the various mattress systems, costs of human resources regarding the nursing staff, and Austrian diagnostic‐related group (DRG) costs for the hospital stay.
Figure 1.
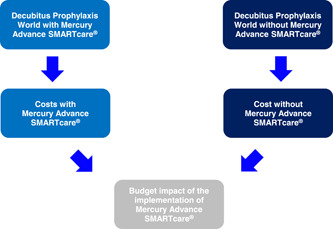
Model design for the budget impact analysis, indicating how the budget impact of the implementation of the powered hybrid device is derived.
2.1. Different mattress systems of the analysis
The Mercury Advance SMARTcare® (Direct Healthcare Group Ltd, Withey Court, Western Industrial Estate) provides dual therapy in a single surface for patients at very high risk of pressure ulcers up to 254 kg by combining clinically proven technologies previously only available in separate hybrid surfaces. Air displacement technology integrated into a four‐zone configuration, which can also be operated in unpowered mode, provides more effective pressure redistribution. The “air only” heel zone reduces pressure on the heel area. In dynamic mode, the hybrid mattress provides pressure relief through the interconnected alternating foam and air cells. 11
The Arjo Simuflex® (ArjoHuntleigh AB) is a static mattress system with a polyurethane core. It includes a reversible four‐way turn and the core is protected by a two‐way stretch, vapor permeable, water‐resistant cover. 12
The Arjo TheraKair Visio® is a low air loss therapy system which also includes pulsation therapy for miming natural body movements, stimulating lymph and blood flow for the prevention of skin damage, controlling the skin microclimate, and preventing edema. 13
The Arjo BariAir® is a therapy system designed for managing different risk factors of obese and immobile patients (136–386 kg). It consists of a low air loss therapy system for pressure control combined with pulsation and percussion therapy for pulmonary functioning as well as built‐in scales to weigh patients. 14
2.2. Simulated cohort (epidemiology)
In 2019, the epidemiological calculation was based on the total number of hospital admissions at the single center which was 4991 cases. 15 The average (25.1%) of the Braden scale (34.9%) and clinical gaze (15.3%) was used for identifying ~1253 patients who have a potential risk of developing a decubitus ulcer (patients “at‐risk”). 6 The Braden scale is a standardized tool for assessing the risk of pressure ulcer. 6 , 16 Out of the 1253 patients “at‐risk,” the prevalence with a type of decubitus ulcer was based on all categories of the Braden scale. Subsequently, these patients with a type of decubitus ulcer were categorized into those who developed their pressure ulcer injury before or after the hospital admission. According to the classification system of the EPUAP/NPIAP/PPPIA listed in Table 1, the 44 patients who developed their pressure ulcer injury after the hospital admission were subclassified based on the six‐staged distribution of decubitus ulcer cases in percentages at general hospitals (Figure 2). 6
Figure 2.
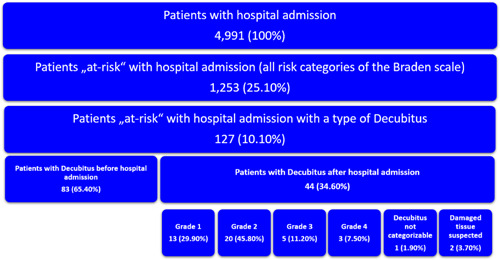
Patient flow of decubitus ulcers at the single center, showing the number of patients admitted to the hospital within the study period, those who developed a pressure ulcer (split between present on admission, and developed after admission), and the categorization of the pressure ulcers that were developed after hospital admission. Source: [6, 15].
2.3. Survey of the nursing staff
In 2019, a full survey with a sample size comprising all members of the nursing staff of the single center was conducted. At the single center, the total number of nursing staff members consisted of 75 individuals in 2019 and all 75 members participated in this survey. Therefore, no sample size calculator was used. The aim of this survey was to identify the total amount of care‐effort needed in terms of time (minutes or days) associated with the Arjo products (2017) and the hybrid system (2019) at the single center 17 (Table 2). Due to this survey, the decision‐making and provision of each mattress system in minutes per patient and day, the number of repositioning in minutes per patient and day, the time of cleaning and disinfection per patient in minutes per day and week, and the time of documentation per patient and day in minutes were identified. In addition, the average hospital stay per mattress system was determined as part of this employee survey. 17 Therefore, this was solely a resource use survey of the parameters associated with the use of the different mattress systems.
Table 2.
Results of the nursing staff survey in terms of the temporal resource use of different mattress systems in 2019.
| Mattress systems | Decision making and provision (in minutes) | Repositioning (minutes per day) | Cleaning and disinfection (minutes per day) | Documentation (minutes per day) | Subtotal temporal nursing staff resources per patient and system (minutes per day) | Inpatient LOS (in days) | Total temporal nursing staff resources per patient and system (in minutes) |
|---|---|---|---|---|---|---|---|
| Dyna‐Form Mercury Advance SMARTcare® | 0.00 | 131.47 | 5.09 | 70.12 | 206.68 | 7.70 | 1591.07 |
| Arjo rental systems BariAir® | 120.45 | 164.67 | 4.77 | 72.82 | 242.26 | 7.98 | 2054.49 |
| Arjo rental systems TheraKAir® | 120.45 | 164.67 | 4.77 | 72.82 | 242.26 | 7.98 | 2054.49 |
| Arjo Simuflex® | 47.10 | 271.36 | 4.93 | 71.47 | 347.76 | 7.84 | 2773.81 |
Note: Bold values represent the subtotal and the total temporal nursing staff resources per patient and system in minutes.
Abbreviation: LOS, length of stay.
Source: [17].
The tool that was used to conduct this specific resource use survey was an own developed questionnaire by the authors of this study (see Supporting Information S1: Appendix S1). Before the submission of this questionnaire to the 75 nursing staff members, a pretest was performed with three experts (two nursing experts and one expert for medical technology) for the purpose of validation. The entire duration of this pretest phase was 1 month. After the revision of the own developed resource use questionnaire, the full survey was initiated using “LimeSurvey,” a tool for conducting online surveys by submitting an online link to a participant for filling out a questionnaire. This online survey tool generated an online link which was submitted to the head of the nursing staff at the single center who forwarded this online link to all the 75 members of the nursing staff who participated in this resource use survey. The entire survey duration was three and a half months (Start: middle of August 2019; Closed: at the end of November 2019). All 75 members of the nursing staff completed the online survey (response rate of 100%).
During the analysis of this questionnaire, an arithmetic mean was calculated for all parameters which were relevant for identifying the resource use of the different mattress systems (the hybrid mattress system and the rental system Arjo TheraKair Visio®). Furthermore, the mean values were normally distributed by using a standard deviation and a significance level of 5%. This test was two‐sided and a T distribution was used for the confidence intervals. In addition, Microsoft Excel 365 was considered for the calculation. The underlying mean values and confidence intervals are shown in the Supporting Information S1: Appendix Table S2. Regarding the Arjo products which are not included in the resource use survey (Arjo Simuflex® and Arjo BariAir®), for these two Arjo products assumptions in terms of time estimates and work estimates were used. 18 , 19 Those estimates were made in consultation with two nursing experts of the single center. Therefore, the assumptions in terms of time estimates and work estimates were within the range of the confidence interval associated with Arjo TheraKair Visio® for the corresponding parameter in the resource use survey. Due to this fact, those estimates could be classified as plausible (see Supporting Information S1: Appendix Tables S3–S7).
2.4. Resource use and cost assessment
At the single center, the complete capacity of 116 beds was equipped with the hybrid mattress but only 50% of these mattresses required a pump in 2019. 20 In total, 40 beds were equipped with Arjo products in 2017. 21 The financial burden, which was associated with the acquisition and use of the Arjo products, and the purchase of the hybrid mattresses, were totally borne by the single center. Therefore, the analysis was performed from the hospital perspective.
The analysis includes costs of inpatient decubitus ulcer treatment, comprising costs of different mattress systems, inpatient costs of Austrian DRG codes main diagnosis group (HDG)19.07 (complicated affections of the skin) and HDG19.08 (simple affections of the skin) as well as nursing staff costs. 22
In the inpatient setting, resource use (e.g., the type and frequency of medical goods and services provided to patients), as well as monetary value (tariffs and prices) applied to each unit of medical goods and services were used to identify the total direct costs.
Regarding the hybrid mattress and the pump, the lifecycle period of 5 years was extracted from the user manual of the hybrid mattress. 11 This period is substantial for the calculation of the annual depreciation of these medical goods. The unit costs of a hybrid mattress and a pump as well as the maintenance costs associated with each pump were passed on in a written information of the Austrian distribution partner of the Direct Healthcare Group Ltd. 20 Furthermore, the number of units and unit costs, as well as the installation fees per unit of the Arjo products were submitted in a written information of the single center. In addition, the single center passed on the rent per day and the total number of days for both rental systems. 21
To identify the temporal resources per mattress system and patient stay, the results in terms of time of the nursing staff survey described in Table 2 were multiplied with the total patient distribution in percentages based on ~1253 patients “at‐risk,” which were extracted from the epidemiological calculations in Figure 2 and Section 2.2. Based on the number of units used in percent of each Arjo product and the hybrid mattress, these 1253 patients “at‐risk” were distributed in percent to identify the weighted total minutes per patient of the hybrid mattress and the Arjo products.
In 2019, the gross salary per minute of the nursing staff was derived from the KAGes salary scheme, as the resource use was primarily gathered in minutes. Furthermore, the ancillary fee, hazard, and hardship allowance of 2019 was included in the gross salary per minute of the nursing staff. 23 , 24 , 25 , 26 To derive the nursing staff costs of each mattress system and patient, as well as the total nursing staff costs, the results in terms of time described in Table 2 and Section 3.1 were multiplied with the gross salary per minute of the nursing staff of 0.29€ (Table 5). 17 , 23 , 24 , 25 , 26
Table 5.
Results of the nursing staff costs of the resource use of the Arjo products and the Mercury Advance system for the inpatient stay and per patient and system (in Euros 2019).
| Mattress systems | Decision making and provision (one‐off costs) | Repositioning (per day) | Cleaning and disinfection (per day) | Documentation (per day) | Subtotal nursing staff costs per patient and system (per day) | Inpatient LOS (in days) | Total nursing staff costs per patient and system |
|---|---|---|---|---|---|---|---|
| Dyna‐Form Mercury Advance SMARTcare® | 0.00 | 38.66€ | 1.50€ | 20.62€ | 60.77€ | 7.70 | 467.85€ |
| Arjo rental systems BariAir® | 35.42€ | 48.42€ | 1.40€ | 21.41€ | 71.24€ | 7.98 | 604.12€ |
| Arjo rental systems TheraKAir® | 35.42€ | 48.42€ | 1.40€ | 21.41€ | 71.24€ | 7.98 | 604.12€ |
| Arjo Simuflex® | 13.85€ | 79.79€ | 1.45€ | 21.01€ | 102.26€ | 7.84 | 815.63€ |
In the Austrian DRG system the main diagnoses are stated as case flat rates and each of these case flat rates comprise a daily component and a procedure component. Austrian DRG costs per decubitus ulcer case are presented as a weighted procedure component. This weighted parameter was derived using the procedure components of HDG19.07 (complicated affections of the skin) and HDG19.08 (simple affections of the skin). 22 These procedure components were weighted with the Austrian DRG point value of the KAGes, which was derived from KAGes annual reports. 27 , 28 , 29 , 30 , 31
3. RESULTS
3.1. Resources in terms of time
As a result, the hybrid mattress caused weighted total minutes per patient of 1591.07 and the Arjo products caused weighted total minutes per patient of 2414.15 (Arjo BariAir®: 51.36 min; Arjo TheraKair Visio®: 975.88 min; Arjo Simuflex®: 1386.90 min) resulting in temporal savings of 823.07 min per patient when using the hybrid mattress. Considering these weighted total minutes per patient for multiplication with the 1,253 patients “at‐risk” resulted in total minutes of 1,993,204.42 and 3,024,301.63 associated with the hybrid mattress and the Arjo products. Therefore, the comparison of these total minutes led to temporal savings of 1,031,097.20 min when using the hybrid mattress.
3.2. Costs
In 2019, the complete bed capacity of the single center was equipped with a hybrid mattress. According to the lifecycle period, the total costs per year of 68,150.00€ for 116 hybrid mattresses were based on the annual depreciation costs per hybrid system of 447.50€ and the annual maintenance costs per pump of 140.00€ 11 , 20 (Table 3).
Table 3.
Unit costs and total costs of the hybrid system (in Euros).
| Mattress systems | Lifecyle period (in years) | One‐off acquisition costs per unit | Maintenance per unit (per year) | Depreciation per unit (per year) | Total costs (per year) |
|---|---|---|---|---|---|
| Mattress | 5 | 1750.00€ | 0.00€ | 350.00€ | |
| Pump | 5 | 975.00€ | 140.00€ | 97.50€ | |
| Total | 2725.00€ | 140.00€ | 447.50€ | 68,150.00€ |
In 2017, the rental systems Arjo BariAir® and Arjo TheraKair Visio®, as well as the purchased foam mattresses Arjo Simuflex® were provided. The purchased foam mattresses Arjo Simuflex® are associated with total costs of 2134.00€. At the same time, the rental systems caused total costs of 2381.54€ (Arjo BariAir®) and 3074.11€ (Arjo TheraKair Visio®). 21 In total, the use of Arjo products led to total costs of 7589.65€ (Table 4).
Table 4.
Unit costs of the different Arjo products (in Euros).
| Mattress systems | Units or flat rates | One‐off acquisition costs per unit | Installation fee per unit | Rent per day | Days | Total costs (per year) |
|---|---|---|---|---|---|---|
| Arjo rental systems BariAir® | 1 flat rate | 179.26€ | 146.82€ | 15 | 2381.54€ | |
| Arjo rental systems TheraKAir® | 19 flat rates | 40.74€ | 14.74€ | 156 | 3074.11€ | |
| Arjo Simuflex® | 20 | 106.70€ | 2134.00€ | |||
| Total | 7589.65€ |
Source: [21].
Based on the Austrian DRG costs of the KAGes per decubitus ulcer case of 104.84€ (Table 6), the hybrid system and the Arjo products resulted in total costs of 0.00€ and 4589.82€. 6 , 22 , 27 , 28 , 29 , 30 , 31 In 2019, the hybrid mattresses prevented 100% of decubitus ulcer cases 32 whereas some decubitus ulcer cases were caused by the Arjo products (Figure 3).
Table 6.
Case flat rate of the Austrian DRG system 2019 for decubitus grade 1–4 and decubitus, not specified (in Euros 2019).
| Designation | Procedure component | Procedure component (population weighted) | Austrian DRG point value (KAGes) | Procedure components (KAGes) |
|---|---|---|---|---|
| Case flat rate (Decubitus grade 1 and not specified) | 47.00€ | 16.69€ | 0.74€ | 12.34€ |
| Case flat rate (Decubitus grade 2) | 238.00€ | 109.00€ | 0.74€ | 80.61€ |
| Case flat rate (Decubitus grade 3 and 4) | 86.00€ | 16.08€ | 0.74€ | 11.89€ |
| Population weighted average | 141.77€ | 104.84€ |
Figure 3.
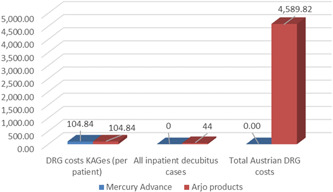
A graph displaying the DRG costs (KAGes) per patient, the number of inpatient decubitus cases, and the total Austrian DRG costs, split between the different product types, in Euros (2019). Source: [6, 15, 22, 27, 28, 29, 30, 31, 32].
Accordingly, the hybrid mattress caused nursing staff costs per patient of 467.85€ and the Arjo products caused nursing staff costs per patient of 709.88€ (Arjo BariAir®: 15.10€; Arjo TheraKair Visio®: 286.96€; Arjo Simuflex®: 407.82€) resulting in savings of 242.02€ per patient when using the hybrid mattress. Due to 1,253 patients “at‐risk,” the total nursing staff costs of 586,097.63€ and 889,289.62€ for the hybrid mattress as well as the Arjo products led to savings of 303,191.99€ associated with the hybrid mattress.
3.3. Budget impact analysis results
Based on 1253 patients “at‐risk” of developing decubitus, the total yearly costs implementing hybrid mattress amounts to 654,247.63€ compared to 901,469.09€ when using Arjo products. As a result, the budget impact shows a cost advantage of 247,221.47€ associated with the hybrid mattress (Figure 4).
Figure 4.
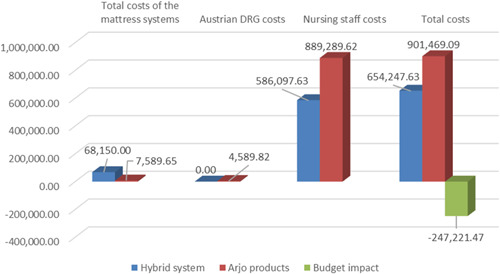
A graph displaying the results of the total costs of the mattresses systems, the total Austrian DRG costs, the total nursing staff costs, and the summation of all of these costs, in Euros (2019). This provides a final budget impact analysis result.
3.4. Payback period of the hybrid system
Regarding the payback period, the total costs of the hybrid systems of 68,150.00€ were divided by the total savings of the hybrid system of 307,781.82€, which comprise the difference in nursing staff costs (303,191.99€) and the difference in Austrian DRG costs of the KAGes (4,589.82€). Accordingly, the 116 hybrid mattresses were amortized after a period of ~80 days.
4. SENSITIVITY ANALYSIS
As economic data (in example pooled data sets, meta‐analyses, unverifiable assumptions) are usually incomplete and subject to uncertainty, assumptions are often made about certain parameter values. Therefore, it seems particularly important to perform a sensitivity analysis. Following this analysis, a test of the stability of the results is carried out. The assumptions and uncertain parameters are systematically changed to be able to consider the effects of this change on the result of the analysis. A one‐way sensitivity analysis (OWSA), also called univariate sensitivity analysis, is performed. As part of the OWSA, the values for uncertain parameters are systematically varied over a certain range to analyze their effects on the result. 33
In the scope of this sensitivity analysis, the following parameters were varied (only the top ten parameters, displayed in Figure 5, are described):
-
(1)
Arjo products total costs
-
(2)
Arjo products total personnel costs
-
(3)
Mercury Advance total costs
-
(4)
Mercury Advance total personnel costs
-
(5)
Mercury Advance total personnel costs per patient and system
-
(6)
Mercury Advance hospitalization
-
(7)
Patients at‐risk for pressure ulcers
-
(8)
Arjo Simuflex total personnel costs per patient and system
-
(9)
Arjo Simuflex hospitalization
-
(10)
Arjo Simuflex costs repositioning (min per day)
Figure 5.
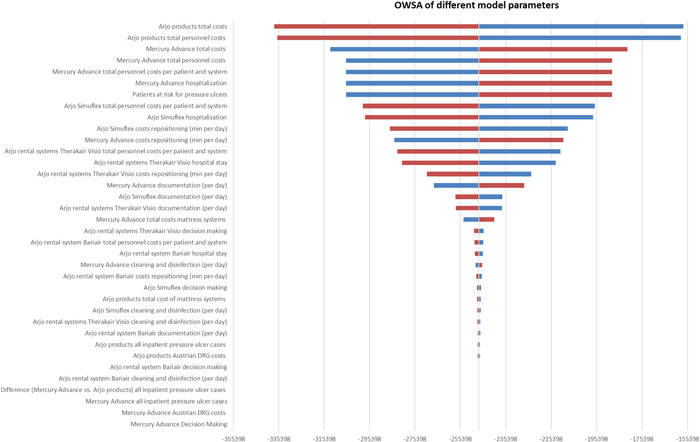
A graph displaying the results of the one‐way sensitivity analysis (OWSA) by showing the different model parameters with their effect on the budget impact in descending order. The vertical axis which separates the two horizontal bars is marking the budget impact. These normally distributed bars display their effect on the budget impact in descending order (Figure 5).
5. DISCUSSION
This economic evaluation was performed to analyze the budget impact of the implementation of the hybrid mattress Dyna‐Form Mercury Advance SMARTcare® in 2019 compared to the use of Arjo products (Arjo BariAir®, Arjo TheraKair Visio®, Arjo Simuflex®) in 2017. Despite the higher total costs of the mattress systems depicted in Figure 4, these saving potentials outline the considerable economic, clinical, and nursing benefits associated with the hybrid system in comparison with the Arjo products.
The key strength of this model is the real‐world character of the present analysis. In 2019, a full survey of 75 members of the nursing staff was conducted to measure the total amount of care‐effort needed in terms of time (minutes or days) associated with the Arjo products (2017) and with the hybrid system (2019) at the single center. 17 During this survey, it was possible to gather real‐world data on clinical resource use for each mattress system in terms of time (minutes or days) regarding the parameters listed in Table 2.
Another strength of this economic evaluation is the integration of the Austrian nursing quality survey of 2017 into the epidemiological calculation, 6 which was based on the total number of hospital admissions, accounting for 4991 cases, 15 at the single center in 2019. Furthermore, the actual KAGes gross salary scheme of the nursing staff in Styria and the associated ancillary fee, hazard and hardship allowance of 2019 were used in the present model. 23 , 24
A limitation of this analysis is the conduction of the nursing staff survey at only one center. Due to the use of a single center, a broader view over the situation in Austrian hospitals is missing. If this full survey had been conducted at multiple centers much more data on clinical resource use for each mattress system could have been gathered. Therefore, in the present analysis it is not possible to compare various hospitals with each other in terms of temporal resources and associated costs saved due to the use of the hybrid mattresses and the Austrian DRG costs saved due to the preventive effect against pressure ulcers associated with the hybrid mattresses. Moreover, the use of a multicenter approach would enable the comparison and weighing of budget impacts from multiple hospitals.
A further limitation of this analysis is the use of 100% prevention against pressure ulcers associated with the implementation of the hybrid mattress. This information originates from the publication “Gardner and Fletcher.” 32 Regarding different mattress systems for the prevention of pressure ulcers, it investigated the extent of the preventive effect before and after the implementation of the hybrid mattress over an entire period of 1 year. In the first 6 months, no hybrid mattress was used and 10 decubitus ulcer cases categorized as Stage 1 or Stage 2 (Table 1) were reported. However, when the hybrid mattresses were implemented on the 31 bedded ward, there could not any pressure ulcer be documented for the second half‐year. 32 Due to that circumstance, this 100% prevention rate against decubitus ulcers associated with the hybrid system was used in the present analysis although the time span of 6 months was too short to investigate the preventive effect of the hybrid mattress in detail.
Regarding this analysis, further limitations are associated with the full survey of the nursing staff. The authors of this study did not use a standardized questionnaire. The tool used for the full survey of the nursing staff was an own development by the authors because it was solely a resource use survey in terms of time spent while using different mattress systems (see Supporting Information S1: Appendix S1). Due to this fact, this own developed questionnaire could be associated with a bias. In addition, a reporting bias could also be associated with this survey because the information regarding the Arjo products used in 2017 as well as the information regarding the hybrid system used since 2019 were retrospectively gathered during the conduction of this resource use survey in 2019. Furthermore, these data were self‐reported for both years by each of the 75 members of the nursing staff at the single center. Therefore, they retrospectively estimated their time entries as well as their work entries associated with the different mattress systems used in 2017 and in 2019, which is why these entries could also be associated with a reporting bias.
Another limitation associated with this full survey is the fact that only two different (the hybrid mattress system and the rental system Arjo TheraKair Visio®) of the four various mattress systems described in this study were included in this resource use survey. During the pretest phase, it was the common opinion of the three experts that there is no significant difference between all Arjo products used in the present study regarding all topics included in the resource use survey. Therefore, the information gathered on the rental system Arjo TheraKair Visio® could be used to derive time estimates and work estimates for the remaining two Arjo products (purchased foam mattresses Arjo Simuflex® and rental system Arjo BariAir®).
Future research is needed to evaluate the use of the hybrid system over an extensive period in the Austrian health care and social care system. In addition, an economic model identifying the indirect costs saved from a patient and nursing staff perspective (loss of income, reduction in productivity, burden on informal caregivers) to derive the impact on the societal perspective due to the implementation of the hybrid mattress is needed.
6. CONCLUSION
The implementation of the hybrid mattress has a positive budget impact when compared to the use of previous systems that included static foam mattresses and the rental of dynamic alternating surfaces. Despite the higher total outlay of costs associated with the hybrid mattress, the long‐term savings potential showed a cost advantage of 247,221.47€ per annum. These savings can be derived from both temporal savings of 823.07 min per patient, the elimination of ongoing rental costs once the initial capital outlay has been made, as well as the comparative prevention of pressure ulcer development and the associated costs.
The implementation of the hybrid mattress offers the opportunity to reduce the massive work intensity and workload of the nursing staff by releasing considerable resources, in terms of time, to a physically and mentally more comfortable level. In this way, the nursing quality can be increased directly for each individual patient, solely by redistributing these free resources to other core nursing activities. As a result, the financial resources gained can in turn be invested in further measures which, on the one hand, contribute to the health promotion of the nursing staff and, on the other hand, increase the associated nursing quality. In summary, the implementation of the hybrid mattress provides a positive budget impact, reduces the enormous workload of the nursing staff, and leads to considerable economic, clinical, and nursing benefits.
AUTHOR CONTRIBUTIONS
All authors have read and approved the final version of the manuscript. Gerald Eichhober and Marco Voit had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
CONFLICT OF INTEREST STATEMENT
Evelyn Walter has received an educational grant from DHG ‐ Direct Healthcare Group Ltd. Gerald Eichhober, Franz Meyer, and Marco Voit have no conflict of interest regarding the subject matter or materials discussed in the present paper. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
TRANSPARENCY STATEMENT
The lead author Gerald Eichhober affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Supporting information
Supporting Information
ACKNOWLEDGMENTS
This work was supported by an unrestricted educational grant from DHG ‐ Direct Healthcare Group Ltd (Caerphilly, United Kingdom). Furthermore, we would like to thank Gepa‐Med Medizintechnik GmbH (Vienna, Austria) and LKH Südsteiermark (Bad Radkersburg), a hospital in the Austrian region of Styria, for supporting us with data that were used for calculations. DHG was not involved in any aspect of the study design, collection, analysis, interpretation of the data, or writing of the report. DHG did confirm their acceptance in the authors decision to submit the report for publication.
Eichhober G, Voit M, Meyer F, Walter E. A budget impact analysis of a powered hybrid mattress to prevent pressure ulcers in the Austrian inpatient setting: an original research. Health Sci Rep. 2024;7:e1887. 10.1002/hsr2.1887
Gerald Eichhober and Marco Voit contributed equally to this manuscript.
Contributor Information
Gerald Eichhober, Email: g.eichhober@ipf-ac.at.
Marco Voit, Email: m.voit@ipf-ac.at.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Gefen A, Brienza DM, Cuddigan J, Haesler E, Kottner J. Our contemporary understanding of the aetiology of pressure ulcers/pressure injuries. Int Wound J. 2022;19(3):692‐704. 10.1111/iwj.13667 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Shi C, Dumville JC, Cullum N, Rhodes S, Jammali‐Blasi A, McInnes E. Alternating pressure (active) air surfaces for preventing pressure ulcers. The Cochrane Database Syst Rev. 2021;5(5):CD013620. 10.1002/14651858.CD013620.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Kottner J, Black J, Call E, Gefen A, Santamaria N. Microclimate: A critical review in the context of pressure ulcer prevention. Clin Biomech. 2018;59:62‐70. 10.1016/j.clinbiomech.2018.09.010 [DOI] [PubMed] [Google Scholar]
- 4. Yusuf S, Okuwa M, Shigeta Y, et al. Microclimate and development of pressure ulcers and superficial skin changes. Int Wound J. 2015;12(1):40‐46. 10.1111/iwj.12048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. European Pressure Ulcer Advisory Panel (EPUAP), National Pressure Injury Advisory Panel (NPIAP) and Pan Pacific Pressure Injury Alliance (PPPIA) . Prevention and Treatment of Pressure Ulcers/Injuries: Quick Reference Guide. EPUAP/NPIAP/PPPIA; 2019. [Google Scholar]
- 6. Lohrmann C, Bauer S, Lampersberger L, et al. Pflegequalitätserhebung 2022 2.0 [Nursing quality survey 2022 2.0]. Medical University of Graz; 2023. [Google Scholar]
- 7. Husereau D, Drummond M, Augustovski F, et al. Consolidated health economic evaluation reporting standards 2022 (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. Value Health. 2022;25(1):3‐9. 10.1016/j.jval.2021.11.1351 [DOI] [PubMed] [Google Scholar]
- 8. Sullivan SD, Mauskopf JA, Augustovski F, et al. Budget impact Analysis‐Principles of good practice: report of the ISPOR 2012 budget impact analysis good practice II task force. Value Health. 2014;17(1):5‐14. 10.1016/j.jval.2013.08.2291 [DOI] [PubMed] [Google Scholar]
- 9. Walter E. Österreichische guidelines zur gesundheitsökonomischen evaluation. PharmacoEcon German Res Articles. 2006;4(2):55‐63. 10.1007/BF03321566 [DOI] [Google Scholar]
- 10. Wing C, Simon K, Bello‐Gomez RA. Designing difference in difference studies: best practices for public health policy research. Annu Rev Public Health. 2018;39:453‐469. 10.1146/annurev-publhealth-040617-013507 [DOI] [PubMed] [Google Scholar]
- 11. Direct Healthcare Group (DHG) Ltd . Mercury Advance SMARTcare®: a step change in care delivery (User manual). DHG; 2019. [Google Scholar]
- 12. ArjoHuntleigh . Simuflex®: 4‐Way Turn Mattress Replacement System (Instructions for Use). ArjoHuntleigh AB; 2021. [Google Scholar]
- 13. ArjoHuntleigh TheraKair Visio®: Mattress Replacement System (Instructions for Use). ArjoHuntleigh AB; 2019. [Google Scholar]
- 14. ArjoHuntleigh . BariAir® Therapy System (User Manual). ArjoHuntleigh AB; 2014. [Google Scholar]
- 15. Single Center . Written Information Regarding the Hospital Admissions in 2019 from the LKH Südsteiermark (Location: Bad Radkersburg), 2019a. [Google Scholar]
- 16. Zegelin A. Skalen zur Ermittlung des Dekubitusrisikos [Scales for determining the risk of decubitus ulcers]. In: Bienstein C, Schröder G, Braun M, Neander KD, eds. Die Herausforderung für Pflegende. Georg Thieme Verlag; 1997:81‐93. [Google Scholar]
- 17. Institute for Pharmaeconomic Research (IPF) . Employee Survey of the Nursing Staff in Terms of the Resource Use of Different Mattress Systems. LKH Südsteiermark; 2019. [Google Scholar]
- 18. Single Center . Oral Information Regarding the Use of Arjo Simuflex® from the LKH Südsteiermark (Location: Bad Radkersburg), 2019c. [Google Scholar]
- 19. Jones L, Fletcher J. Improved patient experience and outcomes using Dynaform Mercury Advance mattress. Wounds UK. 2014;10(3):88‐91. [Google Scholar]
- 20. Gepa‐Med Medizintechnik . Written Information Regarding the Powered Hybrid Mattress Dyna‐Form Mercury Advance SMARTcare® and its Pump, 2019. [Google Scholar]
- 21. Single Center . Written Information Regarding the Total Number of Arjo Products and the Installation Fees As Well As the Rent Per Day and the Total Rental Days Per Each Arjo Product from the LKH Südsteiermark (Location: Bad Radkersburg), 2019b. [Google Scholar]
- 22. Federal Ministry of Labour, Social Affairs, Health, and Consumer Protection . Leistungsorientierte Krankenanstaltenfinanzierung (LKF) System 2019: LKF Modell 2019 [Austrian DRG system 2019: Model 2019], 2019. [Google Scholar]
- 23. Legal Information System of the Republic of Austria . Gesamte Rechtsvorschrift für Dienst‐ und Besoldungsrecht der Bediensteten des Landes Steiermark [Entire legal regulation for service and salary law of the employees of the state of Styria], 2020a. [Google Scholar]
- 24. Legal Information System of the Republic of Austria . Gesamte Rechtsvorschrift für Erhöhung der Gehälter, Monatsentgelte und Zulagen der Beamten/Beamtinnen und Vertragsbediensteten im Steiermärkischen Landesdienst [Entire legislation to increase the salaries, monthly remunerations and allowances for officials and contract staff in the Styrian state service], 2020b. [Google Scholar]
- 25. Federal Ministry of Labour, Social Affairs, Health, and Consumer Protection . Pflegepersonal‐Bedarfsprognose für Österreich [Nursing staff demand forecast for Austria], 2019. [Google Scholar]
- 26. Styrian Hospital Institution (KAGes) . Gehaltsansätze 2019 [Salary scheme 2019], 2019b. [Google Scholar]
- 27. Styrian Hospital Institution (KAGes) . Geschäftsbericht 2014 [Annual report 2014], 2015. [Google Scholar]
- 28. Styrian Hospital Institution (KAGes) . Geschäftsbericht 2015 [Annual report 2015], 2016. [Google Scholar]
- 29. Styrian Hospital Institution (KAGes) . Geschäftsbericht 2016 [Annual report 2016], 2017. [Google Scholar]
- 30. Styrian Hospital Institution (KAGes) . Geschäftsbericht 2017 [Annual report 2017], 2018. [Google Scholar]
- 31. Styrian Hospital Institution (KAGes) . Geschäftsbericht 2018 [Annual report 2018], 2019a. [Google Scholar]
- 32. Gardner S, Fletcher J. An Investigation into the Use of Hybrid Mattress Technology to Reduce Pressure Ulcer (PU) Incidence and Costs. Intelligent Pressure Care Management; 2017.
- 33. Schöffski O, Schulenburg J. Gesundheitsökonomische Evaluationen [Health‐economic evaluations]. 4th edition. Springer Berlin; 2012. 10.1007/978-3-642-21700-5 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Information
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.